
Conference Topics Announced!
Services Tools & Solutions Conference Topics Announced! Join us in Philadelphia, May 16-17 for our 2012 Annual Conference "Developing a Culture of Change: The Picture of Compliance". The topics for this year's conference will cover: CMS CoPs Environment of Care & Life Safety Tracer Activity Patient-Provider Communication Testimonials C&A E-Newsletter Contact January 30, 2012 Struggling With How to Manage Your IC Calendar? By: Jill Ryan, HACP Organizations often struggle with the planning, monitoring and evaluation requirements related to infection prevention and control requirements. These activities are vital to the integrity of an organization’s infection control program. A breakdown in the process cannot only lead to RFIs during survey, but much more importantly, to compromises in the program resulting in patient safety issues. Organizations that follow a planned, consistent approach to these activities demonstrate a commitment to reducing risk from healthcare acquired infections and to the well-being of hospital staff, LIPs and visitors. The following outlines a suggested annual calendar of activities that can be amended to meet the needs and timeline of any organization. Calendar Month January Fiscal Year Month st 1 month February 2 month March End of 1 Quarter th 4 Month Care Planning Meaningful Use Register now to receive the early bird discount at $549/person! About C&A April nd st Activity Annual review and update of Infection Control Plan Effectiveness of prior year goals and implementation of activities Development of current year goals based on identified risks and factors outlined in IC.01.04.01 (and last year’s results) Review and updating of infection prevention and control activities Quarterly analysis of surveillance activities, hand hygiene practice, outbreaks, etc. Review and updating of infection and prevention policies and procedures New Publication! C&A has developed the CMS ESRD Compliance Forecaster to aid your organization in tracking compliance with CMS' CfC requirements for End Stage Renal Disease facilities! Finally, your organization can have a simple method for tracking compliance with all of the ESRD CfCs in one convenient electronic document! Get yours today! th May 5 Month June July End of 2 Quarter th 7 Month August 8 Month September End of 3 Quarter th 10 Month th 11 Month Fiscal Year End October November December nd th rd Updating/Affirmation of identification of person with clinical authority for infection prevention and control program (assuring “Letter of Authority” is present in the employee or Medical Staff member’s file) Quarterly analysis of surveillance activities, hand hygiene practice, outbreaks, etc. Review of allocation of resources to support infection prevention and control initiatives Updating and implementation of flu vaccine program Quarterly analysis of surveillance activities, hand hygiene practice, outbreaks, etc. Annual IC education (in conjunction with International Infection Prevention Week) Report flu vaccination rate; analysis of reasons for LIP and staff declination of vaccine Risk assessment based on patient population, care, treatment and services, surveillance activities and past year’s data Were You Aware? 1. We’re starting off the New Year with an old topic! With continued focus on infection prevention and control, a few reminders: a) Be sure that appropriate staff can speak to the process for monitoring temperature, humidity, air exchanges and any other key environmental factors and that documentation of such monitoring is available. Items to consider: i. Temperature of kitchen dishwashers ii. Temperature & humidity in surgical settings iii. Air exchanges in central processing areas b) Laryngoscope blades are to be sterilized or processed using high-level disinfection. They then must be packaged in some way to maintain integrity. c) Check out the article in this edition of C&A e-News for an annual IC planning calendar! 2. Some revisions to the TJC accreditation requirements have recently been published. See the pre-publication standards for: a) LD.03.01.01 which broadens the culture of safety requirements to include “behaviors that undermine a culture of safety.” b) MM.02.01.01 requiring organizations to consider “populations served” when selecting and procuring medications c) Under the Ambulatory Health Care Accreditation program, see new requirements related to patient notices, for ambulatory surgical centers using TJC for deemed status. 3. Hospitals seeking TJC Advanced Certification for Palliative Care may be eligible for a grant from the LIVESTRONG® foundation. See this link to TJC’s website for more information. 4. C&A has updated its resource to provide a summary of topics requiring education for hospital staff members and LIPs. We hope you will enjoy this useful resource! Were You Aware 2012 Recap Maintaining a Patient-Safe Environment According to the Centers for Disease Control and Prevention, one out of twenty hospitalized patients will have a hospitalacquired infection. The estimated financial impact on US hospitals ranges from $28 billion to $45 billion (with a "b") dollars annually! The link between appropriate maintenance of the physical environment and the provision of clinical care is key to infection prevention. Join our March 19th webinar to learn how to integrate environmental and infection prevention rounds and tracer activity and engage non-clinical and clinical staff in identifying and managing associated patient safety risks. Contact us at (704) 573-4535 or [email protected] for more information! Courtemanche & Associates Charlotte, NC | Parsippany, NJ Phone 704-573-4535 | Fax 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions What's New? What's Scoring? How Can We Fix It!? Testimonials C&A E-Newsletter About C&A Contact February 29, 2012 Believe it or not, the end of the first quarter of 2012 is drawing near! What are we seeing in organizations that have been surveyed in the last few months? Will 2012 trends differ from those we saw in 2011? What are organizations doing to comply with the new patient-provider communication and visitation requirements? What documents are surveyors really reviewing? Join us for our April 16th webinar, "What's New? What's Scoring? How Can We Fix it?" to get the answers to these, and many more, questions! For more information and to register, visit www.courtemancheassocs.com, Have You Registered Yet? You won't want to miss out on our 2012 Annual Conference hosted in Philadelphia, PA on May 16th - 17th! The topics for this year's conference cover CMS CoPs, Environment of Care & Life Safety, Tracer Activity, Patient Provider Communication, Care Planning and Meaningful Use! Ann Scott Blouin, Executive Vice President for the Division of Accreditation and Certification Operations at The Joint Commission, will be this year's keynote speaker! We will also have an interactive session directly with Joint Commission to navigate through the new TJC E-Application! Sign up now! Early Bird Rate is still available! contact us at [email protected] or call us at (704) 573-4535. Developing "Plans" That Meet Regulatory Requirements - A Quick Primer By: Nancy McLean, RN, BSN, MSHA, NHA, HACP We Want to Hear From You! C&A prides itself on delivering accurate and relevant information to the healthcare industry. As we are constantly trying to improve our newsletter, we ask that you take 5 minutes to complete the online survey below. Your responses will help us to address any issues that you may have as well as to better design our enewsletter to meet your needs. Click Here to take the 5 minute survey! To meet regulatory and accreditation requirements, organizations must develop and implement several plans and perform annual, or as needed, evaluations of their effectiveness. Plans requiring an annual review include the five Environment of Care plans (that can be incorporated into one overall Environmental or Safety Plan): Safety and Security Hazardous Materials and Wastes Fire Safety Medical Equipment Utilities Management In addition to these, The Joint Commission also requires plans in the following areas: Emergency Operations with a twice a year drill and evaluation Infection Prevention and Control that is evaluated annually Capital expenditure plan updated annually The appropriate chapters in The Joint Commission’s Comprehensive Accreditation Manual for Hospitals (2012) list the specific requirements for each plan. Commonalities among the processes for developing and evaluating plans include: Assigned responsibility for oversight Development of related policies and procedures using evidence-based practices in their development Completion of a risk assessment Development of measurable goals based on the results of the risk assessment Prioritization of the measurable goals selected Measuring and assessing the effectiveness of the plan in meeting the prioritized goals Leadership input and approval on the recommended priorities and final plan While each hospital may take a different approach to this planning and evaluation function, based on organizational structure, here are some helpful hints to assure a robust process. Completion of the annual risk assessment includes a review of data and progress made toward the prior year’s goals. To assure a process that demonstrates compliance with requirements and is meaningful to operations, the review of data should be accomplished through easy-to-view graphs or by other statistical methods easy to understand. It is recommended that these graphs be incorporated into the final evaluation of the year’s plan and provide a picture of whether of not goals were achieved. The evaluation of the prior year’s plan can be a separate document included in the appropriate committee meeting minutes or it can be incorporated into the coming year’s plan. It is important to review the data from the prior year to determine whether goals were achieved at the levels specified. Goals that were achieved and have a track record for sustainability can be dropped. Goals that were not achieved need to be examined closely to determine if they should be carried into the next year’s plan. To assure compliance to the requirement it would be prudent to report the progress toward goals to the Performance Improvement Committee (or the organization’s equivalent committee) on a scheduled basis, monthly or quarterly. Remember that selected goals should be approved by the appropriate committee and senior leaders of the organization. The goals should also be shared with the departmental staff affected by the goals and those that can influence the achievement of the goals. In addition to the plans outlined above, “as needed” evaluations are required for plans that address: Utilization Review (if not in a binding review agreement with a Quality Improvement Organization (QIO)) Managing internal and external information and interruptions in the information (IT) process Provision of nursing care and nurse staffing Quality control plans for Waived Tests evaluated as needed Creating an annual organizational calendar can help assure that these plans are updated and evaluated as necessary. Were You Aware? 1. CMS has provided clarification and revised interpretive guidance on the issue of orders for rehabilitation and other outpatient services. In its Survey & Certification Memo dated February 17, 2012, CMS clarified that it is not its intent to limit those permitted to order or make referrals for such services only to practitioners credentialed and privileged by the organization. As is fully outlined in the S&C Memo, orders for outpatient services can be accepted from non-credentialed LIPs as long as the hospital has a process for assuring the orderer is licensed in the state and practicing within their scope. This process needs to be defined in policy and approved by the governing body. 2. The Joint Commission has launched its new EApplication. In addition to the improvements made to the E-App, TJC is also requiring organizations to update their applications at 9, 18 and 27 months post-survey. Organizations are reminded that they must also still meet the requirements under APR.01.03.01 and report any “changes in ownership, control, location, capacity or services offered” within 30 days of the change. 3. Just a reminder that the tracking and logging requirements for tissue and transplant products begins at the point of entry into the hospital. So, if those products are received by the Receiving Department as they arrive on the loading dock before being transported to the responsible department, the tracking process begins with Receiving. That would include verification of package integrity and required temperature monitoring as applicable. 4. Hospital organizations acquiring physician practices are encouraged to consider the regulatory implications in the initial stages of that process. If the physician practice will meet TJC’s organizational and functional criteria for survey applicability under the hospital, then the practice must meet accreditation requirements. This is often a challenge for previously independent physician offices. Issues including the physical environment of the practice, infection control practices, medical record content and responsibilities of professional and support staff should be reviewed. (2012). Be compliance-ready: what to consider when acquiring a physician practice. Journal of Healthcare Management, 57(1), 12-16. 5. Patient identification is starting to re-emerge as a hot topic for organizations. Issues include staff being unable to articulate the organization’s designated identifiers, not using the identification process, not labeling specimens in the presence of the patient. This might be an area where a “mini-tracer” can identify circumstances related to non-compliance so that process improvements can be made. 2012 Were You Aware Recap Courtemanche & Associates Charlotte, NC | Parsippany, NJ Phone 704-573-4535 | Fax 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions Early Bird Ends Next Week! You won’t want to miss out on our 2012 Annual Conference hosted in Philadelphia on May 16th & 17th! Ann Scott Blouin, Executive Vice President for the Division of Accreditation and Certification Operations at The Joint Commission will be this year's keynote speaker! We will also have an exciting, interactive session directly with Joint Commission to navigate through the new TJC EApplication! Sign Up Now! The Early Bird Rate ends April 5th! Click Here to view the 2012 Conference Brochure! Testimonials C&A E-Newsletter About C&A Contact March 30, 2012 It Could Happen To You... C&A is excited to present "It Could Happen to You," hypothetical case studies for you to solve. These are scenarios that could happen during your next survey, during the postsurvey process, or any average day. We have dramatized a situation to seek your reaction and input. So, take a moment, review the case, and provide us with your opinion on the scenario, because it could happen to you! We want to hear from you ... send us your thoughts and comments at [email protected]. We will share your insights in our next issue! "The Case of the Care Before the Patient" Was Mary Right or Over-Reacting? Mary is at the command center and it's the first day of her Joint Commission (TJC) survey. The surveyor is tracing patients in the Perioperative area when Mary receives a call from a surveyor escort (SE) alerting her to a potential problem. The SE told Mary that while the surveyor was in pre-op, medical records were reviewed for patients coming in for procedures later that day who had not yet arrived. The surveyor reviewed three medical records for patients, and saw documentation in one record that the immediate preanesthesia assessment was completed before the patient arrived in the area. The surveyor asked if this happens often and the OR staff said, "We never saw it before." Staff tried to Two New Publications! C&A has developed the CMS ESRD Compliance Forecaster & the CMS LTC Compliance Forecaster to assist your organization with its ongoing compliance with CMS CoPs and CfCs! These electronic workbooks are organized with individual worksheets for each ESRD CfC and LTC CoP, featuring columns organized by tag and requirements! Finally, healthcare organizations have a simple method for tracking compliance with all of the ESRD CfCs & LTC CoPs in one convenient electronic document. Get Yours Today! find the anethesiologist completing the documentation, but he was already in surgery with a patient. When the SE alerted Mary about this, thoughts of falsification loomed in her head. She had heard that documenting care before it occurs could be viewed as pre-charting the course of care or falsification, and might invoke an Accreditation Participation Rule (APR). Mary also knew that the leadership had taken a firm stance on this and that policies and procedures were in place for medical record documentation and to hold people accountable when performance was unacceptable. Mary quickly reviews the APR and learns that this could invoke an automatic decision rule for Preliminary Denial of Accreditation. Mary, realizing that this could end the survey, immediately calls the anesthesiologist of record to find out why the record was completed before the patient arrived. The anesthesiologist angrily explained that he had four surgeries back to back; he had reviewed the patient history and knew there would be no problem, so he filled in the paperwork. Big deal! He also reminded Mary that he had an excellent record with this hospital, and that she had no right to question him on this one incident. The anesthesiologist then threatened to call leadership to complain about Mary and the trouble she caused him. Now, Mary is in a quandary about how to address this issue with TJC and mitigate scoring this APR. Mary realizes that she needs to inform leadership about the potential of an adverse outcome and enlist their support in explaining what happened to TJC, but she is not sure how to go about it. Could the situation be avoided? How? Should Mary have called the anesthesiologist? What would you do? We want to hear from you… send us your thoughts and comments at [email protected]. We will share your insights in our next issue! Editor’s Note: “It Could Happen to You” scenarios are inspired by true stories, but are changed to sharpen the dilemmas involved in order to present a specific issue and evoke dialogue among our readers. The names of the characters, organizations and locations are fictional and are not to be confused with real people or places. Were You Aware? 1. The Centers for Medicare & Medicaid Services has released its Financial Report for FY2011. The report is quite detailed and contains over 35 pages related to CMS’ oversight of accreditation organizations. While C&A will incorporate key information into its future newsletters and educational offerings, here are several interesting highlights: a. TJC offers the most accreditation programs (6); AOA/HFAP offers 3; all other accrediting organizations offer 2 or less. Three accrediting organizations provided deemed status to hospitals in FY2010: TJC (3,841 facilities), AOA/HFAP (186 facilities); DNV (117 facilities). b. 85% of hospitals are “deemed” through accreditation by an accrediting organization with 15% “non-deemed” and surveyed by the State Agency for compliance with CMS COPs. c. CMS validates the work of accrediting organizations through two types of validation surveys – sample validation and focused or forcause surveys. Three percent (3%) of hospitals experienced a validation survey in FY2010. d. The hospital disparity rate (missed ConditionLevel findings) between accrediting organization findings and State Agency (surveying for CMS) findings continues. Here’s a snapshot: i. All Accrediting Organizations (FY2010): 1. Overall disparity = 38% 2. Physical Environment disparity = 31% 3. Health disparity = 17% ii. Overall Disparity Rate by Accrediting Organization (FY2008-2010): 1. AOA/HFAP = 80% 2. DNV = 43% 3. TJC = 34% e. After Physical Environment, the disparity has been found most frequently in the following COPs: Governing Body, Infection Control, Quality Assurance, Nursing Services, Food/Dietetic and Surgical Services. 2. Practitioners granted initial or new clinical privileges must undergo focused professional practice evaluation (FPPE) at that hospital to assure competency. Additionally, any triggered evaluation (issue-based) FPPE must also be performed at the organization. This assures that FPPE is conducted within the physical environment, using the equipment and resources available, where care is to be provided. Some organizations have sought to use evaluation data from other hospitals to meet this requirement. That would not meet the intent of this standard. 3. Hospitals, especially those within larger healthcare systems, are encouraged to review any affiliated ambulatory settings, physician practices, etc. that either fall under the hospital’s accreditation application or might be perceived as belonging to the hospital. These affiliated entities are not always involved in ongoing accreditation readiness and survey preparation activities and often do not meet requirements. Begin by assuring that related entities do, indeed, meet TJC’s criteria for inclusion in survey (see the Organizational & Functional Integration Criteria in the Accreditation Process chapter of the TJC manual). Once inclusion in the survey process has been confirmed, consider the following: a. Are clinical and administrative activities integrated with the hospital – i.e., are policies and procedures consistently implemented? b. Are applicable credentialing and privileging processes implemented? c. Have staff been oriented and trained for their specific roles and care setting? Are competencies assessed? d. Are any contracted services defined, performance expectations identified and evaluations conducted? e. Do key planning activities, i.e., emergency management, environment of care, infection prevention and control, involve the ambulatory and/or offsite locations? Were You Aware 2012 Recap Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions In the News! Congratulations to Senior Consultant, Nancy McLean, RN, BSN, MSHA, NHA, who was selected to speak at the North Texas Association for Healthcare Quality's 2012 Annual Conference! Ms. McLean spoke on "Quality as Defined by Regulations & Standards" which provided insights necessary to become more knowledgeable in the role quality plays in healthcare. In the News! Congratulations to Senior Consultant, Sharon Dills, MSN, RN, HACP, who was selected to speak at the Maryland Health Information Management Association's 2012 Annual Meeting! Testimonials About C&A C&A E-Newsletter Contact May 7, 2012 Conclusion: It Could Happen To You... "The Case of the Care Before the Patient" Was Mary Right or Over-Reacting? about it. As you may remember from last month's edition of C&A e-News, we left Mary in a quandary about how to address this issue with TJC and mitigate scoring this APR. Mary realized that she needed to inform leadership about the potential of an adverse outcome during their TJC survey and enlist their support in explaining what happened to their surveyors, but she is not sure how to go We asked for your thoughts and insights on how you would address this situation and those responses came pouring in! Thanks to everyone who responded! Great job! Here are just a few thoughts from our readers: “In this situation I’d have the anesthesiologist review the preanesthesia assessment at the arrival for pre-op and document another note. I think it was appropriate to speak with the anesthesiologist” – Sue “In our organization, I would have been able to discuss it with our VP of Risk Management and Accreditation and he would inform our Chief Medical Officer and/or the CEO. I would have asked one of them to speak with the Anesthesiologist” – Jennifer Ms. Dills spoke on "TJC & CMS Requirements and the Electronic Health Record" which provided insights into how the electronic health record can assist with regulatory compliance. See You in Philly! We are excited to host our 2012 Annual Conference "Developing a Culture of Change: A Picture of Compliance" in Philadelphia, May 16-17th! Keynote Speaker, Ann Scott Blouin, Executive Vice President for the Division of Accreditation and Certification Operations at The Joint Commission will be speaking on "Developing a Culture of Continuous Improvement Toward High Reliability". We look forward to seeing everyone there! “This situation can be avoided by having “hard stops” in place for patient safety.” – Julie “In my opinion, the situation should be faced head-on at all levels.” – Judy “I think speaking with anesthesia was not the best solution due to the high stress of dealing with the surgical cases at the time and not really having a plan of action due to not discussing the issue with leadership first. “ - Susan “The situation could possibly have been avoided if the present leadership had refreshed the medical staff and reviewed the policies all ready in place prior to the survey.” – Tanna In Conclusion: In the end Mary and her leadership team were able to persuade The Joint Commission survey team that this was not an acceptable practice in the organization, that policies and procedures existed to guide medical record documentation, that the Chief of Anesthesia had already counseled the anesthesiologist, and explained that focused professional practice evaluation procedures were instituted to monitor this provider’s pre-anesthesia assessment documentation for the next two weeks to assure appropriate documentation. Mary and the executive team were able to convey that the leadership had the right structures in place to guide practice, hold people accountable, and that the organization takes action when individuals do not follow those guidelines. The Joint Commission surveyor scored this under LD.04.01.05, EP 4 (staff are held accountable), rather than under APR.01.02.01, which addresses issues of inaccurate information or falsification, and could have resulted in a preliminary denial of accreditation. References The Joint Commission Comprehensive Accreditation Manual for Hospitals, 2012: LD.04.01.05: The hospital effectively manages its programs, services, sites, or departments. EP4: Staff are held accountable for their responsibilities. APR.01.02.01: The hospital provides accurate information throughout the accreditation process. EP1: The hospital provides accurate information throughout the accreditation process. (See also APR.01.01.01, EP 1) Note 1: Information may be received in the following ways: Provided verbally Obtained through direct observation by, or in an interview or any other type of communication with, a Joint Commission employee Derived from documents supplied by the hospital to The Joint Commission Submitted electronically by the hospital through a performance measurement system to The Joint Commission Note 2: For the purpose of this requirement, falsification is defined as the fabrication, in whole or in part, of any information provided by an applicant or accredited organization to The Joint Commission. This includes redrafting, reformatting, or deleting document content. However, the organization may submit supporting material that explains the original information submitted to The Joint Commission. These additional materials must be properly identified, dated, and accompanied by the original documents. Look at a future edition of C&A e-News for our Next Case Study: “Is it Clutter or Not? That is the Question!” Developing "Care Plans" That Guide Patient Care & Meet the Standards & Regulations By: Nancy McLean, RN, BSN, MSHA, NHA, HACP Both The Joint Commission and the Centers for Medicare and Medicaid Services (CMS) require that organizations develop patient care plans to meet the assessed need of the patient. CMS specifically requires that there be "nursing care plans" that guide patient care from the nursing perspective and "rehabilitation care plans" that guide all rehabilitation disciplines in providing care and treatment. There are also separate, specific requirements for pain, restraints and/or seclusion and discharge planning. Regardless of the discipline developing or contributing to the care plan, or the topic of the care plan, all care plans are divided into four distinct parts: Measurable patient goals Timeframe for achieving goals Interventions planned to assist in goal achievement Evaluation of progress toward goals Review of current electronic health record (EHR) designs often demonstrate confusion between patient-specific measurable goals and staff-specific interventions used to assist in meeting the goals. Distinguishing between the two is easy if the person completing the care plan asks the question, “Is this what a staff member would do to assist the patient?” If the answer to the question is, “Yes,” then it is an intervention and not a patientcentered goal. It is also recommended that in developing goals, the goal statement begins with, “The patient will…” This statement clearly marks this as a patient-specific goal. When selecting from a computerized menu of applicable care plan actions, these words are often not included. A simple mental check of mentally saying, “The patient will,” before an action on the menu will assist in distinguishing goals from staff interventions. Remember that the patient’s goals must be measurable within defined timeframes. This requires selecting a timeframe. Not all goals are for the length of stay. An example of this would be in the case of a patient admitted with severe pain from a fractured hip but scheduled for ORIF. A goal of, “The patient’s pain will be controlled prior to surgery with intravenous pain medication” might be documented. Both TJC and CMS require reassessment of the patient’s needs if the condition changes and updating the care plan based on the reassessed needs. Reassessment of this patient’s pain after the procedure would be appropriate. The reassessment should include whether the pain goal should be extended or if a change to oral analgesics would be more appropriate. If you are in the process of designing an EHR or have the ability to revise the EHR consider grouping patient goals separately from staff interventions. Finally, consider the requirement to “evaluate progress toward goals.” Can you create a pop-up of patient-specific goals every time the notes are accessed as a reminder to address patient progress or can the software automatically transfer goals to a table that triggers a required assessment, (similar to how most systems input information on restraints). Remember that both CMS and TJC have basically the same requirements and consider the care plan an vital tool in managing the patient’s care and a important part of the medical record. Were You Aware? 1. Over the last several months, CMS has published some updates to the Interpretive Guidelines for hospitals. Those (and all) Survey & Certification Memos can be found on the Policies & Memos to State Regions page on CMS’ website. Highlights of updates published in the last few months include: A. Medication Administration (482.23(c) and (c)(1); S&C-12-05-Hospital Memo dated 11/18/11) i. Timing of Medication Administration a. Removed reference to “30-minute rule” b. Hospitals must establish policies re: timing of medication administration and address specific circumstances outlined in the CMS memorandum c. Evaluation of medication administration timing policies ii. Standing Orders – Defining policy re: S&C memo 10/24/2008 a. Policies must address use of standing orders involving medication administration and include the process for development, approval, monitoring, initiation, authentication, etc. of standing orders b. Patient-specific orders must be initiated by an LIP c. Specific criteria for initiation of standing orders d. i.e., Specific clinical situation – Rapid response scenario e. Must assure professional staff are practicing within scope of practice B. Hospital Equipment Maintenance Requirements (482.41(c)(2) – S&C-12-07-Hospitals dated 12/2/2011) i. Allows alternate equipment maintenance schedules in certain circumstances a. Must be based on maintenance strategies and an evidence-based assessment process b. Cannot be adjusted for equipment critical to patient health & safety (i.e., life support, resuscitation equipment) c. Maintenance methods cannot be adjusted C. Life Safety Code – Waiver Instructions (S&C-1221-LSC, dated 3/9/2012) i. Allows hospitals & nursing homes to request waivers (without need to demonstrate ii. undue hardship) to allow them to use the 2012 LSC (rather than 2000) related only to: a. LSC 18/19.2.3 – Means of Egress – Wheeled equipment & fixed furniture b. LSC 18/19.3.2.5 – Cooking Facilities – Allow certain alternative type of kitchen cooking requirements c. LSC 18/19.5.2 – HVAC – Allow direct vent gas fireplaces in patient sleeping rooms; solid fuel burning fireplaces in other areas d. LSC 18/19.7.5 – Furnishings, Mattresses, Decorations – Allow combustible decorations on walls, doors, ceilings C&A Note: We have not yet seen how this process will be handled/determined by CMS, State Agencies & TJC. More to come! D. Requirements for Orders for Outpatient Services (482.56(b), 482.57(b) – S&C-12-17-Hospitals dated February 17, 2012) i. Rehab, Respiratory (& other) Outpatient Orders ii. Does NOT require the physician to be credentialed or privileged by the hospital iii. DOES require that the ordering practitioner: iv. Be responsible for the care of the patient v. Be licensed in state/jurisdiction where he/she sees the patient vi. Is practicing within scope of license vii. DOES require board-approved policy E. Patient Privacy & Medical Record Confidentiality (482.13(c)(1), 482.13(d)(1), 482.24(b)(3) – S&C12-18-Hospitals dated 3/2/2012) i. Consistent with HIPAA requirements to limit incidental uses & disclosures, i.e., using dividers and space where confidential information is discussed, limiting access to areas where white boards display patient information, etc. ii. Also addresses access to, and release of, medical records 2. TJC is now provides a mobile (via smartphone) notification of onsite survey activity! Organization contacts can sign up via their TJC Extranet site. Were You Aware Recap Tracer Workshop: Procedural Areas A Focus on Consent, Sterilization and Anesthesia You already know that TJC surveyors focus on procedural areas and operating rooms so they may make multiple visits to these areas – prepare your staff and physicians. You probably also know that surveyors must visit 100% of anesthetizing areas. Let’s face it, there are so many interesting items to survey – anesthesia, infection control, medication administration and safety, sterilization, staff competency, humidity, vendors, documentation, well the list just never ends. And, we can’t forget site marking and time outs. Even though these items have been required for years, organizations continue to struggle with ongoing compliance in many or all of these areas and the RFIs come easy. Many times staff don’t feel comfortable or well informed about what to look for in these areas. Join us on June 18th for our webinar on tracing in procedural areas. This presentation will provide a tracer example and give staff tips on how to survey for compliance. Contact us at (704) 573-4535 or [email protected] for more information! Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions Publication Spotlight C&A's Score Ongoing Accreditation ReadinessSOAR to Success, Electronic Workbook has been updated with the new 2012 Joint Commission Standards! This valuable tool can help you quickly and easily find the standards and scoring information you need. It puts the latest accreditation requirements, policies and procedures at your fingertips and includes scoring information at every element of performance. The SOAR to Success Electronic Workbook also comes in the following editions: Testimonials C&A E-Newsletter About C&A Contact June 28, 2012 It Could Happen To You... C&A is excited to present "It Could Happen to You," hypothetical case studies for you to solve. These are scenarios that could happen during your next survey, during the postsurvey process, or any average day. We have dramatized a situation to seek your reaction and input. So, take a moment, review the case, and provide us with your opinion on the scenario, because it could happen to you! We want to hear from you! Send us your thoughts and comments at [email protected]. We will share your insights in our next issue! "Is It Clutter or Not?" That is the Question! The Life Safety Surveyor was conducting the building tour on 4 West. As they walked through the patient care unit, he observed 4 isolation carts, an emergency cart, 3 linen hampers, 6 computers on wheels, a housekeeping cart, 2 beds, 2 bedside tables, three chairs, and two carts full of traction supplies. Tim, the manager on 4 West, was shocked to see the surveyor and Armand, the Safety Officer, walk on the unit. The surveyor took one look at the corridor and started writing something down. Armand started scowling as he looked around the unit. He thought Tim knew that you couldn’t store this stuff in the corridor and now it was too late to fix it. The surveyor said, “Let’s go to 3 West.” And, they left the unit without further explanation. Hospital, Critical Access Hospital, Behavioral Health, Ambulatory, Long Term Care and Home Care. Click Here to Order Now! There's Still Time! There's still time to register for the "Building a Successful Performance Improvement & Patient Safety Program" webinar on July 23rd! You won’t want to miss out on this valuable education session that shows it's more than a plan on paper! Contact Us Today! (704) 573-4535 [email protected] After the surveyor left, Tim called Gina, the survey coordinator and said, “I think we’re in trouble. The surveyor was just here, saw lots of stuff in my corridor and started writing it all down. He never asked for an explanation and now they are on the way to 3 West.” Gina starts to sweat. She knows that not only could this be scored as corridor clutter, but she has also heard whispering about life safety issues being scored as an immediate threat to life. What should Gina do? Should this be scored as clutter or immediate threat to life? Can this be avoided? Corridor Clutter Revisited... Again! By: Marty Piepoli, MSW, LISW/CP, HACP Most organizations, especially those built before the turn of the last century, have had multiple challenges with storage and assuring clear and unobstructed access through corridors to exits. Over the past several years, Maintaining the Means of Egress (LS.02.01.20, EP13), has been scored in the Top 10 of annual TJC findings. Challenged with the task of maintaining fire safety each day, organizations have employed Environment of Care rounding teams, focused strategies during fire drills for clear corridor access, determined how to use dead-end corridors and constructed storage alcoves in order to comply with Means of Egress expectations. CMS and TJC currently recognize Life Safety Code (LSC) 101, 2000 edition. Sections 19.2.3 & 7.3 address the Means of Egress. Since 2004, CMS has provided several Survey & Certification Letters (S & C) in order to address exceptions to the LSC specifically related to corridor clutter. CMS issued S&C LSC-10-18 in May, 2010 (excerpt below) revising guidance on what could be permitted in corridors: Allowance for wall mounted computers and other items to be wall-mounted in corridors as long as they do not project out more than 6 inches from the corridor wall or conflict with other sections of the Life Safety Code; projections shall not exceed a length of 36 inches, shall be separated by at least 48 inches from other projections, shall be installed at least 40 inches or greater above the floor, and shall only be installed in corridors that are at least 6 feet in width. Projections shall be permitted on either side of the corridor. Placement of items associated with the use of these wall mounted pieces of equipment such as chairs, tables, cabinets, carts, etc. in the corridor, which would reduce corridor to less than the required width, are not permitted when not in use. An item is considered “not in use” if it is left unattended or is not moved for more than 30 minutes. In addition, corridor wall alteration to reduce the projection of a wall-mounted item is prohibited if it reduces the protective requirements of the wall. Items such as linen carts, medication carts, and janitorial equipment would not be included in these exclusions. Infection control supply cabinets outside of a specific room are allowed in the corridor while precautions are in force for that room. Crash carts are allowed in the corridor for quick access in an emergency. Despite the guidance, clutter continued to be an issue for hospitals and was addressed by the revised 2012 edition of LSC101 which has not yet been adopted by CMS. However, in order to provide some relief related to this ongoing challenge, CMS issued an S&C Letter 12-21 on March 9, 2012 providing Instructions Concerning Waivers of Specific Requirements of the 2012 Edition of the National Fire Protection Association (NFPA) 101, the Life Safety Code (LSC), in Health Care Facilities. This guidance addresses exceptions for both the nursing home and acute care hospital settings. CMS will consider a waiver to allow uses that meet the requirements found in the 2012 edition: LSC sections 18/19.2.3 Capacity of Means of Egress and more specifically the requirements at 18/19.2.3.4 which allow, under certain circumstances, projections into the means of egress corridor width for wheeled equipment and fixed furniture. CMS will consider a waiver to allow the use of the requirements found at LSC section 18/19.7.5 Furnishings, Mattresses, and Decorations including sections 18/19.7.5.6 which allow the installation of combustible decorations on walls, doors and ceilings. Previous guidance concerning “not in use” criteria found in S&C-10-18-LSC is still applicable. What does this mean for your organization today? In considering whether or not to apply for a waiver as outlined above, start with a review of the 2012 edition of the LSC101 to assess your organization’s ability to comply with the new exceptions noted related to egress, corridor storage and wall-coverings. Seek input from your Facilities Leadership, Architect, or Physical Engineer. Also, you may want to seek the guidance of your local Authority Having Jurisdiction (fire marshal) in determining the information needed for the waiver. Follow CMS guidelines for submitting a waiver to your CMS regional office. Also submit a Traditional Equivalency request to The Joint Commission detailing the request, the related LSC requirement and how the organization meets the expectations of that requirement. In conclusion, it is important to note that organizations cannot simply adopt these practices. Both CMS and TJC require formal submission, and subsequent approval, of a request to comply with these less restrictive corridor requirements. Sources: CMS S & C Letter 10-18-LSC issued May 14, 2010Revision of S&C-04-41 dated August 12, 2004, Corridor Width & Corridor Mounted Computer Touch Screens in Health Care Facilities CMS S & C Letter 12-21-LSC issued March 9, 2012Instructions Concerning Waivers of Specific Requirements of the 2012 Edition of the National Fire Protection Association (NFPA) 101, the Life Safety Code (LSC), in Health Care Facilities The Joint Commission Comprehensive Accreditation Manual for Hospitals, 2012 The Joint Commission Perspectives, June, 2012 LSC 101, 2000 edition, LSC101, 2012 edition Were You Aware? CMS has CMS has published revisions to the Conditions of Participation related to several key areas. These revisions were published in the Federal Register on May 16, 2012 and include: Governing Body – 482.12 – Allow multi-hospital systems to have one governing body Will allow one governing body to oversee multiple hospitals in a multi-hospital system. Added a requirement for a member, or members, of the hospital’s medical staff to be included on the governing body as a means of ensuring communication and coordination between a single governing body and the medicals staffs of individual hospitals in the system. Patient Rights – 482.13 – Revise report requirement for deaths that occur when patient is only in soft two-point soft wrist restraints Replacing the requirement that hospitals must report deaths that occur while a patient is only in soft, 2-point wrist restraints with a requirement that hospitals must enter specific information in the patient’s chart and maintain a log (or other system) of all such deaths. Log is internal to the hospital but must be made available to CMS upon request and must include patient’ name, DOB, DOD, name of attending or other LIP, medical record number and primary diagnosis. Medical Staff – 482.22 – Privileges can be granted to those not on the medical staff and clarification around language for privileging non-physician staff Broadened the concept of “medical staff” to allow for inclusion of other practitioners as eligible candidates for the medical staff with hospital privileges to practice in the hospital in accordance with State law. All practitioners will function under the rules of the medical staff. This change will clearly permit hospitals to allow other practitioners (e.g. APRNs, PAs, pharmacists) to perform all functions within their scope of practice. Requiring that the medical staff must examine the credentials of all eligible candidates (as defined by the governing body) and then make recommendations for privileges and medical staff membership to the governing body. Medical Staff – 482.22 – Including podiatrists in list of those permitted to assume medical staff leadership This change will allow podiatrists to assume a new leadership role within hospitals, if hospitals so choose. Nursing Services – 482.23 – Allow an integrated, interdisciplinary plan of care & provision for patient selfadministration of medications (with parameters) Will allow hospitals the option of having a stand-alone nursing care plan or a single interdisciplinary care plan that addresses nursing and other disciplines. Allow hospitals to have an optional program for patient(s)/support person(s) on self-administration of appropriate medications. The program must address the safe and accurate administration of specified medications; ensure a process for medication security; address self-administration training and supervision; and document medication self-administration. Nursing Services – 482.23 – Minor changes related to blood transfusions/IV Eliminated the requirement for non-physician personnel to have special training in administering blood transfusions & intravenous medications and have revised the requirement to clarify that those who administer blood transfusions and intravenous medications do so in accordance with State law and approved medical staff policies and procedures. Nursing Services – 482.23 – Broadening those from who RNs are permitted to act on drug/biological orders (i.e., APRNs, PAs, PharmDs) Allowing for drugs & biologicals to be prepared and administered on the orders of practitioners (other than a doctor), in accordance with hospital policy and State law, and have also allowed orders for drugs & biologicals to be documented and signed by practitioners (other than a doctor), in accordance with hospital policy and State law. Medical Record Services – 482.24 – Broadening permitted use of standing orders to include not only emergency response situations but also ED and Post-op and defining the parameters for development, approval and use, including criteria for initiation, standing orders and protocols Will allow hospitals the flexibility to use standing orders and have added a requirement for medical staff, nursing, and pharmacy to approve written and electronic standing orders, order sets, and protocols. Requires that orders & protocols must be based on nationally recognized and evidence-based guidelines and recommendations. Still does NOT allow nurse-initiated orders (except influenza & pneumococcal) without physician order. Medical Record Services – 482.24 – Removal of 48 hour timeframe for authentication and continued allowance for “another practitioner responsible for care” to sign off on verbal orders Eliminated the requirement for authentication of verbal orders within 48-hours and have deferred to applicable State law to establish authentication timeframes. Made permanent the previous temporary requirement that all orders, including verbal orders, must be dated, timed, and authenticated by either the ordering practitioner or another practitioner who is responsible for the care of the patient and who is authorized to write orders by hospital policy in accordance with State law. Infection Control Services – 482.42 – Removal of the need for a separate infection control log Eliminated the obsolete requirement for a hospital to maintain an infection control log. Hospitals are already required to monitor infections and do so through various surveillance methods including electronic systems. Outpatient Services – 482.54 – Removal of the requirement that one, singular individual have responsibility for all outpatient services, allowing more than one leader to have responsibility Removed the burdensome and outdated requirement for a single Director of Outpatient Services position that oversees all outpatient departments in a hospital. Hospitals already have separate directors for individual outpatient departments, so having a single overall Director position is duplicative and unnecessary. Transplant Center – 482.92 – Reducing unnecessary duplication of blood type verification processes Eliminated a duplicative requirement for an organ recovery team that is working for the transplant center to conduct a “blood type and other vital data verification” before organ recovery when the recipient is known. The verification will continue to be completed at two other times in the transplant process. The full detail of these revisions can be found at: http://www.gpo.gov/fdsys/pkg/FR-2012-0516/html/2012-11548.htm Were You Aware 2012 Recap Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions Congrats! Congratulations to Christine Candio, Chief Executive Officer at Inova Alexandria Hospital in Fairfax, VA, for receiving the 2012 Brava! Women Business Achievement Award by Washington SmartCEO magazine! Testimonials About C&A C&A E-Newsletter Contact July 30, 2012 Conclusion: It Could Happen To You... "Is It Clutter or Not?" That is the Question! As you may recall from last month's edition of C&A e-News, Gina, the survey coordinator, was concerned about a potential survey finding on 4 West. Tim, the unit manager, had seen the Life Safety surveyor taking notes about "clutter" he observed in the corridor. The LS surveyor was now on his way to 3 West. This award honors women business leaders who We asked for your thoughts on how Gina combine their should have handled this situation. Thank you for all your irrepressible responses, we appreciate the feedback! entrepreneurial spirit with a passion for giving back to Here are two responses that echo the thoughts of others: the community. Tamara contributed: There's Still Time! There's still time to register for the "How to Meet TJC's Accountability Measures" webinar on August 20th! “First, Gina should call 3 West immediately and have someone ensure hallways are clear before surveyor arrives. Second, Gina or Tim should have someone move unused items out of the corridors on 4W and possibly the surveyor will be back and notice it is gone according to the 30 minute rule. If at all possible, everything should be on one side of the corridor for safety. Isolation carts are permitted as long as in use next to patient room Emergency (crash carts) are permitted Linen hampers are best in the dirty utility rooms You won’t want to miss out on this valuable education session that focuses on how to build processes that support compliance in your organization! Contact Us Today! Computers should be in use, otherwise stored in an area not considered a corridor The housekeeping cart should be in use or kept in a “housekeeping closet” The 2 beds, 2 tables, 3 chairs and traction carts should not be in the hallway longer than 30 minutes, and should be moved to another location. Hopefully, they were sitting there waiting for transport.” And Judy shared: “First, Gina should notify 3 West immediately of impending surveyor entry & have them move anything that is blocking exits or that (704) 573-4535 cannot be justified as being in place for actual immediate use. In info@courtemanche- addition, a general confidential, urgent message to all department assocs.com managers should be issued to quick sweep their units for such issues and correct immediately. Publication Spotlight Next, manager on 4 West should write down items viewed in hall & start mental justification process for himself using TJC allowable guidelines. Some items can be explained but probably not all. This would be damage control. Should also find unit education records that cover TJC guidelines on hallway use & criteria for equipment C&A's Score placement in hallways, to show attempts to educate staff. Should Ongoing also find any environmental rounds on unit that support appropriate Accreditation hallway findings if available. This info should be presented during Readinessexit interview by Gina and/or unit manager on that day wrap up SOAR to Success, session or at least on exit interview, as a rebuttal. Finally, this unit should clean itself up as much as possible immediately and stay Electronic that way until survey conclusion, hoping that surveyor will Workbook has accidently pass thru there again! been updated with the new Finally, safety officer, unit manager and survey coordinator should 2012/2013 Joint be prepared for rebuttal comments when surveyor findings are Commission presented, in a non-confrontational manner but with the intent to Standards! try to explain the finding and support any validity to equipment This valuable tool can help you quickly and easily find the standards and scoring information you need. It puts the latest accreditation requirements, policies and procedures at your fingertips and includes scoring presence that might exist. A prayer service for leniency and understanding prior to discussion with the surveyor would be in order!” In Conclusion: Now was not the time to panic! Gina composed herself and quickly took control. She contacted the unit manager on 3 West and advised that the LS surveyor was on his way and that he had concerns about corridor clutter. The 3 West manager indicated sweeps had already been done, but she’d double check to be sure the corridor was in appropriate order! Gina then asked the survey Command Center to send an email to all information at every managers reminding them of the need to maintain means of egress and noting that the only items not in immediate use that are element of permitted to be in corridors are: isolation and chemotherapy carts performance. (when associated with patients) and emergency carts. Finally, yet all within a matter of two minutes, Gina called Tim and asked if he Click Here to needed assistance in locating appropriate storage places for the Order Now! equipment that had been on his unit. Setting Gina’s mind at ease, Tim advised that task was already well underway! The survey blitz team were sent on rounds to assure that corridors and stairwells were clear from obstructions and reported back to the Command Center that all areas looked to be in good shape! In the end, the Life Safety surveyor, having found no other concerns related to means of egress, scored a Requirement for Improvement (RFI) under LS.02.01.20, EP13. Included in the organization’s Evidence of Standards Compliance for this finding was development and implementation of a “Means of Egress” policy & education on the importance of maintaining clear corridors to assure safe, expeditious evacuation in the event of smoke or fire conditions. References: The Joint Commission Comprehensive Accreditation Manual for Hospitals, 2012 LS.02.01.20: The hospital maintains the integrity of the means of egress. o EP13: Exits, exit accesses and exit discharges are clear of obstructions or impediments to the public way, such as clutter (for example, equipment, carts, furniture), construction material, and snow and ice. (For full text and any exceptions, refer to NFPA 1012000: 7.1.10.1). Coaching Staff in a Healthcare Setting - Part 1 By: Nancy McLean, RN, BSN, MSHA, NHA, HACP Several years ago, the buzz words, "blame free," were suggested as a foundation for an organizational culture that would lead to improved patient safety and quality. However, there are times when blame free does not address the inappropriate behaviors we may be faced with, such as, theft, medication diversion, abuse, etc. We now recognize that a "just culture" is more appropriate. Just like the change from "blame free" to "just culture," healthcare organizations should consider a change from the approaches of disciplinary action, corrective action and disciplinary process to "coaching." Coaching supports the philosophy of a "just culture." Coaching implies "team". Hundreds of books and thousands of articles have been written on the concept of “team.” Teams require a coach or coaches. In the healthcare setting, work teams are rarely formalized and nurtured by the leadership of the organization. Informal teams often develop in healthcare based on work flow and work load without the guidance or support of a coach. These teams are often singledisciplinary though we continue to hear requirements that are dependent on multidisciplinary or interdisciplinary concepts. These teams are often short-lived – the staff come together to tackle a specific problem or situation and then return to their individual issues and priorities. There is no coach to assure the team stays together. Development of a team culture in healthcare starts with leadership support of a coaching philosophy. Leaders can begin the process by turning discipline into coaching. Coaching begins with identification of the coach and team members that will comprise the “team.” The team then jointly establishes the team goals. Two things bring a team together: a common enemy or common goals. When a common enemy is the foundation for team cohesiveness, the team is short lived. The team breaks apart when the enemy is defeated. When common goals are a foundation for a team, the team stays together to achieve goals and build new goals based on past achievements. The coach must assure: Team members know their positions on the team Team members know and understand the value of all positions Individual team members understand how their position contribute to the overall success of the team The team develops realistic measurable, common goals The team has the education, support and resources to help meet the goals The coach routinely provides the team with feedback on their progress toward meeting the agreed upon goals and celebrates with the team as they score each touchdown Healthcare organizations can lay the foundation for a team philosophy by: Establishing common goals that each employee understands their role in helping to achieve Developing a philosophy of coaching for achievement of the goals Coaching begins with jointly establishing and documenting performance goals, targets and deadlines with the employee. It proceeds with routine review of the progress toward goals and targets. It includes the exploration of reasons that goals are not being met and revised targets or deadlines, when necessary. It encourages acceptance or responsibility for the employees own performance. It assists the employee in self-reflection related to the right job and right organization for them. It replaces the disciplinary process, not so much as to the flow of the process, but as to the punitive sound and philosophy. Ultimately an organizational philosophy of coaching leads to employee commitment and dedication, reduced turnover, increased job satisfaction, and improved performance resulting in improvement in care and treatment provided and winning teams. Go team! Look for Coaching Part 2 in an upcoming edition of C&A e-News! Click here to learn more about coaching for regulatory success! References: Team climate, intention to leave and turnover among hospital employees: Prospective cohort study, 2007, Mika Kivimäki, Anna Vanhala, Jaana Pentti, Hannakaisa Länsisalmi, Marianna Virtanen, Marko Elovainio and Jussi Vahtera http://www.thomasgroup.com/eLibrary/IndustryInsights/Healthcare-and-Life-Sciences/NursingRetention.aspx Nursing Retention. © 2012 Thomas Group, Inc. All rights reserved Were You Aware? 1. Late Breaking News: On July 13th, the CDC published an article related to two recent outbreaks of staphylococcus aureus infections. Investigation revealed both outbreaks related to the use of single-dose vial (SDV) medications for more than one patient. These two outbreaks involved a total of ten patients who required treatment. Administering drugs from one SDV to multiple patients without adhering to USP 797 Compounding Sterile Preparations is NOT ACCEPTABLE. Both the CDC and CMS (see reference links below) require that organizations using SDVs for multiple patients adhere strictly to infection control practices and USP 797 Sterile Compounding Guidelines for repackaging and storage. Organizations must be aware of the following broad expectations: Single dose vials (SDVs) are intended for single use, and are labeled as such, because they typically lack antimicrobial preservatives The use of SDVs for multiple patients increases the risk of infection transmission SVDs that are repackaged under USP 797 Sterile Compounding Guidelines consistent with aseptic conditions and stored consistent with USP 797 and manufacturer guidelines is permissible USP 797 requires specific conditions, trained and qualified staff, ISO Class 5 conditions for air quality, ISO class 7 buffer zone, proper attire and controls Medications are repackaged properly Repackaged medications are labeled properly with correct name, concentration, volume, route, beyond use date and storage conditions For additional information on the safe use of SDVs: http://www.cms.gov/Medicare/Provider-EnrollmentandCertification/SurveyCertificationGenInfo/Downloads/S urvey-and-Cert-Letter-12-35.pdf http://www.cdc.gov/injectionsafety/cdcpositionsingleusevial.html 2. Summer is the time to unwind, refresh and get energized! It’s also time to be sure that your organization has implemented any changes promulgated by regulatory and accrediting organizations during the year and has a process in place to address upcoming changes. Some helpful hints for staying on top of all those changes: Frequently review TJC’s website (http://www.jointcommission.org) and “The Joint Commission Perspectives” for new and updated FAQs, pre-publication standards and proposed standards that are in field review. Some recent updates include: Updated (July) FAQs related to the Human Resources requirements for unlicensed persons serving as scribes and responsibilities for nonlicensed, non-employee individuals in the organization. Note that both of these FAQs are further clarifications of FAQs issued earlier this year. Revisions to the patient flow requirements to assure that organizations address potential safety issues related to boarding both medical and behavioral health patients awaiting placement. Revisions to emergency management exercise requirements for home care settings. A “loosening up” of the requirement for quality control checks for waived testing. Check the CMS website regularly for changes to the State Operations Manual, Appendix A (Interpretive Guidelines) and outlined in Survey & Certification Memoranda. See the May/June edition of C&A eNews for recent changes. For new or revised requirements that are effective in 612 months, establish work teams to assess current state, identify gaps related to new requirements, strategize solutions and create the plan and timeline for implementation. For example, for the patient flow requirements, consider a team comprised of ED, BH, Quality & Ancillary representatives. And, most importantly, don’t forget the medical staff! 3. Were you aware . . . that you can easily avoid a potential Situational Decision Rule and Accreditation with Follow-up Survey result with a simple policy update? LS.01.02.01, EP3 requires that organizations have a written Interim Life Safety Measure (ILSM) policy that addresses situations when the organization cannot immediately address Life Safety Code deficiencies – either due to construction, renovation or other factors. The policy must include criteria for evaluating the extent of ILSM to be implemented. Many organizations have policies that only address LSC deficiencies related to construction and/or do not contain evaluation criteria. Take a few moments to review your ILSM policy & make the necessary adjustments to the procedure and practice. Were You Aware Recap Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com Services Tools & Solutions Enjoy the Last Days of Summer! Testimonials C&A E-Newsletter About C&A Contact August 27, 2012 It Could Happen To You... C&A is excited to present "It Could Happen to You," hypothetical case studies for you to solve. These are scenarios that could happen during your next survey, during the postsurvey process or any average day. We have dramatized a situation to seek your reaction and input. So, take a moment, review the is month's cases and provide us with your opinion (a simple yes/no) on the scenario, because it could happen to you! There's Still Time! There's still a few spots left to register for the "TJC Update: The Latest on Executive Briefings" webinar on September 24th! You won't want to miss out on this valuable education session that focuses on the latest standards and survey process changes! Contact Us Today! (704) 573-4535 [email protected] We want to hear from you! Send us your thoughts and comments at [email protected]. We will share your insights in our next issue! "It's All in the Way You Label It" Scenario 1: It was 2:30 p.m. and Ronda, RN had prepped all medications and solutions for Mrs. Tructon’s hip surgery. Each was labeled with the medication name, the strength, quantity, dosage amount, and expiration time. The surgery proceeded and was going a bit longer than had been anticipated. It was time for Ronda to go to off duty. Betty, the nurse replacing Ronda, came into the room as the procedure continued. Ronda thanked Betty for relieving her, indicated that everything was in order and that “all the solutions are already out for you” and left the room. If a Joint Commission surveyor had observed this exchange, would there have been an RFI? Coming Soon! Be on the lookout for the launch of C&A's all new leadership series LEAD: Lead, Explore, Achieve, Develop! This essential leadership series uses your organizational concepts to provide the tools to get started while acquainting new, existing and soon to be leaders in their changing roles and responsibilities. More information coming soon! Scenario 2: Ms. Mercy was Ms. Mercy was in her room just before she was scheduled to go into surgery for a hip replacement. Mary, Ms. Mercy’s nurse, was preparing the antibiotic that Ms. Mercy was to receive before her procedure. Mary drew up the appropriate medication and did not label it as she was going directly to the patient’s bedside. Just then, Ms. Mercy’s family entered the room to wish the patient well. Giving them a moment of privacy, Mary left the room for just a moment, spoke to her colleague at the nurse’s station & returned to Ms. Mercy’s bedside to administer the medication. If a Joint Commission surveyor had been onsite would Mary have been scored? Remember to send us your thoughts and comments at [email protected]. We will share your insights in our next issue! The Latest on the EC & LS Front By: Marty Piepoli, LISW/CP, HACP "What's the current buzz" in the physical environment related to the day to day operations in your healthcare organization? Well, the 49th American Society for Healthcare Engineering (ASHE) Annual Conference, held in July, sought to discuss the current buzz in facilities management. With the largest attendance on record, the program's theme of "Dealing With and Managing Through Change" was very appropriate. Some of the many topics during the conference were designed to provide insight and education for the more than 11,000 members across the country representing 2,500 hospitals. Dialogue and discussion ranged from the approval of LSC 101, 2012 for future adoption by CMS, discussion around creating uniformed life safety codes via the International Codes Commission, educational how to’s for managing your departments more effectively, a TJC update, basics of the life safety code and “Why Hospitals Should Fly,” a great closing plenary session by John Nance, one of the founding members of the National Patient Safety Foundation (NPSF). With several topics of interest regarding the environment, I thought focusing on the key points made by The Joint Commission’s George Mills, Director, Department of Engineering, would be of special interest. The session began with disclosure of the top scoring Environment of Care and Life Safety standards that continue to be a concern for organization’s to manage. George was quick to point out that these findings have continued to find their way into the top 10 for several years. LS.02.01.20—56%: Maintaining egress o Emphasis on what is permitted in the corridors o Proper use of dead-end corridors that are <50 sg.ft. for stored items o Importance of “Suite Designations” on the organization’s life safety drawings o Using legends to denote fire and smoke barrier rated walls LS.02.01.10—52%: Building & fire protection features designed/maintained to minimize the effects of fire, smoke, and heat o Beware of EP’s 5 & 9 pertaining to latching and penetrations o Consider including the doors as part of a Building Maintenance Program to assist with ongoing surveillance of the facility LS.02.01.30—45%: Providing & maintaining building features to protect individuals from the hazards of fire and smoke o Of interest, how organizations define hazardous storage locations and corresponding aspects of proper smoke barrier protection EC.02.03.05—40%: Maintaining fire safety equipment & fire safety building features o Noted documentation as the number one reason for additional Life Safety Surveyor time o Discussed how vendors should be working with you to mitigate differences related to devices under NFPA72 and NFPA25 for fire alarm and sprinkler testing o Referenced LD.04.01.05 to demonstrate how accountability for oversight is demonstrated LS.02.01.35—31%: Providing & maintaining systems for extinguishing fires o Second consecutive year in the top 10 scoring standards with focus on the 18” storage rule o o Grease-producing cooking devices with extinguishing systems activating properly Bundles of cable lying on top of fire suppression risers, not attached to a bracket or through some type of easy-pass system Mills provided the formula for determining how many Life Safety Surveyor (LSS) days an organization would receive: two surveyor days for all organizations and more than two based on the combination of >1.5 million sq.ft. of patient care space and more than three buildings on the campus. Facilities managers should be sure to confer internally with accreditation leaders and the TJC Account Executive regarding LSS days. The LSS will focus intently on EC.02.03.05, EC.02.05.07 and EC.02.05.09 during the document review to assure compliance with feature of fire safety equipment, generator testing and medical gas testing. He added that the Life Safety Surveyors are part of the survey team for smaller hospitals and Critical Access hospitals and will conduct the EC and EM sessions for these settings and as directed by the Team Leader in other settings. Additional points of interest addressed during this session included the need for risk assessment to determine where you are place eye wash stations, emphasis on temperature and humidity in procedural and sterile areas citing the ASHRAE ventilation guidelines. George added that with the increased emphasis on infection control, surveyors are looking for chipped or bubbling paint and wall board as well as positivenegative pressure relationships. George also addressed the CMS S & C Letter of March 9, 2012 regarding application for a waiver to utilize certain aspects of the new Life Safety Code 101, 2012 edition. He addressed the five areas of the new code and noted that TJC will grant Traditional Equivalencies for these aspects of the new code. He did point out, however, that CMS approaches this reactively and that in all likelihood a facility would be cited at the CMS/State level and then use the waiver request as part of the plan of correction. The ASHE conference was jam-packed with information to provide facility managers with tools and strategies to manage an ever- changing healthcare environment. Facilities management integrates the need to clearly define the life cycle of a system and the return on investment for a project or new capital infrastructure expense. Both new and seasoned facility managers must be equipped with the knowledge and tools to not only manage the day to day operations, but implement sound financial approaches as well. Resources: o Presentations provided at 49th Annual Conference, American Society for Healthcare Engineering, July 1618, 2012 o The Joint Commission Comprehensive Accreditation Manual for Hospitals, 2012 o www.cms.gov Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com 12/ 5/ 12 C&A Newslet t er - Sept em ber Services Tools & Solutions Well Wishes! Please join us in sending well wishes to Lauren Hannan, Education & Client Relations Coordinator, as she pursues an exciting new career opportunity. We thank Lauren for her many contributions to the company over the last two years and wish her the best of luck in all future endeavors! If you have any questions regarding any educational concerns, please feel free to call us at 704-573-4535. Don't Miss Out on C&A's 2013 TJC & CMS Webinar Series! Register on or before December 7th to receive the early bird rate! The 2013 TJC & CMS Webinar series focuses on the ht t ps: / / ui. const ant cont act . com / visualedit or / visual_edit or _pr eview. jsp?agent . uid=1111101796629&f or m … Testimonials C&A E-Newsletter About C&A Contact September 27, 2012 Conclusion: It Could Happen To You... "It's All in the Way You Label It" As you may recall from last month's edition of C&A e-News, we had two scenarios which involved medication labeling. Our first scenario, opened with Ronda, an RN, preparing a patient's medications for surgery and was getting ready to leave her shift. In our second scenario Mary was getting ready to administer medications to a patient at their bedside. In each scenario we invited you to respond to our poll asking if a Joint Commission surveyor had been onsite would the scenario been scored. We appreciated the outstanding feedback to our poll. Check out the responses. They may surprise you.... Read More Coaching in a Healthcare Setting - Part 2 By: Nancy McLean, RN, BSN, MSHA, NHA, HACP In a prior article we discussed how a healthcare culture based on coaching and team concepts can lead improvement in care and treatment provided. These same concepts can apply to the organization's role in assuring physician competence. In 2009 the Joint Commission published the Medical Staff standards requiring the hospital to develop methods of evaluating physician practice in focused situations and on an ongoing basis. This formalized oversight of the Medical Staff member's 1/ 2 12/ 5/ 12 C&A Newslet t er - Sept em ber "how to" of regulatory and accreditation compliance while keeping you up to date on the latest accreditation and regulatory news, changing standards, and best practices for compliance throughout the year! Click Here to view the entire brochure complete with dates, topics & more information! individual performance was initially met with hesitation, with some organizations taking up to 18 months to implement the requirements. Three years later there is still confusion, hesitation and strong reaction from some Medical Staff members as to the degree of required performance monitoring and what is being monitored. Executive leaders are also mentioning the reaction of the physicians when presented with... Read More Were You Aware? Sentinel Event #49: Safe use of opioids in hospitals On August 8, 2012, TJC published Sentinel Event #49 regarding the use of opioids in hospitals. While many believe that the use and administration of opioids is safe in a hospital setting because of frequency of use and ongoing monitoring... Pain assessments and pain goals... are often not effective? Working with hospital organizations, we often have conversations (ok sometimes heated debates) related to the subject of pain. Typically, these conversations revolve around... Read More Courtemanche & Associates Charlotte, NC | Denville, NJ P: 704-573-4535 | F: 704-573-4538 [email protected] | www.courtemanche-assocs.com Forwa rd e m a il This email was sent to [email protected] by [email protected] | Update Profile/Email Address | Instant removal with SafeUnsubscribe™ | Privacy Policy. Courtemanche & Associates | PO Box 23659 | Charlotte | NC | 28227 ht t ps: / / ui. const ant cont act . com / visualedit or / visual_edit or _pr eview. jsp?agent . uid=1111101796629&f or m … 2/ 2 Andrea Marsh Courtemanche & Associates [[email protected]] on behalf of Courtemanche & Associates [[email protected]] Friday, November 30, 2012 10:53 AM [email protected] C&A Newsletter - November 2012 From: Sent: To: Subject: Services Tools & Solutions 2013 Annual Conference Testimonials C&A E-Newsletter About C&A Contact November 30, 2012 Registration Now Open! Conclusion: It Could Happen To You... April 30th - May 1st Chicago Renaissance Downtown, Chicago, IL C&A's most exciting conference to date! Stay up to date on all the latest trends in accreditation and regulatory compliance, in addition this conference will offer a real "hands on" approach providing you with tools that will help your organization stay compliant throughout the year. Click here to view the brochure or Call us (704) 573-4535 to find out how to register! ʺThe Right Patientʺ As you may recall from last month's edition of C&A e-News, we presented a case study which involved proper patient identification. Our scenario, opened with Ben, a six year old boy who was in the hospital awaiting his tonsillectomy. Jeremy the nurse had come into Ben's room to make final preparations for the surgery. Jeremy needed to confirm the patient's identity. For this scenario we invited you to respond to our poll asking if Jeremy had followed appropriate procedures to make sure that he indeed had the right patient. We appreciated the outstanding feedback to our poll. Check out the responses. They may surprise you... Read More Endoscopy Equipment Processing Room Requirements In April, 2012, EC News, distributed by Joint Commission Resources, addressed Endoscopy Equipment Processing Room 1 Early Bird Rates Ending Soon! There is still time to register for C&A's 2013 Webinar Series. This series not only keeps you current with the latest TJC/CMS trends, it also offers practical solutions for everyday regulatory compliance issues. Early Bird Rates end on Dec. 7th, so be sure to send in your registration details soon. Click Here to register and learn more! Requirements regarding air flow and negative pressure which provided guidelines for Gastrointestinal Endoscopy rooms. This same article referenced the 2010 Facilities Guidelines Institute (FGI) for design and construction of health care facilities, section 3.9 and The Joint Commission relevant standards. Although this article... Read More Were You Aware? - Lack of documentation leads to RFIs According to TJC survey results, 40% of all hospital surveys completed in 2011 and the first half of 2012 received an RFI in standard EC.02.03.05, which relates to documentation. This standard requires documentation for approximately 20 different tests of fire safety and alarm systems. One of the reasons for the high RFI rate is.... - ECRI Releases Top 10 Health Technology Hazards for 2013 It seems like almost every day there is some new technology being created or introduced to make healthcare work easier; however... Read More Irene, Sandy, Snowfall, Flooding, Power Loss, LEAD Lead, Explore, Achieve, Develop Create a culture of compliance every day by empowering your entire organization. This C&A Leadership training program is available to organizations in many different formats to best fit your style and budget. Click Here Are just a few of the issues that every healthcare organization considers in assuring that the Emergency Operations Plan (EOP) is up to date. With the recent devastating impact left by hurricane Sandy organizations are taking a very hard look at the structure of their EOP and are asking if the plan will really work. Now is a good time to review your current EOP plans. Join us on January 14th from 11:00am - 12:15pm, for C&A's first webinar for the 2013 series: "Emergency Management Planning, Drilling, Critiquing: Tips on Assuring a Manageable Yet Comprehensive Emergency Operations Plan." This important webinar will address aspects specific to an all-hazards approach to emergency management to assure that your organization doesn't have a paper product, but an EM Plan that actually works. Click Here to Register 2






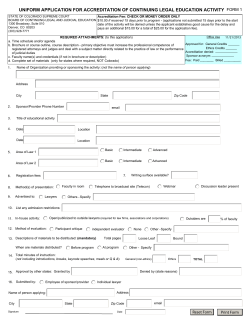



© Copyright 2026