
BC’s New P3 Evaluation Process Drives Facility Solutions to Bend the
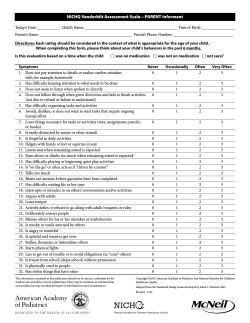
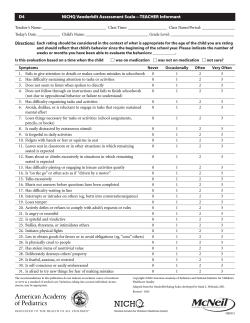
BC’s New P3 Evaluation Process Drives Facility Solutions to Bend the Healthcare Cost Curve Interior Heart & Surgical Centre PRESENTERS <insert B&W photo> Leslie Gamble Clinical Coordinator <insert B&W photo> Rick Steele Assistant Vice President Mike Marasco CEO Overview • Project description • Procurement process overview • Evaluation criteria • Desired outcomes • How the Plenary Health team responded • Procurement challenges from a government perspective • How the process will evolve in BC 3 Project Overview Interior Heart & Surgical Centre • 152,000 ft2 facility – 3 story addition to Kelowna General Hospital, Kelowna, B.C. • 15 operating rooms (2 cardiac) • Pre- and post-operative patient areas • Cardiac intensive care unit • Central sterilization and reprocessing department Total Project Cost: $110 million Total Financing: $80 million Consortium: Plenary Group, PCL, Johnson Controls Financial Close: June 2012 Target Completion: March 2015 Status: Construction Drawings 4 Scored Elements Identify main cost drivers Identify where design enhancements can enhance user outcomes and operational savings Estimate the cost savings and benefits for each design enhancement 5 Evaluation Framework Compliance Scored 6 Scored Elements -- IHSC Wellness Environment (14.5 points) (Access to direct light and outdoor space, natural features) Optimize Clinical Utilization (32.5 points) (Location, orientation and distance to medication rooms, location of storage space) Score Benefit Enhanced Site Development Features (9.5 points) (Ease of access and wayfinding, site parking, and vehicular flows) 100 Enhanced Patient Safety (43.5 points) (Travel routes, room standardization, ability to safely monitor patients) 0 Indicative Design Features (Baseline) How the Evaluation Criteria was Developed 1. “Quantifiable benefits/outcomes” were determined through use of internal and external research/data. 2. IH priorities reflected in the weighted points/scored element. 3. IH worked with consultants/PBC to develop scoring methodology and min/max for each element 4. PBC determined value/point and “fair processes” 8 Weighting of Scored Elements Enhance Patient Safety by Reducing # of Adverse Events Data Calculation Annual # of Surgeries 19000 % preventable errors (BN) X 3.3% Average increase in LOS/AE (BN) X 6.2 days Cost / inpatient day (IH) X $2528 % attributed to design (Fable) X 20% % attributed to scored components (IH) X 40% Annual Savings $806,876 9 10 Results Process: • Proponents went after all points with exception of AEDET • Clearly defined methods of scoring were essential • Objective/detailed scoring = time commitment from evaluation team Clinical Priorities: • Efficient high risk patient transport routes • Additional staircases to increase physician/staff access • Patient rooms/bays/OR’s standardized – column interference was minimal • Natural light in all departments; healing elements incorporated • Major building and MDR flows optimized 11 The Plenary Health Team Response Team Structure: • Shifted the structure to make it “design led” focus to optimize design • Utilized IPD to optimize solutions that responded to evaluation criteria 12 Focus for Most PPP / P3 Procurements 40 Year Facility Cost of Operations1 29.0% 0.1% 0.9% O&M Refurbishment 8.7% Planning 3.1% Design Construction Transition 58.0% Note 1: From July 2010 Healthcare BIM Consortium ,An Organization consisting of Department of Defense Military Health System (DoD MHS), Department of Veterans Affairs (DVA), Kaiser Permanente (KP), and Sutter Health, representing $26B of Healthcare construction 13 Focus for IHSC is to Drive Total Cost 40 Year Cost of Operations1 2.5% 0.0% Program 0.1% O&M 0.8% 91.2% Refurbishment Planning 8.8% 5.1% 0.3% Design Construction Transition Note 1: From Massachusetts Hospital Association, July 2010 Update to Hospital Costs in Context Report 14 The Plenary Health Team Response Team Behavior • Moved away from focusing on low NPV • Evaluated the cost versus NPV benefit of pursuing scored elements • More importantly, focused on EBD and Clinical Best Practices rather than simply meeting the output specification • We were concerned that some of the design solutions we put forward that responded to the scored elements were producing a result that IHA was not anticipating or liked 15 The Plenary Health Team Response 16 Government Perspective – Overall Cost 40 Year Cost of Operations1 2.5% 0.0% Program 0.1% O&M 0.8% 91.2% Refurbishment Planning 8.8% 5.1% 0.3% Design Construction Transition Government Challenges with Process • Cost and time • • • • • • • Consistency Compliance vs. scoring Credibility Obtaining data Valuation over concession term Tracking outcomes Privacy and transparency 18 Lessons Learned • Less is sometimes better • • • • Unrealistic accuracy Be careful what you ask for – unintended consequences Stand back and look at the big picture Process works! 19 How the BC Model will Evolve • Greater acceptance of process • • • • • • Planned for all upcoming health projects Data will become more available Integration with lean thinking Lower costs to implement New indicators as evidence emerges Concept will spread to other sectors 20 Questions & Discussion [email protected] [email protected] [email protected] 21










© Copyright 2026