
COUNTY OF MENDOCINO HEALTH PLAN Administered by Delta Health Systems
COUNTY OF MENDOCINO HEALTH PLAN Summary Plan Description Effective January 1, 1994 Updated January 2008 Administered by Delta Health Systems HOW TO REACH US CUSTOMER SERVICE For medical claims status, benefit information, identification cards, claim forms or to change your primary care physician call: Employee Health Benefits Mendocino County Human Resources 707-463-4445 Please mail claims and correspondence to: Delta Health Systems P O Box 1199 Stockton, CA 95201-1199 Delta TeamCare– within Mendocino and Lake Counties or Out of the State of California For assistance and information regarding out of network referrals and prior authorizations, employees may contact Delta at (877) 464-1441 BLUE CROSS – outside of Mendocino and Lake Counties, within the State of California For assistance and information regarding prior authorizations, employees may contact Blue Cross at 1-800-274-7767 PRESCRIPTION DRUG CARD PROGRAM For questions on the program, please call: 1-800-711-0917 Mail your prescriptions to: Medco Health Solutions PO Box 3938 Spokane, WA 99220-3938 ELIGIBILITY AND ENROLLMENT For information concerning eligibility, when coverage begins and ends, life insurance issues, clarification of benefits, claims appeals and continuation of coverage call: Employee Health Benefits (707) 463-4445 EMPLOYEE ASSISTANCE PROGRAM (EAP) For assistance with personal, family or work problems, and referral for mental or emotional health treatment call: Employee Assistance Program (707) 468-3405 EMPLOYEE WELLNESS PROGRAM For health and wellness educational materials, for information about health risk assessments, for schedules of County employee programs, activities available to help you make health behavior changes, and to support you in maintaining your new lifestyle choice(s) call: (707) 463-4040 For copies of the health plan or related forms, please go to www.co.mendocino.ca.us/hr THIS PLAN IS NOT A GUARANTEE OF BENEFITS AND IS SUBJECT TO PROCESS CHANGES 2 TABLE OF CONTENTS Administrative Contacts……………………………………………………………………………………. 2 Summary of Benefits……………………………………………………………………. 6 The Health Plan……………………………………………………………...…… …….9 Eligibility………………………….………………………………………………………… 9 Enrollment……………………………………………………………………………….. 10 The Medical Plan Plan I……………………………………………………………………………………… 12 Plan II…………………………………………………………………………………….. 13 Primary Care Physicians……………………………………………………………… 14 Referrals………………………………………………………………………………….. 14 Prior Authorization………………………………………………………………… …...15 Case Management Services…………………………………………………………… 18 Mental Health……………………………………………………………………………. 18 Emergency Care………………………………………………………………………… 18 After-hours Assistance………………………………………………………………… 19 Pre-Existing Conditions……………………………………………………………….. 19 Covered Services…………..…………………………………………………………. ...20 The Dental Plan Benefit Determination…………………………………………………………………. 26 Alternate Procedures…………………………………………………………………… 27 Covered Services………………………………………………………………………… 27 The Vision Plan………………………………………………………………………… 29 Management & Confidential…………………………………………………………..29 Non-Management……………………………………………………………………….. 30 Covered Services (All]…………………………………………………………………. 31 The County’s Health Plan General Exclusions…………………………………………………………………….. 31 How to File a Claim………………………………………………………………………32 How Claims are Paid…………………………………………………………………….32 How to Appeal a Claim………………………………………………………………….33 Coordination of Benefits………………………………………………………………..33 Employee Assistance Program (EAP) How to Use the Program………………………………………………………………. 35 Prescription Card Program How to Use the Program………………………………………………………………. 35 COBRA Continuation of Coverage………………………………………………………………37 Disability Medical Care Benefit……………………………………………………….38 3 Dental Care Benefit After Termination………………………………………………………………….39 Layoff or Leave of Absence……………………………………………………………. 39 Life Insurance Plans Basic Life Accidental Death……………………………………………………………39 Eligibility…………………………………………………………………………..39 Coverage………………………………………………………………………….. 39 Exclusions……………………………………………………………………….. 40 How to File a Claim……………………………………………………………. 40 Claims Appeals…………………………………………………………………. 41 Conversion……………………………………………………………………… 41 Voluntary Term Life …………………………………………………………………… 41 Eligibility…………………………………………………………………………. 41 Coverage………………………………………………………………………….. 42 How to Apply……………………………………………………………………. 43 Conversion………………………………………………………………………..43 Portability………………………………………………………………………… 44 Beneficiary……………………………………………………………………….. 44 How to File a Claim……………………………………………………………. 44 Claims Appeals…………………………………………………………………. 44 Voluntary Accidental Death……………………………………………………………44 Eligibility…………………………………………………………………………. 44 Coverage………………….………………………………… ……………………45 How to Apply………………………………….…………… ……………………46 Additional Benefits…………………………………………………………….. 47 Education……………………………………………………………….. 47 Spouse Training……………………………………………………….. 48 Coma Benefit………………………………… …………………………48 Seatbelt Benefit……………………………… …………………………48 Felonious Assault…………………………… …………………………49 Conversion………………………………………………………………………..49 Definitions……………………………………………………………… ……………….49 4 SUMMARY OF BENEFITS The following is only a summary of benefits under the County of Mendocino’s Health Plan. Please refer to the various plans in this book for specific information and limitations. You should familiarize yourself with the rest of this booklet before you need services so that you will understand the benefits and your responsibilities for meeting Plan requirements. Preventive/ Diagnostic DENTAL PLAN 100%, no deductible Annual Deductible $25 per person $75 per family for services other than Preventive and certain Diagnostic & Therapeutic General Services 85% Major Restorative 50% Annual Benefit Limit $1,500 per person VISION PLAN Eye Exams 1 every 12 months/$60 maximum Eyeglasses Lenses 1 lenses every 24 months Single vision $60 maximum Bi-focal $80 maximum Tri-focal $100 maximum Lenticular $200 maximum Eyeglass Frames 1 set every 24 months/$60 maximum Contact Lenses (per pair) $400 if medically necessary $110 if other 5 LIFE INSURANCE PROGRAMS Basic Life $20,000 General Employees $50,000 Appointed and Elected Department Heads/Unrepresented Employees, DSA, & MCLEMA Accidental Death & Dismemberment $5,000 General Employees $50,000 MCLEMA & DSA Voluntary Term Life Employee – Can purchase units of $10,000 to the greater of 5 times salary or $300,000 Guarantee Issue Limit–$100,000 Spouse-Units of $10,000 to $250,000 Dependent Children over age 6 months – Units of $2,000 to $10,000 Dependent Children between age 14 days and 6 months–$500 Completely portable 6 MEDICAL PLANS PLAN I PLAN II Annual Deductible $350 individual/$1050 family $500 individual/$1500 family Annual Out-of-Pocket Max (including deductible) $3,000 per person/$6,000 family $4,000 per person/$8,000 family Co-Insurance 85% of allowable in network/ 70% of UCR out-of-network 80% of allowable in network/ 60% of UCR out-of-network Emergency Room Visits $50 co-pay does not count toward deductible nor out of pocket maximum $50 co-pay does not count toward deductible nor out of pocket maximum Hospital Precertification (required in all plans) $200 deductible for non precertification $200 deductible for non precertification Second Surgical Opinion Recommended, paid at 100% No deductible Recommended, paid at 100% No deductible Pre-Admission Testing Paid 100%, No deductible Paid 100%, No deductible Prescriptions—Generic Brand-Formulary Brand Non-formulary $10 or 10% $20 or 20% $30 or 30% Co-payments do not apply toward your deductible or out of pocket max. $10 or 10% $20 or 20% $30 or 30% Co-payments do not apply toward your deductible or out of pocket max. Wellness Benefits Paid 100% no deductible; Annual exams (physical, pap smears, mammograms, PSA tests, blood tests, wellness counseling) Childhood Immunization Well Baby (10 visits to age 2) Related Lab & X-rays – for preferred providers only. Paid 100% no deductible; Annual exams (physical, pap smears, mammograms, PSA tests, blood tests, wellness counseling) Childhood Immunization Well Baby (10 visits go age 2) Related Lab & X-rays – for preferred providers only. Nervous/Mental Outpatient: 60% of allowable in-network/50% of UCR out network; 52 visits/calendar year. Inpatient: Same as other illnesses Max. 28 days/ calendar year. Outpatient: 60% of allowable in-network/50% of UCR out network; 52 visits/calendar year. Inpatient: Same as other illnesses Max. 28 days/ calendar year. Drug/Alcohol Inpatient and Outpatient: $16,000 annual benefit $50,000 maximum benefit You must complete treatment before plan will pay. Inpatient and Outpatient: $16,000 annual benefit $50,000 maximum benefit You must complete treatment before plan will pay. Employee Assistance Program EAP is a preferred provider, 6 free visits, then 60% EAP is a preferred provider, 6 free visits, then 60% 7 THE HEALTH PLAN WHO IS ELIGIBLE? Employee You are eligible if you are a full-time employee or you are employed in a permanent position, which is allocated for a minimum of 16 hours per week. Dependents Your eligible dependents are: • Your wife or husband. • Your Domestic Partner (see Human Resources Website for details www.co.mendocino.ca.us/hr/). • Your unmarried children under 19. • Your unmarried children 19 or older, but under the age of 25, who are registered students enrolled in 12 or more units at school.. Dependents who are students must be primarily dependent on you for care and support. They cannot be employed on a regular full-time basis by one or more employers for a total of 30 or more hours per week. Delta Health Systems will request proof of full-time student status from a dependent for Fall and Spring semesters each year. If Delta does not receive this information within 30 days the dependent will be dropped from the health insurance plan (see COBRA). Dependent children also include: • Your stepchild. • Your legally adopted child (including a child for whom legal adoption proceedings have been started). • Any other child who is related to you by blood or marriage, who is mainly dependent on you for care and support, and living with you in a parent-child relationship. • Any other child for whom you are required to provide health plan coverage under a Qualified Medical Child Support Order. If husband and wife are both eligible as employees only one may cover their dependents for the dependents benefits. WHEN DOES COVERAGE BEGIN? As a new employee, you must enroll within 31 days of eligibility. If you enroll any dependents on your health plan you must submit proof of dependency ie, marriage certificate, birth certificate, domestic partner registration form with the enrollment form If you choose not to enroll in the health plan, you must complete an Opt Out form and must submit it along with proof of coverage under another plan within 31 days of eligibility. If you do not complete an enrollment form or submit an Opt Out form within the time limit you will automatically be enrolled in Plan II (employee only) Turn in all forms and documentation to Employee Health Benefits. Employees with dependent children under the age of 19 who have applied for the Healthy Families Program will have 90 days in which to enroll those dependent children. For more information on the Healthy Families Program, please contact the Public Health Department at (707) 463-4461. The only time you may make changes to your election is during the County’s annual open enrollment period in November or December of each year. The exception is a qualified change in family status. Qualified change includes marriage, divorce, birth, death, 8 adoption, loss or gain of other health insurance, or a qualified change in the employment status of yourself or your spouse/domestic partner. Your coverage begins on the latest of: • The first day of the pay period after the pay period in which you start work. • The date you enroll for any contributory coverage. Your dependents’ coverage starts on the latest of: • The date you become covered. • The first day of the pay period after you acquire your first dependent. • The date you enroll for the dependents’ coverage. • You must enroll newborn children within 30 days of birth. Adopted children must be enrolled within 30 days of placement. Dependent children under age 19 for whom the employee has applied for coverage under the Healthy Families Program within 30 days of eligibility may be enrolled in the County’s plan up to 90 days after initial eligibility. You will have to wait until the next open enrollment if you don’t enroll your dependent within 31 days of eligibility unless employees with dependents have applied for the Healthy Families Program in which they will have 90 days to enroll. HOW TO ENROLL FOR COVERAGE You enroll by submitting an enrollment form. You must enroll yourself in order to enroll your dependents. If you acquire a dependent after you initially enroll, you may enroll for the newly acquired dependent’s benefits as soon as he or she becomes eligible. Any employee or dependent who originally declined coverage under this Plan because they had coverage under another medical plan and who subsequently loses coverage under the other plan, may be able to enroll in this plan, provided the individual meets all of the following requirements: • The individual was covered under another health benefit plan at the time that individual was eligible to enroll in this Plan; • The individual certified at the time of initial eligibility that he or she had coverage under another health plan and this was the reason for declining coverage; • The individual has lost or will lose coverage under another employer health benefit plan as a result of termination of employment or change in employment status of the individual or of a person through whom the individual was covered as a dependent, termination of other plan’s coverage, significant change in coverage, reduction of hours, cessation of an employer’s contribution toward an employee or dependent’s coverage, death of a person through whom the individual was covered as a dependent, legal separation or divorce; • The individual requests enrollment within 30 days of losing the other coverage; and • A certificate of creditable coverage is provided by the previous insurance plan. Coverage will become effective on the first day of the next pay period following the date the documents are received by Employee Health Benefits. WHEN DOES COVERAGE END? Coverage will stop on the earliest of the following: • The last day of the pay period in which your employment ends. • The first day of the pay period in which you stop being an eligible employee. 9 • When the plan stops. When you stop being an active employee, contact Employee Health Benefits about what rights you have to continue coverage. Coverage for all of your dependents ends when your coverage ends or when you stop making contributions, whichever happens first. • Coverage for an individual dependent stops sooner if one of the following happens: • The dependent becomes covered as an employee under this plan, or • He or she is no longer your eligible dependent. A mentally or physically handicapped child’s health coverage will not stop due to age. It will continue as long as your dependent coverage continues and the child continues to meet the following conditions: • The child is handicapped. • The child is not capable of self-support. • The child depends mainly on you for support. You must give Delta Health Systems proof that the child meets these conditions when requested. Delta Health Systems will not ask for proof more than once a year. Delta Health Systems will provide you and your dependents with a certificate of prior coverage when your coverage ends, your employment terminates or your COBRA coverage ends. You have the choice of two medical plan options: Plan I and Plan II, each of which provides a different level of premium payment and benefits. This gives you the flexibility to choose the medical coverage that best suits your needs. Our medical plans emphasize managed care, which means that the medical services you use are guided by a primary care physician (PCP). Like the family doctor from an earlier era, the PCP will be your health care partner, treating most of your problems, keeping track of your medical history, performing annual physical exams, and referring you to specialists when appropriate. The plans are designed so that you will get the highest benefit when your PCP manages your care. The medical plan is administered by Delta Health Systems. The plan contains a managed care network through the Foundation for Medical Care (FMC). The plan also has a statewide hospital network and a network of preferred doctors outside Mendocino County, which is provided by Blue Cross Network. If you would like to check to ensure you are receiving care by a Blue Cross provider please log onto www.bluecrossca.com WHAT DOES THE PLAN PAY? In many ways, you can control the level of benefit you receive. First of all, the medical plan option you choose at enrollment time will make a difference in how much the plan pays. Secondly, you will receive the highest benefit if you use network providers. You always have the freedom to go to any licensed provider, but you receive a higher benefit for using a preferred provider. The maximum medical benefit per lifetime, per enrollee is $2,000,000.00. 10 If you are seeking services within Mendocino County FMC will be the preferred network. If you are seeking services outside of Mendocino County but within the State of California, Blue Cross will be the preferred network. If there are no primary care physicians in the County where you or your dependents live in California, or if you or a dependent lives outside of the state, you will receive benefits at the network (or higher) level. Finally, you must remember to coordinate all your medical care through your primary care physician. By teaming up with your primary care physician, you will receive the highest benefit in the plan. It’s important to remember, however, that you will still receive a benefit if you would rather visit a non-network provider or bypass the primary care physician. Your out-ofpocket costs will just be higher for that expense. For example: The difference between the amount billed by a non-preferred provider and what is usual and customary becomes your responsibility and does not count toward your deductible nor your out of pocket maximum. The following two sections highlight the payment levels of the various plan options. PLAN I • • • • • • • • • • • • • • There is a $350 per individual ($1050 per family) annual deductible. The plan pays 85% of allowable for most network services. The plan pays 70% of UCR for non-network services. Your maximum out-of-pocket expense is $3,000 per person/$6,000 family per year, including your deductible. The plan pays 60% of allowable charges for preferred providers and 50% of usual, customary, and reasonable (UCR) charges for non-preferred providers when treating covered outpatient nervous and mental disorders up to a maximum of 52 visits per calendar year. Your expenses for outpatient mental and nervous treatment do not count toward your annual out-of-pocket limit. Inpatient nervous and mental care is paid up to a maximum of 28 inpatient days per calendar year. Inpatient and outpatient chemical dependency (alcohol and drug treatment) is paid as any other illness. The combined outpatient and inpatient maximum payable for covered alcohol and drug treatment is $16,000 per calendar year and $50,000 per lifetime. You must complete treatment before the plan will pay. Wellness and preventive care is covered at 100% with no coinsurance or deductible for preferred providers only. The Employee Assistance Program (EAP) is available through the County. The first six visits to the EAP are free to you and your covered dependents. Hospital prior authorization is required. There is a $200 deductible for failure to obtain prior authorization. Pre-admission testing is paid at 100% with no deductible. Emergency Room Co-pay of $50, which does not count toward your deductible nor your out of pocket maximum. The co-pay is waived if admitted. Second Surgical Opinion may be recommended and must receive prior authorization from Health Care Evaluation if services are performed within the County of Mendocino or out of the State of California. It is paid at 100% with no deductible. Covered services or supplies must be provided or referred by your primary care physician in order for you to receive the highest level of benefits. 11 • • Please see Prior Authorization list for hospitals in Mendocino County and outside of Mendocino County. Outpatient prescriptions are paid through the Prescription Drug Card Program, with no deductible. Co payments for prescription drugs do not count toward your annual out-ofpocket limits. PLAN II • • • • • • • • • • • • • • • • There is a $500 per individual ($1500 per family) annual deductible. The plan pays 80% of allowable for most network services. The plan pays 60% of UCR for non-network services. Your maximum out-of-pocket expense is $4,000 per person/$8,000 family per year, including your deductible. The plan pays 60% of allowable charges for preferred providers and 50% of usual, customary, and reasonable (UCR) charges for non-preferred providers when treating covered outpatient nervous and mental disorders up to a maximum of 52 visits per calendar year. Your expenses for outpatient mental and nervous treatment do not count toward your annual out-of-pocket limit. Inpatient nervous and mental care is paid up to a maximum of 28 inpatient days per calendar year. Inpatient and outpatient chemical dependency (alcohol and drug treatment) is paid as any other illness. The combined outpatient and inpatient maximum payable for covered alcohol and drug treatment is $16,000 per calendar year and $50,000 per lifetime. You must complete treatment before the plan will pay. Wellness and preventive care is covered at 100% with no coinsurance or deductible for preferred providers only. The Employee Assistance Program (EAP) is available through the County. The first six visits to the EAP are free to you and your dependents on the health plan. Hospital prior authorization is required. There is a $200 deductible for failure to obtain prior authorization. Pre-admission testing is paid at 100% with no deductible. Emergency Room Co-pay of $50, which does not count toward your deductible nor your out of pocket maximum. The co-pay is waived if admitted. Second Surgical Opinion may be recommended and must receive prior authorization from Health Care Evaluation if services are performed within the County of Mendocino or out of the State of California. It is paid at 100% with no deductible. Covered services or supplies must be provided or referred by your primary care physician in order for you to receive the highest level of benefits. Please see Prior Authorization list for hospitals in Mendocino County and outside of Mendocino County. Outpatient prescriptions are paid through the Prescription Drug Card Program, with no deductible. Co payments for prescription drugs do not count toward your annual out-ofpocket limits. 12 PRIMARY CARE PHYSICIANS Whenever you need medical advice or care and to be sure you get the highest benefits, you should seek direction from your primary care physician. Designating a primary care physician (PCP) for yourself and your dependents is your first responsibility as a covered person. Your primary care physician will assume formal responsibility for your health care, either by treating you directly or by referring you to a preferred specialist. When your health needs require the care of a specialist, your primary care physician may decide to see you before making a referral, however this is not a requirement of the Plan. This provides a coordinated approach to your health care needs and results in a high quality treatment program for you. All non-emergency care must be received from your primary care physician or other preferred providers when referred by your PCP in order to receive the higher benefit. The PCP you designate must be listed in the provider directory. You may choose a different physician for you and each dependent. Internists, family practice physicians, general practice physicians and pediatricians may be selected as primary care physicians. OB/GYN’s may not be selected as a PCP. However, annual exams and obstetric care may be obtained from your OB/GYN without a referral after you have designated a PCP. If your primary care physician’s name was put on your enrollment application, it will appear on your ID card. If you did not designate a primary care physician at the time of enrollment or if you selected an invalid primary care physician, your ID card will indicate “Not Selected.” If you need help selecting a physician or if you need non-emergency care before you have designated a primary care physician, call Delta Health Systems for assistance. CHANGING PRIMARY CARE PHYSICIANS You may change your primary care physician up to three times per year by calling Employee Health Benefits with the name of the new primary care physician. When a new primary care physician has been designated, a new ID card will be issued confirming the physician’s name and effective date of the change (immediately after notification). You must wait until the effective date of the change to visit your new PCP. REFERRALS TO SPECIALISTS – HEALTH CARE EVALUATION – WITHIN MENDOCINO COUNTY AND OUT OF THE STATE OF CALIFORNIA ONLY Your primary care physician will refer you to a specialist or other health provider when appropriate. 13 In-Network: To do this, your primary care physician will refer you directly to an in-network specialist. The in-network specialist will fill out a form, which they will submit to Delta Health Systems, stating that your primary care physician referred you for services. Out-of-Network: To do this, your primary care physician will call Health Care Evaluation (HCE), notify staff of the referral to be made, and obtain a specific referral number. HCE will mail you a confirming copy of all pertinent information, including the referral number and the number of authorized specialist visits. Be sure to bring this referral number with you to your specialist appointment. For same-day appointments, your primary care physician can simply give you the referral number to bring with you to the specialist’s office: a form from HCE is not required. Remember to show the specialist your ID card in addition to the referral number. In and Out of Network: A specialist to whom you are referred by your primary care physician will need to contact that primary care physician for any referral to another specialist. However, specialists can refer you directly to ancillary providers such as physical therapists and optometrists. A few services do not require a referral from your primary care physician: • On-call physicians. The on-call physician for your primary care physician can provide care in your doctor’s place. • Emergency services. A referral is not needed in an emergency. • OB/GYN. Care received from OB/GYN doctors does not require a referral once you have designated a primary care physician. Should your OB/GYN physician want you to see another preferred specialist physician, your OB/GYN will need to contact your primary care physician for a referral. • Accessing the Employee Assistance Program. • The first two visits (per diagnosis) to a preferred mental health provider (paid at the higher rate) or a non-preferred mental health provider (paid at the lower rate and employee pays the difference between what is billed and what is usual and customary), however after the two visits you must obtain prior authorization from Health Care Evaluation. Authorizations are only given to preferred providers. If you are currently seeing a preferred specialist (e.g., cardiologist, dermatologist, surgeon), you must obtain a referral from your primary care physician before you receive further services from the specialist. Please notify your primary care physician that you have been seeing a preferred specialist, so the two physicians can coordinate your care. When your physicians agree that you no longer need specialty services, your primary care physician will resume providing your health care. PRIOR AUTHORIZATION Prior authorization is normally required before you are admitted for inpatient hospitalization. In an emergency situation, you will have 48 hours to report the admission to Health Care Evaluation (HCE-in Mendocino County and Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California). However, there are other circumstances that will also require prior authorization in order for you to receive the higher benefit. These services are covered at the highest benefit level only if you have written approval, prior authorization, from Health Care Evaluation (in Mendocino County and Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California) before your appointment. 14 Prior authorization permits HCE and Blue Cross to confirm that the proposed services are medically necessary and at the appropriate level of care. Prior Authorization must be requested and obtained by your primary care physician before you receive certain services. Failure to obtain prior authorization when required for hospitalization will result in a $200 co-pay that will not be applied to your deductible. When a request for services is approved or denied, you and your physician will be notified in writing. Your physician is the first person to ask questions regarding a pending or denied authorization request. If you still have questions or concerns after talking to your physician, call Health Care Evaluation for assistance or Blue Cross. To appeal a decision, you must contact Health Care Evaluation at (800) 333-3018 for questions (in Mendocino County or Out of the State of California) or contact Blue Cross at 800-274-7767 for out of Mendocino County within the State of California questions. Emergency services received in an emergency room do not require prior authorization. If you or a covered dependent reside within the service area (Mendocino County): • Only preferred physicians in Mendocino County or Out of the State of California may request prior authorization from HCE and those preferred physicians outside of Mendocino County within the State of California may request prior authorization from Blue Cross. • Prior authorization is required for a higher benefit for all elective inpatient admissions and certain outpatient procedures. • Services from non-preferred providers will not normally be authorized unless the services cannot be provided by a preferred provider. However, if your primary care physician determines that he/she needs to send you to a non-preferred provider, a prior authorization must be obtained. If prior authorization is not obtained for non-preferred providers, through HCE (in Mendocino County and Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California), no benefit will be given. • If you are traveling outside the service area, emergency services provided in an emergency room or doctor’s office is a covered benefit. • Should you be hospitalized because of an emergency, you must notify Health Care Evaluation (in Mendocino County and Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California) within 24 to 48 hours. If you are unable to make the call, have someone at the hospital make it for you. Health Care Evaluation and Blue Cross will work with the hospital and doctors to coordinate care and, when appropriate, will arrange for you to be transferred to a preferred hospital. If you or a covered dependent reside within the service area (Mendocino County) and are requesting service within the service area: • Prior authorization is required from Health Care Evaluation in order for you to receive the higher benefit for services from either a preferred physician or any non-preferred provider within Mendocino County and Out of the State of California. • A preferred specialist physician may request a prior authorization from HCE to do a procedure or to send you to an ancillary provider if there is a referral in place from your primary care physician to see that specialist within Mendocino County or Out of the State 15 • • of California. The specialist may not obtain prior authorization for you to see another physician. Only your primary care physician can refer you to another physician. In addition, HCE determines whether services are available from a preferred provider. Whenever services are available from a preferred provider, services from a non-preferred provider will not be authorized and will not be paid at the higher benefit level. Authorization of second, surgical opinions can be requested from Health Care Evaluation and, when authorized, will be paid at 100% with no deductible within Mendocino County and Out of the State of California. If you reside outside the service area: • Any preferred or non-preferred physician may request prior authorization. • Prior authorization is required for all elective inpatient admissions and certain outpatient surgeries only. • Emergency services in an emergency room do not require prior authorization. Delta TeamCare PRIOR AUTHORIZATION IF YOU LIVE IN MENDOCINO COUNTY OR OUT OF THE STATE OF CALIFORNIA AND ARE SEEKING SERVICES WITHIN MENDOCINO COUNTY OR OUT OF THE STATE OF CALIFORNIA Prior authorization is required from Delta TeamCare for all surgical procedures performed in a hospital outpatient department or freestanding surgery center. In addition, prior authorization is required for the following: • Ambulance transport (non-emergency) • All Dietary Visits • Chemical Dependency • All Computerized tomography scan (CT scan) (non emergency) • Durable medical equipment if cost exceeds $2,000.00. • IV Therapy (outpatient in hospital setting) • All Magnetic Resonance Imaging (MRI) (non-emergency) • All Mental Health Services after the first 2 visits (per diagnosis) (Please note that the first 2 visits DO NOT require a Referral nor prior authorization). Authorizations are only given to preferred providers. • Non-participating consultations (Prior authorization will serve as approval for lab and diagnostic testing immediately associated with requested consultation.) • Occupational therapy after first 12 visits • Physical therapy after first 12 visits • Psychological testing • Sclero Therapy • Second Surgical Opinions • Speech therapy • Surgical procedures performed in a hospital outpatient department or freestanding surgery center. • All elective inpatient hospitalization 16 Blue Cross PRIOR AUTHORIZATION IF YOU LIVE IN MENDOCINO COUNTY WITHIN THE STATE OF CALIFORNIA AND ARE SEEKING SERVICES OUTSIDE OF MENDOCINO COUNTY WITHIN THE STATE OF CALIFORNIA Prior authorization is required from Blue Cross for all non-emergency hospitalizations or surgeries, including Mental and Nervous and Chemical Dependency and for surgical procedures performed in a hospital outpatient department or freestanding surgery center. In addition, prior authorization is required for the following: • Durable medical equipment if cost exceeds $2,000.00 • IV Therapy (outpatient in home setting only) • Occupational therapy after first 12 visits • Physical therapy after first 12 visits • Speech therapy • Home Health Care • Skilled Nursing Facilities • All elective inpatient hospitalization Prior authorization guidelines are reviewed annually and may be revised from time to time. CASE MANAGEMENT SERVICES – IN AND OUT OF COUNTY Hospital Concurrent Review All acute hospital and skilled nursing facility admissions are reviewed for medical necessity by a Delta TeamCare Nurse Coordinator or Blue Cross nurse. The review will be completed either onsite or via phone. This process enables the plan to manage the quality and cost of care by identifying unnecessary admissions or days in the hospital or by using alternate levels of care (i.e., skilled nursing or home care) when appropriate. Concurrent review also provides a system of early referral for the implementation of discharge planning and case management services. The review process also assists you or your dependent in transferring to a preferred provider after emergency treatment in a non-preferred facility has been provided and your condition is stable. This approach assures that the needed care is rendered in the most cost-effective setting. Discharge planning Delta TeamCare’s Nurse Coordinator or Blue Cross nurse will assist with discharge planning including appropriate transfer or discharge from the acute hospital. The Nurse Coordinator can arrange for home care, skilled nursing admissions or outpatient services. Referrals to case management may also occur. Medical Case Management Medical case management is a benefit to County of Mendocino employees who find themselves at physical and financial risk because of complex illnesses, injuries, or a catastrophic medical event. Case management services can facilitate communication between patient, family, physicians, service providers, and your medical plan. Using this team approach may result in timely discharge from acute care settings or prevent an acute admission altogether. Case management has also proven helpful to employees who must go out of their county for services because of complex problems. Some typical situations, which would benefit from case management, might be premature births, motor vehicle accidents with many injuries, transplants, or people who require multiple hospitalizations. 17 A nurse case manager provides an in-depth evaluation of your needs, develops a plan with you and your doctor, and coordinates your care during the course of treatment. Mental Health If you are seeking services within Mendocino County or Out of the State of California, all mental health services require prior authorization from Delta TeamCare with the exception of the first two visits. Authorizations are only given to preferred providers. Please note that you do not need a referral to a preferred provider (paid at higher rate) or a non-preferred provider (paid at lower rate) for the first two visits (per diagnosis). If you feel in need of mental health care you may first contact the County EAP. Emergency Care Hospital emergency room care is required in some situations. However, whenever possible, you should call your primary care physician before seeking emergency care. To avoid long waits, needless medical expenses, and possible payment of claims at the lower benefit level, call your physician in advance. There is a $50 copay for emergency room use, which does not go toward your deductible. This copay is waived if the patient is admitted into the hospital. Keep these points in mind: • If taking time to call your primary care physician puts a life in jeopardy, don’t wait! Call 911 or go immediately to the nearest emergency room. • Whenever time allows, call your primary care physician. • If you have time to call and an emergency arises during non-office hours, dial your doctor’s telephone number and speak with the answering service. Be assertive. Explain that you have a potential emergency situation and ask to speak with the doctor on call. • Follow-up care after an emergency room visit is not an emergency and should be coordinated by your primary care physician who will treat you or direct you to an appropriate preferred provider. After-Hours Assistance If you need urgent medical care or advice after business hours, call your primary care physician’s office. Don’t worry about bothering your physician or calling during non-office hours. Your PCP is the first person to notify when you’re considering a trip to the hospital. If your primary care physician is not available, you will be taken care of by the physician on call. There is someone ready to help you 24 hours a day, seven days a week, including holidays. If your after-hours medical problem is not urgent, please wait until regular business hours to call your doctor. Remember, for information about coverage, benefit limits, or co-payments, call Delta Health Systems at 1-800-291-0726. PRE-EXISTING CONDITIONS If you or your dependent has received medical care or treatment for an injury or sickness at any time during the 3 months before coverage starts under this plan, coverage under this benefit will be postponed for the injury or sickness until the earliest date below: • 3 months after the last time care or treatment was given for the injury or sickness. • When you have been covered under this plan during active work for 6 months. 18 • When your dependent has been covered under this plan for 6 months. The above rules also apply to medical care or treatment for a pregnancy-related condition. However, if you were covered by a group medical plan within 90 days, or an individual medical plan within 30 days of enrolling in this plan, you will be credited with one month toward satisfying the pre-existing condition waiting period for each month you were covered by your previous plan. So, if you were covered for six months by your previous coverage, you will not have to wait for any medical coverage under this plan. Any of your dependents who were previously covered also qualify for this exception. Be sure to provide information on your previous medical coverage to Employee Health Benefits. WHAT IS COVERED? This section of your booklet describes the services and supplies covered by this plan. If you have questions about specific coverage, please contact Delta Health Systems. Benefits are available for a service or supply described in this section when it meets all of these requirements: • It must be furnished in connection with the diagnosis or treatment of a covered illness or accidental injury or be furnished in connection with a wellness exam. • It must be, in Health Care Evaluation's, Blue Cross’s or Delta Health Systems' judgment, medically necessary. • It must not be excluded from coverage under this program. • The expense for it must be incurred while you or your dependent is covered under this program and after any applicable waiting period required under this program is satisfied. • It must be furnished by a provider that is covered under the applicable benefit. COVERED SERVICES Hospital Inpatient care Services include semiprivate room, intensive and coronary care units, plus services and supplies such as diagnostic X-ray and laboratory services, surgical dressings, and drugs, furnished by and used while confined in the hospital. Hospital outpatient care Emergency, procedure, operating, and recovery rooms services are covered as well as services and supplies such as diagnostic X-ray and laboratory services, surgical dressings, and drugs, furnished by and used while at the hospital. Skilled nursing facility Services include semiprivate room, plus services and supplies furnished by and used while confined in a Medicare-approved skilled nursing facility. In addition to General exclusions, this benefit will not be provided for custodial care or care that is primarily for senile deterioration, or mental deficiency or retardation. Ambulatory surgical center Covered services and supplies are those furnished by and used while at the center such as surgical dressings and drugs. 19 Physicians’ services Services include home, office, emergency room, and inpatient visits, surgery, and anesthesia administration. Benefits are only provided for services of an assistant surgeon when medically necessary. Therapeutic nuclear medicine Services and supplies are those furnished in connection with radium, radioisotope, and X-ray therapy. Diagnostic X-ray and laboratory services Services include administration and interpretation of diagnostic X-ray and laboratory tests, and diagnostic and screening mammography recommended by your physician, advanced registered nurse practitioner, or physician’s assistant. Organ and bone marrow transplant Please call Health Care Evaluation (in Mendocino County or Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California) as soon as you learn you need an organ or bone marrow transplant. Benefits for organ and bone marrow transplants are only provided when the transplant is authorized as medically necessary by HCE or Blue Cross and benefits are verified by Delta Health Systems in an approved transplant center. Rehabilitation and neurodevelopment therapy Rehabilitation services are designed to restore the individual to a level of function equal to the level present prior to an illness or accidental injury. Services may be provided on an inpatient or outpatient basis, and may include a single modality or a concentrated program of several modalities. Rehabilitation treatment plans are individualized protocols to achieve a specified goal. The rehabilitation potential of each case must be assessed in accordance with the patient’s diagnosed condition, special circumstances and abilities prior to the illness or injury. The plan requires a prior authorization from HCE (in Mendocino County and Out of the State of California) or Blue Cross (outside of Mendocino County or within the State of California) and initially provides a benefit for 12 visits, then requires a progress report from the physician to HCE or Blue Cross. Chemical dependency treatment Inpatient and outpatient chemical dependency treatment, including detoxification, is covered up to a benefit maximum of $16,000 per person during the calendar year that starts January 1. Chemical dependency treatment benefits are also limited to a lifetime maximum benefit of $50,000 per covered person. You must complete a program of treatment in order to receive a benefit from the plan. Covered services must be furnished by a state-approved treatment facility, hospital, physician (M.D. or D.O.), licensed clinical psychologist, community mental health agency, or a government-approved methadone clinic. Benefits for inpatient and outpatient treatment are provided as follows: • In Network: 85% (for Plan 1) and 80% (for Plan 2) of allowable charges. • Out of Network: 70% (for Plan 1) and 60% (for Plan 2) of usual, customary, and reasonable charges. Prior authorization from Health Care Evaluation or Blue Cross is required in order to receive a benefit for inpatient care. 20 In addition to General exclusions, the County will not provide this benefit for: • Treatment of nondependent alcohol or drug use or abuse. • Voluntary support groups, such as Alanon or Alcoholics Anonymous. • Court-ordered services, services related to deferred prosecution, deferred or suspended sentencing, or to driving rights, except as deemed medically necessary by Health Care Evaluation or Blue Cross. Home Health and Hospice Care Covered services are those furnished and billed by a home health agency or hospice that is licensed or certified as such by the state in which it operates or approved under Medicare. To be covered, home health and hospice services must be part of a written plan of care prescribed, periodically reviewed, and approved by a physician (M.D. or D.O.). Covered services or providers of a home health or hospice agency are a registered nurse, a licensed practical nurse, a licensed or registered physical therapist or occupational therapist, a certified respiratory therapist, a speech therapist certified by the American Speech, Language, and Hearing Association, and a home health aide who is directly supervised by one of the above providers (performing services prescribed in the plan of care to achieve the described medical results). Home Intravenous Services include therapy, professional services, supplies, drugs and solutions furnished and billed by one of the following providers: • A home health agency that is Medicare-certified as such or licensed or certified as such by the state in which it operates. • An intravenous therapy provider that is state-licensed. Licensed Ambulance Service Transportation is covered, when medically necessary, to the nearest medical facility equipped to treat your condition. Ambulance services are medically necessary for the following situations: • When the patient’s condition makes use of any other method of transportation life threatening. • Air ambulance only when medically necessary for transportation to the nearest hospital qualified to provide necessary care and treatment. • When ordered by the police at the scene of an accident. Note: Transportation charges for a private automobile are not considered a covered benefit and are not reimbursed. Durable Medical Equipment and Medical Supplies Durable medical equipment and medical supplies are covered when medically necessary, as follows: Durable medical equipment rentals are covered (not exceeding the purchase price) when prescribed by a physician required for therapeutic use in direct treatment of a covered illness or injury. Durable medical equipment requires prior authorization from HCE (in Mendocino County or Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California) if the amount exceeds $2,000.00. 21 The County may provide benefits for the initial purchase of equipment in lieu of rental. Examples of durable medical equipment are a wheelchair, a hospital-type bed, traction equipment, and an intermittent positive pressure breathing apparatus. Repair or replacement of durable medical equipment medically necessary due to wear caused by normal use or growth of a child is covered. Medical supplies and orthopedic appliances such as braces, rib belts, and crutches are covered. In addition to General exclusions, the County will not provide this benefit for: • Special or extra cost convenience features. • Items such as corrective shoes, exercise equipment or weights, and whirlpool baths. • Orthopedic appliances prescribed primarily for use during participation in sports, recreation, or similar activities. • Used equipment, unless approved by HCE or Blue Cross prior to purchase. Prosthetic Devices The plan covers any device that replaces all or part of an absent body limb or replaces all or part of the function of a permanently inoperative or malfunctioning body organ. The loss of the body part or an organ’s function must have resulted from accidental injury that occurred on or after your effective date of coverage, a surgery for which benefits were provided under this program, or a congenital anomaly of a child continuously covered under this program since birth. This benefit also covers the first intraocular lens prescribed to replace the lens of an eye that is surgically extracted while you are covered under this program. Benefits will only be provided for the initial purchase of a prosthetic device, unless the existing device cannot be repaired, or replacement is prescribed by a physician because of a change in your physical condition. Blood transfusions The cost of blood and blood derivatives is covered. PKU dietary formula Dietary formula, which is medically necessary for the treatment of phenylketonuria (PKU) is covered. Obstetrical care Pregnancy, childbirth and related conditions for you (or your spouse) are covered the same as any other condition. Care connected with a dependent child’s pregnancy is also covered. Covered services include screening and diagnostic procedures during pregnancy, and related genetic counseling, when medically necessary for prenatal diagnosis of congenital disorders. Delivery and related expenses for your dependent child and newborn are not covered. 22 Newborn care Hospital and physician nursery care for natural newborn children is covered as follows: Hospital nursery care at birth for a well baby, provided the mother is an inpatient and is receiving benefits for obstetrical delivery under this program. Benefits are provided under the newborn’s coverage The plan covers physician services for well-baby care during the initial hospital confinement of the newborn at birth, provided the newborn is properly enrolled. The newborn of a dependent child is not covered. Mental health care Inpatient and outpatient treatment of psychiatric conditions, including treatment of eating disorders (such as anorexia nervosa, bulimia, or any similar condition), when furnished by a hospital, licensed community mental health agency, physician, or licensed psychologist, is covered up to a maximum benefit for inpatient mental health care of 28 inpatient days per calendar year. Benefits for inpatient treatment and intermediate care are provided as follows: • In Network: 85% (for Plan 1) and 80% (for Plan 2) of allowable charges. • Out of Network: 70% (for Plan 1) and 60% (for Plan 2) of usual, customary, and reasonable charges. Prior authorization from HCE (within Mendocino County or Out of the State of California) or Blue Cross (outside of Mendocino County within the State of California) is required in order to receive a benefit for inpatient care. Prior authorization is also required to obtain intermediate care. Intermediate care is defined as: • Partial hospitalization: Daily mental health treatment in a designated outpatient facility or program in which medication management, individual therapy, group therapies and other services are available. • Structured outpatient programs: Coordinated programs that combine services from different outpatient locations such as the provider’s office, group meetings or a day treatment facility. • Intensive outpatient psychotherapy: Patients are treated 3 to 5 times per week in the mental health provider’s office. • Home care: Home visits may be appropriate in an acute crisis where transportation is problematic or inadvisable. Benefits for outpatient treatment are paid at 60% of allowable charges for services of a preferred provider and 50% for services of a non-preferred provider. The first 6 visits to the Employee Assistance Program (EAP) are paid at 100%. Outpatient benefits are paid for a maximum of 52 visits per calendar year. Wellness Programs Medical preventive care - Preventive health screenings including annual physical exams, pap smears, mammograms, PSA tests, wellness counseling, well-baby and well-child checkups, immunizations paid at 100% with no deductible. The specific wellness procedures are: 23 • • • • • • An annual physical exam for each of you and your dependents from your primary care physician, including the office visit and associated X-rays and laboratory tests. (1 visit per calendar year) An annual gynecological exam from your OB/GYN. An annual mammogram. Standard childhood immunizations as prescribed by your child’s primary care physician. Well-baby visits to the baby’s primary care physician up to a maximum of 10 visits to age 2. Hepatitis A & B shots. Caution: Anything done related to specific diagnosis is subject to deductibles and coinsurance. Employee Wellness Program - This program includes educational presentations, resource materials, health risk appraisals, some health screenings, activities and further education to encourage healthy behavior changes and support individuals to maintain the new healthier behavior. The Employee Wellness Program is available to all employees and their family members on a voluntary basis. The Employee Wellness Program began as a response to requests from employee groups to provide educational awareness and active support for employees and their family members who wish to improve their health and well-being through lifestyle changes. There are four phases to this program. 1. Educational Awareness: This voluntary program begins with educational presentations, activities and the availability or wellness educational materials and tapes in the Wellness Resource Center. 2. Individual Health Assessments: Each year, individuals may assess their own health status through a health risk appraisal and certain health screenings such as cholesterol, blood pressure, and body fitness. 3. Health Behavior Change Activities and Support: Following this personal assessment, individuals choose an area of desired health behavior change such as becoming more physically active, eating better, practicing stress management, or developing a stronger social support network. The program will provide help to support these healthy changes through a variety of means such as walking groups, exercise classes, or nutritional counseling. The activities are available in Fort Bragg, Ukiah, and Willits. 4. Maintenance of New Healthy Behavior: Individual wellness coaching, support groups and continuing education will be available to encourage and support the incorporation of the new behavior as a lifetime habit. Information, educational materials or schedules of upcoming events are available at the Wellness Resource Center, 405 Observatory Ave., Ukiah, or call 463-4040. Chiropractors’ services Services include those of a chiropractor (D.C.), operating within the scope of his or her license, on the same basis as for any covered physician. Acupuncture services Services include those of a acupuncturist, operating within the scope of his or her license, on the same basis as for any covered physician 24 WHAT IS NOT COVERED? • Care and treatment of the teeth and gums is not covered except for the following: 1. Cutting procedures on gums or mouth tissues needed to treat a disease. 2. Full or partial dentures, fixed bridgework or prompt repair to natural teeth, if needed because of accidental injury which happens while covered. • Eye glasses, eye refractions and hearing aids, unless required by accidental injury which happens while covered. See Vision Plans. • Injury or sickness caused by war or international armed conflict. • Services of a person who is a member of your immediate family. • Services of a person who resides in your home. • Smoking cessation/RX. (covered under wellness) • Sexual dysfunction treatment/RX • Obesity Treatment/RX (covered if medically necessary) • Learning disabilities (covered if medically necessary) • Infertility diagnosis. • Cosmetic services. • Homeopathic. • Sterilization reversals. • Artificial insemination. • Dental implants Other exclusions that apply to this benefit are in General exclusions. DENTAL PLAN Our dental benefit is administered by Delta Health Systems. The dental plan provides payment for a wide range of dental expenses, charged to you or your dependents by a dentist or a physician. These expenses must be needed for necessary dental care and treatment due to one of the following: • Dental disease. • Dental defect. • Accidental injury to the teeth or mouth. • Routine preventive dental services such as exams and teeth cleaning are also included as covered charges. These services are shown below. Each covered person must satisfy a deductible each calendar year before any payment is made for certain covered charges. Then the plan pays the percentage of covered charges for the rest of that year up to $1,500. WHAT DOES THE PLAN PAY? The plan pays 100% of preventive and diagnostic services such as routine exams and teeth cleaning. General services like X-ray, amalgam fillings, and lab tests are paid at 85%. Finally, major services, which are paid at 50% include crowns and denture work. The plan has an annual limit of $1,000. 25 You will have to pay a $25 per person annual deductible for all services except preventive care. The most your whole family will have to pay for deductibles in any year is $75. This family deductible applies no matter how large your family may be. ACCIDENT FEATURE If two or more covered family members have injuries to the teeth or mouth in the same accident, only one deductible will have to be paid for these injuries each year. This covers all of the combined family expenses due to that accident during that year. BENEFIT DETERMINATION The benefit pays for dental treatment that begins after you or your dependents become covered. The person must be covered on the date dental treatment is received. Most dental treatment is considered to have been received on the date the work is done. However, there are some kinds of treatment that take more time to complete. In these cases, treatment will be considered to have been received on the date shown below: • Fixed bridgework, crowns, inlays, onlays and gold restorations - the date the tooth or teeth are first prepared. • Full or partial removable dentures - the date the impression is taken. • Root canal work – the date the tooth is opened. PRE-DETERMINATION OF BENEFITS This is a way of telling you ahead of time how much will be paid for dental work. It will help to avoid surprises. Many times dental work is likely to cost more than $100. If so, ask the dentist to file for predetermination of benefits with Delta Health Systems. Most dentists know about this procedure. Here is how it works: • Get a dental claim form from your department. • Give it to your dentist. The dentist will tell Delta Health Systems what work needs to be done. This work is called the treatment plan. • The dentist lists the services and charges on the claim form and sends it to Delta Health Systems. • Delta Health Systems tells you and the dentist what amount the benefit will pay. You should discuss the treatment plan with the dentist before the work is done. If the dentist changes the treatment plan, the amount of the payment may change. If the dentist makes a major change, a new dental claim form should be sent to Delta Health Systems. If you do not use predetermination of benefits, payment will be based on whatever information Delta Health Systems has about the case. ALTERNATE PROCEDURES There is often more than one way used by a dentist to treat a dental problem. Different materials or procedures may be used to correct the same problem. For example, a tooth could be repaired with an amalgam filling. That same tooth could also be repaired with a more expensive cap (crown) or gold filling. Delta Health Systems will allow as covered charges only the least expensive services and supplies which are appropriate and meet acceptable dental standards. You and the dentist may decide you want the more expensive treatment. If so, you must pay the charges which are greater than the covered charge for the least expensive appropriate treatment. Because Delta Health Systems has this alternate procedures provision, it is important for you to 26 use pre-determination of benefits. It will tell you how much Delta Health Systems will pay for treatment. WHAT IS COVERED? Covered charges are the charges for dental services and supplies listed on this and the following page. The benefit is intended to cover treatment that is customarily given by dentists throughout the country to eliminate oral disease and to replace missing teeth. Delta Health Systems will compare the charge for each treatment with the charges for comparable treatment made by the other dentists in the area. Covered charges are charges, which are not more than the amount customarily charged by the majority of dentists in your area, as determined by Delta Health Systems. In most cases, the dentist’s charges will be well within the range of prevailing fees in the area. However, if the dentist’s charge is more than the usual, customary, and reasonable charges determined by Delta Health Systems, you will have to pay the difference. Of course, unusual dental complications will be taken into consideration. The possibility of an alternate treatment can also affect the amount of the covered charge. SERVICES PAID AT 100% (Deductible Waived) Preventive services and supplies • Cleaning and scaling teeth (prophylaxis) once every 6 months. • Fluoride treatments for a child’s teeth once each calendar year. Under the age of 18. • Space maintainers and their fitting. (These are appliances used to keep teeth from moving into the space left when a tooth is pulled or lost.) Diagnostic services and supplies • Routine oral exams once every 6 months. • Sealants under the age of 12 for dependent children are covered. Therapeutic services and supplies • Emergency treatment for dental pain when no other treatment but X-rays is given. If other treatment is given, payment will be made only for the other treatment. SERVICES PAID AT 85% Diagnostic services and supplies • X-rays and laboratory tests needed to diagnose a dental problem or to check the progress of treatment. • Full mouth X-rays as part of a routine exam once every 3 years. • Bitewing and other X-rays as part of a routine exam once every 6 months. Therapeutic services and supplies • Pulling teeth (extractions) and cutting procedures in the mouth (oral surgery). Extra charges for removing stitches and exams after surgery are not covered. • Root canal work (endodontic treatment). • Treatment of gums and mouth tissues (periodontic treatment). • General anesthetics for oral surgery, fractures, dislocations and treatment of gums. Delta Health Systems considers local anesthetics as included in the charges for treatment. Extra charges for local anesthetics are not covered. • Antibiotic drugs which are injected by a dentist or physician. 27 Fillings • Silver (amalgam), silicate, plastic, porcelain and composite fillings. Prosthetic services and supplies (repairs and rebasing) • Repairs to broken crowns, inlays, bridgework and dentures. This does not include adjustments made to new denture or bridgework during the first 6 months after they are installed. Those charges are considered to be included in the cost of the new denture or bridgework. Extra charges are not covered. • Rebasing or relining dentures, which are over 6 months old. If the benefit pays for a new denture. It will not pay to rebase or reline the old denture. • Adding teeth to fixed bridgework or partial dentures to replace missing natural teeth. The teeth that are being replaced must be lost while the person is covered. SERVICES PAID AT 50% Restorative services and supplies • Crowns and gold fillings to repair a tooth broken down by decay or injury. Charges for these restorations are covered only if the tooth cannot be repaired with a less expensive type of filling. If the tooth can be repaired by a less expensive method, only that charge will be covered. • Charges for replacement crowns and gold fillings are covered only if the old crown or filling is over 5 years old. Prosthetic services and supplies (dentures and fixed bridges) • Full or partial dentures and fixed bridgework to replace missing natural teeth. The teeth that are being replaced must be lost while the person is covered. • Full or partial dentures and fixed bridgework to replace an existing denture or bridge that cannot be made serviceable. The existing denture or bridge must be over 5 years old. Charges for special techniques or precision attachments are not covered. Charges for any special work that you ask to have done on a standard denture are not covered. Charges made for adjustments to new dentures or bridgework during the first 6 months after they are installed are not covered. Those charges are considered to be included in the cost of the new denture or bridgework. Extra charges are not covered. A permanent denture may replace a temporary one. In this case, charges for both are limited to the charge for the permanent one. WHAT IS NOT COVERED? • Orthodontic treatment except necessary space retainers and pulling of teeth. • Treatment by someone other than a dentist, physician, or dental technician under the direction of a dentist or physician. • Work done mainly to improve appearance (cosmetic treatment). • Any work done or appliance used to increase the distance between nose and chin (vertical dimension). • Any work done or appliance used to change the way the top and bottom teeth meet or mesh (occlusion; Mouth Guards; Treatment of Temporomandibular Joint (TMJ)). • Facings or veneers on molar crowns or molar false teeth. • Training or supplies used to educate people on the care of their teeth. • Injury caused by war or international armed conflict. 28 • • • Charges for crowns and fillings not shown in the covered charges section of this benefit. Appliances for harmful habits (thumb sucking, tongue thrusting, etc.) Dental implants. Other exclusions that apply to this benefit are in General exclusions. VISION PLAN The vision benefit is also provided through Delta Health Systems. The plan will pay for basic vision care such as a vision exam once every 12 months, vision materials once every 24-months. You may use any licensed provider you choose. WHAT DOES THE PLAN PAY? You will be paid the actual cost to you of the UCR charges only for the services and supplies in the vision care schedule below up to the maximum amounts shown. Vision Care Schedule Eye Exam $60 Lenses per pair* Single Vision Bi-focal Tri-focal Lenticular $60 $80 $100 $200 Frames $60 Contact Lenses ($400) per pair if prescribed in one of the following cases: • Your vision cannot be corrected to 20/70 in the better eye except by the use of contact lenses. • You need contact lenses after cataract surgery. • You are being treated for a condition such a keratoconus or anisometropia and contact lenses are routinely used as part of the treatment. These are considered to be medical conditions and are covered under the medical plan, which is subject to your deductible and co-insurance. Contact lenses ($110) per pair if, prescribed for any other reason. *Important: You will be paid one half of the maximum amount for a single lens. Any amount that is less than the maximum amount for each service or supply listed in the schedule may not be applied toward any other service or supply. 29 WHAT IS COVERED? Both plans provide per covered person in any 24 consecutive month period: • 1 complete eye exam (12 mo.). • 2 lenses. • 1 set of frames Each time period begins when the service or supply is first charged to the covered person. An eye exam is charged on the date it is performed. Lenses or frames are charged on the date they are ordered. WHAT IS NOT COVERED? The following are not covered by both plans: • Charges for orthoptics (eye muscle exercises). • Charges for vision training or subnormal vision aids. • Lenses that can be ordered without a prescription. • Any service or supply which is not shown in the vision care schedule. • Radial keratotomy. Other exclusions that apply to this benefit are in General exclusions. GENERAL EXCLUSIONS The health plan does not cover the following: • Injury which happens during work at any job for pay or profit. • Sickness for which payment is made or available through workers’ compensation or a similar law. • Expenses incurred before you or your dependents become covered. • Your dependent’s expenses if he or she is receiving benefits for the same expenses under the plan as an employee. • Education, training, and bed and board while confined in an institution which is mainly a school or other institution for training, a place of rest, a place for the aged or a nursing home. • Custodial care. • Shots to prevent disease (except as specified in Wellness programs) • Medical exams or tests not needed to treat accidental injury, sickness or pregnancy (except as specified in Wellness programs) • Charges for a surgical procedure to correct refraction errors of the eye, including any confinement, treatment, services, or supplies given in connection with or related to the surgery. • Experimental or investigational services and supplies. • Routine newborn well baby care (except as specified in Wellness programs and in Newborn care). • Confinement in a United States government or agency hospital. However, the reasonable cost incurred by the United States or one of its agencies for inpatient medical care and treatment given by a hospital of the uniformed services may be covered under the plan. Cost of inpatient medical care and treatment given will be covered if the charges for the care and treatment are otherwise covered under the plan. This coverage applies only to care and treatment provided to: 1. A person retired from the uniformed services. 2. A family member of a person who is retired from the uniformed services. 30 • • 3. A family member of a person who is active in the uniformed services, or 4. A family member of a deceased member of the uniformed services. Expenses which you yourself are not legally required to pay. However, the reasonable cost incurred by the United States for medical care and treatment given to a veteran by the United States or one of its agencies may be covered under the plan. The cost of the care and treatment will be covered if: 1. The veteran does not have a service-related disability, and 2. Charges for the care and treatment are otherwise covered under the plan. Radial Keratotomy. The health benefits may be reduced if you or your dependent has health benefits under another plan, HOW TO FILE A CLAIM Claim forms are available from your department. Please read the instructions on the form carefully and fill out the Claim Form from Delta Health Systems. Be sure to answer all questions and to send any required information along with the completed claim form to Delta Health Systems. If you ask for a claim form but do not receive it within 15 days, you can file a claim without it by sending in the bill. Be sure that the bill includes your name, social security number, and group number. Be sure to save all bills and attach copies of them to the claim form. Keep a record of the date of service and the type of service given. To claim health benefits you must give Delta Health Systems an itemized statement within 90 days after the date of the loss or the date the expenses are incurred. If the plan provides any periodic payment which depends on continuing loss, the proof must be given within 90 days after the end of the period for which Delta Health Systems is liable. If it is not possible to give the proof within 90 days, give the proof as soon as possible. Delta Health Systems will not reduce or deny your claim if you give the proof as described above. The only time that this one-year limit will not apply will be if the person is legally unable to do so. It is important to keep separate records for each person in your family since maximum amounts, deductible amounts and other provisions apply separately to each person. Delta Health Systems has the right to examine anyone filing a claim. If a medical exam is needed, you will not have to pay for it. Delta Health Systems can request any needed proof of loss in connection with a claim under the dental plan. This includes the following: • Dentist’s or physician’s statement of treatment. • Study models. • X-rays taken before and after surgery. HOW AND WHEN CLAIMS ARE PAID All benefits will be paid to you or your assigned provider as soon as possible after Delta Health Systems receives an itemized statement. Any health benefits continued for your dependents after your death will be paid to one of the following: • Your surviving spouse. • Your dependent child who is not a minor, if there is no surviving spouse. • A hospital or a person who makes charges to your dependents for services that are covered under this plan. • The legal guardian of your dependent. 31 HOW TO APPEAL A CLAIM You will be notified in writing by Delta Health Systems if a claim or any part of a claim is denied. If you are not satisfied with the explanation of why the claim was denied, you may ask to have your claim reviewed within 60 days of receiving the denial. The claim denial will tell you the name and address of the person you can write to for the review. If you think you have more information that can help your claim, you can send it with your request. You can ask for and receive copies of documents important to the claim. In some cases approval may be needed to release confidential information such as medical records. You may submit issues and comments in writing. A decision will be made within 60 days after receipt of request for review or the date all information required from you is given. Delta Health Systems will notify you in writing about the decision on your review. The reasons for the decision will be stated in a manner you can understand. If you are not satisfied with the outcome of your appeal with Delta Health Systems, you may appeal to the County by writing Employee Health Benefits. The Plan Administrator will rule on the appeal. If you are not satisfied with the ruling of the Plan Administrator, you have the opportunity to have the Health Benefits Committee hear your appeal, so long as your appeal does not contain any Private Health Information (according to HIPAA rules and regulations). COORDINATION OF BENEFITS This provision will coordinate the health benefits payable under this plan with similar benefits payable under other plans you may have such as another group health plan, another employer, or a government or tax-supported program. This does not include some government-sponsored programs. Whenever there is more than one plan, the total amount of benefits paid in a calendar year under all plans cannot be more than the reasonable expenses charged for that calendar year. The medical expenses must be covered in part under at least one of the plans. Dental care expenses must be a covered charge under that benefit. Vision care expenses must be covered under that benefit. HOW DOES COORDINATION WORK? One of the plans, which is called “primary”, will pay benefits first. The other plans, which are called “secondary”, will pay benefits next. If this plan is primary, it will pay benefits first. Benefits under this plan will not be reduced due to benefits payable under any other plans. If this plan is secondary, benefits under this plan may be reduced due to benefits payable under other plans primary to this plan. The amount of reasonable expenses will be determined first. Then the amount of benefits paid by plans primary to this plan will be subtracted from this amount. This plan will pay you the difference but no more than the amount it would have paid without this provision. WHICH PLAN IS PRIMARY? In order to pay claims, Delta Health Systems must find out which plan is primary and which plans are secondary. These are rules to find out which plan is primary and which plan is secondary. The rules are used until one is found that applies to the situation. They are always used in the following order: • A plan that has no coordination of benefits provision will be primary to a plan that does have a coordination of benefits provision. 32 • • A plan that covers the person as an employee will be primary to a plan that covers the same person as a dependent. A person may be covered as a dependent under two or more plans. The plan that covers that person as a dependent of the person whose birthday is earlier in the calendar year will be primary to a plan which covers that person as a dependent of a person whose birthday is later in the calendar year. The other plan may not have a rule based on birthdays similar to this rule. The rule in the other plan will determine which plan is primary. However, the person may be covered as a dependent under two or more plans of divorced or separated parents. The rules that are used to find out which plan is primary and which plan is secondary are as follows: • The plan of the parent with custody will pay benefits first. • The plan of the stepparent with custody will pay benefits next. • The plan of the parent without custody will pay benefits next. There may be a court decree, which gives one parent financial responsibility for the medical, dental or other health expenses of the dependent child. A plan of the parent with this financial responsibility will be primary to any other plan that covers that dependent child. A plan may cover a person as an employee who is not laid-off or retired, or as a dependent of that employee. This plan will be primary to any plan that covers the person as a laid-off or retired employee, or as a dependent of that employee. The other plan may not have a rule for laid-off or retired employees similar to this rule. In this case, this rule will not apply. If none of the above rules apply, the plan that has covered the person for the longest time will be primary to all other plans. You will have to give information about any other plans when you file a claim. Effect of Medicare on Benefits All medical care benefits under this plan will be coordinated with Medicare benefits and will be subject to the Coordination of Benefits provision described above. Any person who is not enrolled for all coverage for which she/he becomes eligible under Medicare will have her/his benefits under this plan coordinated with the amount of benefits to which he would have been entitled had she/he enrolled for Medicare coverage. No benefits will be paid for that part of any expenses for which benefits are available under any plan or program established pursuant to the laws or regulations of any government. This arrangement will become effective on the date a covered person becomes eligible for Medicare. Except to the extent modified herein, the type and level of benefits under the plan in effect immediately prior to a covered person’s eligibility for Medicare, including its exceptions and exclusions, continue to apply. Subrogation In the event an Employee or eligible Dependent suffers an injury or sickness as a result of a negligent or wrongful act or omission of a third party, the Plan has the right to pursue subrogation. If the Employee or eligible Dependent does not take timely action to recover from a 33 tortfeasor, the Plan will subrogate and succeed to the Employee’s or eligible Dependent’s right of recovery. This right may be used to the extent of the benefits under this plan. Employee Assistance Program (EAP) The EAP is a worksite-based program designed to assist clients in identifying and resolving personal concerns (including, but not limited to, health, marital, family, financial, alcohol, drug, legal, emotional, stress, or other personal issues) that may affect job performance. The EAP is available to all County employees, and their insured family members, on a voluntary basis. www.co.mendocino.ca.us/aodp/eap.htm EAP services include: • Confidential and timely problem identification and assessment services for clients with personal concerns. • Referral of clients to a variety of community resources for assistance, including referral for diagnosis and treatment with licensed clinicians experienced in working with a wide range of work-related and personal issues. • Outreach to and education of employees, managers, supervisors, and union stewards about the availability of EAP Services. The EAP office is located at 405 Observatory Drive, Ukiah. The first six (6) visits to the EAP are free to employees and their insured dependents. If necessary, the EAP may authorize additional visit to EAP preferred providers for a low fee once the clients insurance deductibles have been met. Please refer to the Mental Health Section of the Plan for procedures dealing with Mental Health care after your visit through the EAP have been completed. Prescription Drug Card Program How to Use the Retail Program • Doctor issues prescription. • Check list for the nearest pharmacy location or you may call (1-800-711-0917) You must select a pharmacy listed within the Medco Health Network in order to receive benefits. • Present prescription ID card (your medical card provided by the County is also your Prescription Drug Card) to the pharmacist. The computer system will calculate the correct copayment. Non-Covered Drugs (Retail and Mail Service) • Blood • Fertility • Depo Provera (however this item is covered under the medical plan when administered in a medical facility or office. The medical facility or office must supply the medication). • Diaphragms • Experimental Drugs • Fertility Drugs • Hair Replacement treatment • Medical Devices or appliances • Over-the-Counter • Oxygen • Pharmaceutical Aids 34 • • • Sexual Dysfunction treatments Smoking Deterrents Vitamins Retail Copay (up to a 30 day supply) • Generic drugs require a $10 or 10% copay-whichever is higher. If your prescription cost is under $10 you will be responsible for the entire amount of your prescription. • Brand formulary name drugs require a $20 or 20% copay-whichever is higher. If your prescription cost is under $20 you will be responsible for the entire amount of your prescription. • Brand non-formulary name drugs require a $30 or 30% copay-whichever is higher. If your prescription cost is under $30 you will be responsible for the entire amount of your prescription. If you or your covered dependents choose a non-formulary preferred brand prescription when a generic is available, you will be charged the brand-name copay as listed above plus the difference in cost between the generic and brand counterpart. If you or your covered dependents are unable to use a generic drug due to medical necessity, please have your physician fill out a prior authorization form. This form is located on the Human Resources website at www.co.mendocino.ca.us/hr/. You may also obtain this form by contacting Employee Health Benefits directly. When the form has been completed, please submit the form along with your written request to override coverage to Employee Health Benefits for consideration. If Employee Health Benefits has determined that the employee or covered dependent has established medical necessity, the otherwise non-formulary drug would be treated as though it would be a formulary. Mail Service Copay (up to a 90 day supply) • Generic drugs require a $20 copay. • Brand formulary name drugs require a $40 copay. • Brand non-formulary name drugs require a $60 copay. How to Use the Mail Service Program • Complete the Order Form and Patient Profile located inside the mail service brochure. Please contact Employee Health Benefits for a copy of the mail service brochure. • Have your doctor write the prescription for a 90 day supply for your maintenance medication. • Send the profile with your new prescription and copayment in the postage paid envelope provided in your Welcome Packet. • Your doctor may fax the prescription to Medco Health. Please have your physician contact Medco Health at 1-888-327-9791 for information on how to fax your prescription. Prescriptions for controlled medications cannot be faxed. • Allow 2 to 3 weeks from the time you mail your order until it is delivered to your mailbox. Allow 1 to 2 weeks from the time you phone in a refill until it is delivered to your mailbox. • The prescription will be mailed to your home, postage paid. 35 How to Pay for the Order • Check or money order, VISA, MasterCard, or Discover Card can be used to pay for your order. How to Order Refills • You may order refills via the internet at http://www.medcohealth.com • You can call in your refills to 1 800 4REFILL (1 800 473-3455) • You can mail the refill sheet enclosed with your prescription to Medco Health. Medco Health’s Member Service Hours: • Medco Health’s member services is open 24-hours a day, seven days a week, 365 days a year. CONTINUATION OF COVERAGE - COBRA (Consolidated Omnibus Budget Reconciliation Act) If the health coverage under this plan stops because of any of the following qualifying events, you and your family members can continue coverage through a federal law called COBRA, provided: • Your employment ends (except in the case of gross misconduct) or your work hours are reduced, • You become entitled to benefits under Medicare, • Your death, • Your marriage is dissolved, • You become legally separated from your spouse (where applicable), or • Your dependent child stops being an eligible dependent. The coverage being continued will be identical to the coverage provided to persons similarly situated to whom a qualifying event has not occurred. It will continue for at least the period starting on the date of the qualifying event and ending not earlier than the earliest of the following: • The date which is at least 36 months (18 months in the case of your employment stopping or your work hours being reduced) after the qualifying event, • The date this policy stops being in force, • The date a qualified beneficiary fails to make the required payments to the County for the coverage, or • The date a qualified beneficiary, after electing this continuation, becomes either: 1. Covered under any other group health plan, or 2. Entitled to benefits under Medicare. Coverage for up to 29 months may be available if you were disabled at the time of termination or reduction in hours. Your family members can continue their coverage for up to 36 months if their coverage ends because of: • Divorce or legal separation from the employee, • The death of the employee, • The employee becoming eligible for Medicare, or • The child reaching age 19 (unless he or she qualifies as an incapacitated child or benefit eligible dependent student age 25 or younger) or no longer qualifying as a dependent under the plan. 36 Please note: You are responsible for notifying Employee Health Benefits when one of these events occurs. Employee Health Benefits will inform Delta Health Systems who will then send you an election form for COBRA enrollment and a list of conditions that apply to continued coverage. You must return the completed forms within 60 days to Delta Health Systems to enroll in COBRA coverage. If you elect to continue coverage under the plan, you must pay on a monthly basis 102% of the cost of that coverage. You must make the payment for continued coverage for the period before your election within 45 days of the date you sign the election form. After that, payment is due to Delta Health Systems before the first of the month for that month’s coverage. There is a 30-day grace period for payments. If payment is not made by the end of this grace period, your coverage will be cancelled. The coverage you receive under COBRA will be exactly the same health coverage you or your family members would have been entitled to if your employment or dependent status had not changed. Any future changes in the benefits or cost of coverage for the plan also will apply to you. This is only a summary of your rights under COBRA. If you do become eligible for COBRA benefits, you will receive a more detailed explanation of the program. In the meantime if you do have questions, please contact Employee Health Benefits. Election period There is at least 60 days during which continued coverage may be elected. The 60-day period begins on the later of: • The date coverage would have stopped due to the qualifying event, or • The date the person receives notice of the right to continue coverage. Your election to continue coverage will be considered an election on behalf of your spouse/domestic partner and dependent children who would also lose coverage because of the same qualifying event, also, a former spouse’s/domestic partner’s election to continue coverage will be considered an election for dependent children who would also lose coverage because of the same qualifying event. Notification requirements A qualified beneficiary must notify the County when any of the following qualified events happen: • Your marriage is dissolved, • You become legally separated from your spouse, • Termination of Domestic Partnership, or • A child stops being an eligible dependent. The County will send the appropriate election form to the qualified beneficiary within 14 days after receiving this notice. SPECIAL DISABILITY MEDICAL CARE BENEFIT If you terminate employment because of a disability, the plan will provide medical benefits for treatment of that disability after you terminate. The benefit is limited to the calendar year in which coverage stops and for the next calendar year as long as you are totally disabled due to the same cause for the entire time from when coverage stops until charges are made. Benefits are 37 payable only for covered expenses charged for the accidental injury, sickness or pregnancy which caused the total disability. You must be terminated in order to receive this benefit. It is provided at no premium cost to you. DENTAL CARE BENEFIT AFTER TERMINATION After you terminate employment, the plan will pay dental care benefits in the following cases if work began before you terminated: • When a tooth or teeth are first prepared for fixed bridgework, crowns, inlays, onlays or gold restorations while the person is covered and the service or supply is given within 90 days after coverage stops. • When the impression for full or partial removable dentures is taken while the person is covered and the dentures are installed within 90 days after coverage stops. • When a tooth is opened for root canal work while the person is covered and the work is completed within 90 days after coverage stops. • When accidental injury to natural teeth happens while the person is covered and supplies are given within 90 days after coverage stops. The person must be totally disabled due to the injury for the entire time from when coverage stops until charges are made. You must be terminated in order to receive this benefit. It is provided at no premium cost to you. LAYOFF OR LEAVE OF ABSENCE The County may continue coverage if you are away from work due to leave of absence or temporary layoff. For information regarding your rights under the Family and Medical Leave Act of 1993 contact the Human Resources Department. THE LIFE INSURANCE PLANS BASIC LIFE ACCIDENTAL DEATH & DISMEMBERMENT The County pays for employee Basic Life Insurance and Accidental Death and Dismemberment Insurance through ReliaStar. The Basic Life plan pays a death benefit only. There is no cash value or savings component. If you die or become seriously injured in a covered accident, the County provides you with Accidental Death and Dismemberment Insurance (AD&D). This is in addition to the Basic Life Insurance. WHO IS ELIGIBLE? You are eligible if you are an active participant in the County’s Health Plan, full-time employee who works a minimum of 32 hours a week, or if you are employed in a permanent position which is allocated for a minimum of 16 hours per week. WHEN DOES COVERAGE BEGIN? Your coverage will begin on the latest of the following dates: • The policy effective date. • The date that you joined an eligible class. • If you were required to enroll for your coverage, on the effective date shown on your enrollment form. 38 • If you were absent from work because of injury or sickness on the date your coverage would begin, your coverage will not begin until you have returned full time to the duties of your work. WHEN DOES COVERAGE END? Coverage will end on the earliest of the following: • The last day of the pay period in which your employment ends. • The first day of the pay period in which you stop being an eligible employee. • When the plan stops. Termination will not affect a claim that begins while coverage is in force. AMOUNT OF INSURANCE The plan pays a Basic Life benefit equal to $20,000 at your death. ($50,000 for Appointed and Elected Department Heads or Unrepresented Employees) The full AD&D benefit amount is $5,000. If you have an accident while covered which results in any loss listed below, the AD&D benefit will be paid as follows: For Loss of Life Two/more members One member Payment Full Benefit Full Benefit Half Benefit Member here means hand, foot or eye. Loss of hand or foot means complete severance through or above the wrist or ankle joint. Loss of an eye means the total, permanent loss of sight in the eye. The loss must occur within 365 days of the accident for the benefit to be paid. AD&D EXCLUSIONS ReliaStar does not pay benefits for injuries: • Caused by suicide, attempted suicide, or whenever you injure yourself on purpose. • Caused by war or acts of war, whether or not declared. • While you are on full-time active duty in any armed forces. • Caused by any bacterial infection that was not caused by an accidental cut, wound, or food poisoning. • Caused by travel or flight in, or getting in or out of: 1. An aircraft being used for test or experimental purposes. 2. An aircraft you are flying, are learning to fly, or are a member of the crew. 3. A military aircraft, other than transport aircraft flown by the U.S. Military Airlift Command (MAC), or a similar air transport service of another country. 4. An aircraft owned or leased by or for you, the County, or a member of your household. 5. An aircraft that does not have a valid FAA normal or transport type certificate of airworthiness. 6. An aircraft that is not flown by a pilot with a valid license. • Caused by you taking any drug that was not prescribed by a doctor. • Caused by sickness. 39 HOW TO FILE A CLAIM Employee Health Benefits should be contacted within a week of the loss. Written notice must be sent to ReliaStar by the policyholder within 30 days after the loss or as soon as reasonably possible. It must include information to identify you such as your name, address and group policy number. The policyholder is the County unless you have converted your insurance. In that case, you are the policyholder. You will be sent a claim form within 15 days after ReliaStar receives notice of your claim. The claim form must be returned within 90 days after the loss. Please contact Employee Health Benefits for more details. CLAIMS APPEALS If you or your beneficiary has any questions or concerns about claims payment, please call Employee Health Benefits CONVERSION When you leave the County, your insurance can be continued. You may convert your insurance without a physical exam by applying and paying the first premium for an individual policy within 31 days after your employment is terminated. VOLUNTARY TERM LIFE The County provides you with the opportunity to gain greater financial security for you and your family members with Voluntary Term Life (VTL) Insurance through ReliaStar. This program allows you to supplement your County-paid Basic Life and Accidental Death and Dismemberment Insurance with reliable group protection at economical rates. WHO IS ELIGIBLE? Employee You are eligible to apply for VTL insurance if you are an active, full-time employee who works a minimum of 32 hours a week, or if you are employed in a permanent position which is allocated for a minimum of 16 hours per week. Dependents You may also apply for coverage for your lawful spouse under age 70 whether or not you apply for coverage for yourself. (You may not be legally separated from your spouse.) The premium you pay for your coverage and or your spouse’s coverage will be based on your age. If spouse only coverage is desired, the premium is based on your spouse’s age. You may apply for coverage for your unmarried, dependent children under age 19 or to age 25 if a full-time student, as long as you apply for coverage for you or your spouse. Your eligible children can be insured for a single bi-weekly premium, regardless of how many children you have. No one may be covered more than once under this plan. If you are covered as an employee, you cannot also be covered as a spouse or dependent child. You must request coverage within 31 days of becoming eligible. If you want coverage for your spouse or a dependent child, you must request that coverage within 31 days of the date he or she becomes eligible. If coverage is applied for after this period, you may only apply during the open 40 enrollment. Evidence of insurability will be required in order to get coverage under this program. Evidence of insurability will also be required if your application is received by the insurance company more than 31 days after you have signed WHEN DOES COVERAGE BEGIN? All benefit amounts up to the guaranteed issue amount will be effective on the later of: • The plan effective date, • The individual’s eligibility date, or • The date you completed and the insurance company receives signed application. An individual must apply for coverage within 31 days of eligibility or he or she will be required to provide medical evidence of insurability for all benefit amounts. Amounts above the guaranteed issue will be effective the later of the plan effective date, the individual’s eligibility date, or the date the insurance company agrees in writing to insure the individual for coverage above the guaranteed issue amount. Your coverage will be effective provided you are actively at work on the effective date. If you are not actively at work on that date, your insurance coverage will begin when you return, fulltime to your duties. Coverage for your eligible spouse and children will be effective provided they are not hospitalized and can perform activities normal for persons the same sex and age. WHEN DOES COVERAGE END? Employee Coverage will stop on the earliest of the following: • The last day of the pay period in which your employment ends. • The first day of the pay period in which you stop being an eligible employee. • The first day of the pay period in which you do not make the required contribution toward your monthly premium. • When the plan stops. Spouse Spouse coverage will stop on the earliest of the following: • When there is a divorce decree. • When your coverage ends. • When you do not make the required contribution toward the monthly premium for family members. • When your spouse turns age 70. Dependent children Dependent children coverage will stop on the earliest of the following: • When the child reaches age 19 unless he or she qualifies as a benefit eligible dependent student age 25 or younger. • When he or she is no longer dependent upon you for support. • When your coverage under the plan ceases. • When you do not make the required contribution toward the monthly premium for family members. AMOUNT OF LIFE INSURANCE Employee coverage is purchased in “units” of $10,000. You can apply for as many units as you want, up to five times (5x) your base annual salary rounded up to the next $10,000 unit amount or 41 $500,000, whichever is less. However, under a feature of this insurance program, any employee may apply for up to 25 units - $250,000 - regardless of salary. The amount of your coverage will decrease as follows: • Beginning at age 70, each $10,000 unit of coverage has a value of $6,500. • Beginning at age 75, each $10,000 unit of coverage has a value of $4,500. • Beginning at age 80, each $10,000 unit of coverage has a value of $3,000. Spouse coverage is purchased in “units” of $10,000. You may apply for up to 25 units - a maximum of $250,000 - of VTL coverage for your spouse. Spouse coverage ends at age 70. Dependent children coverage is purchased in “units” of $2,000. You may apply for up to 5 units $10,000 - of coverage that protects each of your unmarried dependent children, age 6 months to 19 years, or up to 25 years if your child is a full-time student. One monthly premium will insure all your eligible children, regardless of the number of children you have. You must have coverage for at least one parent in order to have coverage for your children. Children from 0 to 14 days of age receive no coverage. For children from age 14 days to 6 months, coverage is $500 - regardless of the amount of coverage you select. After your child reaches 6 months of age, the amount of coverage you selected for your eligible children will go into effect. HOW TO APPLY To apply for coverage, see or call Employee Health Benefits for an application. Make sure you answer all the questions and indicate the amount of coverage you want for yourself, your spouse and dependent children. While rates may not be increased on an individual basis, the company reserves the right to increase rates on a group basis. ACCEPTANCE Insurance coverage is subject to satisfactory evidence of insurability and approval of the application by ReliaStar. The insurance company will require additional medical information to approve applications for certain amounts of coverage. If you apply for coverage for your spouse, ReliaStar must review and approve the application. Coverage for children, however, will not require medical underwriting if enrolled within 31 days of eligibility. HOW TO KEEP COVERAGE IN FORCE You can keep this life insurance coverage; either as part of the group plan or as an individual policy, provided you pay the premium. If you are an active regular employee of the County, the County participates in the plan, and the master group policy remains in force, you can be covered regardless of your age as long as you pay the premium when due. After age 70, benefits will be reduced. As long as premiums are paid for your spouse, his or her coverage will continue to age 70, at which time conversion can be elected. In the event of legal separation or divorce, your former spouse may continue coverage by paying the required premium directly to the insurance company. When your covered children are no longer eligible, they can apply for term coverage of their own in the amount of $25,000 or $50,000. If accepted by the insurance company, they will receive their own policies and be billed directly. 42 CONVERSION During the 31 days following your last day of employment, you can convert your group coverage to an individual permanent policy with a level premium by completing a conversion application. Coverage is guaranteed. PORTABILITY If you terminate your employment before age 70, your coverage can be continued at the same group term rates. You have the ability to elect portability, which allows you to keep the same privileges you had as an active employee, provided you apply for continuation of coverage within 31 days of your last day of employment and pay the premium directly to the insurance company. YOUR BENEFICIARY In the event of your death, benefits will be paid to your beneficiary. You will name your beneficiary on your insurance application. If you ever want to change your beneficiary, you must give written notice to the insurance company, or to Employee Health Benefits if you are still an employee. Your beneficiary can receive insurance proceeds in a single payment or in any method then offered by the insurance company. In the event your covered spouse or child dies, you (or your estate) are the beneficiary unless there is another beneficiary on file with the insurance company. FILING CLAIMS To file a claim for benefits, you or your beneficiary should request a claim form from Employee Health Benefits. Complete the claim form according to directions and return it to Employee Health Benefits. From the date the beneficiary’s notice of claim is returned, ReliaStar has 90 days to review the claim to determine whether or not benefits are payable in accordance with the terms and provisions of the group policy. Under special circumstances ReliaStar may require an extension of this 90 day period and will send written notice prior to the end of the initial 90 days informing the beneficiary of the need for an extension. Once the claim has been approved, the beneficiary will receive the appropriate benefit. EXCLUSION Benefits are not paid for suicide during the first 2 years of coverage. CLAIMS APPEALS If you or your beneficiary has any questions or concerns about claims payment, please call Employee Health Benefits. VOLUNTARY ACCIDENTAL DEATH AND DISMEMBERMENT The Voluntary Accidental Death and Dismemberment (VAD&D) plan is provided through Hartford. The plan offers full 24-hour accident protection anywhere in the world, on or off the job, on business, vacation, or at home. Air travel is included while you and your family members are flying as passengers only, subject to the exclusions as shown. WHO IS ELIGIBLE? Employee 43 You are eligible to apply for VAD&D insurance if you are an active, full-time employee who works a minimum of 32 hours a week, or if you are employed in a permanent position which is allocated for a minimum of 16 hours per week. Dependents You may also apply for coverage for your lawful spouse under age 70 whether or not you apply for coverage for yourself. (You may not be legally separated from your spouse.) You may apply for coverage for your unmarried, dependent children over age 14 days and under age 19 or age 25 if a full-time student, as long as you apply for coverage for you. Your eligible children can be insured for a single bi-weekly premium, regardless of how many children you have. No one may be covered more than once under this plan. If you are covered as an employee, you cannot also be covered as a spouse or dependent child. You must request coverage within 31 days of becoming eligible. If you want coverage for your spouse or a dependent child, you must request that coverage within 31 days of the date they become eligible. After that date, employees will be given an opportunity to sign up during the open enrollment period. No evidence of insurability will be required. WHEN DOES COVERAGE BEGIN? All benefit amounts will be effective on the later of: • The plan effective date, • The individual’s eligibility date, or • The date you completed and the insurance company receives signed application. Your coverage will be effective provided you are actively at work on the effective date. If you are not actively at work on that date, your insurance coverage will begin when you return, fulltime to your duties. Coverage for your eligible spouse and children will be effective provided they are not hospitalized and can perform activities normal for persons the same sex and age. Please read the Hartford brochure for more on the insurance effective date. WHEN DOES COVERAGE END? Employee Coverage will end on the earliest of the following: • The last day of the pay period in which your employment ends. • The first day of the pay period in which you stop being an eligible employee. • The first day of the pay period in which you do not make the required contribution toward your monthly premium. • When the plan stops. Spouse Spouse coverage will stop on the earliest of the following: • When there is a divorce decree. • When your coverage ends. • When you do not make the required contribution toward the monthly premium for family members. • When your spouse turns age 70. Dependent children Dependent children coverage will stop on the earliest of the following: 44 • • • • When the child reaches age 19 unless he or she qualifies as benefit eligible dependent student age 25 or younger. When he or she is no longer dependent upon you for support. When your coverage under the plan ceases. When you do not make the required contribution toward the monthly premium for family members. AMOUNT OF VAD&D Your benefit amount is purchased in “units” of $25,000. You can apply for as many units as you want: however, amounts in excess of $150,000 are limited to ten times (10x) your base annual salary rounded up to the next $10,000 unit amount or $300,000, whichever is less. You may choose either 100% or 50% of your selected benefit amount as your spouse’s benefit to a maximum of $300,000. Spouse coverage ends at age 70. Your children may be covered at 10% of your benefit amount to a maximum of $30,000. One monthly premium will insure all your eligible children, regardless of the number of children you have. You must be covered in order to have coverage for your children. Children from 0 to 14 days of age receive no coverage. HOW TO APPLY To apply for coverage, see or call Employee Health Benefits for an application. Make sure you answer all the questions and indicate the amount of coverage you want for yourself, your spouse, and dependent children. While rates may not be increased on an individual basis, the company reserves the right to increase rates on a group basis. HOW TO KEEP COVERAGE IN FORCE You can keep this insurance coverage; either as part of the group plans or as an individual policy, provided you pay the premium. If you are an active regular employee of the County, the County participates in the plan and the master group policy remains in force, you can be covered regardless of your age as long as you pay the premium when due. After age 70, benefits will be reduced. As long as premiums are paid for your spouse, his or her coverage will continue to age 70, at which time conversion can be elected. In the event of legal separation or divorce, your former spouse may continue coverage by paying the required premium directly to the insurance company. Coverage for your dependent children will continue until your coverage terminates, when their premiums are not paid, or when they no longer qualify for coverage. COVERAGE If bodily injuries result in death or dismemberment within one year of the date of the covered accident, the plan will pay as follows: For loss of Life Payment Full benefit 45 Two/more members Speech and hearing Speech or hearing One member Thumb and index finger of same hand Full benefit Full benefit Half benefit Half benefit 3/4 benefit Member here means hand, foot, or eye. Loss of hand or foot means complete severance through or above the wrist or ankle joint. Loss of an eye means the total, permanent loss of sight in the eye. Only one amount, the largest to which you are entitled, is paid for all losses resulting from one accident. ADDITIONAL BENEFITS Special benefit schedule for insured children. Severe accidental injuries to a child can result in continuing medical expenses, rehabilitation programs, and the need for a specialized education environment. These financial consequences can extend far beyond the time frame of the original loss. Therefore, to help parents cope with such financial consequences, the plan provides special “living” benefits designed specifically for insured children: For loss of Payment Two/more members Double benefit One member Full benefit Thumb and index finger of same hand Half benefit Quadriplegia Double benefit Paraplegia/Hemiplegia Full benefit One hand, one foot or sight of one eye Half benefit Member means hand, foot, or eye. Quadriplegia means total paralysis of both upper and lower limbs. Paraplegia means total paralysis of both lower limbs. Paraplegia means total paralysis of upper and lower limbs on one side of the body. Paralysis means loss of use, without severance, of a limb. This loss must be determined by a physician to be complete and not reversible. The maximum doubled plan benefit amount payable under this provision is $50,000 and the maximum full benefit amount is $25,000. Only one amount, the largest to which the child is entitled, will be paid for all losses resulting from one accident. If the child dies within 90 days of the covered accident or if death occurs within 90 days after the child sustains an accidental loss specified above, the maximum amount payable will be limited to the plan death benefit amount, subject to a maximum of $25.000. Education benefit The Voluntary AD&D plan has a special feature that can help cover the educational costs of your college-aged children in the event of your death. If you have selected the family plan coverage and then die in a covered accident while the policy is in force, the insurance company will pay, in addition to all other benefits, 2% of your benefit amount (to a maximum of $5,000 per year) on behalf of any dependent child, who on the date of the accident, was enrolled as a full-time student in any institution of higher learning beyond the 46 12th trade level, or, was at the 12th grade level and subsequently enrolls as a full-time student in an institution of higher learning within 365 days following the accident. The benefit is payable each year for a maximum of four consecutive annual payments but only if the dependent child continues his or her education. If at the time of the accident, family plan coverage is in force, but there are no dependent children, the insurance company will pay an additional benefit of $1,000 to your designated beneficiary. Spouse training benefit The plan also can help with the costs of your spouse’s training in the event of your death. This benefit is payable only for costs incurred during the first year of the training refresher course. If you have elected to insure your spouse, and then lose your life within a year of, and as a result of, a covered accident, the insurance will pay, in addition to all other benefits, up to $3,000 for actual costs incurred if your surviving spouse enrolls in an accredited school for the purpose of retraining or refreshing skills needed for employment. Coma benefit The coma benefit is payable if you or your insured spouse or insured children become comatose within 31 days after (and as a result of) a covered accident and remain comatose beyond the waiting period. Comatose or coma means being in a profound stupor or a state of deep and total unconsciousness. The waiting period is the 31 days from the date you or your insured spouse or insured children become comatose. Following the waiting period, comatose or coma means being in a profound stupor or a state of deep and total unconsciousness. The waiting period is the 31 days from the date you or your insured spouse or insured children become comatose. Following the waiting period, payment is made in monthly installments equal to 1% of the comatose insured’s principal sum as indicated in the policy. These payments will cease after 11 installments have been paid, the insured’s recovery from the coma, or death, whichever occurs first. In addition to the monthly installments specified above, if the insured is still in a coma as the result of a covered accident after the 11 monthly installments have been paid’ the insured is entitled to a lump sum payment equal to the full principal sum under the dismemberment and paralysis schedules of the policy less any amounts already received. If the principal sum is paid under the coma benefit, coverage under the policy ends and no additional benefits will be payable for subsequent death or dismemberment under the policy. Coma benefit payments are made to the comatose insured’s legal guardian or if there is none, the person, who in the opinion of the company, is responsible for the insured’s care. If the insured dies as a result of a covered accident while monthly coma benefits are payable, benefits for accidental death will be paid to the insured person’s beneficiary. In addition to the plan’s general exclusions, no coma benefit payments will be made for loss resulting from sickness, disease, bodily infirmity or medical or surgical treatment thereof, or bacterial or viral infection. Any bacterial infection caused by covered accidental injury or food poisoning is covered. 47 Seatbelt benefit This special benefit is payable if an insured person dies as the result of injuries sustained in a covered accident while driving or riding in a private passenger car equipped with seatbelts. If that person had been protected by a properly fastened seatbelt (or if the insured is a child, by a child restraint as defined by state law), the plan’s benefit will be increased by 10%, but not by less than $1,000 nor by more than $10,000. The correct position of the seatbelt must be certified to by the investigating officer or included in the official report of the accident, and a copy of the police accident report must be submitted with the claim for this benefit. If it is unclear whether the insured had been wearing the required protection, the plan will pay a benefit of $1,000 to the designated beneficiary. *A validly registered four-wheel private passenger car (or policyholder-owned car), station wagon, jeep, pick-up truck, or van-type car. Felonious assault benefit (Employee only) If accidental death or dismemberment is sustained by you while at work or while traveling on company business as a result of felonious assault (inflicted by person other than fellow employees or member of your family or household), robbery, holdup or attempted holdup, or kidnapping during a holdup, your benefit amount will be increased by 25%. EXCLUSIONS The Voluntary AD&D policy does not cover loss resulting from intentionally self-inflicted injuries or any attempt threat: commission of a felony by the insured; war or any act of war, while on full-time, active duty in the armed forces; sickness, disease or bodily or mental infirmity or medical or surgical treatment thereof or bacterial or viral infection, regardless of how contracted (except as noted previously); while traveling in aircraft being used by or for the policy-holder; travel in experimental aircraft or aircraft used or designed for use beyond the earth’s atmosphere; travel in aircraft operated by a military authority other than MAC (Military Airlift Command) or similar service of another country; hang gliding; parachuting (except for self-preservation); and while serving as a pilot, crew member, or student taking a flying lesson, in any aircraft. CONVERSION If you leave the County, or if, for any reason other than non-payment of premium, this group coverage is terminated before you reach age 70, you may convert your insurance to coverage under an individual policy at the premium then in effect for your age and occupation, provided you make application for the conversion policy and pay for the first premium within 31 days after termination of your group coverage. Medical certification is not required to obtain a conversion policy. Coverage cannot exceed the amount purchased under your group plan and cannot be less than $25,000 nor more than $250,000. Insurance on family members can also be converted. Coverage under the conversion policy will provide full benefit amount payment for accidental loss of life or loss of two or more members (head, foot, eye), one-half benefit amount for loss of one member, and one-quarter benefit amount of loss of thumb and index finger of the same hand. DEFINITIONS These are the general definitions for terms used throughout the book unless otherwise specified in a particular section. Accidental injury. Physical harm caused by a sudden and unforeseen event at a specific time and place. 48 It is independent of illness, except for infection of a cut or wound. Actively Working. The active performance of an employee’s normal job duties at the County’s usual place and places of business. Allowable Charge. The fee that the provider has agreed to accept as full payment for medically necessary covered services. Ambulatory Surgical Center. Any public or private establishment with an organized medical staff of physicians; permanent facilities that are equipped and operated primarily for the purpose of performing surgical procedures; continuous physician services whenever a patient is in the facility; and which does not provide services or accommodations for patients to stay overnight. Appeal. Refers to any enrollee’s right to request review of decisions relating to the enrollee’s rights under the Plan. Approved Alcoholism or Drug Treatment Facility. A facility licensed by the state in which it is located to treat alcoholism or drug addiction. Beneficiary. Your beneficiary is the person or persons who will be paid if you die while covered by the plan. A person becomes your beneficiary only if you have named that person on the card you sign when you enroll. You may change your beneficiary at any time by filling out a change of beneficiary form. The form must be received and recorded by the County before the change becomes effective. Blue Cross Network. Blue Cross Network is a statewide provider organization providing all hospital services and those physician services in California but outside of Mendocino County. A managed care organization providing prior authorization, hospital review, case management, managed mental health and chemical dependency services outside of the County of Mendocino within the State of California. Calendar Year. A period commencing at 12:01 a.m. on January 1 and terminating at 12 midnight Pacific Standard Time on December 31 of the same year. Chemical Dependency. A Condition characterized by a physiological or psychological dependence, or both, on alcohol or a state-regulated controlled substance. It is further characterized by a frequent or intense pattern of pathological use, to the point that the user loses self control over the amount and circumstances of use; develops symptoms of tolerance, or psychological and/or physiological withdrawal if use is reduced or stopped; substantially impairs or endangers his or her health or substantially disrupts his or her social or economic function. Chemical dependency includes alcohol and drug psychoses, and alcohol and drug dependence syndromes. Children. Includes stepchildren, foster children and legally adopted children to age 19, dependent children through age 25 are eligible if they are attending an accredited school, college or university on a full-time basis. Chiropractic Services. A system of therapy which holds that disease results from a lack of normal nerve function and which employs manipulation and specific adjustment of body structures. 49 Co-insurance. The out-of-pocket percentage you pay which is also subject to a maximum outof-pocket limit. Cosmetic Procedure. Any surgery, service, drug or supply designed to improve the appearance of an individual by alteration of a physical characteristic which is within the broad range of normal but which is considered unpleasing or unsightly. Covered Charge. See definition for Usual, Customary, and Reasonable (UCR). Covered Family Members. You and your wife or husband and dependent children who are covered under the plan. Custodial Care. Care provided either in the home or in a facility primarily for the maintenance of the patient or which is designed essentially to assist the patient in meeting his or her activities of daily living and which is not primarily provided for its therapeutic value in the treatment of illness or accidental injury. Custodial care includes, but is not limited to, help in walking, bathing, dressing, feeding (including the use of some feeding tubes not requiring skilled supervision), preparation of special diets, and supervision over self administration of medication not requiring constant attention of trained medical personnel. Deductible. A specified dollar amount of covered expenses which must be incurred during a benefit period before any other covered expenses can be considered for payment according to the applicable benefit percentage. Delta Health Systems. A third party administrator which is located in Stockton, CA and provides claims processing, member eligibility, and customer services. Dentist. A person licensed to practice dentistry by the appropriate authority in the area where the dental service is given. Domestic Partner. Please see the Human Resources website at www.co.mendocino.ca.us/hr/ for information regarding covering qualified domestic partners. Durable Medical Equipment. Mechanical equipment that can stand repeated use and is used in connection with the direct treatment of an illness or accidental injury. It is of no use in the absence of illness or accidental injury. Elective (Non-emergency) Services. Services provided when the patient’s condition permits adequate time to schedule the necessary diagnostic work-up and/or initiation of treatment. Eligible employee. Full-time employee and employee who is employed in a permanent position which is allocated for a minimum of 16 hours per week. Emergency Care Services. Those services required for alleviation of severe pain or the immediate diagnosis and treatment of an unforeseen medical condition which if not immediately diagnosed and treated could lead to further disability or death, or which would so appear to a prudent layperson. Experimental or Investigational. Any treatment, therapy, procedure, drug or drug usage, facility or facility usage, equipment or equipment usage, device or device usage, or supplies 50 which are not recognized in accordance with generally accepted professional medical standards as being safe and effective for use in the treatment of an illness, injury, or condition at issue. Services which require approval by the federal government or any agency thereof, or by any state governmental agency, prior to use, and where such approval had not been granted at the time the services were rendered, shall be considered experimental or investigational. Services which themselves are not approved or recognized as being in accord with accepted professional medical standards, but nevertheless are authorized by law or a government agency for use in testing, trials, or other studies on human patients, shall be considered experimental or Investigational. Any issue as to whether a protocol, procedure, practice, medical theory, or treatment is experimental or Investigational will be resolved by Delta Health Systems, HCE and/or Blue Cross, which will have full discretion to make such determination on behalf of the Plan and its participants. Full-time Student. Your dependent child who physically attends classes at a school with a regular teaching staff, curriculum, and student body and attends the school for the number of credits, hours, or courses required by the school for full-time students. Health Care Evaluation (HCE). A managed care organization based in Stockton providing primary care referral services (out of network only), prior authorization, hospital review, case management, managed mental health and chemical dependency services within the County of Mendocino and Out of the State of California. Home Health Care. In-home care provided when you are unable to leave home because of illness or injury but do not need the full inpatient services of a hospital or skilled nursing facility. It may include nursing care by a licensed nurse (RN, LPN); physical, respiratory, speech, and occupational (except diversional) therapy; home health aid services; and other services which are medically necessary and which would have been covered if the patient were hospitalized. Hospice Care. Care received under a program that is: (1) designed to provide palliative and supportive care to individuals who have received a diagnosis of terminal illness; (2) supportive to the covered family members by providing certain services; (3) licensed or certified in the jurisdiction where the program is established; (4) directed and coordinated by medical professionals; and (5) approved by the Plan. Hospital 1. A licensed facility which is primarily engaged in providing, for compensation, medical, diagnostic and surgery facilities for the care and treatment of ill and injured persons on an inpatient basis, and which provides such facilities under the supervision of a staff of physicians and 24-hour-a-day nursing service by registered nurses. An institution which is principally a rest home, nursing home or home for the aged is not included; or 2. A psychiatric hospital licensed by the California State Department of Health Services; or 3. A facility operated primarily for the treatment of chemical dependency and licensed by the California State Department of Health Services; or 4. A psychiatric health facility as defined in Section 1250.2 of the Health and Safety Code. Incurred Charge. A charge shall be deemed “incurred” on the date the particular services or supply is provided or obtained. The Foundation for Medical Care FMC is a physician organization providing physician services in Mendocino County. Injury. A bodily injury sustained suddenly and accidentally during the period of coverage. 51 Inpatient. An individual who has been admitted to a hospital as a registered acute bed patient (overnight) and is receiving services which could not be provided on an outpatient basis, under the direction of a physician. Medical Facility. A hospital, skilled nursing facility, a state-approved facility for treatment of chemical dependency, or hospice. Open Enrollment. A period of time established by the County during which eligible employees may enroll in a health benefits plan, add family members, or change their enrollment from one health benefits plan to another without having a qualifying event. Open enrollment is currently set for November or December of each year. Other Services and Supplies. Services and supplies furnished to the individual and required for treatment, other than the professional services of any physician and any private duty or special nursing services (including intensive nursing care by whatever name called). Outpatient. An individual receiving services under the direction of a physician but not incurring overnight charges at the facility where services are provided. Participating Pharmacy. A pharmacy, which is under a valid agreement with RxAmerica, to provide prescriptions drug services to plan members. Person Eligible under Medicare. You or your dependent if eligible to enroll and be covered under the voluntary portion of Medicare. Pharmacy. A licensed establishment where prescription drugs are dispensed by a pharmacist licensed under the laws of the sate where such pharmacist practices. Physician. A physician is a provider who is licensed and qualified as a doctor of medicine and surgery (M.D.), doctor of osteopathy and surgery (D.O.). and doctor of podiatry (D.P.M). Pre-Admission Tests. Tests performed on you or your dependent in a hospital before confinement as a resident inpatient provided they meet all of the following requirements: • The tests are related to the performance of scheduled surgery. • The tests have been ordered by a physician after a condition requiring surgery has been diagnosed and hospital admission for surgery has been requested by the physician and confirmed by the hospital. • You or your dependent are subsequently admitted to the hospital, or the confinement is concealed or postponed because a hospital bed is unavailable or because there is a change in your or your dependent’s condition which precludes the surgery. Pre-Existing Condition. An illness, injury or condition which existed during the six (6) months prior to the enrollment date of coverage if, during that time, any medical advice, diagnosis, care or treatment was recommended or received from a licensed health practitioner. Preferred provider. Any provider who is part of the FMC or Blue Cross networks or who is listed in your “Provider Directory” as preferred. Prescription Drugs: (1) all drugs which under federal or state law require the written prescription of a physician, dentist podiatrist or osteopath; (2) insulin; (3) hypodermic needles 52 and syringes if prescribed by a physician for use with a covered drug; (4) glucose test strips; and (5) such other drugs and items, if any, not set forth as an exclusion. Preventative Care. Under Wellness, which includes annual physical exams, pap smears, mammograms, PSA tests, wellness counseling, well-baby and well-child checkups, immunizations. These are paid at 100% with no deductible. Primary Care Physician (PCP). The enrollee’s health care provider who treats most problems, keeps track of member's medical history, performs annual physical exams, and refers member to specialists. Prior Authorization. Required of enrollee’s before admitted for inpatient hospitalization except for in an emergency situation. Prosthesis (or Prostheses). The replacement of a missing body part or an organ by an artificial substitute. Provider. A physician or other health care professional or facility named in this program that is licensed, registered, or certified as required by the state in which the services were received to provide a medical service or supply, and who does so within the lawful scope of that license, registration, or certification. Psychiatric Care. Psychoanalysis, psychotherapy, counseling or other care most commonly provided by a psychiatrist, psychologist, licensed clinical social worker, or marriage, family and child counselor to treat a nervous or mental disorder, or to treat mental or emotional problems associated with illness or injury. Psychiatric Condition. A condition listed in the current edition of “Diagnostic and Statistical Manual of Mental Disorders”. Psychiatrist. A physician that deals with mental, emotional, or behavioral disorders. Psychologist. A person with a doctoral degree in psychology (Ph.D.) licensed in the State of California to provide clinical psychology services, including psychotherapy and psychological testing. Qualifying Event. Includes marriage, divorce, birth, death, adoption, legal separation, or a qualified change in the employment status of a plan member or spouse. Rehabilitation or Rehabilitative Care. Care furnished primarily to restore an individuals’ ability to function as normally as possible after a disabling disease, illness, injury or addiction. Rehabilitation or rehabilitative care services consist of the combined use of medical, social, educational, occupational/vocational treatment modalities and are provided with the expectation that the patient has restorative potential and will realize significant improvement in a reasonable length of time. Room and Board. Room, board, general duty nursing, intensive nursing care by whatever name called, and any other services regularly furnished by the hospital as a condition of occupancy of the class of accommodations occupied, but not including professional services of physicians nor special nursing services rendered outside of an intensive care unit by whatever name called. 53 Rx Generic: Represents drugs that have lost their patent exclusively. The original patent has expired and drug manufacturers produce generic versions of the original branded product. The generic version of the drug contains the exact same active ingredient as the brand product. In fact, some of the generic drugs are actually made by the original brand manufacturer and simply marketed under the generic label. Rx Brand: Denotes a drug, which is marketed by only one manufacturer without a generic product available. The manufacturer will hold the patent or exclusive rights to a brand drug until the patent period expires. Once the patent expires, generic manufacturers can replicate the brand product. These represent the most expensive or costly drugs available. Rx Brand with Generic: This simply means that there is a generic version of the original on the market. Since the generic version of a drug also represents a dramatic difference in price, the member is required to pay the difference in cost if they select the brand product. Rx Formulary: The words “Formulary” and “Preferred” mean exactly the same thing and can be interchanged. A drug formulary or preferred drug list represents a list of drugs that is compiled to offer high quality, cost-effective, rational drug therapy. Services. Includes medically necessary health care services and medically necessary supplies furnished incident to those services. Sickness. The term “sickness” used in connection with newborn children will include congenital defects and birth abnormalities, including premature births. Skilled Care. Skilled supervision and management of a complicated or extensive plan of care for a patient institute and monitored by a physician, in which there is a significantly high probability as opposed to a possibility, that complications would arise without the skilled supervision or implementation of the treatment program by a licensed nurse or therapist. Skilled Nursing Facility. A medical facility providing services that require the direction of a physician and nursing supervised by a registered nurse, and that is approved by Medicare or would qualify for Medicare approval if so requested. Social Worker. Only a person who specializes in clinical social work and is licensed or certified as a clinical social worker by the Board of Behavioral Science Examiners. Temporomandibular Joint (TMJ) The joint that connects the lower jaw (mandible) to the skull. Specialist. One who devotes himself/herself to a special occupation or branch of learning. Terminal Illness. An illness in which it is reasonably certain that the patient has less than six (6) months to live. The patient’s treating physician must provide written certification that the patient is terminally ill. Total Disability 1. With respect to an employee or person otherwise eligible for coverage as an employee, a disability, which prevents the individual from working with reasonable continuity individual reasonably, might be expected to engage; 54 2. With respect an annuitant or a family member, a disability which prevents the individual from engaging with normal or reasonable continuity in the individual’s customary activities or in those in which the individual otherwise reasonably might be expected to engage. Usual, Customary, and Reasonable (UCR) also Covered Charge. The charge, which is most frequently charged to most patients or customers for a similar service or procedure (usual)within a region. The range of charges by poviders within a region for administering a similar service or procedure. Sometimes there are too few providers in your area to show a customary range. When this happens, we will determine the amount we will pay based on the customary range in a wider geographical area (customary). Unusual circumstances or complications that may require additional time, skill, and experience in providing a particular service or procedure (reasonable). Wellness. A Program within the County which includes educational presentations, resource materials, health risk appraisals, some health screenings, activities and further education to encourage healthy behavior changes and support individuals to attain the new healthier behavior. This program is available to all enrollee’s and their family. 55





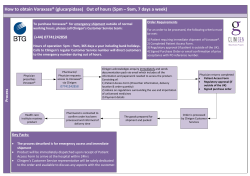



© Copyright 2026