
Reduce Allograft Risk with Intraoperative Flow Measurements
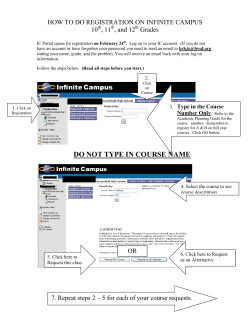
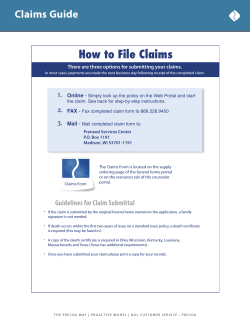
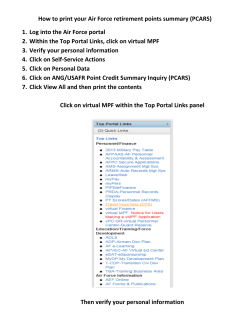
Research Transplant Surgery Reduce Allograft Risk with Intraoperative Flow Measurements • Identify Impaired Blood Flow before Closure • Assess Flow Quickly and Quantitatively • Document Restored Flow Research Transplant Surgery Intraoperative Measurements Inform during Transplantation Surgery Lifesaving transplant surgeries challenge a transplant surgical team to perform at their highest level. During these high stake surgeries, intraoperative blood flow measurements provide quick, quantitative assessments of blood flow that may either confirm a clinical impression or alert the team to potential problems while they still can be more easily addressed. Orthotopic liver transplantation, in particular, presents a unique opportunity for intraoperative flow measurements. Measurements are incorporated into the protocol for the multicenter Adult-to-Adult Living Donor Liver Transplantation (A2ALL) study. Since simple visualization of a pinkto-red reperfused liver doesn’t ensure that both the hepatic artery and portal vein are each functioning, simultaneous hepatic/ portal measurements provide an essential quality assurance. In addition to checking the quality of anastomoses in liver, renal, pancreatic, lung and heart transplant surgeries, intraoperative measurements also identify potential kinking of conduits, particularly veins, and are useful in identifying donor-to-recipient mismatches. No other flow technology produces flow data as quickly, accurately and non-intrusively during transplant surgery as Transonic® intraoperative flow measurements. ”We used Flowprobes to evaluate flows in the hepatic artery and portal vein in the setting of living donor liver transplantation. This formal process allowed us the evaluate the impact of flows on eventual graft function and correlate with risk factors for graft failure.” Emond, J, MD, Chief of Transplantation, Columbia Presbyterian Medical Center, Co-chair, A2ALL Study. “The routine use of intraoperative flow measurements of the hepatic artery may be a useful adjunct in identifying the hepatic artery reconstruction, which is at risk of subsequent hepatic arterial thrombosis (HAT).” Lin M et al, “Hepatic Artery Thrombosis and Intraoperative Hepatic Artery Flow Rates in Adult Orthotopic Liver Transplantation, ANZ J Surg 2002; 72: 798-800. “Impaired hepatic arterial blood flow after reperfusion along with primary non-functioning organ (PNF) are significant predictors of increased graft injury and is associated with diminished long-term graft survival. ...Intraoperative transit time ultrasound flow measurements of the hepatic artery may allow identification of organ transplants at risk for poor outcomes. ...Hepatic arterial flow < 100 ml/min presents a significant risk on organ survival.” Pratschke S et al, “Arterial Blood Flow Predicts Graft Survival in Liver Transplant Patients,” Liver Transplantation 2011; 17: 436-445. TRANSIT-TIME ULTRASOUND TECHNOLOGY MEASURES VOLUME FLOW, NOT VELOCITY Two transducers pass ultrasonic signals, alternately intersecting the vessel in upstream and downstream directions. The difference between the two transit times yields a measure of volume flow. Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] TransplantCover(TX-500-fly) Rev. A 4-13 Transplant Surgery Flowprobes for Transplant Surgery Transonic® Flowprobes work with HT300-Series-FT Flowmeters to measure volume flow in blood vessels and grafts from 0.5 to 36.0 mm. The measurement of flow in vessels during transplant procedures can guide surgical decisions. The ability to correct otherwise undetectable flow restrictions provides the surgeon with an opportunity to improve the outcome for the patient. Probe body Flexible neck Handle Reflector Fig. 1: 4 and 6 mm Vascular Flowprobes recommended for measuring hepatic arterial flow. Picture shows Flowprobe handle with size of Probe in mm, the Probe’s flexible neck for optimal positioning of the Probe around the vessel, the Probe body that houses the ultrasonic transducers, and the Probe reflector. Vessel is positioned within the Probe sensing window that is defined by the Probe body and its stationary reflector. Fig. 2: 8 mm, 10 mm, 12 mm and 14 mm Vascular Flowprobes recommended for measuring portal venous flow. FLOWPROBES: TRANSPLANT SURGERY LIVER Probe Size (mm) Probe Series hepatic artery 4, 6 FMV portal vein 10, 12, 14 FMV, -AU ascending aorta 4, 6 FMV, -FSB pulmonary artery 10 FMV, -FSB 8 FMV, -FSB KIDNEY PANCREAS common iliac artery TXFlowmetersFlowprobes (TX-501-ds)RevA 6-13 Flowmeters for Transplant Surgery Transonic’s new Optima Flow-QC® Flowmeter takes transit-time ultrasound flow measurement resolution to the highest level. The Optima’s unprecedented resolution accompanies lower offsets, and doubles the accuracy for low flows. The Optima Flowmeter enables use of the entire line of resterilizable Flowprobes for liver, renal, heart, lung and pancreas transplants. Flowprobe sizes range from 0.7 mm to 36 mm. The flexible neck of handle Flowprobes permits optimal Probe positioning for measurement ease. • Provides unsurpassed accuracy • Ensures vessel patency • Immediate, quantitative flow measurements HT354 Single-channel Optima Flowmeter for measuring flow of one vessel during transplantation procedures. The AureFlo® is a versatile system used to continuously measure, display, and record absolute volume flow and other derived parameters. Shown here with the new HT364 dual-channel Optima Flowmeter, it can be used with Transonic’s extensive line of Flowprobes for every application. HT364 Dual-channel Optima Flowmeter permits simultaneous measurements with two Flowprobes, particularly useful for measuring hepatic arterial and portal venous flows during liver transplantation. www.transonic.com Liver Transplant Medical Note Intraoperative Blood Flow Measurement during Adult Orthotopic Liver Transplantation Courtesy of J. Michael Henderson, M.D., F.A.C.S. Introduction Abnormal hepatic hemodynamics and physiology in the transplanted liver pose continuing challenges for the surgeon. A practical method for measuring two of these hemodynamic parameters, portal venous and hepatic arterial flows, is by intraoperative flow measurements. Transit-time ultrasound technology is well suited to measure these flows. Flowprobes are easily applied and do not have to be applied tightly to vessels; they simply encompass the vessel. Surgical Approach Measurement of portal venous and hepatic arterial flows can be easily done at the completion of orthotopic liver transplantation using Transonic Flowprobes. Following completion of the vascular anastomoses, the new liver is reperfused, and hemostasis achieved. Prior to biliary reconstruction, the Flowprobes are placed on the reconstructed portal vein and hepatic artery. The Probes are chosen to comfortably encompass - but not constrict - the vessels, and are placed such that extraneous tissue is excluded. The field is then immersed in saline which serves as a good acoustic contact with the vessels. Readings stabilize rapidly, usually within 1-2 minutes, and in stable patients fluctuate less than ± 10% when left in situ for 10-15 minutes. If there is wider fluctuation, this usually indicates improper positioning of the Flowprobes with poor alignment or extraneous tissue, and can normally be corrected by repositioning. Arterial flow readings are meaningful over a brief snapshot period. Venous flow exhibits a far slower rhythm, dictated by events such as gastric motility. A one-to-five minute observation period is often adequate. LiverTransplantMedicalNote(TX-503-mn)Rev E 2013 Discussion Combined portal venous and hepatic artery flow are usually 15 - 25% of cardiac output. Of clinical importance is hepatic artery patency and flow, as survival of the graft depends on this. Flowprobes provide a volumetric measure of hepatic artery flow, and when this is low can be used to determine if there is a fixed anatomic limitation to flow or a physiologic limitation. For example, in a patient with a cardiac output of 10 L/min, portal flow of 2000 ml/min and hepatic artery flow of 75 ml/min, reduction of portal flow to 1000 ml/ min resulted in a hepatic artery flow increase to 125 ml/min. Thus, the low basal hepatic artery flow resulted from a high physiologic resistance rather than a fixed, potentially surgically correctable low inflow. This kind of data can be collected on the flowmeter’s strip chart recorder for a permanent record. The information obtained with these transit-time ultrasound Flowprobes is often at variance with “clinical impression.” A transplant with obstructed hepatic artery may show a strong pressure pulse on the artery, and a healthy organ color due to its venous perfusion. Accurate information on volumetric flow at the time of operation can either be reassuring, or may indicate an unexpected problem which can be fixed at this time. Intraoperative Blood Flow Measurements F l o w - A s s i s t e d L i v e r References LIVER HEMODYNAMICS TRANSPLANTED LIVER (N = 34)1 Vessel Flow: Mean ± SD (L/mm) Tr a n s p l a n t a t i o n Range Total Liver 2.091 ± .932 .570 - 4.540 Portal vein 1.808 ± .929 .300 - 4.500 Hepatic artery 0.268 ± 157 0.30 - 0.675 In a procedure such as liver transplant, where the stakes are high, this technology can be a useful adjunct in operative decision. Subsequent studies have identified the following intraoperative flow indices related to poor outcomes: • Poor outcome is associated with graft hyperfusion. Recipient portal venous flow in the recipient should be lowered when graft to recipient body weight ratio (GRBWR) < 0.8 is accompanied by portal inflow of > 250 mL/min/100g graft weight.3 • Hepatic arterial flow < 100 mL/min presents a significant risk on organ survival.4 • Hepatic artery flows of less than 200 mL/min following orthotopic liver transplantation increase the risk of subsequent hepatic artery thrombosis six times.5 1Henderson JM et al, “Hemodynamics During Liver Transplantation: The Interactions Between Cardiac Output and Portal Venous and Hepatic Arterial Flows,” Hepatology 1992; 16(3): 715-718. 2Henderson JM et al, Volumetric and Functional Liver Blood Flow Are Both Increased in the Human Transplanted Liver,” J Hepatology 1993; 17: 204-207. 3Troisi R, de Hemptinne B, “Clinical Relevance of Adapting Portal Vein Flow in Living Donor Liver Transplantation in Adult Patients, Liver Transplantation 2004; 9(9): S36-S41. 4 Lin M et al, “Hepatic Artery Thrombosis and Intraoperative Hepatic Artery Flow Rates in Adult Orthotopic Liver Transplantation, ANZ J Surg 2002; 72: 798-800. 5 Pratschke S et al, “Arterial Blood Flow Predicts Graft Survival in Liver Transplant Patients,”Liver Transplantation 2011; 17: 436-445. Hashimoto K, Miller CM, Quintini C, Aucejo FN, Hirose K, Uso TD, Trenti L, Kelly DM, Winans CG, Vogt DP, Eghtesad B, Fung JJ, “Is impaired hepatic arterial buffer response a risk factor for biliary anastomotic stricture in liver transplant recipients?” Surgery 2010; 148(3): 582-8. (9648AHM) Kelly DM, Shiba H, Nakagawa S, Irefin S, Eghtesad B, Quintini C, Aucejo F, Hashimoto K, Fung JJ, Miller C., “Hepatic blood flow plays an important role in ischemia-reperfusion injury.” Liver Transpl. 2011 Dec;17(12):1448-56. (9647AHM) FLOWPROBE RECOMMENDATIONS VESSEL Equipment Needed Probe Series 4-8 -FMV Portal vein 8 - 14 -FMV, -AU 8 -FMV, -FSB Common iliac a HT364 Dual-channel Optima Flowmeter permits simultaneous measurements with two Flowprobes. Probe Size (mm) Hepatic artery 4 mm and 6mm FMV Vascular Handle Flowprobes are recommended for hepatic arterial flow measurements. 8-14 mm -AU COnfidence Flowprobes® provide highly accurate measurements in vessels with fluctuating flows such as the portal vein. The Probes may be left in place for extended measurements and then easily removed via a ring attached to the pliable liner that cushions and protects the vessel. 8 to14 mm FMV Vascular Handle Flowprobes are recommended for portal venous flow measurements. Adult Liver Donor Liver Transplantation H e p a t i c A r t e r y Protocol & P o r t a l V e i n Living Donor Measure right hepatic arterial and portal venous flow before hilar dissection. Document measurements to serve as guide for expected flows in the recipient. Recipient Recipient Hepatic Flow Recipient Portal Flow Measure hepatic blood flow Measure portal blood flow - following reperfusion - before biliary anastomosis - before wound closure - following reperfusion - after portal pressure measurement - before biliary anastomosis Compare with pre-transplant hepatic arterial flow Compare with pre-transplant portal venous flow Flow increased up to 3 times pre-transplant portal flow < 50 mL/min Examine anastomosis for arterial thrombosis > 100 mL/min Flow increased > 3 times pre-transplant portal flow or >250 mL/min/110 gram graft weight Reduced graft inflow by shunting portal flow away from liver1 Remeasure hepatic flow Remeasure portal flow Flow has increased Document flows and save waveforms for the operative record for post-op diagnostic consideration Troisi R, de Hemptinne B, “Clinical Relevance of Adapting Portal Vein Flow in Living Donor Liver Transplantation in Adult Patients,” Liver Transplantation 2004;9(9) Suppl 1 pp S36-S41. (6884AH) Liver Transplant Hepatic/Portal References Cont. Quintini C, Hirose K, Hashimoto K, Diago T, Aucejo F, Eghtesad B, Vogt D, Pierce G, Baker M, Kelly D, Miller CM, “Splenic artery steal syndrome” is a misnomer: the cause is portal hyperperfusion, not arterial siphon.” Liver Transpl. 2008 Mar;14(3):374-9.(9649AHM) Aucejo, FN, Hashimoto, K, Quintini, C, Kelly, D, Vogt, D, Winans, C, Eghtesad, B, Baker, M, Fung, J, Miller, C, “Triple-Phase Computed Tomography and Intraoperative Flow Measurements Improve the Management of Portosystemic Shunts during Liver Transplantation,” Liver Transplantation 2008; 14: 96-99. (7606AH) Jakab F, Rath Z, Schmal F, Nagy P, Faller J, “A New Method to Measure Portal Venous and Hepatic Arterial Blood Flow in Patients Intraoperatively” HPB Surgery 1996; 9(4) 238-243. (855AH) Jakab F, Rath Z, Schmal F, Nagy P, Faller J, “The Afferent Circulation of the Liver in Patients with Primary Hepatocellular Carcinoma,” Hepatogastroenterology 1995;42(4) 399-402. (704AH) Jakab F, Rath Z, Schmal F, Nagy P, Faller J, “Blood Flow Measurement in Patients with Hepatocellular Carcinomas,” Acta Chir Hung 1994;34(1-2): 87-94. (559AH) Wagener G, Gubitosa G, Renz J, Kinhabwala M, Brentjens T, Guarreram JV, Emond J, Lee HT, Landry D, “Vasopressin Decreases Portal Vein Pressure and Flow in the Native Liver during Liver Transplantation,” Liver Transplantation 2008; 14: 1664-1670. (6673AH). Jakab F, Rath Z, Schmal F, Nagy P, Faller J, “The Interaction between Hepatic Arterial and Portal Venous Blood Flows; Simultaneous Measurement by Transit-Time Ultrasound Volume Flowmetry,” Hepatogastroenterology 1995;42(1): 18-21. (560AH Aneman A., Eisenhofer G., Olbe L., Dalenback J., Nitescu P., Fandriks L., Friberg P., “Sympathetic Discharge to Mesenteric Organs and the Liver,” J Clin Invest 1996; 97(5)1640-6. (1488AH) Jakab F, Rath Z, Schmal F, Nagy P, Faller J, “Intraoperative Estimation Bueno J, Escartin A, Baisells J, Margarit C, “Intraoperative Flow Measurement of Native Liver Allograft during Orthotopic Liver Transplantation in Children, Transplant Proc. 2007 39:7:2278-9. 7605AHM) Doi R, Inoue K., Kogire M., Sumi S., Takaori K., Suzuki T., Tobe T., “Simultaneous Measurement of Hepatic Arterial and Portal Venous Flows by Transit-time Ultrasonic Volume Flowmetry,” Surgery, Gynecology & Obstetrics 1988;167(1):65-69. (26AH) Doi, R., Inoue, K., Kogire, M., Sumi, S., Takaori, K., Suzuki, T., Tobe, T., “Study on Splanchnic Circulation: Measurement of the Liver Blood Flow,” Nippon Geka Gakkai Zasshi, 1988;89(4):560-7. (109AH) Figueras L., Llado L., Ramos E., Jaurrieta E., Rafecas A., Fabregat J., Torras J., Sabate A., Dalmau A, “Temporary portocaval shunt during liver transplantation with vena cava preservation. Results of a prospective randomized study,” Liver Transpl, Vol. 7, No. 10, p. 904-11, 2001. (2201AH) Panaro F, Bouyabrine H, Carabalona JP, Marchand JP, Jaber S, Navarro F, “Hepatic artery kinking during liver transplantation: survey and prospective intraoperative flow measurement,” J Gastrointest Surg. 2012 Aug;16(8):1524-30. (9796AHE) Rasmussen, A., Hjortrup, A., Kirkegaard, P., “Intraoperative Measurement of Graft Blood Flow - A Necessity in Liver Transplantation,” Transplant Int 1997;10(1):774-77. (1761AHM) Nanashima A, Pillay P, Crawford M, Nakasuji M, Verran DJ, Painter D, “Analysis of post-revascularization syndrome after orthotopic liver transplantation: the experience of an Australian liver transplantation center,” J Hepatobiliary Pancreat Surg, Vol. 8, No. 6, p. 557-63, 2001. (2276AH) Gontarczyk GW, Łagiewska B, Pacholczyk M, Trzebicki J, Jureczko L, Kołacz M, Kosieradzki M, Adadyński L, Wasiak D, Rowiński W, “Intraoperative blood flow measurements and liver allograft function: preliminary results,”Transplant Proc. 2006 Jan-Feb;38(1):234-6. Jakab F, Rath, Z. Schmal F, Nagy P, Faller J, “Changes in Hepatic Hemodynamics Due to Primary Liver Tumours,” HPB Surgery 1996; 9(4) 245-248. (854AH) Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. www.transonic.com AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] Renal Transplant Medical Note Intraoperative Blood Flow Measurement during Renal Transplantation Courtesy of Anders Lundell, MD, PhD, Nils H. Persson, MD, PhD, Dept. of Transplantation, Dept. of Surgery, Malmö General Hospital, Malmö, Sweden Renal Arterial Flow Measurement Donor: Living Donor Kidney Retrieval The first measurement is made on the renal artery before the kidney is removed from the donor. Recipient: Living Donor or Cadaver Kidneys In primary transplantations, we use the hypogastric artery for the arterial anastomosis. In re-transplantations or in cases where the internal iliac is atherosclerotic the external iliac artery is used. In selected cases, we use a flow measurement to decide which artery to use. For the venous anastomosis, the external iliac is used. No venous flow measurements are made. After completion of the arterial and venous anastomoses, and immediately after restoration of blood flow to the kidney, but before completion of the ureteroneocystostomy, the flow in the renal artery is measured. We use a 4 or 6 mm Flowprobe which is placed, preferably, distal to the anastomosis. The space between the Probe and the vessel is filled with sterile physiological saline. Care is taken to avoid kinking the artery and to place the Probe perpendicular to the longitudinal axis of the vessel. Before the flow is recorded, we allow the flow signal to stabilize for 15-20 seconds. At the end of the operation, after the ureteroneocystostomy is completed and before the wound is closed, we make a second measurement. MEAN RENAL ARTERIAL FLOWS TRANSPLANTED KIDNEY (N = 34)1 Flow: Cadaver Kidney (mL/mm) Donor Flow: Living Donor Kidney (mL/mm) 381 ± 150 SD Post flow restoration 283 ± 148 SD 338 ± 155 SD At end of operation 422 ± 204 SD 505 ± 177 SD RenalTransplantMedicalNote (TX-505-mn)Rev D 2013 Schematic of Perivascular Flowprobe measuring flow in the Renal Artery Intraoperative Blood Flow Measurement R e n a l A r t e r y M e a s u r e m e n t Donor P r o t o c o l Living Donor Kidney Cadaver Kidney Measure renal arterial flow before removing the kidney No measurements Document measurements to serve as guide for expected renal flow in the recipient. Recipient Measure renal arterial blood flow following arterial anastomosis Adequate flow: > 250 mL/min1 NO YES Check for technical error: Apply vasodilator & wait several minutes (up to 1 hour) YES Remeasure renal flow Continue attempts to improve flow. NO Adequate flow: > 250 mL/min YES NO Document measurement for operative record: Document flows and save waveforms for the operative record. Assess other clinical parameters (perfusion, urine output) Consider post-op prophylactic treatment.2 1 Lundell A et al, “Impaired Renal Artery Blood Flow at Transplantation Is Correlated to Delayed Onset of Graft Function” Transplant International 1996;9(1)57-61. 2 Bretan PN Jr et al, “Assessment of Preservation Induced Reperfusion Injury Via Intraoperative Renal Transplant Blood Flow and Endothelin Concentration Studies,” J Urology 1997;158(3):714-18. Renal Transplantation C a s e Fig. 1: The donor’s renal arterial blood flow prior to excision of the kidney measured 376 mL/min. After anastomosis to the recipient’s renal artery, post-reperfusion renal flow measured 91 mL/min. A second measurement was made after 30 minutes. Renal arterial flow had increased to 290 mL/min. Fig. 2: The donor’s renal arterial blood flow before traditional removal of the kidney measured 538 mL/min. After anastomosis to the recipient’s renal artery, renal flow post reperfusion measured 766 mL/min. R e p o r t s Fig. 3: Before a difficult laparoscopic removal of the kidney, the donor’s renal arterial blood flow measured 622 mL/min. After anastomosis to the recipient’s renal artery, renal flow post-reperfusion measured 322 mL/min. One hour later, flow had increased to 442 mL/min. Fig. 4: Before laparoscopic removal of the kidney, the donor’s renal arterial blood flow measured 91 mL/min. After anastomosis to the recipient’s renal artery, renal flow post-reperfusion measured 290 mL/min. Waveforms courtesy of Renal Transplantation Unit, Hermann Hospital, Texas Medical Center, Houston, TX. Renal Transplant Equipment HT354 single-channel Optima Flowmeter to acquire precise actual flow measurement quickly and easily. FMV Vascular Handle Flowprobes for spot flow checks during renal transplant surgery FLOWPROBE RECOMMENDATIONS VESSEL HT363 dual-channel Optima Flowmeter. permits simultaneous measurements with two Flowprobes. This allows the ability to compare flows simultaneously, or in quick succession, without the need for a second meter. Probe Size (mm) Handle Probe Series Renal artery 4, 6 -FMV Renal vein 10 -FMV External iliac artery 6, 8 -FMV Hypogastric a 4, 6 -FMV References: Lundell A, Persson NH, Kallen R, Ekberg H, “Impaired Renal Artery Blood Flow at Transplantation Is Correlated to Delayed Onset of Graft Function” Transplant International 1996;9(1)57-61. (Transonic Reference # 685AH) Wolffenbuttel KPet al, “Measurement of urinary flow rate using ultrasound in young boys and infants,” Journal of Urology, Vol. 47, No. 3, p. 312-8, 2001. (Transonic Reference # 2618AH) Wolters HH et al, “The anastomosis between renal polar arteries and arteria epigastrica inferior in kidney transplantation: an option to decrease the risk of ureter necrosis? Transplant International 14(6): (Transonic Reference # 7025AH) Bhatt KA et al, “Intraoperative graft verification in renal transplants,” Vasc Endovascular Surg. 2002; 36(2): 93-6. (Transonic Reference # 2713AHM) Bretan PN Jr et al, “Experimental and Clinical Assessment of PreservationInduced Reperfusion Injury Comparing Renal Transplant Blood Flow and Renal Endothelin Concentrations,” Transplantation Proceedings 1997; 29(8): 3520-3521. (Transonic Reference # 1092AH, 54V) Bretan PN Jr et al, “Assessment of Preservation Induced Reperfusion Injury Via Intraoperative Renal Transplant Blood Flow and Endothelin Concentration Studies,” J Urology 1997; 158(3): 714-18. (53V)(Transonic Reference # 1093AH) Alejandro V et al, “Mechanisms of filtration failure during postischemic injury of the human kidney. A study of the reperfused renal allograft,” J Clin Invest 1995; 95(2): 820-31.(Transonic Reference # 7026AH) Chiu C et al, “Intraoperative Reperfusion Blood Flow Predicts Post Warm Ischemic Kidney Transplant Survival and Efficacy of Preservation Maneuvers,” Transplantation Proc 1999; 31: 1049-1050 (Transonic Reference # 1302AH) Ramaswamy D et al,“Maintenance and recovery stages of postischemic acute renal failure in humans,” AJP 2002;. 282(2): D271-80.(Transonic Reference # 2326AH) Dominici A et al,“Cystic leiomyosarcoma of the kidney: an unusual clinical presentation,” Urol Int 2000; 65(4): 229-31. (Transonic Reference # 2122AH) Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. www.transonic.com AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] Transplant Surgery Transplant Medical Note Portal Vein Blood Flow Measurement during Auto Islet Cell Transplantation after Pancreatectomy Flow Measurement during Islet Infusion Excising a diseased pancreas removes not only pancreatic cells that produce digestive enzymes but also islet of Langerhans cells that produce insulin to control blood sugar. Without insulin a patient becomes diabetic and requires lifelong use of insulin to control blood sugars. Auto islet cell transplantation takes these islet of Langerhans cells from the pancreas and transplants them to the liver to reduce the diabetic risk. To do this, the removed pancreas is processed to isolate the insulinproducing islets of Langerhans cells. The isolated cells are suspended in a solution and are then slowly infused through the splenic vein back into the patient’s liver where it is hoped that they will implant, grow and produce insulin to metabolize sugar. Typically, 800 - 1500 cc of solution is infused into the portal vein distal to the splenic vein (Fig. 2) over an extended period of time. The team may elect to infuse a small amount over 5 minutes and allow the patient to recover before resuming the infusion. Blood pressure and flow are monitored continuously and for ten minutes after the infusion is completed (Fig. 1). Infusion bag Auto Islet Cell Transplantation After Pancreatectomy c) Liver d) Islet cells e) b) a) Pancreas Fig. 1: Steps: Auto Islet Cell Transplantation a) Removal of pancreas (pancreatectomy) b) Isolation of Islet cells from removed pancreas c) Islet cells placed in Infusion bag with solution d) Islet cells infused into splenic vein e) Islet cells implant in liver Flow Measurement during Islet Infusion Surgeons measure portal venous flow during islet cell infusion to detect any sudden decrease in flow that may foreshadow a problem with the infusion. A 10 mm to 14 mm Perivascular Flowprobe is placed on the portal vein and flow is measured continuously. The Flowprobe is chosen to comfortably encompass - but not constrict the portal vein. If needed, saline can be used to provide acoustic contact between the vein and Flowprobe. Readings stabilize within 1-2 minutes. Wide fluctuation of measurements may indicate improper positioning of the Flowprobe with poor alignment or fat within the ultrasonic sensing window. Repositioning can normally correct this problem. Discussion In this high stakes auto islet cell transplantation procedure, Flowprobes provide a continuous volumetric measure of portal vein flow to inform the surgeon about the safety, fluidity and success of auto islet cell transplantation. IsletCell (TX-524-mn) Rev B 2013 Infusion bag Flowprobe Islet cells Portal vein Splenic vein Superior Mesenteric Vein Fig. 2: Enlarged view of islet cell infusion into the splenic/portal venous system. Transplant Surgery Portal Vein Blood Flow Measurement during Auto Islet Cell Transplantation after Pancreatectomy Cont. Equipment Needs HT354 Single-channel Optima Flowmeter. Acquire precise actual flow measurement quickly, easily and cost effectively. 8 mm to 14 mm FMV Vascular Handle Flowprobes are recommended for portal venous flow measurements during islet cell infusion. COnfidence Flowprobe® COnfidence Flowprobes® provide highly accurate measurements in vessels with fluctuating flows such as the portal vein. The Probes may be left in place for extended measurements and then easily removed via a ring attached to the pliable liner that cushions and protects the vessel. References Sutherland DE, Radosevich DM, Bellin MD, Hering BJ, Beilman GJ, Dunn TB, Chinnakotla S, Vickers SM, Bland B, Balamurugan AN, Freeman ML, Pruett TL. “Total pancreatectomy and islet autotransplantation for chronic pancreatitis,” J Am Coll Surg. 2012 Apr;214(4):409-24. Bramis K, Gordon-Weeks AN, Friend PJ, Bastin E, Burls A, Silva MA, Dennison AR, “Systematic review of total pancreatectomy and islet autotransplantation for chronic pancreatitis.”Br J Surg. 2012 Jun;99(6):761-6. http://www.hopkinsmedicine.org/transplant/programs/auto_islet/description. html#total_pancreatectomy Henderson JM et al, “Hemodynamics During Liver Transplantation: The Interactions Between Cardiac Output and Portal Venous and Hepatic Arterial Flows,” Hepatology 1992; 16(3): 715-718. Henderson JM et al, Volumetric and Functional Liver Blood Flow Are Both Increased in the Human Transplanted Liver,” J Hepatology 1993; 17: 204-207. Troisi R, de Hemptinne B, “Clinical Relevance of Adapting Portal Vein Flow in Living Donor Liver Transplantation in Adult Patients, Liver Transplantation 2004; 9(9): S36-S41. Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. www.transonic.com AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] Transplant Surgery Medical Note Distal Spleno-renal (Warren) Shunt: Intraoperative Blood Flow Measurements Courtesy of J. Michael Henderson, M.D., F.A.C.S.,The Cleveland Clinic Foundation Rationale Splenic vein A distal spleno-renal shunt (DSRS) provides selective variceal decompression to control bleeding gastroesophageal varices, while maintaining portal hypertension and prograde portal flow to the liver (Fig. 2). Thrombosis of distal spleno-renal shunts occur in less than 10% of patients, but usually occurs early (in the first week) and requires reoperation. Intraoperative measurement of shunt flow shows great potential to reduce the risk of this complication. Surgical Approach On completion of the distal spleno-renal shunt anastomosis, 2-3 cm of the splenic vein is free below the pancreas before it is anastomosed to the left renal vein. A Transonic® Flowprobe can be placed on this segment of the splenic vein for volumetric flow measurement (Fig. 2). A Probe is chosen to fit comfortably around the vein without compressing it. It should lie in line with the vessel, and no tissue should be interposed. Contact is assured by immersing the field in saline. Flow measurements stabilize within one minute, and fluctuate less than ± 10%. Discussion What should the flow be in a distal spleno-renal shunt? This is a high flow shunt, with volumetric flows determined largely by spleen size. There appears to be approximately 1 mL/min flow per cubic centimeter spleen volumes - i.e. a 750 cc spleen will give a shunt volumetric flow of approximately 750 mL/min. After first removing the clamps, flow tends to be higher than it will be after 5-10 minutes when the initial hyperemia has resolved. If flow is significantly less than this approximation, a technical error should be considered. • Is the splenic vein kinked? • Is there a problem with the anastomosis? Now is the time to identify and correct a technical problem: transit-time ultrasound Flowprobes offer a method for identifying low flow in this shunt. Reference http://www.vesalius.com/cfoli frms.asp Spleno-renalshunt (TX-507-mn)Rev B 2013 Portal vein Renal vein Fig. 1: Schematic of splenic vein in relation to renal vein. Spleno-renal shunt Splenic vein Anastomosis Portal vein Renal vein Fig. 2: Schematic of anastomosis of the splenic vein to the renal vein to create a distal Spleno-renal shunt. Flowprobe on Splenic vein Portal vein Renal vein Fig.3: Flowprobe measuring flow in the splenic vein following anastomosis of the splenic vein to the renal vein. Transplant Surgery Distal Spleno-renal (Warren) Shunt: Intraoperative Blood Flow Measurements Cont. Equipment Needs HT353 Single-channel Optima Flowmeter. Acquire precise actual flow measurement quickly, easily and cost effectively. 8 mm, 10 mm and 12 mm FMV Vascular Handle Flowprobes are recommended measurement of distal spleno-renal shunt (venous) flow. Background Alcoholic (Laennec’s) cirrhosis of the liver is a common cause of portal hypertension. Portal hypertension extends to esophageal veins via gastric, splenic and gastroepiploic veins. When bulging esophageal varices are eroded by food passage through the esophagous, massive bleeding can result. A distal spleno-renal shunt is a high volume shunt that diverts splenic venous flow from the portal venous system to the renal venous system. An enlarged spleen (splenomegaly) is common in patients with end-stageliver disease. A distal spleno-renal shunt provides good long-term control of variceal bleeding. In 40% of U.S. cirrhosis patients, portal hypertension causes acute bleeding from the varices of the esophagus or stomach. This variceal bleeding accounts for one-third of all deaths related to cirrhosis. A significant bleeding episode is fatal 50% of the time. Of those surviving, two-thirds will rebleed. It is therefore crucial to first arrest the acute bleeding episode and then treat the portal hypertension. How Is a Distal Spleno-renal Shunt Constructed? One way to treat portal hypertension is through portal decompression via a surgically-created distal splenorenal (DSRS) or Warren shunt. The abdomen is opened. The stomach and pancreas are elevated to expose the splenic vein which is isolated and mobilized by detaching it close to its junction with the portal vein. The vein is then reattached to the renal vein via an end-to-side anastomosis (Figs. 2,3). Intraoperative flow measurement during creation of a DSRS ensures good shunt flow without kinking of the vein or a problem with the anastomosis. Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. www.transonic.com AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] Surgery Transonic Perivascular Flowprobes ® The widest selection of Flowprobes available Transonic’s application-customized Flowprobes measure volume flow in blood vessels and grafts from 0.5 mm to 36 mm to: •Quantify blood flow • Identify technical problems early • Improve patient outcomes FlowprobeFlyer(CV-500-fly)RevB 2014 Microvascular Flowprobes Flaps • Reattachments Transonic® Microvascular Flowprobes measure volume flow in blood vessels or grafts from 0.5 to 4.0 mm diameter. Flow measurement in these vessels during microvascular procedures quantify flows in the smallest vessels in order to objectively assess the quality of the reconstruction or replantation, guide better surgical decisions and give the surgeon the opportunity to correct otherwise undetectable flow restrictions before closing the patient. Due to extreme accuracy requirements, this Microvascular Flowprobe Series is only available with the Optima Flowmeter. Flexible neck Probe body Flowprobe handle Reflector Microvascular Flowprobe (2 mm) showing handle and flexible probe neck for easy positioning of the Flowprobe around a vessel. 0.7 mm 1.0 mm 1.5 mm 2.0 mm 3.0 mm Ultrasonic sensing windows of Microvascular Flowprobe (MU) Series. Side-by-side comparison of a 0.7 mm Flowprobe with a tip of a 25g. needle. Microvascular Flowprobe (-MU) Series including 0.7 mm, 1 mm, 1.5 mm, 2 mm, and 3 mm Flowprobes. Cardiac Flowprobes Coronary Artery Grafts • Ascending Aorta Transonic® Cardiac Flowprobes include FMC-Series Flowprobes for coronary artery bypass grafting surgery and COnfidence Flowprobes® for continuous measurement on great vessels with turbulent flows. Coronary Flowprobes Elongated curved neck Probe body Probe handle Flexible neck segment FMC-Series Coronary Handle Flowprobes are available in sizes 1.5 mm to 4 mm. They feature a J-style reflector, designed for spot flow checks of coronary artery bypass grafts and an extended neck with a flexible end to reach coronary grafts even behind the heart. COnfidence Flowprobes® Probe shell Ultrafit liner COnfidence Flowprobes consist of a Flowprobe shell and a single-use soft, flexible Ultrafit liner. This novel concept for ultrasonic signal coupling enables immediate, accurate beat-to-beat flow measurements with a minimum of ultrasonic coupling gel. The form-fitting Ultrafit Liner slips into the transducer shell to encircle the vessel and keep the vessel in place. The liner cushions and protects the vessel during a flow measurement. Liners are incrementally sized for optimal fit on the target vessel. ® Pictured, from left to right, are 1.5 mm, 2 mm, 3 mm and 4 mm coronary Flowprobes showing their blue Probe bodies, J reflectors and ultrasonic sensing windows. 28 mm 20 mm 16 mm 14 mm 12 mm 10 mm 8 mm 24 mm COnfidence Flowprobes® (-AU-Series), designed with four transducers, provide highly accurate measurements in vessels with highly turbulent flows such as the ascending aorta. The Flowprobe’s slim, ergonomic profile creates a minimal footprint that fits in tight anatomical sites. The soft, pliable liner cushions and protects the vessel. Available in 15 sizes from 8 mm to 36 mm. Port-Access Flowprobes Port-Access Flowprobes, a customer-driven innovation, feature a long endoscopic handle to extend through robotic ports and measure flows on coronary grafts. They are available in three sizes: 2 mm, 3 mm, and 4 mm. Vascular Flowprobes Peripheral Vascular • Carotid Endarterectomy Transonic’s spectrum of Vascular Flowprobes measure volume flows intraoperatively in vessels and grafts from 0.5 mm to 20 mm to detect blood flow obstructions before leaving the operating room. This ability to correct otherwise undetectable flow restrictions provides the surgeon with a unique opportunity to improve the outcome for his or her patient. Handle Vascular Flowprobes Probe body J Reflector Flexible neck Handle Short Handle Vascular Flowprobes: The FMV-Series features a short handle and a J reflector designed for spot flow checks. Available in a wide range of sizes from 1.5 mm to 14 mm. Carotid Flowprobes Non-handle Flowprobes Sliding cover Probe body L reflector L reflector Flexible neck FME-Series Flowprobes feature an L-shaped reflector to protect against dislodging of plaque (such as during carotid endarterectomy) as the Flowprobe is applied. The L reflector design allows the probe to be slipped on and off a carotid artery easily, facilitating quick pre- and post-procedure measurements. Available in 1.5 mm to 10 mm sizes. Non-Handle Flowprobes (FSB-Series) feature an ultrasonic flowsensing window defined by an L reflector with a sliding cover so that the Flowprobe can remain positioned around the vessel for extended measurements. FSB-Series Flowprobes are available in sizes from 2 mm to 14 mm. OptiMax® Flowprobes ® The OptiMax® family with J reflectors (shown) and L reflectors (not shown) are available in 4, 6, 8, 10 and 12 mm. OptiMax Flowprobes’ two reflector shapes and multiple probe sizes accommodate different surgical preferences and patient anatomies. The skin tabs secure the Flowprobe so that continuous measurements can guide vascular constructions, banding or revisions until a target flow is achieved. Cerebrovascular Flowprobes Aneurysm Clipping • EC-IC Bypass • AVMs • Fistulas Transonic® Cerebrovascular (Charbel) Flowprobes measure volume flow in intracranial and extracranial vessels during cerebrovascular flow preservation or flow augmentation surgeries. Intraoperative measurements of volume flow assure the integrity of flow in cerebral vessels or they alert the surgeon to dangerous flow deficits at a time when every minute counts. Intracranial Flowprobes Flexible neck Probe body Long bayonet neck Reflector Probe head Close-up Long bayonet neck Long bayonet neck intracranial Charbel Micro-Flowprobes® are available in three sizes, 1.5 mm, 2 mm and 3 mm, for aneurysm clipping, AVM and dural fistula obliteration surgeries. -MB & -MR-Series Charbel Micro-Flowprobes® are designed to measure flow in major intracranial vessels of the Circle of Willis. Their long bayonet neck permits use under a surgical microscope and a flexible neck segment permits bending the Flowprobe as needed to most easily position the probe around the vessel. Extracranial Flowprobes Short bayonet neck Short bayonet neck extracranial Charbel Probes® are available in three sizes, 3 mm, 4 mm and 6 mm, for extracranial vessels such as the superior temporal artery during extracranial-intracranial (EC-IC) bypass surgeries. Their short bayonet neck permits use under a surgical microscope and a flexible neck segment permits bending the Flowprobe as needed to most easily position the probe around the vessel. Side-by-side comparison between intracranial Charbel Micro-Flowprobes® and shorter neck extracranial Charbel Flowprobes® used during EC-IC bypass surgery. Surgery Transplant Flowprobes Liver • Renal • Heart/Lung • Pancreas Transonic® Flowprobes work with HT300-Series Flowmeters to measure volume flow in blood vessels and grafts from 0.5 to 36.0 mm. In critical transplant surgeries, intraoperative measurement of flow in vessels can guide surgical decisions to ensure vessel patency prior to closing. Probe body Flexible neck Reflector Handle FMV-Series 4 and 6 mm Vascular Flowprobes recommended for measuring hepatic arterial flow. Picture shows Flowprobe handle with size of Probe in mm, the Probe’s flexible neck for optimal positioning of the Probe around the vessel, the Probe body that houses the ultrasonic transducers, and the Probe reflector. Vessel is positioned within the Probe sensing window that is defined by the Probe body and its stationary reflector. Vascular Flowprobes (FMV-Series) in sizes 8 mm to 14 mm are used for spot portal venous flow measurements. COnfidence Flowprobes® (-AU-Series) can also be used for continuous portal venous flow measurements. Transonic Systems Inc. is a global manufacturer of innovative biomedical measurement equipment. Founded in 1983, Transonic sells “gold standard” transit-time ultrasound flowmeters and monitors for surgical, hemodialysis, pediatric critical care, perfusion, interventional radiology and research applications. In addition, Transonic provides pressure and pressure volume systems, laser Doppler flowmeters and telemetry systems. www.transonic.com AMERICAS EUROPE ASIA/PACIFIC JAPAN Transonic Systems Inc. 34 Dutch Mill Rd Ithaca, NY 14850 U.S.A. Tel: +1 607-257-5300 Fax: +1 607-257-7256 [email protected] Transonic Europe B.V. Business Park Stein 205 6181 MB Elsloo The Netherlands Tel: +31 43-407-7200 Fax: +31 43-407-7201 [email protected] Transonic Asia Inc. 6F-3 No 5 Hangsiang Rd Dayuan, Taoyuan County 33747 Taiwan, R.O.C. Tel: +886 3399-5806 Fax: +886 3399-5805 [email protected] Transonic Japan Inc. KS Bldg 201, 735-4 Kita-Akitsu Tokorozawa Saitama 359-0038 Japan Tel: +81 04-2946-8541 Fax: +81 04-2946-8542 [email protected] Surgery Flowprobe Selection Guide PERIVASCULAR FLOWPROBE SERIES & AVAILABLE SIZES SUFFIX DESCRIPTION SIZES (mm) -FMC Coronary 1.5, 2, 3, 4 -FMV Vascular 1.5, 2, 3, 4, 6, 8, 10, 12, 14 -FME Carotid (L-reflector for carotid endarterectomy) 1.5, 2, 3, 4, 6, 8, 10 -FTV OptiMax (hands-free, J-reflector) 4, 6, 8, 10, 12 -FTE OptiMax (hands-free, L-reflector carotid endarterectomy) 4, 6, 8, 10, 12 -MU Microvascular (handle) 0.7, 1, 1.5, 2, 3 -AU Cardiac Output COnfidence Flowprobe 8, 10, 12, 14, 16, 20, 24, 28, 32, 36 -MB Intracranial Charbel Micro-Flowprobe® (long bayonet handle) 1.5, 2, 3 -MB-S Extracranial EC-IC Bypass: Micro-Flowprobe (short bayonet handle) 3, 4, 6 -FSB Basic (no handle, L-reflector, sliding cover) 1.5, 2, 3, 4, 6, 8, 10, 12, 14 ® ® ® Recommended Sizes and/or Flowprobe Series for Specific Vessels or Applications CARDIAC SURGERY CABG: ON OR OFF PUMP Probe Size (mm) VASCULAR SURGERY Probe Series Arterial conduits 1.5, 2, 3, 4 -FMC Saphenous vein 2, 3, 4 -FMC CARDIAC OUTPUT Ascending aorta 28, 32, 36 -AU Pulmonary artery 24, 28, 32 -AU Pediatric heart 8, 10, 12, 14, 16, 20 -AU TRANSPLANT SURGERY Probe Size LIVER (mm) Probe Series CAROTID ENDARTERECTOMY Probe Size (mm) Common carotid artery 8, 10 -FTE -FME -FSB External carotid artery 6 -FTE -FME -FSB Internal carotid artery 6 -FTE -FME -FSB Radial artery 2, 3 -FMV Brachial artery 3, 4, 6 -FMV -FTV -FSB Graft venous outflow 4, 6 -FMV -FTV -FSB 4, 6 -FMV -FTV -FSB AV FISTULAS & GRAFTS Renal bypass 4, 6, 8 -FMV -AU Portal vein 10, 12, 14 -FMV -AU Renal artery 4, 6 -FMV -FSB Renal vein 10 -FMV -FSB External iliac artery 6, 8 -FMV -FSB LOWER EXTREMITY BYPASS Hypogastric artery 4, 6 -FMV -FSB 8 -FMV -FSB PANCREAS Common iliac artery CEREBROVASCULAR SURGERY ANEURYSM CLIPPING Cerebral arteries Probe Size (mm) Probe Series 1.5, 2, 3 -MB -MR Extracranial 3, 4, 6 -MB-S MR-S Intracranial 1.5, 2, 3 -MB -MR EC-IC BYPASS -FSB ABDOMINAL Hepatic artery KIDNEY Probe Series Aortoiliac shunt aorta 16, 20 -AU -FSB common iliac 10, 12 -FMV -FTV -AU -FSB Portocaval shunt 10, 12, 14 -FMV -FTV -AU -FSB Splenorenal shunt 10, 12, 14 -FMV -FTV -AU -FSB Profunda femoris 8 -FMV -FTV -AU -FSB Common femoral 8, 10 -FMV -FTV -AU -FSB Popliteal 4, 6 -FMV -FTV -FSB Tibial 3, 4 -FMV -FTV -FSB MICROVASCULAR SURGERY REATTACHMENTS/FLAPS Probe Size (mm) Probe Series Microvessels in hand, wrist 0.7, 1, 1.5, 2, 3 -MU AVM, TUMOR RESECTION, DURAL FISTULA Outflows variable FlowprobeSelectionGuide(CV-66-tn)RevE 2014 -MB, -MR www.transonic.com








© Copyright 2026