
System Quality Review SPECIAL ISSUE
System Quality Review
SPECIAL ISSUE
PROCEEDINGS OF THE SYMPOSIUM
Innovative Differentiation: Distinguishing
Yourself From Other High Performers
November 9, 2012
Co-sponsored by:
Editorial Board
Steven J Corwin, MD
Chief Executive Officer
NewYork-Presbyterian Hospital and Healthcare System
Robert E Kelly, MD
Wayne M Osten
Eliot J Lazar, MD MBA
President
NewYork-Presbyterian Hospital
Kimlee Roldan-Sanchez, MPA
Arthur J Hedge, Jr.
Marcia Brinson, RD MPH
Trustee, NewYork-Presbyterian Hospital and Healthcare
System
Kathleen Ciccone, RN MBA
George F Heinrich, MD
Barry S Gallison, DNP MS APRN-BC NEA-
Chair, Performance Improvement Committee
NewYork-Presbyterian Healthcare System
Chairman, Board of Trustees, New York Hospital Queens
Trustee, NewYork-Presbyterian Healthcare System
BC CPHQ
Deborah Hollenberg, RN MSN
Marc L Boom, MD MBA FACHE
Patricia Keill, RN
President & Chief Executive Officer
The Methodist Hospital System (Houston, Texas)
I-Fong S Lehman, DrPH MS
Roberta L Schwartz
Lisa-Vanessa Magtibay, RN MS
Executive Vice President
The Methodist Hospital System (Houston, Texas)
Wazim Narain, MPH
H Dirk Sostman, MD FACR
Scott W Possley, PA-C MPAS
Executive Vice President, Chief Academic Officer & Chief
Medical Officer
The Methodist Hospital System (Houston, Texas)
President & Chief Executive Officer
The Methodist Hospital Physician Organization (Houston,
Texas)
Professor & Executive Vice Dean
Weill Medical College of Cornell University
Kenneth E Raske
President & Chief Executive Officer
Greater New York Hospital Association
Daniel Sisto
Lorraine M Ryan, Esq RN
Brian K Regan, PhD
Karen A Scott, MD
Angela M Skretta
Brian R Taylor, PhD
Alfred A Villacara, DMD
President & Chief Executive Officer
Healthcare Association of New York State
Acknowledgements
Kevin W Dahill
President & Chief Executive Officer
Northern Metropolitan Hospital Association (NorMet)
The editors of SQR gratefully acknowledge the assistance of
Inez Horton and Anna Malkin for their dedication,
organizational skills, and planning expertise.
Gratitude is expressed most especially to those practitioners
and performance improvement leaders who show their
commitment to quality patient care through their contribution
herein.
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
1. Healthcare Association of New York State (HANYS)
1
HANYS Report on Report Cards
Robert J Panzer, MD; Martha Radford, MD; Brian K Regan, PhD; Kathleen Ciccone, RN MBA;
Christa Christakis, MPP; Christina Miller-Foster, MPA; Mary Therriault, RN MSN
2. Hospital for Special Surgery
3
Implementation of a Bladder Bundle Program in an Orthopedic Specialty Hospital
Eileen A Finerty, MS RN FNP CIC; Helen Renck, MSN RN; Patricia Griffin, MS RN CPHQ; Mary
McDermott, MSN RN ANP NE-BC; Barry Brause, MD; Anne LoBasso, RN MBA
3. Hospital for Special Surgery
7
Implementing an Adult Vaccination Program in an Orthopedic Specialty Hospital
Eileen A Finerty, MS RN FNP CIC; Helen Renck, MSN RN; Patricia Griffin, MS RN CPHQ; Mary
McDermott, MSN RN ANP NE-BC; Barry Brause, MD; Andy Miller, MD
4. Hospital for Special Surgery
10
Perioperative Diabetes Management: HbA1c Screening
Linda Russell, MD; Raquel Mayne, MS MPH RN; Zahava Alter, MBA; Ann LoBasso, MBA RN;
Gregory Liguori, MD; Andrew Martorella, MD
5. Hospital for Special Surgery
13
Risk Factors for Returning to the PACU After Orthopedic Surgery
Michelle Mangini; Ting Jung Pan, MPH; Michael Urban, MD; Mayu Sasaki, MPH; Stephen Lyman,
PhD; Steven Magid, MD
6. Kings County Hospital Center
15
Reducing Restraints in the Inpatient Behavioral Health Setting
Joseph Merlino, MD MPA (Deputy Executive Director); Renuka Ananthamoorthy, MD (Chief of
Service); Jill Bowen, PhD (Sr. Associate Executive Director, Chief of Staff); Roumen Nikolov, MD
(Associate Chief of Service); Linda MSN NPP NEA-BC (Associate Executive Director, Nursing);
Chikodiri Gibson, RN (Sr. Associate Director Nursing); Lora Giacomoni, RN MSN (Sr. Associate
Director Quality & Compliance); Luther Summers Hamilton, MSW (Associate Director Performance
Improvement)
7. Kings County Hospital Center
20
Reducing the Use of 1:1 Observations
Joseph Merlino, MD MPA (Deputy Executive Director); Renuka Ananthamoorthy, MD (Chief of
Service); Jill Bowen, PhD (Sr. Associate Executive Director Chief of Staff); Roumen Nikolov, MD
(Associate Chief of Service); Linda MSN NPP NEA-BC (Associate Executive Director Nursing); Lora
Giacomoni, RN MSN (Sr. Associate Director Quality & Compliance); Luther Summers Hamilton, MSW
(Associate Director Performance Improvement); Akinola Adebesi, MD; Elise Feldman, PhD
8. Krasnoff Quality Management Institute - a Division of the North Shore-LIJ Health System
Use of Quality/Safety Data for Institutional Planning
Marcella De Geronimo, MS; Rosemarie Linton, MPH; Kevin D Masick, PhD
23
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
9. Lawrence Hospital Center
25
Reducing Patient Falls in the Inpatient Setting Through Innovation and Education.
Lisa Hanrahan, RN MSN CENP CPHQ CPHRM; Missy Paolicelli, RN OCN MSN; Majella
Venturanza, RN MA CCRN; Christine Demo, RN MSN TNCC; Michelle Pollack, RN CPHQ
10. Lawrence Hospital Center
28
Increasing Compliance with VTE assessments to Prevent Nosocomial DVT
Sharon Doyle-Hennessy, RN MS; Lorraine Bachman, RN
11. Lawrence Hospital Center
29
Eliminating Non-Medically Indicated Deliveries before 39 weeks Gestational Age
Lisa Hanrahan, RN MSN CPHQ CPHRM; Sharon Doyle-Hennessy, RN MS
12. Lawrence Hospital Center
32
Reducing Central Line Infections in the ICU - Challenges for the Community Hospital
Mary Ann Hauff, RN (Director of Infection Control); Barbara Choy, RN (Nurse Manager Critical
Care); Rose Ann O'Hare, RN (Vice President Patient Care Services)
13. Methodist West Houston Hospital
34
Reducing Utilization of Intravenous Hydromorphone at a New Community Hospital
Huong Le, PharmD BCPS; Echefula Agbara, PharmD RPh
14. Montefiore Medical Center
40
Evolution of Montefiore Medical Center Falls Prevention Program
Jane O’Rourke, RN DNP NEA-BC; Patty Zyloney, RN MSN; Lois Alfieri, RN MSN; Amisha Rai, PA;
Maryrose Defino, RN MS CPHQ; Mary Tesoro, RN-BC DNS; Maryanne Schmid, RN CPHQ; Erica
Schmidt; Jason Adelman, MD; Michael Bogaisky, MD
15. New York Downtown Hospital
44
The Impact of Dementia on Common DRG Hospitalizations in the United States: 2000-2010
William Liao; Suh H. Lee, BS; Robert Y Lin, MD
16. New York Hospital Queens
46
You Can Get There From Here: One Hospital's Continuing Meaningful Use Journey From Stage 1 to
Stage 2
Ken Ong, MD MPH; Phil Myones, MS; Cathy Suspenski, MPA; Teresa McCormack, MHS; Geeta
Natashi, RN MSA; Stephen Rimar, MD MBA; George F Heinrich, MD
17. New York Hospital Queens
50
Efforts to Improve Insufficient Clinician Documentation of Significant Electrocardiographic Findings in
Adults Presenting to the Emergency Department with Dysrhythmias and/or Conduction Disorders
Nidhi Garg, MD; Alison Suarez, MD; Zuhair Ali, MD; Sanjey Gupta, MD
18. New York Hospital Queens
ID Band Errors: A Serious Patient Safety Challenge
Laurie J Gordon, MA MD; Piyush Jain, MD
51
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
19. New York Methodist Hospital
54
Strategies for Reducing Preventable Readmissions for Patients with CHF Patients Discharged to Nursing
Homes
Kathleen Treacy, RN; Steven Silber, DO; Carol Farina, RN; John Heitner, MD; Emil Baccash, MD;
Snow Nguyen, MD
20. New York Methodist Hospital
57
Effects of Integrating Automated Safeguards to Promote Anticoagulation Safety and Efficiency
Erin Y Oh, BA PharmD BCPS; Nasser Saad, PharmD; Teena Abraham, MS PharmD BCPS; Righard
van Niekerk, BPharm; Eric Balmir, MS PharmD
21. New York Methodist Hospital
61
The Clinical Effects of Implementing a Point of Care Ultrasound Division; Data from the Pilot Project
Gerardo Chiricolo, MD; Tim Mooney, MD; Kevin O'Rourke, MD; Lawrence Melniker, MD; Joseph
Bove, MD; Steven Silber, DO
22. New York Methodist Hospital
63
Making the Honor Roll: Reducing Treatment Delays in Acute Stroke
Barbara J Gatton, MD; Matthew Dros; Lawrence Melniker, MD; Linda Fox; Miran Salgado, MD;
Jeffrey Benjamin, MD; Joseph Bove, MD; Steven Silber, DO
23. New York Methodist Hospital
66
Ocular Ultrasound Simulation Lab: Does It Translate to the Bedside?
Kevin O'Rourke, MD; Sharon Yellin, MD; Tim Mooney, MD; Lawrence Melniker, MD; Joseph Bove,
MD; Steven Silber, DO; Gerardo Chiricolo, MD
24. New York Methodist Hospital
68
The Impact of a Protocol Based on Estimated Glomerular Filtration on Dose of Iodinated Contrast
Administered and Image Quality
Joseph Samide, PharmD; Nasser Saad, PharmD; Teena Abraham, MS PharmD; Eric Balmir, MS
PharmD; Claudia Lapidus, MD; Steven Garner, MD; Anthony Mungo, BSRT
25. New York Methodist Hospital
71
The Use of Automated Weight-Based Dosing to Prevent Medication Errors in the Pediatric Emergency
Department
Righard van Niekerk, BPharm; Christopher Kelly, MD; Pramod Narula, MD; Kathleen Treacy, RNVP;
Anna Boyko, PharmD; May Jabra, PharmD; Gary Wu, PharmD; Laura Melville, MD
26. NewYork-Presbyterian Hospital
The Development of a Nursing Quality and Patient Safety Fellowship
Barry S Gallison, DNP MS APRN-BC NEA-BC CPHQ; Judith A Rizzo, PhD RN NEA-BC CPHQ;
Peggy Quinn, MPH RN
74
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
27. NewYork-Presbyterian Hospital
75
Putting the Pressure on Reducing Hospital Acquired Pressure Ulcers
Debra O'Hehir, MSN MBA RN (1); Tochi N Okorie, MBA RN (2); Lourdes Mellino, MA MEd RN NEABC (1); Mary E Quinn, MSN RN (2); Barry S Gallison, DNP MS APRN-BC NEA-BC CPHQ (1)
(1) Nursing, NewYork-Presbyterian Hospital
(2) Division of Quality & Patient Safety, NewYork-Presbyterian Hospital
28. NewYork-Presbyterian Hospital
77
Multi-Disciplinary Bedside Rounds: Improving Communication and Teamwork to Enhance Patient
Engagement and Discharge Planning
Amy Silverstein, MPH; Daniel Sorbello, MPA NEA-BC RN; Ansa Rajan, MSN RN; Jean Flynn, RN
EdD; Patricia Prufeta, MS NEA-BC RN
29. NewYork-Presbyterian Hospital
80
Early Mobilization in the ICU
Katherine Pavlovich, MPH; Suzanne Boyle, RN DNSc; Daniel Brodie, MD; Ernesto Perez-Mir, MSN
RN CCRN; Patricia Rychcik, MSN RN
30. NewYork-Presbyterian Hospital
83
Hand Offs to Skilled Nursing Facilities
Karen A Scott, MD; Eliot J Lazar, MD; Brian K Regan, PhD; Michael J Fosina; Christine AgirDonelly, RN; Margaret McGregor, RN; Ellen Cotter, RN; Donna Tingling-Solages, RN; Denise
Robinson, RN; Alan Levin, RN; Germaine Nelson, RN; Vepuka E Kauari, RN; Audrey Compton, MD;
Eileen Kornfeld, MSW; Paula Roberts, MSW
31. NewYork-Presbyterian Hospital
85
Health Information Technology Supported Improvement of Immunization Rates Across a Multi-Site
Academic Medical Center
Jamie R MacDonald, RN MSN MBA; Karen A Scott, MD MPH; Patricia Prufeta, RN; Peggy Liu, RN
MS; Robert Green, MD; Philip Graham, MD MSC; Eliot J Lazar, MD MBA
32. NewYork-Presbyterian Hospital
89
Correlation of Hand Sanitizer Placement with Good Hand Hygiene Compliance
Samantha Brenner, MD MPH; Samuel Sultan, MD; Susan Faggiani, RN BA CPHQ; David Calfee, MD
MS; Peter Fleischut, MD; Eliot Lazar, MD MBA; Gregory Kerr, MD MBA
33. NewYork-Presbyterian Hospital - Simulation Center
90
Full Scale Multidisciplinary In-Situ Simulation Prior to Opening a New Pediatric Emergency Department
David Kessler, MD; Melissa Cappaert, MA; Christopher Walker, RN; Carolyn Kyne, RN; Daniel Tsze,
MD; William Middlesworth, MD; Meredith Sonnet, MD; Dennis Fowler, MD MPH
34. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
92
An Action-Oriented Patient Safety Conference Model for the New Millennium
Laura Fanucchi, MD MPH; Joseph T Cooke, MD; Eugenia Siegler, MD; Lia Logio, MD
35. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Laboratory Cost Savings Associated with Prospective Review of Physician Orders
Doris O Samide; Jennifer F Zepf, DO; Stephen G Jenkins, PhD; Audrey N Schuetz, MD MPH
94
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
36. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
95
Optimizing Alpha-Numeric Paging on a General Medicine Floor
Parag Goyal, MD; Jennifer Lee, MD; Marianne Moore, MS RN PMHNP-BC; Lia Logio, MD
37. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
98
Designing and Implementing a Comprehensive Protocol for ED Identification and Management of
Agitated Delirium in Older Adults
Tony Rosen MD MPH; Scott Connors BS; Alexis Halpern MD; Michael E Stern MD; Sunday Clark,
MPH ScD; Mark S Lachs, MD MPH; Neal Flomenbaum, MD
(1) Department of Medicine, New York-Presbyterian Hospital/ Weill Cornell Medical College; (2)
Division of Medical Nursing, New York-Presbyterian Hospital
38. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
100
Multidisciplinary Approach to Developing a Protocol for Safe OR Management of a Patient with a
History of Sulfite Anaphylaxis
Ansara Vaz, BA; Antigone C Grasso, MBA; Nicholas Cavalieri; Beryl C Muniz, RN MAS; Laura
Maglione, RN MA CCRN; Alissa Ritter, RD CNSC CDN; Louise Merriman, MS RD CDN; Lai Chin,
RPh; Rafique Khaled; Vinod Malhotra, MD; Peter M Fleischut, MD
39. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Department of Medicine
102
A Multidisciplinary Educational Initiative Encouraging Prescription of Generic Over Brand-Name Proton
Pump Inhibitors (PPIs) at the Time of Hospital Discharge
Karl B Bezak, MD (1); Tara F Bishop, MD MPH (1); Jennifer I Lee, MD (1); Natalie Mohammed, BSN
RNC MA CLNC (2); Lia Logio, MD (1)
(1) Department of Medicine, NewYork-Presbyterian Hospital/ Weill Cornell Medical College; (2)
Division of Medical Nursing, NewYork-Presbyterian Hospital
40. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Department of Medicine
106
Improving the Rate of Resident Review of Routine Daily Electrocardiograms Ordered on Hospitalized
Patients
Adrian Mei, MD; Jennifer I Lee, MD; Cathy Collins, MS RN CCRN; Lia Logio, MD
41. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Division of Geriatrics
109
A Pharmacist-Led Intervention on Medication Education for Heart Failure Patients at Hospital Discharge
Sharda D Ramsaroop, MD; Olga Hilas, BS Phm PharmD; Eugenia L Siegler, MD; M Carrington
Reid, MD PhD
42. NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Weill Cornell Internal Medicine
Associates
111
Apple iPads Positively Impact Clinical Care in a Busy Outpatient Resident Practice
Karl B Bezak, MD; Amanda Carmel, MD
43. NewYork-Presbyterian Hospital/ Westchester Payne Whitney
Interactive Patient Safety Group to Prevent Falls in a Geriatric Psychiatry Unit
Danielle Struble-Fitzsimmons, PT DPT; Kaitlyn Giordano, MS; Elizabeth DiPersia, RN MS
113
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
44. Northern Westchester Hospital
114
Utilization of Electronic Medical Record Data to Re-Engineer Work Flow, Increase Departmental
Efficiency, Capacity and Increase Patient Safety
Elizabeth Coughlin BSN MPA CIC (Director of Infection Control); F Cole Caulfield III EMT (Quality
Management Infection Control Associate); Maryanne Carollo, BS RN CAPA (Patient Care Standards)
45. Northern Westchester Hospital
117
Improving Performance in Appropriate Administration of Perioperative Beta Blockers
Marla Koroly, MD; Kate O'Keefe, RN MSN FNP; Melissa Hershfield, RNC
46. Northern Westchester Hospital
119
Implementation of a Bar-Coded Label System for the Management of Expressed Breast Milk, Neonatal
Services
Anna Lane, BSN RN-C (Staff Nurse-NICU Level IV); Diwata Delarosa, BSN RN-CD; R Mendoza (Staff
Nurse-NICU Level IV); R Perez, RPh (Pharmacist); R Rosenberg, BS MS (Clinical Information
Specialist)
47. Northern Westchester Hospital
121
A Patient Food Service Program Called "Food is Care" Focused on Quality, Education and Service,
Featuring Freshly Prepared, Healthy Meals, Delivered When Patients Want, with Real-Time Nutrition
Education
Maria Hale, MBA
48. Northern Westchester Hospital
124
Improving Blood Culture Contamination Rates in a Community Hospital
S Laduca, RN (Emergency Department); B Wilson (Director Laboratory)
49. Northern Westchester Hospital
126
The Sustained Impact of a Process to Reduce Blood Culture Contamination Rates in a Community
Hospital
D Lajoie, RN MSN PhD(c) (Asst. Director of Research, EBP & Special Projects); Betty Wilson
(Directory Laboratory Services); Mike Zerbo, RN (Emergency Department); K Lawton, RN BSN
(Director Emergency Department)
50. Nyack Hospital
129
Pharmacodynamic (PD) Profiling of Ceftriaxone 1g and 2g daily in Critically Ill Septic Patients with
Normal Renal Function to Severe Renal Impairment
Andras Farkas, PharmD; Rachel Sussman, PharmD
51. Nyack Hospital
130
Dosing of Daptomycin in the Morbidly Obese: Which Body Weight is It?
Andras Farkas, PharmD
52. Nyack Hospital
Pharmacodynamic Profiling of Prolonged Infusion of Ertapenem in Critically Ill Patients with Early Onset
Ventilator Associated Pneumonia Using Monte Carlo Simulation
Andras Farkas, PharmD
131
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
53. Nyack Hospital
132
Pharmacodynamic Profiling of Ertapenem in Critically Ill Patients with Early Onset Ventilator Associated
Pneumonia with Normal Renal Function to Moderate Renal Impairment
Andras Farkas, PharmD
54. Nyack Hospital
133
Dosing of Telavancin in the Obese: Is It the Ideal, Lean, Fat Free or Adjusted Body Weight?
Andras Farkas, PharmD
55. Nyack Hospital
134
Evaluation of Pharmacist Managed Vancomycin Therapy Compared to Physician Managed Dosing in
Establishing Timely and Therapeutic Vancomycin Serum Concentrations at a Community Hospital
Rachel Sussman, PharmD; Andras Farkas, PharmD
56. Nyack Hospital
135
Door to Floor in 4 Hours
Christine Genovesi, RN; Dawn Sugrue, RN; Sachin J Shah, MD MBA; Eric Bachenheimer, MHSA MBA
57. NYU Hospital for Joint Diseases
136
Using Near Miss Analysis to Prevent Wrong-Site Surgery
Joseph Bosco, MD; Lorraine Hutzler, BA; Richard Yoon, MD; Michael Alaia, MD
58. NYU Hospital for Joint Diseases
137
Hospital Acquired Conditions After Orthopedic Surgery Do Not Affect Patient Satisfaction Scores
Michael S Day, MD MPhil; Lorraine H Hutzler, BA; Raj Karia, MPH; Kella Vangsness, BS; Nina
Setia, MS; Marta Cieslak, MPH; Ellen Brophy, BA; Joseph A Bosco, MD
59. NYU Hospital for Joint Diseases
140
Risk Factors for Readmission Following Inpatient Orthopedic Surgery: A Review of 13,663 Cases
Tracey Hunter, BA*; Philip Band, PhD*; Victoria Liublinska, PhD**; Raj Karia, MPH*; Lorraine
Hutzler, BA*; James Slover, MD*; Joseph Bosco, MD* (* NYU Hospital for Joint Diseases; **
Harvard University)
60. NYU Hospital for Joint Diseases
141
Physician-Specific Correlation Between Discharge Disposition Cost, Readmission and Length of Stay
(LOS) Following Total Hip and Knee Replacement: An Analysis of 1,777 Cases
Lorraine Hutzler, BA; Joseph Bosco, MD; James Slover, MD MS; Carlos Alvarado, MD
61. NYU Hospital for Joint Diseases
144
Variance in Discharge Disposition and Cost between Patients with Medicare and Commercial Insurance
following Total Hip and Total Knee Replacements
Lorraine Hutzler, BA; Joseph Bosco, MD; James Slover, MD MS; Carlos Alvarado, MD
62. St. Catherine of Siena Medical Center
Obesity Prevention Initiative
Diane Curley, MSN RN CNOR CBN
146
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
63. St. Catherine of Siena Medical Center
153
Bedside Report
Co-Principal Investigators: Miranda Corcoran, RN MA NE-BC; Bennarda Daly, RN; Catherine
O'Brien, RN BSN; Eileen Piekarski, RN MS OCN; Keri Wilson, RN BSN
64. St. Catherine of Siena Medical Center
155
Maintaining a Safe Patient Environment Without the Use of Restraints
Laurie Yuditsky, RN MBA BSN (Nursing PI Coordinator)
65. St. Catherine of Siena Medical Center
159
Reducing Incident of Hospital Acquired Pneumonia After Acute Stroke Through Implementation of
Simple Bedside Dysphagia Screen
Catherine Videtto, RN MSN ANP CPHQ; Mary Jane Finnegan, RN MSN
66. St. Catherine of Siena Medical Center
162
Cultivating Patient Safety: Integrating Simulation into Staff Development
Deborah A Kohn, BS RN CCRN; J Aidan Boswick, BA NREMT
67. St. Charles Hospital
163
Comparison of Pre and Post Test Scoring in the Pain Management Resource Nurse Program
Nicolette Fiore-Lopez, RN MA CENP; Kathleen LeDoux, MS RN B-C CPHQ
68. Stamford Hospital
168
Bundle Up: Lowering Hospital-Acquired C. difficile Infections in the Face of Rising Community
Prevalence
Merima Sestovic, Brenda Grant, Paula Castellano-Flynn, Michael Parry
69. Stamford Hospital
171
HCAHPS: Responding to the Voice of the Patient
Elizabeth E Longmore, MSN RN CEN; Sarah Sanders, BSN RN
70. Stamford Hospital
174
VENT ALERT! The Rapid Throughput of a Critically Ill Ventilated Patient to the ICU
Christin J Lucia, RN (CCRN Resource Nurse); Melinda Panapada, BS RRT (Respiratory Clinical
Coordinator); Kenneth Pestone, BS RRT (Respiratory Therapy Supervisor); Robert Salvi, MBA RPFT
(Manager Medical Services); Melissa Degnan, BS RRT (Respiratory Clinical Coordinator); Steven
Thau, MD FCCP (Board Certified in Pulmonary Medicine, Critical Care Medicine and Sleep
Medicine); Theresa Miano, RN (ED Charge Nurse)
71. Stamford Hospital
177
Maintaining our Hustle for Muscle: Hard-Wiring Primary PCI Performance
Darlene Sweet BSN RN; Perry Burgess, BSN RN
72. Stamford Hospital
Improving ED Throughput: Creating Change in a Challenging Climate
Rohit Bhalla, MD MPH; Ritu G Jain, MPH; Maher Madhoun, MD; Jayson Podber, MD; Sarah
Sanders, RN; Elizabeth E Longmore, RN MSN; Theresa Miano, RN; John Hegarty; Janet Palladino;
Scott Dunn; Tim Woodward; Kathleen A Silard, RN MS
180
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
73. Steven and Alexandra Cohen Children's Medical Center
183
Using Near Miss Events to Improve Patient Safety, Family-Centered Pediatric Pre-Surgical Experience
and Enhance High Reliability Performance of the Pediatric Pre-Surgical Testing and Evaluation Process
Kathy Albert, DNP; Fiona Levy, MD; Vincent Parnell, MD; Gloria Collura, RN; Pat Abitabile; Nicole
Romanelli; Terri Ann Parnell, DNP
74. Stony Brook Medicine
185
Reducing Complications of Care in the Intensive Care Unit
Denise LeBlanc, RRT (Director, Respiratory Care & Pulmonary Function); Henry MacLellan, RN
MPA (Assistant Director of Nursing, Surgical Critical Care); Christine McMullan, MPA (Director of
Continuous Quality Improvement); Paul Francis Murphy (Data Analyst, Continuous Quality
Improvement); Margaret M Parker, MD FCCM (Director, Pediatric Intensive Care); Grace Propper,
MS RN CPNP NNP-BC (Continuous Quality Improvement); Paul Richman, MD (Director, Medical
Intensive Care); Carolyn Santora, RN MSN (Interim Chief Quality Officer, Associate Director of
Patient Safety & Regulatory Affairs); Christine Schuhmacher, RN MS (Clinical Analyst, Continuous
Quality Improvement); Jeralyn Sigwart, RN MS PNP CNS (Nurse Manager, Pediatrics & Pediatric
Intensive Care); Lisa Sokoloff, BSN (Project Manager, Continuous Quality Improvement); Shanthy
Sridhar, MD (Director, Neonatal Intensive Care); Maureen Turner, RRT (Associate Director,
Respiratory Care Department); James Vosswinkel, MD (Director, Surgical Intensive Care); Donna
Wagner, RN MS (Clinical Nurse Specialist, Medical Intensive Care)
75. Stony Brook University Hospital
193
Automated Electronic Sepsis Alert Promotes Early Identification and Improves Mortality
Grace Propper, MS RN CPNP NNP-BC; Christine McMullan, MPA CPHQ; Paul F Murphy, Data
Analyst
76. SUNY Downstate Medical Center/ University Hospital of Brooklyn
200
Reducing Radiation Exposure to Neonates
Olatokunboh Osineye, MBBS; Adeola Dabiri, MBA MPA; Torrance Akinsanya, RHIA MPA CPHQ;
David Dinhofer, MD; Charles Carbone, LRT ARRT; Michael Vaughn; Umar Jalloh, MPA; James
Shanahan, MS
77. The Children's Medical Center at Winthrop University Hospital
205
Timely Recognition and Antibiotic in Severe Sepsis: The Children's Medical Center at Winthrop Pediatric
and ED Quality Improvement Initiative
Maria Lyn Quintos-Alagheband, MD; Lee Moldowsky MSNRN-BC; Sandee Zaera RN-BC
78. The Valley Hospital
210
Swallowing Safety: "It’s No Gag"
Peter Jarosz, MA MS CCC/SLP; Josephine Bodino, RN MPA NE-BC
79. The Valley Hospital
Eliminating VAPs in CSICU
Alcina Fonseca, RN MS MBA CCRN-CSC NE-BC; Gladys Reyes, MSN ACNP-BC CCRN-CSC-CMC;
Lisa Albarino, RN MSN CCRN CNRN
212
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
80. Vassar Brothers Medical Center
214
A Community Medical Center’s Approach to Reducing Joint Replacement Surgical Site Infections
Allison Essenmacher, RN CNOR; Joanne Ritschdorff, RN MSN CNOR; Michelle Spola, RN CNOR;
Barbara Hirsch, RN; Scott Pietras; Richard Sleight; Mary Ann Magerl, RN MA CIC; Lynn Kemp, RN
MA; Margaret M Cusumano, RN MSN FACHE; Janet L Ready, RN FACHE; Stephen A Katz, MD CPE
FACP
81. Vassar Brothers Medical Center
216
Improving Sepsis Care in ED Patients
Judith T Flaherty, RN CPHQ; Denise Quirk-Hall, NP CNS
82. White Plains Hospital
219
Integrated Delivery System of Disinfection Cap & Flush Syringe, Plus Staff Education, Lowers
Bloodstream Infection Rate & Treatment Costs
Saungi McCalla, MSN MPH RN CIC; Janet Greco, MA RN-BC OCN; Meg Warren, MSN; Joyce
Bogetti, RN; Patricia Byrne, RPh MPA
83. Winthrop-University Hospital
221
Transformational Journey of a Care Delivery Model: Implementation of Evidenced-Based Practice to
Increase Breastfeeding Exclusivity
Eileen Magri, MSN RN NE-BC; Mary Lynn Brassil, MS RN CES; Cathyjo Catalano, MS RN RNC-OB;
Mary Cleary, BSN RN NE-BC; Stephanie Hisgen, MPH RN; Karen Hylton-McGuire, MS RNC NIC
IBCLC RLC; Amy McGuire, MS RN
84. Winthrop-University Hospital
224
Evaluation of a Computerized Physician Order Entry (CPOE) Alert Program on Prescribing of Selected
Drugs Among the Elderly
Liliana Rios-Rojas, MD; Paula E Lester, MD FACP; Irving H Gomolin, MD
85. Winthrop-University Hospital
226
IHI Project on Safe Patient Handling Technique by Using Pink Slip Patient Transfer System
Elizabeth Baynes RN; Carol L. Cohan RN BSN MHA; Manjula R Stanislaus, RN MSN MHA CCRN
CMC RN-BC
86. Winthrop-University Hospital
229
Nurse-Driven Strategies for the Reduction of Hospital Acquired Pressure Ulcers in Three Neuroscience
Units
Janice McGuinness, BSN CNRN; Sherry Persaud-Roberts, BSN CNRN; Susan Marra, BSN RN;
Jeannine Ramos, BSN CNRN; Diane Toscano, RN; Linda Policastro, Nursing Assistant; Lee
Moldowsky, MSN RN-BC; Nancy Epstein, MD
87. Winthrop-University Hospital
Success in Early Patient Discharge in a Medicine/Surgical Unit Through a Collaborative Approach
Proserfina A Ventura, MSN RN (Potter 3 Nurse Manager); Marilynn Domagala, BSN RN (Potter 3
Assistant Nurse Manager); Monica Santoro (Vice President & Chief Quality Officer Department of
Patient Safety, Quality and Innovation); JeanMarie Moorehead, MA RN (Director of NursingMedicine and Surgery); Linnea Drew, RPA-C (Associate Director PA/NP Services, Clinical Manager
General/Vascular Surgery, Chief Surgical Physician Assistant)
231
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Page
88. Winthrop-University Hospital
234
Using the National Surgical Quality Improvement Project (NSQIP) to Decrease Ventilator Days and
Pneumonia in a Surgical ICU
John McNelis, MD FACS; Roseann Grandelli, RN; Maureen Keegan, RN; Eva Chalas, MD FACS;
Monica Santoro, RN CPHQ
89. Winthrop-University Hospital
236
A Tetralogy...Hemorrhage, Hypertension, DVT, Infection. Implementation of a Perinatal Safety Net
Mary Lynn Brassil, MS RN C-EFM; Margaret Celenza, MS RNC-OB C-EFM
90. Winthrop-University Hospital and Children's Medical Center
239
Healthcare in the 21st Century: Bridging the Gap between Medical Education and Quality of Patient Care
Ulka Kothari, MB BS; Joseph Greensher, MD; Jill Leavens-Maurer, MD; M L Quintos-Alagheband,
MD
91. Winthrop-University Hospital, Department of Obstetrics and Gynecology
Patient-Centered Care of the Pregnant Patient with Diabetes Who Uses an Insulin Pump During Labor and
Delivery
Mary Lynn Brassil, MS RN C-EFM; Margaret Celenza, MS RNC-OB C-EFM; Virginia PeragalloDittko, RN BC-ADM CDE (Executive Director of the Diabetes & Obesity Institute); Jane Wendel, RN
BS CDE; Linda Zintl, RN BSN (Inpatient Diabetes Nurse Clinicians)
243
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
HANYS Report on Report Cards
Robert J Panzer, MD; Martha Radford, MD; Brian K Regan, PhD; Kathleen Ciccone, RN MBA; Christa
Christakis, MPP; Christina Miller-Foster, MPA; Mary Therriault, RN MSN
Healthcare Association of New York State (HANYS)
Introduction
Health care providers and facilities are facing a proliferation of publicly released quality information, commonly
known as "report cards." Supporters of these report cards tout their transparency, competitive value, and ability to help
people make choices. However, problems with the accuracy, clarity, timeliness and comparability of measures persist,
limiting the usefulness of these reports for informing consumers and helping providers improve care. HANYS Report
on Report Cards was developed as a resource for hospital leaders and their boards; it serves as a primer for evaluating
publicly available consumer report cards.
Problem
Multiple hospital quality report cards which use inconsistent quality information and methodologies and often yield
dramatically different results create confusion for consumers. Moreover, hospitals are burdened with trying to dissect
each report's methodology to determine whether or not it has merit for its own quality improvement efforts. This is
particularly true for report cards that rely on administrative (billing) data, rather the most valid, clinically based
measures such as those collected as part of the National Health Safety Network (NHSN). With increased pressure from
government, payers and consumers for more efficient and higher quality care, it is critical for hospitals to evaluate the
reliability and validity of publicly available report cards.
Goals
The HANYS Statewide Steering Committee on Quality Initiatives developed resources for hospital leaders and their
boards to assist them in understanding, evaluating and responding to publicly available consumer report cards,
including:
• Guiding principles for evaluating public report cards;
• HANYS' position on the various hospital report cards, based on the guiding principles;
• Media talking points;
• An illustration of the variation among various hospital report cards; and
• A sample presentation.
Methods
The HANYS Statewide Steering Committee on Quality Initiatives first addressed this topic in 2007, issuing its report,
"Understanding Publicly Reported Hospital Quality Measures: Initial Steps Toward Alignment, Standardization, and
Value" which outlined the attributes and short comings of publicly available report cards. The 2012 version of this
report is a condensed and updated version of the 2007 report.
The Committee met several times in 2012 to develop and refine the guiding principles used to evaluate each report card
and develop a scoring methodology to evaluate the report cards based on the guiding principles. The guiding principles
also illustrate the components of an ideal report card on hospital quality.
Quality Symposium 2012
Page 1
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Committee members are currently in the process of finalizing the scoring of each public report card. To develop a score
for each public report card, a subgroup of Committee members conducted an independent analysis of the various report
card methodologies. For each of the established criteria, report cards earn a score of 1 if they fully meet the criteria; 0.5
if they partially meet the criteria; and a 0 if they fail to meet the criteria.
After achieving consensus among the Steering Committee members, scores will then be combined for a total and
translated to a percent, and then a letter grade.
Results
The HANYS Statewide Steering Committee on Quality Initiatives developed a comprehensive package of tools and
resources for hospital leaders to use when communicating with their boards, staff and other constituents, as well as the
media regarding the reliability of these report cards. The guiding principles document not only illustrates the
components of an ideal report card, but also serves as a tool to evaluate publicly available report cards. The Report
will help hospitals focus efforts on findings that can best guide improvement in quality outcomes.
Conclusions
Hospitals and the public should be aware that significant variation exists among the various public report cards. While
the goal is to provide a simple and understandable resource for consumers, multiple reports using conflicting
information are confusing for consumers, and inhibit, rather than enhance, consumer decision making and distract from
hospital quality improvement efforts.
HANYS and its members will continue to promote a federal and state agenda for the national alignment of quality
measures and specifications that are evidence-based and endorsed by the National Quality Forum (NQF).
Quality Symposium 2012
Page 2
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Implementation of a Bladder Bundle Program in an Orthopedic Specialty Hospital
Eileen A Finerty, MS RN FNP CIC; Helen Renck, MSN RN; Patricia Griffin, MS RN CPHQ; Mary
McDermott, MSN RN ANP NE-BC; Barry Brause, MD; Anne LoBasso, RN MBA
Hospital for Special Surgery
Introduction
Hospital for Special Surgery (HSS) conducted a risk assessment to determine the risk of catheter-associated urinary
tract infection (CAUTI) in our adult surgical patients. The majority of the orthopedic surgery patients receive patient
controlled analgesia through an epidural catheter which necessitates indwelling urinary catheter insertion. CAUTI is a
frequent health care-associated infection (HAI) usually accompanied by high cost and prolonged length of stay (LOS).
• Urinary Tract Infections (UTIs) account for >30% of hospital acquired infections (HAI)
• >80% of UTI infections are related to unnecessary indwelling catheters
• Risk of UTI is influenced by catheter duration (CDC, 2009)
• Limiting catheter use assists in reducing CAUTI infection rates
• Compliance reported to both TJC & CMS effective January 2010 (SCIP-Inf-9 measure) discharges
Problem
• Opportunities for improvement in timely urinary catheter removal and associated CAUTI rates were identified.
• In January 2010, baseline compliance in removing urinary catheter by postoperative day one or two was 81%.
• Opportunities for improvement existed regarding bladder assessment practices and indwelling catheter insertion
techniques.
• Opportunities for improvement regarding automation of computerized prescriber order sets and documentation of
indications for catheter use and removal.
Goals
• Formulate an Interdisciplinary Team to review current guidelines, data, products and best practices.
• Review of data and related documentation practices to identify opportunities for improvement regarding catheter
insertion, continuance and discontinuation.
• Analyze data and causes of process variation, inclusive of the use of epidural anesthesia, computerized prescriber
order entry (CPOE), insertion technique, catheter maintenance & patient satisfaction data.
• Timely catheter removal within POD 1 or POD 2 or documentation of assessment for continued need.
• Reduce the institution’s CAUTI rate.
Methods
• FOCUS PDCA team activities focused on performing an Infection Control Risk Assessment and incorporation of
evidence based practices.
• Revised MD order sets to link catheter expiration dates with epidural catheter removal; indications for continued need.
• Automate nursing electronic documentation to include timing of catheter insertion and removal.
• Review of all preoperative patient and staff education.
• Review/revision of the HSS Interdisciplinary Policy and Procedure on the Management of the Patient with an
Indwelling Urinary Catheter.
• Evaluation of, and introduction of hand held bladder scanners to reduce unnecessary invasive catheterizations.
Quality Symposium 2012
Page 3
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Urinary Catheter insertion and drainage products trials conducted.
• Competency and skills validation for insertion completed.
Results
• Significant improvement in timely catheter removal, from 81% (January 2010) to 100% (March 2012) -- see Figure 1.
• CAUTI rates reduced from 6.5 per 1000 catheter days in Q2 2011 to 1.16 per 1000 catheter days in 4Q11 -- see
Figure 2.
• Exceeded National and NYS results as reported by Hospital Compare -- see Figure 3.
• New CPOE order sets implemented.
• New order sets for Nursing to document timing of catheter insertion and removal.
Conclusions
• A systematic evidence based approach improved timely catheter removal.
• Additional improvement opportunities surrounding diagnosis and treatment of CAUTI are in progress such as urine
culture protocols.
• Adoption of external national CDC nomenclature on case definitions, such as symptomatic UTI (SUTI) and
Asymptomatic Bacteremic UTI (ABUTI).
• Explore reasons for extended catheter usage stratified by service.
• Review of antibiotic usage related to CAUTI being investigated.
Quality Symposium 2012
Page 4
Figure 1:
Source: Press Ganey
Figure 2:
Quality Symposium 2012
Page 5
Figure 3:
Source: Hospital Compare (data as of July 2012)
Quality Symposium 2012
Page 6
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Implementing an Adult Vaccination Program in an Orthopedic Specialty Hospital
Eileen A Finerty, MS RN FNP CIC; Helen Renck, MSN RN; Patricia Griffin, MS RN CPHQ; Mary
McDermott, MSN RN ANP NE-BC; Barry Brause, MD; Andy Miller, MD
Hospital for Special Surgery
Introduction
Implementation of an adult inpatient screening program for influenza and pneumococcal vaccination eligibility and the
development of a process to vaccinate interested patients, when indicated, as:
• Development of an immunization program is an important public health initiative
• Compliance reported to both TJC & CMS effective January 2012
• Risk assessment showed opportunities for improvement in vaccination rates for Influenza and Pneumococcus
Problem
• Perceived negative impact of vaccinations on the immediate perioperative patient experience
• Immunization is considered a primary care responsibility
• Difficult to implement practice in a hospital with an average length of stay (ALOS) of 3.9 days
• Vaccinations were ordered on an individual basis
• Absence of a systematized process for vaccination assessment, ordering, administration, and documentation
• Presence of a hybrid documentation system (paper vs. electronic) posed difficulties in standardizing the process
Goals
• Improve compliance with regulatory measures from baseline (December 2010):
Pneumococcal Immunization: 41% compliance
Influenza Immunization: 0% compliance
• Educate hospital staff & community on public health initiative & develop a patient and staff educational program
• Develop a systematic comprehensive vaccination assessment program using a Registered Nurse driven protocol
approved by the Medical Board
Methods
• FOCUS PDCA team activities focused on development of a pre-hospitalization vaccination program, review of
internal screening results and the development of a screening program
• Review/re-design of CPOE order sets to include drop-down selections to match criteria for administration and/or
contraindication
• QM dissemination of unit based vaccination assessment results
• Development of HSS Interdisciplinary Policy & Procedure for Immunization Screening & Vaccination
• Patient education and poster campaign in collaboration with MD Private practice Office Managers
• Service Lines educated on reinforcing with patients need to get vaccinated at least > 7 days before surgery
• Medical staff and leadership educated on this health initiative
• Development of a systematic assessment program
Results
Significant improvement in compliance noted for both Pneumococcal and Influenza Immunization measures.
Quality Symposium 2012
Page 7
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Pneumococcal Overall Compliance went from 41% (December 2010) to 77% (1Q12) -- see Figure 1.
• Influenza Immunization Overall Compliance went from 0% (December 2010) to 85% (1Q12) -- see Figure 2.
Conclusions
• Audit results showed need to re-educate staff about assessing and immunizing patients with chronic diseases
• Develop and rollout Immunization Manager Registry to achieve meaningful use requirements
• Focus on developing a similar program for pediatric immunizations
• Sustain improvement & automate pre-surgical screening vaccination efforts
Quality Symposium 2012
Page 8
Figure 1:
Pneumococcal Immunization
100%
80%
77%
60%
40%
41%
48%
42%
20%
0%
4Q10
1Q11
2Q11
1Q12
Figure 2:
Influenza Immunization
100%
85%
80%
60%
42%
40%
20%
0%
0%
4Q10
1Q11
1Q12
Quality Symposium 2012
Page 9
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Perioperative Diabetes Management: HbA1c Screening
Linda Russell, MD; Raquel Mayne, MS MPH RN; Zahava Alter, MBA; Ann LoBasso, MBA RN; Gregory
Liguori, MD; Andrew Martorella, MD
Hospital for Special Surgery
Introduction
Diabetes Mellitus impacts approximately 10% of surgical patients at HSS, which is consistent with national estimates
(8%) from the Center for Disease Control & Prevention (CDC). In 2010, CDC, estimated that 20-33% of the US
population would have diabetes by 2050. Patients with poor glucose control are at increased risk for infection, poor
wound healing, increased length of stay. As such, an interdisciplinary group was conceived in order to assess
perioperative management of diabetic patients, which generated guidelines for the organization. Efforts were made to
improve physician compliance to the preoperative portion of these guidelines.
Problem
The Perioperative Diabetes Management guidelines consisted of recommended action during each interval of
perioperative period including: preoperative HbA1c screening, recommended actions for elevated HbA1c, and
mandatory surgical cancellation for HbA1c >10%. Quality Management made efforts to assess baseline practice within
the organization noting that preoperative HbA1c screening was not a standard practice amongst diabetics. Only 10% of
diabetic patients were screened during their preoperative medical evaluation/optimization. The focus was turned to
improving timely HbA1c screening.
Goals
(1) Improve preoperative compliance to HbA1c screening among medical staff to 90%.
(2) Increase percentage of patients with HbA1c screening 8 or more days prior to surgery.
Methods
QM audits targeted physician performance related to the preoperative phase of the guidelines with feedback to each
department (i.e. Orthopedic Surgeons and their Office Managers, Dept. of Medicine, Academic Training) via staff
meetings, repeated mass e-mail distributions, and then individualized performance reports (see graph 2 and 3).
Results
HbA1c screening improved from 10% compliance in May 2011 to a peak of 69% in January 2012. Last audits the 2nd
quarter 2012, reflect a compliance rate of 64% (see graph 1).
Conclusions
• Medical staff and their offices respond feedback out their performance as a group and as individuals.
• There were inconsistencies regarding screening pre-diabetics, with some Clinicians opting to screen and others not.
• Acceptable age and source of an HbA1c needed to be considered in clinicians decision to screen as some used
undated or patient reported values.
• Future efforts will focus on compliance to medication titration for elevated lab results.
• Patient outcomes may need to be assessed as a method of changing physician behavior.
Quality Symposium 2012
Page 10
Quality Symposium 2012
Page 11
Quality Symposium 2012
Page 12
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Risk Factors for Returning to the PACU After Orthopedic Surgery
Michelle Mangini; Ting Jung Pan, MPH; Michael Urban, MD; Mayu Sasaki, MPH; Stephen Lyman, PhD;
Steven Magid, MD
Hospital for Special Surgery
Introduction
N/A
Problem
Every year approximately 200 patients who undergo orthopedic surgery at HSS are discharged from the PACU to a
routine nursing floor, only to be readmitted to the PACU (RT-PACU) during the same hospital admission for
observation or treatment of complications. Although this category of patient has been studied in general hospitals, there
is little literature from specialty hospitals without formal ICUs. These patients have longer length of stays and are also
at risk for additional hospital-acquired complications.
Goals
To identify clinical characteristics of patients who were RT-PACU and compare them to patients undergoing similar
procedures who did not return to the PACU. By doing so, we hope to either modify risk factors or monitor this group
of patients more carefully; thereby reducing complications and RT-PACU.
Methods
A cohort of 8,309 patients who underwent primary total hip replacement (THR), partial hip replacement (PHR),
revision of total hip replacement (RTHR), primary total knee replacement (TKR), revision of total knee replacement
(RTKR), spine fusion, and spine refusion during April 2009 - March 2010 were selected. Case patients were those who
were RT-PACU for intensive care after being transferred to a patient floor (n=162; 1.9%). Controls were patients who
had the same procedures as cases during the study time frame but did not return to PACU (n=8,147; 98.1%).
Charlson Comorbidity Index and Elixhauser Comorbidity were calculated to account for the case-mix and
comorbidities present on admission. Logistic regression was performed to determine the influence of age, sex, race,
procedure type, ASA score, sleep apnea and comorbidities on the likelihood of patient returning to PACU. Subgroup
analyses were also done on hip procedures, knee procedures, and spine procedures. The significant level was 0.05.
Results
Most of the patients underwent primary TKR (cases: 70, 43.2%; controls: 3,258, 40.0%), followed by primary THR
(cases: 36, 22.2%; controls: 2,959, 36.3%) and spine fusion (cases: 32, 19.8%; controls: 1,209, 14.8%). Caucasian race
is the dominant racial group in the cohort (cases: 136, 84.0%; controls: 6,966, 85.5%).
TKR patients were 55% more likely than THR patients to return to PACU (OR=1.55 [1.02, 2.34]; p=0.039). Spine
fusion patients were 127% more likely than THR patients to return to PACU (OR=2.27 [1.34, 3.83]; p=0.002). Patients
who underwent spine refusion had (approximately) 12 times the risk of returning to the PACU compared to the
primary THR patients (OR=12.50 [4.68, 33.38]; p=<0.001).
Quality Symposium 2012
Page 13
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Patients who have chronic pulmonary disease, diabetes, renal failure and coagulopathy had a higher risk of RT-PACU
compared to those who did not have these conditions present on admission. Also, patients with a higher Charlson
Comorbidity Index had a higher risk of RT-PACU than patients with a lower Charlson Comorbidity Index.
Conclusions
Patients undergoing total knee replacement, spine fusion or spine refusion procedures or who have chronic pulmonary
disease, diabetes, renal failure or coagulopathy will have an increased risk to return to the PACU after their surgery.
Also patients with a higher Charlson Comorbidity Index have a higher risk of RT-PACU. It is our intention to monitor
these patients more carefully during the perioperative period to reduce complications and RT-PACU. Future studies of
PACU readmission for orthopedic surgeries should incorporate BMI, creatinine and hemoglobin into the logistic
regression model to see if these covariates influence whether a patient returns to the PACU. Studies should also use a
larger cohort population to see if these effects will still be present.
Quality Symposium 2012
Page 14
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Reducing Restraints in the Inpatient Behavioral Health Setting
Joseph Merlino, MD MPA (Deputy Executive Director); Renuka Ananthamoorthy, MD (Chief of Service); Jill
Bowen, PhD (Sr. Associate Executive Director, Chief of Staff); Roumen Nikolov, MD (Associate Chief of
Service); Linda MSN NPP NEA-BC (Associate Executive Director, Nursing); Chikodiri Gibson, RN (Sr.
Associate Director Nursing); Lora Giacomoni, RN MSN (Sr. Associate Director Quality & Compliance);
Luther Summers Hamilton, MSW (Associate Director Performance Improvement)
Kings County Hospital Center
Introduction
Kings County Hospital Center (KCHC) is a member institution of the New York City Health and Hospital Corporation
(HHC) one of the largest municipal health care systems in the country. HHC has 11 facilities operating psychiatric
emergency services and inpatient psychiatric care. With 627 beds, KCHC remains on the cutting edge of healthcare
and provides a wide range of services, and specialties are offered in all fields of modern medicine. KCHC has 160
adult and 45 child and adolescent inpatient psychiatric beds.
The reduction of restraint use has been given national priority by the US government, The Joint Commission, the New
York State Office of Mental Health and many patient advocacy groups. Restraint usage is associated with high rates of
patient and staff injuries, including patient deaths and is a coercive and potentially traumatizing intervention. The staff
of Behavioral Health Services (BHS) realizes that restraint usage is not in and of itself a treatment intervention; rather
restraints are considered a last resort safety intervention. Restraints do not serve to assist patients manage their triggers
that lead to situations resulting in the need for such interventions. Additionally, restraint usage can serve to
retraumatize patients. When deemed absolutely necessary, they should be utilized only by staff that is appropriately
trained to do such.
KCHC has adopted Breakthrough as a philosophy for improving the delivery of healthcare to the community in which
it serves. Lean methodology empowers staff to improve services, the patient experience, and the effectiveness of work
flows. Using Lean methodology BHS set out to reduce the rates of restraint usage in the behavioral setting.
Problem
As a member of HHC, KCHC BHS was able to compare restraint rates with other HHC facilities as well as nationally.
The current state of restraint usage in BHS revealed that the restraint rates were higher than both the HHC Corporate
and national averages for the BHS at KCHC. This became the burning platform out of which the need for action was
identified. A chartered performance improvement team was launched in April of 2011.
Goals
After identifying the reason for action, the Restraint PI team set forth on identifying what the project goal would
consist of. The team envisioned a target state where staff and patients collaborated on early recognition of triggers for
behaviors that lead to restraint episodes along with the patient’s identification of alternative measures which could be
employed during crisis situations. The metrics utilized in order to measure success were identified as restraint rates for
each service -- Adult and Child & Adolescent.
Methods
Quality Symposium 2012
Page 15
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The team began with a monthly review the data on an aggregate and patient level basis. This review informed the gap
analysis. It was identified that a small number of patients are associated with a high number of restraint episodes. The
team’s solution approach was simple; if the restraint episodes for this cohort of patients were reduced or eliminated
then the restraint rate would decrease. A completion plan was created incorporating the creation of a "High Utilizer
Alert" protocol and a restraint reduction algorithm culminating in an individual restraint reduction plan for each
patient.
The high utilizer alert protocol included:
• Identification of patients who had multiple restraint episodes and assigning a category based upon cumulative
episodes; 1: greater than 20 episodes; 2: 10-19 episodes; and 3: 3-9 episodes. In order to create the initial list, the data
shop was able to harvest this information for the prior 18 months from the EMR.
• Process for dissemination to all clinical leadership including the Comprehensive Psychiatric Emergency Program
(CPEP) as well as the peer counselors.
• Upon presentation, either direct admission to an inpatient unit or in the CPEP, the nursing staff review the high
utilizer list. The identification of a high utilizer results in notification to the psychiatrist in charge and the treatment
team. All subsequent communications such as SBARs, huddles, and morning briefings include this alert irrespective of
whether or not restraints have been warranted.
The restraint reduction algorithm is then implemented to formulate the individual restraint prevention plan including
triggers, early warning signs, and coping strategies. This includes:
• Expeditious review of the prior medical record and in particular a review of any prior Individual Behavioral Plans
(IBP) that were in effect.
• Communication with the patient regarding past experiences including restraint episodes and triggers.
• Patients are offered self-management tools.
• All team members are informed of the identified triggers and coping measures chosen by the patient in order to
assist with supporting the therapeutic quality of the milieu and helping the patient feel safe.
The team conducted a rapid experiment with the first patient who was admitted to the adult inpatient service and
identified as a high utilizer. It was noted that this patient had a history of multiple restraint episodes during multiple
admissions which had a negative impact not only on her course of hospitalization but also on the staff and the unit as a
whole. The patient and the staff experienced higher levels of frustration. Upon readmission the team immediately
implemented the algorithm. The patient identified factors which influenced behaviors that resulted in restraint episodes
identifying that she experienced tension release from these behaviors. The team worked with the patient to identify the
interventions that were effective in supportive, soothing, and served to help the patient calm herself. Each discipline
identified their contribution to supporting the plan. The experiment was successful in that the restraints were avoided
during this readmission. The case presentation was incorporated into the roll out of the project to all inpatient areas.
Results
The index case presentation was incorporated into the roll out of the project to all inpatient areas. Lessons learned were
applied to other patients with similar success. Data collection continued on a monthly basis both on a service level and
unit level. Within six months of project initiation, restraint rates for both the adult and child/adolescent units showed
downward trending. Furthermore, rates subsequently were below both the identified threshold as well as the 18 month
average [see control chart].
Quality Symposium 2012
Page 16
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Conclusions
The index case presentation was incorporated into the roll out of the project to all inpatient areas. Lessons learned were
applied to other patients with similar success. Data collection continued on a monthly basis both on a service level and
unit level BHS met it target of reducing restraint rates, however, BHS also was able to influence the culture.
Understanding that restraints are not therapy and actually detract from wellness strengthened the overall culture of
safety. Results were sustainable over time. In addition to posting restraint rates on each unit, white boards indicating
the days since last restraint episode provide visual daily management.
Quality Symposium 2012
Page 17
0.040
Restraint Rate (W/A)‐ Child & Adolescent Inpatient
January 1, 2010‐ July 31, 2012 0.038
0.035
0.030
0.029
0.026
Restraints
0.025
0.021
0.020
Restraints Rate
Threshold
Average
0.015
0.015
0.014
0.013
0.015
0.014
0.012
0.010
0.011
0.011
0.009
0.008
0.007
LCL
0.011 0.011
0.009
0.005
0.005
0.003
0.000
0.014
0.014
0.003
0.002
0.008
0.008
0.007
0.006
0.004
0.003
0.000
Quality Symposium 2012
Page 18
Restraint Rate (W/A)‐ Adult Inpatient
January 1, 2010‐ July 31, 2012 0.012
0.010
0.0100
0.0082
0.008
Restraints
0.0076
0.0074
0.0067
0.006
Restraints Rate
0.0056
0.0054
0.0054
Threshold
0.0052
0.0048
0.004
0.0047
0.0039
0.0038
0.0035
0.0041
0.0040
0.0035
0.0033
0.0029
0.0025
0.0027
0.0021
0.002
0.0016
0.0009
Average
LCL
0.0033
0.0026
0.0026
0.0021 0.0021
0.0017
0.0006
0.000
Quality Symposium 2012
Page 19
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Reducing the Use of 1:1 Observations
Joseph Merlino, MD MPA (Deputy Executive Director); Renuka Ananthamoorthy, MD (Chief of Service); Jill
Bowen, PhD (Sr. Associate Executive Director Chief of Staff); Roumen Nikolov, MD (Associate Chief of
Service); Linda MSN NPP NEA-BC (Associate Executive Director Nursing); Lora Giacomoni, RN MSN (Sr.
Associate Director Quality & Compliance); Luther Summers Hamilton, MSW (Associate Director
Performance Improvement); Akinola Adebesi, MD; Elise Feldman, PhD
Kings County Hospital Center
Introduction
Kings County Hospital Center (KCHC) is a member institution of the New York City Health and Hospital Corporation
(HHC) one of the largest municipal health care systems in the country. HHC has 11 facilities operating psychiatric
emergency services and inpatient psychiatric care. With 627 beds, KCHC remains on the cutting edge of healthcare
and provides a wide range of services, and specialties are offered in all fields of modern medicine. KCHC has 160
adult and 45 child and adolescent inpatient psychiatric beds.
The Behavioral Health Service (BHS) perceived that the use of 1:1 Observation was to prevent patients from injuring
themselves when they were unable or unwilling to, to promote healing or when a clinical screening tool indicated a
high risk of immediate or impulsive suicidal or violent behavior. KCHC has adopted the Lean/ Breakthrough
methodology as a philosophy for improving the delivery of healthcare to the community in which it serves. Lean
methodology empowers staff to improve services, the patient experience, and the effectiveness of work flows.
Problem
BHS was noted to have a high number of orders for 1:1 Observations. This rate was heavily taxing to the department's
human and financial resources, thus impacting the quality of care provided to the patients and served as the reason for
action.
Goals
Baseline data was collected regarding the number of 1:1 orders written for one quarter and resulted in identification of
2,080 orders. A target of reducing orders to 1,456/ quarter was set. Additionally, BHS looked to capture the fiscal
impact of this reduction.
Methods
BHS conducted a Breakthrough Rapid Improvement Event (RIE) process to address the use of 1:1 Observations.
Through a series of observations, discussion, and anonymous survey the current state of high numbers of 1:1s was
identified. The most significant factors influencing this state included a perception of increased safety of the patient,
lack of administrative support should an incident occur while a patient was not on a 1:1, and under-utilized alternatives.
Base line data was collected and targets were set.
An open letter from the Deputy Executive Director to front line staff was issued to address any perception of lack of
support. This issue was subsequently reinforced in a series of meetings between administration and physicians.
Quality Symposium 2012
Page 20
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Incidents rates were superimposed upon the number of 1:1 orders in order to demonstrate the lack of correlation with
use of 1:1 and the perception of increased safety.
Bidirectional communication occurred as each discipline collaborated on the criteria for purpose and use of 1:1s, the
elimination of automatic 1:1s based upon clinical screening tool scores, and any necessary policy revisions.
Clinical leadership conducted rounds to validate the utilization of 1:1s when clinically appropriate. The decision to
utilize a 1:1 was supported through adequate documentation in the medical record.
Results
Data collected revealed that the Rapid Improvement Event was successful at reducing the overall number of 1:1s. The
target goal was reached and surpassed. Results are represented in Table 1.
Conclusions
BHS had realized significant gains in reducing the number of 1:1s utilized.
Quality Symposium 2012
Page 21
1:1 Orders
2000
1800
1600
$678,680
1400
$662,580
$463,500
1200
$584,820
$731,160
1000
1:1 Orders
800
600
400
200
0
1Q 2011
2Q 2011
3Q 2011
4Q 2011
1Q 2012
2Q 2012
Quality Symposium 2012
Page 22
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Use of Quality/Safety Data for Institutional Planning
Marcella De Geronimo, MS; Rosemarie Linton, MPH; Kevin D Masick, PhD
Krasnoff Quality Management Institute - a Division of the North Shore-LIJ Health System
Introduction
Leadership charged the analytic group of the Krasnoff Quality Management Institute with developing and
implementing a tool, a kind of digital nervous system, that would standardize data collection, data analysis, and the
reporting of quality and safety indicators so that the 13 hospitals in the North Shore-LIJ Health System could
effectively and efficiently monitor care across the system and provide hospitals with a user-friendly web-based
opportunity to share best practices. The CMO of the system took ownership of the initiative, underlining the
importance of using data to monitor care and to provide system hospitals with a single valid source of truth. He
challenged the C-suite at both the system and hospital levels to know and understand the monthly reports and to be
accountable for results. For example, hospital leadership would be held responsible for knowing what their sepsis
mortality rate was, how it compared to other hospitals, whether or not there was variation from previous months, and if
it was higher than a defined benchmark, they were expected to explore the reasons for the variation and to institute
corrective actions, if appropriate.
Problem
This initiative addressed the lack of standardized data definitions, disparate data collection techniques, ineffective and
variable reporting of data and poor communication efforts. Hospitals across the system had individualized and different
ways of displaying data, making it difficult to compare results with other system hospitals. With this web tool,
information could be distributed not only to top leadership but to all those in the organization who had a need to know.
Before the introduction of this Quality and Safety Vector of Measures, end-users would call quality management,
Krasnoff Quality Management Institute, finance, human resources or specific departments, such as infection control,
ED, risk management, etc to initiate a report run of their data. Developing a centralized and standardized data
dashboard would overcome the problem of end-users’ lack of immediate access to their own data. Also, since system
hospitals did not have a single data source that would reliably reflect care, there was no integration of clinical,
financial, HR, and organizational variables, which forms a complete picture of care, and is necessary to make informed
decisions about care and resource allocation. Integrating data sources, standardizing definitions, and centralizing the
display on a dashboard would solve these problems.
Goals
The primary goal of the initiative, an innovative performance dashboard, the Quality and Safety Vector of Measures,
was to standardize a framework for data reporting and display across system hospitals to drive clinical practice and
performance evaluation as well as educate users about the power of data to monitor and improve performance. The
analytic group developed a process tool that provided the end-user (clinical and administrative leadership) with a
dynamic interactive platform which would be user-friendly and easily navigated. Leadership was also committed to
promoting transparency. All stakeholders across the system can see performance data of their hospital as well as other
system hospitals and integrated system data. In addition, standardized data, graphically displayed, was developed in
order to enable broad access to information. Users of the innovative web application had the opportunity of providing
feedback about the concurrent data that was reported so that variations in expected data results could be explained in
Quality Symposium 2012
Page 23
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
real time for system wide dissemination. The Quality and Safety Vector of Measures displays 58 standardized
variables, giving leadership valid information to improve oversight and assist hospital executives in making informed
decisions about clinical care and resource utilization.
Methods
To create a standardized platform for data analysis and reporting, the Krasnoff Quality Management Institute Analytic
Team developed a streamlined process to integrate disparate data sources: hospital billing data, Premier 3M APR DRG
risk-adjusted data, clinical information, Press Ganey patient satisfaction data, ambulatory, operational and HR data.
The analytic team developed a special interface that would aggregate these different data sources and stored the data in
a single data warehouse. The web application tool that was developed provides a feedback tab which affords users the
opportunity to comment and explain variation in the standardized data displays (control charts, run charts, T charts).
Thirty-six months of data are displayed to allow for seasonal variation and change. Once 18 months of data have been
entered, there is an automatic conversion from a run chart to a control chart. These innovations in data standardization
and display are highly sustainable. Once the tool was deployed, educational efforts to promote buy-in of the web tool
were conducted. Users were taught how to access the tool, how to interpret the control charts, understand the p-values
and T charts. The education is reinforced monthly through on-line tutorials, web-ex sessions, monthly user group
meetings, and quarterly site visits.
Results
Data on 58 variables that track the management of care of high-volume high-risk conditions, such as sepsis mortality,
Heart Failure readmission, HF mortality, among others, are displayed monthly on control charts, run charts, and T
charts. Clinical and administrative leadership can easily assess whether there are variations in care and whether the
trend is toward improvement or not. This on-line availability is updated monthly so leadership has access to concurrent
data. The system CMO is challenging hospital CMOs to know their numbers and be accountable. He is able to close
the feedback loop by asking site CMOs to supply explanation for variation. The hospital sites are becoming familiar
and comfortable with the feedback capacity and are beginning to use the data to drill down to further analysis and to
ask the Krasnoff analysts for more information. Moving from simple bar graph displays of data to control charts are
helping users to become more sophisticated about understanding and manipulating data. They are becoming familiar
with trend lines and identifying special cause variation. Also, they are exploring the data displays and commenting on
the results. Data are trusted as reliable, valid, standardized across the system and representative of care. Not only can
users look across indicators to see how well their hospital is doing but they can see, on one page, a system report and
all the system hospitals data for one measure on the same scale, enabling easy comparison at a glance. Reports are no
longer unwieldy voluminous paper packets. An unanticipated result of the initiative is how validated hospital personnel
feel because they see that their clinical experience has been quantified and disseminated to others which has opened
lines of communication between analysts, clinicians and administrators.
Conclusions
The successful development of this interactive web-based Quality and Safety Vector of Measures and its adoption and
acceptance by users who were somewhat uncomfortable using data to represent care management has transformed the
identification of gaps in care and best practices. Clinicians and administrations seem knowledgeable about how to use
data and increasingly eager to use the tool. Providing targeted and ongoing education has been most productive as well.
Because results are reported and easily accessed, caregivers require less time to process important information. The
initiative to adopt user friendly interactive data reports which would standardize reporting across the system and be
available transparently to all personnel is efficient and effective. The dashboard has increased accountability and
improved the reliance on data to monitor care. The tool is sustainable and replicable.
Quality Symposium 2012
Page 24
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Reducing Patient Falls in the Inpatient Setting Through Innovation and Education.
Lisa Hanrahan, RN MSN CENP CPHQ CPHRM; Missy Paolicelli, RN OCN MSN; Majella Venturanza, RN
MA CCRN; Christine Demo, RN MSN TNCC; Michelle Pollack, RN CPHQ
Lawrence Hospital Center
Introduction
Falls continue to be a stubborn challenge for hospitals despite implementation of standardized risk assessments and
interventions. Falls are the leading cause of both fatal and non-fatal injury among older adults.
Problem
Despite implementation of a fall prevention program comprised of recognized fall reduction strategies, the hospital saw
a 23% increase in total falls for 2011.
Goals
Reduce patient falls in the inpatient setting through innovation and education to a rate below a 2.00 by the 2nd Quarter,
2012.
Methods
Elemental methods of performance improvement were employed:
• Sample identified
• Data collection tool implemented
• Data analysis conducted
• Prioritization using modified Pareto Principle
• Pilot project begun
• Measure against goal
• Expand initiative throughout the hospital and continue to monitor
Despite implementation of a fall prevention program comprised of recognized fall reduction strategies, the hospital saw
a 23% increase in total falls for 2011. Although falls with injury were well below the 50th percentile for NDNQI, the
hospital theorized that either new strategies were needed or those strategies already in place required better
implementation. A deep dive into the data led the hospital to pursue both of those options; so an innovative approach to
fall risk was combined with meticulous implementation of already existing strategies.
Because the hospital uses the NorMet Patient Falls Debriefing Tool, a detailed look back at each fall in 2011 was
possible. Analysis showed that falls in two categories of "fall related factors" accounted for 37% of falls. These fall
related factors, falls related to toileting and falls with bed alarm in place, became the priorities.
A Rainbow Innovation Pilot: In March, 2012 a pilot was implemented in which patients who were assessed as not
aware of their limitations and unlikely to follow direction, were given a Rainbow Colored wristband instead of the
usual green wristband for patients at high fall risk. These were the patients who tended to fall while toileting; they were
not to be left unattended while toileting.
Quality Symposium 2012
Page 25
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Robust implementation of bed alarms: 14% of falls occurred even though the patient was on a bed alarm. Drill down
revealed that the functionality of bed alarms was adequate, but user proficiency was not. Staff did not have a good
understanding of the nuts and bolts of physically using the alarms. For example, is the 3-second delay set? Is the
volume appropriate? Has the alarm auto-silenced? Is the correct bed alarm associated with the correct bed number? A
detailed, hands-on education and competency assessment was conducted for each RN and Nursing Assistant. Required
documentation was enhanced. Nursing Assistants were provided with their own "status board" so that they would know
at all times which patients had bed alarms.
Results
Rainbow Innovation Pilot (one nursing unit):
• March, 2012 prior to implementation, the fall rate was 5.59.
• Fall rate after implementation: April: 0.0; May: 1.45; June: 2.87; July: 0.0; August: 1.45.
Bed Alarm Implementation Education:
• Enhanced education, competency assessment and documentation began in January, 2012.
• Hospital-wide, the fall rate has decreased from 2.81 in January, 2012 to 0.96 in August, 2012.
Conclusions
• Use of a detailed post fall debriefing tool supplies the data needed for prioritization.
• Reducing the risks associated with toileting reduces the falls rate. The Rainbow Band pilot will be expanded to the
rest of the hospital one nursing unit at a time. Results will be monitored.
• Proper bed alarm implementation requires meticulous education and documentation. Staff education related to fall
reduction strategies must be detailed and well communicated. We will continue to make this education an integral part
of nursing competency.
Quality Symposium 2012
Page 26
Fall Rate Per 1000 Patient Days
5.00
4.50
Bed Alarm
Competency
4.00
Fall Risk
Assessment
documentation
3.50
3.00
2.50
Data Analysis
and Prioritization
2.00
1.50
Fall Pilot 5N
1.00
0.50
0.00
Jan- Feb- Mar- Apr- May- Jun- Jul- Aug- Sep- Oct- Nov- Dec- Jan- Feb- Mar- Apr- May- Jun11
11
11
11
11
11
11
11
11
11
11
11
12
12
12
12
12
12
--- Median
Quality Symposium 2012
Page 27
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Increasing Compliance with VTE assessments to Prevent Nosocomial DVT
Sharon Doyle-Hennessy, RN MS; Lorraine Bachman, RN
Lawrence Hospital Center
Introduction
Venous thromboembolism is the third most common cardiovascular illness after Acute Coronary Syndrome and
Stroke. It is believed that approximately 1 million cases of VTE are diagnosed each year in the United States. Risk
factors may be either hereditary or acquired. Although we may not be able to control for hereditary factors, we can
identify acquired risk factors such as immobilization, surgery, trauma, cancer and medical illness that place patients at
risk for developing VTEs. Identifying these risk factors and being proactive in treating these patients should decrease
morbidly and mortality related to preventable VTEs.
Problem
DVT is a life threatening illness that can lead severe morbidly and mortality and extended length of stay. Patient safety
is the focus of this project because early identification of risk category would lead to appropriate prophylactic
treatment and management. A DVT protocol had been developed but compliance with using the assessment was not
consistent. In addition, many patients were treated based on physician's clinical judgement, without the evidence of a
documented assessment.
Goals
• Identification of patients at moderate and high risk utilizing a standardized assessment
• Appropriate pharmacological prophylaxis and management
• Identification of patients with contraindications - appropriate mechanical prophylaxis ordered
• Decrease the number of preventable nosocomial DVTs
Methods
• Built a standardized VTE assessment originally on paper and subsequently in the EMR.
• Standardized order sets with appropriate treatment based on risk category.
• Built hard stops into documentation such as history and physical, progress notes and brief post op notes.
• Education to physicians and nursing staff on assessment and DVT prevention.
• Review of all positive nosocomial DVTs including readmissions within 30 days--if medical care was deemed
inappropriate--referred to Medical Peer Review.
• SCIPS concurrent reviewer for all surgical procedures--focused on VTE prophylaxis and appropriate treatment.
• VTE concurrent reviewer--focused in on Critical Care and Oncology.
Results
April 2011: Assessment rate was 14%; September 2012: Assessment rate is 75%
Conclusions
More work is required for monitoring and education of physicians for compliance with documentation. Many
physicians are bypassing the written assessment, and just ordering the prophylaxis. Realistically, not all DVT's are
preventable, but it is critical to patient safety to provide the appropriate assessment to identify risk, and then to provide
appropriate prophylaxis and management.
Quality Symposium 2012
Page 28
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Eliminating Non-Medically Indicated Deliveries before 39 weeks Gestational Age
Lisa Hanrahan, RN MSN CPHQ CPHRM; Sharon Doyle-Hennessy, RN MS
Lawrence Hospital Center
Introduction
Nationally, elective induction and cesarean-section rates have increased steadily over time. Multiple research studies
indicate that elective deliveries prior to 39 weeks carry significant risks of neonatal complications, even between 37-39
weeks gestation. There is still an increase in non-medically indicated deliveries despite current guidelines by the
American Academy of Obstetricians Gynecologists (ACOG). Several regulatory agencies, payers, and state quality
organizations have undertaken initiatives to decrease non-medically indicated inductions and c-sections prior to 39
weeks.
Lawrence Hospital Center was chosen as a satellite site for a study with a regional ACOG chapter to decrease the
number of non-medically indicated deliveries before 39 weeks and improve documentation of indications for early
delivery. The relationship is significant in that it provides the perspective of a community hospital with private patients
of a voluntary medical staff. Challenges specific to institutions with all voluntary medical staff include:
• Office versus hospital schedule
• Patients' desire to deliver with a single specific private physician
• Maternal intolerance to late pregnancy
• Logistics such as maternal distance from the hospital
• Physician concern regarding maternal perinatal morbidity, including shoulder dystocia and increased c-section rate at
night
Problem
This Community Hospital was not unique in patient and medical staff concerns with the above noted challenges.
Compounding the issue was a relatively high cesarean section rate of approximately 50%. While scheduled procedure
prior to 39 weeks accounted for only 11 percent of total deliveries, indications were not well documented. Baseline
data collected identified that of the total number of scheduled procedures between 36 and 38.6 weeks, 73.8% of these
were at 38 weeks gestation. Small changes in scheduling and documenting medical indications could yield significant
improvements.
Goals
The project goal is to reduce elective deliveries prior to 39 weeks with non- medically acceptable indicators to zero.
This would also yield a reduction in the overall rate of elective deliveries prior to 39 weeks. Objectives include
improving the documentation of medical indication for delivery to those identified by the National Quality Forum
(NQF).
Methods
• Baseline data was collected and an analysis presented to medical staff
• Policy for scheduling elective c-sections and inductions was implemented based upon NQF approved indications for
medically indicated elective delivery
• Scheduling process requiring hard stop or medical review for non-medically indicated c-sections prior to 39 weeks
Quality Symposium 2012
Page 29
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Rigorous review of all scheduled c-sections for EDC and indication
• Feedback to physicians regarding performance, outcomes, and documentation
• Information on elective delivery prior to 39 weeks including in patient materials during hospital tours and childbirth
education classes
• Documentation of medical indication hardwired into electronic medical record
Results
• Continued performance improvement by physicians in documentation of medical indication
• Improvement in documentation of indication at the time of scheduling
• Opportunity for improvement was focused on a very small group of physicians with limited hospital volume
• While the volume of non-medically indicated deliveries is decreasing appreciably, the overall rate gains have not
been realized due to the decrease in the denominator of number of procedures.
Conclusions
• Administration directive for evidence based practices
• Department Chairman was champion for change and engaged most of the obstetric physicians
• Education on the policy for both physicians and nursing staff
• Education to the patients regarding avoidance of elective early delivery
• Open communication is key between administration, physicians and nursing
Quality Symposium 2012
Page 30
Eliminating Non-Medically Indicated Deliveries before 39 weeks Gestational Age
Percent of Scheduled Procedure Prior to 39 Weeks
25%
20%
15%
10%
5%
0%
Jan-12
Feb-12
Mar-12
Apr-12
% scheduled procedure < 39 weeks
May-12
Jun-12
Baseline Sept- December
Percent of Scheduled Procedure Prior to 39 Weeks
Without Documented Indication
45%
40%
35%
30%
25%
20%
15%
10%
5%
0%
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
% of Procedures w ith no documented indication
Baseline Sept- December
Quality Symposium 2012
Page 31
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Reducing Central Line Infections in the ICU - Challenges for the Community Hospital
Mary Ann Hauff, RN (Director of Infection Control); Barbara Choy, RN (Nurse Manager Critical Care); Rose
Ann O'Hare, RN (Vice President Patient Care Services)
Lawrence Hospital Center
Introduction
Despite widespread adoption of checklists and other best practices aimed at preventing Central Line Associated Blood
Stream Infections (CLABSIs), the CDC estimates that "41,000 central line-associated bloodstream infections
(CLABSI) occur in U.S. hospitals each year. These infections are usually serious infections typically causing a
prolongation of hospital stay and increased cost and risk of mortality."
Problem
The Hospital began to implement the Central Line Insertion Checklist in 2009 and monitored its use. Despite a
successful implementation, surveillance revealed a higher than expected rate of CLABSIs.
Goals
The goal is to reduce the CLABSI rate in the ICU to below the NHSN pooled mean by implementing best practices for
Central Line maintenance by the end of 2012.
Methods
Thorough review of the data and observation of the practice in ICU was conducted. It was established that insertion
was not the point at which the infection began. The conclusion to be drawn was that the insertion checklist was
functioning as expected. The infections that were being seen were attributed to maintenance of the line and the work to
be done would focus on maintenance practices.
In March, 2012, a multidisciplinary team began to meet to conduct a gap analysis of current practice to established best
practices. Gaps were identified and the following steps were taken:
• Decrease central line days: It quickly became apparent that the first strategy would be to decrease the length of time
central lines remained in patients. To further that, the Nurse Manager consults with each Nurse caring for a patient with
a central line to discuss the rationale for continuing the line. If there is not a strong rationale (for example, patient
receiving vasopressors), the physician is contacted and asked for an order to discontinue the line.
• The dressing change practice was reviewed. The Vice President of Patient Care Services, who had made elimination
of CLABSIs an overriding priority, met with nurses individually to ensure that they were following the proper
technique for a sterile dressing. Nurses received the message that leadership was strongly committed to this initiative.
• The Nurse Educator and the IV Nurse created a video demonstrating proper central line maintenance practices. All
ICU nurses were required to view the video.
• Use of Biopatch was mandated for all central line dressing changes.
• Patients were bathed daily using chlorhexedine bath towels. Wash basins were eliminated.
• The Nurse Manager checks each central line each day to confirm that it is secure and the dressing is intact.
• The Nurse Manager reviews the infection statistics with the Nurses making it clear to them that they are
stakeholders in the outcomes.
• A new central line product, impregnated with antimicrobials, was put into use.
Quality Symposium 2012
Page 32
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Alcohol impregnated caps were instituted for ports. Scrub the hub policy was reinfo.
• Blood drawing from ports was only permissible in cases where no other access was available.
• Femoral lines were not permitted except in cases where there was no other access. An Occurrence Report is
generated and reported to Quality Management for each femoral line insertion.
• Suturing of lines was discouraged. Instead, securement devices were put into use.
Results
In 2011, the ICU annual CLABSI rate was 5.7. Since the initiative began in March, 2012, there have been 0 Central
Line Associated Blood Stream Infections in the ICU.
Conclusions
While the Insertion Checklist is effective in preventing CLABSIs which occur as a result of insertion technique, when
central lines remain in patients for longer periods of time, meticulous maintenance is the key to prevention of
CLABSIs. Leadership involvement can motivate and engage staff. When staff see themselves as stakeholders in a
process, that ownership translates to better outcomes.
Quality Symposium 2012
Page 33
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Reducing Utilization of Intravenous Hydromorphone at a New Community Hospital
Huong Le, PharmD BCPS; Echefula Agbara, PharmD RPh
Methodist West Houston Hospital
Introduction
Opioid analgesics remain the cornerstone of pharmacologic management of acute and chronic pain in hospitalized
patients. However, the serious adverse effect profiles of opioids require a balance between an aggressive pain
management strategy and the reduction of these side effects. One synthetic opioid which illustrates the difficulty with
reaching this balance is hydromorphone. Hydromorphone is a potent morphine derivative indicated for moderate to
severe pain such as burns and other extremely painful conditions. Although hydromorphone has been in use for many
years, many misconceptions still exist between it and morphine, its parent drug. Practitioners often underestimate the
potency of hydromorphone, resulting in adverse consequences in many hospitalized patients. In fact, in 2006 the
Institute for Safe Medication Practices (ISMP) Canada noted that hydromorphone ranked third on their list of drugs
most frequently reported as causing harm [1,2].
Problem
Increased intravenous (IV) hydromorphone utilization was first observed in the Pharmacy Department as a result of
increasing purchases in 2011 and from reports by bedside nurses that hydromorphone was the primary pain product
being used by the majority of their patients. Physicians discharging the patients found it difficult to wean their patients
off of intravenous pain medications, specifically hydromorphone. Furthermore, Adverse Drug Reaction (ADR) reports
began surfacing consisting of patients who were on hydromorphone experiencing increased drowsiness, lethargy, and
even respiratory depression requiring usage of reversal agents.
After all reports were gathered and analyzed, two isolated problems concerning hydromorphone were identified. First,
patients were entering the facility requesting hydromorphone over any other pain medication. The number of patients
presenting to the Emergency Department (ED) seeking pain medications stating that only hydromorphone work or that
they were allergic to morphine was becoming overwhelming. The financial and labor costs were becoming
unmanageable considering the cost of testing and treating the vague symptoms reported by the patients. Second,
physicians who were ordering hydromorphone for patients did so discordantly with its official dosing indications, often
times ordering excessively high doses for patients.
Goals
Hydromorphone in itself is an effective medication for pain if used within the appropriate settings. It has many
advantages such as less hemodynamic side effects, higher potency than morphine, and less adverse effects in renal
impairment. Medication safety is compromised when providers underestimate its potency and do not closely follow the
patients’ responses to a high-potency opioid, especially when given to patients who are opioid-naive. Additional
patient co-morbidities such as sleep apnea, chronic obstructive pulmonary disease, congestive heart failure and renal
disease may further obscure patient responses to opioids. However, there are safety measures that can be undertaken
prior to initiating a patient on IV hydromorphone. The following goals were identified to encourage and ensure safe
hydromorphone use:
1. House wide education on appropriate equianalgesic dosing among morphine, hydromorphone, and various other
Quality Symposium 2012
Page 34
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
opioids.
2. Minimize higher doses (>1 mg) of hydromorphone as the initial dosage unless the patient has a pre-existing comorbidity requiring chronic pain management.
3. Encourage initiating patients on less potent opioids, such as morphine, as the initial drug of choice in pain
management when appropriate.
4. Differentiate and educate between true allergy versus pseudo-allergy when patients have a documented history of
morphine allergy.
5. Avoid all types of ADRs involving hydromorphone usages.
Methods
Methodist West Houston Hospital opened in December 2010 and is a growing acute care hospital specializing in
oncology, cardiology and cardiac surgery, neurology and neurosurgery, orthopedics, sports medicine, women and
children’s services and robotic surgery. Based on concerns and recommendations expressed by several medical staff
committees, including Pharmacy and Therapeutics (P&T) Committee and Utilization Review, the hospital started
investigating the issue of excessive hydromorphone usage in mid 2011 and adopted the challenge as an ongoing project
in the Research and Practice Council of Shared Governance Committee. Aside from the increasing utilization, the
hospital also uncovered physician prescribing practices that were contributing to this problem, primarily by not
adhering to approved dosing indications and guidelines. Also, conversations with physicians at committee meetings
revealed that the surrounding community hospitals were experiencing similar issues. Thus, the following actions were
applied to gather more information about hydromorphone usage patterns in order to reduce the amount of inappropriate
hydromorphone utilization:
1. Communicated with nearby hospitals regarding similar hydromorphone inappropriate usage patterns and their plan
of actions
o One of the actions taken by a hospital within the Methodist system included posting a “No Dilaudid” sign within
the patient care rooms in the ED (Figure 1). As a result of that sign, hydromorphone use at that hospital dramatically
decreased in the ED, which is commonly the entry point for patients who seek hydromorphone.
2. Attended various medical staff meetings and inquired physicians’ feedback and guidance on hydromorphone usage
patterns at Methodist West Houston Hospital (MWHH).
o Various suggestions were brought forth by the physician members to help prevent high-dose hydromorphone
orders which could potentially result in a patient overdose. One suggestion included re-evaluating all of MWHH
Computerized Physician Order Entry (CPOE) order sets which contained hydromorphone dosing options that were
greater than 1 mg and removing them. This would minimize physicians choosing any dosing boxes more than 1 mg
hydromorphone. The same actions were applied towards the menu for general dosing of hydromorphone. Electronic
hydromorphone dose menu consisting of check boxes for doses of 0.2 mg, 0.5 mg, 1 mg, 2 mg, 4 mg, and 6 mg were
changed to 0.2 mg, 0.25 mg, 0.5 mg, and 1 mg. Any dose higher than 1 mg would require a conscious manual entry by
the physician. The hospital went a step further in the ED to remove all hydromorphone syringes >1 mg out of the Pyxis
dispensing system. Concurrently, the pharmacy department also generated reports of hydromorphone usages in the ED
to the ED medical director and the director of nursing to track and trend the volume and number of doses used on a
weekly basis.
o Pharmacy also completed a medication usage evaluation (MUE) to determine top prescribers in the hospital and
used this information to schedule one-on-one counter-detailing sessions with identified prescribers. In addition, one of
the conversations included the critical care physician so that hydromorphone would be discouraged as routine use in
the ICU for pain management. The conversations were well received; however, the feedback was that the patients were
Quality Symposium 2012
Page 35
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
requesting hydromorphone as preferential pain medication. This became apparent when patients requested to couple
their hydromorphone with a cocktail of promethazine and diphenhydramine injections.
3. Various postings on online pharmacy forums and listserv also echoed similar hydromorphone dilemmas. Some
hospitals developed an opioid conversion chart of hydromorphone to be posted in the nursing units as part of hospitalwide education.
o Our next step was to raise the awareness of equianalgesic doses of 1 mg IV hydromorphone compared to other
common opioids. An equianalgesic poster was created and posted throughout the main adult nursing stations including
the ICU, ED, and Medical/Surgical wards. Conversations during daily interdisciplinary rounds were used to reinforce
an understanding of the 1:7 conversion ratio of hydromorphone to morphine.
4. An opioid decision algorithm guideline to use for patients with morphine allergy.
5. Attended an ISMP webinar in December 2011: “Hydromorphone: Taking Aim at Events Under the Radar”.
o Based on postings from various hospital forums and listserv, including the newsletter for the ISMP, it was obvious
that misuse of hydromorphone in the inpatient setting is not an uncommon dilemma nationwide. Coincidentally, the
ISMP offered a webinar in which it discussed various processes and actions other hospitals were undertaking regarding
their hydromorphone usage. Nursing leadership members and physicians were invited to attend the webinar during
December 2011.
6. Monitored weekly reports of hydromorphone utilization in the ED.
o The pharmacy department communicated weekly hydromorphone usage reports to the ED medical staff to ensure a
continuous monitoring of hydromorphone increase or decrease usages in the ED.
7. A follow-up retrospective hydromorphone MUE was performed on a sample of MWHH patients in order to better
understand practice patterns for hydromorphone at our hospital. The results showed the following:
• In over 500 patient visits extracted:
o Over 50% of the hydromorphone orders were 1 mg, making that the most common dose. Twenty-two percent of
the orders were greater >1 mg.
o The most common frequency ordered was every 4 hours (43%); However, every 2 and every 3 hours combined
were even more common than every 4 hour frequency.
• Fifty patients with > 1 mg IV hydromorphone orders were randomly selected for evaluation:
o Only 52% of the patients had prior morphine orders and/or less than 1 mg IV hydromorphone orders, indicating
that multiple physicians did not trial the patient on a less potent narcotic (i.e. morphine) or lower hydromorphone dose
(< 1 mg) as the initial order. In addition, for patients that did have morphine orders, most of them ordered <4 mg,
possibly indicating an under dosing of morphine.
o Only 24% of the patient visits had diagnosis or co-morbidities (sickle cell, cancer, and motor vehicle accidents)
which may warrant chronic pain management requiring higher IV hydromorphone doses. Thus, the majority of the
patients (76%) had >1 mg IV hydromorphone orders without any of the above mentioned diagnoses that would warrant
initial high dose hydromorphone orders.
o Over 50% of the patients had sleep apnea or obesity; both of these factors are associated with respiratory
depression when a patient is on concurrent opioids, including hydromorphone.
o Of the 50 patients evaluated, 14% were over the age of 60, in addition to having sleep apnea and/or obesity, all of
which are associated with respiratory depression. These patients are especially in need of initial lower dosing of IV
hydromorphone (i.e., <1 mg).
The results of the MUE were presented at several medical staff meetings (i.e., P&T, CAG, Patient Care Committee) as
educational opportunities on actual hydromorphone practice trends at MWHH versus recommended best practice for
Quality Symposium 2012
Page 36
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
our patients.
Results
Hydromorphone utilization numbers were also being tracked on a monthly basis for the ED, ICU, and
Medical/Surgical wards. Figure 2 illustrates a decrease in hydromorphone usage across the units from April 2011 to
July 2012. Hydromorphone utilization and hydromorphone total amount in milligrams adjusted for Equivalent Patient
Days (EPD) are also represented. As hospital census increased rapidly, one would expect to have all medication use
increase. However, Figure 2 demonstrates that despite the rise in patient census, our hydromorphone utilization
gradually subsided throughout the year, both in utilization per EPD and total amount milligrams per EPD.
In addition, occurrences of hydromorphone related ADR events became minimal. In 2011, there were three reported
ADR reports related to hydromorphone. After extensive hospital-wide education, revisions of policy and procedure,
and positive reinforcements, the last reported hydromorphone related ADR occurred in October 2011, and none have
occurred since then.
As for the dilemma of patients with stated morphine allergy and could only tolerate hydromorphone, the opioid allergy
decision algorithm was created to address that issue. However, the document was approved guideline, not as a policy.
But the management of patients who were demanding and insisting on hydromorphone proved to be extremely
difficult. It was initially thought that creating a hospital policy would assist in filtering out those patients with pseudoallergies, but the true resolution was to empower hospital staff, as the patients’ care providers, and to hold them
accountable for their medication orders.
Conclusions
Hydromorphone related medication incidents have contributed to many medication errors throughout the nation.
Whether the root cause was due to its look-alike sound-alike with morphine, underestimation of its potency, or the lack
of understanding of its dosing indications, hydromorphone has been marked as being the culprit of causing patient
harm. It has also gained enough reputation within the community to become many patients’ medication of choice for
acute pain control. These same issues were observed, investigated and addressed at MWHH.
At times, MWHH experienced an excess number of patients arriving at the ED only to request hydromorphone. Care
for these patients resulted in unnecessary healthcare resources utilized such as additional treatments and tests, as well
as labor resources. Realizing that many patients were aggressively demanding hydromorphone upon ED entry, team
effort focused on methods to minimize patient exposure to this drug as well as other high potency opioids. Because
pain management remains a patient-centered topic that requires prompt attention, consideration was given to the legal
risk of poorly managed pain and the potential for true allergic reactions in patients with stated morphine allergies.
Based on the results of the hydromorphone MUE, over 50% of patients’ morphine allergies did not have documented
serious reactions. Thus, certain patients who decline alternative pain agents to specifically request for hydromorphone
may just require a simple, firm answer of “no”. The hospital empowered the physicians to respond “no” to the patient
for hydromorphone requests when it was clearly medically inappropriate, which helped prevent the return of
hydromorphone seeking patients.
As a new community hospital, setting the culture by establishing open communication across the disciplines from the
beginning will help position the path for the future. The decrease in overall hospital usage of hydromorphone is a result
of effective interdisciplinary action. Talking directly with physicians not only helps establish rapport, but is also
Quality Symposium 2012
Page 37
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
effective in attracting their attention to safety matters which may require modification of practices. The conversations
regarding hydromorphone usage were initiated not only from pharmacists and nurses, but also case management, riskmanagement staff and additional personnel involved in discharge planning. A team centered approach helped MWHH
minimize usage of a high-abuse opioid medication.
Quality Symposium 2012
Page 38
ED
ICU
Med-Surg
Util/EPD
Mg/EPD
Apr
104
100
221
0.30
0.28
May
161
21
549
Jun
155
11
459
0.40
0.37
Jul
119
50
422
0.34
0.33
Aug
142
9
270
0.27
0.26
Sept
136
22
610
0.18
0.17
Oct
97
24
352
0.31
0.24
Nov
72
32
333
0.16
0.12
Dec
93
50
439
0.16
0.18
Jan-12
93
40
349
0.20
0.17
0.16
0.16
Feb-12
120
29
453
Mar-12
111
46
608
0.19
0.18
Apr-12
73
17
350
0.18
0.18
May-12
72
15
339
0.11
0.11
0.11
0.10
Jun-12
68
17
409
Jul-12
61
26
363
0.13
0.12
Total
1616
483
6163
0.11
0.11
Figure 2: Hydromorphone usage per EPD
Total
dispenses
900
0.45
800
0.40
700
0.35
600
0.30
500
0.25
400
0.20
300
0.15
200
0.10
100
0.05
0
Per EPD
0.00
Apr
May
Jun
Jul
Aug
Sept
ED
Oct
ICU
Nov
Med-Surg
Dec
Jan-12
Util/EPD
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Jul-12
Mg/EPD
Quality Symposium 2012
Page 39
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Evolution of Montefiore Medical Center Falls Prevention Program
Jane O’Rourke, RN DNP NEA-BC; Patty Zyloney, RN MSN; Lois Alfieri, RN MSN; Amisha Rai, PA; Maryrose
Defino, RN MS CPHQ; Mary Tesoro, RN-BC DNS; Maryanne Schmid, RN CPHQ; Erica Schmidt; Jason
Adelman, MD; Michael Bogaisky, MD
Montefiore Medical Center
Introduction
Montefiore Medical Center is dedicated to patient safety and recognizes the need for an interdisciplinary team to
minimize patient falls. The Falls Prevention Team identified the value in re-evaluating our program. The process
revealed the need to utilize a validated tool to assess fall risk as an initial step in this programmatic revision.
Problem
To evaluate Montefiore Medical Center’s Falls Prevention Program and identify opportunities for improvement using
evidence-based best practices. Montefiore Medical Center in the Bronx, New York is a multi-campus facility providing
primary, secondary, tertiary and quaternary levels of care. We serve a culturally diverse population of 1.4 million and
have 1500 acute care beds providing treatment to patients with complex medical needs. Given this high volume/high
risk patient population, initiatives for strengthening our Fall Prevention Program were explored.
Goals
1. To decrease the number of falls and falls with injury in Montefiore Medical Center.
2. To implement a comprehensive program which will improve our patient fall risk assessments, promote use of
appropriate patient specific fall prevention interventions, and increase staff awareness of patient fall prevention
initiatives.
Methods
1. Collaboration between Patient Safety, Nursing and Quality Management
2. Retrospective study using chart reviews of patients who fell in 2011
3. Descriptive analysis of all falls occurring in the Moses, Weiler & Children's Hospitals, Montefiore Medical Center
4. Initiated an electronic query to identify all patients who fell in 2011.
5. 1,225 inpatient falls were identified
6. Reviewed and analyzed 1,225 medical records for:
a. fall risk assessment prior to fall
b. fall event on post fall form, nursing provider progress notes
c. associated variables including age, time of fall, activity relating to fall, and National Database of Nursing
Quality Indicators (NDNQI) injury level & harm scale
7. Calculation of Montefiore fall tool sensitivity and specificity
8. Use of Youden Index score to compare Montefiore fall risk assessment tool with other validated tools (Youden
Index reflects both tool sensitivity and specificity)
9. Review of ECRI survey results to identify hospital staff perceptions of Montefiore’s current fall prevention program
(ECRI is Montefiore Patient Safety Organization)
Results
Quality Symposium 2012
Page 40
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
1. Montefiore 2011 fall rate = 3.14 (1,000 patient days)
2. Moses and Weiler aggregate sensitivity = 94.1%
3. Moses and Weiler aggregate specificity = 19.5%
4. Moses and Weiler aggregate Youden Index = 13.6% (0.136)
See Table 1 and Charts 1, 2 and 3
Conclusions
1. The high sensitivity score indicates that our tool correctly identified most of the patients who fell.
2. Our falls risk tool had low specificity. As a result, it incorrectly labeled 81% of patients who would not fall as being
at risk for falls.
3. The Youden Index score showed that the Montefiore Falls Risk Tool is inferior to other validated falls risk
assessment tools, such as the Morse Falls Scale.
4. ECRI survey results reveal 71% of the hospital staff surveyed felt that falls awareness was effective.
5. The following intervention strategies were identified and selected for implementation in the Montefiore Fall
Prevention Program:
a. Use of the Morse Falls Scale
b. Implementation of patient-centered fall prevention strategies linked to patient-specific risk factors
c. Migration to an electronic documentation system
d. Improved education of hospital staff regarding their role in the fall prevention program
e. Utilization of a nursing outcome-based model to structure the fall prevention program
f. Continued comparison of Montefiore fall rates to NDNQI benchmarks
Quality Symposium 2012
Page 41
Quality Symposium 2012
Page 42
Quality Symposium 2012
Page 43
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Impact of Dementia on Common DRG Hospitalizations in the United States: 2000-2010
William Liao; Suh H. Lee, BS; Robert Y Lin, MD
New York Downtown Hospital
Introduction
Dementia is a common affliction in the elderly. While dementia has a known societal impact in terms of care-giver and
custodial resource expenditures, the role of dementia in hospital utilization characteristics has not been well described.
Defining this impact has particular relevance, since with the increasing proportion of elderly In the United States, nonsurgical medical hospitalizations hospitalizations are now predominantly geriatric.
Problem
While the prevalence of dementia in hospitalizations has been estimated to be as high as 43% in some reports, the
effect of dementia on key hospitalization utilization characteristics is not known. Understanding the independent
contribution of dementia on hospitalization length of stay and the ability to be discharged home has important and
obvious economic implications.
Goals
1. To identify types of hospitalizations in which dementia diagnoses are prevalent in the United States for recent years.
2. To quantify the independent contribution of a dementia diagnosis to hospitalization length of stay and the ability of
the patient to be discharged home
Methods
The National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP) datatbases for the years
2000-2009 were queried for patients who had any of three ICD9 dementia codes (331.0 Alzheimer's disease, 294.1
dementia classified elsewhere and Alzheimer's disease type dementia, and 290.* dementias). The most frequent
medical DRG's associated with dementia codes were identified. For each of the frequent DRG hospitalizations,
multivariate modeling was performed using length of stay and discharge to home as dependent variables. Independent
variables included ICD9 codes for common clinical disorders, dementia coding and demographic factors. Stepwise
selection was used to enter significant predictors. Modeling was performed taking into account variability in race
coding (missing in 14-27% of hospitalizations depending on year), injury coding for falls, and redundancy between the
DRG and ICD9 coding (potential collinearity).
Results
The most frequent non-surgical DRGs associated dementia coding were septicemia without prolonged mechanical
ventilation, kidney & urinary tract infections, simple pneumonia & pleurisy, respiratory infections and inflammations,
congestive heart failure, intracranial hemorrhage and stroke with infarction chronic obstructive pulmonary disease and
asthma. Dementia was a significant predictor of increasing length of stay for all DRG categories for all years of the
study. There tended to be a higher coefficient in later years especially kidney & urine tract infection DRG
hospitalizations, consistent with a stronger influence on length of stay. In logistic regression predictor models for
discharge to home (excluding palliative transfers and in-house expiration), dementia was a consistent significant
predictor of not being discharged home in stroke, asthma and pneumonia DRG hospitalizations but not for respiratory
infections and inflammations DRG hospitalizations. For all the later years of the study dementia was a significant
Quality Symposium 2012
Page 44
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
predictor of not being discharged home in kidney & urinary tract infections DRG hospitalizations. In the earlier years
of the study, dementia coding did not have a significant predictor effect for not being discharged home in congestive
heart failure DRG hospitalizations. However, during the latter years of the study, dementia coding was a significant
predictor. Modeling accounting for redundancy between the DRG and the ICD9 coding, with and without race factors,
and excluding patients where a fall was documented did not significant alter these findings.
Conclusions
After adjusting for many clinical and demographic factors, the presence of dementia as a coded diagnosis has a
significant effect on length of stay and the ability of hospitalized patients to be discharged home in common DRGs.
The effect may be increasing in kidney & urinary tract infections DRG hospitalizations. The ability to be discharged
home also appears to have been affected by dementia more in recent years for congestive heart failure DRG
hospitalizations. Dementia has a quantifiable impact on hospitalization utilization parameters, that needs to be
addressed in reimbursement strategies. We hypothesize that the presence of dementia influences clinical decisions of
whether or not to hospitalize patients with certain disorders because of perceived uncertainty relating to meeting
patients' long term care-taker needs. For some patients with dementia, hospitals may represent critical interventions not
because of medical severity but because they allow for a gathering of multiple disciplines to gather and decide on the
appropriate disposition for a patient including the option of long term care. This has implications in the justification of
payors' gatekeeper policies that soley rely on medical necessity for approving hospitalization payment.
Quality Symposium 2012
Page 45
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
You Can Get There From Here: One Hospital's Continuing Meaningful Use Journey From Stage 1 to
Stage 2
Ken Ong, MD MPH; Phil Myones, MS; Cathy Suspenski, MPA; Teresa McCormack, MHS; Geeta Natashi, RN
MSA; Stephen Rimar, MD MBA; George F Heinrich, MD
New York Hospital Queens
Introduction
New York Hospital Queens successfully attested to Stage 1 of Meaningful Use in May, 2012. However, its Meaningful
Use journey has only begun. CMS released the final rule making changes to Stage 1 and the new Stage 2 measures.
Problem
As of this writing only 27 percent (1,333 of 4,985) of U.S. hospitals have attested to received Medicare incentives for
Stage 1. In New York State, 23% (47 of 204) have received Medicare incentives. The total number of MU objectives
for hospitals is 19 for both Stage 1 and 2. The meaningful use objectives require substantial investments in resources
and funding to install and maintain healthcare information technology in a challenging time for acute care hospitals.
Nonetheless, some changes to Stage 1 take place immediately, others are optional in 2013 but required for 2014 and
Stage 2. No matter what stage providers are attesting to in 2014, all must use 2014 certified EHR technology. In
response comments to the NPRM, the reporting period in 2014 will be 3 months, regardless of stage.
Goals
1. Adopt the Final Rule's modifications to the Stage 1 measures to report compliance with year 2 in 2013.
2. Develop a plan to achieve Stage 2 within Federal Fiscal Year 2014.
Methods
The final rule makes some changes to Stage 1 immediately, other changes are optional in 2013 but required for 2014
and Stage 2. No matter what stage providers are attesting to in 2014, all must use 2014 certified EHR technology. In
response comments to the NPRM, the reporting period in 2014 will be 3 months, regardless of stage. The Stage 1 and 2
measures and thresholds follow:
Core Objectives
1. CPOE: Stage 1 - >30% medications; Stage 2 - >60% medications, >30% laboratory, & 30% radiology
2. Demographic: Stage 1 - >50%; Stage 2 - >80%
3. Vital Signs: Stage 1 - >50%; Stage 2 - >80%
4. Smoking Status: Stage 1 - >50%; Stage 2 - >80%
5. Clinical Decision Support: Stage 1 - 1 intervention; Stage 2 - 5 interventions
6. Labs: Stage 1 - >40%; Stage 2 - incorporate >55%
7. Patient List: Stage 1 & 2 - Generate at least one patient list by specific condition
8. eMAR with assistive technology: Stage 2 - >10%
9. Patient Access: Stage 1 - 50% e-copy: stage 2 - >50% can view, download, or transmit (VDT) & >5% actually VDT
10. Patient Education Resources: Stage 1 & 2 - >10%
11. Medication Reconciliation: Stage 1 - >50% (menu); Stage 2 - >z0% (core)
12. Summary of Care: Stage 1 - >50% (menu); Stage 2 - >50% transitions of care, 10% electronically, and at least 1
Quality Symposium 2012
Page 46
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
different DHR vendor (core)
13. Immunizations: Stage 1 - One test; Stage 2 - Ongoing transmission
14: Reportable laboratory results: Stage 1 - One test; Stage 2 - Ongoing transmission
15. Syndromic Surveillance: Stage 1 - One test; Stage 2 - Ongoing transmission
16. Security Analysis: : Stage 1 & 2 - Required
Menu Objectives
1. Progress Notes: NEW for Stage 2: >30% unique patients
2. Electronic prescribing: NEW for Stage 2: >10% discharge medication orders
3. Imaging Results: NEW for Stage 2: >10% of imaging results
4. Family History: NEW for Stage 2: >20%
5. Advanced Directives: Stage 1 - ; Stage 2 - >50% patients 65 years or older
6. Labs: NEW for Stage 2 - Structured electronic lab results to Eps >20%
Clinical Quality Measures (15 required)
1. Emergency Department (ED)-1 Emergency Department Throughput – Median time from ED arrival to ED
departure for admitted ED patients
2. ED-2 Emergency Department Throughput – admitted patients – Admit decision time to ED departure time for
admitted patients
3. ED-3-Median time from ED arrival to ED departure for discharged ED patients.
4. Stroke-2 Ischemic stroke – Discharged on anti-thrombotic therapy
5. Stroke-3 Ischemic stroke – Anticoagulation Therapy for Atrial Fibrillation/Flutter
6. Stroke-4 Ischemic stroke – Thrombolytic Therapy
7. Stroke-5 Ischemic stroke – Antithrombotic therapy by end of hospital day two
8. Stroke-6 Ischemic stroke – Discharged on Statin Medication
9. Stroke-8 Ischemic or hemorrhagic stroke – Stroke education
10. Stroke-10 Ischemic or hemorrhagic stroke – Assessed for Rehabilitation
11. Venous Thromboembolism (VTE)-1 VTE prophylaxis
12. VTE-2 Intensive Care Unit (ICU) VTE prophylaxis
13. VTE-3 VTE Patients with Anticoagulation OverlapTherapy
14. VTE-4 VTE Patients Receiving Unfractionated Heparin (UFH) with Dosages/Platelet Count Monitoring by
Protocol (or Nomogram)
15. VTE-5 VTE discharge instructions
16. VTE-6 Incidence of potentially preventable VTE
17. AMI-2-Aspirin Prescribed at Discharge for AMI
18. AMI-7a- Fibrinolytic Therapy Received Within 30 minutes of Hospital Arrival
19. AMI-8a- Primary PCI Received Within 90 Minutes of Hospital Arrival
20. AMI-10 Statin Prescribed at Discharge
21. PC-01 Elective Delivery Prior to 39 Completed Weeks Gestation
22. PN-6- Initial Antibiotic Selection for Community-Acquired Pneumonia (CAP) in Immunocompetent Patients
23. SCIP-INF-1 Prophylactic Antibiotic Received within 1 Hour Prior to Surgical Incision
24.vSCIP-INF-2-Prophylactic Antibiotic Selection for Surgical Patients
25. SCIP-INF-9- Urinary catheter removed on Postoperative Day 1 (POD1) or Postoperative Day 2 (POD2) with day
Quality Symposium 2012
Page 47
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
of surgery being day zero.
26. Home Management Plan of Care (HMPC) Document Given to Patient/Caregiver
27. Exclusive Breast Milk Feeding Term Newborn
28. EHDI-1a - Hearing screening prior to hospital discharge
Results
In collaboration with our EHR vendor, we developed a project plan to enable compliance by the last quarter of Federal
Fiscal Year 2014 (see Attachment A).
Conclusions
Meaningful Use Stage 2 promotes the adoption of advanced clinical processes and builds on the foundation of Stage 1.
In particular, Stage 2 objectives include technology to improve individual and community health and lower costs:
• Improve transitions of care: Summary of care and structured laboratory results to physicians providing follow-up
care after hospital discharge. Medication reconciliation at time of admission.
• Improve medication safety: Electronic medication administration record with assistive technology, e.g. bar-code
medication administration; electronic discharge prescribing; and, CPOE's scope expanded to laboratory and radiology
orders.
• Patient engagement: Patient portals that provide patients the capacity to view, download, and transmit portions of
their health record.
• Improve care coordination and communication: Electronic physician progress notes; facilitated access to imaging
studies; and, patient lists by condition.
• Transmit syndromic surveillance, immunizations, and reportable laboratory results
Meeting Stage 1 required rigorous project planning, sufficient resources and finances. Achieving Stage 2 will require
commitment no less robust.
Quality Symposium 2012
Page 48
"!
%,"'! *
* *+ * +*#
,! )!* ,! (', ',), /((,
#* % ++ ,.(*$*-
" "!
,# ',(*,%
"$#" "0+##'(-& ',,#('
-*! *0', !*,#('
(', ',
* -+#('
* '! & ',
(#% )!*
%#'#%(*$+
Quality Symposium 2012
Page 49
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Efforts to Improve Insufficient Clinician Documentation of Significant Electrocardiographic Findings
in Adults Presenting to the Emergency Department with Dysrhythmias and/or Conduction Disorders
Nidhi Garg, MD; Alison Suarez, MD; Zuhair Ali, MD; Sanjey Gupta, MD
New York Hospital Queens
Introduction
ECG interpretation and documentation of dysrhythmias and/or conduction disorders may be critical for diagnosis,
treatment and continuity of care between services.
Problem
We sought to determine if documentation of ECGs was adequately captured in our electronic medical record (EMR)
and what factors may impact documentation.
Goals
To determine the rate of documentation of ECGs and compare it after brief intervention.
Methods
This study was performed in 2 phases at an Urban Level 1 trauma center with an annual ED visit of 95,000. Patients
<17 yrs or with normal ECG were excluded. In phase 1, a retrospective chart review was conducted ECGs obtained
during 11/1/07-12/31/07 were reviewed for the diagnosis and documentation of dysrhythmias and/or conduction
disorders. In August 2012, emails were sent reminding about improvement in EKG documentation. In phase 2, a
retrospective chart review was conducted and ECGs obtained during 10/10/12 -10/16/12 were reviewed for the
diagnosis and documentation of dysrhythmias and/or conduction disorders. Results were expressed in percentages and
STATA was used for analysis.
Results
Phase 1:
• 5,590 ECGs were reviewed. 1,797 were eligible for inclusion. In 491 (27%) patients, the EMR lacked
documentation of ECG findings.
Phase 2:
• 2,039 ECGs were reviewed. 130 were eligible for inclusion. In 38 (29.2%) patients, the EMR lacked documentation
of ECG findings despite increased reminders and awareness about ECG documentation.
Conclusions
We conclusion that e blast intervention might not be an effective method of intervention to promote increased
documentation. In addition, documentation may be affected by our institution-specific practice of "signing off" in real
time by health care providers' initials placed directly on the ECG. Another factor that nay have affected documentation
was our institutions' transition of EMR from First Net to All-Scripts in December of 2011.
Quality Symposium 2012
Page 50
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
ID Band Errors: A Serious Patient Safety Challenge
Laurie J Gordon, MA MD; Piyush Jain, MD
New York Hospital Queens
Introduction
Since 2002, the Joint Commission has published National Safety Goals. Every year, the primary goal has been to
improve the accuracy of patient identification using 2 patient identifiers. These patient identifiers appear on the patient
identification (ID) band. Many protocols concerning accurate identification use the information on the ID band for
verification of patient identity. The ID band needs to be on the patient and accurate, however, this is not always the
case. In a 1-year period, the United Kingdom National Patient Safety Agency documented 24,382 reports of patients
being mismatched to their care; 12% of the cases were due to ID band errors [1].
Problem
Many quality initiatives have focused on improving patient identification and assuring that staff use 2 patient
identifiers. There are few studies that have evaluated the accuracy of ID bands, specifically absent, illegible or
inaccurate ID bands. Hain et al [2] showed that ID band error rates can be reduced from 20.4 to 2.6% by a multifaceted
approach. The improvement can be sustained with continued auditing and staff education. In 2009, at the annual
Pediatric Hospital Medicine meeting, a collaborative was formed involving 6 hospitals with pediatric units, ranging
from community hospitals with pediatric units to children's hospitals. The collaborative aimed to learn from each other
to improve ID band accuracy across all 6 institutions. The data reported here is from New York Hospital Queens, one
of the 6 participating institutions.
Goals
1. To assess attitudes and barriers to accurate ID band use
2. To address the barriers to accurate ID band use
3. To reduce pediatric patient ID band error rate by 50% over one year
Methods
A voluntary, anonymous questionnaire was administered to employees who have contact with patients on each of the
clinical units (Pediatric Inpatient Unit, Pediatric Intensive Care Unit, Pediatric Emergency Room, Neonatal Intensive
Care Unit. The survey consisted of 11 questions regarding practices in the use of patient ID band and barriers to correct
utilization.
A baseline audit was done on all 4 units. For each patient on the unit at the time of the audit, the presence and accuracy
of the ID band was assessed. If the ID band was not present or was not accurate, the specific problem was documented;
the auditor spoke with family and/or nursing to clarify the exact reason for the problem. If the ID band had more than 1
error, the failure was only counted once. No attempt was made to find patients who were off the unit at the time of the
audit. The auditor verified patient information by interviewing parents and reviewing the medical record.
For the next 9 months, each unit conducted 4 audits per month. At least 1 audit per month was done on a weekend or
holiday, and at least 2 audits per month were done at night. The audits were performed by trained nursing or medical
staff or one of the researchers. As with the baseline audit, accuracy of ID band information was confirmed by
Quality Symposium 2012
Page 51
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
interviewing parents, if possible, and reviewing the medical record. If there was an ID band error, the auditor spoke to
family and/or nursing to elucidate the reason for the error. This conversation was also used an an opportunity to
provide education to staff, family and patients about the importance of ID band presence and accuracy.
The data was posted in each unit. In addition, meetings were held with nursing and medical staff to discuss best
practices for ID band safety.
The differences in failure rate from baseline to the end of the study was assessed by comparing the failure rate during
the first and last month of study participation, using the chi-square test.
Results
69 surveys were completed. 26% of respondents reported using identifiers other than name and medical record number
(which are the required patient identifiers in pediatrics). 48% of respondents had an encounter with a patient without an
ID in the past 6 months. 10% reported an encounter with a patient who had a wrong ID in the past 6 months. 22%
reported a delay in patient care secondary to a wrong ID in the past 6 months.
17% of the staff reported that the ID band being removed and not replaced as the biggest barrier to have an ID band on
the patient. 17% reported that the ID band getting in the way of patient care as the biggest barrier. 14% reported poor
fit, 8% reported that the patient or family had removed the ID band. 43% believed there were no barriers to having the
ID band on the patient.
The baseline audit of the four units revealed a 23% patient ID error rate, namely that the ID was either not on the
patient or was inaccurate or illegible. 100% (N=8) of the IDs in the NICU were present and accurate. 80% (N=4) of the
IDs in the ED were present; 20% (N=1) were not on the patient. 66% (N=6) of the IDs in the Pediatric Inpatient Unit
were present and accurate; 2 IDs were not on the patient and one ID had an illegible bar code.
Only 50% (N=2) of the IDs in the PICU were present and accurate. One ID was not on the patient and one ID had
illegible patient information. After 9 months, the patient ID error rate was reduced to 7% (chi-square=10.569, df=1,
p<0.001); 94% of the errors were due to the ID band not being on the patient. By unit, the percent of ID bands that
were correct and accurate were: NICU 92%, Inpatient 93%, PICU 100%. The ED had no data reported for the last
month (during the prior month their accuracy rate was 100%).
The most common reason for an ID band error was that the ID band was not on the patient. Common reasons for the ID
band being off the patient included falling off the patient, placement of the ID band on another object, the ID band
being removed for a procedure and not replaced, and the ID band being removed by a parent or patient.
Conclusions
ID band errors are common and occur on all patient units. The most common ID band error is that the ID band is not
on the patient. Improvement in the process of the initial placement of the ID band and the replacement after a
procedure are key. In addition, especially in pediatrics, one ID band does not fit all. The design and comfort of the ID
band is critical in enhancing compliance with its placement and retention.
The initial ID band error rate of 23% was similar to that reported at the other hospitals in the collaborative [3]. The
high rate of ID band error was of concern to all the investigators. Clearly, the first step in accurate patient identification
Quality Symposium 2012
Page 52
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
can be improved. We were able to successfully reduce our ID band error rate to 7% over the course of 9 months, using
auditing, feedback and education of staff, patients and families. Surveillance of ID band errors should be a component
of quality assurance in all patient care areas.
References
1. http://www.npsa.nhs.uk/EasysiteWeb/getresource.axd?AssetID=57989&type=Full&servicetype=Attachment
(Norris, B. Standardising wristbands improves patient safety: guidance on Implementing the Safer Practice Notice.
National Patient Safety Agency, April 19, 2009.
2. Hain, PD et al. An intervention to decrease patient identification band errors in a children's hospital. Quality &
Safety in Health Care, 2010; 19: 244-247.
3. Phillips, SC, Saysana, M, Worley, S & Hain, PD Reduction in Pediatric Identification Band Errors: A Quality
Collaborative. Pediatrics, 2012, 29, e1587-e1593.
Quality Symposium 2012
Page 53
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Strategies for Reducing Preventable Readmissions for Patients with CHF Patients Discharged to
Nursing Homes
Kathleen Treacy, RN; Steven Silber, DO; Carol Farina, RN; John Heitner, MD; Emil Baccash, MD; Snow
Nguyen, MD
New York Methodist Hospital
Introduction
Preventable hospital readmissions are an extremely costly proposition, costing Medicare approximately $12 billion per
year. Congestive Heart Failure (CHF) is the most common condition sending Medicare patients back into the hospital,
with the most recently available national average being approximately 25%. This high rate has multiple etiologies, both
preventable and non-preventable, including severity of illness, comorbid conditions, lack of timely physician follow
up, confusion or non-compliance with medications, health literacy, as well as socioeconomic factors.
Problem
It has been shown that discharge to a Skilled Nursing Facility (SNF) is an independent risk factor for 30-day
readmissions and this cohort of patients are 1.75 times more likely to be readmitted to the hospital than those that go
home who do not require home care service. One expert panel concluded that up to 68 percent of hospital admissions
from nursing homes are avoidable.
New York Methodist Hospital had an extremely high 30-day readmission rate for Medicare Fee For Service (FFS)
patients with CHF discharged to SNFs, with rates of 50% in 2009 and 41% in 2010.
Goals
Our project goal was to significantly decrease the Medicare FFS 30-day readmission rate for patients with CHF
discharged to a SNFs using validated principles derived from highly reliable transitional care coordination programs
used throughout the country, such as Project Red, Project BOOST, and the the Institute for Healthcare Improvement's
State Action on Avoidable Rehospitalizations (STAAR) Initiative. In addition, the hospital collaborated closely with
the SNFs to implement Interventions to Reduce Acute Care Transfers (INTERACT), a quality improvement program
developed under a contract with the Centers for Medicare & Medicaid Services (CMS) specifically to reduce avoidable
nursing home-to-hospital transfers.
Methods
We partnered with 5 SNFs that receive the highest number of hospital discharges to implement cross continuum care
transitional processes to mitigate readmissions. Medical and Nursing Leadership of the hospital met with Medical and
Nursing Leadership of each SNF to identify potentially avoidable reasons for readmissions and to develop strategies to
overcome these obstacles. The interventions began in the first quarter of 2011 and is ongoing.
The interventions included:
1. Improving the quality of transitional documentation for patients being discharged to SNFs.
2. Transitional care case managers communicated directly with their counterparts at the SNFs to better explain the
needs of the patients, including medications, advanced directives, and goals of care. This gave the SNF partners the
ability to ask questions and clarify the information.
Quality Symposium 2012
Page 54
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
3. Transitional care personnel from the SNFs were able to contact their counterpart at the hospital when a patient was
sent to the Emergency Department in order to explain the goals of the visit, which might not be to admit to the hospital.
The transitional care personnel at the hospital would communicate back to the SNF personnel to determine if the goals
of treatment were met and if the patient would be able to return to the SNF.
4. The Palliative Care Service at New York Methodist Hospital became more active, with an expected 450 annual
volume of consults projected for 2012. This is a huge increase from the 72 in 2010. This was very instrumental in
improving the number of patients discharged with advanced directives appropriate for their condition. These advanced
directives were part of the the transitional communication.
5. Hospital nursing and medical personnel went to the SNFs to present goal directed therapy seminars for CHF. This
assisted the SNF's to implement a project INTERACT type program for CHF.
6. The hospital engaged in monthly "facetime" conferences with the SNFs to discuss all readmissions from the
previous month to determine if any of them were preventable and to determine future strategies.
Results
The 30 day readmission rate for Medicare FFS patients with CHF discharged to SNFs from New York Methodist
Hospital decreased significantly since the inception of the program. The data are as follows: (See Figure 1)
QUARTER
2009
2010
Q2 2011
Q3 2011
Q4 2011
Q1 2012
RATE
50%
41%
41%
30%
27%
13%
Conclusions
Improving the coordination and communication across the continuum of care is an essential aspect in providing the
best and most appropriate care for patients discharged from the hospital. Many initiatives, including Project BOOST,
the STAAR Initiative, Project Red, and The United Hospital Fund's Transitions in Care Quality Improvement Project
(TcQuIC) and Preventing Hospital Readmission Initiative (PHRI) strive to prevent readmissions by improving the
coordination of care across the continuum. Project INTERACT has been successfully utilized by SNFs to decrease
their readmission rates. We chose to apply principles derived from the above mentioned initiatives to decrease
preventable readmissions for Medicare FFS beneficiaries with CHF by improving the quality of transitional
communication across the continuum between the hospital and our skilled nursing facility partners.
The data illustrates that our strategy has been successful. Data will need to be collected over time to see if the
improvements are sustainable. The approach that we piloted for CHF patients will be expanded to include all diagnoses
as the Hospital / SNF partnership moves forward with our participation in the CMS Innovation Center's Community
Care Transition Project.
Quality Symposium 2012
Page 55
Figure 1: 30‐Day SNF Medicare FFS CHF Readmission Rate 60
50
40
30
20
10
0
2009
2010
q2 2011
q3 2011
q4 2011
q1 2012
Quality Symposium 2012
Page 56
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Effects of Integrating Automated Safeguards to Promote Anticoagulation Safety and Efficiency
Erin Y Oh, BA PharmD BCPS; Nasser Saad, PharmD; Teena Abraham, MS PharmD BCPS; Righard van
Niekerk, BPharm; Eric Balmir, MS PharmD
New York Methodist Hospital
Introduction
Safety concerns of using anticoagulants have attracted significant attention due to numerous sentinel events relating to
the use of these agents. Due to the complexity of finding a balance between efficacy and safety of anticoagulant
therapy, careful monitoring and medication management processes is warranted. Studies have addressed integrating
safety features with computerized physician order entry (CPOE) systems to reduce the occurrence of medication errors.
Problem
Anticoagulants with a narrow therapeutic index, such as warfarin, have a low threshold between the risk of developing
thrombotic events and bleeding. Agents which require weight-based dosing or dose adjustment based on specific
monitoring parameters, such as heparin and enoxaparin, have also been shown to cause unwanted outcomes. Improper
usage or inadequate monitoring of anticoagulation can cause detrimental outcomes to patients.
Goals
Our goal is to reduce the risk of patient harm by incorporating the anticoagulation safety features in an electronic
medical record.
Methods
From January 2009 to December 2011, at the New York Methodist Hospital (651-bed acute-care teaching facility), we
implemented over time the following automated anticoagulation safeguards:
1) Addition of anticoagulation protocols in the CPOE upon approval by various hospital committees, such as
Pharmacy and Therapeutics Committee and Anticoagulation Committee;
2) Mandate of previous international normalized ratio (INR) documentation in the physician ordering field for
warfarin;
3) Implementation of anticoagulation order sets with approved indications and related monitoring parameters;
4) Double signature by two nurses in the electronic medication administration record (eMAR) prior to administration
of continuous intravenous anticoagulants;
5) Nursing documentation and report of subtle signs and symptoms of bleeding in the eMAR during each
administration;
6) Anticoagulant reference material was embedded into the electronic medical record;
7) Upon completion of pharmacy intervention documentation for the anticoagulation orders, detailed reports were
generated and forwarded to physicians for feedback and education.
All anticoagulation-related pharmacy interventions and medication errors with their respective severity codes were
compiled and reviewed. Comparison between anticoagulation data from 2009, 2010 and 2011 was performed, to
analyze the correlation between implementing automated anticoagulation safeguards with the prevalence of
anticoagulation-related medication errors and pharmacy interventions.
Quality Symposium 2012
Page 57
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Results
There was an average of 130,422 anticoagulation orders and 313,415 anticoagulant doses dispensed per year during the
specified time period. Pharmacy intervened on average of 1.63% of anticoagulants each year.
Warfarin orders had 2.17% pharmacy interventions in 2009, 1.44% in 2010, and 1.73% in 2011.
For heparin used in various treatments, there were 26.64% of pharmacy intervention is 2009, 13.75% in 2010 and
16.33% in 2011.
Enoxaparin orders had 15.03% interventions in 2009, 10.85% in 2010 and 11.51% in 2011.
Anticoagulation-related medication errors reported were 0.019% (23 out of 121,397), 0.01% (14 out of 135,559), and
0.017% (23 out of 134,309) during 2009, 2010 and 2011, respectively.
There were 4 incidences of medication errors that may have contributed to patient harm in 2009, accounting for 3
incidences of category E (error that may have contributed to, or resulted in, temporary harm to the patient and required
intervention) and 1 incidence of category I (error that may have contributed to, or resulted in, patient death). Whereas
in 2010 and 2011, no incidences of anticoagulation medication errors contributing to patient harm (categories E to I)
were reported.
Conclusions
Incorporating anticoagulation safeguards did not show definite trend towards a decrease in anticoagulation-related
medication errors. However, decrease in the severity of the medication errors were observed during the period of
safeguard implementation from 2009 to 2011. The number of pharmacy interventions has also decreased during the
safeguard implementation. Integrating automated safeguards in the CPOE system may have contributed to the
reduction in the medication errors leading to patient harm, as well as, improved efficiency of medication management
process by reducing the need for pharmacy interventions.
Quality Symposium 2012
Page 58
New York Methodist Hospital Pharmacy Department I.
Dispense Reports Year Anticoagulation # of Orders 2009 2010 2011 121397 135559 134309 II.
Anticoagulation Doses Dispensed 276165 324255 339826 Warfarin # of Orders 9841 13596 12200 Warfarin Doses Dispensed
10295 13945 12722 Heparin Heparin Enoxaparin Enoxaparin # of Doses Doses # of Orders Orders Dispensed Dispensed 1742 1798 5623 9468 2735 2966 7494 13853 3209 3625 6758 12510 Anticoagulation Interventions Year % Warfarin % Interventions Warfarin Intervention
Intervention 2009 2010 2011 2138 1859 2363 1.76% 1.37% 1.76% 214 196 211 2.17% 1.44% 1.73% % % Heparin Enoxaparin Heparin Intervention Enoxaparin Intervention
26.64% 15.03% 464 845 13.75% 10.85% 376 813 16.33% 11.51% 524 778 Anticoagulation Pharmacy Interventions
30.00%
26.64%
25.00%
20.00%
13.75% 16.33%
15.00%
2009
15.03%
10.85% 11.51%
10.00%
5.00%
2010
2011
2.17%
1.44%
1.73%
0.00%
Warfarin
Heparin
Enoxaparin
Quality Symposium 2012
Page 59
III.
Anticoagulation Medication Errors Year 2009 2010 2011 Medication Errors
23
14
23
Severity Codes
A‐I
A‐D
A‐D
Anticoagulation medication errors severity codes Year 2009 2010 2011 A 1 1 4 B 3 2 5 C
6
5
5
D
9
6
9
E
3
0
0
F
0
0
0
G 0 0 0 H
0
0
0
I
1
0
0
Quality Symposium 2012
Page 60
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Clinical Effects of Implementing a Point of Care Ultrasound Division; Data from the Pilot Project
Gerardo Chiricolo, MD; Tim Mooney, MD; Kevin O'Rourke, MD; Lawrence Melniker, MD; Joseph Bove,
MD; Steven Silber, DO
New York Methodist Hospital
Introduction
Point of Care Ultrasound (POCUS) has been shown to decrease time to diagnosis, make bedside procedures safer, and
decrease morbidity. Its use is a complete paradigm shift in clinical medicine. Physicians at the point of care perform
the ultrasound examinations, and it is symptom based as opposed to organ-based imaging. The ultrasound is performed
by the treating physician and interpreted by the same. This is in contrast to the traditional method where a physician
orders an ultrasound, a technician then performs the exam, followed by a radiologist who interprets the exam,
ultimately resulting back to the treating physician to correlate the results clinically. POCUS has been well established
in the emergency department (ED) with over 70 fellowships programs nationwide. It is utilized in other medical
specialties but is not as established as in the ED. POCUS is also being taught in various medical schools throughout the
country and it is introduced as early as the first year in conjunction with anatomy and physiology. As more physicians
in various specialties begin utilizing POCUS, there is a need for a division where standardization of the education,
research endeavors, quality assurance, and administrative issues are uniform throughout the institution.
Problem
With various medical specialties utilizing point of care ultrasound (POCUS) in the clinical environment, the risk of
inconsistent education, quality assurance, and administrative oversight could lead to misdiagnoses, poor patient
outcomes and unnecessary patient safety concerns. We also aim to decrease and prevent procedural complications by
utilizing POCUS for most bedside procedures.
Goals
Our aim was to introduce a centralized Division of Point of Care Ultrasound within the Department of Emergency
Medicine at New York Methodist Hospital. The Division is tasked with standardizing a credentialing process, the
educational requirements, the quality assurance, and the administrative guidance for all clinical departments utilizing
POCUS. The project excluded departments and divisions who perform comprehensive ultrasound services, i.e.
radiology and cardiology. The pilot project involved the medical ICU, the Cardio-Thoracic ICU, and the Division of
Pulmonology. We tracked the clinical outcomes of patients where POCUS was utilized after standardized education
and quality assurance was introduced.
Methods
We analyzed data collected from the overall education of POCUS for a select group of examinations, the number of
ultrasounds performed, the diagnosis and clinical outcomes of those patients who underwent POCUS examinations.
The physicians included had a series of one-hour didactic sessions covering basic physics and instrumentation, limited
echocardiography, thoracic and lung ultrasonography, procedural guidance, focused assessment with sonography in
trauma, and abdominal aorta assessment followed by a several hour hands on workshop at the patients bedside. After
several examinations were performed under direct supervision of the POCUS director, the physician was able to utilize
the modality clinically with oversight remotely from the ultrasound director corroborating the clinicians performance
and findings. We began the pilot in late February 2012 and included data up until the pilot project was deemed
Quality Symposium 2012
Page 61
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
successful in May 2012.
Results
In total, there were 211 ultrasound examination performed.
Three (3) of the eight (8) attending physicians have exceeded the number of ultrasounds required for credentialing in
POCUS and have displayed competence in performing those examinations.
There were 2 cases of cardiac tamponade detected in the Cardiothoracic Intensive Care Unit (CTICU), which was
immediately treated, and one suspected case of tamponade that was ruled out by POCUS, avoiding the unnecessary
mobilization of significant hospital resources.
There were 4 cases of deep venous thrombosis (DVT) detected in patients. 2 of the DVT cases were in symptomatic
patients, 1 was detected incidentally during the insertion of a femoral arterial catheter, and 1 was detected just prior to
discharge from the hospital preventing a hospital readmission or possibly a bad outcome such as pulmonary embolism
or even death.
There were 5 cases of pneumothoraces detected via ultrasound prior to chest x-ray performance as well as 20 cases of
pleural effusions which were both detected via ultrasound and treated with ultrasound guided thoracentesis.
Ultrasound has been successfully used in in assisting the physician to determine fluid status, estimate ejection fraction,
and ultimately guide management with intravenous fluids or vasopressors, avoiding many cases of pulmonary edema
or early vasopressor use.
There has yet to be a complication when used during procedural guidance. There are 3 active interdepartmental
research projects currently in data collection.
Conclusions
Implementation of a Point of Care Ultrasound division has proven to be beneficial for both the clinician and patient
alike. It decreased time to diagnosis, decreases morbitiy and procedural complications, and improves patient care.
Quality Symposium 2012
Page 62
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Making the Honor Roll: Reducing Treatment Delays in Acute Stroke
Barbara J Gatton, MD; Matthew Dros; Lawrence Melniker, MD; Linda Fox; Miran Salgado, MD; Jeffrey
Benjamin, MD; Joseph Bove, MD; Steven Silber, DO
New York Methodist Hospital
Introduction
Acute stroke is a devastating disease and we as physicians have adopted a "time is brain" approach for a select group of
acute stroke patients. The American Heart/Stroke Association (AHA/ASA) developed the Target Stroke: Honor Roll to
recognize hospitals that excel in treating acute stroke patients within prescribed time targets. The current standard of
care in acute stroke is to treat patients within three hours of symptom onset with tissue plasminogen activator (tPA).
New York Methodist Hospital is an urban community teaching hospital with 90,000 ED visits per year. We see
approximately 400 stroke patients per year and approximately 20 patients per year meet criteria for acute ischemic
stroke.
To qualify for the Target Stroke: Honor Roll, 50% of patients who are eligible for tPA must receive it within sixty
minutes of hospital arrival. In 2012, out of over fifty 911 receiving hospitals in New York City, only six hospitals,
including New York Methodist, received this award. We were able to achieve this using a Plan-Do-Study-Adjust
methodology.
Problem
There are many barriers to timely treatment of acute stroke. Identifying the patients, having the CT scan completed and
interpreted, identifying contraindications, and performing the appropriate assessments all consume time. To have all of
this completed, then mix and administer the medication within sixty minutes is difficult to achieve in a busy
Emergency Department. Data from a national stroke registry revealed that, from 2005-2009, only 26.6% of eligible
patients received tPA within 60 minutes.
In many of the AHA/ASA quality indicators for stroke, the target has been set as either 75% or 85%. The time
challenges in treating eligible patients with acute stroke with tPA within an hour are so great that 50% is considered the
target; so much so that only 18 hospitals in the state of New York had been able to accomplish it in 2011.
Goals
To improve timeliness of administrative of tPA to eligible patients with acute stroke using American Heart/Stroke
Association Target Stroke: Honor Roll Guidelines.
Methods
We analyzed each step in the evaluation and treatment process for acute stroke patients and identified common causes
for delay. We then developed strategies to eliminate them. We modified our Stroke Protocols accordingly and used a
continuous quality improvement process to assess effectiveness and make adjustments.
We started by improving communication with pre-hospital providers so that we were alerted prior to the patient’s
arrival when possible. We improved stroke education and communication between registration clerks, triage personnel,
Quality Symposium 2012
Page 63
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
and physicians.
We determined that there was a significant delay to CT Scan. Prior to being sent to CT, patients were routinely placed
on oxygen and on cardiac monitors, received point of care (POC) glucose, had an IV placed and bloods drawn, and had
an ECG performed. Then the patient was switched from the wall mounted cardiac monitor to a portable monitor and
switched from wall oxygen to portable oxygen. We evaluated which of these were essential to have prior to CT and
concluded that the only one required was the POC glucose. We could determined that time could be saved by placing
patients on a portable monitors and oxygen from the beginning.
All ED attendings were trained to be Stroke Certified so that they can evaluate the patient, interpret the CT scan, and
make the decision to treat with tPA themselves. The decision is still made in conjunction with the Neurologist, but if
there is a delay in the neurologist getting to the hospital, the decision to treat can be made in their absence, usually after
a telephone conversation with the Neurologist.
There was concern that sending the patient to CT prior to having labs sent would delay lab results and treatment. We
have POC testing for PT/INR so that we may obtain rapid results in high risk patients. Patients who are low risk are
usually treated without having laboratory results.
Results
Median time from arrival to CT went from 93 min to 25 min in three years. During the same time frame, patients
receiving tPA within 60 min of arrival went from 27% (n=11) to 50% (n=12). The median time to tPA dropped from
70.5 min in 2009 to 60 min in 2011.
Conclusions
We found that waiting to do ancillary testing until after CT was performed decreased time to treatment. There were no
significant alternative diagnoses that were missed, or had delayed treatment, as a consequence of moving CT ahead of
other diagnostic work up.
High Impact Interventions:
• ED Attendings Stroke Certified
• CT prior to IV, labs, ECG
• Portable monitor and oxygen
• POC laboratory testing
In the first half of 2012, 54.5% of patients received tPA within 60 minutes, with a median time of 58 minutes,
suggesting that these improvements have been sustained. Having a stroke certified physician already present in the ED
and decreasing the time to CT allowed for rapid treatment decisions and, therefore, decreased time to tPA
administration.
Quality Symposium 2012
Page 64
Quality Symposium 2012
Page 65
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Ocular Ultrasound Simulation Lab: Does It Translate to the Bedside?
Kevin O'Rourke, MD; Sharon Yellin, MD; Tim Mooney, MD; Lawrence Melniker, MD; Joseph Bove, MD;
Steven Silber, DO; Gerardo Chiricolo, MD
New York Methodist Hospital
Introduction
Two percent of ED visits are eye-related complaints. Ocular ultrasound (US) gives the emergency physician the ability
to assess the eye for a variety of disease processes. The Council of Residency Directors Emergency Ultrasound
Consensus Committee does not identify ocular ultrasound as a core US competency for Emergency Medicine resident
graduation but does note that assessing skill in this exam should be incorporated into the resident curriculum. The
accuracy of bedside ocular US has been studied and there are published reports of models used for simulation. The
breadth of knowledge about the effectiveness of using simulations for ocular US is limited. We know simulation is
effective but does simulation with models translate to the bedside?
The goal of this study is to evaluate if an ocular ultrasound lecture and simulation lab leads to increased utilization at
the bedside and to determine what diagnoses were found. This should in turn increase the appropriateness of transfers
to other institutions for further ophthalmalogic management and decrease inappropriate use of consultants and
resources.
Problem
Fundoscopic examination of the eye is extremely limited in the Emergency Department especially when the pupil is
not pharmacologically dilated. This limited ability to perform a comprehensive ocular exam may lead to poor patient
outcomes, inappropriate use of consultants and lead to unnecessary transfers to outside institutions for further
ophthalmologic management.
Goals
The goal was to analyze the effect of an ocular ultrasound simulation lab on its use in the clinical arena, specifically
related to its utilization and the range of pathology detected. All studies were reviewed for quality assurance and had
multiple experienced sonographers independently render an impression to correlate the initial diagnosis with the final
diagnosis.
Methods
On March 21, 2011, the Emergency Ultrasound Division at New York Methodist Hospital hosted a lecture and handson ultrasound training program. Within that program, a lecture was given on ocular ultrasound and participants had the
opportunity to practice on simulated eyeball models with different pathologies.
In this retrospective review, we searched our ultrasound database for all ocular ultrasounds performed the six months
before and after an ocular ultrasound lecture and simulation lab. We included all patients who had ocular US between
September 21, 2011 and September 22, 2012. No patients were excluded. No patient identifiers were included in the
analysis. Data collection included the date that the ultrasound was performed and the diagnosis based on the
performance of the ultrasound.
Quality Symposium 2012
Page 66
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
All ocular ultrasound examinations were independently reviewed by 3 separate blinded physicians who are
credentialed to perform ocular ultrasounds. The agreement was 100% for all cases.
Results
In the six months before the lecture and lab, 18 ocular ultrasounds were performed. The findings included 9 normal
ultrasounds, 2 vitreous hemorrhages (1 with a posterior vitreous detachment, as well), 3 with increased optic nerve
sheath diameter, 2 retinal detachment, 1 with postoperative changes, and 1 with a foreign body.
There were 2 (2/18 or 11%) false positives in the study as determined by expert review of the examinations. The optic
nerve sheath diameter was later deemed to be of normal caliber and one of the retinal detachments was deemed to be
vitreous hemorrhage.
In the six months after the lecture and lab, 28 ocular ultrasounds were performed. The findings included 11 normal
ultrasounds, 7 with increased optic nerve sheath diameter, 5 with vitreous hemorrhage, 1 globe rupture, 1 with
choroidal detachment, and 1 with vitreous detachment and 2 incomplete studies. There were no false negatives or false
positives in these 28 examinations.
There were 10 more ultrasounds performed in the Emergency Department after the intervention, which equates to a
55% increase in ultrasound utilization. There was also a 10% reduction in false positive rate which would have
prevented one unnecessary transfer and one unnecessary CT scan of the brain and subsequent lumbar puncture.
Conclusions
An ocular ultrasound lecture and simulation lab led to increased utilization of bedside ultrasound for patients. In the
future, we anticipate this skill to decrease inappropriate transfers, improve patient outcomes and increase appropriate
and timely evaluations by an ophthalmologist.
Quality Symposium 2012
Page 67
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Impact of a Protocol Based on Estimated Glomerular Filtration on Dose of Iodinated Contrast
Administered and Image Quality
Joseph Samide, PharmD; Nasser Saad, PharmD; Teena Abraham, MS PharmD; Eric Balmir, MS PharmD;
Claudia Lapidus, MD; Steven Garner, MD; Anthony Mungo, BSRT
New York Methodist Hospital
Introduction
Iodinated contrast has become essential to the practice of modern medicine and the use of contast has increased
exponentially since its introduction in the 1950s. Although new generations of iodinated contrast have improved
tolerability, contrast-induced nephrotoxicity (CIN) is still a devastating consequence of contrast use. CIN is the third
leading cause of hospital acquired renal insufficiency. Although CIN is commonly associated with transient renal
insufficiency, permanent damage requiring dialysis can occur. Age, diabetes, hypertension, hypovolemia, and the use
of nephrotoxic agents are all risk factors for the development of CIN, but the most important risk factor is baseline
renal dysfunction. An eGFR of < 60mL/min/1.73m2 has been associated with an increased risk of CIN.
Problem
In order to better understand the risk of CIN at our hospital, we reviewed the current policies and procedures in place at
our institution. The traditional method of screening for patients with renal insufficiency used by many hospitals,
including our own, was lacking.
Clinical trials have shown that using a serum creatinine measurement alone to estimate renal function before contrast
administration is inaccurate, potentially exposing patients with a higher risk for CIN inappropriately to iodinated
contrast. The use of formulas like the Cockcroft-Gault equation or Modification of Diet in Renal Disease (MDRD)
formula to estimate renal function has been associated with increased sensitivity.
Goals
The goal of this project was to measure the impact of screening for renal insufficiency using eGFR instead of serum
creatinine alone. The project was designed to evaluate the the number of non-contrast studies performed and the
volume administered to patients before and after the policy change.
Methods
This trial was designed as a two part study. The first part of the study was a retrospective, computer-generated chart
review. Patients at our institution were traditionally assessed for risk of CIN using a serum creatinine threshold of 1.7
mg/dL. Data was collected on the CT-scans performed with and without contrast using the old policy. Fifty patients
with an eGFR of less than 60 mL/min/1.73m2 were also selected at random for a more comprehensive evaluation. The
average volume of contrast administered, the number of dose reductions, the quality of the image, and the incidence of
CIN were all evaluated in these patients.
After analyzing our data (see Results section) and a thorough literature review, the decision was made to update the
policy at our institution. In collaboration with radiology department, a new policy was drafted. This policy no longer
recognizes a serum creatinine threshold as the most effective way to quantify risk of CIN. Instead patients are screened
using the MDRD equation and those with an eGFR of less than 60 mL/min/1.73m2 should receive a dose adjustment.
Quality Symposium 2012
Page 68
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The new policy also included guidance on physicians on the dosing of contrast at various eGFR thresholds. The policy
was approved by the October 2011 Pharmacy and Therapeutics Committee meeting. The NYMH CPOE system was
modified to reflect the policy change and members of the Radiology department were given access to eGFR
measurements in CERNER.
After policy approval, the second phase of data collection was initiated. The number of CT-scans with or without
contrast was once quantified. Forty-nine patients with renal insufficiency were selected at random and the average
volume of contrast, the number of dose reductions, image quality, and the incidence of CIN were evaluated and
compared with the previous results.
Results
The results of this trial showed that there was a significant reduction on the number of CT-scans performed utilizing
contrast. Before the implementation of the policy, 756 scans with contrast were performed per month. After the policy
was updated, the average number of scans dropped by 57 studies per month. The drop in the number of patients
requiring contrast was especially significant because the total number of CT-scans performed increased over the same
time period.
The average volume of contrast administered declined by 11 mL in the 99 patients with renal impairment after the
implementation of the new policy and the number of dose reductions increased by 2%. Although these numbers alone
do not appear significant, coupled with the overall decline in contrast use at our institution, it appears that our policy
did decrease the volume of contrast being administered to high risk patients.
In addition to monitoring contrast volume, our study assessed image quality and incidence of CIN. The change in
policy did not adversely alter image quality nor did it alter the incidence of CIN. CIN occurred once in each arm and
resolved completely after hydration. Although we would expect the policy change to have a positive influence on the
incidence of CIN at our hospital, our study did not enroll enough patient to capture this outcome.
Conclusions
The implementation of the new hospital policy and the intensive educational sessions that accompanied it reduced the
number of patients receiving contrast and decreased the volume of contrast administered to high risk patients. It is
important to note that this decrease occurred in spite of an overall increase in the number of CT scans performed.
Our results show that the implementation of this process improved the ability to screen for patients with renal
insufficiency and better assess them for the risk of CIN. The study also proved that the dose can be effectively lowered
without sacrificing image quality.
Although the results from this trial appear to be positive, there is still room for improvement as a number of patients
still received full doses of contrast despite have impaired kidney function.
Quality Symposium 2012
Page 69
The Impact of a Protocol Based on Estimated Glomerular Filtration on Dose of Iodinated Contrast Administered and Image Quality Table 1. Average Contrast Volume (mL) Average Contrast Volume (mL/kg) Diagnostic Imaging Number of Dose Reductions Average Volume of Dose Reduction (mL) Incidence of CIN 2010 Policy Arm (n=50) 134.3 20.9
2011 Policy Arm (n=49) 123.0 28.1 1.9 0.6 1.7 0.6
47(96%) 6 (12%) 49(100%) 7 (14%) 40 20.7 41 26.1 1(2%) 1(2%) Data collected during chart review. Quality Symposium 2012
Page 70
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Use of Automated Weight-Based Dosing to Prevent Medication Errors in the Pediatric
Emergency Department
Righard van Niekerk, BPharm; Christopher Kelly, MD; Pramod Narula, MD; Kathleen Treacy, RNVP; Anna
Boyko, PharmD; May Jabra, PharmD; Gary Wu, PharmD; Laura Melville, MD
New York Methodist Hospital
Introduction
In the Institute of Medicine’s landmark report "To Err is Human" it has been revealed that preventable medication
errors ranked higher in death rates as compared to car accidents, breast cancer, and AIDS. According to the Institute for
Safe Medication Practices, the pediatric population has three times the risk for medication errors as compared to adults.
The Pediatric Emergency Department at New York Methodist Hospital (NYM) sees approximately 23,000 patients a
year. Of those, approximately 2,000 patients are admitted for further care. This volume result in thousands of
medication orders prescribed by scores of providers.
Problem
Medication errors not only lead to direct patient harm and or death, but also have financial and psychological costs on
the healthcare system. Serious preventable medication errors occur in over 7 million patients each year. It is estimated
that these errors cost the healthcare industry $21 billion annually, not to mention the loss of public trust in their health
care provider, which is priceless. Among the numerous factors with the potential to lead to medication errors, the one
with the highest impact is the requirement for weight-based dosing. This includes obtaining and documenting the
patient’s correct weight using the appropriate units, and applying the correct dosing regimen to this weight.
A solution to ensure the safe use of medication in this population is the use of technology. The Joint Commission
issued a sentinel event alert in 2008 that illustrated the importance of judicial use of technology and its role in ensuring
appropriate dosing in this special population.
Prior to the implementation of this solution at NYM there was no standardization of weight documentation or
automated weight-based ordering in our Electronic Health Record (EHR). Weight conversions from pounds to
kilograms, as well as application of weight-based dosing, were all done manually by the provider and thus susceptible
to human error. Potential errors included substituting between kilograms and pounds, using the incorrect dosing per
weight and miscalculations. Pharmacists have always double-checked and clarified orders to avoid potential
medication errors, however this manual intervention carried significant time cost and did not take advantage of the
electronic ordering system. And while there were no significant medication errors, a proactive approach was set in
motion to hopefully further minimize the risk.
Goals
The goal of this project was to ensure the safe use of medications in a highly vulnerable population. A
multidisciplinary approach was utilized. The primary intervention was the establishment of weight based dosing in our
computerized provider order entry system (CPOE) to help providers make the correct decisions as well as other
practices to support the intervention. This dosing would be based on a standardized methods of weight entry into the
Quality Symposium 2012
Page 71
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
EHR. This process improvement strategy provided real time decision support, making it "easier to do something right
and much harder to do something wrong." Furthermore, it created yet another level within the safety net to prevent any
potential medication errors, thus protecting our youngest of patients and ensuring that we give the best care possible.
Methods
Acknowledging there was a potential for medication errors, a Pediatric Emergency Medication Safety Committee was
created. Members representing the Pharmacy, Emergency Medicine, Pediatrics and Nursing Departments met regularly
to create processes that would safeguard against potential medication dosing errors. The interventions are described
below.
1. The first part of the project was to ensure that patient’s dosing weights were stored as a discreet value in only one
metric unit, kilograms. Given that most patients, parents and people think in pounds, we felt it imperative that weights
be entered as such. The EHR then automatically converts the weight field into metric units, which are then used for
dosage calculations.
2. Digital standing and infant scales were purchased for the Pediatric Emergency Department to assure the most
accurate weight was obtained for each patient.
3. Once weight entry was standardized, a list of medication orders commonly prescribed in the Pediatric Emergency
Department was obtained. A weight-based drug dictionary was constructed using 55 weight-based medications and 260
order sentences based on each medication’s mg/kg dosing information. The order sentences were added to the CPOE
section of the EHR and grouped separately from adult order entries to prevent selection error.
4. A clinical dose calculator was turned on and evoked every time the specific order sentences were chosen. The
system then utilized the patient's documented medication dosing weight and pre-completed order sentence to calculate
the final dose which the prescriber can round if appropriate.
5. The order is then sent to the pharmacy for review with all the data and calculations the prescriber used.
Data collection involved looking at a 4-month period before and after implementation. The number of pharmacy
interventions for medical clarification and/or correction was analyzed.
Results
The number of pharmacy interventions was reviewed before and after implementation of automated weight based
dosing. Although no serious preventable medication errors occurred in this time frame, several interventions by the
pharmacy staff were performed. These interventions consisted of contacting the provider to clarify an order or change a
miscalculated dose.
In the four month time period prior to policy implementation, 55 dosing interventions occurred for a total of 3,556 total
orders placed in the Pediatric Emergency Department, representing an intervention rate of 1.5%.
In the four months following policy implementation, 18 interventions occurred for a total of 3,852 orders placed,
representing a reduction in intervention rate to 0.5%.
Quality Symposium 2012
Page 72
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The use of standardized weight entry and computerized weight-based dosing led to an important decrease in the
number of interventions, directly following the project. The pharmacy department records an average of 2,829
interventions per month throughout the hospital.
Conclusions
The integration of an automated weight-based dosing calculator into an EHR as well as the standardization of weight
documentation and order sentences has reduced the potential of overdosing errors significantly in the Pediatric
Emergency Department. By eliminating the need for manual calculations by both physicians and nurses, we’ve
eliminated a large potential for human error simply by programming the computer do the work. It is a very sustainable
process in that it is automated, and can be easily adapted to accommodate new medications and changes in existing
dosing regimens. This intervention has been deemed so successful in the ED that it was implemented throughout the
Pediatric Department including the Neonatal Intensive Care Unit.
Quality Symposium 2012
Page 73
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Development of a Nursing Quality and Patient Safety Fellowship
Barry S Gallison, DNP MS APRN-BC NEA-BC CPHQ; Judith A Rizzo, PhD RN NEA-BC CPHQ; Peggy
Quinn, MPH RN
NewYork-Presbyterian Hospital
Introduction
The purpose of this innovative program is to provide staff nurses with a broader understanding of Quality and Patient
Safety in today's healthcare and regulatory environment. Staff nurses participate in the quality improvement process,
perceive experiences as improving the quality of patient care delivered and improve the safety of their patients. Staff
nurses' participation in the program strengthens knowledge, level of comfort and sustains a culture of safety.
Problem
Assist staff nurses to design, implement and evaluate quality improvement projects specific to their unit's needs.
Goals
Information on the program was disseminated through fliers, posters and announcements at local Quality Councils.
Candidates applied by writing an essay about their role in quality and safety, included a resume, and two letters of
recommendation (one from their nurse leader).
Methods
Quality and Safety leaders at the hospital were recruited to present.
The curriculum included classes such as:
Role of Quality Fellow; Evolving State of Quality and Safety; Culture of Safety; Introduction Quality Improvement
Projects; What is DMAIC?; What the Current Infection Data Tell Us; Patient Services: Errors, Events, Families and
Regulatory Agencies; Nurse:Physician Communication; Nursing Documentation: Core Measures and Pay for
Performance; Patient Satisfaction: Press Ganey and HCAHPS; and, Everything You Wanted To know About The Joint
Commission But Were Afraid To Ask.
With minimal budgetary impact the program has developed unit-based Nursing Quality Fellows engaged in
transforming practice, improving outcomes and sustaining a culture of safety.
Results
Program evaluations were conducted based on objectives, class content and class experiences. 99 out of 158 rated the
program as Excellent, 44 out of 158 rated the program as Good, and 5 out of 158 rated the program as poor. The
program is now offered annually. The next cohort is slated for the Fall of 2012.
Conclusions
Over 100 Performance Improvement Projects were developed and implemented across the organization, including:
Hand off communication, Pain management, Medication safety, and Hospital Acquired Conditions (CLABSI, CAUTI,
VAP, HAPU). A new program has been designed to support and strengthen nurse leader engagement.
Quality Symposium 2012
Page 74
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Putting the Pressure on Reducing Hospital Acquired Pressure Ulcers
Debra O'Hehir, MSN MBA RN (1); Tochi N Okorie, MBA RN (2); Lourdes Mellino, MA MEd RN NEA-BC (1);
Mary E Quinn, MSN RN (2); Barry S Gallison, DNP MS APRN-BC NEA-BC CPHQ (1)
(1) Nursing, NewYork-Presbyterian Hospital
(2) Division of Quality & Patient Safety, NewYork-Presbyterian Hospital
NewYork-Presbyterian Hospital
Introduction
The Nursing Department monitors prevalence of hospital acquired pressure ulcers and benchmarks to National
Database of Nursing Quality Indicators. The assessment and identification of patients at risk for hospital acquired
pressure ulcers is an important component of patient management. Hospital acquired pressure ulcers prolongs the
hospital stay, increases the risks of hospitalized acquired conditions, contributes to the seriousness of complications
and increases patient discomfort.
Problem
In 2007, hospital acquired pressure ulcers reach a rate of 5.99%. The Department of Nursing identified the need to map
out a strategic plan to reduce the rate.
Goals
In 2011, the hospital set a goal of reducing hospital acquired pressure ulcers by 5%, focusing on accurate skin
assessment and staging to improve inter-rater reliability and decreasing variance in how staging is specified.
Methods
The Nursing Department revamped the Pressure Ulcer Program by standardizing care, focused on education, and
documentation across all campuses. The hospital conducted a comprehensive review of skin care products. An
algorithm for specialty bed use and approval process was developed and communicated to all nursing units. A
concentrated focus on updating skills on skin assessments in the emergency department and perioperative areas was
conducted. The hospital purchased new beds, emergency department stretchers and operating positioning devices.
Additionally, a new process of reviewing and validating hospital acquired pressure ulcers by wound, ostomy and
continence care nurses. Including a single day point prevalence study conducted monthly to measure pressure ulcers.
Validation process resulted in re-staging of pressure ulcers and re-education on pressure ulcer staging and
management. Focused monitoring of HAPU events allowed for improved trending over time and a reconciliation of
hospital acquired pressure ulcers. Education of 5,000 staff members was conducted and completed through selflearning on-line modules. Educational programs realigned and target staff, patients and families. Provision of adequate
nutritional support in collaboration with the Food and Nutrition staff has proven to be successful in reducing hospital
acquired pressure ulcers occurrences and promoting wound healing.
Results
As a result of these combined efforts, the Nursing Department met the 2011 goal of reducing Hospital Acquired
Pressure Ulcer by 5% compared to 2010.
The Nursing Department has seen a 50% reduction in Hospital Acquired Pressure Ulcer over the last 5 years:
Quality Symposium 2012
Page 75
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• 2007 - 5.99%
• 2008 - 4.07%
• 2009 - 2.69%
• 2010 - 2.48%
• 2011 - 2.39%
Conclusions
The hospital's goal is to sustain its Hospital Acquired Pressure Ulcer rate reduction by reviewing current
documentation processes and introducing an early mobilization initiative: ambulating patients as soon as possible,
especially in the intensive care units (ICU), which will further help reduce ICU HAPU. Additionally, implementing the
Skin Resource Nurse Training Program.
Quality Symposium 2012
Page 76
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Multi-Disciplinary Bedside Rounds: Improving Communication and Teamwork to Enhance Patient
Engagement and Discharge Planning
Amy Silverstein, MPH; Daniel Sorbello, MPA NEA-BC RN; Ansa Rajan, MSN RN; Jean Flynn, RN EdD;
Patricia Prufeta, MS NEA-BC RN
NewYork-Presbyterian Hospital
Introduction
As part of a hospital-wide effort to examine barriers to timely patient discharge planning, two inpatient units
redesigned their multi-disciplinary rounding processes.
Problem
Patients were unhappy with their lack of involvement with discharge preparation. In addition, average length-of-stay
(ALOS) had increased from the previous year.
Patient Satisfaction: Patients’ discontent with discharge process was reflected in Press Ganey scores. Patients and
families were excluded from daily rounds, which occurred in a conference room on the unit.
Staff teamwork / Communication: Rounds were unstructured and inefficient. Communication about patient status was
not coordinated.
Length of Stay (LOS): Average patient LOS (ALOS) exceeded expected LOS (ELOS), and this variance was trending
in the wrong direction.
Goals
Over a 90-day period, beginning April 1, 2012:
(1) Standardize and include patient in daily multi-disciplinary discharge rounding process;
(2) Use this daily opportunity to resolve potential delays in treatment or discharge;
(3) Address patient concerns.
Methods
Changes were initiated on April 1, 2012 by Patient Care Directors (RNs) on two inpatient units. Following preliminary
tests of the changes, a series of working sessions were held to gain feedback and buy-in from all disciplines (Social
Work, Care Coordination, Nursing, Physician Assistants, Physicians and Physical Therapy). By the end of 90-days, on
July 1st, 2012, the bedside rounding process was fully scripted and agreed upon among all disciplines and "official"
implementation occurred.
Project changes tested:
(a) Daily multi-disciplinary rounds held with the patient at the bedside, including:
(b) Development and use of communication guidelines
(c) Introduction of team members
(d) Daily review of discharge goals
(e) Opportunity to answer questions
Quality Symposium 2012
Page 77
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
(f) Update changes to treatment or discharge plan on patient whiteboard
Measurements for improvement:
(1) Length of stay: variance between the actual and expected patient LOS
(2) Patient Satisfaction: Press Ganey survey scores pertaining to patient discharge process
Results
Improvement of the multi-disciplinary rounding process resulted in enhanced teamwork and communication among
staff members as well as better patient engagement with treatment decisions and discharge planning. Patient
involvement in the discussion ensured that their needs and concerns were proactively addressed. The standardization of
the rounds was identified as the most important change. Since residents change every 1-2 weeks, the standardized
communication guidelines help orient new team members and keep the rounds focused.
LOS Variance (ALOS - Expected LOS*): [Figure 1]
(1) Pre-implementation (Jan 2011 - Mar 2012): on average, patient LOS was 22.3 hours greater than expected*
(2) Post-implementation (Apr - Jun 2012 ): on average, patient LOS was 0.48 hours (29 min) less than expected.
(3) Average LOS decreased by 23 hours (0.96 days).
*NYP calculates expected length of stay (ELOS) for patients based on the APR-DRG and Severity of Illness (SOI, 1-4)
for each patient. The ELOS for each APR-DRG/SOI combination is the mean actual length of stay (ALOS) for that
same APR-DRG/SOI combination at a comparison group of Honor Roll hospitals.
Patient Satisfaction with Discharge^ (Mean Press Ganey Score): [Figure 2]
(1) Pre-implementation (Jan 2011 - Mar 2012): Press Ganey score for Discharge overall was 82
(2) Post-implementation (Apr - Jun 2012 ): Press Ganey score for Discharge overall was 86
(3) Patient satisfaction score increased by 4 (5%)
^ Discharge overall includes: Extent patient felt ready for discharge, Speed of discharge process and Instructions given
for care at home
Conclusions
Patient and families appreciate seeing their entire care team together each day in order to ask and receive answers to
questions at one time.
The following activities with all team members were crucial to the successful implementation of the intervention:
• Outlining the benefits and challenges of bedside rounding;
• Defining roles and responsibilities of participants;
• Gaining consensus from key stakeholders.
• Ongoing challenges include helping all team members see the value and positive impact of multi-disciplinary
bedside rounds.
Spread and sustainment: Multi-disciplinary bedside rounds were identified as a hospital-wide best practice and will be
implemented across multiple NY-Presbyterian Hospital campuses.
Quality Symposium 2012
Page 78
Quality Symposium 2012
Page 79
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Early Mobilization in the ICU
Katherine Pavlovich, MPH; Suzanne Boyle, RN DNSc; Daniel Brodie, MD; Ernesto Perez-Mir, MSN RN
CCRN; Patricia Rychcik, MSN RN
NewYork-Presbyterian Hospital
Introduction
Clinical evidence from leading academic medical centers indicates that failing to mobilize critically ill patients in
intensive care units (ICUs) worsens patient outcomes and increases their length of stay (LOS). This is a significant
problem for NewYork-Presbyterian as ICUs at the Weill Cornell (WC) and Milstein campuses experience high
occupancy rates and limited capacity to accommodate volume increases. In order to improve these issues, specialized
ICU mobilization teams in various ICUs were developed in order to improve quality of care, create culture change
related to early physical activity and reduce LOS across both campuses.
Problem
Over the last few years, clinical evidence suggested that the accepted practice of keeping critically ill patients sedated
and immobile resulted in poorer morbidity-associated outcomes. Confining patients to their bed increased functional
impairment, muscular atrophy, mechanical ventilation and thus reduced quality of life post-discharge. During this same
period, ICUs at both WC and Milstein were routinely approaching full occupancy with limited capacity to
accommodate increases in volume of critically ill patients. With no plans to add beds, NYP needed another way to
improve overall ICU efficiency.
Goals
Early Mobilization of patients in the ICU focused on culture change towards earlier patient mobilization as well as
reducing both ICU LOS and total patient LOS in order to increase ICU bed capacity. Specific targets were set for a
reduction in total LOS: a reduction of 3,975 excess days (as compared to baseline measurements, January 2011 - June
2011).
Methods
Based on models used at other academic medical centers, specialized ICU mobilization teams were created across 3
services (Medical, Cardiac and Surgical) on 2 different campuses (WC and Milstein). This multidisciplinary group
included nurses, physicians, pharmacists, and physical, occupational and respiratory therapists, that identified/treated
patients before they developed ICU-associated conditions, reducing the number of days patients spend in the hospital.
Both WC and Milstein currently have one dedicated team that focuses on providing treatment 7 days a week for every
patient that has been medically cleared and resides in one of our 5 participating ICUs (MICU and CCU at WC, MICU
A, MICU B and SICU at Milstein). During the weekdays, the team is led by a Senior Physical Therapist who meets
with the Night Fellow/Nurse Practitioner at change of shift to learn about any clinical changes that happened overnight.
This information is used during the 8:00am bed huddle where the team of Physical and Occupational Therapists,
Respiratory Therapists and staff Nurses all meet together, briefly discussing the status of each patient and creating the
daily plan. The program uses an "opt out" principle: all patients are assumed to be eligible unless they have a legitimate
medically-related exemption. The plan of care is different for each patient, based on prior and current level of
functioning, but could include simple range of motion exercises, eating, dressing or other activities of daily living, or
Quality Symposium 2012
Page 80
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
even ambulation. Because the team is dedicated to the Units on which they are treating patients, questions and changes
in the plan can be vetted with Attendings, Pharmacists and other group members in real time. All treatments throughout
the day are recorded in a mobility log, in order to both track progress and communicate with the rest of the team.
Results
The addition of dedicated therapists to the 5 ICUs increased the number of daily treatments patients receive almost 20
fold, from approximately 0.05 treatments/patient day at the end of 2011 to 1.00 treatments/patient day postimplementation. This is equivalent to each patient getting one treatment every day. 85-90% of medically cleared
patients are being actively mobilized; including passive range of motion as a treatment modality increases this
percentage to almost 100%.
As the Team has been able to provide more treatments, the amount of time patients spend in the hospital has also
decreased. Since implementation on January 11th, 2012, both the ICU and total hospital LOS for patients treated in the
5 ICUs has dropped dramatically: through August 2012, ICU LOS has been 0.85 days lower as compared to the first 6
months of 2011, on par with programs at other academic medical centers. Total hospital LOS has been 2.9 days lower,
as much as 4.7 days lower for patients in the MICUs. This is a reduction of almost 2 days greater than any other MICU
that has published results. These variance reductions have translated into a projected annualized excess day reduction
of 7,050 days -- over 3,000 more days than our target (3,975 excess days). This reduction has also allowed these ICUs
to accommodate almost 170 additional patients, equivalent to an 8% increase in volume.
Conclusions
The ICU Early Mobilization program at NYP was the first to implement outside of the MICU and is currently the
largest in the world. The success of this initiative has been due to our alignment with the hospital's strategic goals,
organizing and standardizing the components of the program across multiple sites, and the extraordinary collaboration
across a multitude of disciplines and services.
As hospitals continue to balance cost and quality, it is imperative to implement initiatives that align clinically and
financially. This initiative had strong organizational commitment due to the large reduction in excess days and
financial savings that were promised if we were able to obtain dedicated resources. More importantly, these reductions
were translated into increased bed capacity and an ability to care for more patients. Regular reporting of metrics (LOS,
frequency and type of treatment) held the team accountable with senior management and finance and also allowed us to
share the impact of this initiative with all group members.
Organization of program development provided a framework for rollout on such a large scale. A small steering
committee was established in the fall of 2011 to define the initiative, guide teams on overall strategy and provide
support for any issues. Clinicians that had successfully implemented this type of program at other institutions came to
speak, reiterating the evidence on the safety, efficacy and benefit of mobilizing patients. Champions from each
discipline and ICU began to meet every week 3 months before implementation in order to plan, troubleshoot barriers
and engender internal support for this practice change. The team developed structured roles and responsibilities, using
WWWs and timelines to track progress on metrics, education and implementation. It was also imperative to
standardize tools, roles and processes in order to set expectations and provide clear guidance about putting this
initiative into practice across many different sites.
The partnerships between disciplines and campuses have been one of the most important components of the program's
Quality Symposium 2012
Page 81
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
success. The focus has always been on doing the right thing for the patient which made it easier for groups who had
never met each other to work together and create shared guidelines, reports and educational materials. The power of
patient experiences also underscored this notion of teamwork: videos, photos and in-person interactions allowed
everyone at NYP to see and celebrate the impact. A monthly newsletter was even developed to share additional
information and patient stories. This cross-campus collaboration has also set the stage for adding other disciplines to
the program as well as potential alignment with other hospital-wide initiatives, like Noise Reduction and Sleep
Deprivation.
Because of the tremendous impact on the patient experience and the hospital's financial outcomes, we will be
expanding this program to 8 additional ICUs in 2013. Partnering with affiliated step down and floor units will be an
integral component of sustainability, continuing the success of significant culture change towards earlier patient
mobilization.
Quality Symposium 2012
Page 82
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Hand Offs to Skilled Nursing Facilities
Karen A Scott, MD; Eliot J Lazar, MD; Brian K Regan, PhD; Michael J Fosina; Christine Agir-Donelly, RN;
Margaret McGregor, RN; Ellen Cotter, RN; Donna Tingling-Solages, RN; Denise Robinson, RN; Alan Levin,
RN; Germaine Nelson, RN; Vepuka E Kauari, RN; Audrey Compton, MD; Eileen Kornfeld, MSW; Paula
Roberts, MSW
NewYork-Presbyterian Hospital
Introduction
Transitions in care, or "hand-offs", represent a time where patients are particularly vulnerable because their care is
being managed by multiple health care providers, often across different departments or settings. Studies have shown
hand-off communication to be a highly variable process, hampered by time constraints, frequent omissions, lack of
crossover in knowledge between specialties and/or departments, high pressure situations, staff turnover, and fear of
redundancy (Ong and Coiera, 2011). Patient transfers from hospitals to nursing homes are often plagued by fragmented
information and poorly coordinated care that result in medical errors and rehospitalizations that place patients at greater
risk for injury or death. It’s clear that standardization/coordination (between individuals/providers) is lacking. Working
with the Joint Commission: Center for Transforming Healthcare, we worked on improving this process by enhancing
hand off communication.
Problem
Inadequate hand-off communication across settings may contribute to overall patient dissatisfaction at best, and at
worse, complications and readmission. An analysis of nearly 12 million Medicare beneficiaries discharged from a
hospital during 2003 and 2004 revealed that 34% were rehospitalized within 90 days, costing Medicare approximately
$17 billion in 2004. The most recent data show that 23.5% of Medicare beneficiaries who were discharged from
hospitals to nursing homes were rehospitalized within 30 days costing taxpayers a total of $4.34 billion. Estimates
show that nearly three-fourths of these readmissions may be preventable (Sherman, 2009).
Goals
While there is an appreciable need for standardized, valid tools to ensure the quality of care during patient transfers,
few institutions have attempted to tackle this issue head on. Coleman and colleagues in Denver, Colorado created a
Care Transition Measure, which was designed as a patient-centered tool to evaluate hand-off communications (2002).
Parry and colleagues instituted a Care Transitions Intervention model, attempting to stave off subsequent
rehospitalizations in a Medicare fee-for-service population (2009).
During the Joint Commission’s Center for Transforming Healthcare Collaborative on Hand-Off Communication, we
felt that by improving communication, and standardizing our tool, we would see a positive impact on readmissions,
and staff satisfaction.
Methods
Our pilot study, conducted at the Columbia Campus of NewYork-Presbyterian Hospital, was part of the Joint
Commission Center for Transforming Healthcare Hand-Off Communication Project. We aimed to look at transfers
from our hospital to a non-acute care facility.
Quality Symposium 2012
Page 83
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
In an effort to understand the impact of hand-off communication, we issued surveys to both the senders (on our pilot
unit) and receivers involved in the transfer of care. Specifically, the senders were health care providers at NewYorkPresbyterian Hospital, and the receivers were on staff at a nearby nursing home. We wanted to measure the impact of
standardized communication in these areas: 1) staff satisfaction, 2) readmission rates and 3) Bouncebacks:
readmissions within 72 hours. The implementation of the surveys was aimed at highlighting vulnerable points in handoff communication, improving staff satisfaction, and reducing "bounce backs."
The intervention was implementation of the use of Skilled Nursing Facility Transfer format the Allen Hospital. The
Skilled Nursing Facility Transfer form was modeled off the Transition document called the Interact Form. Once we
compiled input on the document from our clinical staff and the nursing home care providers, we were able to tailor its
content to fit our needs. Adding a section where nurses must specify any high-alert medications, the patient is taking
was among one those changes. Our Skilled Nursing Facility Transfer form also stipulates that a three day medical
admitting record (MAR), in addition to an updated patient discharge medication list, must be distributed to the nursing
home at the time of patient transfer. Currently, nurses are expected to complete both discharge instructions, and this
standardized tool which became electronic effective Dec 2011, thus the burden of paperwork has been alleviated.
Staff surveys were first distributed in June 2010, before the Skilled Nursing Facility Transfer form was put into use.
We readministered the surveys in November 2010 after the form had been implemented. As a secondary aim, we also
measured readmission rates at 3 days (or 72 hrs), and 30 days.
Results
Our initial survey results should that sender satisfaction was 78%, while receiver satisfaction was 71%. Our baseline
readmission rate at our pilot site was 26%, our bounceback rate was 4%. On repeat survey after implementation of
transfer document our satisfaction rate for sender satisfaction was 88% while receiver satisfaction increased to 85%.
Our readmission rate went from baseline of 26% to 11% (current baseline)and our bounceback rate decreased to 1% .
We have maintained this 50% decrease in readmission rate through second quarter 2012 across all sites. We feel as
though these results can be contributed to improved communication, we also feel that the success has been
multifactorial. Nursing homes have initiated programs to address readmissions, as well early identification of patients
who are decompensating; changes also include changes to staff mix, cohorting patients, and implementation of care
plans including treatment recommendations.
Conclusions
Improved, structured hand off communication has had a positive impact on readmissions, bouncebacks and staff
satisfaction. We have also begun to expand to all facilities and we are working on the use of this document for any
patients returning to the hospital. We will continue to work on enhancing communication, monitoring readmission
rates, and ultimately measuring patient/ family satisfaction and working closely with skilled nursing facilities to
develop pathways for treating disease locally rather than sending the patient back to an acute setting.
Quality Symposium 2012
Page 84
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Health Information Technology Supported Improvement of Immunization Rates Across a Multi-Site
Academic Medical Center
Jamie R MacDonald, RN MSN MBA; Karen A Scott, MD MPH; Patricia Prufeta, RN; Peggy Liu, RN MS;
Robert Green, MD; Philip Graham, MD MSC; Eliot J Lazar, MD MBA
NewYork-Presbyterian Hospital
Introduction
Although providing preventive care in the course of an acute hospitalization can be challenging, inpatient encounters
are increasingly viewed as an opportunity to offer preventive services to patients. The Centers for Medicare and
Medicaid Services (CMS) have emphasized this opportunity by including immunization rates for pneumococcal
disease and influenza as hospital core measures. In 2012, CMS updated the specifications to include a global inpatient
population (including pediatric patients).
Problem
Publicly reported data show that excelling in vaccination has been challenging to many hospitals regionally and across
the nation. Under specifications through 2011, the average rate of compliance with pneumococcal vaccine for adult
pneumonia patients from January-December 2008 was 84% nationally; 87% for New York State, and 74% for
NewYork-Presbyterian Hospital (NYP), with similar performance for influenza vaccination. At the end of 2011, the
national rates were 95% for pneumoccocal vaccination and 93% for influenza vaccination [1]. But, moving into 2012
with the new global inpatient population specifications, many hospitals saw declining rates. In Q1 2012, for
pneumococcal vaccine, NYP fell to 78%, while the national average dropped to 88%.
[1] Hospitalcompare.hhs.gov, accessed November 12, 2009; and September 27, 2012.
Goals
To improve patient safety by improving pneumococcal and influenza vaccination rates in the global inpatient
population.
Methods
In 2008, NYP began an institution-wide initiative to improve adult immunization rates. Several specific changes were
implemented, which required the engagement and participation of numerous disciplines and departments across the
hospital. A multidisciplinary leadership group, which includes representatives from quality, epidemiology, pharmacy,
medicine, bio-medical informatics, information technology, and nursing was tasked to drive improvement. This group
has continued to meet monthly through the past five years. When the new regulations began in 2012, another layer of
improvement effort was necessary.
The leadership group led the following changes:
• Development of a series of alerts in the electronic health record
• Discharge Instructions hard stop alert if active vaccine orders are present (April 2012)
• Discontinue vaccine order alert to capture appropriate documentation (February 2012)
• Not Given on medication administration record alert to capture appropriate documentation (February 2012)
• Development of a report to show vaccine orders left active at discharge (April 2012)
Quality Symposium 2012
Page 85
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Associated root cause analysis and clinician re-education based on non-compliant cases
• Updated verbiage in contra-indication fields in the admission order set in the electronic health record to comply with
the new regulations (January 2012)
• Updated verbiage in nursing admission histories in the electronic health record to comply with the new regulations
(December 2011)
• Development of an admission orderset that guides the admitting physician to screen all patients for vaccine eligibility.
If eligible, the orderset automatically places an order for appropriate vaccines to be given during hospitalization
(implemented February 2009);
• Many updates and improvements to the vaccine portion of the admission order set have been necessary since
February 2009.
• Communication to attendings, housestaff, physician assistants, and nurse practitioners on the new orderset and alerts,
and importance of addressing immunizations;
• Communication and education for nursing personnel about these orders, documentation, and alerts;
• Development of biweekly reports that were fed back to individual units to monitor performance, and determine
barriers;
• Development of RN Audit Tool to identify training opportunities for administering vaccines;
• Updated to target patients under age 65 (July 2012)
• Collection of specific data elements that facilitated root cause analysis to identify process problems and how they
could be improved.
Results
Prior to the new 2012 specifications, for inpatients with Pneumonia, we had seen steady and sustained improvement in
immunization rates:
• Pneumococcal Vaccine Rates increased from 73% in Q4 2008 to 90% in Q4 2011
• Influenza Vaccine Rates increased from 82% in Q4 2008 to 91% in Q1 2011
With the new 2012 specifications, we have seen significant improvement from Q1 to Q3:
• Pneumococcal Vaccine Rates increased from 78% in Q1 to 95% in Q3 (preliminary) [Figure 1]
• Influenza Vaccine Rates were 92% in Q1 (not abstracted during Q2 and Q3) [Figure 2]
Key Changes
1. Clinical Information System
• Electronic Alerts in the Electronic Health Record (February - April 2012)
• Electronic report to monitor active vaccine orders (April 2012)
• Documentation verbiage updates to electronic notes and orders (December 2011 - January 2012)
• Hospital Admission Order set (February 2009)
• Duplicate order alert added (March 2009)
• Biweekly Data reports from Electronic Health Record (November 2008)
• Medication Administration Record documentation updated (September 2009)
• Ability to view historical vaccine data for physicians and nurses (May 2010)
• Electronic alert at the time of discharge if the RN has not documented the vaccines as given (November, 2009)
2. Policy/Practice/Communication
Quality Symposium 2012
Page 86
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Hospital wide multidisciplinary leadership committee in place (reports to Chief Medical Officer)
• Nursing Chart Audits - with counseling and re-education when non-compliant
• RN/MD/Housestaff Communication
• Policy Revision - immunizations given during hospitalization; influenza vaccine available on unit
• Nursing education/ communication on policy revisions and IT documentation changes
• Pharmacy Report to track vaccine doses
Conclusions
• Significant and sustained improvement has been seen in placement of vaccine orders, as well as in the number of
patients who either received the vaccine or had appropriate documentation for not receiving the vaccine.
• This is an ongoing quality improvement initiative, using continued monitoring of immunization rates to identify
additional opportunities to improve the process.
• A focused, multidisciplinary approach led to improved immunization rates. Targeted changes to the institution’s
admission process, through an orderset (where vaccine eligibility was linked with the computerized provider order
entry system) combined with broad communication and education were instrumental in achieving improved
immunization rates. The ability to monitor the effects of the intervention through regular reports derived from our
electronic health record was critical in fostering an atmosphere of continual improvement.
• Targeted use of the electronic health record to create changes to support compliance
• Nursing audit tool provides immediate feedback on the units, and provides the Quality Improvement committee with
issues for improvement or resolution.
• Because The Joint Commission considers immunizations priority ‘accountability’ measures and because vaccine
compliance is a CMS core measure, all hospitals must comply. We hope that they work done at NYP will help others
around the country who are struggling with similar issues.
Quality Symposium 2012
Page 87
Figure 1
NYP Pneumococcal Vaccine Rates
Pneumococcal vaccination
Hospital Compare National Avg
100%
95%
90%
85%
80%
75%
70%
NEW: Q1 2012 Specifications for Global Inpatient Population
Figure 2
NYP Influenza Vaccine Rates
Influenza vaccination
Note: Influenza data is
abstracted during flu
Hospital Compare National Avg
100%
95%
90%
85%
80%
75%
70%
65%
NEW: Q1 2012 Specifications for Global Inpatient Population
Quality Symposium 2012
Page 88
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Correlation of Hand Sanitizer Placement with Good Hand Hygiene Compliance
Samantha Brenner, MD MPH; Samuel Sultan, MD; Susan Faggiani, RN BA CPHQ; David Calfee, MD MS;
Peter Fleischut, MD; Eliot Lazar, MD MBA; Gregory Kerr, MD MBA
NewYork-Presbyterian Hospital
Introduction
Hand hygiene compliance is essential to infection control in hospitals.
Problem
Physicians are often found to be less compliant relative to other health care workers.
Goals
To determine if observer-based hand hygiene compliance data correlate with workflow-based placement of alcohol
hand-rub (AHR) dispensers.
Methods
A survey was conducted to determine the locations of AHR dispensers in patient rooms relative to physician workflow
patterns. AHR dispenser location data were compared to historic observational hand hygiene compliance rates on
individual hospital units.
Results
Unit-based hand hygiene compliance rates were correlated with adequate placement of dispensers (R-square = 0.45)
but not with dispenser density per bed (R-square = 0.04).
Conclusions
This study suggests that placement of AHR dispensers based on workflow patterns may significantly improve hand
hygiene compliance, particularly in groups where improvement in compliance rates has been difficult, by using AHR
dispenser placement to capitalize on the automaticity required for good hand hygiene compliance.
Quality Symposium 2012
Page 89
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Full Scale Multidisciplinary In-Situ Simulation Prior to Opening a New Pediatric Emergency
Department
David Kessler, MD; Melissa Cappaert, MA; Christopher Walker, RN; Carolyn Kyne, RN; Daniel Tsze, MD;
William Middlesworth, MD; Meredith Sonnet, MD; Dennis Fowler, MD MPH
NewYork-Presbyterian Hospital - Simulation Center
Introduction
In-situ simulation, or simulation training that is integrated into actual clinical environments, can help identify latent
patient safety threats and system issues in the environment. Few articles exist on how best to utilize simulation in
preparing for clinical work in a new space. We describe our experiences using in-situ simulation to prepare for the
opening of a new Level 1 pediatric emergency department at the Morgan Stanley Children's Hospital at NewYorkPresbyterian Hospital.
Problem
Prior to the public opening, members of Pediatric Emergency Department (PED) and a variety of non-clinical team
members sought to provide a full complement of pediatric critical care staff with non-emergency and emergency
preparedness within the new environment.
Goals
Our objectives were to familiarize staff with the environment and to stress the system in an effort to reveal latent
patient safety and system concerns.
Methods
Members of the PED and a variety of non-clinical team members formed a committee tasked with non-emergency and
emergency preparedness for the new PED. We focused the planning on three levels: large volume disaster
management, normal flow of patient care, and acute care. A multidisciplinary tabletop exercise was conducted to assess
our preparedness for disasters in the new space. Normal flow was evaluated using walk through exercises in the new
space with representatives from key stakeholder groups. Finally, once patient rooms were fully stocked with supplies
and equipment, we conducted a "mock opening" for three hours that utilized a full complement of staff including
residents, nurses, respiratory therapists, pre-hospital care providers, registrars, radiology technicians, pharmacists,
social workers, child life specialists, pastoral care, security, information technologists and attending physicians from
pediatric emergency medicine, trauma surgery, anesthesia and the pediatric intensive care unit.
A matrix of patient cases was carefully designed to systematically cover a range of low to high acuity scenarios that
were portrayed by either actors or computerized human patient simulators. Observers were assigned to specific cases
and followed a scenario through the trajectory of intake to discharge in order to record issues using a checklist
developed for this event. Semi-structured debriefing took place in groups following the simulation.
Results
Simulation provided basic familiarity for the staff and uncovered latent safety threats including: need for code button
in the waiting room; changes to layout of supplies in trauma room; moving equipment for easier access to emergency
outlets; modified route to preferred CT scanner; and the need for curtains in trauma rooms for privacy.
Quality Symposium 2012
Page 90
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Conclusions
In-situ simulation provided an invaluable contribution to the preparation of the new PED for patients. The exercises
also led to the development of ongoing weekly mock codes and monthly mock trauma curriculum in the PED.
Quality Symposium 2012
Page 91
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
An Action-Oriented Patient Safety Conference Model for the New Millennium
Laura Fanucchi, MD MPH; Joseph T Cooke, MD; Eugenia Siegler, MD; Lia Logio, MD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Introduction
Most residency training programs incorporate a morbidity and mortality conference (M&MC) to analyze adverse
events and medical errors and promote quality assurance, though there is no standard format, and the focus is mostly
on pathology or pathophysiology.
Problem
Given the growing focus on patient safety in residency education, we re-defined our M&MC as an interdisciplinary
Patient Safety Conference (PSC).
Goals
Educate residents in system-based practice as it applies to patient safety.
Provide an open, non-judgmental forum to discuss patient care episodes that did not go as intended.
Increase resident interaction and communication with nursing, pharmacy, hospital administration, and departmental
leadership
Methods
Format:
• Monthly Conference
• Part of core educational conferences
• Interdisciplinary representation
• Nursing
• Pharmacy
• Administration
• Modified Root Cause Analysis
• Action Items
Two cases highlighted:
• Case A: A PICC line was pulled on the wrong patient.
• Case B: Delay in antibiotic administration for a patient with neutropenic sepsis.
Results
CASE A:
• Mandatory patient education (including medical students)
• Patient identification and verification
• Time-out protocols - treat reversal of procedures as a procedure (ie. removal of a line same as placing a line)
• Notification of nursing staff prior to any procedure
Quality Symposium 2012
Page 92
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
CASE B:
• Intervention unit: 56 orders required revision or verification over 6 weeks (75% of the orders were revised or verified
within 120 minutes).
• Comparison unit: 39 orders required revision or verification over 4 weeks (57% of the orders were revised or verified
within 120 minutes).
Conclusions
Guiding Principles:
• Medicine is difficult
• Errors are inevitable
• Errors are unintentional
• Goal is to learn from adverse events and work towards a systems-based solution to keep them from recurring
An interdisciplinary Patient Safety conference promotes open discussion about medical errors, promotes collaboration
between housestaff, Nursing, Pharmacy and other staff. It provides for resident education on tools such as Root Cause
Analysis. It promotes use of Plan Do Study Act as a structured means making things better today. This conference is an
on-going effort of our Department of Medicine and has become integral to the training program and our new Patient
Safety elective for housestaff.
Quality Symposium 2012
Page 93
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Laboratory Cost Savings Associated with Prospective Review of Physician Orders
Doris O Samide; Jennifer F Zepf, DO; Stephen G Jenkins, PhD; Audrey N Schuetz, MD MPH
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Introduction
In the current era of tightening laboratory budgets, superfluous test orders are problematic. ViraCor-IBT Laboratories
(Lee’s Summit, MO) performs the majority of the send-out reference molecular virology testing for the Clinical
Microbiology Laboratory at NewYork-Presbyterian Hospital.
Problem
Charges to the Clinical Microbiology Laboratory for Viracor send-out testing had been increasing steadily each year.
In 2007, before this initiative, ViraCor charges approximated $386,000 for inpatients for our laboratory. We
proactively involved the laboratory staff and pathology residents in prospective reviews of certain inpatient orders
received by our laboratory.
Goals
Our goal was to reduce send-out costs associated with potentially unnecessary testing.
Methods
Guidelines for testing were developed in 2009 by a team of microbiologists and Infectious Diseases and
Transplantation/ Immunology clinicians for over 20 common and uncommon viruses from a wide variety of specimen
types and patient populations. Based on these guidelines, orders on inpatients for ViraCor testing which were listed as
potentially inappropriate were previewed by the laboratory staff or the pathology resident on service. The orders were
either approved or cancelled, based on discussions with the clinicians. The number and type of ViraCor orders received
and cancelled by the lab were recorded monthly from November 2009 to December 2010.
Results
After the institution of our initiative, 26% of all tests ordered in 2010 were cancelled, leading to a cost savings of
approximately $82,500. The percentages of cancelled tests by virus varied month-to-month by an average of 20%.
However, the total number of tests cancelled decreased over the 14-month period. The highest percentages of cancelled
tests included herpes simplex virus from specimens other than cerebrospinal fluid (74%) and human herpes virus 8
from any specimen source (89%). The highest numbers of cancelled tests were adenovirus and BK virus. The most
common reason for cancellation was multiple orders over a short time course for a single patient.
Conclusions
Cost savings were substantial, albeit dependent on month. As the ordering guidelines became more known and
widespread throughout the hospital, the numbers of tests which were cancelled decreased over time. The influence of
variables, such as ordering trends, was considerable. In particular, approval thresholds and patient outcomes are
deserving of further study. The findings support the use of prospective order review processes to manage the burden of
unnecessary inpatient testing.
Quality Symposium 2012
Page 94
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Optimizing Alpha-Numeric Paging on a General Medicine Floor
Parag Goyal, MD; Jennifer Lee, MD; Marianne Moore, MS RN PMHNP-BC; Lia Logio, MD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Introduction
Over the past decade, alphanumeric paging has replaced numeric-only paging in many hospitals across the country.
Whereas numeric-only paging can only communicate a callback phone number, alphanumeric paging provides the
opportunity to include clinically-relevant information such as patient name and condition. This allows physicians to
triage and prioritize pages received while performing other important tasks including caring for patients, rounding,
and/or attending lectures and meetings. Several studies indicate that alphanumeric paging decreases disruptions in
patient care, educational activities, and physician workflow; they also suggest a connection between fewer
interruptions and improved patient safety.
Problem
Anecdotally, alphanumeric paging is underutilized on the general medicine service at NewYork-Presbyterian
Hospital/Weill Cornell (NYPH/WC) despite being the standard communication modality used to send pages. There is
an opportunity to improve its use, and therefore reduce disruptions to patient care, educational activities, and physician
workflow.
Goals
Our aim is to increase the use of the alphanumeric paging system on one general medicine unit at NYPH/WC by 50%
in 8 weeks through an educational initiative with the nursing staff. We also hypothesize that our intervention will
improve patient care as perceived by nurses.
Methods
Over the course of an 8-week internal medicine residency quality improvement curriculum (June to August 2012), we
designed an educational initiative with the day shift (7 A.M. to 7 P.M.) nursing staff on Greenberg 5-Central (5C)
which was led by the Patient Care Director (PCD) during the morning huddle. During the session, we reviewed the
format of an optimal alphanumeric page (pt name, brief scenario, RN name and extension). After 4 weeks, we
expanded the intervention to include the night shift nurses (7 P.M. to 7 A.M.).
To measure the number of alphanumeric pages, we reviewed the paging logs of the interns on 5C during the study
period one week before and after our educational intervention. Pages tagged with extensions other than 5C were
excluded. All pages were categorized as "optimal," "suboptimal," or "numeric-only." (Figure 1)
We also measured nursing perspectives on paging through surveys distributed to the unit nurses one week before and
after our intervention. Questions were designed with the assistance of the PCD to assess the impact of alphanumeric
paging. Survey questions utilized a Likert-scale.
Results
The number of "optimal" pages increased from 44% to 60%. The percentage of "Numeric-only" pages decreased from
15% to 6% (Figure 2A). Following the night shift intervention, the percentage of "optimal" pages increased from 78%
Quality Symposium 2012
Page 95
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
to 96%, and "numeric-only" pages decreased from 19% to 4% (Figure 2B).
Twenty-eight nurses completed the pre-intervention survey, and fourteen nurses completed the post-intervention
survey. Following the intervention, 86% (12 out of 14 nurses) agreed or strongly agreed that alphanumeric paging was
more efficient than numeric-only paging. 71% (10 out of 14 nurses) felt that patient care would be improved with more
consistent use of alphanumeric paging. A common concern was the uncertainty about whether or not a page was
received if there was no call back from the resident.
Conclusions
In two months, residents were able to effectively design and implement a brief educational initiative that successfully
changed the paging practices of the nurses on one general medicine inpatient unit, and subsequently improved the
efficiency and quality of patient care. An important finding was the concern among nurses that they were unable to
close the communication loop with the residents using one-way texting. Designing a study implementing two-way
pagers has the potential to address this concern while continuing to improve teamwork among nurses and physicians,
and therefore patient care.
Acknowledgements: The authors thank the residents and nurses for their hard work and contributions to the study.
Isaac Bowman MD, Mark Diamond MD, Jonathan Gordin MD, David Fernandez MD, Timothy Glew MD, Kunal
Karia MD, Joseph Marmora MD, John Morris MD, Michael Mulock MD, Karla Nieves MD, Vikram Palanivel MD,
Rachel Sanford MD and Maryam Shafaee MD were all members of the research team. A special thank you to Brian
Eiss MD and Paula Tinghitella MSN, RN for their supervision and support.
Quality Symposium 2012
Page 96
Quality Symposium 2012
Page 97
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Designing and Implementing a Comprehensive Protocol for ED Identification and Management of
Agitated Delirium in Older Adults
Tony Rosen MD MPH; Scott Connors BS; Alexis Halpern MD; Michael E Stern MD; Sunday Clark, MPH
ScD; Mark S Lachs, MD MPH; Neal Flomenbaum, MD
(1) Department of Medicine, New York-Presbyterian Hospital/ Weill Cornell Medical College; (2) Division of
Medical Nursing, New York-Presbyterian Hospital
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Introduction
Agitated delirium occurs frequently in older patients in the emergency department (ED), is under-recognized, and has
potentially serious consequences.
Problem
Despite its seriousness, delirium is frequently missed by emergency providers, and patients with unrecognized delirium
are often discharged from the ED. Even when it is appropriately recognized, managing agitated delirium in older adults
poses a significant challenge for ED providers. Geriatric delirium is typically caused by the interaction of multiple
factors, including several which are commonly missed in the ED evaluation: pain, urinary retention, constipation,
dehydration, and polypharmacy. Appropriate management includes non-pharmacologic management with medication
intervention reserved for emergencies.
Goals
• To design and implement a new, comprehensive, evidence-based protocol for diagnosis/ recognition, management,
and disposition of geriatric agitated delirium in the ED with a focus on identifying and treating commonly missed
contributing causes.
• To improve and standardize care for older adults with agitated delirium in the ED.
• To provide a model for the design and implementation of future geriatric-focused protocols in the ED.
Methods
The protocol was developed through collaboration between the Divisions of Emergency Medicine and Geriatrics &
Gerontology at NewYork-Presbyterian/ Weill Cornell and was based on expert consensus after an exhaustive literature
review over a six-month period. The protocol focuses on evaluation of commonly missed contributing causes of
delirium in older adults and interventions to treat them. The protocol includes a mnemonic to assist ED providers with
remembering to evaluate for commonly missed contributing causes: A-B-C-D-E-F (A=analgesia, B=bladder/ urinary
retention, C=constipation, D=dehydration, E=environment, F=f(ph)armacy/ medications). For each contributing cause,
the protocol describes critical action(s) in evaluation and treatment.
An educational intervention, consisting of a 15-minute scripted slide presentation was developed to introduce the
protocol and to emphasize the importance of geriatric delirium in the ED. The educational intervention and protocol
were implemented in the NewYork-Presbyterian/ Weill Cornell Emergency Department.
Prior to protocol launch, the intervention was presented to a convenience sample of attending emergency physicians,
Quality Symposium 2012
Page 98
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Emergency Medicine (EM) residents, physician assistants, nurse practitioners, and nurses working in the ED.
Presentations were conducted at scheduled staff meetings and in-service training sessions between June and July 2012.
Written surveys were administered to all participants before and after the intervention. The pre-intervention survey was
designed to assess providers’ baseline knowledge, attitudes, and practice surrounding ED delirium in older adults. The
post-intervention survey was developed to measure the immediate impact of the presentation on knowledge and
attitudes and the potential for the protocol to affect future practice. Both surveys included previously validated
questions from published instruments and additional questions customized for this intervention. The surveys were
modified to reflect the clinical role of participants from different disciplines, so four forms of each survey were used:
for attending physicians, EM resident physicians, nurse practitioners / physician assistants, and nurses. Each survey
form was pilot tested using potential research subjects and revised based on comments and suggestions during this
testing. Data analysis for survey responses was conducted with Stata v12.0.
The protocol was launched in the NewYork-Presbyterian/ Weill Cornell ED on July 28, 2012 after the completion of
all educational intervention sessions. To reinforce the details of the protocol after launch, we designed and mounted
posters in all ED clinical areas. In addition, we distributed pocket cards displaying the protocol to all participants. This
research was reviewed and approved by the Weill Cornell Medical College Institutional Review Board.
Results
161 ED staff members participated in the pre-launch educational intervention, including 20 attending emergency
physicians, 45 EM resident physicians, 20 nurse practitioners/ physician assistants, and 76 nurses. Prior to the
intervention, 56% of participants reported feeling uncomfortable managing delirium and 91% reported believing they
would benefit from additional geriatrics training. After the presentation of the protocol, 94% of participants reported
feeling more comfortable with the differential diagnosis of delirium, 92% reported feeling more comfortable with
delirium management, and 95% reported feeling more comfortable with appropriate medication management in
geriatric delirium. Before the intervention, an average of 56% of respondents reported frequently evaluating patients
for the commonly missed delirium causes emphasized in the protocol. After the survey, 94% of participants reported
intent to evaluate for these causes. 93% of respondents reported believing that the A-B-C-D-E-F mnemonic would help
them remember the underlying contributing causes requiring assessment. On the initial survey, 45% of respondents
reported using benzodiazepines most commonly to manage agitation in older adults, despite the existence of clinical
guidelines that discourage its use. After the intervention, 16% of participants reported that they would still use
benzodiazepines most commonly. Initially, 29% of respondents reported using atypical antipsychotics most commonly
to manage geriatric agitation. Post-intervention, 57% of participants reported intent to use atypical antipsychotics most
commonly. 31% of respondents reported believing that the protocol may increase their workload.
Conclusions
Increased training on ED management of geriatric syndromes including delirium is clearly needed. Introduction of this
comprehensive, evidence-based protocol has increased provider awareness of this common, complex, potentially lifethreatening syndrome has given them confidence to more completely evaluate for and treat older adults presenting with
it, including interventions that might obviate the need for chemical sedation. We believe this will improve care for our
patients and are in the process of following up to assess the longer-term impact of the intervention and protocol,
including surveying participants at 1- and 6-month intervals, conducting comprehensive chart reviews, and analyzing
changes in prescribing patterns. Internal medicine ward units and intensive care units at NYP/ Weill Cornell are
considering adapting this protocol and integrating it into their clinical pathways. We intend the successful
implementation of this protocol to provide a model for future geriatric ED interventions.
Quality Symposium 2012
Page 99
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Multidisciplinary Approach to Developing a Protocol for Safe OR Management of a Patient with a
History of Sulfite Anaphylaxis
Ansara Vaz, BA; Antigone C Grasso, MBA; Nicholas Cavalieri; Beryl C Muniz, RN MAS; Lai Chin, RPh;
Rafique Khaled; Laura Maglione, RN MA CCRN; Alissa Ritter, RD CNSC CDN; Louise Merriman, MS RD
CDN; Vinod Malhotra, MD; Peter M Fleischut, MD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center
Introduction
Sulfite additives are used in a number of products spanning several industries--comestibles, pharmaceuticals, textiles,
cosmetics, manufacturing and sterilization. As a result of repeated exposures, some individuals have developed
sensitivities to sulfites with reactions ranging from urticaria, dermatitis and gastrointestinal symptoms to flushing,
hypotension, bronchoconstriction and anaphylaxis. The amount of sulfite in food products is rather small. However
inert ingredients, such as sulfites in medications, may constitute the bulk of the product and pose a great risk to those
with sulfite sensitivities. In addition, due to their widespread use, sulfites may be present in a number of obscure
products such as latex and pool water.
Problem
A patient with a known history of sulfite sensitivity, the most severe reaction being anaphylaxis, was scheduled to
undergo an ambulatory surgery at the Weill Cornell campus of the NewYork-Presbyterian Hospital (NYP).
Goals
Several NYP departments collaborated to form a multi-disciplinary team to evaluate potential sources of sulfite
exposure across the hospital with the goal of developing a protocol for establishing sulfite-free pre-, intra- and postoperative environments for patients with sulfite sensitivities.
Methods
A multi-disciplinary team was created with representatives from anesthesiology, surgery, allergy and immunology,
materials management and equipment, transfusion medicine, nursing, pharmacy, environmental services, and nutrition.
The patient was also encouraged to be an active participant in the development of this protocol.
In a joint effort, the team collaborated to identify all products that the patient would possibly come into contact during
her stay at NYP/WC. A catalog of over 200 items was created, including but not limited to, sterilization products,
linens, sutures, tubing, adhesives and medications. The manufacturer for each item was contacted individually to
confirm the presence or absence of sulfite in their products, and alternatives were obtained for those items that
contained greater than 0.1% sulfite.
Results
Due to the concerted efforts of this multi-disciplinary team, a sulfite-free environment was created and the patient's
exposure to sulfites was minimized, if not eliminated. The patient provided extensive background information,
including how the sulfite sensitivity was diagnosed and the context of past reactions. The surgeons and nurses
identified all instruments and products needed for the procedure, which materials management and environmental
services successfully ensured were free of sulfites. The holding area, operating room, and recovery room in which the
patient would stay were prepared with sulfite-free cleaners and all sulfite-containing items were removed. An allergist
Quality Symposium 2012
Page 100
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
was consulted and recommended pretreating the patient with an antihistamine and steroid to combat any incidental
exposure. The nutritionists developed a sulfite-free diet. The anesthesiologists collaborated with the pharmacists to
acquire a repository of sulfite-free medications and were able to create a portable, sulfite-free medication box, as well
as sulfite-free medication trays for the anesthesia cart in the operating room. In addition, transfusion medicine
recommended that if a transfusion were needed, it would be best to use autologous blood products, given the inability
to certify blood products as sulfite-free.
Conclusions
This collaboration involving multiple NYP departments culminated in the creation of a protocol for developing a safe
environment for patients with severe sulfite sensitivities. The diligence of this group allowed for the aforementioned
patient to have a necessary procedure done without complication. Not only was this patient discharged the same day,
this patient returned one year later for another surgical procedure at NYP/WC, where the measures that had already
been meticulously researched and established were easily re-implemented, allowing for another same day surgery to be
completed with no incident.
This sulfite-free protocol may be used for future sulfite-sensitive patients as well as patients treated at other institutions.
Quality Symposium 2012
Page 101
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
A Multidisciplinary Educational Initiative Encouraging Prescription of Generic Over Brand-Name
Proton Pump Inhibitors (PPIs) at the Time of Hospital Discharge
Karl B Bezak, MD (1); Tara F Bishop, MD MPH (1); Jennifer I Lee, MD (1); Natalie Mohammed, BSN RNC
MA CLNC (2); Lia Logio, MD (1)
(1) Department of Medicine, NewYork-Presbyterian Hospital/ Weill Cornell Medical College; (2) Division of
Medical Nursing, NewYork-Presbyterian Hospital
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Department of Medicine
Introduction
The use of proton pump inhibitors (PPIs) in the United States has increased over recent years. In 2009, 119 million
prescriptions for PPIs accounted for $13.6 billion in sales, making this class of drugs the 3rd highest moneymaker in
the United States. In 2010, esomeprazole (Nexium) alone accounted for $6.3 billion dollars in sales. Studies have
shown that generic PPIs are similarly effective and cost at least $200 dollars less per month than a comparable brandname drug.
Problem
At NewYork-Presbyterian Hospital/Weill Cornell (NYPH/WC), anecdotal evidence suggests that patients discharged
from the general medicine service on a PPI are prescribed Nexium since this is the preferred PPI on hospital formulary.
Goals
As part of an 8-week internal medicine residency quality improvement curriculum (June to August 2012), we designed
an educational initiative to increase the proportion of new PPI prescriptions of omeprazole compared to Nexium given
to patients being discharged from one general medicine unit by 40% over a 4-week period.
Methods
We convened a multidisciplinary team of Internal Medicine residents, pharmacists, and the Patient Care Director on
Greenberg 5 North to develop an educational initiative to help residents identify patients started on a PPI while
hospitalized who required a new prescription on discharge. Our intervention included a brief educational session with
all team members (interns, residents, physician assistants, students) as well as medication review by a clinical
pharmacist during interdisciplinary rounds (Figure 1). We excluded patients who were taking a PPI prior to admission.
We assessed the efficacy of our intervention by reviewing the discharge medication list for each patient discharged
from 5 North over three time periods: pre-intervention, immediately post-intervention, and 4 weeks post-intervention
(Figure 2). Cost savings was calculated using publicly available PPI cost data.
Results
In the pre-intervention period, 80% of patients were prescribed Nexium at the time of discharge. In the two weeks
immediately post-intervention, this percentage decreased to 40% of discharged patients. 4 weeks post-intervention,
Nexium was prescribed to 20% of patients newly started on a PPI. The estimated cost savings to the health care system
is $3,584/month or $43,008/12 months.
Conclusions
In two months, residents designed and implemented a simple and effective multidisciplinary educational initiative that
successfully changed PPI prescribing patterns. The effect was sustainable at least 4 weeks post-intervention and
Quality Symposium 2012
Page 102
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
represents significant cost savings to the health care system.
Quality Symposium 2012
Page 103
Quality Symposium 2012
Page 104
10/23/2012
PreͲIntervention
41 Total Discharges From 5 North General Medicine Teams:
6/25/12 – 7/9/12
Excluded: 2 patients (5%) Deceased
Excluded: 14 Patients (34%) Admitted on PPI
25 Patients (61%)
Included
20 Patients (80%) No PPI indicated
5 Patients (20%) New prescription for PPI
4 Esomeprazole (80%)
1 Lansoprazole (20%)
ImmediatelyPostͲIntervention
42 Total Discharges From 5 North General Medicine Teams:
7/10/12 - 7/21/12
4WeeksPostͲIntervention
24 Total Discharges From 5 North General Medicine Teams:
8/5/12 - 8/11/12
Excluded: 1 patients (2%) Deceased
Excluded: 11 Patients (26%) Admitted on PPI
30 Patients (72%)
Included
Excluded: 6 Patients (25%) Admitted on PPI
18 Patients (75%)
Included
20 Patients (80%) No PPI indicated
5 Patients (20%) New prescription for PPI
2 Esomeprazole (40%)
3 Omeprazole (60%)
13 Patients (80%) No PPI indicated
5 Patients (20%) New prescription for PPI
1 Esomeprazole (20%)
4 Omeprazole (80%)
Quality Symposium 2012
Page 105
1
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Improving the Rate of Resident Review of Routine Daily Electrocardiograms Ordered on Hospitalized
Patients
Adrian Mei, MD; Jennifer I Lee, MD; Cathy Collins, MS RN CCRN; Lia Logio, MD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Department of Medicine
Introduction
A patient on antipsychotic medications presented to the emergency department with recurrent syncope and torsades de
pointes, following his discharge only a few days earlier. Upon chart review of his prior hospitalization, the patient had
daily electrocardiograms (ECGs) to monitor his known prolonged QTc interval. The ECG from the day of discharge
was noted to have a severely prolonged QTc (>700 msecs). It seems the ECG was not adequately reviewed prior to
discharge.
Problem
Routine daily electrocardiograms (ECGs) are ordered on hospitalized patients for a variety of monitoring purposes
relevant to their clinical care. At NewYork-Presbyterian Hospital/Weill Cornell (NYPH/WC), residents sometimes rely
on the official interpretations of the ECGs after they are reviewed by a cardiologist rather than conducting their own
initial review. On weekdays, ECGs are available in the electronic medical record (Eclypsis) with the cardiologist’s
interpretation the afternoon they are completed. If there are abnormalities that require clinical correlation, residents are
paged directly by the cardiologist at that time.
There is a delay in both posting and communication for ECGs completed over the weekend or if they are read by the
cardiologist following a patient’s discharge. Initial review of ECGs by residents would help to improve and expedite
clinical care and help prevent the medical error illustrated above.
Goals
As part of an 8-week internal medicine residency quality improvement curriculum (June to August 2012), we designed
an intervention to improve the percentage of routine daily ECGs initially reviewed by residents to >75% on one
general medicine unit.
Methods
As part of an 8-week internal medicine residency quality improvement curriculum (June to August 2012), we designed
an intervention to improve the percentage of routine daily ECGs initially reviewed by residents to >75% on one
general medicine unit.We convened a multidisciplinary team to design an educational and workflow intervention
which we implemented on two general medicine units using Plan-Do-Study-Act (PDSA) rapid improvement cycles. A
brief educational session was held with the geographically localized resident teams on both Greenberg 5 Central (5C)
and Greenberg 5 West (5W) to remind them on a daily basis to sign and date all ECGs ordered that day for their
patients. Reminders were verbal and sent by email.
In addition, we implemented a workflow intervention on 5W. After receiving the morning order for routine ECGs for
the unit, technicians generally completed the cardiograms by 11 A.M. and place the completed studies next to the unit
clerk. Our workflow intervention included educating the technicians to place all completed ECGs in a designated bin.
The unit clerks were asked to page the general medicine team alerting them that their studies were completed. Once
Quality Symposium 2012
Page 106
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
reviewed, signed and dated by the resident, the ECGs were filed in the patient’s chart.
We conducted daily chart rounds for one week post-intervention on both units to quantify how many of the routine
daily ECGs ordered were signed and dated by the medical team indicating that they had been reviewed. We also did an
initial review of the paging logs and interviews with the residents on 5W to count the number of days pages were sent
by the clerk. Based on our preliminary findings, we added to our workflow intervention by clearly marking the ECG
bin on 5W with the pager numbers for the general medicine teams, and working with the Patient Care Director to
provide daily reminders to the unit clerk on duty. We then conducted a second round of chart reviews for one week
following our modifications.
Results
During our first data collection period, 53.8% (7/13) of routine daily ECGs ordered in 1 week for both units were
available in the patients’ charts. Of those, 1 (1/2; 50%) was signed by the resident on 5W and none were signed on 5C
(see Figure 1). Following our modification to the workflow intervention, 40% (4/10) of the ECGs we found in the
charts on 5C were signed by the resident. On 5W, where both educational and workflow initiatives were implemented,
the percentage of ECGs performed that were reviewed by residents was 100% (14/14) (see Figure 2).
Conclusions
Timely review of the routine ECGs by the medicine teams was improved when both the educational and workflow
interventions were coupled. There is a role for expansion of this project to other general medicine units. However,
success of the intervention is highly dependent on the cooperation of the unit clerks who are not consistently on the
same unit, particularly over the weekends, a vulnerable time for our patients given the delay in cardiology
interpretation of ECGs.
Another recommendation is to implement a system whereby ECGs can be scanned directly into Eclipsys with the final
read pending, similar to the way radiologic studies currently appear in PACS. This would simplify the workflow
further and allow residents to automatically access ECGs electronically once they are completed.
Acknowledgements: The authors thank the residents, unit clerks and ECG technicians for their hard work and
contributions to the study. Waridibo Allison MD, Daniel Amoruso MD, Muhamed Baljevic MD, Robert Daly MD,
Jessica Furst MD, Elizabeth Greig MD, Scott Kramer MD, Joseph Krepp MD, Lenette Lu MD, Olanma Okoji MD,
Chiti Parikh MD, Lourdes Sanso MD, David Seto MD, and Stephanie Tang MD were all members of the research team.
Quality Symposium 2012
Page 107
Quality Symposium 2012
Page 108
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
A Pharmacist-Led Intervention on Medication Education for Heart Failure Patients at Hospital
Discharge
Sharda D Ramsaroop, MD; Olga Hilas, BS Phm PharmD; Eugenia L Siegler, MD; M Carrington Reid, MD
PhD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Division of Geriatrics
Introduction
One in five patients suffers an adverse event within 3 weeks of hospital discharge; 66% are medication related. Thirtyday readmission rates average 20% for the state of NY. Also, there have been significant changes in hospital
reimbursement for patients with admitting diagnoses of heart failure (HF), acute MI and pneumonia, who are
readmitted within 30 days. Therefore, quality improvement (QI) interventions which address care needs during the
transition from the hospital are important to providing care for older adults.
Problem
Heart failure is one of the most common hospital admission diagnosis in patients age 65 and older. Patients with heart
failure have complex medication regimens. Medications are one of the greatest sources of confusion and error during
transition points. Medications frequently change during transitions; in one hospital study, 28-40% of medications were
discontinued, and 45% of the drugs prescribed on discharge were started in the hospital. Further studies show that
patients have limited recall of discharge instructions and difficulties with medication adherence after discharge.
Evidence indicates that patient education about drug regimens and chronic disease management may increase
medication health literacy and reduce hospital readmission and mortality.
Goals
The objective of this study is to implement a pharmacist-led intervention for heart failure patients which provides
medication education prior to discharge and evaluate the intervention's impact on patient outcomes.
Methods
The study was conducted on the inpatient, geriatrics, Acute Care of Elders (ACE) unit at Weill Cornell Medical Center,
NewYork-Presbyterian Hospital. The interdisciplinary team on the ACE unit consists of a geriatrics, attending
physician, two, PGY-2 Internal Medicine residents, two Physician Assistants, one clinical pharmacist, one social
worker, one care coordinator and unit nurses. This team meets daily to discuss the disposition plan for each patient.
The clinical pharmacist identified heart failure patients and interviewed them within 24 hours of admission. This
interview assessed understanding of disease and medication regimens and identified barriers to obtaining medications.
On the day of discharge, the pharmacist reviewed the medications with the patient and provided education about
medications. Any barriers to obtaining to medications were communicated to the other members of the
interdisciplinary team and methods for overcoming these barriers were pursued. The pharmacist made follow-up phone
calls to patients 48 hours after discharge and 7 days after discharge to review issues with medications.
Outcomes measures were medication discrepancies after discharge, patient satisfaction, physician receptivity, 30-day
readmissions and mortality. The pharmacist also cataloged all the tasks and time required to complete intervention and
barriers to completing the intervention.
Quality Symposium 2012
Page 109
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Results
Thus far, 34 patients have been included in the study. The average age was 80 (72-94) and the mean length of stay was
10.8 days. 56% of patient were discharged home and 41% were discharged to a skilled nursing facility (SNF).
Mortality was 3%. 9% of patients were readmitted within 30 days of discharge. 5% of patients had discrepancies in
medications at 48 hours after discharge.
The average amount of time the clinical pharmacist spent educating each patient on day of discharge was 30 minutes
(20-45 minutes). Average time spent speaking with patient by phone at 48 hours of discharge was 20 minutes (10-25
minutes) and time spent on phone call at 7 days of discharge was 15 minutes (10-20 minutes). All patients expressed
appreciation and satisfaction with the pharmacist education. The most common barrier to completing pharmacist
education was coordinating a time for the pharmacist to meet with both the patient and primary caregiver.
Conclusions
A pharmacist-led intervention to educate heart failure patients about their medications at discharge was well received.
It is a time consuming process and further study is needed to determine the full impact of this intervention.
Quality Symposium 2012
Page 110
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Apple iPads Positively Impact Clinical Care in a Busy Outpatient Resident Practice
Karl B Bezak, MD; Amanda Carmel, MD
NewYork-Presbyterian Hospital/ Weill Cornell Medical Center, Weill Cornell Internal Medicine Associates
Introduction
Recent studies have shown that Apple iPads have the potential to increase clinical efficiency, resident compliance with
duty hours, conference attendance, and improve the quality of doctor-patient interactions. Several Internal Medicine
residency programs and medical schools have incorporated iPads into inpatient care and educational programming,
however the impact of iPads in the outpatient setting are not known.
Problem
Time management and clinical efficiency are major challenges at Weill Cornell Internal Medicine Associates
(WCIMA), a busy resident outpatient clinic associated with Weill Cornell Medical College, in part, because many
patients have complex biopsychosocial problems and are often cared for by more than one resident who must also be
supervised by an attending physician. Optimizing time available for each patient while in-office and responding to postvisit concerns are crucial aspects of providing efficient care but are challenging given high clinical demands.
Goals
As part of an internal medicine residency quality improvement curriculum, we implemented a short term pilot program
of iPad use at WCIMA and aimed to show an increase in residents’ overall clinical efficiency and several clinical
factors pertaining to clinical care.
Methods
Six Internal Medicine residents rotating at WCIMA during March 2012 (2 interns, 2 junior residents, 2 senior
residents) who had not previously used an iPad in clinic volunteered to participate in this study. Each resident was
loaned an iPad with Citrix software and access to the EPIC outpatient electronic medical record (EMR) after being
given a 15 minute tutorial on operation and suggestions for efficient use in clinic. The residents utilized the iPad over a
two week period consisting of 10-12 half-day clinic sessions.
Pre- and post-study data was collected by questionnaire regarding each resident’s own perceived clinical efficacy,
access to information, ability to address patient clinical issues during each visit, and ability to address patient phone
calls/ messages. Responses were recorded utilizing a Likert Scale. Data from five residents (one senior resident did not
use the iPad) was analyzed and mean values were compared.
Results
The use of iPads increased residents’ overall self-assessed clinical efficiency, access to information, number of patient
clinical issues addressed per visit, as well as improved ability to answer patient phone calls and messages in a timely
manner.
Conclusions
iPads proved to be an effective tool in improving overall clinical efficiency in our busy outpatient resident practice as
well as optimizing a provider’s ability to provide excellent medical care.
Quality Symposium 2012
Page 111
Quality Symposium 2012
Page 112
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Interactive Patient Safety Group to Prevent Falls in a Geriatric Psychiatry Unit
Danielle Struble-Fitzsimmons, PT DPT; Kaitlyn Giordano, MS; Elizabeth DiPersia, RN MS
NewYork-Presbyterian Hospital/ Westchester Payne Whitney
Introduction
The weekly Safety Group was an original program designed by physical therapy and psychosocial rehabilitation staff
to help reduce falls on an inpatient geriatric psychiatry unit. The program was initiated in February 2012, and continues
to meet every Friday on the unit.
Problem
Unit 2N is a geriatric psychiatry unit with a high fall rate.
Goals
(1) Educate patients about fall risk factors and reduction strategies on a weekly basis.
(2) Reduce the number of overall falls on the unit.
Methods
The weekly Safety Group is a thirty minute program held each Friday on unit 2N, and is led by physical therapy and/or
psychosocial rehabilitation staff. The pre-set agenda includes three main areas for discussion: (1) safety on the unit, (2)
fall risk factors in the hospital, (3) patient safety techniques. The groups are structured through these three areas, and
allow ample time for individual patient participation. Patients are asked to respond to questions posed and also
encouraged to ask any relevant questions. Patients may choose to simply attend the group without providing verbal
feedback, as verbal participation is not mandatory.
Outcome measures require fall rate data based on the Maryland Indicator Project (calculated by # falls/patient days x
100). This project compares the fall rate for safety group participants with the overall concurrent monthly fall rate for
2N, from March 2012-August 2012.
Results
This project has shown that Safety Group participants are less likely to fall than non-participants. For this six-month
period, there were 21 patient falls on unit 2N. Of these 21 patient falls, 15 were non-participants in the Safety Group.
Only 6 of the 21 falls occurred with patients who attended the Safety Group prior to their fall (please see attached
chart).
Conclusions
The patient Safety Group is an effective tool in reducing falls. The group is well attended and patients consistently
provide positive feedback. This group does not require any additional financial resources or staffing. It can easily be
incorporated into all inpatient unit schedules. We would like to recommend incorporating this program into all
inpatient units at Payne Whitney Westchester.
Quality Symposium 2012
Page 113
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Utilization of Electronic Medical Record Data to Re-Engineer Work Flow, Increase Departmental
Efficiency, Capacity and Increase Patient Safety
Elizabeth Coughlin BSN MPA CIC (Director of Infection Control); F Cole Caulfield III EMT (Quality
Management Infection Control Associate); Maryanne Carollo, BS RN CAPA (Patient Care Standards)
Northern Westchester Hospital
Introduction
On April 27, 2004 President Bush issued Executive Order 13335 which called for widespread adoption of interoperable
electronic health records (EHR) within 10 years. Included in this directive was the mandate that quality improvement
and Infection Control data be HIPPA compliant, portable and interoperable internally as well as with external
institutions and agencies while increasing the patient safety. This initiative was codified by The Health Information
Technology for Economic and Clinical Health (HITECH) Act of 2009 which set forth prescriptive definitions of EMR
"meaningful use". In a recent survey by the American Health Information Management Association (AHIMA) it was
noted that between 17-20% of hospitals nationwide have extensively implemented interoperable health information
systems.
Problem
The Hospital implemented a robust electronic medical record almost eight years ago. The platform has evolved and
matured over the intervening years of use and is meeting the challenges of phase 1 "meaningful use" validation with
considerable success. This substantial source of data has been under-utilized as a means of streamlining processes of
data acquisition by the department of Infection Control. Efficacious use of all available resources is imperative in the
context of the current health care environment wherein there are ever increasing demands for near real time data by
regulatory agencies and concomitant fiscal constraints.
Hospital acquired infections (HAIs) are the second most frequent adverse patient event making accurate, effective and
efficient surveillance methods pivotal to identifying these important patient safety issues. The earliest identification
and rapid formulation of evidence based interventions are essential in assuring a safe patient care environment. CMS &
The Joint Commission on Hospital Accreditation, have recognized that the presence of invasive medical devices are a
major risk factor for the development of HAIs. Subsequently these regulating bodies have mandated hospital wide
surveillance of devices such as indwelling urinary catheters and central lines as well as the daily assessment of their
medical necessity ,analysis of utilization rates and device associated infections.
Due to the labor/resource intensive, nature of daily surveillance and error prone process manually counting of these
devices throughout all inpatient units, the Department of Infection Control at Northern Westchester Hospital
implemented methods of extracting, and transforming of siloed data from separate unidirectional modules within the
EHR.
Goals
1. Increase departmental efficiency 25%.
2. Increase departmental capacity by 25%.
3. Improve patient safety through early identification of individuals with indwelling urinary and central venous
Quality Symposium 2012
Page 114
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
catheters.
4. Increase staff awareness of the presence & appropriate use of these devices.
5. Assure earliest possible discontinuation of indwelling urinary and central venous catheters.
6. Identify opportunities for improvement in processes and patient care.
7. Normalization and integration of data into actionable form.
8. Increased consistency and accuracy of data.
9. Produce a dovetail data integration product in alignment with NWH "Meaningful Use" efforts to increase internal
external interoperability.
Methods
Using a combination Structured Query Language and Visual Basic a set of instructions are triggered at a specified time
each day automating query executions and report generation. These automated processes are know as Macros. Multiple
discrete fields from 2 siloed (non-communicating) modules, the financial and the patient care modules, were queried
for the necessary data points every day and saved in 3 separate text-delimited reports.
• Patient Care Module System, Nursing Assessment, voiding method field equal to "Indwelling Catheter".
• Patient Care Module System, IV Site/Invasive Line Record equal to "PICC", or "Central Line" or "Mediport" or
Dialysis Catheter".
• Additional data points gathered in extraction from Patient Care System Device reports include:
• Location
• Last Name
• First Name
• Medical Record Number
• Date of Insertion
Financial Module, Inpatient Location Statistics data points extracted include:
• Location
• Patient days per location
Data then imported into an Excel spreadsheet for tabulation and further analysis.
Results
Prior to implementation of this solution, an average 20 man-hours per week or nearly 27% of total personnel/labor
resources were allocated and diverted to the manual tracking of devices across 14 medical-surgical units. Weekends
and holidays posed a particular challenge in that alternate staff, (usually already extended nursing staff) were requested
to collect the device data. Assuring consistency of the data with less than optimally trained, auxiliary staff gathering
off-hour data points is a challenge nearly impossible to meet. The implementation of our quasi-data data mining
process facilitates access of data points by bridging the isolated modules within the NWH EHR and creates reciprocity
where none existed. The Department of Infection Control has increased their capacity and flexibility by freeing
essential resources (man hours) allowing energies to be redirect in addressing the myriad of other concerns placed upon
it by rapidly evolving requests for near-real time information. An additional benefit from this re-engineering is the
transformation of the data to a delimited format accessible across both internal and external platforms uniformly.
Further, the Department of Infection Control has been able to drill down daily to the patient level on all devices for the
past year. During that time, the Department has been enabled to conduct granularly focused education and surveillance
Quality Symposium 2012
Page 115
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
interventions, across the institution. Simultaneously indwelling urinary catheter usage has decreased by greater than
50% (n=23% ~ n=12%).
Finally, during the augmented IC efforts the CA-UTI rate decreased from 4/1,000 patient days to 0.8/1,000 patient
days; equivalent to an 80% decrease in the rate of CA-UTIs through the 2nd quarter 2012. An overall estimate of
monetary savings reflected in these outcomes is approximately $100,000 in 2007 dollars adjusted Consumer Price
Index in avoidance of device related infections alone. There were $2,150 monthly labor costs that were redirected into
high impact patient and device safety interventions.
Conclusions
This somewhat ambitious project, based on frugality, utility and flexibility proved well worth the many painstaking
hours of work of testing and validating our methods and resulting data alike. The designed IT integration solution
provided accurate, actionable data so that risks of these devices could be minimized. Patient level data is reviewed and
acted on by IC addressing a very important patient safety concern. In addition to monetary savings this effort has
prevented additional morbidity and mortality.
We stand on soft, shifting sands in the face of rising demands for quality care within an environment of increasingly
limited health care resources. We are shadowed by mounting mandates for the digital submission of data driven
processes and outcome information. The Health care continuum resonates with change as it struggles to comprehend
exponential complexities in the evolving health care delivery system. There are enormous multi-faceted gains to be
attained through the application of the formats and directives of Meaningful Use.
Quality Symposium 2012
Page 116
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Improving Performance in Appropriate Administration of Perioperative Beta Blockers
Marla Koroly, MD; Kate O'Keefe, RN MSN FNP; Melissa Hershfield, RNC
Northern Westchester Hospital
Introduction
Perioperative cardiovascular (CV) complications, such as myocardial infarction, pulmonary edema, dysrhythmia, or
CV death, occur in ~1.4% of patients undergoing non-cardiac surgery. Preoperative revascularization to lower the risk
of surgery is generally not recommended unless such intervention is indicated irrespective of the preoperative context.
One of the few interventions that may reduce the risk of perioperative CV complications is the use of Beta Blockers,
though studies have been conflicting. Five randomized controlled trials of preoperative Beta Blockers showed a
reduction in mortality and/or myocardial infarction with atenolol (10% vs. 21%), bisoprolol (12% vs. 32%) and
esmolol/metoprolol (2% vs 6%) in populations with various CV risk levels. Three more recent randomized controlled
trials did not show any improvement in in-hospital or 30 day CV events with metoprolol and in some cases led to
significantly increased harm related to symptomatic bradycardia, hypotension, and ischemic stroke. The POISE trial
evaluated 18,351 patients with 3 or more CV risk factors undergoing non-cardiac surgery and found that for every
1,000 patient, perioperative Beta Blockers will prevent 15 MIs, 3 revascularizations, and 7 atrial fibrillation events, but
led to an excess of 8 deaths, 5 disabling strokes, 53 hypotension events, and 42 bradycardia events. Despite all of this
conflicting data, all of the studies have consistently shown a significant net benefit in those patients who are already
receiving Beta Blockers for angina, symptomatic arrhythmias, hypertension, or other indications. The ACC/AHA
therefore recommends continuing Beta Blockers perioperatively in this patient population as a Class I recommendation.
Problem
Many patients who are on Beta Blockers do not receive them perioperatively, which increases their risk of CV events.
The reasons for discontinuation of their Beta blockers often relate to inadvertent system and communication failures
and therefore provide an opportunity for improvement. The compliance in 2009 was 99% however this then dropped to
93% in 2010. By 2011, compliance had improved to 97% however the goal was 100%. As Value Based Purchasing
(VBP) and third party "Pay for Performance" programs link quality of care to payment it is imperative that
organizations achieve the goals set forth by the Centers for Medicare and Medicaid (CMS).
Goals
• Implement process improvements consistent with best practice to support the physician and nursing staff.
• Engage the physician/ nursing staff and establish "ownership" of the appropriate use of perioperative use of Beta
Blockers.
• Support the medical and nursing staff through the use of technology.
• Administer perioperative Beta Blockers to 100% of patients who are already receiving Beta Blockers and have no
documented contraindication.
Methods
Through the efforts of a multi-disciplinary team (Nursing, Anesthesia and Pharmacy), beginning in the 4th Quarter of
2011, the following strategies were developed to create a multi-pronged approach to ensure 100% compliance with the
appropriate administration of Beta blockers in the perioperative setting:
1. Development of a flow map identifying the patient movement throughout the perioperative process thereby
Quality Symposium 2012
Page 117
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
discovering gaps and opportunities for improvement.
2. Revised anesthesia documentation to ensure documentation of a history of Beta blockers and last dose taken.
3. Created a hand off communication tool that included Beta blocker history and last dose taken in conjunction with
three other network hospitals. This hand off communication tool was then refined to be consistent with the
methodology of the LifeWings patient safety initiative implemented in the surgical services department. The checklist
follows the patient through the perioperative period (Pre-admission testing through discharge/transfer to the floor/ICU)
and is used for hand off communication at each transition of care.
4. Pharmacist review of home medications pre-operatively in addition to reconciliation with postoperative orders.
5. Educational sessions with Surgical Services nursing staff and Anesthesiologists regarding perioperative Beta
blockers.
6. Education of all staff in new employee orientation and annual competencies regarding Inpatient and Outpatient
Quality Measures.
7. Collaboration among the treating team (RNs, MDs and Pharmacists) to create "ownership" of the Beta blocker
Inpatient Quality (SCIP) Measure.
8. Optimized technology:
• Developed perioperative checklist initiated preoperatively that includes the information regarding patient history of
Beta blockers and last dose taken;
• Created standardized order sets for physician computerized order entry.
9. Review of outliers - mini root cause analysis - to identify opportunities for improvement.
10. Engaging the Anesthesiologist group by presenting core measure data, oppportunities for improvement and
successess at the monthly Anesthesia QI meeting.
11. Performance based variable compensation for all physician and staff leaders.
Results
As a result of the strategies developed and implemented, the post intervention scores for 2012 have been 100%
reflecting consistent compliance with the administration of Beta blockers.
Conclusions
The most dramatic effect was the result of Anesthesia physician staff engagement in establishing ownership of the
measure. Although the Nursing staff and Pharmacists were key members of the team, it was not until the
Anesthesiologists took "ownership" that the scores reflected consistent improvement. In so doing, the organization
remains true to the mission and goals of ensuring quality care for the surgical patients with cardiac disease. There are
ongoing challenges of maintaining consistent practice in a setting of staffing turnover which will be addressed through
ongoing diligence and monitoring of the quality data.
Quality Symposium 2012
Page 118
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Implementation of a Bar-Coded Label System for the Management of Expressed Breast Milk,
Neonatal Services
Anna Lane, BSN RN-C (Staff Nurse-NICU Level IV); Diwata Delarosa, BSN RN-CD; R Mendoza (Staff NurseNICU Level IV); R Perez, RPh (Pharmacist); R Rosenberg, BS MS (Clinical Information Specialist)
Northern Westchester Hospital
Introduction
The purpose of the program is to improve practice, quality, and prevent errors in the administration of stored breast
milk through the application of a bar-code system and bedside medication verification. Using an interdisciplinary
approach and the principles of medication administration, a process was developed to adapt the bar coded label system
to improve the efficacy of stored expressed breast milk (EBM) administration. A work flow algorithm was developed
to define the process steps and user accountabilities. A physician's order initiates the process and generates the first
EBM bar-code labels. Parental involvement is essential to the appropriate identification of EBM. The parent receives
the bar-code labels from the nurse after two identifiers, name and birth date, are verified. It is the responsibility of the
parent to label each EBM container with a bar-code label and the date and time of pumping. The nurse is accountable
for scanning EBM into the electronic medication record at the bedside. A corresponding policy was approved and
distributed. A staff competency tool was completed prior to the implementation of the new process.
Problem
The greatest risk identified in the literature and supported by data is infant misidentification. A common
misidentification error in the NICU involves feeding a mother’s EBM to the wrong infant. In a study conducted by
Gray et al. in a 40-bed NICU in Massachusetts over one year, it was determined that, "Not a single day was free of risk
for patient misidentification." Gray et al. also cited results from the Vermont Oxford Network, a voluntary errorreporting system conducted for one year, in which 25% of reported misidentification errors (i.e., 11% of 1,230
submitted reports) involved EBM (PA-PRSA 2007). These factors included "incorrectly labeled specimens, difficult-toread handwritten specimen labels, errors in verification of patient/aliquot identification, and systematic problems with
the way EBM aliquots are stored."
Goals
• To decrease the potential for administration errors and improve patient safety in the neonatal population.
• To adapt and implement a bar coded label system utilizing IT and a bedside medication verification process in NICU.
• To assess and redesign the workflow process of breast milk management.
• To increase parental confidence that the infant is receiving the correct breast milk.
• To increase nurse efficiency at the bedside.
Methods
• Conceptual framework: Evidence based practice. The process involves identifying a clinical problem or question at
the point of care. A systematic literature or evidence search to identify current best practices, and interpretation of the
patient’s needs and perspectives when making clinical decisions.
• Interdisciplinary approach for addressing clinical practice. This project included Registered Nurses at the point of
care, pharmacy, and information technology. Ongoing support from Senior Hospital Management
• A "Just Culture" approach to safety, quality and outcomes
Quality Symposium 2012
Page 119
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Life cycle of a quality improvement project: Innovation, Pilot, Implementation, Spread using Small tests of change
(PDSA)
• The Human Side of Quality Management: overcoming resistance to change; culture change versus process change
• Real time education based on adult learning principles
• Measurement: creating a data collection process and using the data to support the change process
• Communication and Safety Principles to develop highly functioning healthcare teams (Team STEPPS/AHRQ).
• Ongoing and visible support from senior management
• Clear communication and teamwork
• Data available to staff at the point of care to support the significance of the project and the staff nurses role in quality
and safety outcomes for their vulnerable population
• Ongoing education
• An process to identify non-adherence and management involvement in employee counseling and remediation
Results
• Initial compliance after 4 weeks of the new process was 92%.
• Data were tracked and after 10 months of the new process, scanning compliance was 99.4%. The compliance goal is
100%.
• Through analysis of the data, documentation standards were assessed and potential points for documentation errors
were identified and addressed through ongoing support and education.
• Nurses recognized the significance of applying quality and safety principles to express breast milk verification and
supported the process.
• Ongoing education is necessary to maintain a sustainable project.
• Through collection of data for this project, other processes were identified for assessment and remediation.
Conclusions
The project has lead to the development of a sustained bar-code labeling system for the NICU. Ongoing data
collection describes a compliance rate of 99.4%. The entire NICU teams shares responsibility for ensuring adherence to
the process. The project has also helped the staff to identify other potential areas for quality improvement.
Next Steps:
• Ongoing data collection and dissemination at the point of care
• Translation of this project to the administration of other body fluids including blood and blood products.
• Expansion of the scope of the project to include other clinical units.
Quality Symposium 2012
Page 120
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
A Patient Food Service Program Called "Food is Care" Focused on Quality, Education and Service,
Featuring Freshly Prepared, Healthy Meals, Delivered When Patients Want, with Real-Time
Nutrition Education
Maria Hale, MBA
Northern Westchester Hospital
Introduction
Production based institutional models to hospital food have become commonplace because they maximize food
production while minimizing cost. However, a sole focus on cost and productivity runs the risk of poor quality and
patient dissatisfaction. In today’s healthcare arena, patients want to be active participants in their healthcare and
demand hospitals to do more than address acute problems. Patients want a wellness plan for post hospitalization
success; they want to stay healthy and out of the hospital-the same goal as the hospital! Focus on creating a robust food
program is paramount to a successful patient wellness plan as well as readmission re-reduction strategy. As hospitals
are beginning to be financially penalized for avoidable readmissions, it is increasingly important for them to consider
ways to ensure patients are educated, informed and prepared to manage their health and diet upon discharge.
The "Food is Care" program was developed and includes a room service component in which patients order what they
want when they want it. However, by emphasizing the necessity of partnerships between dietary staff, physicians,
nursing and patients, "Food is Care" goes beyond simply enhancing customer service, focusing instead on patient care
quality.
Although there is currently no question on the HCAHPS survey that specifically references patients’ perceptions of the
food services program, recent studies suggest that satisfaction with food may be a driver of how the patient rate their
experience overall, which is captured by the HCAHPS survey.
Problem
Patient food was production based; based on the needs of the staff and kitchen rather than the patient. Food arrived at
predetermined times, menu selections were limited; Diet order process was very cumbersome with too many choices
for physicians to select from; Delays in progressing diet orders caused many return trays, lost trays or delays in
receiving trays; Food was prepared in large batches and re-heated rather than freshly prepared; Delivery of food was
done at a time where the patient may not be ready to eat (at a test, not positioned properly) all resulting in patient
dissatisfaction. Press Ganey Scores hovered around the 30th percentile nationally for patient satisfaction with food; a
complete contrast to the overall patient satisfaction which was in the top 5th percentile. The Hospital made the redesign
of patient food a top priority.
Goals
• Meals are freshly prepared with plenty of variety
• Patients have choice and control over the delivery time and meal selections
• Patients would have clinical education about their diet available in their room and through interactions with specially
trained staff; nutrition associates and dieticians
• The Unit Staff; the Patient Care Associates would be the Patient’s Food Advocate; providing guidance, support and
Quality Symposium 2012
Page 121
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
ensuring adequate nutrition
• The new model would be effective and financially sustainable as well as replicable
Methods
"Food is Care" includes a room service component in which patients order what they want when they want it.
However, by emphasizing the necessity of partnerships between dietary staff, physicians, nursing and patients, "Food
Is Care" goes beyond simply enhancing customer service, focusing instead on patient care quality.
To achieve this, a redesign of Food Service was necessary which included the following elements:
• Patient Focus Groups to identify patient expectations of food and nutrition in a hospital setting.
• Best Practice Site Visits to high performing Hospitals and Hotels (The Ritz-Carlton).
• Use of Industry Experts - The Culinary Institute of America (CIA) was utilized to train cooks on how to cook freshly
prepared made to order meals.
• Recruitment of Executive Chef, a CIA graduate.
• Process Mapping methodology used to map out current and redesigned processes.
• Multidisciplinary Committee of dieticians, nurses, physicians, patients, patient care associates and administrators to
redesign process in a patient centered manner.
• Food and Nutrition Advisory Group formed of culinary, restaurant industry and clinical nutritional industry experts
to guide the Hospital and provide on-going feedback.
• Nurses and physicians streamlining diet orders and ensuring accurate and timely entry of diet orders.
• Patient Care Associates ensure patients order, delivery of meals and ensure patients are comfortably positioned and
ready to enjoy their meal, assist with feeding and confirm adequate intake.
• Food Service prepares all meals made-to-order and delivers meal trays to patient units.
• A dedicated Call Center, with Nutrition Associates, take patients' food orders, providing on-the-spot-clinical
nutrition education (using dietary software called CBORD) guiding patients to menu options best for their diet and
general health.
• Technology - Kitchen and unit needed real time communication channel to address issues; implementation of Vocera
(point to point communication system).
• Meals are delivered within 45 minutes from the time of order; with the goal of providing patients choice, control and
ability to enjoy a healthy meal - receiving the nutrition needed to aid in healing and recovery.
• A commitment to purchasing locally grown when available. Dedicated community committee formed to create a
sustainable food aggregator to assist with group purchasing from local and regional farms to address needs of the
hospital and its community partners.
• Hospital signed "Healthcare without Harm Food Pledge" blueprint for sustainable strategies in Hospital Food
Service.
• Kitchen infrastructure (Cooks line, air curtains) all purchased with highest energy efficiency rating.
• Cyrovac machine purchased to maximize freshness and and accessibility.
• Onsite herb and perennial garden; herbs used for cooking and aromatherapy program; perennials used to garnish
patient trays.
Results
• Successfully deployed to Medical Surgical Units, Maternity and Behavioral Health Unit and Infusion Therapy
• Meals delivered within 45 minutes of patient order.
• Food waste significantly decreased since implementing initiative.
Quality Symposium 2012
Page 122
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Positive Patient Comments on:
• The diverse in-room menu and nutrition guidelines
• Speaking with a specially trained nutrition associate
• Being able to eat what and when they want; many choosing to eat more frequent smaller meals
• Visitors being able to order from the menu and eat with the patient
Data: Program Launched 1/2012
Question 2011
Temperature of the food Mean - 78.4
Quality of the food
Mean - 75.9
Rank - 32
Rank - 48
Question YTD 2012
Temperature of the food
Quality of the food
Rank - 81
Rank - 89
Mean - 83.5
Mean - 81.5
Source: Press Ganey
Conclusions
• A Hospital Food Service Redesign is very complex; many moving parts, diverse staff; complex order entry, patient
movement; replacement of an aging production based kitchen infrastructure; the build of a clinical nutrition software to
ensure efficiency, quality and safety - all need to be in place - budget adequate time
• Lots of Training! - Cooks shifted from large production to restaurant style-made to order preparation; patient care
units had to adjust workload to be ready to deliver trays arriving at differing times
• A commitment to purchasing locally grown when available. Dedicated community committee formed to create a
sustainable food aggregator to assist with group purchasing from local and regional farms to address needs of the
Hospital and its community partners;
• Food waste significantly decreased since implementing initiative
The "Food is Care Program" has recently been featured on Eyewitness News by Dr. Sapna Parikh;
http://abclocal.go.com/wabc/story?section=news/health&id=8619813 as well as featured other publications such as
Edible Hudson Valley; as well as guest lecturers at the Culinary Institute of America for students interested in entering
the healthcare market.
Next: The hospital will continue to evaluate the program and continue to make it more efficient and cost effective
without compromising quality. Next on the horizon, program expansion to intensive care and the emergency
department as well as room service for staff.
Quality Symposium 2012
Page 123
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Improving Blood Culture Contamination Rates in a Community Hospital
S Laduca, RN (Emergency Department); B Wilson (Director Laboratory)
Northern Westchester Hospital
Introduction
The purpose of the program is to improve practice, quality, and prevent contamination in blood cultures. Using an
interdisciplinary approach, a PICOT question was developed to identify the best practices and current evidence related
to the reduction of blood culture contamination. A literature search was conducted and through a shared governance
model of nursing, it was identified that the use of chlorhexadine could decrease blood culture contamination rates
based on the literature assessing the use of chlorhexadine with central venous access devices (CVADs). Benchmark
data was obtained which showed that 64% of blood cultures at NWH were drawn in the Emergency Department. The
contamination rate with Emergency Department collection was 5.2%. The Emergency Department supported the work
of the EBP Council to reduce blood culture contamination.
Problem
Do patients have a reduced risk for blood culture contamination when Chlohexadine products are used for skin
preparation?
Goals
• Reduce the level of blood culture contamination in a community hospital.
• Reduce health care costs.
Methods
• Conceptual framework: Evidence based practice. The process involves identifying a clinical problem or question at
the point of care. A systematic literature or evidence search to identify current best practices, and interpretation of the
patient’s needs and perspectives when making clinical decisions.
• Interdisciplinary approach for addressing clinical practice. This project included Registered Nurses at the point of
care, the laboratory, and a MSN and a doctorally prepared nurse to mentor the project.
• Ongoing support from Senior Hospital Management
• A "Just Culture" approach to safety, quality and outcomes
• Life cycle of a quality improvement project: Innovation, Pilot, Implementation, Spread using Small tests of change
(PDSA)
• The Human Side of Quality Management: overcoming resistance to change; culture change versus process change
• Real time education based on adult learning principles
• Chloraprep kits were obtained and placed in the Emergency Department.
• A corresponding policy, based on the literature, was approved and distributed.
• An educational program and a staff competency tool were completed prior to the implementation of the new process.
• Measurement: creating a data collection process and using the data to support the change process
• Communication and Safety Principles to develop highly functioning healthcare teams (Team STEPPS/AHRQ).
Results
• Initial results after 4 weeks of the new process demonstrated a 8% contamination rates of blood cultures when
Quality Symposium 2012
Page 124
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
provodine iodine was used for skin preparation (n=424).
• Blood cultures that were collected when 2% Chlorhexadine and 70% Alcohol was used, demonstrated a
contamination rate of 0.00% (n=110).
• Ongoing data analysis demonstrates that the 2012 blood culture contamination rate was the lowest to date at 1.1%.
Conclusions
The use of Chlorhexadine significantly reduced the blood culture contamination rate at a community hospital. Through
analysis of the data, documentation standards were assessed and potential points for documentation errors were
identified and addressed through ongoing support and education. Nurses recognized the significance of applying
quality and safety principles to the blood culture collection process and took ownership of the process. Staff embraced
the opportunity to improve outcomes for our patient population and implemented the process into clinical practice.
Effective teamwork and communication assured compliance with best practices and a significant reduction in blood
culture contamination. The practice is routinely accepted and used however ongoing data collection is necessary to
sustain the project. Ongoing education is necessary to maintain a sustainable project.
Quality Symposium 2012
Page 125
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The Sustained Impact of a Process to Reduce Blood Culture Contamination Rates in a Community
Hospital
D Lajoie, RN MSN PhD(c) (Asst. Director of Research, EBP & Special Projects); Betty Wilson (Directory
Laboratory Services); Mike Zerbo, RN (Emergency Department); K Lawton, RN BSN (Director Emergency
Department)
Northern Westchester Hospital
Introduction
Blood cultures contribute to the diagnosis and treatment of patients with serious, possibly life threatening
illness/infections. Outcomes of blood culture contamination is measured in both human and financial terms, and is
associated with potentially unnecessary antibiotic administration as patients with positive blood culture must be treated
immediately. An increased length of stay including additional hospital, pharmacy and laboratory charges, as well as an
impact on patients' quality of life is seen. According to the American Society for Microbiology, the acceptable standard
for blood culture contamination should not exceed 3%. Blood culture contamination represents a costly, preventable,
system failure for hospitals. Studies (Bates et al, 1991; Schifman, 1998) had described that the cost associated with
contaminated blood cultures was approximately $5,000 per patient and was associated with an additional length of stay
of 4.5 days. A 2006 study by Zwang and Albert (Tepus, Fleming, Cox, Hazlett, & Kropp) showed that false positive
blood culture results were associated with an extra 1,450-2,200 extra hospital days per year at an annualized cost of
$1.4 to $1.8 million ($8,750/patient).
Problem
The purpose of the program is to improve practice, quality, and prevent contamination in blood cultures. Using an
interdisciplinary shared governance approach , a process was developed to identify the best practices and current
evidence related to the reduction of blood culture contamination. After implementation of the process in the
Emergency Department, results demonstrated that chlorhexadine was associated with a significant decrease in blood
culture contamination rates. Sustained data collection showed that contamination rates were 1.1%. It is known that the
reduction of blood culture contamination rates is associated with significant hospital cost savings. The purpose of this
study is to describe the cost savings of a sustained process to reduce blood culture contamination rates in a community
hospital.
Goals
• To reduce the blood culture contamination rate to less than 3%.
• To demonstrate the cost savings associated with a sustained process to reduce blood culture contamination.
Methods
A initial project was developed by S. Laduca, RN (Emergency Department), to hardwire the use of chlorhexadine as a
skin preparation for all blood culture draws. The problem of blood culture contamination originating in the Emergency
Department was identified by the care providers at the point of care. A literature search identified that the use of
chlorhexadine could decrease blood culture contamination rates based on the literature assessing the use of
chlorhexadine with central venous access devices (CVADs). Benchmark data was obtained and showed that 64% of
blood cultures at NWH were drawn in the Emergency Department. The contamination rate with Emergency
Department collection was 5.2%. The Emergency Department supported the work of the EBP Council to reduce blood
Quality Symposium 2012
Page 126
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
culture contamination. Initial results after 4 weeks of the new process demonstrated a 8% contamination rates of blood
cultures when provodine iodine was used for skin preparation (n=424).
Chlorhexadine kits were obtained and placed in the Emergency Department. A corresponding policy, based on the
literature, was approved and distributed. An educational program and a staff competency tool were completed prior to
the implementation of the new process.
Blood cultures that were collected when 2% Chlorhexadine and 70% Alcohol was used, demonstrated a contamination
rate of 0.00% (n=110).
Phase 2:
Ongoing blood culture contamination rates were collected by the laboratory through a quality improvement initiative
led by B. Wilson. This data is used to calculate the financial cost reductions associated with a sustained process to
reduce blood culture contamination led by D. Lajoie.
• Conceptual framework : Evidence based practice. The process involves identifying a clinical problem or question at
the point of care. A systematic literature or evidence search to identify current best practices, and interpretation of the
patient’s needs and perspectives when making clinical decisions.
• Interdisciplary approach for addressing clinical practice. This project included Registered Nurses at the point of care,
the laboratory, and and a doctorally prepared nurse researcher.
• Ongoing support from Senior Hospital Management
• A "Just Culture" approach to safety, quality and outcomes
• Life cycle of a quality improvement project: Innovation, Pilot, Implementation, Spread using Small tests of change
(PDSA)
• The Human Side of Quality Management: overcoming resistance to change; culture change versus process change
• Real time education based on adult learning principles
• Measurement: creating a data collection process and using the data to support the change process
• Communication and Safety Principles to develop highly functioning healthcare teams (Team STEPPS/AHRQ).
• Cost benefit analysis
Results
• Initial results after 4 weeks of the new process demonstrated a 8% contamination rates of blood cultures when
provodine iodine was used for skin preparation (n=424).
• Blood cultures that were collected when 2% Chlorhexadine and 70% Alcohol was used, demonstrated a
contamination rate of 0.00% (n=110).
• Ongoing data analysis demonstrates that the 2012 blood culture contamination rate was the lowest to date at 1.1%.
The initial data demonstrates that an 8% contamination rate (n=424) is associated with an additional cost of $296,800.
Reduction of this rate of contamination to 3% would result in an cost savings of $185,500 during a 1-month period.
The use of Chlorhexadine significantly reduced the blood culture contamination rate at a community hospital.Staff
embraced the opportunity to improve outcomes for our patient population and implemented the process into clinical
practice. The practice is routinely accepted and used.
Quality Symposium 2012
Page 127
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Ongoing data analysis is needed to sustain to sustain the project and to demonstrate the impact of a small practice
change at the bedside. Significant costs savings are demonstrated through the use of chlorhexadine to reduce blood
culture contamination.
Conclusions
• Effective teamwork and communication assured compliance with best practices and a significant reduction in blood
culture contamination.
• Ongoing education is necessary to maintain a sustainable project.
• Nurses recognized the significance of applying quality and safety principles to the blood culture collection process
and took ownership of the process.
Significant patient and cost benefits are seen with the use of chlorhexadine as a skin preparation for blood culture
draws.
Quality Symposium 2012
Page 128
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Pharmacodynamic (PD) Profiling of Ceftriaxone 1g and 2g daily in Critically Ill Septic Patients with
Normal Renal Function to Severe Renal Impairment
Andras Farkas, PharmD; Rachel Sussman, PharmD
Nyack Hospital
Introduction
Ceftriaxone (CRO) is a well tolerated, primarily renally eliminated cephalosporin antibiotic. We aimed to describe the
effects of renal function on the Probability of Target Attainment (PTA) of CRO in critically ill patients with sepsis.
Problem
N/A
Goals
N/A
Methods
Published population pharmacokinetic (PK) data for CRO in critically ill patients with sepsis was used in this analysis.
Free CRO concentrations were calculated using a single binding site model equation and in vivo binding parameters.
CRO 1g and 2g daily were evaluated for PTA with Monte Carlo simulation (MCS, n=5,000) at the renal function
categories from 20 to 140 ml/min for MICs up to 8 mg/L targeting the PK/PD index of ƒT>MIC from 25% to 60%.
Results
CRO 1g daily dose is expected to achieve at least 90% PTAs up to an MIC of 1 mg/L at all renal function categories
for all targets evaluated. The PTA at this MIC is likely to be suboptimal at the renal function of greater than 140
ml/min targeting a ƒT>MIC of 60%. At the ƒT>MIC of 50% and the MIC of 2 mg/L, the PTA achieved by the 1g dose
is expected to be suboptimal for all patients with renal function higher than 60 ml/min. To adequately reach MICs of 4
mg/L at the ƒT>MIC of 25%, CRO 1g daily should only be used in severe renal impairment. CRO 2 g daily is expected
to achieve greater than 90% PTA at the MIC of 4 mg/L targeting a ƒT>MIC of 25%, and similarly high PTAs at the
MIC of 2 mg/L targeting a ƒT>MIC of 50% of the dosing interval across all renal function categories evaluated.
Conclusions
In critically ill patients with sepsis the use of CRO 1g daily should provide adequate exposure when treating isolates
with MICs of 1mg/L or less. When achieving the ƒT>MIC of 60% is desired at this MIC, at least 2 g daily CRO should
be considered for all patients with renal function greater than 140 ml/min. CRO 2g daily is also likely to provide
superior PTAs when treating organisms with MICs greater then 1 mg/L as compared to the 1g daily dose across the
renal function categories evaluated here.
Quality Symposium 2012
Page 129
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Dosing of Daptomycin in the Morbidly Obese: Which Body Weight is It?
Andras Farkas, PharmD
Nyack Hospital
Introduction
Dosing Daptomycin (DAP) based on total body weight is expected to result in higher drug exposure in the obese
patient compared to patients with normal body weight. Prior analysis using population pharmacokinetics and Monte
Carlo simulation (MCS) suggested the use of lean body weight for dosing of DAP in the obese, but provided no
analysis for the population of morbidly obese. The objective of our study was to assess for the bases of using
alternative body weight estimations for dosing of DAP in the morbidly obese.
Problem
N/A
Goals
N/A
Methods
Published DAP pharmacokinetic data of matched morbidly obese patients with subjects of normal body weight was
used in this analysis. Dosing of DAP based on total (TBW), ideal (IBW), adjusted (ABW), lean (LBW), and fat free
(FFW) weight of 4 and 6 mg/kg doses were evaluated with MCS (n=10,000) to assess for the magnitude of drug
exposure. The dosing methods that resulted in the magnitude and dispersion of AUC0-24 most similar to that of the
matched normal body weight patients was then compared with the exposure achieved by the patients in the trial of
bacteremia and endocarditis.
Results
Dosing based on ABW best approximates the exposure at the dose of 4 mg/kg in the morbidly obese when compared to
the matched subjects. Simulated mean AUC0-24 values of dosing DAP based on IBW, LBW, and FFW were 19.5%,
18.7%, and 13.1% smaller, respectively, in the morbidly obese compared to the patients with normal body weight.
Simulated exposure provided by DAP 6 mg/kg based on ABW with correction factors of 0.4 in the morbidly obese
provide slightly more robust mean + SD AUC0-24 of 601 + 166.2 mg.h/L when compared to the population of the
bacteremia and endocarditis clinical trial.
Conclusions
We conclude that dosing of DAP based on IBW, LBW, and FFW would result in sub-optimal exposure based on the
simulated AUC0-24 values in the morbidly obese. Since the pharmacodynamic index most likely predictive of
outcomes is the ratio of AUC/MIC, dosing of DAP based on IBW, LBW or FFW should be avoided in this population.
Instead, dosing based on ABW can be considered in the morbidly obese.
Quality Symposium 2012
Page 130
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Pharmacodynamic Profiling of Prolonged Infusion of Ertapenem in Critically Ill Patients with Early
Onset Ventilator Associated Pneumonia Using Monte Carlo Simulation
Andras Farkas, PharmD
Nyack Hospital
Introduction
Ertapenem (ERT) is a broad spectrum carbapenem antibiotic with nonlinear protein binding characteristics best
described by a two class binding site model. The effect of prolonging ERT infusion time on the Probability of Target
Attainment (PTA) is currently unknown. The aim of our study was to describe the PTA of prolonged infusion ERT at
doubling MICs.
Problem
N/A
Goals
N/A
Methods
Published population pharmacokinetic data for ERT in critically ill patients with early onset VAP was used in this
analysis. Free ERT concentrations were calculated using the previously validated two class binding site model and
measured protein concentrations. Standard dose of 1 g ERT was evaluated for PTA with Monte Carlo simulation
(MCS, n=5000) using 0.5-, 1-, 2-, 3-, and 4-hour infusion times at doubling MICs for bacteriostatic (20%) and
bactericidal (40%) ƒT>MIC targets. Additionally, 0.5 g at 12 h interval infused over 0.5 h was simulated to evaluate
for the impact of more frequent administration on attaining the desired pharmacodynamic target.
Results
ERT 1g PTAs to achieve bacteriostatic effect were more than 90% up to an MIC of 0.5 mg/L for all regimens. All
infusion strategies showed higher than 85% PTA up to the MIC of 0.25 mg/L for bactericidal targets, with an increase
of nearly 3% by each hour added to the infusion time. Noteworthy, when the total daily dose of 1 g was divided into
equal 0.5 g doses and modeled at 12 h intervals over 0.5 h, greatly improved (14% or higher) PTAs were showed over
the range of MICs for the bactericidal target when compared to the standard 1 g dose infused over 0.5 h.
Conclusions
We conclude that prolonging the infusion time of ERT would have minimal effects on the PTA. Instead, more frequent
administration or giving the total daily dose in divided doses at more frequent intervals should be considered to
optimize the pharmacodynamics of this highly protein bound compound.
Quality Symposium 2012
Page 131
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Pharmacodynamic Profiling of Ertapenem in Critically Ill Patients with Early Onset Ventilator
Associated Pneumonia with Normal Renal Function to Moderate Renal Impairment
Andras Farkas, PharmD
Nyack Hospital
Introduction
Ertapenem (ERT) is a renally eliminated broad spectrum carbapenem antibiotic. We aimed to describe the effects of
renal function on the Probability of Target Attainment (PTA) of ERT at doubling MIC dilutions in critically ill patients
with early onset VAP.
Problem
N/A
Goals
N/A
Methods
Published population pharmacokinetic data for ERT in critically ill patients with early onset VAP was used in this
analysis. Free ERT concentrations were calculated with a validated two class binding site model. ERT 1g daily was
evaluated for PTA with Monte Carlo simulation (MCS, n=5,000) at normal, mild and moderate renal function
categories for MICs up to 4 mg/L for bacteriostatic (20%) and bactericidal (40%) ƒT>MIC targets. Additionally, 0.5g
at 24 h interval was modeled to assess for the impact of current renal dose adjustment recommendations on attaining
the desired targets in this patient population.
Results
ERT given at the 1g dose is expected to achieve optimal PTAs for bacteriostatic effect up to an MIC of 0.5 mg/L at all
renal function categories. At the bactericidal target, 1g ERT daily is expected to achieve 90% PTAs in simulated
patients with mild to moderate renal impairment up to an MIC of 0.25 mg/L, while patients in the normal renal
function category are expected to achieve suboptimal PTAs at this MIC. ERT 0.5g daily is expected to achieve optimal
target attainment up to a creatinine clearance of 40 ml/min over the ranges of MICs from 0.0625 through 0.25 mg/L for
the target of 40% ƒT>MIC.
Conclusions
Current dosing recommendations of ERT provide optimal PTAs for this population of patients with mild to moderate
renal function categories up to an MIC of 0.25 mg/L, while patients with normal renal function are likely to benefit to a
lesser extent using the 1 g daily dosing strategy. The 0.5 g dose daily at the current creatinine clearance breakpoint
recommended by the manufacturer for renal dose adjustment also achieves optimal PTA at this MIC.
Quality Symposium 2012
Page 132
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Dosing of Telavancin in the Obese: Is It the Ideal, Lean, Fat Free or Adjusted Body Weight?
Andras Farkas, PharmD
Nyack Hospital
Introduction
Dosing Telavancin (TLV) based on total body weight is expected to result in up to 35% higher drug exposure in the
obese patient compared to the patients with normal body weight. The objective of our study was to assess for the bases
of using alternative body weight estimations for dosing of TLV in the obese.
Problem
N/A
Goals
N/A
Methods
Published TLV population pharmacokinetic data of obese and normal body weight patients was used in this analysis.
Dosing of TLV based on total (TBW), ideal (IBW), adjusted (ABW), lean (LBW), and fat free (FFW) weights were
evaluated with Monte Carlo simulation MCS (n=5,000) to assess for the magnitude of drug exposure. The dosing
method that resulted in the magnitude and dispersion of AUC0-24 most similar to that of the normal body weight
patients was then selected as the most likely candidate for the dosing of TLV using an alternative body weight in the
population of the obese.
Results
Dosing based on ABW with a correction factor of 0.4 best approximates the exposure with simulated mean + SD
AUC0-24 of 701.9 + 202 mg.h/L in the population of the obese when compared to the normal body weight subjects.
Simulated median AUC0-24 values of dosing TLV based on IBW, LBW, and FFW were 23.2%, 23.7%, and 17%
smaller, respectively, in the obese compared to the patients with normal body weight
Conclusions
We conclude that dosing of TLV based on IBW, LBW, and FFW would result in sub-optimal exposure based on the
simulated AUC0-24 values in the obese. Since the pharmacodynamic index most likely predictive of outcomes is the
ratio of AUC/MIC, dosing of TLV based on IBW, LBW or FFW should be avoided in this population. Instead, dosing
based on ABW with correction factor of 0.4 can be considered in the population of the obese.
Quality Symposium 2012
Page 133
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Evaluation of Pharmacist Managed Vancomycin Therapy Compared to Physician Managed Dosing in
Establishing Timely and Therapeutic Vancomycin Serum Concentrations at a Community Hospital
Rachel Sussman, PharmD; Andras Farkas, PharmD
Nyack Hospital
Introduction
Vancomycin (VAN) remains a mainstay for the treatment of serious infections caused by gram-positive organisms. The
purpose of this study was to assess if pharmacist managed therapy can at least as effectively produce timely therapeutic
levels compared to physician managed dosing of VAN.
Problem
N/A
Goals
N/A
Methods
A total of 100 patients were evaluated for baseline characteristics. Demographic, laboratory and VAN monitoring data
were collected. Percentage of patients with initial, second, and third levels within subtherapeutic (<10 mg/l),
therapeutic (10 to 20 mg/l) and supratherapeutic (>20 mg/l) ranges were compared. Secondary end points included,
comparing initial mean ± SD VAN concentrations, levels between 8 and 22 mg/l, percentage of patients never reaching
concentrations of ≥ 10 mg/l, and time to reach the therapeutic range.
Results
There were no statistically significant differences in baseline characteristics between the two groups evaluated. VAN
levels within the therapeutic range for initial, second and third measurements were 77%, 71%, 74% for pharmacist
managed therapy and 37%, 58%, 55% for the comparator. Initial mean ± SD VAN levels were 13.4 ± 3.6 mg/l and 8.8
± 3.9 mg/l (p <0.05), while levels between 8 and 22 mg/l were 88% and 63%, for the intervention and comparator
groups, respectively. An additional 40% of patients never reached 10 mg/l in the physician group compared to the
intervention group. Median ± SD number of days to reach therapeutic range was 1.9 ± 0.9 days for the intervention
group versus 2.5 ± 2.7 days for the comparator group (p<0.5).
Conclusions
In conclusion, the pharmacist managed VAN therapy is at least as or more effective in achieving pre-specified
laboratory endpoints when compared to physician dosing of VAN at our institution. Pharmacist managed VAN therapy
resulted in both a greater percentage of therapeutic levels and a shorter time to reach therapeutic range.
Quality Symposium 2012
Page 134
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Door to Floor in 4 Hours
Christine Genovesi, RN; Dawn Sugrue, RN; Sachin J Shah, MD MBA; Eric Bachenheimer, MHSA MBA
Nyack Hospital
Introduction
In preparation for CMS OP-1, median time from arrival to departure for admitted patients, our hospital set out to
improve our arrival to admission times. We examined processes within the emergency department as well as within the
hospital to find areas with opportunities for improvement.
Problem
Nationwide, one of the major problems faced in emergency departments daily is patient boarding. With ever increasing
emergency department volumes, an aging population, and consolidation of acute care facilities, this problem will
continue to become worse. Boarding has been shown to increase morbidity and mortality for patients as well as
decrease patient satisfaction. Boarding also increases overall length of stay in the hospital.
Goals
Our goals were to first, measure our median times from arrival to departure for admissions. Second, we sought to bring
the median time down to under 4 hours.
Methods
Using our ED information system and business intelligence software systems (Emergisoft and EMars) we measured the
median admission times on a monthly basis both before and after the interventions took place.
Results
We achieved a nearly 40% decrease in disposition to departure time (median 1.9 hours in September 2011 to 1.2 hours
in August 2012). We also achieved a 20% decrease in median overall turnaround time for admitted patients from 5
hours in September 2011 to 4 hours in August 2012.
Achieving a goal of 4 hour turnaround time for admitted patients from the ED represents one of the highest
benchmarks for emergency department performance nationally.
Conclusions
Improving throughput for emergency department patients who are admitted to the hospital requires careful planning
and collaboration. Due to the complexity of the processes combined with the fact that the optimization of the process
requires collaboration of multiple departments (emergency department, medical staff, hospital administration, case
management, hospitalist group, inpatient services) a solid plan must be developed with the support and buy in of all
vested departments. The end result is a rapid ED admission process that can result in improved patients experience,
reduced inpatients length of stay, greater quality of care and patient safety.
Quality Symposium 2012
Page 135
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Using Near Miss Analysis to Prevent Wrong-Site Surgery
Joseph Bosco, MD; Lorraine Hutzler, BA; Richard Yoon, MD; Michael Alaia, MD
NYU Hospital for Joint Diseases
Introduction
The purpose of our study was to reduce the number of near miss events pertaining to wrong-site surgery, including
incorrectly sided surgical bookings and incorrectly performed pre-operative time-out procedures. Incorrectly booked
cases and improperly performed pre-surgical time-out procedures were recorded. We then educated each surgeon and
their staff regarding the importance of and proper way to perform these tasks. Subsequently, the monthly percentage of
incorrectly booked surgical procedures and improperly performed time-outs were significantly decreased.
Problem
In 2004, the Joint Commission published comprehensive guidelines to prevent wrong-site surgery. Seven years have
passed, and the incidence has not declined. The Joint Commission estimates that wrong-site surgeries occur at least 40
times a week in the United States. "Near misses" are events that could have harmed a patient, but did not due to chance
or mitigation. Improperly performed time-out procedures and inaccurate surgical bookings are considered near misses
and could ultimately lead to "never events", such as wrong-site surgery. Near-miss analysis is a highly effective
method of preventing rare, "never events". We hypothesize that proper education of surgeons and staff will be effective
in reducing the number of near misses.
Goals
1. Reduce Near Miss events.
2. Educate physicians and staff on importance of appropriate time-out procedures.
Methods
Beginning in August 2010, inaccurately booked procedures were entered into a database. We tracked these cases and
educated each attending physician and his/her staff about the importance of accurate surgical bookings. Additionally,
we began an observational program to carefully review pre-surgical time-out procedures as they occurred. We tracked
the percentage of these improperly performed time-outs and counseled members of the operating room team regarding
the deficiencies that caused the time-out to be ineffective. The number of near misses that occurred before and after the
interventions were recorded and analyzed.
Results
In the first four months of the study, the monthly percentage of incorrectly booked cases was 0.75%. Since the
intervention, the rate decreased to 0.41% (p=0.0139). The percentage of improperly performed time-out procedures
decreased from 18.7% to 5.9% after the educational interventions were performed (p<0.0001).
Conclusions
A program designed to educate physicians to the importance of decreasing near misses for wrong site surgery is
effective. When analyzing the literature, it is clear that the reduction in near misses observed in this study decreases the
likelihood of a wrong-site surgery.
Quality Symposium 2012
Page 136
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Hospital Acquired Conditions After Orthopedic Surgery Do Not Affect Patient Satisfaction Scores
Michael S Day, MD MPhil; Lorraine H Hutzler, BA; Raj Karia, MPH; Kella Vangsness, BS; Nina Setia, MS;
Marta Cieslak, MPH; Ellen Brophy, BA; Joseph A Bosco, MD
NYU Hospital for Joint Diseases
Introduction
The purpose of this study was to determine whether development of a Hospital Acquired Condition (HAC) affected
responses to Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions. We
hypothesized that patients who developed an HAC would be less satisfied with their care.
Problem
We hypothesize patients who develop a HAC during their hospitalization would be less satisfied with their care.
Goals
To determine whether HAC affect patient satisfaction scores.
Methods
Approval to carry out this study was obtained from our institution’s Institutional Review Board. We randomly
distributed the HCAHPS survey, a validated, standardized measure of patient satisfaction, to 6,056 patients discharged
from our institution for any orthopaedic admission over a two-year period. All patients who develop HACs are logged
by our hospital quality assurance monitoring system. We reviewed the HCAHPS database, identified completed
surveys associated with patients who had developed an HAC, and compared satisfaction scores between patients with
HACs and patients without HACs. Survey scores were normalized to a 100-point scale. Parametric and non-parametric
analyses were performed for two global ratings, and six specific satisfaction categories. Sub-group analysis was
performed for surgical site infections (SSI) and venous thromboembolic disease (VTE).
Results
2,876 controls and 159 HAC cases were identified from completed surveys. The cases and controls were similar terms
of race; however the HAC group contained significantly more women (p<0.001). Patients in the HAC group also were,
on average, significantly older with a mean age of 66.84 versus 58.65 (p<0.001). There was no difference in
satisfaction scores in patients' mean rating of communication by nurses (p=0.811), communication by doctors
(p=0.313), communication about medications (p=0.694), pain control (p=0.662), the cleanliness of the hospital
environment (p=0.542), and the quietness of the hospital (0.589). The mean normalized score for overall satisfaction
was 93.99 (out of 100) for controls and 94.84 for HAC cases (p=0.612). The mean normalized score for overall
willingness to recommend the hospital to others was 90.22 for controls and 90.65 for HAC cases (p=0.774). There was
no statistically significant difference in satisfaction for patients with SSI versus VTE versus all other HACs (p>0.05 for
each satisfaction category by analysis of variance [ANOVA]).
Conclusions
Women and older patients are more likely to both develop an HAC and return a satisfaction survey. Development of a
HAC did not affect satisfaction scores in a population of orthopaedic surgery patients at a private, university-affiliated
specialty center. This could be due to the orchestrated efforts of the caregivers in response to the HAC and the patient
satisfaction with after-care in the recovery period after development of an HAC, the sensitivity of the survey
Quality Symposium 2012
Page 137
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
instrument, or possibly patient expectations of surgery, with SSI and VTE as known potential complications of
orthopaedic surgery.
Quality Symposium 2012
Page 138
HAC
No HAC
p value
Communication
with Doctors
Score (n)
91.1 (157)
92.2 (2834)
0.313
Communication
with Nurses
Score (n)
89.3 (156)
89.0 (2843)
0.811
SSI
VTE
Other*
p value
88.8 (118)
90.5 (32)
92.2 (7)
0.504
88.9 (116)
91.7 (33)
89.5 (7)
0.969
Characteristic
Communication
Pain Control
About Medications
Score (n)
Score (n)
78.0 (117)
88.3 (147)
78.8 (2149)
88.9 (2727)
0.694
0.662
75 (87)
58.3 (27)
79.6 (3)
0.236
89.6 (111)
93.8 (30)
89.1 (6)
0.663
Clean
Environment
Score (n)
87.3 (159)
88.1 (2872)
0.542
84.1 (119)
85.7 (33)
88.1 (7)
0.595
Quiet
Willingness to
Overall Rating
Environment
Recommend
Score (n)
Score (n)
Score (n)
83.5 (158)
94.8 (155)
90.6 (155)
82.6 (2876)
94.0 (2853)
90.2 (2863)
0.589
0.612
0.774
79.5 (118)
89.3 (33)
83.3 (7)
0.575
94.2 (115)
95.7 (33)
94.5 (7)
0.993
89.4 (115)
89.3 (33)
90.7 (7)
0.963
Satisfaction scores (out of 100) for each domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. Variable n across
domains reflects surveys incompletely filled out. HAC: hospital acquired condition; SSI: surgical site infection; VTE: venous thromboembolism.
*Foreign object retained after surgery (n=0), air embolism (n=0), blood incompatibility (n=0), stage III and IV pressure ulcers (n=1), falls and trauma (n=1),
manifestations of poor glycemic control (n=0), catheter associated urinary tract infection (n=7), vascular catheter-associated infection (n=0)
Quality Symposium 2012
Page 139
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Risk Factors for Readmission Following Inpatient Orthopedic Surgery: A Review of 13,663 Cases
Tracey Hunter, BA*; Philip Band, PhD*; Victoria Liublinska, PhD**; Raj Karia, MPH*; Lorraine Hutzler,
BA*; James Slover, MD*; Joseph Bosco, MD* (* NYU Hospital for Joint Diseases; ** Harvard University)
NYU Hospital for Joint Diseases
Introduction
Previous studies have reported that co-morbidities and socioeconomic status are risk factors for orthopaedic
readmission, the latter evaluated using Medicare and Medicaid status as a surrogate for income. Because individuals
with relatively high incomes may be receiving Medicare coverage, Medicare status may not be an appropriate
surrogate for socioeconomic status. We therefore used an alternative method to evaluate socioeconomic status as a risk
factor for readmission, and evaluated other risk factors to put socioeconomic status into perspective.
Problem
We hypothesize that a patient’s socioeconomic status is correlated with a hospital readmission post-operatively.
Goals
To determine if socioeconomic status is a risk factor for orthopaedic readmission.
Methods
The socioeconomic status, co-morbidity status, and length of stay (LOS) for the index admission were analyzed using
an administrative database that included 325 30-day readmission cases and 13,338 non-readmission cases, for
orthopaedic patients admitted during the September 2008 to April 2011 time period. Each patient’s zip code provided a
surrogate for income, using median household income values for each zip code from 1999 US Census data. The
patients were divided into quintiles based on income. Co-morbidity was categorized by combining groups of DRGbased classifications into 3 classifications: no co-morbidities, minor co-morbidities, or major co-morbidities. Risk
factors were analyzed for readmission using a Bayesian logistic regression model. Differences in readmission rate for
co-morbidity categories were analyzed using the chi-square test.
Results
There were 1272 unique zip codes in the analyzed patient population, with median incomes ranging from $6,450 to
$189,763. The regression model found a significantly increased risk of readmission for LOS (OR = 1.45, p < 0.0001),
minor co-morbidities (OR = 1.74, p < 0.0001) and income quintile 4 ($32,303- $42,374, OR = 1.46, p=0.04). The
reference income range was $70,101-$189,763 (quintile 1). The proportion of patients readmitted was significantly
different across co-morbidity categories (p < 0.0001). There was a 126% increase in the readmission rate when
comparing patients with no co-morbidities to those with major co-morbidities (p < 0.0001).
Conclusions
These data suggest that LOS and co-morbidity status are primary risk factors for orthopaedic readmission.
Socioeconomic status had a moderate impact on risk, with patients of low-mid income having a significantly higher
risk of readmission. A limitation of our analysis is that zip code-level income may measure area-level effects (e.g.
neighborhood resources) more so than individual socioeconomic status.
Quality Symposium 2012
Page 140
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Physician-Specific Correlation Between Discharge Disposition Cost, Readmission and Length of Stay
(LOS) Following Total Hip and Knee Replacement: An Analysis of 1,777 Cases
Lorraine Hutzler, BA; Joseph Bosco, MD; James Slover, MD MS; Carlos Alvarado, MD
NYU Hospital for Joint Diseases
Introduction
In an effort to reduce costs healthcare payers, led by the Federal government, are requiring patients to be discharged
home rather than to an acute care rehabilitation facility, following uncomplicated lower extremity joint replacements.
Problem
Discharge to an acute rehab facility is significantly more costly than discharge home with outpatient physical therapy.
However there is concern that discharge to home will result in an increased LOS and readmission rate compared to
discharge to an inpatient rehabilitation facility. We analyzed all 1,777 discharges following total hip replacement
(THR) and total knee replacement (TKR) at our institution in fiscal year 2010 to determine their physician specific
discharge disposition. We then analyzed the effect of discharge disposition on physician specific LOS and readmission
rate.
Goals
To determine the effect of discharge disposition on physician-specific LOS and readmission rate.
Methods
We reviewed the medical records of each of the 1,777 patients discharged from our institution following a hip or knee
replacement over a one-year period (September 2009 - August 2010) to determine length of stay, 30-day readmission
rate and discharge arrangement. Each patient was discharged to one of 4 scenarios: 1) Acute Inpatient Rehabilitation 2)
Skilled Nursing Facility 3) Home Health with Home Therapy and 4) Routine Discharge with Outpatient Therapy.
Using Medicare claims data, we determined the cost of each discharge scenario. We included all 20 surgeons who
performed joint replacements in our analysis. The discharge scenarios for each surgeon were determined. We then
calculated the entire cost of all the discharge scenarios for each individual physician and divided this number by the
number of discharges for each physician. We then determined the average cost per discharge for each physician. We
compared the average cost per discharge for each physician to each physician’s LOS and readmission rate to determine
if there was a correlation between these variables.
Results
The average discharge costs between physicians varied from $16,464.00 to $3,642.98 (± $9,044.62) for TKRs and
$16,464.00 to $733.00 (± $11,102.28) for THRs. The correlation coefficient for LOS and discharge costs following
TKRs was r=0.10 (weakly positive) and for THRs was r=0.12 (weakly positive). The correlation coefficient for
readmissions and discharge costs for TKRs was r=-0.27 (weakly negative) and for THRs was r=0.19 (weakly positive).
For all joint replacements (THR and TKR combined) the correlation coefficients were r=0.11 (weakly positive) and r=0.09 (weakly negative) for LOS and readmissions respectively vs. cost of discharge.
Conclusions
Discharge patterns following joint replacement varied widely between physicians at our institution. However we could
find only weak correlations between the cost of discharge and LOS or readmission rates. Patients discharged home did
Quality Symposium 2012
Page 141
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
not have a greater LOS or readmission rate than those discharged to a rehab center or skilled nursing facility. The large
inter-physician variance in discharge cost did not correlate to a difference in quality, as measured by the LOS and
readmission rates.
Quality Symposium 2012
Page 142
Table 1: Highest Lowest Total Knee Replacement Average Cost of Discharge Disposition $16,464.00 Average Cost of Discharge Disposition $3,642.98 Total Hip Replacement $16,464.00 $733.00 Table 2: The correlation coefficient (r) for LOS and discharge disposition costs were weakly positive. TKR r= 0.10 THR r= 0.12 The correlation coefficient (r) for readmissions and discharge disposition costs for: TKR (weakly negative) r= ‐0.27 THR (weakly positive) r= 0.19 Quality Symposium 2012
Page 143
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Variance in Discharge Disposition and Cost between Patients with Medicare and Commercial
Insurance following Total Hip and Total Knee Replacements
Lorraine Hutzler, BA; Joseph Bosco, MD; James Slover, MD MS; Carlos Alvarado, MD
NYU Hospital for Joint Diseases
Introduction
An episode of care is defined as all care rendered 72 hours prior to admission, the care during admission and all care
provided within 30 days of discharge. A significant portion of the cost involved in an episode of care for a total joint
replacement occurs during the 30 days after discharge and is highly dependent on where the patient is discharged to.
Problem
Discharge to an acute rehab facility is significantly more costly than discharge home with outpatient physical therapy.
Goals
To determine if discharge disposition costs varied by insurance type.
Methods
We reviewed the medical records of each of the 1,777 patients discharged from our institution following a Total Hip or
Total Knee Replacement over a one-year period (September 2009 - August 2010) to determine costs of discharge by
procedure, disposition location, and insurance type. Each patient was discharged to 1 of 4 scenarios: 1) Acute Inpatient
Rehabilitation 2) Skilled Nursing Facility 3) Home Health with Home Therapy and 4) Routine Discharge with
Outpatient Therapy. Using Medicare claims data, we estimated the total cost of each discharge scenario to be $16,464
Acute Inpatient Rehabilitation, $6,768 Skilled Nursing Facility, $4,239 Home Health with Home Therapy, and $733
Routine Discharge with Outpatient Therapy. We then calculated the average cost per discharge for Medicare and NonMedicare hip and knee replacement patients by summing the average cost of each patient’s discharge disposition for
these groups, and dividing that sum by the total number of cases performed.
Results
68.73% of Medicare patients were discharged to Acute Inpatient Rehabilitation or a Skilled Nursing Facility compared
to 30.72% of the non-Medicare patients. Thus non-Medicare patients were 2.2 times more likely to be discharged home
following joint replacements than Medicare patients. This resulted in Medicare patients discharge costs being
significantly greater than non-Medicare patients for both hip and knee replacements. The costs were ($16,464 to
$2,485) vs. ($8,762.61 to $733) (p<0.0001) and ($16,464 to $3,642.98) vs. ($9,475 to $4,021.41) (p<0.0001) for hip
and knee replacements respectively.
Conclusions
Discharge disposition following joint replacement surgery accounted for a significant variation in costs. Medicare
discharge disposition costs were significantly greater than non-Medicare discharge disposition costs because Medicare
patients are less likely to be discharged home.
Quality Symposium 2012
Page 144
Table 1: Average Cost/Discharge Standard Deviation TKR All Other Medicare Payments THR Medicare All Other Payments $9,699.62 $6,184.80 $9,883.82 $5,203.71 $3,211.45 $1,531.90 $3,467.08 $1,660.62 Table 2: Number of Patients by Discharge Disposition and Insurance Type Discharge Disposition Acute Inpatient Rehabilitation Skilled Nursing Facility Home Health with Home Therapy Routine Discharge with Outpatient Therapy TOTAL Non‐
Medicare Medicare
47.17% 9.99%
21.55%
20.73%
28.45%
56.48%
2.83%
12.80%
100.00% 100.00% Quality Symposium 2012
Page 145
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Obesity Prevention Initiative
Diane Curley, MSN RN CNOR CBN
St. Catherine of Siena Medical Center
Introduction
A disparity exists in the care provided to patients for the assessment, prevention and treatment of obesity. As a result,
the health of the population has declined due to the rising prevalence of obesity and obesity-related comorbidities.
Costs of care have increased as a result of the decline in the health of the population. This initiative seeks to elevate the
level of care provided to patients to include the assessment, prevention and treatment of obesity, equal to the level and
standard of care provided to patients to assess, prevent and treat other at-risk behaviors that diminish health such as
domestic violence and tobacco use. The result: better care, better health, reduced cost.
Problem
About one-third of US adults (35.7%) are obese (Body Mass Index (BMI) >30). Obesity-related comorbidities include
heart disease, stroke, type 2 diabetes and certain types of cancer, some of the leading causes of death (Centers for
Disease Control (CDC) www.cdc.gov). Consequently, medical costs associated with obesity increased 42% ($1,429
per capita) since 1998 (Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual Medical Spending Attributable To
Obesity: Payer- And Service-Specific Estimates. Health Affairs, 2009; 28(5):w822-w831.)
Goals
St. Catherine of Siena Medical Center (SCS) recognized these concerns represented an area for improvement. In 2012,
as part of the Affordable Care Act, Centers for Medicare and Medicaid Services (CMS), Center for Medicare and
Medicaid Innovation (CMMI) Innovation Advisors Program, SCS endeavors to achieve the goals of the 3-part aim:
better care, better health, reduce costs.
AIM Statement:
Prevent obesity and reduce the prevalence and cost of obesity and obesity-related comorbidities by screening 100% of
patients accessing care at SCS to assess for obesity/ risk for obesity, provide brief intervention and referral to treatment
for 100% of patients assessed as obese/ at risk, enrollment and participation in treatment of 50% of referred patients
with subsequent weight loss of 50% of enrolled patients and BMI below 25 (healthy weight) in 10% of enrolled
patients by December 31, 2012 (see Initiative and Driver diagrams).
Methods
The Obesity Prevention Initiative at SCS establishes a model of care where every patient is assessed for obesity (BMI
>30) /risk of obesity (BMI 25-29), provided with targeted education, resources, support and referral to treatment based
on the results of the assessment and shared decision making.
SCS has partnered with community providers and physician providers as resources for referral to treatment and data
collection. Process and outcome measures/data is collected daily and analyzed monthly to determine progress towards
attainment of goals: better care, better health, reduce costs. (See "Shared Decision-making Continuum Diagram"
(adapted from Dartmouth) and "Treatment Options Diagram" (adapted from NIH (National Institute for Health).)
Quality Symposium 2012
Page 146
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Results
To date the project has resulted in demonstrated improvement of process measures related to the first dimension of the
3 part aim, better care:
• An increase from 0% to 100% of patients accessing care at SCS are assessed to determine obesity/risk for obesity.
• An increase from 0% to 20% of brief interventions (education, resources, support) provided to patients assessed as
obese.
• An increase from 0% to 20% of patients assessed as obese referred to treatment.
• Patients are beginning to enroll and participate in treatment programs (MD, YMCA Weight Watcher's)
Outcome measures:
• As of 3rd quarter 2012 patients have demonstrated weight loss (see "Process and Outcomes Measures" diagram and
run charts).
Conclusions
To date the project has resulted in demonstrated improvement of process measures related to the first dimension of the
3 part aim, better care. Results of outcome measures related to the second dimension of the 3 part aim, better health
(improved health of the population), are expected to begin 4th quarter 2012 and continue. Results of outcome measures
related to 3rd dimension of the 3 part aim, reduce costs (reduced per capita cost attributed to obesity and obesity related
comorbidity), are expected to be realized during 2013 and continue.
Discussion:
As data is analyzed over time, continued improvements in process measures drive improvement in outcome measures.
An increase in the # of patients assessed generates identification of at-risk patients provided with brief intervention and
referred to treatment. Weight loss and/or weight maintenance is achieved as patients continue to enroll in and
participate in treatment, thereby improving the health of the population, reversing the trend of 42% ($1,429 per capita)
cost increase since 1998 associated with obesity.
Recommendations-Next Steps:
Implement the program to advance the process and outcome measures for the at-risk population (BMI 25-29),
essentially preventing obesity. Currently we are exploring funding options and working with area food banks to
provide an on-site healthy food pantry to meet the needs of the financially insecure. As the initiative continues to meet
program goals, the initiative is to be considered for scale-up.
Quality Symposium 2012
Page 147
Quality Symposium 2012
Page 148
Quality Symposium 2012
Page 149
Quality Symposium 2012
Page 150
Project:
Person:
Date:
Obesity Prevention
Diane Curley
1‐Jun‐12
Notes:
In June we focused on two primary activities: (1) Testing the process of EMR prompts (system go-live was 6.23.12) to RN's to provide
education, resources, support and referral to treatment to patients with BMI 25-29. (2) Testing the same process with EMR prompts to
Dieticians for patients with BMI 30 and above. Two barriers we are struggling with are (1) report from EMR not yet available and (2) RN's
transitioning to EMR feeling overwhelmed, which we hope to resolve by end of July by providing additional super user support to RN's and
optimizing reports.
Obesity Prevention‐Assessment
Obesity Prevention‐Identified as at‐risk 45
14
40
12
35
10
25
Value
Value
30
20
15
8
6
4
10
2
5
0
0
Jan‐12
Apr‐12
Jul‐12
Oct‐12
Jan‐13
Apr‐13
Jul‐13
Oct‐13
Jan‐12
Apr‐12
Jul‐12
Month
Apr‐13
Jul‐13
Oct‐13
Obesity Prevention‐Education, Resources, Support
16
20
14
18
12
16
14
10
12
Value
Value
Jan‐13
Month
Obesity Prevention‐Identified with Obesity
8
6
10
8
6
4
4
2
2
0
0
Jan‐12
Apr‐12
Jul‐12
Oct‐12
Jan‐13
Apr‐13
Jul‐13
Jan‐12
Oct‐13
Month
Apr‐12
Jul‐12
Oct‐12
Jan‐13
Apr‐13
Jul‐13
Oct‐13
Month
Obesity Prevention‐Referred to Treatment
Obesity Prevention‐Enrolled in Treatment
20
18
4.5
16
3.5
4
14
3
12
Value
Value
Oct‐12
10
8
6
2.5
2
1.5
4
1
2
0.5
0
0
Month
Month
Quality Symposium 2012
Page 151
Obesity Prevention‐Losing Weight
Obesity Prevention‐Healthy Weight
1
0.9
0.8
0.8
0.7
0.7
0.6
0.6
Value
Value
1
0.9
0.5
0.5
0.4
0.4
0.3
0.3
0.2
0.2
0.1
0.1
0
0
Month
Month
Quality Symposium 2012
Page 152
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Bedside Report
Co-Principal Investigators: Miranda Corcoran, RN MA NE-BC; Bennarda Daly, RN; Catherine O'Brien, RN
BSN; Eileen Piekarski, RN MS OCN; Keri Wilson, RN BSN
St. Catherine of Siena Medical Center
Introduction
St. Catherine of Siena Medical Center is a community hospital located in Smithtown, New York. A new staff member
expressed dissatisfaction with the quality of report given at change of shift. At that time, report was given outside the
room and did not include the patient. This nurse stated that she routinely had to spend up to an hour and a half
reviewing medical records to have a clear picture of the status and needs of each of her patients.
The South Tower leadership team recognized this as an opportunity for process improvement as well as improvement
in patient satisfaction scores. The Hospital Consumer Assessment of Health Care Providers and Systems survey
(HCAHPS) scores for the involved units were less than desirable so we established a committee made up of both nurse
leaders and RN representatives from each unit.
Problem
The Joint Commission has determined that lapses in communication are the root cause of up to 70% of all sentinel
events. Change-of-shift report has been determined to be a dangerous time for hospital in-patients. The Joint
Commission standard for hand-off communication requires face-to-face report and the opportunity to ask questions.
We wanted to improve the process of how report was given. The literature search demonstrated that patients who
experience quality communication with the staff rated their hospital stay as more satisfying than those who perceived a
lack of communication.
Goals
Our goal was to improve patient satisfaction, patient safety, and over-all quality of care. Patient satisfaction is fiscally
significant due to HCAHPS scores directly impacting reimbursement.
Methods
The subjects (nurses) received a half hour educational training from their managers during regularly scheduled council
meetings and additional half hour demonstrations at the bedside. This training lasted for a period of six months. The
study took place within the normal work environment, at staff council meetings, and within the units where patient care
was delivered.
The success of the project was measured by a significant increase in our HCAHPS scores for nursing sensitive
indicators. The data metrics used to measure the efficacy of the education was the HCAHPS reports, which are
published quarterly and are publicly available records. HCAHPS are existing data that is recorded in such a manner
that the subjects cannot be identified directly or through identifiers linked to subjects. The equipment used were
computers, to access the data and the instrument used was a checklist recording the education of each nurse.
Results
Comparison of the third quarters of 2010 and 2011 demonstrated significant improvement in several nurse sensitive
Quality Symposium 2012
Page 153
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
indicators. Nurse communication was rated five times higher, and communication about medications was four times
higher. The likelihood to recommend the hospital increased threefold. These results validated our hypothesis that
Bedside Report improves communication and patient satisfaction.
Chi-square tests of independence were performed to examine the relationships between HCAHPS results on Nurse
Communication, Responsiveness of Staff, Pain Management, Communication about Medicines, Overall Rating of
Hospital, and Likelihood to Recommend Hospital and bedside report. All of the relationships between the HCAHPS
measures and Bedside Report were significant with associated p values < 0.01 respectively.
Conclusions
Bedside Report was an effective strategy in improving communication and patient satisfaction. We continue to monitor
HCAHPS results quarterly, as well as staff compliance with Bedside Report. With the introduction of the Electronic
Medical Record in June 2012, we recognize that other variables will continue to affect HCAHPS scores.
Quality Symposium 2012
Page 154
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Maintaining a Safe Patient Environment Without the Use of Restraints
Laurie Yuditsky, RN MBA BSN (Nursing PI Coordinator)
St. Catherine of Siena Medical Center
Introduction
Restraints are supposed to be used only when other non-restrictive methods have been deemed unsuccessful, but often
patients are placed in restraints for other reasons, such as staff convenience. Healthcare professionals have a
responsibility to maintain patient safety and uphold the patient's dignity while under our care. Restraints can result in
negative outcomes, some mild and temporary while others can be serious and irreversible; these can include agitation,
confusion, repeated falls that can have more serious injuries, muscle atrophy leading to functional decline,
incontinence, pressure ulcers, social isolation, and even death. Financial penalties associated with hospital acquired
conditions (HACs) can be a significant burden on a hospital’s bottom line. CMS has deemed many HACs preventable,
and increased hospital length of stays due to the HAC will not be reimbursable. More than just financial
considerations, it is our moral duty to protect and advocate for the patient. As stated in the VA National Center for
Patient Safety Falls Toolkit, "restraints do not reduce the rate of serious falls."
Problem
From 2007 to 2009, our restraint usage increased by 21%, at this same point in time our fall rate increased by 20%. Our
fall and restraint rates were both above our benchmark as well as system wide benchmarks. Initial efforts included unit
based discussions, but due to staff resistance and fear for the wellbeing of their patients, no reductions were seen. There
was a significant amount of staff concern that without restraints the patients would either fall or would dislodge
medical equipment causing self inflicted harm. We identified that staff were very quick to determine that restraints
were necessary for situations including confusion and/or impulsive behaviors; without first considering and trialing
other non-restrictive options. In 2009 our restraint rates for Med/Surg was 13.9, Critical Care was 58.1, and an Acute
Care Rate of 18.8. (The restraint rate is defined as the number of restraint episodes per number of patients in a defined
area x 1,000.)
Goals
The initial goal of St. Catherine of Siena Medical Center was to decrease the restraint usage by 5%, but in order to
meet system wide benchmarks M/S would have to decrease by 73%, Critical Care 39%, and Acute Care by 45%. The
restraint reduction goal also was to prevent an increase in patient falls and improve patient safety while maintaining
patient dignity.
Methods
The initial restraint reduction began with one M/S unit trialing an elimination of restraints in the Q1 of 2010. This unit
which is comprised primarily of elderly nursing home patients saw an 86% reduction over a three month timeframe. It
was decided at several Nursing driven committees that the elimination of restraints would be extended to a hospital
wide initiative. Extensive staff education regarding non-restrictive alternatives such as frequent patient visualizations,
non-secured hand mitts, distraction techniques, bringing patients to the nursing station (if medically appropriate), and
the use of bed alarms was conducted and also reinforced at unit based meetings. Additional bed alarms were purchased
as well as non-secured hand mitts. Non-secured hand mitts were identified as a new alternative to either replace or
decrease the use of wrist restraints. The standard 1:1 was changed with Physician approval to two separate patient
Quality Symposium 2012
Page 155
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
observation categories. Depending on the situation, the patient could be placed on either a CVO (constant visual
observation) in which the patient is always within the view of the staff member, or a FIM (frequent intermittent
monitoring) where the patient is visualized every 10-15 minutes, and commonly more often, by a staff member that
rounds on, up to 6 patients, and this is their only task. The admitting department was involved in this initiative by
participating with the proper bed placement of patient and assisting with room transfers when patients required a room
change to be closer to the nursing station. The restraint reduction initiative was discussed at many multidisciplinary
team meetings including Nursing Leadership, Departmental Leadership, Fall Prevention Committee, and Nursing
Performance Improvement and involved nursing, physical therapy, pharmacy, housekeeping, transport, and hospital
leadership. A restraint log was developed and kept in the nursing office; every shift any patient that was found to be in
restraints was evaluated by a Nurse Manager or Supervisor to determine if it could be discontinued. Patients that were
in restraints were discussed daily at unit based ICC (interdisciplinary care coordination) rounds to establish restraint
discontinuation goals to maintain patient safety. Towards the end of Q2 2010 we had a significant reduction in
restraints, but there were still episodes of restraints showing up without other non-restrictive options being utilized.
Starting on August 1, 2010 all vest and wrist restraints were removed from all hospital units, med/surg, critical care,
the emergency department and even central supply. If a nurse wanted to obtain a restraint, that nurse would have to
request it from either the Nurse Manager or Nursing Supervisor and provide evidence that other methods to keep the
patient safe have been used and deemed unsuccessful.
Results
The restraint reduction initiative project has resulted in a decrease in Acute Care restraints by 94%, Med/Surg restraints
by 98%, and Critical Care restraints by 87%, while seeing a 16% reduction in our Acute Care fall Rate. Not only did
we meet system wide benchmarks, we exceeded them and further lowered our benchmarks which we have consistently
stayed significant below since inception of this initiative. The percentage of Medical Surgical patients episodes of
restraints differed by year (2009, 2010, 2011), χ2(2, N=171,772) = 889, p=<.001. The percentage of Critical Care of
patients episodes of restraints differed by year (2009, 2010, 2011), χ2(2, N=21,452) = 3100, p=<.001. The percentage
of Acute Care of patients episodes of restraints differed by year (2009, 2010, 2011), χ2(2, N=192,938) = 11,780,
p=<.001. 2012 Q1 and Q2 data was not included in the statistical inferential analysis as we did not have a full year of
data.
Conclusions
The actual decrease in restraint use throughout the facility demonstrates that restraining patients does not keep them
safer than if less restrictive alternatives are utilized. The results confirmed that our decrease in use of restraints aligned
with a decrease in our fall rate. We do not have any evidence to indicate that the elimination of restraints increased the
removal of medical devices by patients. The cultural change among the staff regarding restraint usage has been
astounding, more than was even anticipated. All patient care providers have embraced this initiative and are very proud
of their accomplishments. "We can not stop using restraints, the patients will fall," was the commonly heard statement
in the early months of 2010, however, after 2 years, staff will appear insulted if asked, "do you have any patients in
restraints?" and will reply, "we do not use restraints here."
Quality Symposium 2012
Page 156
Critical Care Non-Violent Restraint Reduction Initiative
2011 Critical Care Benchmark<20
2011 Annual Rate=7.26, 2010=28.37, 2009=58.1
70
# of Restraint Episodes per CC Patient Days X 1000
64.1
63.9
60
2010 5% Reduction
Benchmark <41.1
53.8
53
50.3
50
45.3
40
30
2011 Revised
Benchmark
20
10.8
9.44
10
7.49
10.5
5.72
4.41
4.94
4.44
Q4
2012
Q1
0
2009
Q1
Q2
Q3
Q4
2010
Q1
Q2
Q3
Q4
2011
Q1
Q2
Q3
Q2
-10
Restraint Rate
Linear (Restraint Rate)
Med/Surg Non-Violent Restraint Reduction Initiative
2012 Med/Surg Benchmark <3
2011 Annual Rate=0.23, 2010=5.20, 2009=13.9
18
# of Restraint Episodes per Med/Surg Patient Days X 1000
17.8
16
15
14
13.5
14.9
13.6
12.6
12.5
12
12
10.5
10
8
7.3
Trendline
6
4
Benchmark<3
2
0.78
0.5
0.07
0.19
0.2
0
0.2
0
Q2
Q3
Q4
Q1
2012
Q2
0
2005
2006
2007
2008
Q1
2009
Q2
Q3
Q4
Q1
2010
Q2
Q3
Q4
Q1
2011
Quality Symposium 2012
Page 157
ST. CATHERINE OF SIENA MEDICAL CENTER
PATIENT FALLS AND RESTRAINT UTILIZATION
2003-2012
fall rate
restraint rate
Restraint Rate Trendline
Fall Rate Trendline
5
20
CHS Pt Fall Benchmark <3.5 to 4.5
18
# of Patient Falls per 1,000 Acute M/S Patient Days
17
4
16
3.9
15
3.5
3.5
13.5
3
3.7
3.68
3.11
3.2
12.5
14
3.28
13.6
12
3
2.5
10
7.88
2
8
1.5
6
1
4
0.5
# of Restraint Episodes per 1,000 Acute M/S Patient Days
4.5
2
0.98
0.77
0
0
2005
2006
2007
2008
2009
2010
2011
2012 to date
Quality Symposium 2012
Page 158
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Reducing Incident of Hospital Acquired Pneumonia After Acute Stroke Through Implementation of
Simple Bedside Dysphagia Screen
Catherine Videtto, RN MSN ANP CPHQ; Mary Jane Finnegan, RN MSN
St. Catherine of Siena Medical Center
Introduction
Hospital acquired Pneumonia is estimated to occur in approximately 6.7-22% of hospitalized acute stroke patients. A
three-fold increase in 30-day mortality is associated with pneumonia. Many pneumonia cases are preventable with
implementation of stroke protocols which include standardized bedside dysphagia screening.
Problem
Incidence of Hospital acquired Pneumonia (HAP) in Acute Stroke patients hospitalized at this non-academic
community hospital was reported as 3.5 per 173 stroke patients in 2009 and 4.2 per 191 stroke patients in 2010. It is
reported in the literature that adverse outcomes for stroke patients can be reduced with increased adherence to
standardized evidence based stroke management protocols. Aspiration pneumonia is the most important complication
of stroke related dysphagia. St. Catherine of Siena Medical Center's compliance with completion of the simple bedside
dysphagia screen in stroke patients prior to anything by mouth was reported as 83.6% in 2009 and 87.5% in 2010
showing performance was lower than desired. There was no standardized dysphagia screen in place prior to 2011,
resulting in inconsistent performance of assessment of patient's swallow integrity prior to oral intake. Individual
practitioners were not held accountable for completing and documenting the dysphagia screen.
Goals
St. Catherine of Siena Medical Center is committed to being on the leading edge of quality and safety innovation. The
project goal was to achieve 100% compliance with completion and documentation of dysphagia screening for all stroke
patients prior to the patient receiving anything by mouth. Improved adherence to completion of dysphagia screening
will yield a reduction in the incidence of hospital acquired pneumonia in the stroke population. Members of the stroke
performance improvement committee determined that a specific individual will be identified as the responsible person
who must document the outcome of the dysphagia screen, and a standardized method of completing this screen will be
adhered to by our health care professionals.
Methods
The performance improvement strategies that were identified and implemented:
• Review of current literature to identify a simple evidence based dysphagia screen with high sensitivity and
specificity that could be effectively and efficiently implemented by the nurse at the bedside.
• Develop a clear procedure which explains performance of the dysphagia screen to facilitate a standardized approach
to performing this screen.
• Provide competency training for all nursing staff to ensure that staff will be successful in performing the screen at the
bedside.
• Identify the specific individual responsible for the completion and documentation of the dysphagia screen and update
the Stroke Management policy to include the performance of the dysphagia screen by the ED RN on all patients
admitted with a Emergency Severity Index score of 1, 2 or 3 and identify that RN assigned to care for in-house patient
will complete and document this screen at any time a patient is identified at risk for aspiration.
Quality Symposium 2012
Page 159
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• Add the completion of the dysphagia screen as a core measure in the electronic medical record standardized stroke
order set, including that it be built into the RN worklist as a prompt to complete the screen in the flowsheet section of
the chart.
• Recognize individual practitioners for improved adherence to completion and documentation of the dysphagia screen
by implementing the Penumbra Recognition Award for providing excellence in stroke care.
• Enhance collaboration between Emergency Department and Stroke Unit nursing staff.
Results
• A standardized dysphagia screen was adopted and added to the stroke policy.
• Individual staff accountability yielded improved compliance with performance and documentation of the dysphagia
screen.
• A 41.3% reduction in Hospital Acquired Pneumonia in the Stroke patient population was achieved in the 2011-2012
monitoring period compared with the 2009-2010 baseline period (figure 1).
• Compliance with completion of documentation of the bedside dysphagia screen increased from 83.6% in 2009 to
94.4% in 2011 and 100% compliance January-July of 2012.
• Outcome of the bedside dysphagia screen is discussed during hand-off communication.
• If the patient does not initially pass the dysphagia screen but neurologic deficit rapidly improves as in a TIA, the RN
will repeat the screen if appropriate.
• If the patient shows continuing neurologic deficit and remains at risk for aspiration, the patient is maintained NPO
until a formal swallow evaluation is performed by the Speech and Language Pathologist.
• Consistent concurrent monitoring by the stroke coordinator allows timely follow-up with responsible staff to improve
overall compliance and as a result facilitate improved patient care.
• Dysphagia screen successfully built into the electronic medical record which prompts physician to order this screen
and triggers the RN caring for the patient to complete and document the screen.
Conclusions
Through increased adherence to completion of standardized dysphagia screening protocol a 41.3% reduction in
incidence of hospital-acquired pneumonia in our stroke population was achieved (figure 2). The implementation of an
evidence based screening protocol that has proven high sensitivity and specificity, will result in improved quality of
care for all of the patients that are identified at risk for aspiration. Sustaining this successful reduction in HAP through
2012 shows evidence of staff buy-in to practice changes when proven to benefit our patients and demonstrates that
individual accountability as well as appropriate recognition can effectively improve staff performance and commitment
to delivering quality care.
Quality Symposium 2012
Page 160
Percentage of Compliance with Completion of
Simple Bedside Dysphagia Screen in Stroke Patient
Prior to Anything By Mouth
105
100
% o f co m p lian ce
100
94.4
95
90
87.5
83.6
85
80
75
2009
2010
2011
2012 Jan-July
Figure 1 St. Catherine of Siena Medical Center “Reducing Incident of Hospital Acquired
Pneumonia After Acute Stroke Through Implementation of Simple Bedside Dysphagia Screen”
St. Catherine of Siena Medical Center
Incidence of Hospital Acquired Pneumonia (HAP) in Stroke Patients
2009 - Q1 - Q3 2012
HAP reported as high as 22% Hospitalized Stroke Patients
4.5
4
3.5
3
2.5
2
1.5
1
0.5
0
4.2
3.5
2009 n=173
Trendline
2010 n=191
2.3
2.3
2011 n=222
2012 n=172
Figure 2 St. Catherine of Siena Medical Center “Reducing Incident of Hospital Acquired
Pneumonia After Acute Stroke Through Implementation of Simple Bedside Dysphagia Screen”
Quality Symposium 2012
Page 161
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Cultivating Patient Safety: Integrating Simulation into Staff Development
Deborah A Kohn, BS RN CCRN; J Aidan Boswick, BA NREMT
St. Catherine of Siena Medical Center
Introduction
Catholic Health Services of Long Island (CHSLI) introduced the Patient Safety Simulation Center as a centralized
location dedicated to enhancing the quality and safety of patient care by promoting effective education and increasing
intrasystem collaboration between hospitals.
Problem
Facilitating more efficient utilization of critical care units necessitated safely increasing the level of acuity of the
patient population and the quality of care on several step-down units at Saint Catherine of Siena Medical Center.
Goals
The Simulation Center was utilized to support a series of innovative staff development programs which were designed
to strengthen clinician assessment skills, promote effective communication and collaboration, and enhance clinical
decision making.
Methods
Educational needs on step-down units within the hospital were assessed by conducting focus groups with unit
managers, staff, hospital leadership, and physicians. Simulation was selected as an effective method for achieving
identified educational objectives and course programming was developed in conjunction with the corporate Simulation
Center. Simulated patient cases were designed using data such as Rapid Response reports and other performance
improvement indicators assuring clinical relevance. Structured debriefing was facilitated by the simulation program
manager and the nurse educator to support the transfer of new and reinforced knowledge, skills, and attitudes to the
clinical setting. Participants were evaluated using a pre-developed list of critical actions. Participants evaluated the
entire simulation experience after completing the course.
Results
Anecdotal responses indicate a significant shift toward a more positive, curious, team-oriented nursing culture on each
unit. Participant evaluations of the experience have been overwhelmingly enthusiastic.
Conclusions
Ongoing evaluation of quality and performance improvement indicators and patient satisfaction reports may provide
further statistical data to support the effectiveness of this simulation-based educational program in translating to
improved patient outcomes. The integration of simulation and structured debriefing strategies can be a valuable
complement to staff development education programs.
Quality Symposium 2012
Page 162
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Comparison of Pre and Post Test Scoring in the Pain Management Resource Nurse Program
Nicolette Fiore-Lopez, RN MA CENP; Kathleen LeDoux, MS RN B-C CPHQ
St. Charles Hospital
Introduction
The correlation between education and improved pain management outcomes for patients has been well cited in
literature. The 2011 Institute of Medicine Report, "Relieving Pain in America" notes that "Pain management is now
considered an essential responsibility for nurses and nursing organizations acknowledge the need for prompt, safe, and
effective pain management." As part of a "joint position statement the American College of Emergency Physicians and
The American Society for Pain Management Nursing core principles enunciated that clinical education and resources
should support optimal pain management and that research and education are encouraged to support widespread
dissemination of evidenced based analgesic practices.” (IOM pg. 202-203)
Problem
To demonstrate a relationship to AONE Guiding Principles for Future Patient Care Delivery: The development of the
Clinical Nurse Leader, who demonstrates strengthened knowledge of evidenced based practice to improve patient care
and outcomes is strongly aligned with the “nursing profession that views pain as a complex multi dimensional
experience that responds subjectively to both physical and psychological stressors.” (IOM 2011 pg. 203)
Goals
To utilize a standardized pre and post test as evidence of improved clinical knowledge as it relates to caring for patients
with potential or actual pain during the presentation of a Pain Management Resource Nurse program at St. Charles
Hospital, Port Jefferson, New York.
Methods
Replicability: The course curriculum and pre- and post-tests are provided by the PRN Program Curriculum and
Planning Guide, copyright 2008, University of Wisconsin Board of Regents. The program is an evidenced based
approach, developed by The Resource Center of the Alliance of State Pain Initiatives, the University of Wisconsin and
The Mayday Fund. The current pre- and post-test questions have been selected from the course curriculum and have
been utilized since the class inception at St. Charles in 2009.
A 30-question pre- and post-test is administered to class participants. The identity of the class member is unknown. All
tests are linked by paired numbers only. Participants are encouraged to complete each test on an individual basis. The
test allows the nurse to mark each answer as True/ False or Don’t Know. Test analysis would be conducted as follows:
Number correct on pre test, Number correct on post test, the Measure of Success is indicated by the improvement in the
post test scores: For the purpose of consistent scoring questions answered incorrectly or "I don’t know" were graded as
incorrect.
Results
PERFORMANCE IMPROVEMENT
MEASURES /INDICATOR September 30, 2011
N = 23 November 18, 2011
Quality Symposium 2012
Page 163
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
N = 17 Average 2011 Result
Total N = 40
Mean Score of Pre-Test 52.26% 53.86% 53.06%
Total Number of Pre-Test Questions Answered as “Don’t Know” 67 42 54.5
Mean Score of Post-Test 82.65% 75.41% 79.03
Total Number of Post-Test Questions Answered as “Don’t Know” 6 2 4
Improvement from Pre-Test to Post-Test Scoring 30.39 points 21.55 points 25.97
Size or Sample for the Project N = 23 N = 17 Total N = 40
Conclusions
The mean pre-test score for both class sessions was 53.06%. The mean post-test score for both sessions was 79.03%.
The variance between the two scores was an improvement of 25.97 points, demonstrating improved understanding of
the subject matter. In addition, nurses were able to come together in a collegial manner to share their work and life
experiences relating to pain and pain management. We will continue to utilize this methodology on a periodic basis to
evaluate the teaching strategies utilized and to provide information relating to the need for course updates and revision.
Quality Symposium 2012
Page 164
PERFORMANCE IMPROVEMENT MEASURES /INDICATOR September 30,2011 November 18,20111
N = 23
N = 17
Average 2011 Result
Total N = 40
Mean Score of Pre‐Test
52.26%
53.86%
53.06%
Total Number of Pre‐Test Questions Answered as “Don’t Know”
Mean Score of Post‐ Test 67
42
54.5
82.65%
75.41%
79.03
Total Number of Post‐Test Questions Answered as “Don’t Know”
6
2
4
Improvement from Pre‐Test to Post‐ Test Scoring
30.39 points
21.55 points
25.97
Size or Sample for the Project
N = 23
N = 17
Total N = 40
Quality Symposium 2012
Page 165
PRN Class Comparison of Pre and Post Test Scores
St. Charles Hospital September 30,2011
Comparison of PRN Test Scores September 30,2011
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
pre test
36.63 53.28 46.62 59.94 38.96 59.94 23.31 63.37 53.28 76.59 39.96 46.62 36.63 23.31 43.29 53.28 63.27 66.60 36.63 79.92 79.92 56.61 63.27
120.0089.91 76.59 83.25 76.59 73.26 89.91 86.58 79.92 89.91 86.58 79.92 96.93 76.59 89.91 63.27 79.92 86.58 93.24 66.60 89.91 100.00 76.59 96.57
post test
100.00
89.91
89.91
76.59
89.91
86.58
83.25
80.00
Test Scores
100.00
96.93
89.91
86.58
79.92
76.59
96.57
73.26
59.94
89.91
86.58
79.92
79.92
79.92 79.92
76.59
76.59
63.37
60.00
93.24
63.27
63.27
59.94
66.60 66.60
76.59
63.27
56.61
53.28
53.28
53.28
46.62
46.62
40.00
36.63
43.29
39.96
38.96
36.63
23.31
20.00
36.63
23.31
0.00
1
2
3
4
5
6
7
8
9
10
pre test
11
12
13
14
15
16
17
18
19
20
21
22
23
post test
Quality Symposium 2012
Page 166
November 18,2011
1
pre test
post test
120.00
2
3
49.95
23.21
53.28
56.61
56.61
66.60
St. Charles Hospital
8
9
10
11
12
13
14
15
36.63 46.62 63.27 56.61 76.59 39.96 79.92 49.95
Comparison of PRN Test Scores November 18,2011
66.60 66.60 73.28 73.26 73.26 73.26 76.59 79.92 79.92 79.92 83.25 89.91
4
66.60
5
6
53.28
7
53.28
49.95
16
17
53.28
63.27
89.91
96.57
100.00
96.57
89.91
80.00
79.92
76.59
Test Score
73.28
66.60
66.60
73.26
73.26
79.92
76.59
79.92
89.91
83.25
79.92
73.26
66.60
63.27
60.00
56.61
56.61
63.27
56.61
53.28
53.28
53.28
53.28
49.95
49.95
49.95
46.62
40.00
39.96
36.63
23.21
20.00
0.00
1
2
3
4
5
6
7
8
pre test
9
10
11
12
13
14
15
16
17
post test
Quality Symposium 2012
Page 167
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Bundle Up: Lowering Hospital-Acquired C. difficile Infections in the Face of Rising Community
Prevalence
Merima Sestovic, Brenda Grant, Paula Castellano-Flynn, Michael Parry
Stamford Hospital
Introduction
C. difficile infections have become a national problem despite efforts to improve hand hygiene, environmental hygiene
and antibiotic use. Collaborative hospital initiatives have devised strategies to control these infections and have met
with modest success. Despite these efforts, and compounded by the spread of new hypervirulent strains in the
community, C. difficile infections have become the most common hospital acquired infection in some institutions,
including our own.
Problem
At Stamford hospital we experienced annual increases in rates of hospital acquired C. difficile from 2001 to 2008,
peaking at 17.2 cases per 10,000 patient days in 2008. A multi-faceted approach to reduce these infections was
undertaken beginning in January 2008. At the same time the incidence of community-acquired cases was rising,
creating added risk in the hospital environment by increasing case density.
Goals
The goal was to reduce the annual incidence of hospital acquired C. difficile infections.
Methods
Single room isolation, gown and gloves (contact) precautions, elimination of rectal thermometers, a comprehensive
hand hygiene initiative and antibiotic stewardship program had been in place since 2002.
The following elements were incorporated in stages into a C. difficile bundle:
• Bleach for terminal cleaning of C. difficile rooms was introduced in 3/05, expanded to terminal cleaning of all rooms
in 2/08 and for daily cleaning of all rooms in 6/12
• Environmental cleaning improvement initiative begun in 6/07 with modest effect. This improved after a revised
monthly monitoring plan was introduced in 6/11
• Isolation of C. difficile patients for the full length of their hospitalization was implemented in 7/08
• Booklet titled 'What you need to know about C. difficile' created for patients and family education in 7/08
• New isolation sign to highlight the need for hand hygiene with soap and water, as distinguished from other types of
contact isolation, was introduced in 9/08. This was further revised in 10/11.
• Chlorhexidine bathing for all isolation patients started in 9/08
• Flagging readmissions with history of C. difficile through registration began in 10/08
• Incorporation of probiotic reminders into many antibiotic order sets in 6/09
• PCR technology for C. difficile detection introduced in 7/09
Results
From 2008 to 2012, despite annual increases in community-acquired C. difficile cases of 17.6% per year, hospital
acquired cases have been reduced by 11.4% per year. This equates to 6.3 cases per month, down from 10.2 cases per
Quality Symposium 2012
Page 168
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
month in 2008 (see figures 1 and 2).
In achieving this goal, we perform an average of 215 C. difficile PCR tests per month with 15.6% positivity, of which
16.8% are NAP-1 positive. Environmental terminal cleaning has increased from 55% to 85% of high touch surfaces
cleaned. Hand hygiene rates have increased from 83% in 2009 per month to 94% compliance in the last 2 years.
From 2008 through 2011 we calculated that 68 cases of C. difficile were prevented for an estimated cost savings of
$488,172 based on estimates of 4.5 days excess length of stay and up to $7,179 excess costs per episode (Dubberke et
al, Clin Infect Dis, 2008; 46:497-504). With an attributable mortality averaging 10%, this equates to potentially 7 lives
saved (Dubberke et al, Emerg Infect Dis., 2008;14:1031-1038).
Conclusions
Despite increasing prevalence of C. difficile in the community and in the hospital, implementation of a comprehensive
C. difficile bundle can successfully reduce the number of new hospital-acquired cases resulting in dramatic savings in
healthcare costs, patient morbidity, and mortality.
Quality Symposium 2012
Page 169
Stamford C. difficile Cases Per Year
140
number of cases per year
120
100
80
60
40
20
20
12
*
20
11
20
10
20
09
20
08
20
07
20
06
20
05
20
04
20
03
20
02
20
01
20
00
19
99
0
calendar year
Figure 1: Annual number of C. difficile cases at Stamford Hospital from 1999 thru 2012.
*2012- annualized from January through August.
Stamford Trending for New C. difficile cases
55
number of quarterly cases
50
y = 21.229e
0.0423x
45
40
35
30
25
20
y = 30.914e
15
-0.0214x
10
5
Hospital-acquired
Community-acquired
0
08
20
1
2
3
4
09
20
1
2
3
4
10
20
1
2
3
4
11
20
1
2
3
4
12
20
1
2
calendar quarter
Figure 2: Comparison of new hospital- and community-acquired C. difficile cases per quarter Quality Symposium 2012
Page 170
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
HCAHPS: Responding to the Voice of the Patient
Elizabeth E Longmore, MSN RN CEN; Sarah Sanders, BSN RN
Stamford Hospital
Introduction
Since the inception of Value Based Purchasing (VBP), hospitals have found themselves racing to improve the patient’s
perception of care as measured by the Hospital Consumer Assessment of Healthcare Providers and Systems
(HCAHPS) Survey. As a determinant of federal fiscal year 2013 Medicare payments, VBP has two components: the
Clinical Process of Care Domain, accounting for 70% of the total performance score, and the Patient Experience of
Care Domain, accounting for 30% of the total performance score.
Problem
In 2006, Stamford Hospital began its participation in the HCAHPS survey. From 2006 to the summer of 2011, the
Hospital experienced stagnant performance in all 8 of the HCAHPS domains. Stamford Hospital is a Planetree affiliate.
Planetree is a model of care focused on personalizing, humanizing and demystifying the healthcare experience for
patients and their families. Despite Stamford Hospital’s focus on the patient experience and commitment to the
Planetree philosophy, many of our initiatives did not specifically address HCAHPS measures, which are largely
focused on provider communication.
Goals
Our goal was to identify and implement high impact, sustainable interventions that would rapidly improve our scores
in all 8 domains of the HCAHPS Survey.
Methods
In April of 2011, our HCAHPS improvement plan began with the initiation of discharge phone calls. This phase was
strategically designed to concurrently monitor feedback from our patients and identify themes related to the patient
experience. This also provided an opportunity for the clinical staff performing the phone calls to address concerns
regarding the patient’s transition of care from the hospital to their home.
The next phase of the improvement plan began in June of 2011 with the rollout of hourly rounding. Hourly rounding
provides the infrastructure for staff to interact with patients and families at regular intervals. In order to evaluate the
effectiveness of this process, nursing leadership consistently validated the staff’s performance on "8 key behaviors."
The behaviors are targeted at developing effective communication between the patient and their caregiver, and
anticipation of the patient’s needs.
The third phase of our implementation was the adoption of a multidisciplinary approach to improving and sustaining
outcomes related to the patient’s perception of care. In December of 2011, a multidisciplinary Patient Satisfaction
Steering Committee (PSSC) was formed. This committee is comprised of 8 task forces, each focused on one of the 8
domains of the HCAHPS Survey. Nursing leadership provides direct feedback from the discharge phone calls, hourly
rounding, leadership rounding, and survey comment reports to the PSSC. The PSSC then assigns the appropriate task
force to address the identified themes.
Quality Symposium 2012
Page 171
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
This approach of using concurrent data along with analysis of performance on our surveys, has led to rapid and
consistent improvements in patient experience outcomes. A specific example is our "Ask the Pharmacist Program,"
which has addressed deficiencies in patient’s knowledge of their medications. This is a consultative service provided
by the pharmacy, which brings the pharmacist to the patient’s bedside to provide education on medications, side effects
associated with them, and assists in discharge instruction (Figure 1 summarizes key interventions for each of the eight
HCAHPS domains).
Results
In the 12-month period since implementation of the three phases of improvement, Stamford Hospital has experienced a
3-8 percentage point gain in all 8 of the HCAHPS domains (see Figure 2).
Conclusions
Our greatest successes have come from our strategic approach in the implementation of measurable interventions and
innovations. This along with the multidisciplinary engagement of key stakeholders has contributed to gains in
HCAHPS scores. We recognize that sustaining the gains that we have made is no longer sufficient in the VBP
environment. The organization continues to develop the staff's communication skills, their ability to anticipate patient
needs during the stay and following discharge, and the staff's responsiveness.
Quality Symposium 2012
Page 172
Figure 1:
Figure 2:
Quality Symposium 2012
Page 173
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
VENT ALERT! The Rapid Throughput of a Critically Ill Ventilated Patient to the ICU
Christin J Lucia, RN (CCRN Resource Nurse); Melinda Panapada, BS RRT (Respiratory Clinical
Coordinator); Kenneth Pestone, BS RRT (Respiratory Therapy Supervisor); Robert Salvi, MBA RPFT
(Manager Medical Services); Melissa Degnan, BS RRT (Respiratory Clinical Coordinator); Steven Thau, MD
FCCP (Board Certified in Pulmonary Medicine, Critical Care Medicine and Sleep Medicine); Theresa Miano,
RN (ED Charge Nurse)
Stamford Hospital
Introduction
The American Heart Association (AHA) recommends that healthcare systems implement a comprehensive, structured
and multidisciplinary system of care for the treatment of post-cardiopulmonary arrest patients. A "Rapid Response"
approach to treating other critically ill patients with stroke or myocardial infarction is practiced internationally due to
the attendant improvements in patient outcomes and mortality. The critically ill ventilated patient may have multiple
additional risk factors that can affect their mortality and morbidity, so we elected to address this issue.
Problem
Between April 2011 and December 2011, Stamford Hospital saw an increased length of stay for ED critically ill
mechanically ventilated patients waiting to be transferred to the ICU. Upon initial review, the average time a critically
ill mechanically ventilated patient spent in the ED until arrival to the ICU was 106.1 minutes. This lengthy ED stay
delayed the patient from receiving critical interventions in a higher level of care, i.e., induced hypothermia treatment.
Goals
The goal was to develop and implement a safe and rapid transport and admission process for the critically ill
mechanically ventilated medical patient, for transfer from the ED to the ICU, by:
• Decreasing the time that vital hospital resources are utilized in the ED with the patient.
• Facilitating quicker throughput to the ICU allowing faster treatment of other emergency room patients.
• Expediting a smaller patient ratio to allow for early goal directed therapies and closer patient monitoring.
• Reducing other risk factors that can affect the mortality, morbidity and length of stay of these patients by
implementing VAP, CLABSI and CAUTI bundles earlier in the patient's care.
Methods
A systematic review of current Rapid Response teams and other emergency alerts (for example, stroke alert and PAMI
alert) best practices, was undertaken. Stamford Hospital's ED Vent Team was then created to identify the critically ill
ventilated patients in a more timely fashion and to implement early treatment to improve outcomes.
The team began by creating the "ED Vent" team. Key steps in the process are as follows:
• ED staff notifies the switchboard operator once a mechanically ventilated patient is en route to ED or pending
intubation while in the ED.
• The operator sends a notification page to the vent team pager group, "ED Vent".
• The team members consist of: Switchboard operator (network engineer), Nursing Supervisor/Bed manager, Resource
RN/ Rapid Response RN, ICU Medical Resident, ICU Clinical Coordinator, ED staff, and 2 Respiratory Therapists.
The Resource RN, ICU Medical Resident and two Respiratory Therapists are expected to report to the ED immediately.
Quality Symposium 2012
Page 174
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• The patient is rapidly stabilized in the ED and prepared for transport to ICU.
• The ED Physician is responsible for assessing the patient and for ordering the ED/ventilator order set.
• The Respiratory Therapist and the Resource Nurse help the ED Nurse to assess and stabilize the patient. They also
help transport the patient to any immediate testing and then directly to ICU.
• The ICU Medical Resident is responsible for rapidly assessing the patient as well as for ordering the ICU general
admission order set.
• The Nursing Supervisor and the ICU Clinical Coordinator assist in making sure a bed is ready and available for the
patient.
• Report on the patient is called to the ICU Nurse by the ED Nurse in the ED or from the testing site prior to arrival in
the ICU.
• If at any time it is deemed that the patient does not qualify as a medical ICU admission, the patient is triaged to the
appropriate location.
"Door time" was defined as the ED arrival time if intubated in the field, or the time of intubation in the ED. "CT time"
was defined as time of arrival in CT scan. "ICU time" was defined as time of arrival in the ICU. Door time to ICU time
included the time spent in CT scan or other testing prior to ICU arrival. The only patient population excluded from this
process were intubated trauma codes.
Baseline data, before Vent Team implementation, were collected from May 5th, 2011 to February 23rd, 2012. Data for
analysis after Vent Team implementation were collected from February 27th, 2012 to August 29th, 2012.
Results
Prior to implementation of the Vent Team, the average time from door to CT scan was 64.9 minutes. After
implementation of the Vent Team, Door to CT time decreased to 42.5 minutes, a 34.5% improvement.
The average Door to ICU time for a critically ill ventilated patient was 106.1 minutes prior to Vent Team
implementation. After implementation, the Door to ICU time fell to 87.4 minutes, a decrease of 17.6%.
We also noted a decreased door to procedure time for patients going to the operating room or cath lab instead of the
ICU. Time intervals in these instances fell from 56.5 minutes before, to 38 minutes after implementation of the Vent
Team, an improvement of 32.7% (see Figure 1).
A more efficient process has lead to a decrease in variation of length of stay in the ED (see Figure 2).
Conclusions
Creation of a novel, multidisciplinary Vent Team enabled critically ill patients ventilated in the ED to be more rapidly
triaged to CT scan, the ICU, or the OR, resulting in more rapid implementation of definitive treatment and early goal
directed therapy. Door to CT scan time fell by 34% to 43 minutes, and Door to ICU time fell by 17% to 87 minutes.
The Vent Team allowed for a more efficient use of essential hospital resources and a decrease in the length of stay in
the ED.
Quality Symposium 2012
Page 175
Quality Symposium 2012
Page 176
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Maintaining our Hustle for Muscle: Hard-Wiring Primary PCI Performance
Darlene Sweet BSN RN; Perry Burgess, BSN RN
Stamford Hospital
Introduction
American College of Cardiology (ACC) and American Heart Association (AHA) guidelines recommend treatment of
ST segment elevation myocardial infarction (STEMI) patients with primary percutaneous coronary intervention (PCI).
For optimal outcomes, a door-to-balloon (DTB) time of 90 minutes or less is recommended. The Centers for Medicare
and Medicaid Services (CMS) has adopted the percent of STEMI patients receiving primary PCI within 90 minutes as
a quality improvement (QI) measure in its Hospital Inpatient Quality Reporting and Value Based Purchasing Programs.
Problem
Stamford Hospital began its efforts to improve primary PCI performance five years ago. DTB times were inconsistent
with X% of primary PCI procedures completed within 90 minutes, and a median procedure time of X minutes. The
organization developed a protocol inclusive of a number of evidence based strategies to reduce DTB times. The
collective interventions resulted in the organization first completing over 90% of primary PCI cases within 90 minutes
in the X quarter of 20XX. However, it was challenging to sustain this high level of performance continuously. The
multidisciplinary primary PCI team sought to define, implement, and evaluate interventions that would "hard-wire" this
high level of performance. This required close evaluation of the intermediate time intervals comprising the DTB time,
and implementation of more durable process changes.
Goals
The over-arching goal of the QI effort was to maintain DTB times within 90 minutes of 95% or greater on a continuous
basis. To achieve this, the QI team developed the following process objectives:
1. Maintain more standardized processed for movement of patients from the emergency department (ED) to
catheterization laboratory.
2. Utilize common processes for emergency medical services arrivals and transfers from the organization's
intermediate care center across town.
3. Ensure accurate and consistent monitoring of time intervals.
4. Maintain ongoing interdisciplinary awareness, review, and accountability for results.
Methods
Practice changes were implemented throughout year 2010. This was enabled by a structured monthly interdisciplinary
DTB meeting attended by leadership and staff from the catheterization laboratory, cardiology, ED, nursing, regional
emergency medical services (EMS), and clinical effectiveness groups.
Key interventions were as follows:
A. Development of a "FEDEX" package bundle
1. Rapid patient registration process
2. Reliance on EMS interpretation for initial electrocardiogram reads
3. Development of a primary PCI box, including various PCI specific equipment to enable timely patient prep.
4. Standardized PYXIS medication kits
Quality Symposium 2012
Page 177
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
B. Analysis
1. Review of sub-intervals and process interdependencies with a Gantt chart for every primary PCI case
2. Use of a primary PCI documentation tool for each case, which was available online
C. Promotion of the effort, with the motto of "We Hustle for Muscle!
Results
Sustained Door to Balloon time of less than 90 minutes for 100% of CMS qualified cases for 6 consecutive quarters,
including a decrease in mean D2B time from 60 minutes in FY2011 to 55 minutes in FYTD 2012 through August (See
Figure 1).
Conclusions
Stamford Hospital was able to continue to reduce DTB times and sustain performance at 100% for nearly 2 years. An
effort that combines continuous interdisciplinary teamwork, a clearly defined and standardized bundle of interventions,
intensive real-time analysis, and proactive promotion can result in sustained high levels of performance.
Quality Symposium 2012
Page 178
Figure 1:
Figure 2:
D2B Process: Percent < 90 Minutes
FY 09 - FY 12 ytd by Quarter
100
90
80
70
60
50
40
% <90
FY 09 FY 09 FY 09 FY 09 FY 10 FY 10 FY 10 FY 10 FY 11 FY 11 FY 11
Q1
Q2
Q3
Q4
Q2
Q3
Q4
Q1
Q1
Q2
Q3
100
83
92
100
78
80
80
100
67
100
100
FY
11Q4
100
FY 12 FY 12 FY 12 STATE NATIO
Q1
Q2
Q3
CT
NAL
100
100
100
93
93
Quality Symposium 2012
Page 179
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Improving ED Throughput: Creating Change in a Challenging Climate
Rohit Bhalla, MD MPH; Ritu G Jain, MPH; Maher Madhoun, MD; Jayson Podber, MD; Sarah Sanders, RN;
Elizabeth E Longmore, RN MSN; Theresa Miano, RN; John Hegarty; Janet Palladino; Scott Dunn; Tim
Woodward; Kathleen A Silard, RN MS
Stamford Hospital
Introduction
The Institute of Medicine issued three reports in 2006 on the future of emergency care. The reports highlighted the
degree to which emergency department (ED) capacity and funding constraints have led to overcrowding, potentially
unsafe care, and the inability to accommodate volume surges accompanying disasters. Accordingly, patients often
experience high wait times for evaluation, management, and admission. Absent major structural and policy changes,
organizations have developed varied approaches to facilitate ED throughput.
The Robert Wood Johnson Foundation developed a national collaborative, Urgent Matters, to promote development of
strategies and organizational learning related to ED management. A toolkit of best practices for improving patient flow
was developed, and an updated version was released in 2011. However, a recent policy analysis found that such
strategies are widely under-utilized (Rabin, et al, Health Affairs, 2012). The Centers for Medicare and Medicaid
Services now requires the collection of ED throughput parameters as part of its quality reporting programs.
Problem
The organization's ED was designed to accommodate up to 30,000 visits per year, but annual visit volumes were
nearing 50,000 visits. This was increasing times to disposition and admit patients, and was contributing to staff and
patient dissatisfaction. Accordingly, the organization sought to improve ED throughput, and the project focused on
reducing ED length of stay for admitted patients, which was averaging six hours.
Goals
The goal of the project was to decrease ED length of stay for admitted patients by 25%. Two key process steps were
identified for intervention: the admission-decision to admission-orders process, and the bed request initiation process.
Methods
The initiative was coordinated and enabled through formation of a broad-based multidisciplinary team. Members
included leadership and staff from the ED, Hospitalist program, Admitting, Pathology, Radiology, Care Management,
Information Technology, and Clinical Effectiveness groups. Lean Six Sigma methodology was used to analyze
problems and manage solution development. The group, led by the Executive VP of Operations, initially convened in
2009, and conceptualized interventions in 3 broad areas: 1) performance information management, 2) staffing, and 3)
workflow processes.
In the arena of performance information management, a comprehensive process map of ED throughput was developed,
facilitating analysis of key limitations of the then current processes. An ED Throughput Scorecard was developed,
which allowed definition of parameters such as throughput time subintervals (e.g., time from arrival to decision to
admit), ED volume by time of day, and performance of specific physician groups (e.g., Hospitalist patients).
Evaluation of scorecard data allowed for the identification and development of pertinent changes to enhance
Quality Symposium 2012
Page 180
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
throughput, and to accommodate volumes at peak times in the afternoon and evenings. A weekly e-mail distribution
was created to assess patients with throughput times over 500 minutes.
Planning, analysis and solution development progressed through mid 2010. Key interventions were initiated at that
time and continued thereafter. These included increasing nurse staffing, and adding a mid-level practitioner focused on
admissions during peak hours. ED physician presence at triage was extended, and there was increased education
regarding admission criteria. These changes were complemented by use of the Situation Background Assessment
Response (SBAR) communication approach among interdisciplinary staff. Hospitalist physicians were migrated to a
unit based approach, allowing for clearer communication between ED and unit based physicians.
A key workflow process change related to obtaining orders for patients who were to be admitted. Previously, in order
to request an inpatient bed, the ED physician required a comprehensive evaluation and set of orders by the accepting
physician. The process was changed to allow for the accepting physician to issue a set of holding orders to expedite
patient care and to allow for an inpatient bed to be requested. An escalation protocol was developed in the event that
the ED and accepting physicians did not concur on the decision to admit a patient. Other workflow changes included
obtaining expedited CT scans for patients requiring oral contrast, and more rapid creatinine results for patients
requiring CT scans with intravenous contrast.
Results
Figures 1 and 2 depict the changes in ED throughput processes over a three and a half year period. The pre-period
encompasses 18 months from January 2009 to June 2010, where the project was being conceptualized, and analysis
and planning were occurring. The post-period encompasses the 24-month intervention phase, where interventions were
initiated and rolled out.
In the period prior to intervention, ED visit volume increased by 4%, and the time from ED arrival to admission (for
admitted patients) increased by 1% (see Figure 1).
In the intervention period, ED visit volume increased by 9%, but the time from ED arrival to admission decreased by
14% (see Figure 2).
Conclusions
Formation of a broadly multidisciplinary team, intensive analysis, and changes in key processes resulted in a
significant improvement in ED throughput. Persistence of change was greatly facilitated by establishment of clear
accountabilities and ongoing assessment of performance data. Improvements in ED throughput can be achieved with
tailored process improvement approaches in the context of ongoing ED capacity constraints.
Quality Symposium 2012
Page 181
Figure 1:
Figure 2:
Quality Symposium 2012
Page 182
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Using Near Miss Events to Improve Patient Safety, Family-Centered Pediatric Pre-Surgical
Experience and Enhance High Reliability Performance of the Pediatric Pre-Surgical Testing and
Evaluation Process
Kathy Albert, DNP; Fiona Levy, MD; Vincent Parnell, MD; Gloria Collura, RN; Pat Abitabile; Nicole
Romanelli; Terri Ann Parnell, DNP
Steven and Alexandra Cohen Children's Medical Center
Introduction
Achieving and maintaining a high level of quality involves changing organizational culture. At the Steven and
Alexandra Cohen Children’s Medical Center of New York, the healthcare team has ventured beyond the traditional
role of quality improvement to an evolved methodology of utilizing "near miss" events as an indicator of the need for a
more robust look at the opportunity to implement risk reduction strategies which will prevent harm from omissions or
errors. Our quality journey takes us to a vision for the future - to measure and achieve the highest quality outcomes for
our pediatric patients. In keeping with the Institutes of Medicine's six domains of quality: safe; effective; efficient
timely; patient centric and equitable care; we have enhanced high reliability performance using data to engage the
physicans, nurses and departments to engage and embrace improvement changes which will be sustainable and
predicate harmful errors.
Problem
The purpose of this project was to improve the safety and efficiency of the pediatric pre-surgical process while creating
a more family-centered experience. Pediatric pre-surgical patients must have a completed History & Physical (H&P)
on their chart on the day of surgery demonstrating that they have been examined by a licensed practitioner to ensure
that they can safely undergo surgery and the rigors of anesthesia. Data analysis showed that 20% of pediatric presurgical patients did not have a completed H&P on their chart on the day of surgery. This is a threat to high reliability
patient safety as well as a family, patient, and staff dissatisfier and a compelling reason to improve the process as it
potentially posed a serious risk to patient safety and outcomes.
Goals
1) 100% of H&Ps present on chart on day of surgery
2) Reduction of delay times from scheduled start to actual start by 50 min
3) Improve the patient/family likelihood to recommend score
Methods
A root cause analysis collaboration between Quality Management and a multidisciplinary team of experts utilized Lean
methodology to identify sources of waste and process variation. Swimlane diagrams identified points of potential and
real failure. Lean methodology, data analysis and statistical process control were used to achieve buy-in, identify and
prioritize issues, conduct small tests of change, and sustain results. Concurrent data was collected for one month and
showed variability in the method of how H&Ps arrived in Ambulatory Surgery and if they arrived prior to or on the
day of surgery. Not having the H&P present delayed OR start times by an average of almost 40 minutes.
Results
Improvements included developing a standardized process for distributing the pre-surgical information to the families,
Quality Symposium 2012
Page 183
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
an inclusive screening form reviewed by the family, Pediatrician, Surgeon, Anesthesiologist, and Ambulatory Surgery
RN, role-appropriate clinical assessment and decision-making by the Ambulatory Surgical RN, and a comprehensive
review of the medical record 24-48 hours prior to surgery. As a result of meaningful process change, 99.8% of H&Ps
are present on the medical record on the day of surgery.
RESULTS SUMMARY:
• Yield of H&Ps on chart on day of surgery rose from 80% to 99.8%
• Sigma value rose from 2.4 to 4.4
• Delay from scheduled start to actual start of surgery decreased from 60 minutes, to 21.3 minutes to 9.6 minutes (84%
reduction)
• Regression analysis showed a positive correlation between the family’s likelihood to recommend Cohen Children’s
Medical Center based on the improved pre-surgical information that they received.
Conclusions
• A single, all-inclusive Pre-Surgical Screening Form that the parent/guardian, pediatrician, surgeon, anesthesiologist,
and Ambulatory Surgery Unit (ASU) RN complete, review, and sign
• The ASU RN contacts the family prior to surgery to review food guidelines and answer clinical questions. This was
previously done by the Admitting Office staff
• The ASU RN reviews the medical record for completeness and escalates issues to the physician according to an
action algorithm to standardize practice
• Packets containing the guide and medical forms are distributed by the surgeons’ offices for standardization and waste
reduction
• Increased scheduling flexibility and operational hours of the Child Life Orientation Program to help prepare families
and patients for surgery
• Total re-creation of the pre-surgical information for the family. The "Guide to Surgical Services for Parents and
Guardians" was vetted through the Office of Diversity, Health Literacy, and Inclusion
Quality Symposium 2012
Page 184
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Reducing Complications of Care in the Intensive Care Unit
Denise LeBlanc, RRT (Director, Respiratory Care & Pulmonary Function); Henry MacLellan, RN MPA
(Assistant Director of Nursing, Surgical Critical Care); Christine McMullan, MPA (Director of Continuous
Quality Improvement); Paul Francis Murphy (Data Analyst, Continuous Quality Improvement); Margaret M
Parker, MD FCCM (Director, Pediatric Intensive Care); Grace Propper, MS RN CPNP NNP-BC (Continuous
Quality Improvement); Paul Richman, MD (Director, Medical Intensive Care); Carolyn Santora, RN MSN
(Interim Chief Quality Officer, Associate Director of Patient Safety & Regulatory Affairs); Christine
Schuhmacher, RN MS (Clinical Analyst, Continuous Quality Improvement); Jeralyn Sigwart, RN MS PNP
CNS (Nurse Manager, Pediatrics & Pediatric Intensive Care); Lisa Sokoloff, BSN (Project Manager,
Continuous Quality Improvement); Shanthy Sridhar, MD (Director, Neonatal Intensive Care); Maureen
Turner, RRT (Associate Director, Respiratory Care Department); James Vosswinkel, MD (Director, Surgical
Intensive Care); Donna Wagner, RN MS (Clinical Nurse Specialist, Medical Intensive Care)
Stony Brook Medicine
Introduction
Stony Brook University Hospital is a 593 bed tertiary care and academic teaching hospital located on the east end of
Long Island, New York. We are a principal teaching hospital, physically linked to the State University of New York at
Stony Brook School of Medicine as well as four other graduate professional schools. We have a very diverse patient
population and a mix of adult and pediatric intensive care units. In 2004 we began our participation in the IHI Saving
100,000 Lives campaign with efforts continued and growing through the years. Multidisciplinary teams were formed in
several intensive care units, each led by a joint Medical Director and Nurse Manager team. The diverse team,
comprised of unit staff, infection control, quality, pharmacy, respiratory therapy and others, held monthly meetings and
utilized performance improvement tools such as FOCUS PDCA, and rapid cycle change to implement evidence based
bundles of care (as described by the Institute of Healthcare Improvement’s Saving 100,000 Lives Campaign) for
patients on ventilators and with central lines.
Problem
Complications of care increase morbidity, mortality, length of stay and costs.
Goals
• Reduce Mortality
• Improve patient outcomes: Reduce VAP and CLABSI
• Improve communication ( support multidisciplinary rounding process)
• Reduce LOS
Methods
• Improvement Teams were formed for all ICUs
• Senior leaders are involved to remove barriers and facilitate change
• Evidence based best practice is identified and process changes planned and trialed as per rapid cycle tests of
change, and successful process redesign is adopted
• Tools to enhance standardization of work and communication are developed and utilized
• Opportunities were identified based on outcomes data (VAP and CLABSI rates as defined by the Centers for Disease
Quality Symposium 2012
Page 185
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Control and comparison data as per the NHSN Project)
• Data related to compliance to process and outcomes is collected and shared with all stakeholders and directs
improvement efforts
• Decisions related to process improvement cycles is made by the individual teams and the ICU Committee, all of
whom include senior clinical and administrative leaders
Results
In our organization the Hospital Epidemiology Department collects both the Ventilator and Central Line Days and
performs chart reviews to assess all intubated ICU patients for VAP or Line infection based on CDC criteria. Rates and
detail information is initially shared with unit leadership and eventually discussed during the Multidisciplinary IHI
Team meetings.
Current overall ICU CLABSI rates exhibit an 85.9% improvement these past 12 months when compared with our
baseline period. Our current mean for 2012 is proving to be our lowest yet at just 0.61 for the first 6 months of the
year. Our adult units continue to hold their gain with an overall improvement rate of 92.3%. Our CICU leads this field
with a total improvement of 100%, followed closely by our MICU, 97.7%. Both of these units meet the NHSN best
quartile goal. Our pediatric units are holding at nearly 70% improvement, with our Pediatric Hem/Onc unit well below
the evidence-based literature mean (see Table 1).
Current overall ICU VAP rates exhibit a 100% improvement these past 12 months when compared with our baseline
period. As of June 2012, our hospital has gone an unprecedented full year without a ventilator-associated pneumonia.
All units are currently at or below their NHSN best quartile performance (see Table 2).
These improvements in both VAP and CLABSI equate to nearly $7.5 million in saving for our 2011 calendar year.
Similar savings were realized each year since our implementation periods. CLABSI savings are calculated using the
John Hopkins University CLABSI Opportunity Estimator, providing both LOS and cost-savings based on realized
improvements. Saving attributed to VAP reductions are calculated from the First Do No Harm website, providing
similar cost estimates.
Conclusions
Recent years have demonstrated success with reduction in VAP and CLABSI in our pediatric and adult units. We have
been able to reach this goal and sustain improvement because we have changed clinical practice and put systems of
care into place that support best practice.
Quality Symposium 2012
Page 186
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 187
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 188
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 189
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 190
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 191
Abstract Application
New York-Presbyterian Healthcare System Quality Symposium 2012
Quality Symposium 2012
Page 192
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Automated Electronic Sepsis Alert Promotes Early Identification and Improves Mortality
Grace Propper, MS RN CPNP NNP-BC; Christine McMullan, MPA CPHQ; Paul F Murphy, Data Analyst
Stony Brook University Hospital
Introduction
Sepsis is a complex syndrome that is difficult to define, diagnose, and treat. It is a range of clinical conditions caused
by the body's systemic response to an infection, which if it develops into severe sepsis, is accompanied by single or
multiple organ dysfunction or failure, leading to death. It is a major cause of mortality, killing approximately 1,400
people worldwide every day.
Patient safety was and continues to be one of our hospital’s leading strategic goals. Since mortality associated with
severe sepsis is high (30-50%), and our critically ill patients are particularly at risk, our hospital agreed to devote
resources to this initiative. Consequently, we actively engaged in the Surviving Sepsis Campaign via the Institute for
Healthcare Improvement’s Critical Care Learning Collaborative in January 2006. We agreed to adopt the Surviving
Sepsis Campaign’s goal of a 25% reduction in mortality. Our severe sepsis initiative was folded into pre-existing
critical care unit interdisciplinary teams and an interdisciplinary team was formed in our Emergency Department.
SBUMC implemented a modified version of the sepsis resuscitation bundle developed by the Surviving Sepsis
Campaign under the direction of the Society of Critical Care Medicine. The sepsis resuscitation bundle is administered
within the first six hours after presentation. The modified resuscitation bundle requires blood culture collection prior to
antibiotics, serum lactate measured, antibiotic timing and selection, and fluids and vasopressors for hypotension. An
adult severe sepsis resuscitation order set was developed for use hospital-wide.
Problem
Each of our critical care units developed a severe sepsis screening tool pertinent to their population. All patients are
screened in the critical care units at admission, daily and as needed. Severe sepsis screening was also built into our
triage system in the emergency department. The severe sepsis screening tool was copied on the back of our rapid
response team (RRT) form to ensure sepsis screening at each RRT call. Through this process we recognized that early
detection of severe sepsis was far more recognizable in our emergency department and intensive care units than on the
"floor." Since severe sepsis is an infrequent diagnosis on the "floor," nursing and medical staff are not always
conscious of discrete medical changes that may indicate the early signs of severe sepsis. Simultaneously the roll out of
our electronic medical record was proceeding making paper processes obsolete and more often incomplete as staff’s
focus changed.
Goals
Knowing that early identification and treatment of severe sepsis contributes to increased survival and decreased
hospital stay we began to develop an electronic alert system with the goal of increasing early detection of severe sepsis
hospital wide and improving compliance with delivery of the modified resuscitation bundle (first four elements).
Methods
Our paper sepsis screening process asked three questions: 1) Is the patient’s history suggestive of a NEW infection; 2)
Are any two of the following signs and symptoms both present and new to the patient? (Temperature < 36° C or >
38.3° C, Heart Rate > 90 bpm, Respiratory Rate > 20 breaths/min, White Blood Cell Count > 12,000 or < 4,000
Quality Symposium 2012
Page 193
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
cells/mm3, Acutely altered mental status; 3) Are any organ dysfunction criteria that are not considered to be chronic
conditions present? Due to the success of the paper system we developed a process that mimicked the paper screen.
Two medicine units were chosen to pilot the electronic sepsis alert and evaluate for usefulness. A team of physicians
and nurses from the two units as well as IT, clinical informatics and quality management personnel was created late in
2010.
SBUH utilizes FOCUS PDCA as the performance improvement methodology for process improvement. Changes were
identified and implemented in order to increase efficiency and effectiveness. Modified changes were then retested and
re-evaluated. Data was displayed on control charts on an ongoing basis to monitor improvements attained by process
changes. Evidence based literature supported all of the process improvements implemented by the team. Outcome data
and compliance data were monitored on a monthly basis to determine if the implemented improvement achieved the
desired results.
A "Notify MD-Suspicion of Sepsis" order was built into the Medicine Admission Power Plan (admission order set).
This order is activated when the patient meets criteria as follows:
• No active Comfort Measures order within the last 48 hours
• Patient meets any two of the SIRS criteria in the last 4 hours and it hasn’t fired for the same patient for any user in
the last 8 hours.
When the "Notify MD-Suspicion of Sepsis" order is activated the RN is tasked to complete an electronic screen. The
screen asks the nurse if she is concerned that the patient may have developed a new infection or an escalation of an
existing infection in the past 48 hours. If she answers yes, she notify’s the physician, the order is complete and a lactic
acid order is ordered and waiting for the nurse to collect. If she says no there is no further action required.
Lactate was determined by the team to be inexpensive and helpful to the physician in evaluating patients suspected of
having severe sepsis. A "lactic acid when patient meets criteria" order was built into the Medicine Admission Power
Plan (admission order set) and is activated when the nurse answers yes, she is concerned. When the physician goes into
his rounds list he will see an icon telling him that the lactic acid was ordered due to the patient meeting sepsis criteria.
A similar process was created in the case that the Medicine Admission Power Plan is not used.
Enhancements implemented during the paper process continued including an automatic call by the lab to the
unit/department for a lactate critical value (= 4 mmol/L), and automatic reorder of a serum lactate within 2 hours after
an elevated result of = 2mmol/L is received to monitor efficacy of treatment.
Approximately one month prior to unit roll out the process is formally presented at faculty meetings and to unit staff
and leadership and the orders are built into the unit’s admission power plan. Flowcharts were developed to identify
steps in the process and aid in staff education (see Figures 1 & 2).
Approximately 80 beds "go live" every three months. Weekly conference calls are held with representation from the
units, IT, clinical informatics, and quality management personnel to discuss challenges and successes. Weekly
compliance data is provided by quality management to units for the first three months after "go live". Clinical nurse
specialists and nurse managers have access to the daily compliance reports for ongoing real time management of their
Quality Symposium 2012
Page 194
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
units. In addition the quality management practitioner for each service conducts reviews of all cases with a lactate > 2
to evaluate the components of the resuscitation bundle. Cases are discussed with the CNS of the service as well as
medical leadership and presented at the monthly interdisciplinary quality meeting along with compliance with the
resuscitation bundle components.
Results
• Our hospital-wide severe sepsis mortality has declined by 40% as compared to our 2006 baseline. Our hospital-wide
12-month running mortality rate is currently at 15.33, compared to our original baseline rate of 26.70 (see Chart 1).
• 2011 shows more than a 100% increase from the 2009 average of 42 lactates/month on our two pilot units (see Chart
2).
• The annual number of cases identified on the medicine floors has increased with 20 cases identified in the first 2
quarters of 2012 compared to 15-22 annually for the past three years (see Chart 3).
• The 2012 mortality rate to date for units with early identification using the electronic alert is zero (see Chart 3).
• Next steps include focus on compliance with the first four sepsis bundle measures. While lactate ordered within 6
hours (95%) and antibiotics within one hour (90%) are improving there are opportunities with blood cultures before
antibiotics (85%) and especially adequate fluid delivery (42.9%) (see Chart 3).
Conclusions
The current process has been successfully rolled out on seven units (approximately 190 beds). The roll out is limited by
available resources to monitor the units for the first three months until compliance goals (>95%) are met and they
begin to self monitor. Approximately 80 beds are rolled out every 3 months. The ICU’s, ED, oncology and pediatrics
will require some modifications to the process based on patient population. Units who have completed roll out are
focusing on delivery of early goal directed therapy.
Quality Symposium 2012
Page 195
Quality Symposium 2012
Page 196
Quality Symposium 2012
Page 197
Quality Symposium 2012
Page 198
Quality Symposium 2012
Page 199
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Reducing Radiation Exposure to Neonates
Olatokunboh Osineye, MBBS; Adeola Dabiri, MBA MPA; Torrance Akinsanya, RHIA MPA CPHQ; David
Dinhofer, MD; Charles Carbone, LRT ARRT; Michael Vaughn; Umar Jalloh, MPA; James Shanahan, MS
SUNY Downstate Medical Center/ University Hospital of Brooklyn
Introduction
There is an ongoing movement in radiology to reduce exposure to all patients, particularly in children. The American
College of Radiology (ACR) has an ongoing campaign with the slogan "Image Gently" which has been the governing
paradigm in the Department of Radiology’s dose reduction initiatives.
Problem
There is an ongoing movement in radiology to reduce exposure to all patients, particularly in children. The American
College of Radiology (ACR) has an ongoing campaign with the slogan "Image Gently" which has been the governing
paradigm in the Department of Radiology’s dose reduction initiatives. However, an article published in the New York
Times on February 27, 2011 titled "X-rays and Unshielded Infants" brought attention to Downstate Medical Center.
This article, which focused on collimation errors "also known as babygrams," reprioritized leadership goals to expedite
reduction in neonatal radiation exposure and resulted in a top down review of the x-ray practices in our NICU.
The project focused on three areas of improvement that have an impact on radiation exposure:
1. S values: A reference number used by manufacturers of x-ray equipment as an indirect measure of radiation
exposure from a radiograph. It measures x-ray exposure on a digital plate. As such, it is an indicator of relative
radiation dose.
2. Image Collimation: Used to reduce exposure of the body outside of the area of clinical concern.
3. Gonadal Shielding: Used to reduce exposure to the gonads, which are more sensitive to radiation than other tissues.
A lead shield is place over the gonads to reduce radiation exposure.
Goals
The main goal for this project was to promote the culture of safety by reducing the amount of radiation exposures in
neonates and exceeding the standards of the New York City Bureau of Radiological Health and New York State
Department of Health within 6 months through:
• The Utilization of S values greater than 100 in 100% of neonates
• Improving image collimation to 100% for all neonates
• Improving Gonadal Shielding to 100% for male neonates
Methods
The S-value, which appears on digital images, was made the focus of observation for NICU images. The number was
checked to make sure it was within the new standards by the supervisory staff. For our hospital’s equipment the
standard is an S-value greater than or equal to 100 and less than 800. Weekly reviews were conducted by the Chief
Technologist with immediate feedback to staff. All errors were counted and subtracted from the total number of exams
for each month in order to come up with a compliance index. 100% of cases in the NICU were reviewed.
The Pediatric Radiologist and the Radiation Safety Officer also reviewed the New York City Bureau of Radiological
Quality Symposium 2012
Page 200
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Health technical standards for proper collimation and educated the radiology technicians on proper collimation
technique. The images produced by the staff were then reviewed by the supervisory staff for proper image collimation.
All correctly collimated images were counted and divided by the total number of exams for each month in order to
come up with a compliance index. 100% of cases in the NICU were reviewed. Proper positioning was a subject of
education for the radiology technologists. The chief technician conducted weekly reviews of images for the presence
and proper positioning of the lead shield. All errors were counted and subtracted from the total number of exams for
each month and divided by the total number of exams in the sample in order to come up with a compliance index.
100% of cases in the NICU were reviewed.
Results
The baseline data in January 2011 showed an image with the required S-Value was 93% (77/83) compliant. Gonadal
shielding was 34% (28/83) compliant and compliance for collimation was 58% (43/83). As of December 2011, the
compliance for S-Value was at 99%, and 100% for gonadal shielding. Proper collimation was achieved in 100% of
cases for the reduction of radiation exposure to neonates. The Radiology Department has continued to maintain the
gain. Results of review findings were shared at the monthly Radiology and Neonatal Departments’ Performance
Improvement Committees, Faculty, the hospital-wide Performance Improvement Committee and Governing Body
meetings. Since implementation of this project, the Commissioner for NYSDOH has directed hospitals to develop
standards for radiation safety.
Conclusions
Our project demonstrated the importance of reducing radiation exposure to neonates to improve patient safety and it
long term negative effects.
The following changes were implemented to achieve success:
• The Director of Pediatric Radiology reviewed the exposure requirements and adjusted the Radiology Equipment
(Philips Convenio Portable Unit) S value to the lowest level that would give a satisfactory image and trained the
radiology technologists in this technique
• Verbal additions to Neonatology Radiology orders were discontinued and strongly enforced with an absolute
requirement for a clear and concise written, signed order for all imaging procedures.
• Training for position of lines, anatomy and physiology and pathology were given to all technologists
• The Performance Improvement Plan was revised accordingly and approved by our hospital leadership
• Policies were also developed and shared with Radiology and NICU Staff
• A special Grand Round on Radiation Dose Reduction in Diagnostic Imaging was held with participation of
Radiology Technicians, Radiologists, Residents and Administrative staff. Radiation Safety was included in the
Department of Neonatology monthly orientation of Residents’
• Technologists involved in the creation of non-compliant images were identified and reviewed individually
• The Radiation Safety Committee was made a subcommittee to the Medical Executive Committee and a hospital
administrator was appointed to oversee the committee
• The Radiation Safety Officer was appointed to the Radiology Department Performance Improvement Committee to
enhance communication and follow Through
Lesson Learned
Leadership commitment and visibility was a key factor in the success of this project. Normalized deviance must be
discouraged and zero tolerance for practice variation must be enforced to foster patient safety. Ongoing education and
vigilance.
Quality Symposium 2012
Page 201
SUNY DOWNSTATE MEDICAL CENTER
Radiology
NICU Radiograph S Values
100
92
92
90
80
75
99.3 99.3 100 98
100 99.4 100 100 99.3
10099 100100 99 99
100 100
100
98.8
93.9
94 93.692.3
80
84
70
60
60
50
40
30
20
10
0
41121
41090
41060
41029
40999
40968
40939
40907
40877
40847
40816
40786
40755
40724
40694
40679
40663
40643
3/29/2011
3/2011
1/2011
12/2010
11/2010
1/2010
12/2009
11/2009
1/2009
12/2008
11/2008
7/2007
Definition: % of Images with an S value over 100
Operational Indicator
Numerator: number of Images with an S value over 100
Denominator: Total number of Images recieved from NICU
Data Source:
Easy Vision (PACS)
Exclusions: Note: S Values are not a direct measure of patient dose.
It is used as a proxy to trend dose. A value < 100 does not imply an incident
Control Limits: 3 consecutive months below threshold
Target/Response Threshold: 100%
References: Staff meeting Sept. 2007, NYSDOH and NYCDOH Surveys
CC/WR
Quality Symposium 2012
Page 202
SUNY DOWNSTATE MEDICAL CENTER
Radiology
NICU Gonadal Shielding
Pediatric revised protocol for shielding of NICU was established on March 18, 2011
100 99.4100
100
100
100 100
100
100 100 100
100
99.1 100 99.4
100
90
81
80
70
60
First data collection 3-1 to 3-17-2011
50
40
30
20
10
41060
41029
40999
40968
40939
40907
40877
40847
09/30/11
08/31/11
7/31/11
6/30/11
5/31/11
5/16/11
4-30-11
4-9-11
40631
40619
Shielding
Definition: % of Images with shielding
Operational Indicator
Numerator: number of Images with shielding
Denominator: Total number of Images recieved from NICU 100% of Images
Data Source:
Easy Vision (PACS)
Exclusions: Written Physicians' order for no shielding
Control Limits: 1 month below threshold
Target/Response Threshold: 100%
References: Protocols X-Ray 21, NYSDOH Survey and NYCDOH Survey
CC/WR
Quality Symposium 2012
Page 203
SUNY DOWNSTATE MEDICAL CENTER
Radiology
NICU Collimation
100
90
Pediatric revised protocol for shielding of NICU was established on March 18, 2011
100 98
100
100
99.4 99.4
99.5 99.3100 99 100 99.4 99.1
100
98 99
92
99.3
80
70
60
50
40
30
First data collection 3-1 to 3-17-2011
20
10
41060
41029
40999
40968
40939
40907
40877
40847
09/30/11
08/31/11
7/31/11
6/30/11
5/31/11
5/16/11
4-30-11
4-9-11
40631
40619
Collimation
Definition: % of Images with collimation
Operational Indicator
Numerator: number of Images with collimation
Denominator: Total number of Images recieved from NICU
Data Source:
Easy Vision (PACS)
Exclusions: Written Physicians' order for wider collimation
Control Limits: 1 month below threshold
Target/Response Threshold: 100%
References: Protocols X-Ray 21, NYSDOH Survey and NYCDOH Survey
CC/WR
Quality Symposium 2012
Page 204
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Timely Recognition and Antibiotic in Severe Sepsis: The Children's Medical Center at Winthrop
Pediatric and ED Quality Improvement Initiative
Maria Lyn Quintos-Alagheband, MD; Lee Moldowsky MSNRN-BC; Sandee Zaera RN-BC
The Children's Medical Center at Winthrop University Hospital
Introduction
The Surviving Sepsis Campaign presents one of the most compelling argument for quality improvement and
standardization of care. A decade from the Barcelona declaration a direct line of evidence exist that timely and
effective care can influence outcome in patients with severe sepsis. Further, recent evidence shows that the critical
determinant of survival in human septic shock appears to be the time to initiation of effective antimicrobial therapy
(Kumar et al, Crit Care Med 2006).
Problem
At the Children's Medical Center Winthrop University Hospital our mortality from 2005-2009 included 4 pediatric
patients with severe sepsis and multiorgan failure. Our retrospective quality improvement review revealed opportunity
for earlier recognition and initiation of therapy. As early as 2009 we set out to develop and adopt a multifaceted model
based on teh surviving sepsis campaign and tailored for our institution to increase timely and appropriate recognition of
severe sepsis in our pediatric population, and to institute timely and evidence based management.
Goals
Our primary objective is to change bedside practice to be consistent with recently published guidelines for pediatric
patient with severe sepsis.
Primary Quality Performance Measure:
• Time to antibiotic in one hour from ED triage and floor recognition.
Secondary Quality Performance Measure:
• ED door to doc time under 15 minutes;
• Time to recognition of Severe Sepsis for in-patient pediatrics;
• Blood Culture prior to antibiotic administration and Serum Lactate Determination.
Methods
2009 - We organized a multidisciplinary team consisting of representatives from both the Pediatric and emergency
department. We designated champions from our physician and nursing staff to ignite the campaign.
I. Education Campaign
To build awareness and improve quality of care in pediatric patients with severe sepsis our initial efforts were centered
on an education campaign emphasizing early recognition and timely and evidence-based management. We introduced
our local campaign in 2009 through Pediatric grand rounds to reach both pediatric and ED faculty, housestaff and
community pediatricians. We then provided continuing education for our floor and PICU team through monthly case
conferences and review to reinforce the practice guidelines. The surviving sepsis campaign is integrated in the
residents monthly PICU and in-patient pediatric floor curriculum. We created a video conference module for our
Quality Symposium 2012
Page 205
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
nursing staff to educate them on core components of the surviving sepsis campaign. This module is now included in
nursing orientation. Our strategy was to target our front line staff resident and nursing to fuel the campaign.
II. Triage tools, Order sets and QI data collection tool:
To decrease door to doc time in pediatric sepsis we work with the pediatric ED team to developed a user friendly triage
screening tool for sepsis. During triage once a pediatric patients meets age based vital signs criteria for sepsis they are
assessed an ESI of 2. Our target is for patients with sepsis to be seen by a physician within 15 minutes and assessed for
severe sepsis.
We created a standardized pediatric severe sepsis order set which embodies evidence-based practice guidelines that is
trigerred once a diagnosis of severe sepsis is established.
To assessed our performance we designed a quality improvement audit tool. We set our primary performance outcome
measure to be time to first antibiotic administration under one hour. Our secondary quality performance indicators
include doc to door time in 15 minutes, timely recognition of Severe Sepsis syndrome, blood culture prior to antibiotic
administration and serum lactate measurement. All patients admitted to Pediatric Intensive Care Unit from April 2010
with a diagnosis of Severe sepsis were included in our quality improvement review.
Results
A total of 32 patients met criteria for Severe Sepsis from April 2010. 23 patients presented and met criteria for severe
sepsis in the Emergency Department. 9 patients met criteria for diagnosis of severe sepsis in the pediatric in-patient
service.
Patient Characteristics: Table I
Primary Quality Performance Measure: Time to antibiotic under one hour (see graph)
< 60 mins. > 60 mins.
ED 17 (74%)
6 (26%)
Floor 8 (89%)
1 (11%)
Secondary Quality Performance Measure: ED Door to Doc time
< 15mins.
> 15 mins
N 11 (48%)
12 (52%)
Floor time to Recognition:
4 (50%) - Recognized at first onset of VS abnormalities and clinical criterias
4 (50%) - Delayed recognition with mean time at 4 hours
Other Quality Performance Indicator
I. Blood Culture prior to Broad spectrum Antibiotic Therapy: 100%
Microbiology: Organism identified: 24/32 (75%)
II. Blood Lactate Measurement: 100%
Conclusions
Quality Symposium 2012
Page 206
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Recent evidence evidence shows that the single measure that appears to influence patient outcome is the timeliness and
appropriateness of broad spectrum antibiotic therapy. For that reason, our group set our primary target goal to be time
to antibiotic therapy within one hour. Overall we are able to achieve 75% compliance in this measure.
Further data analysis shows that a major factor that influences time to antibiotic in the ED is door to doc time. Patient
with door to doc time > 15mins, had mean time to antibiotic = 91mins. On the floor the major determinant of delayed
therapy is the failure to recognized the syndrome of severe sepsis. In 2012, we put a strong emphasis in a joint
collaborative with the Emergency Department to improve our triage process and through put. One of the big challenge
we face in pediatrics is the complexity of the triage process because of factors like developmental milestone, wide
range of age dependent Vital Signs limit, family dynamics and triage staff experience with pediatric patients. Through
the patient safety committee we have created a team to target specifically issues related to pediatric triage.
As in any campaign our biggest challenge is overcoming resistance from late adopters, particularly the faculty. Our
strategy is to focus on our housestaff and nursing staff who are the often the first responder at the bedside. Since 2010
we have put emphasis on educating our front line staff for in patient pediatrics.We will continue to focus our campaign
towards continuing education. Direct observation at this point demonstrate that our nursing and resident staff are more
likely to recognized and escalate concerns for severe sepsis.
Currently we are collaborating with IT to explore potential use of electronic medical record to set critical vital signs
and laboratory value alerts that will trigger stat evaluation for pediatric severe sepsis. In August 2012, we started our
first Pediatric ED Collaborative Care conference to strengthen our team relationship, share lessons learned, benefit
from mutual learning, explore grounds for improvement and celebrate team success. Our ongoing goal is to target
100% compliance on all quality measures.
Quality Symposium 2012
Page 207
Patient Characteristics
Age
1 month- 24 years
Sex
Males: 9, Female: 24
Vasopressor/Inotrope
N = 15
Mechanical ventilation
N=7
Average number of organ
dysfunction variables
2.5
Average PICU LOS
7 days
Mortality
3 (9.3%)
Quality Symposium 2012
Page 208
“Efficacy is Change Over Time”
Quality Symposium 2012
Page 209
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Swallowing Safety: "It’s No Gag"
Peter Jarosz, MA MS CCC/SLP; Josephine Bodino, RN MPA NE-BC
The Valley Hospital
Introduction
In late 2010, the need to establish a dysphagia screening tool to assess CVA patients was established as a quality
improvement Initiative. A comparison of our hospital to the American Stroke Association database indicated below
average scores in 2010 and 2011 for the Dysphagia Screening indicator. Additional research indicated our hospital was
also significantly lower than state registry scores.
Problem
American Stroke Association Database
Year
My Hospital All Hospitals
2009
75.7
75.9
2010
73.9
78.1
2011
74.7
80.0
New Jersey State Registry
Quarter My Hospital Statewide
2Q 2011 66.3
86.0
In 2011, The Acute Stroke Committee felt it to be imperative to improve this indicator. Speech Pathology research
reveals that Dysphagia is a serious complication following onset of CVA, which contributes to Aspiration Pneumonia,
increased length of stay and even death! The Agency for Healthcare Research and Quality (AHRQ) has practice
guidelines highlighting the importance of assessing a patient’s ability to swallow prior to oral intake.
Goals
1. Emergency Department nurses to be trained to complete the Simple Water Screening to identify those HRS patients
at risk for aspiration prior to PO medication presentation.
2. Prevent patient complications such as aspiration pneumonia, malnutrition and increased length of hospital stay.
Methods
Over the last two years, this performance improvement project led by Peter Jarosz, Speech Pathology Supervisor,
organized numerous meetings with Emergency Department physicians, Nurses, Nursing Educators and Information
Systems to study the existing problem and develop a plan for remediation. Various strategies were incorporated
including contacting surrounding hospitals to determine existing swallowing screening procedures and literature search
to establish best practice.
The goals were: 1) to develop and implement a simple swallowing screening tool for the Emergency Department
nurses to quickly assess the ability of patient to swallow and 2) improve the timeliness in completing this screening in
anticipation of administering PO medication.
Quality Symposium 2012
Page 210
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Following creation of the tool, Emergency Department nurses were educated by the ED clinical Practice Specialist,
Advance Practice Nurse/Stroke Coordinator and Speech Therapist. Procedure and progress was shared at the Clinical
Support Performance Improvement Council and the Acute Stroke Committee meetings.
Nursing was instructed to complete the above Dysphagia/Swallowing Screening immediately upon admission to the
ED. Any identifiable difficulty/coughing triggers The Speech Pathologist for a formal Bedside Swallowing evaluation
with patient remaining NPO.
To further ensure patient "capture", additional admitting diagnoses were added requiring the Dysphagia/Swallowing
Screening in order to further enhance compliance with the GWTG expectations.
Results
% Compliance
2010
73.9
2011
74.7
2012 YTD 86.9
Jan
80
Feb
81.6
Mar
85.7
Apr
88.2
May
94.1
Jun
100
The above numbers illustrate the marked improvement since initiation date. Since Implementation, an additional “rule”
has been added whereby hospital information system/MAR requires a “PASS” by nursing or Speech Pathologist prior
to nurse gaining access to PYXIS system. Both Screening and formal Speech Pathology documentation have been
synched with the MAR prohibiting any administering of PO medication prior to this PASS from either party. This
“rule” will further ensure compliance with new protocol.
Conclusions
The goal of our stroke team is patient safety. We are certain that our collaborative effort coupled with the
determination of the entire team will enable us to reach our goal with regard to Patient safety and GWTG compliance.
As our most recent month indicates 100% compliance, we intend to continue our focus until the entire process is
enhanced and all those who are entrusted in our care are well taken care of.
Quality Symposium 2012
Page 211
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Eliminating VAPs in CSICU
Alcina Fonseca, RN MS MBA CCRN-CSC NE-BC; Gladys Reyes, MSN ACNP-BC CCRN-CSC-CMC; Lisa
Albarino, RN MSN CCRN CNRN
The Valley Hospital
Introduction
Ventilator associated pneumonia (VAP) is one of the most common healthcare acquired infections. According to the
American Association of Critical Care Nurses (2012) VAPs are associated with:
• Increased length of stay > 2 days
• Prolonged mechanical ventilation
• Increased morbidity and mortality
• Patient and family dissatisfaction
• Cost - $40,000 per patient or $1.2 billion annually in the United States
• Extended use of antimicrobial medication
The Center for Disease Control (CDC) and other regulatory agencies have joined to develop guidelines and best
practices to assist the healthcare practitioners in eliminating VAPs.
Problem
In 2009, the Cardiac Surgery Intensive Care Unit (CSICU) experienced an increase in VAPs. Three VAPs were
identified which translated to a rate of 3.6%. We benchmark with other hospitals that report to the Society of Thoracic
Surgery (STS) and also with the National Healthcare Safety Network. For 2009, the national benchmark for Surgical
Cardiothoracic ICU was 4.7%. While we were below the national benchmark we wanted to implement strategies to
prevent further VAPs. We promptly coordinated a multi-disciplinary team including respiratory therapy, nursing staff,
Advanced Practice Nurse (APN), Director, Manager, and Clinical Shift Supervisors (CSSs) from CSICU. We audited
the practices of nursing and respiratory therapy and found that the practice of instilling normal saline when suctioning
endotracheal tubes (ETT) or tracheostomies was still being utilized. Upon further exploration the staff verbalized that
the use of saline thinned and mobilized secretions.
Goals
Our objective was to achieve a goal of zero VAPs in the CSICU and to empower the nursing staff to apply evidence
based practice into their daily patient care.
Methods
We identified unit champions on each shift to assist with the education and practice change. A literature review was
conducted and presented by a staff nurse at the unit-based journal club. A poster was created and presented at the staff
meetings and displayed on the unit for all to review. The APN provided educational breakfast and lunch sessions to
further educate nursing and respiratory with current evidence based practice designed to eliminate VAPs.
We proceeded to remove all normal saline bullets from the bedside carts. A new oral hygiene care kit was purchased
and placed in the patient rooms by the Patient Care Associates daily at 0600. The kit was modified, with staff input, to
include all supplies required to provide oral hygiene in a 24-hour period. In addition to all of the above, we
Quality Symposium 2012
Page 212
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
implemented a VAP Bundle that is ordered by the MD or licensed independent practitioner (LIP) which includes
interventions such as head of bed elevation of 30 degrees, peptic ulcer prophylaxis, chlorhexidine gluconate oral care,
and the use of nasal bactroban. During multidisciplinary rounds the daily goals are communicated verbally and
documented on a daily goal sheet, which includes the following bundles: VAP, deep vein thrombosis (DVT), glycemic
control and other core measures.
Results
We continue to monitor our rates and we have achieved our objective of zero VAPs from October 2009 through June
2012, for a total of 32 months VAP free! We celebrated our accomplishments with Portuguese rolls for breakfast or
pizza per staff request. The nurses have continued their journey of success by holding each other and other members of
the multi-disciplinary team accountable.
Conclusions
CSICU is proud of its accomplishments. We encourage other units that are struggling with VAPs to incorporate some
of the steps we have taken to address the situation. First, form a multidisciplinary task force with the front line staff
members spear-heading the project. Second, share results and include the financial and negative impact on patient
outcomes.
Celebrate the minor successes with your staff as you continue the journey to zero VAP. As you experience a "bump"
on the road, have a non-punitive debriefing session with your team to brainstorm and refocus on how to learn from
these minor setbacks and continue moving forward towards achieving your goal.
Quality Symposium 2012
Page 213
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
A Community Medical Center’s Approach to Reducing Joint Replacement Surgical Site Infections
Allison Essenmacher, RN CNOR; Joanne Ritschdorff, RN MSN CNOR; Michelle Spola, RN CNOR; Barbara
Hirsch, RN; Scott Pietras; Richard Sleight; Mary Ann Magerl, RN MA CIC; Lynn Kemp, RN MA; Margaret M
Cusumano, RN MSN FACHE; Janet L Ready, RN FACHE; Stephen A Katz, MD CPE FACP
Vassar Brothers Medical Center
Introduction
Surgical Site Infections account for 17% of healthcare associated infections (HAI), making these the second most
common HAIs among hospital patients.
Problem
In 2008, our 365 bed community medical center experienced a higher than expected rate of surgical site infections
associated with total knee replacement and in 2009, it experienced an increased rate of surgical site total hip infections.
This increase was investigated and a multifaceted remediation plan was designed and implemented.
Goals
A comprehensive multi-faceted approach to reduce orthopedic surgical site infection.
Methods
A cluster of total knee joint infections was reported during the spring of 2008. A multidisciplinary management team,
along with the hospital’s Surgical Site Infection Committee initiated an investigation and gathered data on all
orthopedic patients, physicians, operating room suites, implant manufacturer and supplier lot numbers and organisms.
Based on the investigation’s results, the hospital initiated pre-surgical MRSA testing for all total joint patients in
August 2008.
Between May and July 2009, six total hip infections occurred. One surgeon was associated with four cases and one
surgeon each with the other two. All six procedures were performed in one operating room and various environmental
contaminating organisms were identified.
During the second half of 2009, the Quality Improvement Team addressed operating room physical plant issues and
engaged an outside environmental group to evaluate the orthopedic suite and perform airflow and exchange
assessments. Based on the results, positive airflow monitors were installed in all operating rooms.
In January 2010, the team identified drains, faucets and aerators as potential sources of contamination; these were
removed, cleaned and a preventive maintenance schedule was instituted. Additionally, the Facilities Department
removed overhead anesthesia columns from operating rooms found to have high levels of environmental contaminants.
A Clinical Outcomes and Coding group was formed and charged with reviewing all healthcare associated infections.
Its membership included representatives from Administration, Nursing, Hospital Information Management, Quality
Systems and Infection Prevention.
In 2011, the Surgical Site Infection Committee developed a shared electronic data base that was accessible to Surgical
Quality Symposium 2012
Page 214
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Services, Quality Systems and Infection Prevention. This electronic document storage system was designed to improve
information access and communication among the various interested parties.
Results
After implementing our multifaceted intervention, our total knee replacement surgical infection rate dropped from
5.6% in 2008 to 0.0% for 2009 through July 2012. Our 2009 total hip replacement surgical infection rate was 6.8%. In
2010 it was reduced to 3.1% and from 2011 through July 2012, the infection rate was 0.0%.
Conclusions
A comprehensive multi-faceted approach to orthopedic surgical site infection prevention reduced our infection rate to
0.0% during the study period.
Quality Symposium 2012
Page 215
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Improving Sepsis Care in ED Patients
Judith T Flaherty, RN CPHQ; Denise Quirk-Hall, NP CNS
Vassar Brothers Medical Center
Introduction
Sepsis is one of the more common disease processes causing hospital admissions. It is also one of the most expensive,
accounting for high pharmaceutical interventions and lengthy admissions. The STOP Sepsis Collaborative begun by
GNYHA / UHF partnership lead us to look at our practice with identification and treatment of septic and possibly
septic admissions to identify opportunities for improvement. It is the tenth leading cause of death in the United States,
with a mortality rate for severe sepsis and septic shock between 40% and 60%. Numerous studies have shown that
early intervention in the emergency department (ED), including antibiotic administration within the first hour of
recognition of severe sepsis, early and aggressive fluid resuscitation, and early critical care consultation can make a
significant difference in mortality. As the first six hours of treatment are considered the most crucial for outcomes, the
responsibility for prompt recognition and treatment often rests on the ED.
Problem
Early research in our ED revealed several barriers to optimal care, including lack of early recognition, standardized
treatments, and effective communication of concerns regarding plan of care. Further drill downs as well as literature
search identified gaps in the treatment protocols previously established. It was felt that a more comprehensive
treatment plan would lead to improved care and better outcomes.
Goals
In an effort to improve both process measures and outcomes, we launched a sepsis quality improvement project
primarily targeting the ED.
The goals of the initiative are:
(a) Improve early recognition of septic and early septic patients
(b) Standardize the early and efficient treatment of these patients with established and proven pathways
(c) To enhance communication between care givers, thus improving the care and outcomes of the patients
(d) Adequately educate staff (nursing and medical) with ongoing reviews of the process
Methods
The standardized sepsis protocol was developed within the ED, with the consensus of medical and nursing staff. This
was accompanied by education for nurses and physicians in the ED. Data that includes identified process measures
(e.g., time to sepsis recognition, time to antibiotic initiation, final disposition of patient) was collected on an ongoing
basis for all severe sepsis/septic shock/sepsis patients that presented to the ED, within the guidelines set by the review
group (age >18, curative goal, hospital admission).This data was and continues to be reviewed monthly at an
interdisciplinary team meeting that includes representatives from the ED, quality, and nursing management. Any
fallouts to established parameters are investigated as to the root cause, with ongoing education as necessary.
An invaluable piece of this project was the education of the nursing staff to identify possible sepsis patients with the
more subtle sequelae of the disease process, such as change in mental status, low B/P, vague complaints of "just not
Quality Symposium 2012
Page 216
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
feeling well", particularly in our large elderly population. The establishment of a "Code Sepsis" was initiated, with the
ability of any nursing staff, when presented with any possibly septic patient, to raise the alarm. This then set into
motion a well-choreographed sequence of events, after orders. These included bolusing of crystalloid fluids,
appropriate lab tests, and appropriate antibiotics dependent of the suspected source of infection, administered quickly.
As this progressed, our data points were edited. For example, the were no identifiable trends in fall outs of care when
looked at by day of the week or practitioner. Length of stay in the ED and as an inpatient led to many discussions but
no real actionable improvements.
Timing of recognition of a septic patient, speed in antibiotic administration and transfer to the appropriate level of care
(critical care when necessary) have been identified as salient data points, with high compliance leading to shorter
length of stay and improved outcomes (survival rates).
Results
Gross mortality for severe sepsis and septic shock patients identified during the first six months of our project exceeds
60%. Mean time to initial identification of sepsis, time to antibiotics, quantity of fluid resuscitation, and appropriate lab
testing have all improved significantly since the start of the project. There has been an average of decrease in
recognition and treatment times of greater than 50%. Survival rates, the ultimate outcome measure, have doubled with
the timely, aggressive treatment.
Conclusions
Sepsis is a complex problem that requires cooperation by many professions and disciplines across the hospital,
beginning with the ED. Ongoing data collection and review by an interdisciplinary team can be effective in improving
the process of care for this highly fatal illness. Engaging the support of medical, nursing, pharmacy and laboratory staff
with continuous review and feedback is necessary to maintain the commitment to improved care. The unquantifiable
measure that has most likely improved from this initiative is the patient who is not truly septic but benefits from the
improved intervention resulting from this initiative.
Quality Symposium 2012
Page 217
SEPSIS / SEVERE SEPSIS TREATMENT TIMES AND SURVIVAL RATES
70%
SURVIVAL RATE
60%
50%
40%
AVG DOOR TO RECOGNITION
(H:M)
30%
20%
10%
AVG RECOGNITION TO
ANTIBIOTIC (H:M)
0%
1Q10
2Q10
3Q10
4Q10
1Q11
2Q11
3Q11
4Q11
1Q12
2Q12
Quality Symposium 2012
Page 218
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Integrated Delivery System of Disinfection Cap & Flush Syringe, Plus Staff Education, Lowers
Bloodstream Infection Rate & Treatment Costs
Saungi McCalla, MSN MPH RN CIC; Janet Greco, MA RN-BC OCN; Meg Warren, MSN; Joyce Bogetti, RN;
Patricia Byrne, RPh MPA
White Plains Hospital
Introduction
Our hospital prides itself as a center of excellence, providing services that set it apart from most community hospitals.
Unfortunately its unique qualities were not able to insulate the hospital from a problem that plagues medical facilities
nationwide: incomplete disinfection of IV connectors. The conventional method for disinfecting connectors involves
scrubbing them with an isopropyl alcohol (IPA) swab for at least 15 seconds, then waiting an additional 30 seconds for
the alcohol to dry.
Because manual scrubbing involves several steps that each must be performed accurately, variance is common. Noncompliance is common, as well, because nurses who feel time pressure may skip the protocol entirely. With both
variance and noncompliance, the failure to appropriately disinfect connectors increases the risk of central line
associated blood stream infections (CLABSIs).
The hospital noted that although our CLABSI rate in the critical areas were below the national benchmark, the
CLABSI rate in the PICCs were problematic. PICC line use was relatively new to the hospital and had grown
significantly due to line stability and patient convenience. An interdisciplinary team was developed to review the gaps
in our current protocol and practices, and to also research and apply other evidenced based practices as appropriate.
Problem
In January 2010, the hospital began CLABSI surveillance on peripherally inserted central catheters (PICCs) as the
usage of these central lines had grown. The data revealed an unsatisfactory CLABSI rate of 3.85/1,000 central line
days). The PICC Team and Infection Control staff investigated the matter, which included interviewing nurses. They
found that both variance and noncompliance were indeed occurring, making them likely factors in the high CLABSI
rates.
To address the problem, the hospital trialed a combination IV flush syringe and disinfection cap. The cap dispenses
IPA when twisted onto luer-lock IV connectors, supplementing and compensating for lapses in manual disinfection.
The trial was a success with great reviews from staff.
Goals
• To improve staff compliance with catheter hub disinfection
• To prevent and/or reduce central line associated blood stream infections (CLABSIs) in our PICC lines.
Methods
The kit was developed to improve compliance with disinfection cap use. Instead of nurses’ having to remember to
bring caps with them on their rounds, they can retrieve the cap from the kit after using the syringe to flush a patient’s
IV during a line access. The final flush serves as a cue to use the cap.
Quality Symposium 2012
Page 219
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
The hospital conducted a two-week trial of the IV flush syringe and disinfection cap system/kit. The trial was
conducted in the critical care, step-down and medical surgical units and was successful. Nurses were pleased with caps
design and ease of use.
The evidence supporting use of the kit and the feedback from the trial was presented to the hospital’s Infection Control
and Product Evaluation committees which approved the product for implementation.
The kit was implemented hospital wide in July 2011. The kit was used on all central lines, including PICCs; all
peripheral IVs (PIVs); and on all tubing components such as y-sites to create a closed IV system. Because it is
constituted a new protocol, the kit was reinforced with staff education and compliance monitoring.
Increase in staff awareness of hospital acquired blood stream infections and infection prevention strategies.
Results
After implementation of the kit, the hospital allowed two months for staff to adjust to the new connector disinfection
protocol and then began recording post-implementation surveillance data. To assess the value of the kit, CLABSI data
on PICC lines from the post-kit implementation period of September 2011 to February 2012 was compared to the preimplementation period of September 2010 - February 2011.
In the six months pre-implementation period, there were 14 CLABSIs suffered by PICC line patients, for a CLABSI
rate of 3.85/1000 central line days. During the six months of the kit use, only four CLABSIs were observed to occur
and the CLABSI rate dropped to 1.14/1000 central line days - a 70.4% decrease in infections.
The ten avoided CLABSIs suggest significant financial savings for the hospital. The CDC assumes an excess
healthcare costs of $29,166 per CLABSI. At that rate, the hospital avoided $291,660 in CLABSI-related costs during
its six-month data collection period. This results is an annual savings of $583,320.
Current data shows two PICC infections since January 2012, which makes our current rate 0.4/1000 central line days.
Conclusions
The choice to implement the disinfection cap and flush kit rather than just the stand a lone cap was effective in
smoothing the transition to the new approach. The system also allowed the nurses easy access to the cap when they
administer their final flush.
Utilizing the cap on all IV connector hubs including peripheral IVs improved patient safety by creating one standard of
care across the hospital. This also helps create a closed system, which has obvious advantages when you’re trying to
close off all avenues for bacteria to enter your lines. We keep caps on the hubs and the tube openings to protect the
entire IV system.
Comprehensive disinfection cap use is associated with lower bloodstream infection rates. Avoided treatment costs are
much greater than cap acquisition costs.
Quality Symposium 2012
Page 220
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Transformational Journey of a Care Delivery Model: Implementation of Evidenced-Based Practice to
Increase Breastfeeding Exclusivity
Eileen Magri, MSN RN NE-BC; Mary Lynn Brassil, MS RN CES; Cathyjo Catalano, MS RN RNC-OB; Mary
Cleary, BSN RN NE-BC; Stephanie Hisgen, MPH RN; Karen Hylton-McGuire, MS RNC NIC IBCLC RLC;
Amy McGuire, MS RN
Winthrop-University Hospital
Introduction
Transforming the Care Delivery Model for mothers and babies began in 2010 with an invitation to participate in the
New York State (NYS) Breastfeeding Quality Improvement in Hospitals Learning Collaborative. Twelve hospitals
were selected to participate with the following objectives: increase exclusive breastfeeding; improve hospital
breastfeeding policies, practices and systems that are consistent with NYS hospital regulations, laws and recommended
best practices; increase staff skills and knowledge of breastfeeding and lactation support through education; empower,
educate and support new mothers to successfully breastfeed and change the culture and social norm relative to
breastfeeding.
Problem
Evidence-based practice supports the benefits of exclusive breastfeeding for mother and child. Barriers exist in
hospitals which inhibit exclusive breastfeeding of newborn infants at the time of discharge and fail to meet the
recommendations outlined by the World Health Organization (WHO) and New York State Department of Health (NYS
DOH). Transforming the Care Delivery Model at a NYS Regional Perinatal Center evaluated all aspects of
mother/baby care to increase breastfeeding exclusivity and meet the recommendations.
Goals
To fully evaluate maternity practices within a NYS Regional Perinatal Center to comply with and support the
recommendations for exclusive breastfeeding outlined by the World Health Organization (WHO) by changing the Care
Delivery Model.
Methods
The changes listed below are in the order in which they occurred. Priority was given to those changes that could be
accomplished quickly and sustained.
1) Establishment of skin-to-skin in Labor and delivery for all deliveries including formula fed infants.
2) Increase time infants spend in mother's room on postpartum by changing "routine collection" time. Infants are
brought back to the nursery upon mother's request.
3) Revision of newborn order sets; breast fed and formula fed order sets separated.
4) Revision of newborn flowsheet to accurately reflect time infant spends in mother's room and 8-12 feedings per day.
5) Nursery RNs are present in L&D to assess, transition and admit newborns, keeping mothers and infants together.
The Model for Improvement utilized Plan-Do-Study-Act cycles to test each change in the work environment and revise
accordingly. Critical to the success of this program was the active participation of the direct care nursing staff
evaluating their practice with each change and providing feedback.
Quality Symposium 2012
Page 221
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Results
June 2010 - May 2012
• Exclusive breastfeeding increased from 6% to 44%
• Rooming-in increased from 0% to 70%
• Skin-to-skin, initial latch and breastfeed increased from 50% to 100% within one (1) hour for vaginal deliveries and
two (2) hours for cesarean births.
• Newborn Transition care is relocated to the Delivery Room and the newborn nursery is utilized for respite care.
Conclusions
The journey to transform the Care Delivery Model supporting exclusive breastfeeding began in June, 2010. The
hospital formed a comprehensive team to evaluate current processes and potential barriers that inhibit exclusive
breastfeeding. Team members were selected based on knowledge of the hospital systems and commitment to change.
Priority was given to changes that could be accomplished quickly and sustained. The initial change focused on placing
all newborns skin-to-skin in the delivery room, successfully latching and breastfeeding within one hour for vaginal
deliveries and two hours for cesarean deliveries. To increase rooming-in on the postpartum unit, newborns were
brought back to the nursery only upon request by the mother. Physician order sets were revised to distinguish orders
for formula fed and breastfed infants to discourage supplementation of breastfed infants. The most dramatic change in
practice implementing the Care Delivery Model involved closing the transitional nursery and providing transition care
in Labor and Delivery by the nursery RNs eliminating the separation of mother and infant.
Skin-to-skin has influenced exclusive breastfeeding by increasing the number of infants that have latched on in the
delivery room. This increases the mother's confidence and also makes it easier for infants to continue to feed at the
breast. Maternity care practice and processes need to be re-evaluated to remove barriers that inhibit successful
breastfeeding. Trying to fit new strategies into old processes will create frustration for the staff. Staff involvement in
"how to" implement the change is key. Their observations can identify barriers and guide the change which in turn,
will support sustainability.
Quality Symposium 2012
Page 222
Quality Symposium 2012
Page 223
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Evaluation of a Computerized Physician Order Entry (CPOE) Alert Program on Prescribing of
Selected Drugs Among the Elderly
Liliana Rios-Rojas, MD; Paula E Lester, MD FACP; Irving H Gomolin, MD
Winthrop-University Hospital
Introduction
The Beer's Criteria for Potentially Inappropriate Medication Use in Older Adults identifies medications that pose risks
outweighing their potential benefits for people 65 and older. This information can help prevent harmful and lifethreatening medication side effects and other "adverse drug events" among older adults.
Problem
Many practitioners may not be fully aware of the potential risks of medications they prescribe in older adults. Previous
studies have demonstrated the impact of Computerized Physician Order Entry (CPOE) in reducing prescribing errors.
This study was conducted to evaluate the impact of CPOE alerts on prescribing patterns on selected high risk
medications from the Beer's Criteria.
We reviewed the Beer's Criteria and selected the following medications for which to create alerts: diphenhydramine,
metoclopramide and all antipsychotics.
• Diphenhydramine is prescribed commonly in hospital setting, as a preventive measure to decrease transfusion
reactions, but studies of its use for the prevention of allergic and febrile non-hemolytic transfusion reactions have been
not shown effectiveness. However, diphenydramine can cause delirium, confusion, urinary retention, and constipation
in the elderly.
• Metoclopramide is prescribed as an anti-emetic. However, it has risks for extrapyramidal side effects and other
adverse effects. Alternative anti-emetics are available.
• Antipsychotics are widely used in geriatric psychiatric disorders, especially for delirium related agitation in the
hospital setting. However, an FDA black box warning cautions about increased risk of death among patients with
dementia-related psychosis.
Goals
A series of alerts for patients 65 and older were built into CPOE for selected medications and included links to relevant
papers including FDA black box warnings and the Beer's Criteria for Potentially Inappropriate Medication Use in
Older Adults. Alerts were created for diphenhydramine, metoclopramide and all antipsychotics. We hoped to reduce
the prescribing frequency of these high risk medications by increasing awareness of their risks.
Methods
Winthrop Hospital is a community teaching institution located in Long Island, NY with residencies, fellowships and a
PA/NP service. All clinicians, including attending physicians are able to enter orders through CPOE, which became
operational by 2009. In January 2011, a series of alerts were built into CPOE for selected medications and include
links to relevant papers.
Quality Symposium 2012
Page 224
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
We evaluated the effect of alerts (for diphenhydramine, metoclopramide and all antipsychotics) on prescribing
frequency by comparing the number of patients for whom these medications were prescribed during second quarters of
2009, 2010 and 2011. Prescribing patterns were evaluated by ascertaining the pharmacy database which contained all
medication orders since the introduction of CPOE. Frequency was adjusted for total admissions among those over 65
years during each quarter of interest. Chi square was used to compare pre- and post-frequency.
Results
Diphenhydramine prescriptions were reduced:
• 38% reduction 2011 vs. 2010, RR=0.63, 95% CI=0.58-0.67, p<0.0001
• 32% reduction 2011 vs. 2009, RR=0.66, 95% CI=0.61-0.71
Reduction in metoclopramide was noted:
• 24% reduction 2011 vs. 2009, RR=0.76, 95% CI=0.69-0.83, p<0.0001
No reduction in antipsychotic prescribing was found.
Conclusions
This study revealed a significant decrease in the number of orders of diphenhydramine and metoclopramide after
implementation of the CPOE "Geriatric Alerts." The impact was greatest for diphenhydramine. This is probably
because it is usually ordered prophylactically for transfusions (which was debunked by the alert) or as a hypnotic
(which the alert advised against, and alternative medications are available).
The lesser impact for metoclopramide is likely related to it being used to treat an active symptom. Additionally, the
alerts for metoclopramide and the antipsychotics caution about long-term use. Our study did not evaluate the number
of days the medications were prescribed.
Antipsychotics in elderly patients may have been continued from home regimens or were ordered because of acute
aggressive, psychotic, or delirious symptoms. As such, prescribing patterns were likely not to be reduced as the drugs
are used for an acute symptom without simpler alternatives to use.
Our study did not evaluate whether the alert increased the discussion or documentation of the FDA black box warning
with caregivers. Our study has some limitations. The analysis is based on number of written prescriptions (both
standing and PRN orders) and not actual doses administered. The study was not designed to include a chart review or
assess clinical outcomes.
Our study found that a CPOE “Geriatric Alert” system for the geriatric patient in the hospitalized setting can be an
effective tool to increase awareness about the dangers of high risk medications and effect drug prescribing patterns.
Future research may show the impact on clinical outcomes and include a chart review of impact of the alerts on
documentation of discussions with patients and caregivers about the FDA warnings.
Quality Symposium 2012
Page 225
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
IHI Project on Safe Patient Handling Technique by Using Pink Slip Patient Transfer System
Elizabeth Baynes RN; Carol L. Cohan RN BSN MHA; Manjula R Stanislaus, RN MSN MHA CCRN CMC RNBC
Winthrop-University Hospital
Introduction
This project is mainly based on IHI model with small steps of rapid PDSA cycle to create the change with in the
organization. Team members are from different departments with various view points, we started working together
with the guidance of Monica Santora, Chief Quality Officer, Department of Patient Safety, Quality and Innovation and
her presentation on quality improvement project. As well as with several productive meeting as per Christine’s
(Director of Professional Nursing Practice and Education Model) for meetings with purpose.
This improvement project focuses on use of safe patient handling technique and policy while transferring,
moving/repositioning any inpatient adult population will help to prevent work related back injuries. Nursing personnel
are consistently listed as one of the top ten occupation for work related injuries, according to recent studies 8.5 per 100
in hospital settings and 13.5 per 100 in nursing home setting are suffering from work related injuries. Especially with
unreporting the incidents, most of incidents are not reported mainly because nurses thinks that it’s not important to
report, secondly lack of time in filling paper work.
Lifting and moving patient from one surface to other demands lot of physical work and strength from nurses.
According to recent literature cumulative weight lifted by a nurse in an 8 hour shift is equivalent to 1.8 tons. Patient are
presented with multiple challenges such as loss of balance cognitive function, unable to follow instructions, different
sizes, body weight are not equally distributed, and combative. Even though these above mentioned challenges are
present in everyday life, nurse keeps involved in positioning and repositioning the patient to prevent bed sores, to make
patient comfortable, and to maintain cleanliness (Nelson, A., Baptiste, A. September 30, 2004).
There is "no lift" national policy was started in United Kingdom in 1992, progressively with multiple evidence based
literature this policy was followed in Australia, Canada, and some of the European countries. No lift policy involves
not using manual handling to move patients unless in an emergency situation to reduce work related injuries. Nurses
transfer their job or go for a different profession because of work related injuries; this is one of the contributing factors
for nursing shortage.
Problem
1. Work-related musculoskeletal back injuries related to lifting patients
2. Non-compliance with use of pink slip patient transfer system in transferring patients from bed to stretcher
3. Unable to use the pink slip patient transfer system correctly
4. Pink slip patient transfer system are not accessible to the transporter
Goals
The aim of this project focuses on increasing compliance on use of pink slip in GP3 while transferring patient laterally
will help to prevent work related back injuries and reduce hospital’s expenditure on work related back injuries to zero.
Quality Symposium 2012
Page 226
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Methods
Safe patient handling project was implemented in one of the telemetry floor to see the change. Even though pink slip inservices were done in the past, when we conducted survey in one of the unit, there was zero compliance. We
interviewed some of the transporters, they mentioned that pink slip breaks whenever they use to transfer patient & the
second reason was time consuming. We were involved in IHI project with our chief Quality Compliance officer,
Monica Santoro. Our project is focusing on safe patient handling with the use of pink slip for lateral transfer. We were
looking to improve compliance, prevent back injuries to staff, as well as to prevent friction associated injuries to
patients in GP3.
Unit chosen to implement pilot project: GP3
Sampling: Randomized sampling technique
Design
• Training to all the employee
• Availability of pink slip to avoid manual handling
• Accessibility of pink slip
• Confidence and ability to use the equipment
Safe patient handling program helps to avoid moving patient with manual lifting, also prevents pressure ulcer due to
friction and assisted falls in the hospital settings. As well as it will save money on work related injuries on the
employee (Nelson, A., Baptiste, A., 2004). We started measuring the compliance and ability to use pink slip with
confidence in April 2012.
Results
In June 1st to 15th 2012:
• Compliance rate in documenting on transport log sheet is only: 8.4%
• Non-Compliance rate of documenting the use of pink slip: 91.4%
June 16th to June 30th 2012:
• Compliance rate in documentation increased to 95%
• Non-Compliance rate of documenting the use of pink slip: 5%
July 1st to July 5th 2012:
• Compliance rate in documentation decreased to: 64.2%
• Non-Compliance rate of documenting the use of pink slip: 35.7%
Conclusions
When we initiated our improvement project we re-in serviced all the transporters to ensure they were using the right
technique. They claimed there was an issue with accessibility. As a result, Pat nurses manager from GP3 spent money
to buy and placed a holder with pink slip in every single patient’s bedside, as well as we placed pink slips in a canister
in the hallway. The third aspect we changed was communication, asking the transporters to approach the primary care
nurse to determine the patient’s ability to move and not approaching patient’s directly. We also changed the transport
log sheet three times as per the need. When we did the in-service most of the transporters admitted, that, “the pink slip
works like a charm”.
Quality Symposium 2012
Page 227
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Nurses were not expected to clean-up patients HIV positive blood without wearing the gloves. Likewise nurses are not
suppose to put themselves and next generation at risk when there is a clear evidence of better practice exit. The change
is not easy, nurses must demand for the safer work environment; this change of practice will have a positive impact on
the nursing profession.
Quality Symposium 2012
Page 228
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Nurse-Driven Strategies for the Reduction of Hospital Acquired Pressure Ulcers in Three
Neuroscience Units
Janice McGuinness, BSN CNRN; Sherry Persaud-Roberts, BSN CNRN; Susan Marra, BSN RN; Jeannine
Ramos, BSN CNRN; Diane Toscano, RN; Linda Policastro, Nursing Assistant; Lee Moldowsky, MSN RN-BC;
Nancy Epstein, MD
Winthrop-University Hospital
Introduction
Winthrop University Hospital’s inpatient neuroscience unit (NSU) consists of a 14-bed intensive care unit, 7-bed neuroobservation unit and an 18-bed general neurology floor. In 2008, the incidence of hospital acquired pressure ulcers
(HAPU) was noted to increase in the NSU negatively affecting mortality, morbidity, and the patient experience. In
response to this increase, a Skin and Wound Assessment Team (SWAT) comprised of existing nursing staff without the
use of overtime was deployed. Their goal was to empower the direct care staff to reduce the incidence of hospital
acquired pressure ulcers (HAPU) through prevention, assessment and early intervention in the neurologically
compromised inpatient population.
Problem
In 2008, 40 HAPUs occurred in the NSU. The reduction of HAPUs was identified as a performance improvement
priority for our institution, not only to limit HAPU-related morbidity and mortality, but also to mitigate or avert the
average $43,000 (Armstrong, et al. 2008) increased cost reportedly associated with these pressure injuries.
Goals
• To reduce HAPUs by 50% in the first year and sustain improvement over time.
• To develop a cost effective plan for a nurse-driven skin and wound assessment team aimed at reducing the incidence
of hospital acquired pressure ulcers in the neuroscience unit.
• Develop a team of expert nurses, responsible for educating other nurses and nursing assistants in the identification
and preventative of pressure ulcers.
Methods
In 2008, the NSU developed a specialized SWAT Team to reduce the incidence of pressure ulcers by targeting risk
assessment and prevention. The team is comprised of both nurses and nursing assistants who are already on staff and
who take on this added responsibility without incurring overtime. They serve as resources, mentors and change agents
for the NSU. The team rounds weekly and collaborates with the bedside nurse to identify patients at risk and
implements appropriate preventative strategies. The SWAT Team trialed skin care products and positioning devices
and brought the most effective product choices into SWAT protocols.
Beginning in 2010, newly hired nursing and ancillary staff spend one shift shadowing the SWAT Team. During this
experience, they receive hands-on training and resources including the Braden Scale, Pressure Ulcer Staging Guide,
and Guide to Skin Care Products and Positioning Devices. Following this hands on experience, they are then required
to complete the NDNQI Pressure Ulcer Training Module. By the end of 2010, the NSU team facilitated the role out of
SWAT to all inpatient nursing units at Winthrop University Hospital.
Results
Quality Symposium 2012
Page 229
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Incidence of HAPUs decreased 52% the first year. The NSU was able to sustain their outcomes over the next 3 years
achieving an overall reduction in incidence of 67.5%. The reduced incidence of HAPUs in the NSU over the 3-year
period represents an estimated cost savings of over 3 million dollars. Two units have maintained a zero NDNQI HAPU
prevalence rate for five consecutive quarters; the third achieved a zero rate for four of five quarters.
Conclusions
In 2010, the SWAT concept was adopted hospital wide and the NSU served as project champions. Best practices are
identified and shared at monthly HAPU reduction and prevention committee meetings. All inpatient units that adopted
these practices were able to replicate the outcomes. Direct care staff experienced a culture change, recognizing the
impact a nurse driven initiative has on patient outcomes by reducing morbidity, mortality and costs. The direct care
nursing staff’s ownership of this initiative is ongoing and we anticipate continued success in sustaining these outcomes.
Quality Symposium 2012
Page 230
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Success in Early Patient Discharge in a Medicine/Surgical Unit Through a Collaborative Approach
Proserfina A Ventura, MSN RN (Potter 3 Nurse Manager); Marilynn Domagala, BSN RN (Potter 3 Assistant
Nurse Manager); Monica Santoro (Vice President & Chief Quality Officer Department of Patient Safety,
Quality and Innovation); JeanMarie Moorehead, MA RN (Director of Nursing-Medicine and Surgery); Linnea
Drew, RPA-C (Associate Director PA/NP Services, Clinical Manager General/Vascular Surgery, Chief
Surgical Physician Assistant)
Winthrop-University Hospital
Introduction
Potter 3 is a Medical/Surgical Unit with 30 patient bed capacities. 75% of the total patient population of Potter 3 are
surgical patients. Potter 3 receives patients from Ambulatory Surgical Unit, Post Anesthesia Care Unit, Surgical
Intensive Care Unit, Medical Intensive Care Unit, Emergency Department, direct patient admits, and transfers from the
different inpatient care units. Potter 3 is divided into four districts with four Registered Nurses (RN) and four Nursing
Assistants during the 7AM to 3PM shift. The four districts are divided into A and B with even room numbers, and C
and D districts with odd room numbers. Surgeons, Medical Residents, and Physician Assistants (PA) regularly start
patient rounds as early as 6 AM.
The average daily patient turnover rate of Potter 3 is 24%, the average daily census is 27, and the average monthly
patient care day is 755. Currently, Winthrop University Hospital utilizes TeleTracking® system for patient flow
monitoring in each unit. Bed board personnel, usually RNs, manage the teleTracking® system. They are responsible
for assigning the patients in each unit. The teleTracking® monitor screen shows each unit with room and bed number
in numeric order. The system enables RNs in each inpatient care unit to monitor assigned incoming patients. Although
the teleTracking® system is a hospital wide system, the individual units do not have access to other unit’s data.
Winthrop University Hospital (WUH) makes use of the Computerized Provider Order Entry (CPOE). Significant
benefits of CPOE include a decrease in delays in order completion, entry of orders from point of care or off site, and a
reduction in errors related to handwriting and manual transcription.
WUH employs Winthrop Express as a centralized patient transport system. Winthrop Express serves up to 450 patients
from 35 distinct areas, which include both inpatient-nursing units, and testing areas. This service includes
transportation for patient discharges.
Problem
Due to the high daily patient turnover rate on Potter 3, unit leadership receives verbal complaints from direct care
nursing staff related to fatigue, workflow disruption, and medication errors. Contributory to the workflow challenge of
Potter 3 is how teleTracking® displays room and bed numbers in a numeric order. Bed board personnel are not
sensitive to the impact of the admissions coming from the different units per Potter 3’s districts. RNs frequent
complaints were delayed patient discharge orders, and incomplete discharge instructions, which is the root of
simultaneous patient discharges and patient admissions.
In addition to this, prior to the start of the initiative in March 2012, Potter 3 had a record of seven medication errors,
Quality Symposium 2012
Page 231
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
2.5 of the medication errors happened during the morning shift. Seven medication errors that occurred were related to
work flow issues. Aside from this, Potter 3’s nurse turnover rate for the first quarter was 5.32%. Two RNs left the unit
for transfer and resignation. Work dissatisfaction related to work flow is the primary reason during exit interview.
Additionally, patients frequently complain of a lengthy discharge process such as delayed patient discharge order, and
frequent long wait time for Winthrop Express transportation.
Goals
• Improve patient traffic flow through a collaborative approach that involves provider buy-in to expedite patient
discharges in AM.
• Increase RN awareness of patient readiness for discharge in the morning.
• Decrease RN interruption during medication pass and treatment regimens.
• Improve Nurse satisfaction.
• Improve Patient satisfaction through early patient discharge.
Methods
The Institute of Healthcare Improvement recommendation to implement the Plan-Do-Study-Act cycle has been
instrumental in resolving Potter 3’s challenges in patient throughput, patient satisfaction, and nurses’ satisfaction. A
survey tool was created by Potter 3 leadership to help identify the peak hours of patient discharges versus peak hours
of patient admissions during Monday to Friday from 7am to 3pm. This initiative excluded the evening shift due to the
availability of the evening shift admission nurse. The initiative also did not include Saturday and Sunday because most
of the elective surgeries are scheduled on weekdays. This data served as a baseline data for our initiative.
One of the features of the CPOE is the pending discharge instruction that a PA can utilize to help lessen workload and
expedite patient discharge. However, even with this feature, some of the PAs did not use this because of personal
preference, lack of understanding of the benefit for using the pending discharge instruction, and lack of understanding
of the positive impact for completing the discharge instruction to expedite patient discharge and help with nurse’s
workflow resolution. Potter 3 leadership collaborated with Monica Santoro, Vice President and Chief Quality Officer
of the Department of Patient Safety, Quality and Innovation; Jeanmarie Moorehead, Director of Nursing Medicine and
Surgery Division; and Linnea Drew, Associate Director PA/NP Services, Clinical Manager General/Vascular Surgery,
and Chief Surgical Physician Assistant. Poor compliance with the use of the pending discharge function was discussed
with Ms. Drew. Nursing collaborated with Ms. Drew in developing an educational and coaching opportunity for the
mid-level providers aimed at increasing their use of the pending discharge process.
The second intervention was monitoring of the unit’s discharge process. At the beginning of each shift, unit leadership
monitors patients for completion of discharge orders in CPOE. Once patient discharge orders are completed and
identified, unit leadership visits the patient to perform an exit interview. Information obtained through the patient
interview was utilized by the direct care nurse to plan and prioritize patient care needs. This process helped to facilitate
a more timely discharge of patients.
The third intervention included the purchase of a unit wheelchair. WUH employs Winthrop express as transport system
of patients throughout the hospital. Unit leadership collaborated with Winthrop Express to identify target opportunities
for improvement on the process of patient discharge. Like any other institution, staffing and the availability of
resources was identified by Winthrop Express Leadership as a barrier to timely facilitate discharge. The unit based
wheelchair is utilized when Winthrop Express cannot provide a timely response.
Quality Symposium 2012
Page 232
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Results
First intervention: Reinforced Pending Discharge Instruction with PAs.
• The reeducation of PAs was started by Linnea Drew. Compliance was monitored for a period of time and Linnea
Drew’s coaching resulted in an increase in compliance to 90%. Improvement in patient readiness for discharge resulted
in early patient discharge and a decrease in the burden on nurses resulting in increased satisfaction with work
environment. After 4 months of implementing changes, there was a 40% reduction in medication errors, a decrease in
the recorded medication errors.
Second intervention: CPOE monitoring of patient discharge orders and patient exit interview.
• This intervention helped nurses plan and prioritize their patient care. In some cases, unit leadership helped to
facilitate patient discharge. It also served as an opportunity for leadership to identify improvement in patient care, and
achieve service recovery. The patients were appreciative of the leadership visit and verbalized that this was a unique
experience that they had not experienced before.
Third intervention: Purchase of unit wheelchair.
• The easy access of wheelchair made it faster for patient discharge when Winthrop Express was unable to
accommodate patient timely. It was also an opportunity for leadership to build a stronger, professional and caring
relationship with their patients before they leave the facility.
1300 hours was identified as the peak hour of patient discharge in Potter 3 and 1400 hours as the peak hour for
admissions. Following the first intervention, 29% of the total patient discharges were discharged before 1300 hours.
After the second intervention, 40% of the total patients for discharge were discharged before 1300 hours. After the
third intervention, a steady rate of 40% was maintained.
Conclusions
There was scant literature found that focused on early patient discharge in the Medical Surgical departments. The
majority of the literature discussed early patient discharge primarily in the Emergency Department and in the Intensive
Care Units. Rarely did the literature speak of early patient discharges in the Medicine and Surgical units such as Potter
3. Although the intention was to improve workflow issues with the nurses and improve patient satisfaction, it was
imperative to disregard the variables identified during the intervention phase of the initiative. Such variables are
unavoidable. These variables include: time availability of family member for patient pick up at the day of discharge;
diet tolerance; the need to complete the last dose of an intravenous antibiotic; waiting for laboratory test result; and
completion of discharge packets for Skilled Nursing Facilities.
WUH recently purchased an upgrade of the TeleTracking® system to TeleTracking XT® with more advance features
that can further help resolve nurse’s workflow challenges.
Activating the pending patient discharge instructions, access of wheelchair, preparing the patient for early discharge,
and nurses and providers buy-in with the goal and purpose of the initiative, all helped alleviate the workflow challenge
of Potter 3. The nurses experienced a more calming atmosphere and a mental preparation for patient admission. Patient
needs were accommodated as safely and as timely as possible.
Quality Symposium 2012
Page 233
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Using the National Surgical Quality Improvement Project (NSQIP) to Decrease Ventilator Days and
Pneumonia in a Surgical ICU
John McNelis, MD FACS; Roseann Grandelli, RN; Maureen Keegan, RN; Eva Chalas, MD FACS; Monica
Santoro, RN CPHQ
Winthrop-University Hospital
Introduction
The NSQIP database is a risk adjusted program developed by the American College of Surgeons to track surgical
outcomes. Since its inception in the VA system, NSQIP has been demonstrated to improve surgical outcomes by
decreasing complications, mortalities and costs. Improvements result from action upon the outcome data provided by
the ACS through rigorous Failure Modes Effect Analysis and where appropriate, the incorporation of best practices. In
many instances, merely being aware that outcomes are being measured leads to improvements through modifications in
behavior.
Problem
Knowledge of NSQIP Surgical Outcomes Data regarding Ventilator Management and Post Operative Pneumonias will
lead to adjustments in practice patterns with subsequent improvement in complications.
Goals
To decrease the number of patients on the Ventilator Greater than 48 hours and post-operative pneumonias in general
surgery patients.
Methods
Winthrop University Hospital entered the NSQIP program in 2010 training two specialized Nurse Reviewers. Each
collected preoperative through 30-day postoperative data on randomly assigned patients. Data acquired included
demographic, peri-operative, hemodynamic and outcome data. Specific Outcome measures in general surgical patients
included mortality, cardiac events, Pneumonia (PNEU), Ventilator > 48 hours (V48), Thrombo-embolic events Renal
Failure, and Surgical Site Infection. Data points were entered into a central database and a comparative, risk adjusted
Semi-annual Report (SAR) was generated. Data is reported as Observed to Expected Odds Ratio (O:E) with 1 being
performance as expected, less than 1 better than expected and greater than 1 worse. Based on the data, interventions
were taken and the impact on the bi-annual SAR was measured. Interventions taken included enforcement of existing
protocols, early mobilization, nutrition, daily assessment of need for sedation and initiation of the weaning process
immediately post-op.
Results
During the Study Interval three SARs were generated: July 2011, January 2012 and July 2012. In July 2011 the O:E
for PNEU was 1.8 (5/368, 1.36%), while V48 was 2.54 (7/368, 1.9%). By January 2012, the O:E for PNEU was 1.48
(13/926, 1.4%) while V48 declined to 1.11 (10/925, 1.08%). July 2012 the O:E for PNEU was 1.25 (13/1081, 1.2%)
(p<.05) and V48 was 1.04 (12/1080, 1.11%) (p<05) (see chart).
Conclusions
In the study interval, progressive improvements in both PNEU and V48 were observed. The authors believe that
process changes implemented in the SICU were responsible for the improvement. The authors believe that simply
Quality Symposium 2012
Page 234
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
ending the routine process of "resting patients overnight" on sedatives made an especial impact. NSQIP data allowed
for tracking and benchmarking of progress. Given an estimated annual Volume of 20,000 cases per year at Winthrop
with an established cost of $22,097 per episode of Pneumonia and $27,654 per each Ventilator day greater than 48
hours, an estimated 130 avoided episodes of Pneumonia and 210 avoided episodes of vent days greater than 48 hrs
could be realized. This results in a projected potential savings of over eight million dollars.
PNEU O:E
V48 O:E
July 2011 SAR
1.80
2.54
Jan 2012 SAR
1.48
1.11
July 2012 SAR
1.25
1.04
Est Savings
$2,872,610
$5,807,310
Quality Symposium 2012
Page 235
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
A Tetralogy...Hemorrhage, Hypertension, DVT, Infection. Implementation of a Perinatal Safety Net
Mary Lynn Brassil, MS RN C-EFM; Margaret Celenza, MS RNC-OB C-EFM
Winthrop-University Hospital
Introduction
Pregnancy and childbirth generally a normal event may become an unexpected obstetrical emergency. The Centers for
Disease Control and Prevention, National Center for Health Statistics (2004) report the rate of perinatal mortality in the
U.S. has increased since 2002. Maternal mortality and permanent severe morbidity in New York State is on the rise
(NYS DOH, 2010).
Maternal hemorrhage is the most common cause of maternal mortality in NY. Thromboembolic events increase during
pregnancy & postpartum due to an altered coagulation state. Pulmonary embolism remains a leading cause of death
after hemorrhage in NY State. Hypertensive disorders/emergencies, the most common medical complication of
pregnancy affects 5-10% of all pregnant women and is the 2nd leading cause of maternal death in the United States
(McCoy & Baldwin, 2009). Advanced maternal age, obesity, cesarean delivery and significant chronic disease also
contribute to febrile morbidity and postpartum infection.
Incomplete assessments, breakdown in communication, inadequate therapies and follow up are contributing factors to
failure to rescue and deliver suboptimal patient care. The Joint Commission issued a Sentinel Event Alert in January
2012, Preventing Maternal Deaths, is directly linked with National Patient Safety Goal #16; to recognize and respond
to changes in patient condition. The Institute for Healthcare Improvement's (IHI) "100,000 Lives Campaign" continues
to stress the significance and value of communication and the implementation of rapid response teams.
Adverse events are often preceded by one or more warning signs. The inability to recognize the signs and symptoms
reflective of early deterioration in a patient's clinical condition is considered Failure to Rescue.
A perinatal safety initiative utilized a Team STEPPS approach to establish a process to identify obstetrical patients at
risk for hemorrhage, hypertension, thromboembolic events, and infection, along with an evidence-based plan of care
and implementation of an emergency response team.
Problem
Develop strategies to prevent and minimize the effects of hypertension, hemorrhage, thromboembolic events, and
infection to the obstetrical patient in order to formulate an evidence-based plan of care.
Goals
1. Initiate a "Realistic" screening process to identify obstetrical patients at risk for hemorrhage, hypertension,
thromboembolic events, and infection, after delivery.
2. Enhance nursing and medical staff education regarding evidence based standards of care.
3. Establish specific triggers for earlier recognition of at risk patients by responding to changes in maternal vital signs
and condition, and activation of emergency response teams.
4. Identify the process established to assist the nurse and physicians recognize and respond to early deviations in the
Quality Symposium 2012
Page 236
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
plan of care.
5. Conduct multidisciplinary obstetrical emergency drills on the mother baby unit and in Labor & Delivery
Methods
A Team STEPPS approach established a process to identify obstetrical patients at risk for hemorrhage, hypertension,
thromboembolic events, and infection, the tetralogy. Obstetrical emergency drills emphasizing team goals, knowledge,
mutual support, situation monitoring and, SBAR communication were conducted in labor & delivery and the mother
baby units using video play back to assist with debriefing.
A shared mental model is the foundation of this safety initiative to assist the nurse and physician recognize and respond
to early deviations in the plan of care. The medical RRT quickly identified it was imperative to collaborate with
obstetrical nurses and physicians to safely recognize and address the physiological needs of pregnant/postpartum
women.
Results
Obstetrical patients are screened using specific criteria for the four risk factors after delivery. The plan of care,
medications, treatments and referrals are driven by pre printed postpartum physician orders. Identifying a patient at risk
for one or more factors assists the provider and nursing staff implement and individualized plan of care that includes
more frequent assessment. The plan of care, medications, treatments and referrals are driven by physician orders.
Education provided to physicians, residents and nursing staff included evidence-based standards of care, the specific
triggers for responding to changes in maternal vital signs and condition, and activation of emergency response teams.
Emergency supplies, and obstetrical emergency medication available for immediate use in L&D and mother baby units
are treated the same way as materials and medications in the crash cart. Hemorrhage standing orders and Hypertensive
Emergency standing orders for Labetalol and hydralazine administration have been developed based upon current
ACOG guidelines. Simulated obstetrical emergency drills identified the need for the development of an obstetrical
crisis assessment record similar to Cardiac Arrest/Code Record to assist the nurse scribe document real time during the
emergency.
The medical Rapid Response Team (RRT) recognized it was imperative to collaborate with obstetrical nurses and
physicians to safely recognize and address the physiological needs of pregnant/postpartum women. The Code H Team
(Hemorrhage) and Obstetrical Crisis Team (OCT) were established. The medical RRT is activated simultaneously with
either the OCT or Code H team via one phone call to the emergency operator who notifies team members via an alpha
numeric pager. The Code H Team comprises the In-house Obstetrical attending physician, L&D Charge Nurse, OB
Chief Resident, OB Anesthesia, the blood bank, and main OR.
The OCT consisting of the OB attending in house physician, OB chief resident and the L&D charge nurse respond to
obstetrical emergencies, i.e. hypertensive emergency, seizures, cardiac compromise, change in patient status or when
the nurse feels something is not right on any unit in the hospital. Activating the OCT and RRT simultaneously is a
ramp up, ramp down emergency response approach with full medical and obstetric capabilities. Activating the Medical
RRT along with the OCT facilitates a smoother transition outside of the obstetrical area. It provides a Safety Net,
increases effectiveness, fosters team adaptability and begins intensive care unit level of care at the bedside When
changing needs of the patient are quickly identified, a plan of care formulated and implemented, and consults are made
this often enables the mother baby couplet to remain together on the mother baby unit. Obstetrical patients who require
a higher level of care are transferred to the intensive care.
Quality Symposium 2012
Page 237
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
In order to provide safe and comprehensive care to the obstetrical patient a thorough understanding of the physiologic
adaptations of pregnancy and postpartum is essential. It was identified by nurses and physicians working in the
intensive care areas and Emergency Department they were uncomfortable and not familiar with specific standards of
care for pre-eclampsia/ eclampsia and magnesium sulfate administration. An aggressive education plan was put into
motion highlighting the physiological changes that occur in pregnancy and postpartum, evidence based plans of care
and the value of co-managing the patient with the obstetrician.
Conclusions
• Strategies developed to prevent & minimize the effects of hypertension, hemorrhage, DVT, and infection to the
obstetrical patient.
• A process established to identify patients at risk for hypertension, hemorrhage, DVT, and infection, and make
necessary referrals for nutrition, and Home Care.
• Evidence based Standards of Care developed.
• Obstetrical emergency response teams developed.
• Unit based education and on-line education provided in the Obstetrical and Emergency Department.
• Doctors orders developed
o NSVD/C-section: the tetralogy
o Emergent Therapy for Acute-Onset Severe Hypertension with Preeclampsia or Eclampsia
o Obstetrical Hemorrhage
o DVT Risk assessment and reassessment post delivery, includes anti coagulation prophylaxis recommendations
• Multidisciplinary emergency drills with obstetrical staff and the Emergency Department physicians and nurses.
• Emergency flow records developed
• Obstetric hemorrhage and hypertensive crisis debriefing tool developed
• DVT pre and post delivery risk assessment tool developed
A Team STEPPS approach established a realistic process to identify obstetrical patients at risk for hemorrhage,
hypertension, thromboembolic events, and infection, the tetralogy after delivery. An evidence-based plan of care, a
method to facilitate communication and escalation of patient care needs and development of obstetrical emergency
response teams, emerged as a multidisciplinary obstetrical improvement team perinatal safety initiative. The core
principles behind this improvement project was to have the bedside caregivers recognize early and respond to
deviations in the plan of care, potential problems or dangerous situations/circumstances to improve patient outcomes,
improve patient satisfaction, improve staff satisfaction. The implementation of this perinatal safety initiative has
fostered team work creating an Obstetrical Safety Net.
Quality Symposium 2012
Page 238
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Healthcare in the 21st Century: Bridging the Gap between Medical Education and Quality of Patient
Care
Ulka Kothari, MB BS; Joseph Greensher, MD; Jill Leavens-Maurer, MD; M L Quintos-Alagheband, MD
Winthrop-University Hospital and Children's Medical Center
Introduction
Healthcare in the 21st century is ushered by a growing appreciation that a gap currently exists between the quality of
care our patients receive and what they should receive. A parallel gap exists in resident education on Patient Safety and
Medical Errors (PSME). The Committee on Quality of Health Care in America has challenged professional societies to
develop and implement curriculums on Patient Safety and adopt them into training and certification requirements. To
bridge this gap we designed a model to implement the ACGME mandated curriculum.
Problem
The landmark Institute of Medicine publication in 1999 drew attention towards the urgent need to address patient
safety and medical errors. According to the report medical errors were the 8th leading cause of hospital associated
mortality. Residents are the frontline staff and are often not aware of the challenges of the complex interactions and
systems based practice in healthcare. Many of these residents have not received any formal training on preventing
medical errors and are not well equipped to deal with errors once they occur.
Goals
Our goal was to implement a multifaceted curriculum that would improve residents knowledge of patient safety and
medical errors, affect a positive change in their attitudes when dealing with errors and increase their preparedness to be
proactive in safeguarding the safety of their patient.
Quality Outcome Measures: Improvement in Knowledge, Attitudes and Preparedness regarding PSME of current
Pediatrics Residents at Winthrop University Hospital (WUH), before and after implementation of the ACGME
mandated curriculum on patient safety.
Methods
Setting: Pediatric Intensive Care Unit and Pediatric Inpatient Units at Winthrop University Hospital.
Participants: Pediatric Residents (PGY1 to PGY3)
We designed a hybrid model of curriculum implementation (Didactic and Experiential) based on a model adopted at
University Hospitals at Cleveland and modified for our local needs.
Part I: Pre-intervention survey -- Residents completed an anonymous self-assessment survey (blinded to investigators)
assessing 3 major domains regarding PSME:
1) Knowledge- of epidemiology, identification and classification, root causes and reporting of adverse events.
Knowledge was tested through multiple choice questions.
2) Attitudes regarding reporting and likeliness to intervene was tested with the help of Likert Scale.
3) Preparedness - The barriers perceived by residents to acknowledge and report medical errors and their personal
assessment of readiness to deal with PSME. These were tested through open-ended questions.
Quality Symposium 2012
Page 239
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Part II: Intervention (implementation of curriculum) comprised of 2 components:
i) Didactic: Conferences were conducted to introduce the concept of medical errors and their impact on health care. A
major focus of these sessions was to highlight complex interactions between systems in health care and the
vulnerabilities that permit errors to occur. It also introduced the concept of a "just culture".
ii) Experiential: Each resident was required to identify a case of medical error in which they were involved, analyze it
for the type of error that occurred using the Leap’s classification of Medical Errors and the system(s) failure associated
with the event. After identifying the gap between "best care" and what occurred in the patient, the resident was asked to
reflect on a corrective course of action including systems changes that could be implemented to prevent occurrence in
the future. Faculty mentors with experience in patient safety were chosen to provide feedback on whether the proposed
actions were appropriate and actionable. Every quarter of the year the chief residents identified a case of near miss or
adverse events and held workshops where the case was discussed with the help of Vanderbilt’s Matrix.
Part III: Post-intervention survey and post-test: At the end of their Inpatient and PICU rotations (during which period
the curriculum was implemented), residents’ completed a self-assessment survey and post-test (identical to preintervention survey) to determine if the intervention improved residents’ knowledge, attitudes and preparedness
regarding PSME.
Results
We have observed a significant improvement in resident's knowledge regarding PSME (see Table I). In the attitudes
domain although there was some improvement from baseline the change was not statistically significant (see Table II).
Many barriers were identified pre intervention with litigation and fear of attending being the most cited barrier. There
were less barriers reported post intervention. Direct observations demonstrate that residents are now more forthcoming
in acknowledging not only incident cases of medical errors but also cases involving near misses. They are now more
likely to escalate such incidents or near misses.
Conclusions
The implementation of a comprehensive Patient Safety Curriculum does increase resident’s knowledge and awareness
of the complexity of our healthcare environment and its fallibility. Although a change in attitude is not readily
measurable, we acknowledge that behavior change takes time. The transference of knowledge to bedside practice
demands consistency and time. Litigation and fear of seniors still continue to be a significant barrier reflecting the
overwhelming need for a cultural change in order to address the issue of PSME.
The implementation of this curriculum has been well-received by the pediatric housestaff and have served as an
opportunity for open reporting and discussions of their concerns regarding the safety of patients. Our faculty mentors
also filter the information for integration to our quality improvement initiatives in pediatrics.
Hospitals are complex service organizations and medical residents are front-line medical professionals involved in
patient care. Training in Patient Safety and Medical Errors (PSME) is now part of ACGME mandated curriculum.
However, implementation of this curriculum is challenging with no definite published guidelines. In our study we have
convincingly demonstrated an improvement in knowledge and the attitudes regarding PSME among Pediatric residents
at WUH. We designed a hybrid delivery model comprising of experiential case-based learning and didactic series of
lectures and workshops - to increase residents' understanding of system-based and practitioner based medical errors. It
was emphasized that though medical errors are sometimes practitioner-centered they are more often systems-based.
Quality Symposium 2012
Page 240
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Our goal is to enhance residents’ understanding of the complexity of our healthcare environment in which errors occur
and to establish a "just culture" in which residents feel comfortable addressing and escalating potential medical errors,
near misses or adverse events.
Quality Symposium 2012
Page 251
Healthcare in the 21st Century: Bridging the Gap between Medical Education
and Quality of Patient Care
Ulka Kothari, MD and ML Quintos-Alagheband MD
Table 1. Number of correct responses Knowledge Pre‐intervention Post‐intervention Odds Ratio P‐value PGY1 (N=11) 33 54 4.5 (2.195‐9.2240 <0.0002 PGY2 (N=13) 39 53 2.944 (1.558‐
5.564) 0.001 PGY3 (N=11) 33 50 3.33 (1.676‐6.63) 0.0008 Table 2. Changes in Attitudes – measured on a Likert scale Pre‐intervention Post‐intervention P‐value 91.5 93.5 0.287 Disclosure to parents 85 85 1.000 Likeliness to intervene 80 87 0.12 Reporting References
•
Kohn KT, Corrigan JM, Donaldson MS. To Err Is Human: Building a Safer Health
System. Washington, DC: National Academy Press; 1999
•
National Research Council. Crossing the Quality Chasm: A New Health System for the 21st
Century. Washington, DC: The National Academies Press, 2001.
•
Accreditation Council for Graduate Medical Education. 2001. Outcome project timeline—
Working guidelines.
•
Leape L et al. Preventing medical injury. QRB Qual Rev Bull.1993;19:144-149.
•
Quinn, Doris C., Paul Q. Reynolds, Jane Easdown, and Amanda Lorinc. "Using the Healthcare
Matrix with Interns and Medical Students as a Tool to Effect Change." Southern Medical Journal
102.8 (2009): 816-22.
Quality Symposium 2012
Page 242
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Poster
Presentation
Patient-Centered Care of the Pregnant Patient with Diabetes Who Uses an Insulin Pump During
Labor and Delivery
Mary Lynn Brassil, MS RN C-EFM; Margaret Celenza, MS RNC-OB C-EFM; Virginia Peragallo-Dittko, RN
BC-ADM CDE (Executive Director of the Diabetes & Obesity Institute); Jane Wendel, RN BS CDE; Linda
Zintl, RN BSN (Inpatient Diabetes Nurse Clinicians)
Winthrop-University Hospital, Department of Obstetrics and Gynecology
Introduction
A review of the literature revealed the following:
• For women with type I diabetes continuous subcutaneous insulin infusion (CSII) pump therapy is associated with
better quality of life and in some studies better glucose control than the standard multiple dose insulin injections.
• Better glucose management in pregnancy has been shown to reduce perinatal morbidity and mortality. At the time of
delivery, it is important to avoid maternal hyperglycemia and reduce newborn hypoglycemia and avoid separation of
mother and neonate for resulting interventions. In a review of outcomes of women with Type 1 diabetes, improved
A1C and decreased cesarean section rates were demonstrated in the women using CSII pump therapy versus multiple
dose insulin injections.
Problem
1. A person with diabetes who uses an insulin pump for blood glucose management considers the insulin pump as a
lifeline. Disconnecting from the insulin pump raises concern and triggers unnecessary anxiety. Winthrop University
Hospital is committed to encouraging use of insulin pumps in hospitalized patients unless the patient who is the pump
operator is unable to safely operate the pump because of sedation, pain or debilitating illness.
2. Insulin pump users may demonstrate different levels of skill as there is no uniform education process. Some patients
demonstrate advanced pump skills while others have had limited introductory pump training with no follow-up. At
Winthrop, a patient’s ability to use an insulin pump is determined by the person’s ability to use the pump to locate
basal and bolus rates and discuss his/her pump management decisions. Because the patient will be operating the insulin
while hospitalized, the patient must demonstrate basic pumping skills or it will not be safe to use the insulin pump
while hospitalized.
3. The abrupt changes in glucose metabolism and the dynamic nature of the labor and delivery process posed myriad
challenges to developing insulin pump procedures.
• Maternal insulin needs drop precipitously after delivery.
• Avoiding intrapartum maternal hyperglycemia may prevent fetal hyperglycemia and reduce the likelihood of
subsequent neonatal hypoglycemia.
• Sufficient glucose needs to be infused during labor to provide for increased energy needs and to prevent starvation
ketosis.
• Labor can begin at any hour, planned vaginal deliveries can become emergency cesarean sections, and multiple
health care professionals will be involved in the care of these patients.
4. Because patients using insulin pumps are admitted intermittently, it is challenging for staff to remember the forms
and processes involved.
Quality Symposium 2012
Page 243
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
Prior to the Obstetrics Insulin Pump Pilot, no guidelines existed for providing inpatient care to our pregnant patients
with Type 1 diabetes using insulin pumps. Managing insulin requirements during pregnancy and immediately
postpartum can be difficult and requires close follow up. Most patients were told to discontinue their pumps on
admission. Sometimes an attending physician would write an order to allow a patient to continue using the pump which
was problematic because no supervision of insulin delivery or assessment of the patient’s ability to manage the pump
was taking place by the nursing staff or resident physicians. The obstetricians were not familiar with the intricacies of
dosing and need for quick, abrupt changes in post partum dosing. Frequently the patient’s endocrinologist did not have
privileges at the hospital. There was no established way to document the variety of insulin doses that were given via
the pump on the MAR. The nurse simply documented receiving insulin via pump.
Goals
Partnering with Virginia Peragallo-Dittko, RN, BC-ADM, CDE, Executive Director of the Diabetes and Obesity
Institute, a decision was made to develop a pilot program in an effort to develop the tools unique to the obstetrical
setting, provide concurrent monitoring and document quality improvement. The documentation forms that were
developed as part of the Pediatric Insulin Pump Pilot project were used for the Obstetric Insulin Pump Pilot as well.
The most important component of this patient-centric journey was the use of an Insulin Pump Agreement. This
agreement between patient and Nurse outlines basic elements such as the patient’s need to provide her own pump
supplies while hospitalized to the most important element of partnering with the nurse to communicate all pump setting
and bolus/correction doses. Because patients who use an insulin pump make daily insulin dose adjustments
independently, it was critical to empower both the insulin pump-using patient and Nurse to form a partnership
concerning insulin dosing while the patient was hospitalized. The agreement addressed the following key points:
• Showing the nurse bolus and basal rates and changes
• Frequency of infusion set and infusion site changes
• Reporting symptoms of hypoglycemia and pump problems
• Situations when the pump may need to be discontinued
• Disconnecting the pump’s sensor and using the hospital’s blood glucose meter (may use own lancet)
Methods
Our first step was the development of standardized admission orders related to insulin pump therapy management in
the intrapartum and immediate postpartum periods. Order sets were developed for the patient admitted in labor, for
induction of labor and cesarean section. They were accepted by the OB Improvement Committee and all forms were
approved by the Documentation/Medical Records Committees.
The order sets addressed the following:
• Order to leave the pump in place or when to appropriately disconnect the pump
• Type of insulin used by the patient
• Current basal rates and bolus amounts
• Target blood glucose ranges
• Frequency of blood glucose monitoring and checking for urine ketones
• Directions for alternative source of insulin if the pump is discontinued for any reason
• Nutrition prescription diet orders and carbohydrate allotment
• Hypoglycemia management
• Endocrine consult for postpartum insulin pump dosing
Quality Symposium 2012
Page 244
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
We adopted the specialized Medication Administration Record (MAR) utilized by the pediatric pilot program which
allowed for documentation of the basal rates and prandial and correction boluses.
Educational sessions were scheduled for all nurses, mid level providers and resident physician staff with Jane Wendel,
RN, BS, CDE and Linda Zintl, RN, BSN, CDE, Inpatient Diabetes Nurse Clinicians. The sessions addressed rationale
for and technical aspects of CSII pump therapy, intrapartum and postpartum guidelines for insulin pump therapy,
carbohydrate counting, Patient Insulin Pump Therapy Agreement, and specialized MAR’s for documentation of insulin
delivery via insulin pump. It was very important to communicate not only the clinical aspects of peripartum insulin
pump management but the patient’s emotional connection to the pump as well so a woman with diabetes who uses an
insulin pump participated in every session. This unique element underscored the patient-centric message. The
Executive Director of Winthrop’s Diabetes and Obesity Institute provided education about insulin pump therapy and
the pilot program to physician staff and private attending physicians at the Obstetric departmental meeting.
Certain hospital-wide processes have supported the Obstetric Insulin Pump Pilot as well. The Inpatient Nurse
Clinicians are notified when a patient using an insulin pump is admitted to the hospital so they can assist both nurses
and providers with process issues such as orders, documentation and preparing for radiologic procedures. The outcome
has been the formation of a collaborative team partnering to provide care that is safe, effective and patient centered.
All inpatients using insulins pumps have an endocrine consult. The Endocrinologist assesses the patient's ability to
manage self care during hospitalization, and determines the postpartum insulin dosages to be programmed in the pump.
These patients are reevaluated daily by endocrinologists and adjustments to their insulin regimens ordered when
necessary.
Results
Information regarding the insulin pump therapy program was disseminated to the obstetrician staff offices through the
hospital’s physician liaison. Patients are offered the opportunity to meet with the Inpatient Diabetes Nurse Clinician,
Jane Wendel, RN, BS, CDE, prior to delivery in order to review key points and expectations regarding the use of their
insulin pumps when hospitalized.
Shortly after the information regarding the pump program was disseminated, Jane Wendel RN, BS, CDE was notified
by an obstetrician of patient with type 1 diabetes who uses an insulin pump and due to deliver her baby at Winthrop in
a couple of months. He said that the patient wanted to be able to continue to wear her insulin pump during her
hospitalization and that she was very anxious about delivery and her diabetes management. Jane set up a meeting with
the patient to review Winthrop’s labor and delivery insulin pump protocol and address her concerns. The patient saw
the Insulin Pump Therapy Patient Agreement form that she would be asked to sign upon admission, learned why her
pump needed to be re-programmed for her immediate post partum needs and had an opportunity to ask many questions.
She described lower levels of anxiety following the meeting as she knew what to expect and felt supported.
The patient’s cesarean section was scheduled for February 2012. She and her husband reported that they were very
happy with their experience at Winthrop throughout their labor and delivery and post partum stay. The patient was
extremely pleased that she was able to keep her insulin pump and had much praise for the Obstetric staff at Winthrop.
The Obstetric Insulin Pump Pilot was launched with the expectation of enrolling ten patients, evaluating the process
Quality Symposium 2012
Page 245
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
and monitoring documentation.
We have just reached our goal of ten patients and the pilot has been successful. Our tenth patient is a Labor and
Delivery Nurse with Class B diabetes who uses an insulin pump when pregnant but typically manages her blood
glucose with healthy eating and exercise. She had a vaginal delivery two years ago at another hospital and she reported
that her insulin pump doses were not monitored by the nursing or medical staff during her hospital stay and she
experienced a severe hypoglycemic event with loss of consciousness postpartum. The reason she chose to come to
Winthrop was because of Winthrop’s Insulin Pump Program. She was admitted to our Labor and Delivery Unit for
induction of labor at 38 weeks for preeclampsia. She was made aware of and agreed with the terms of the Insulin Pump
Patient Agreement. The nurses transcribed the basal, prandial and correction insulin doses onto the specialized MAR,
and these doses were rechecked every change of shift and patient handoff.
Her glucose levels were checked regularly and remained stable during her entire labor. The standardized order sets for
Intrapartum and Postpartum Care of the Patient Using an Insulin Pump were followed. The nurse who was with her for
most of her labor and delivery, Pat Patterson RN, is one of our unit representatives in the Diabetes Champion Program.
This program is offered by the Diabetes Inpatient Nurse Clinicians to educate staff nurses in various aspects of diabetes
care and inform them of Diabetes Quality Improvement Initiatives being launched hospital wide. Pat stated that this
involvement helped her to feel confident in providing and planning nursing care for this patient. This patient was also
very determined to breastfeed her baby, and was knowledgeable of the benefits of lactation for both her and the baby.
Our NICU policy is that babies of mothers with Class B diabetes or greater must be transferred to NICU within the first
15 minutes in order to assess and treat neonatal hypoglycemia. Pat’s assessment of the patient’s medical history and
antepartum blood glucose management indicated that the patient’s newborn was at low risk for neonatal hypoglycemia.
Pat discussed this with the obstetrician who spoke with the patient and then with the attending neonatologist covering
NICU. The decision was made to let the baby stay with mom and breastfeed, with close monitoring. The mom had a
vaginal delivery with no complications. The neonate, weighing 5lbs 13oz, was able to stay with the patient skin to skin
and breastfeed. All the blood glucose readings were within range were normal and the baby was breastfeeding well
with a normal transition. I visited the mom her 2nd day postpartum. She was to be discharged home that afternoon. I
explained my role in the development of the Obstetric Insulin Pump Therapy Program and asked if she could provide
us with any feedback. She smiled and said, very enthusiastically "I am so glad I chose Winthrop." She asked for the
names of all the nurses involved in her care and promised that she would provide us with some feedback.
Our hospital is currently working toward Joint Commission Disease Specific Care Certification for Advanced Inpatient
Diabetes Care. A hospital-wide, standardized, nurse-initiated hypoglycemia protocol, standardized insulin dosing, the
Diabetes Champion Program for RN’s and Nursing Assistants, Inpatient Diabetes Nurse Clinicians to assist and
educate staff, and the Obstetric and Pediatric insulin pump therapy programs are just a few examples of initiatives that
have been instituted to provide safer, evidence based and patient-centered care for our patients with diabetes. It is this
strengthened foundation that supported us through the development of this new program for our obstetrical patients
utilizing insulin pump therapy.
Conclusions
All the charts of our CSII pump therapy patients were reviewed these essential data. Review of chart data:
• 100% of the patients had signed a patient agreement upon arrival to the hospital.
• 100% had written doctors orders antepartum and postpartum with appropriate insulin dosing changes after delivery
• 100% of the patients received endocrine consults and nutrition consults with registered dietitian
Quality Symposium 2012
Page 246
NewYork-Presbyterian Healthcare System Quality Symposium 2012
Innovative Differentiation: Distinguishing Yourself from Other High Performers
• 100% of the patients were able to stay on the pump during their hospital stay
Nursing documentation:
• 100% plan of care included insulin pump therapy
• 100% had completed Insulin bolus MAR and basal rate MAR completed
• 30% had documented disposition of pump on Personal Property Record
• 0% had documentation of assessment of insertion site or documentation of site change
The results of the Obstetric Insulin Pump Pilot will be presented to the OB Improvement Committee. Because of the
pilot, we are evaluating the possibility of the patient using her own blood glucose meter and the feasibility of keeping
the pump connected during cesarean delivery.
Pregnant patients using insulin pump therapy are a low volume, high risk population that can present a challenge for
staff. The support of the experts, the Inpatient Nurse Clinicians and our endocrine physicians have eased this challenge
and supported our staff to effectively care for these patients.
Quality Symposium 2012
Page 247


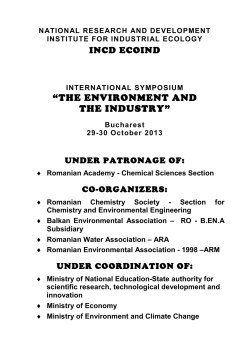

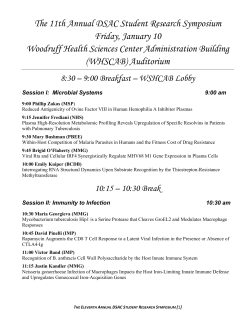

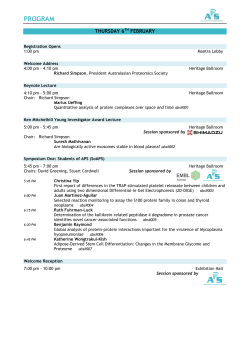

© Copyright 2026