
High-Risk Human Papillomavirus Detection In Situ Hybridization
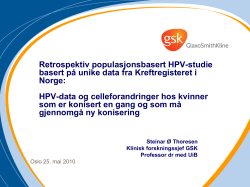
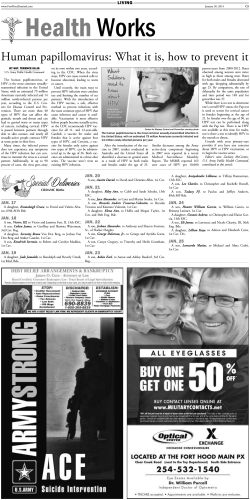
Anatomic Pathology / HPV TESTING: HC II VS CISH High-Risk Human Papillomavirus Detection A Split-Sample Comparison of Hybrid Capture and Chromogenic In Situ Hybridization Carol L. Schiller, MD,1 Angel G. Nickolov, MA,2 Karen L. Kaul, MD, PhD,1 Elizabeth A. Hahn, MA,2 Janine M. Hy, CT(ASCP),1 Maura T. Escobar, CT(ASCP),1 William G. Watkin, MD,1 and Charles D. Sturgis, MD1 Key Words: Human papilloma virus; HPV; Hybrid Capture; HC II; Chromogenic in situ hybridization; CISH; Atypical squamous cells of undetermined significance; ASC-US DOI: 10.1309/13NMAK8J3N1YJXU1 Abstract The American Society for Colposcopy and Cervical Pathology (ASCCP) has proposed high-risk human papillomavirus (HPV) testing as the “preferred” triage for women with atypical squamous cells of undetermined significance. We studied 401 atypical squamous cells of undetermined significance liquidbased cervicovaginal cytology split samples for HPV by chromogenic in situ hybridization (CISH) and by Hybrid Capture (HC) II (Digene, Gaithersburg, MD); 202 underwent HC II followed by CISH, and 199 underwent CISH followed by HC II. Of 401 vials, 101 (25.2%) were positive for HPV by 1 or more methods. HC II labeled 83 of 401 (20.7%) samples as positive, while 38 of 401 (9.5%) were positive by CISH. Positive attributes of CISH include the provision of a cytomorphologic link in assessing HPV positivity and comparative ease of use in laboratories without trained molecular diagnosticians. Greater efficacy and quantitative design are advantages of HC II. Comparing data by sequence of testing showed a lower likelihood of positive test results on the second ancillary test than on the first ancillary test, regardless of age or testing method (odds ratio, second/first = 0.58; P = .003). This finding suggests that liquid-based cervicovaginal cytology samples are not homogeneous throughout. Correlative studies with histology and polymerase chain reaction may clarify predictive values for both methods. The concept of studying epithelial cells exfoliated from the uterine cervix as a means of establishing the diagnosis of and screening for cervical carcinoma is roughly 60 years old.1,2 Although this is a brief period in the scheme of medical development, it is a comparatively long span for a modern laboratory medicine test to exist and be used widely in an unchanged method. In this sense, some would say that cytopathologists have lingered behind other laboratory professionals in implementing new technologies and pushing diagnostic limits. Hematopathologists, for example, have become fluent in the biology and terminology of their diagnoses at the level of nucleic acids, chromosomes, and proteins.3,4 One of the reasons that hematopathologists are decades ahead of their cytopathology colleagues is the disease types studied. Leukemias and lymphomas provided their investigators with innumerable discrete islands of sameness, each with cytogenetic, molecular-genetic, and protein-level information neatly packaged for discovery in natural cell suspensions. Cytopathologists have only recently begun working in a “liquid” cervical milieu.5,6 This transition is opening many avenues for clinical use and scientific investigation. The application of biotechnology to cervicovaginal cytology was seen first during the 1980s when morphologic criteria for the diagnosis of preneoplastic cytologic changes were compared successfully with human papillomavirus (HPV) DNA hybridization studies.7 These early cytologicmolecular correlation studies were limited to research settings and relatively small samples. Such studies were empowering for the cytodiagnostic community because they provided a “gold standard” for comparison other than histology, an equally imprecise science.8 Since then, an ancillary testing corner has been turned on the course of Am J Clin Pathol 2004;121:537-545 © American Society for Clinical Pathology 537 DOI: 10.1309/13NMAK8J3N1YJXU1 537 537 Schiller et al / HPV TESTING: HC II VS CISH cervicovaginal cytology screening. In many centers, such as ours at Evanston Northwestern Healthcare, Evanston, IL, almost all cervical cancer screening tests are collected and processed using a liquid-based approach that permits increased detection of preneoplastic lesions.9-16 In addition, liquid-based exfoliative cytology methods prepare samples for filtration of excess blood and inflammation, resulting in decreased “unsatisfactory” rates. Liquid-based cervical cytology also provides monolayer distributions for ease of interpretation and, perhaps most important, permits 1-visit, split-sample preparations of cellular material for ancillary studies. Cervicovaginal cytology screening has changed dramatically during the short time from the late 1980s to today. Information from the multicenter randomized Atypical Squamous Cells of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesion Triage Study has shown that testing for the genetic material of high-risk HPV types can be a valuable colposcopy-determining step for women interpreted to have atypical squamous cells of undetermined significance (ASC-US) in their cervicovaginal samples.17,18 This triage mechanism has been presented by the American Society for Colposcopy and Cervical Pathology as the “preferred” management algorithm for women interpreted to have ASC-US cells in their cervicovaginal cytology samples.19 In light of these developments, substantial time and financial resources have been invested in bringing manageable, reproducible, and reliable HPV DNA testing to the routine diagnostic cytology arena. We report our experience with 2 different HPV testing methods, Hybrid Capture (HC) II (Digene, Gaithersburg, MD) and chromogenic in situ hybridization (CISH). A comparison of high-risk HPV testing by the methods was performed on split samples from liquid-based cervicovaginal cytology specimens in a population of women diagnosed with ASC-US at our center. Approximately half of the vials underwent CISH followed by HC II (group 1), and the remaining underwent HC II testing followed by CISH (group 2). The results of these studies are discussed with attention given to testing outcomes, trends, statistical analysis, and methodological limitations and advantages. Materials and Methods Samples, Preparation, and Interpretation Cellular residua from 401 nonconsecutive, clinically ordered, ThinPrep (Cytyc, Boxborough, MA) cervicovaginal vials diagnosed as ASC-US ❚Image 1❚ by pathologists at Evanston Northwestern Healthcare Laboratory Services between January 2002 and August 2002 were retrieved and submitted for testing by HC II HPV high-risk probe (HPV 538 538 Am J Clin Pathol 2004;121:537-545 DOI: 10.1309/13NMAK8J3N1YJXU1 ❚Image 1❚ ThinPrep cervicovaginal cytology slide (from a 38year-old group 1 patient [samples underwent chromogenic in situ hybridization followed by Hybrid Capture II testing]) with cells interpreted as atypical squamous cells of undetermined significance. Nuclear enlargement and mild hyperchromasia were identified cytomorphologically (Papanicolaou, ×600). For proprietary information, see the text. types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) microplate assay and CISH using the INFORM HPV liquidbased prep high-risk probe (HPV types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 68, and 70) (Ventana, Tucson, AZ). During the study period, 27,479 gynecologic cytology specimens were processed at Evanston Northwestern Healthcare Laboratory Services, with an overall rate of ASC-US diagnoses of 4.24% (1,164/27,479). Some vials were excluded from the study owing to insufficient quantity of sample to perform further parallel testing. Approximately half of 401 samples underwent CISH followed by HC II testing (group 1; n = 199), and the remaining samples underwent HC II testing followed by CISH (group 2; n = 202). HC II testing of group 2 specimens was performed within 21 days of initial specimen collection. CISH analysis of group 1 and group 2 specimens and HC II testing of group 1 specimens were performed at intervals ranging from 22 to 219 days after collection. The 202 group 2 samples had been ordered by clinicians to have HPV testing performed following cytomorphologic diagnosis. Of these, 123 were to have HPV testing performed as a “reflex” following a diagnosis of ASC-US, 22 were to have HPV testing performed regardless of cytomorphologic diagnosis, and 57 had supplementary HPV testing ordered after initial specimen processing. The HC II test was the assay in clinical use for all ordered HPV testing by the Molecular Diagnostics Laboratory, Evanston Hospital, at that time. The 199 group 1 © American Society for Clinical Pathology Anatomic Pathology / ORIGINAL ARTICLE cases did not have HPV testing ordered by submitting physicians. All specimens used for analysis were the residua of clinically ordered cervicovaginal cytology samples. All HC II testing was performed in the Molecular Diagnostics Laboratory, Evanston Hospital (K.L.K.). The details of the HC II method have been described.20,21 Consistent with the testing protocol, the results of HC II studies were reported as positive or negative. The CISH procedure was performed in the Cytology Preparation and Immunocytochemistry Laboratories, Evanston Hospital (C.L.S.). Unstained slides were prepared from cellular samples in PreservCyt fixative solution (Cytyc), using the ThinPrep 2000 Processor (Cytyc). Slides were stored refrigerated until testing. The CISH procedure was performed on the Benchmark Automated Slide Stainer (Ventana), according to the manufacturer’s standard protocol.22-25 After initial incubation periods and buffer rinses, an endopeptidase was applied to and incubated on the slides, permitting exposure of nuclear DNA to the liquid-based prep high-risk reagent probe. The probe consisted of a cocktail of fluorescein-labeled DNA oligonucleotides that had been demonstrated to hybridize to specific high-risk HPV genotypes. Initially, a mouse antifluorescein primary antibody bound the probe. Then, a biotinylated secondary horse antibody formulation bound to the primary mouse antibodies. This step was followed by the addition of a streptavidin enzyme (alkaline phosphatase) conjugate that bound to the biotin present on the secondary antibody. The specific antibody–secondary antibody–streptavidin enzyme complex then was visualized by light microscopy using nitroblue tetrazolium as a substrate for a precipitating enzyme-generated product, resulting in a deep blue to black staining of cellular areas where there had been successful probe hybridization. A nuclear fast red–based counterstain was used. Positive control slides consisted of commercially available prepared cytocentrifuged slides using a CaSki cell line preparation containing approximately 400 copies of HPV type 16 DNA per cell (Ventana). Negative control slides were prepared in house from the cellular residua of liquidbased cervicovaginal samples that had been diagnosed cytomorphologically as no intraepithelial lesion or malignancy. The CISH slides were screened by 2 cytotechnologists (J.M.H. and M.T.E.), who referred all potentially positive slides for definitive interpretation. Definitive positive or negative results were determined by the consensus microscopic interpretation of 2 pathologists (C.L.S. and C.D.S.). A positive result was defined as any convincing blue to black nuclear staining, whether focal or global within the given nucleus ❚Image 2❚. Convincing staining within a single cell was interpreted as positive per manufacturer guidelines. All testing was performed in a blinded manner. ❚Image 2❚ Positive chromogenic in situ hybridization slide from the same patient as in Image 1. This study was interpreted as positive for high-risk human papillomavirus DNA based on discrete blue-black nuclear staining from successful probe hybridization, antibody-enzyme complex formation, and nitroblue tetrazolium substrate precipitation (×600). Statistical Analysis The Wilcoxon rank sum test was used to compare the patient age distributions in groups 1 and 2 (A.G.N. and E.A.H.). To account for correlated data owing to the crossover design, we implemented a logistic regression model for repeated binary measures.26 The outcome variable was assigned a value of 1 if the test used was reported as having a positive result for HPV and 0 if the result was negative. There were 3 explanatory variables: age group (<30 years vs 30-39 years vs ≥40 years), test (CISH vs HC II), and sequence (first ancillary aliquot tested vs second). The initial model included all 3 explanatory variables and their second- and third-order interactions. Nonsignificant interaction terms were dropped one at a time by using a backward elimination strategy and likelihood ratio tests. A P value of less than .05 was considered statistically significant. Data were entered into an Excel worksheet (Microsoft, Redmond, WA) and exported into SAS software (1999, release 8.2; Cary, NC) for statistical analyses. Results The 401 patients whose samples were included in the study ranged in age from 14 to 90 years, with an overall mean age of 37.8 years ❚Figure 1❚. The mean age of group 1 patients was 38.7 years (range, 14-76 years) ❚Figure 2❚ and Am J Clin Pathol 2004;121:537-545 © American Society for Clinical Pathology 539 DOI: 10.1309/13NMAK8J3N1YJXU1 539 539 Schiller et al / HPV TESTING: HC II VS CISH group 40 years or older, the odds ratio for a positive CISH test was 1.94 for the group younger than 30 years and 1.31 for the group 30 to 39 years old. Despite the observed trend, these 2 odds ratios were not significantly different from 1.00 (P = .082 and P = .574, respectively). Compared with the group 40 years or older, the odds ratio for a positive HC II test was 6.64 for the group younger than 30 years and 2.51 for the group 30 to 39 years old. In contrast with the ratios for CISH, the 2 odds ratios for HC II were significantly greater than 1.00 (P < .001 and P = .018, respectively; Table 2). A significant interaction between age and test was identified (Figure 4; Table 3). For group 1, the odds ratio for a positive CISH result compared with a positive HC II result was 0.43 (P = .006) for the group younger than 30 years, 0.77 (P = .525) for the group 30 to 39 years old, and 1.47 (P= .343) for the group 40 years or older. The sequence effect manifested itself through smaller corresponding odds ratios for group 2, with an odds ratio for a positive CISH result compared with a positive HC II result of 0.14 (P < .001) for the group younger than 30 years, 0.25 (P = .001) for the group 30 to 39 years old, and 0.49 (P = .095) for the group 40 years or older. The CISH test generally was less 140 70 120 60 No. of Samples No. of Samples for group 2 patients was 36.9 years (range, 19-90 years) ❚Figure 3❚. There were more patients aged 30 to 39 years in group 2 than in group 1 and more patients aged 40 to 49 years in group 1 than in group 2. In the final logistic model, the primary explanatory variables (test, sequence, and age group) and 1 second-order interaction (test-age group) were statistically significant. Of the 401 samples tested, 101 (25.2%) were positive for the presence of high-risk HPV DNA by one or both methods; 18 (4.5%) were positive by CISH alone and 63 (15.7%) by HC II alone; 20 (5.0%) were positive by both methods. A total of 38 (9.5%) were positive by CISH and 83 (20.7%) by HC II. The probabilities of a positive CISH and/or HC II test result were significantly dependent on the order in which the tests were administered; specifically, a positive result was less likely when either test was performed on the second aliquot removed for ancillary testing from a given sample. The odds ratio of obtaining a positive result when performed second in sequence vs when performed first in sequence was 0.58 (P = .003) ❚Table 1❚. With respect to age, the likelihood of a positive test result was associated negatively with age and varied by test ❚Figure 4❚ , ❚Table 2❚ , and ❚Table 3❚ . Compared with the 100 80 60 40 20 50 40 30 20 10 0 <20 0 20-29 30-39 40-49 50-59 60-69 70-79 79+ < 20 Age (y) No. of Samples ❚Figure 1❚ Age distribution of all 401 patients whose cervicovaginal cytology samples were studied. 80 70 60 50 40 30 20 10 0 30-39 40-49 50-59 Age (y) 60-69 70-79 ❚Figure 2❚ Age distribution of 199 group 1 patients (samples underwent chromogenic in situ hybridization followed by Hybrid Capture II testing) whose cervicovaginal cytology samples were studied. For proprietary information, see the text. ❚Table 1❚ Odds Ratios for a Positive Test Result by Sequence* <20 20-29 30-39 40-49 50-59 60-69 70-79 79+ Age (y) ❚Figure 3❚ Age distribution of 202 group 2 patients (samples underwent Hybrid Capture II testing followed by chromogenic in situ hybridization) whose cervicovaginal cytology samples were studied. For proprietary information, see the text. 540 540 20-29 Am J Clin Pathol 2004;121:537-545 DOI: 10.1309/13NMAK8J3N1YJXU1 Sequence Second (N = 401) First (N = 401) * Odds Ratio (95% Confidence Interval) P 0.58 (0.40-0.82) 1.00 .003 — Positive human papillomavirus testing results were found with significantly greater likelihood when testing was conducted on the first ancillary liquid aliquot out of the vial than when conducted on the second ancillary liquid aliquot, regardless of testing method. © American Society for Clinical Pathology Anatomic Pathology / ORIGINAL ARTICLE 100 Frequency of Positive Results (%) likely to have a positive result than the HC II test in groups 1 and 2, especially in younger patients (with the exception of the 40 years or older age group in group 1, in which the second-order action of test-age group interaction prevailed). A comparison of the charts of predicted and observed probabilities for a positive test result demonstrated that the logistic model fit the data well and was able to capture the reversed trend in the group 40 years or older in group 1 ❚Figure 5❚, ❚Figure 6❚, ❚Table 4❚, and ❚Table 5❚. CISH 1st in Sequence CISH 2nd in Sequence HC 1st in Sequence HC 2nd in Sequence 80 60 40 20 0 <20 20-29 30-39 40-49 50-59 60-69 70-79 79+ Age (y) ❚Figure 4❚ Positive high-risk human papillomavirus results by age, testing method, and split-sample sequence. CISH, chromogenic in situ hybridization; HC, Hybrid Capture. For proprietary information, see the text Discussion In the 60 years since the introduction of exfoliative cervicovaginal cytology as a screening test for precursor dysplastic and malignant cells, the incidence of invasive cervical carcinoma in the United States has dropped dramatically. Despite this testament to the value of what arguably has been the most successful cancer screening test in medical history (cervicovaginal screening cytology), approximately 6,400 American women still died of cervical carcinoma during the year 2000, and approximately 233,000 women died of cervical carcinoma worldwide.27,28 How can the cytopathology community improve these numbers? The obvious answer would be to somehow ensure that all women at risk have access to regular screening (universal health policy) and to somehow ensure that the best possible testing methods be used for all women. It is beyond the scope of this article to address the institution of health care policy changes; the focus of this work is on preventing patients who are screened and who have cellular atypia of undetermined significance from slipping through the diagnostic “cracks.” Because the vast majority of cervical carcinomas are HPVdriven, ancillary HPV testing to triage patients diagnosed with ASC-US has been proposed as one management option. Molecular-genetic HPV testing not only has the capability of clarifying cellular atypia but also has the potential to limit unnecessary and potentially expensive procedures such as colposcopies and biopsies. In addition to cytomorphologic testing, many testing methods have been used to detect the presence of HPV in cervicovaginal specimens, including viral load quantification, Southern blot, polymerase chain reaction (PCR), ViraPap (Life Technologies, Gaithersburg, MD), Hybrid Capture tube testing, Hybrid Capture microtiter plate assays, and CISH. While PCR likely would be considered the gold standard for the detection of viral DNA, its performance requires a laboratory with a highly trained technical and professional staff. In addition, commercially available high-risk HPV PCR cocktail assays are only now coming to market. In our study, we set out to explore and compare the performance characteristics of 2 methods, a Hybrid Capture microtiter plate assay and CISH. While our data clearly demonstrate that both HC II and CISH are capable of detecting the presence of HPV DNA, they also highlight differences in performance between the 2 methods. Perhaps owing to its nature as a signal amplification technique, HC II detected the presence of HPV DNA more frequently than CISH. In our series overall, a patient was more than twice as likely to have a test result positive for the presence of high-risk HPV DNA by HC II (83/401) than by CISH (38/401). The greater HC II percentage of positivity was seen in all age groups regardless of the order in which the tests were performed, except in the group 40 years or older in group 1, in which a trend toward a greater percentage of positive CISH results was observed (Figures 4 and 5; Table 3). The comparatively greater HPV DNA detection rate of HC II is one of the method’s positive attributes. In addition, the nature of the numeric cutoff value for determining positivity ❚Table 2❚ Odds Ratios (95% Confidence Intervals) for a Positive Test Result by Age Group and Test* Test CISH (N = 401) Hybrid Capture II (N = 401) <30 y 1.94 (0.92-4.10) 6.64 (3.49-12.63) P 30-39 y P ≥40 y P .082 <.001 1.31 (0.51-3.37) 2.51 (1.17-5.38) .574 .018 1.00 1.00 — — CISH, chromogenic in situ hybridization. * Younger women (<40 years) had positive test results for human papillomavirus nucleic acids more commonly than did older women. These differences were statistically significant with the Hybrid Capture II method. For proprietary information, see the text. Am J Clin Pathol 2004;121:537-545 © American Society for Clinical Pathology 541 DOI: 10.1309/13NMAK8J3N1YJXU1 541 541 ❚Table 3❚ Odds Ratios for a Positive Test Result by Test and Age Groups* Group Odds Ratio (95% Confidence Interval) P <30 (n = 2 × 68) 30-39 (n = 2 × 28) ≥40 (n = 2 × 103) 0.43 (0.23-0.79) 0.77 (0.34-1.74) 1.47 (0.66-3.25) .006 .525 .343 <30 (n = 2 × 71) 30-39 (n = 2 × 57) ≥40 (n = 2 × 74) 0.14 (0.07-0.28) 0.25 (0.11-0.57) 0.49 (0.21-1.13) <.001 .001 .095 1 2 In group 1 (n = 199), samples underwent chromogenic in situ hybridization (CISH) followed by Hybrid Capture (HC) II testing; in group 2 (n = 202), samples underwent HC II testing followed by CISH. The odds of detecting human papillomavirus genetic material were significantly higher by HC II than by CISH in younger women. For proprietary information, see the text. Positive High-Risk HPV DNA Test (%) * 50 42.3% 45 40 35 13.2% 32.4% 26.3% 30 25 20 12.2% 12.7% 15 7.1% 7.1% 9.7% 8.8% 10 4.9% 4.1% 5 0 <30 y 30-39 y ≥40 y <30 y 30-39 y ≥40 y Group 1 Group 2 ❚Figure 5❚ Observed probabilities for positive high-risk human papillomavirus (HPV) DNA testing by age, method, and sequence. More overall positive results are noted with Hybrid Capture (HC) II (white bars) than with chromogenic in situ hybridization (CISH; black bars). More overall positive results are noted in the first test in sequence, regardless of method. In group 1 (n = 199), samples underwent CISH followed by HC II testing; in group 2 (n = 202), samples underwent HC II testing followed by CISH. For proprietary information, see the text. virtually eliminates interobserver variability, removing subjectivity from the reporting of HC II results. Despite labeling fewer samples as HPV DNA positive than HC II, the CISH method offers the opportunity to view the cytologic location of HPV infection (ie, nuclear localization in cytomorphologically abnormal cells), which permits a morphologic link in assessing positivity. The flip side is that CISH results can be difficult to interpret. Multiple factors, including bacteria, yeast, improper dehydration in the staining process, and cellular clumping and degeneration, can cause staining artifacts that, if overinterpreted, might lead to false-positive results. In our experience, there is a substantial learning curve in the interpretation of CISH results, which might introduce interobserver variability and subjectivity in reporting. One interesting if unexpected finding in our series was the number of samples that were positive by CISH but negative by HC II (18/401 total 542 542 Am J Clin Pathol 2004;121:537-545 DOI: 10.1309/13NMAK8J3N1YJXU1 Positive High-Risk HPV DNA Test (%) Schiller et al / HPV TESTING: HC II VS CISH 50 43.5% 45 40 35 16.0% 30.7% 30 22.6% 25 20 11.4% 14.4% 15 8.9% 6.3% 9.9% 6.9% 10.4% 10 5.4% 5 0 <30 y 30-39 y ≥40 y <30 y 30-39 y ≥40 y Group 1 Group 2 ❚Figure 6❚ Predicted probabilities for positive high-risk human papillomavirus (HPV) DNA testing by age, method, and sequence. Comparison of this graph to the graph in Figure 5 demonstrates that the predicted and observed probabilities for positive testing mirror each other, indicating a good fit for the logistic regression model. The model was able to capture the reversed trend in the group 1 patients who were older than 40 years. Black bars, positive results with CISH; white bars, positive results by Hybrid Capture (HC) II testing. Group 1 samples underwent CISH followed by HC II testing; group 2 samples underwent HC II testing followed by CISH. The age distributions were as follows: group 1: younger than 30 years, 68; 30-39 years, 28; 40 years or older, 103; group 2: younger than 30 years, 71; 30-39 years, 57; 40 years or older, 74. For proprietary information, see the text. samples; 18/38 positive CISH results). A possible explanation for this finding is the increased likelihood of finding a needle in a haystack when you know where to look, ie, nuclear localization in cytomorphologically abnormal cells might lend a practical sensitivity to the technique. The slight difference in probe cocktails of the 2 methods (CISH includes HPV type 70 but not 59; HC II includes type 59 but not 70) also might account for some variance in positivity. Interpretive overdiagnosis (CISH-only false-positive results) also might explain some of these results. Alternatively, an unequal distribution of lesional cells in 1 aliquot of a sample vs another portion might partly explain this finding. Given the known epidemiology of cervical preneoplasia, 28 it is not entirely surprising that in our series, patients in the younger than 30 years and the 30- to 39-yearold age groups had a higher likelihood of a positive test result by either method than patients in the group 40 years or older. These trends were statistically significant with respect to HC II results and not with respect to CISH results (Table 2). These trends fit with the idea that HPV, a sexually transmitted agent, is present at higher frequencies in younger persons. The absence of statistical significance with the CISH method might relate to the comparatively smaller number of positive results in all age distributions. Statistical significance of these trends might or might not be achieved with a larger sample number. © American Society for Clinical Pathology Anatomic Pathology / ORIGINAL ARTICLE ❚Table 4❚ Observed Probabilities for Positive CISH Results by Age and Sequence* Sequence No. of Observations Age (y) First Second CISH First in Sequence CISH Second in Sequence Total (N = 401) <20 20-29 30-39 40-49 50-59 60-69 70-79 >79 20.0 12.7 7.1 10.9 4.2 16.7 0.0 — 50.0 11.6 8.8 7.9 0.0 0.0 0.0 0.0 5 63 28 64 24 12 3 0 2 69 57 38 23 7 5 1 7 132 85 102 47 19 8 1 * Positive samples contained high-risk human papillomavirus DNA. Sequence data are given as percentages. In group 1 (n = 199), samples underwent chromogenic in situ hybridization (CISH) followed by Hybrid Capture (HC) II testing; in group 2 (n = 202), samples underwent HC II testing followed by CISH. For proprietary information, see the text. ❚Table 5❚ Observed Probabilities for Positive HC II Results by Age and Sequence* Sequence No. of Observations Age (y) First Second <20 20-29 30-39 40-49 50-59 60-69 70-79 >79 100.0 40.6 26.3 7.9 21.7 14.3 0.0 0.0 40.0 31.7 7.1 6.3 4.2 0.0 0.0 — * HC II First in Sequence HC II Second in Sequence Total (N = 401) 5 63 28 64 24 12 3 0 7 132 85 102 47 19 8 1 2 69 57 38 23 7 5 1 Positive samples contained high-risk human papillomavirus DNA. Sequence data are given as percentages. In group 1 (n = 199), samples underwent chromogenic in situ hybridization (CISH) followed by Hybrid Capture (HC) II testing; in group 2 (n = 202), samples underwent HC II testing followed by CISH. For proprietary information, see the text. An intriguing finding in our series was the effect of sequence on testing outcomes. Regardless of patient age or testing method, samples were more than 1.5 times as likely to receive a positive test result from the first aliquot than from the second aliquot, ie, the first ancillary test in the sequence was more likely to be positive than the second ancillary test performed on the same liquid-based sample. This observation was not merely a trend but a statistically significant difference with a P value of .003 (Table 1). Of particular interest is that the effect of sequence was seen more dramatically in HC II results than in CISH results, ie, the comparative decrease in the number of positive results between the first and second aliquots was greater for HC II than for CISH. The noted decrease in positive results as more liquid sample was removed from the specimen vials might be explained by nonhomogeneous cell suspensions or by preferential separation of pertinent cellular material by the proprietary filtration process. Keeping in mind that all HC II second aliquots came from samples that already had 2 ThinPrep slides prepared from them (1 for cytologic diagnosis and 1 for CISH), the cellularity of the sample might be a limiting factor in sensitivity if an attempt is made at performing multiple ancillary tests from 1 vial. Our study is somewhat limited by design flaws, the most important of which is the imperfect randomization used in establishing the crossover groups. The use of data from the clinically ordered HC II tests (group 2 samples) was done to minimize reagent cost. This resulted in a slightly different patient population in group 1 than in group 2, as evidenced by the slightly differing mean ages in the 2 groups (group 1, 38.7 years; group 2, 36.9 years). The fact that these patients had clinically ordered HPV testing might indicate a higher index of suspicion by their health care providers. Another limitation of study design is the fact that both test manufacturers (Digene and Ventana) recommend that their tests be performed within 21 days of sample collection. These recommendations are made because of the concern that cellular degeneration over time might decrease the sensitivity of both tests. Approximately 75% of our 802 data points were obtained from specimens older than 21 days (maximum 219 days). This delay in processing is an admitted flaw and is not reflective of “real world” practices. In addition, 2 of the CISH-negative control slides, prepared from cytologically negative cervicovaginal patient samples, each showed a single Am J Clin Pathol 2004;121:537-545 © American Society for Clinical Pathology 543 DOI: 10.1309/13NMAK8J3N1YJXU1 543 543 Schiller et al / HPV TESTING: HC II VS CISH focus of seemingly convincingly positive nuclear staining. Commercially dispensed known negative controls were not available. Last, our overall ASC-US high-risk HPV positivity rate, in the low 20th percentile range, is lower than what might be expected in some centers. This is thought to be secondary to a comparatively low frequency of disease in our suburban, relatively affluent patient population and not to represent potential compromise in the patient samples. Our overall laboratory atypia (ASC-US and higher) rate falls in the 8% range, and our ASC-US rate falls in the 4% range, resulting in an ASC-US/squamous intraepithelial lesion ratio of approximately 1:1. While this might mean that the overall percentage of HPV positivity in our specific population might be lower than in some other centers, we believe that our data truly reflect our population. According to the recently released Bethesda System guidelines and the American Society for Colposcopy and Cervical Pathology recommendations for management,19 HPV testing is the preferred triage mechanism for liquidbased cervicovaginal cytology samples that have been labeled cytomorphologically as ASC-US. This confined use of HPV testing underscores the important “ancillary” nature of HPV testing and its use as an adjunct to cytomorphologic examination. The goal of the present study was to compare 2 HPV DNA detection methods; however, these data would be best interpreted by comparison with the current clinically available gold standard of cytohistologic correlation and with ultrasensitive DNA detection techniques such as PCR. It is our goal, after a window of time for collection of correlative data, to study sensitivities, specificities, and predictive values of HC II and CISH for the detection of HPV DNA and morphologically documented preneoplastic and malignant changes. The presence of HPV genetic material is not by itself indicative of cervical disease, and some testing methods might prove too sensitive for routine clinical use. From the 1Department of Pathology, Evanston Northwestern Healthcare, Evanston Hospital, and Northwestern University Feinberg School of Medicine; and 2Center on Outcomes, Research and Education (CORE), Evanston Northwestern Healthcare, Evanston, IL. Presented in part in poster form (abstract 355) at the meeting of the United States and Canadian Academy of Pathology, Washington, DC, March 2003. Address reprint requests to Dr Sturgis: ENH Director of Cytopathology, 2650 Ridge Ave, Evanston, IL 60201. References 1. Papanicolaou GN, Traut HF. The diagnostic value of vaginal smears in carcinoma of the uterus. Am J Obstet Gynecol. 1941;42:193-206. 544 544 Am J Clin Pathol 2004;121:537-545 DOI: 10.1309/13NMAK8J3N1YJXU1 2. Papanicolaou GN, Traut HF. Diagnosis of Uterine Cancer by the Vaginal Smear. New York, NY: Commonwealth Fund; 1943. 3. Nowell PC, Hungerford DA. A minute chromosome in human granulocytic leukemia. Science. 1960;132:1197. 4. Harris NL, Jaffe ES, Diebold J, et al. The World Health Organization classification of hematological malignancies report of the clinical advisory committee meeting, Airlie House, Virginia, November 1997. Mod Pathol. 2000;13:193207. 5. Hutchinson ML, Agarwal P, Denault T, et al. A new look at cervical cytology: ThinPrep multicenter trial results. Acta Cytol. 1992;36:499-504. 6. Wilbur DC, Cibas ES, Merritt S, et al. ThinPrep Processor: clinical trials demonstrate an increased detection rate of abnormal cervical cytologic specimens. Am J Clin Pathol. 1994;101:209-214. 7. Schneider A, Meinhardt G, De-Villiers EM, et al. Sensitivity of the cytologic diagnosis of cervical condyloma in comparison with HPV-DNA hybridization studies. Diagn Cytopathol. 1987;3:250-255. 8. Stoler MH, Schiffman M, ALTS Group. Interobserver reproducibility of cervical cytologic and histologic interpretations: realistic estimates from the ASCUS-LSIL Triage Study. JAMA. 2001;285:1506-1508. 9. Chhieng DC, Talley LI, Roberson J, et al. Interobserver variability: comparison between liquid-based and conventional preparations in gynecologic cytology. Cancer. 2002;96:67-73. 10. Park IA, Lee SN, Chae SW, et al. Comparing the accuracy of ThinPrep Pap tests and conventional Papanicolaou smears on the basis of the histologic diagnosis: a clinical study of women with cervical abnormalities. Acta Cytol. 2001;45:525-531. 11. Bernstein SJ, Sanchez-Ramos L, Ndubisi B. Liquid-based cervical cytologic smear study and conventional Papanicolaou smears: a metaanalysis of prospective studies comparing cytologic diagnosis and sample adequacy. Am J Obstet Gynecol. 2001;185:308-317. 12. Monsonego J, Autillo-Touati A, Bergeron C, et al. Liquidbased cytology for primary cervical cancer screening: a multicentre study. Br J Cancer. 2001;84:360-366. 13. Diaz-Rosario LA, Kabawat SE. Performance of fluid-based, thin-layer Papanicolaou smear method in the clinical setting of an independent laboratory and an outpatient screening population in New England. Arch Pathol Lab Med. 1999;123:817-821. 14. Papillo JL, Zarka MA, St John TL. Evaluation of the ThinPrep Pap test in clinical practice: a seven-month 16,314case experience in northern Vermont. Acta Cytol. 1998;42:203-208. 15. Linder J, Zahniser D. The ThinPrep Pap test: a review of clinical studies. Acta Cytol. 1997;41:30-38. 16. Limaye A, Connor A, Huang X, et al. Comparative analysis of conventional Papanicolaou tests and a fluid-based thinlayer method. Arch Pathol Lab Med. 2003;127:200-204. 17. Solomon D, Schiffman M, Tarone R. Comparison of three management strategies for patients with atypical squamous cells of undetermined significance: baseline results from a randomized trial. J Natl Cancer Inst. 2001;93:293-299. 18. Sherman ME, Schiffman M, Cox JT. Effects of age and human papilloma viral load on colposcopy triage: data from the randomized Atypical Squamous Cells of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesion Triage Study (ALTS). J Natl Cancer Inst. 2002;94:102-107. © American Society for Clinical Pathology Anatomic Pathology / ORIGINAL ARTICLE 19. Wright TC, Cox JT, Massad LS, et al. 2001 consensus guidelines for the management of women with cervical cytological abnormalities. JAMA. 2002;287:2120-2129. 20. Manos MM, Kinney WK, Hurley LB, et al. Identifying women with cervical neoplasia using human papillomavirus DNA testing for equivocal Papanicolaou results. JAMA. 1999;281:1605-1610. 21. Digene HPV DNA Test Hybrid Capture II [package insert]. Gaithersburg, MD: Digene; 2000. 22. ISH iView Blue Detection Kit [package insert]. Tucson, AZ: Ventana; 2002. 23. INFORM HPV Liquid-Based Prep High-Risk Probe [package insert]. Tucson, AZ: Ventana; 2002. 24. HPV LBP High-Risk Positive Specimen Slides [package insert]. Tucson, AZ: Ventana; 2002. 25. Menezes G, Euscher E, Schwartz B, et al. Utility of the in situ detection of HPV in Pap smears diagnosed as within normal limits. Acta Cytol. 2001;45:919-926. 26. Hardin JW, Hilbe JM. Generalized Estimating Equations. Boca Raton, FL: Chapman & Hall/CRC; 2003. 27. Ferlay J, Bray F, Pisani P, et al. GLOBOCAN 2000: Cancer Incidence, Mortality and Prevalence Worldwide. Version 1.0. IARC Cancer Base No. 5. Lyon, France: IARC Press; 2001. Limited version available at: http://www-dep.iarc.fr/globocan/ globocan.htm. Accessed February 18, 2003. 28. Munoz N. Human papillomavirus and cancer: the epidemiological evidence. J Clin Virol. 2000;19:1-5. Am J Clin Pathol 2004;121:537-545 © American Society for Clinical Pathology 545 DOI: 10.1309/13NMAK8J3N1YJXU1 545 545






© Copyright 2026