
CONTENTS EXPLANATION OF CHARGES “TIME SPENT”: . . . . . ....
Ms. Marie Perriott i CONTENTS EXPLANATION OF CHARGES “TIME SPENT”: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 IDENTIFICATION: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 DESCRIPTION: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 CURRENT COMPLAINTS: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 ACTIVITIES OF DAILY LIVING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 HISTORY OF THE PRESENT ILLNESS: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 EDUCATIONAL/OCCUPATIONAL HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 PAST PSYCHIATRIC HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 PAST MEDICAL HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 FAMILY HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 DEVELOPMENTAL HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 SOCIAL HISTORY: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 RESULTS OF PSYCHOLOGICAL TESTING: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Hamilton Depression Rating Scale: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Hamilton Anxiety Rating Scale: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Rey 15-Item Memorization Test and Rey Dot Counting Test: . . . . . . . . . . . . . . . . . . . . 12 REVIEW OF MEDICAL RECORDS: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 1) Various Dates: Series of Doctor’s First Report of Occupational Injury or Illness by Various Providers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 2) 2/23/91: Emergency Room Record by [illegible], Queen of the Valley Hospital. . . . 14 3) Various Dates: Series of MRI Reports by Various Providers. . . . . . . . . . . . . . . . . . . . 15 4) Various Dates: Series of Reports by Thomas O. Bryan, M.D., Diplomate, American Board of Orthopaedic Surgery, Clinical Assistant Professor of Orthopaedics, University of Southern California School of Medicine, Metcalf Orthopaedic Medical Group, Inc. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 5) Various Dates: Series of Operative Reports by Various Providers. . . . . . . . . . . . . . . 24 6) Various Dates: Series of Progress Notes by Various Providers, Bergman Medical. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 7) Various Dates: Series of Radiology Reports by Various Providers. . . . . . . . . . . . . . . 25 8) Various Dates: Series of PR-2 Progress Report/Industrial Records by Philip Baily, M.D., Presbyterian Intercommunity Hospital. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 Ms. Marie Perriott ii 9) Various Dates: Series of Non-Certification Letters by Various Providers, Concentra. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 10) 11/07/07: Agreed Medical Reexamination by Lawrence A. Feiwell, M.D., Diplomate of the American Board of Orthopaedic Surgery, Fellow of the American Academy of Orthopaedic Surgery, The Greater Long Beach Orthopaedic Surgical and Medical Group. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 11) Various Dates: Series of Office Notes by Various Providers, Inland Region Medical Group. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32 12) Various Dates: Series of Application for Adjudication of Claim. . . . . . . . . . . . . . . . 32 13) Various Dates: Series of Reports by Hamid Rahman, M.D., Orthopedic Sports & Spine Medical Group. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 14) 7/15/09: Electrodiagnostic Studies Report by Aaron Coppelson, M.D., Diplomate of the American Board of Electrodiagnostic Medicine, Physical Medicine & Rehabilitation, & Pain Management, Restore Medical Group. . . . . . . . . . . . . . . . . . . . . . . . . . . 35 15) Various Dates: Series of Depositions of Marie Perriott. . . . . . . . . . . . . . . . . . . . . . . 35 16) Various Dates: Series of Reports by Scott Goldman, M.D., Board Certified Orthopedic Surgeon. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38 17) 7/11/11: Notification of Non-Certification by Rosalyn Beaty, M.D., Coventry. . . . . 40 18) Various Dates: Series of Secondary Treating Physician’s Progress Reports by Thomas K. Donaldson, M.D. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40 19) Various Dates: Series of Clinic Notes by Gail Maloff, L.M.F.T., Perry Maloff, M.D., & Associates. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41 20) Various Dates: Series of Reports by Luigi F. Galloni, M.D. . . . . . . . . . . . . . . . . . . . 42 21) Various Dates: Series of Secondary Treating Physician’s Progress Reports by Thomas K. Donaldson, M.D., Empire Orthopedic Center. . . . . . . . . . . . . . . . . . . . . . . . . 46 DIAGNOSIS: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47 SUMMARY AND CONCLUSIONS: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48 Temporary Disability: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Permanent and Stationary: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Causation: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Medical Care: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Ability to Work: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 Discussion of Apportionment: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 RESEARCH FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51 MEDICAL-LEGAL DISCLOSURE INFORMATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64 November 9, 2012 Janet John, Esq. DEFENSE ATTORNEY LAW OFFICE 801 S. Figueroa Street, 15th Floor Los Angeles, CA 90017 Robert C. Eckl, Esq. APPLICANT ATTORNEY 8291 Utica Ave., #101 Rancho Cucamonga, CA 91730 RE: Employee: Employer: D/Injury: Claim No.: Date of Service: Marie Perriott Rose Hills Company 2/12/2009 000731-028715 October 24, 2012 AGREED MEDICAL EVALUATION REPORT Dear Ms. John and Mr. Eckl: This evaluation consisted of a psychiatric history, mental status examination, review of medical records and the administration of five psychological tests: the Hamilton Depression Rating Scale, the Hamilton Anxiety Rating Scale, the Minnesota Multiphasic Personality Inventory-2, the Rey 15-Item Memorization Test, and the Rey Dot Counting Test. The entire interview was conducted by me and dictated in its entirety by me as well. Ms. Perriott was evaluated for a full session, which lasted approximately one hour, during which I obtained all of the information in the report, including current complaints, history of present illness, past history, and mental status examination. In addition to this period of time during which I elicited the necessary clinical information, additional time was spent in the administration, scoring and interpretation of the psychological tests. None of this time was part of the interview. When Ms. Perriott left, it was explicit and apparent that she had provided a full account of the substance of her alleged problems, which is contained herein. The Hamilton Depression Rating Scale and the Hamilton Anxiety Rating Scale were administered by me. The Minnesota Multiphasic Personality-2 (MMPI-2) was scored and interpreted by Alex B. Caldwell, Ph.D. and is attached to this report. The Rey 15-Item Memorization Test and the Rey Dot Counting Test were scored and interpreted by Carla Back-Madruga, Ph.D., Clinical and Neuropsychologist, and the results were reviewed by me. The medical records were reviewed by me. Proofreading was done by my office staff. Ms. Marie Perriott November 9, 2012 Page 2 The evaluation was in compliance with the guidelines established by the Industrial Medical Council or the administrative director pursuant to paragraph (5) of subdivision (j) of Section 139.2 or Section 5307.6 of the Labor Code. EXPLANATION OF CHARGES “TIME SPENT”: This case is billed as an Agreed Medical Evaluation Report. Breakdown of hours for the CPT 96100 is the following: Hamilton Depression Rating Scale: . . . . . . . . . . . . . . . . . . . . 45 minutes Hamilton Anxiety Rating Scale: . . . . . . . . . . . . . . . . . . . . 45 minutes Rey 15-Item Memorization Test . . . . . . . . . . . . . . . . . . . . 30 minutes Rey Dot Counting Test: . . . . . . . . . . . . . . . . . . . . . . . . . . 30 minutes Minnesota Multiphasic Personality Inventory-2: . . . . . . . . . . . 120 minutes Total hours for testing: . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.5 hours Face-to-face . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 hour Record Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.25 hours Report Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.5 hours Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.5 hours Activities of Daily Living . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45 minutes TOTAL TIME SPENT: . . . . . . . . . . . . . . . . . . . . . . . 25.5 HOURS Ms. Marie Perriott November 9, 2012 Page 3 Ms. Perriott is a 62-year-old woman who was seen in my Riverside office on October 24, 2012 for the purpose of an agreed medical evaluation. IDENTIFICATION: Ms. Perriott was born on May 19, 1950. She reports the date of the alleged injury as February 12, 2009. She states that she last worked at the job to which this claim pertains on May 7, 2012. She is currently not working. The following questions are addressed in this report: 1) Has Ms. Perriott ever been psychiatrically injured on an industrial basis? 2) Is Ms. Perriott permanent and stationary, and, if so, what is the rating? 3) What, if any, are the factors of apportionment? 4) Does Ms. Perriott require any psychiatric treatment on an industrial basis? DESCRIPTION: Ms. Perriott is wearing a casual striped shirt, melon-colored capri pants, brown sandals, and eye glasses. She is also wearing a back brace for support. She describes herself as 5'7" tall, weighing 210 pounds, with dark brown hair and brown eyes. There is no evidence of any psychomotor retardation or agitation. She speaks fluently and understands everything said to her. She is generally pleasant and cooperative throughout the interview. Ms. Marie Perriott November 9, 2012 Page 4 CURRENT COMPLAINTS: In regard to her emotional symptoms, she reports stress due to no income, fatigue, and depression. “My depression started after I was told that back surgery wouldn’t help me. I feel sad most of the time because I can’t do anything and I don’t have any income.” She denies crying spells. She reports insomnia. “I go to bed at 11:00 PM but it takes me a half hour to one hour to fall asleep. I wake up several times at night due to pain. In the morning, I wake up around 7:30 AM.” She does not have nightmares. Her appetite is fair but she has gained approximately 20 pounds in the past three years. Her energy level is poor. She is not sexually active at this time. She reports that her memory and concentration are “okay.” She denies anhedonia, which is an inability to enjoy life stating, “I love to read my Bible.” She is not able to finish her routine chores and responsibilities. According to Ms. Perriott, her overall mood is sad, worried, troubled, and sometimes irritable. Ms. Perriott was asked if she was able to work at this time. She replied, “No, I cannot work because I cannot sit up, drive, or walk for long periods of time due to back pain. Also, I don’t sleep well at night.” ACTIVITIES OF DAILY LIVING Self Care: Ms. Perriott finds that self care activities are uncomfortable and are done slowly. She has difficulty with cooking, laundry, housekeeping or shopping a lot or most of the time. Physical Activities: Ms. Perriott is able to perform very light activities for a period of 2 minutes, can only lift and carry very light objects and has some difficulty reaching and grasping items off a shelf at chest level. She finds some difficulty with reaching and grasping items off an overhead shelf. She can push or pull very Ms. Marie Perriott November 9, 2012 Page 5 light objects, has no difficulty with gripping, grasping, holding and manipulating objects with her hands and also experiences no difficulty with repetitive motions such as typing on a computer. Ms. Perriott has some difficulty with forceful activities that include her arms and hands. She has found that there has been no sexual functioning because of her injury and she cannot do any work at all. Sensory Functionality: Ms. Perriott notes that there has been no change in her sense of touch, writing, typing, seeing, hearing, speaking, tasting and smelling abilities. Movement Abilities: Ms. Perriott finds she can only walk short distances. She notes a lot of difficulty climbing one flight of stairs, can only sit for a period of less than 15 minutes at a time and can only stand/walk for a period of 15 to 30 minutes at a time. She finds she has a lot of difficulty with kneeling, bending or squatting. Sleeping Functions: Ms. Perriott notes that her sleep is greatly disturbed, experiencing 3 - 5 sleepless hours. Pain Interference: Ms. Perriott indicates that on average during the past week her pain has been at a level of 8/10 and that at its worst during that same period it was at a level of 10/10. She reports moderate pain most of the time and rates her pain at the moment as severe. She notes that her pain interferes all of the time with her ability to travel and with her engagement in social and recreational activities. A lot or most of the time her pain affects her concentrating and thinking as well as causes her emotional distress with depression or anxiety. Ms. Perriott has indicated that areas of the body that hurt due to her pain are: neck and lower back. Ms. Marie Perriott November 9, 2012 Page 6 Self Analysis: Ms. Perriott indicates that she is afraid that if she exercises she will injure herself; that her body is telling her she has something dangerously wrong and that her injury has put her body at risk for the rest of her life. She feels that resting is the best thing she can do to prevent more pain and injury; that it’s really not safe for her to be physically active; that she can’t do much because it’s too easy for her to get injured and that no one should have to exercise when they are in pain. Ms. Perriott believes that there is little hope for her at this point and she would rather be left alone. HISTORY OF THE PRESENT ILLNESS: Ms. Perriott began working for Rose Hills Co. as a memorial service counselor on October 6, 2003. She reports that she injured herself at work on February 12, 2009. “I was driving back to the office from a presentation and I was making a left-hand turn on a left arrow, when I saw an oncoming van so I stopped my vehicle but the van hit the front end of the passenger side of my car. I injured my lower back and right hip.” Ms. Perriott reported the job injury to her supervisor. However, she became ill with the flu so she was off work for two weeks. She went to her primary care physician, Dr. Cecilio; however, he told her it was a job injury and he could not treat her. She then went to another primary care physician, Dr. Boozer, and was again told that it was a work-related injury. Her supervisor sent her to Presbyterian Intercommunity Hospital emergency room on May 29, 2009, where she saw a physician assistant, Dave Weitzel, who prescribed pain medication and treated her with physical therapy. She was sent to the company physician at Health Works and was given an injection for pain. Ms. Perriott went back to work with job restrictions. Subsequently, she consulted an attorney and was sent to Dr. Rahman, who took her off work. Her last day of work was on May 7, 2012. He sent her for a nerve conduction test, got x-rays and an MRI on her, treated her with physical therapy and acupuncture and prescribed unspecified medication for her. Later, Ms. Perriott changed to Dr. Goldman, an orthopedist, who got x-rays and an MRI Ms. Marie Perriott November 9, 2012 Page 7 on her. He prescribed various pain medications including Percocet, Morphine, and Celebrex. He also gave her Omeprazole. He treated her with physical therapy. She was sent to Dr. Laderhaus, an orthopedist, for an evaluation. He told Ms. Perriott that he did not recommend back surgery. Ms. Perriott saw a pain management specialist, Dr. Rho, who gave her an epidural injection. She was referred to another orthopedist, Dr. Samuderale, who also told her that he did not recommend back surgery. “That put me in a depression because there was nothing they could do for my back pain,” according to Ms. Perriott. She reports that she developed left shoulder pain because “I couldn’t lie on my right side due to right hip pain.” She was sent to a psychiatrist, Dr. Maloff, because “I was depressed.” Dr. Maloff offered to prescribe medication for her but she declined to take the medication. She was referred to a therapist, Gail Maloff, for individual psychotherapy sessions. She saw an AME orthopedist, Dr. Chong, twice for an evaluation. She has another appointment for reevaluation with Dr. Chong on November 16, 2012. According to Ms. Perriott, she went to San Antonio Hospital emergency room due to shortness of breath, hot flashes, and lightheadedness. She was told that she was “okay.” She was then referred to a cardiologist who did an EKG on her and told her that it was normal, so she was clear for surgery. She was referred to Dr. Goldman who got an MRI on her right hip. He sent her to Dr. Donaldson, an orthopedist, who performed a total right hip replacement surgery on her on March 6, 2012. She was then sent to a nursing home for three weeks and was treated with postoperative physical therapy. Dr. Donaldson prescribed Robaxin and Vicodin for her. Ms. Perriott changed physicians and began seeing Dr. Galloni, an orthopedist, who treated her with physical therapy. He is currently prescribing Naproxen for her. She was sent to a pain management specialist, Dr. Anguizola, who is prescribing topical creams for her. He told Ms. Perriott that he wanted to give her a facet block injection. In regard to her current physical complaints, Ms. Perriott reports right hip pain, headaches and lower back pain that radiates down her right leg. Ms. Marie Perriott November 9, 2012 Page 8 She is taking the following medications: 1. Hydrocodone. 2. Naproxen. 3. Amitriptyline. 4. Flurbiprofen. 5. Mometasone. 6. Desonide. EDUCATIONAL/OCCUPATIONAL HISTORY: Ms. Perriott graduated from Huntington High School. She has held the following positions: 2003 - 2012: Rose Hills Co./Memorial Service Counselor 2002 - 2003: Big Lots/Bookkeeper Undated: WMA Securities/Field Compliance Officer Undated: WMA Securities/Office Manager Undated: B. Ghosh, M.D./Office Manager Undated: A. Vargas, M.D./Office Manager Ms. Marie Perriott November 9, 2012 Page 9 1983 - 1984: LAPD/Recruit Officer Excluding this claim, Ms. Perriott reports that she lost substantial time from work, while employed at Rose Hills Company in 2007 after a right shoulder surgery. She also sustained injury to her low back while working for the LAPD in 1983. She also broke her right hand finger in 1976. PAST PSYCHIATRIC HISTORY: With the exception to this claim, she has never seen a psychiatrist, psychologist or mental health professional in the past. She has never been treated for a psychiatric or emotional problem either on an inpatient or outpatient basis. PAST MEDICAL HISTORY: She reports the following medical and/or surgical problems: 1. 2. 3. Right rotator cuff surgery in 2007. Low back injury in 1983. Broken right hand finger in 1976. She returned to Dr. Boozer, her primary care physician, because she had asthma and shortness of breath. Dr. Boozer referred her to a pulmonary specialist who prescribed an inhaler for her. According to Ms. Perriott, she developed a dermatitis on her hands and scalp so Dr. Boozer referred her to a dermatologist who diagnosed her with eczema and prescribed topical creams for her. FAMILY HISTORY: Ms. Perriott states she was born in Los Angeles, California. Ms. Marie Perriott November 9, 2012 Page 10 She reports that her parents were married. Her 84-year-old father passed away in 2002 and her 79-year-old mother passed away from leukemia. She has four brothers, ages 71, 68, 55, and 53 and one deceased brother. She also has four sisters, ages 73, 71, 60, and 58. Her relationship with her family is close. She is unaware of anyone in her family having past psychiatric problems. No one in her family has a history of alcohol, drugs, or gambling. Ms. Perriott has been married twice. She first married at the age of 18 and divorced when she was 21. She remarried at age 25 and divorced at age 27. She has a 42-year-old son and 37-year-old daughter. Both of her children are healthy. DEVELOPMENTAL HISTORY: As far as she can recall, Ms. Perriott states that she reached all of her developmental milestones including sitting up, standing up, walking, talking, being toilet trained and attending the first day of school without difficulties and within the normal time limits. She further says that she cannot recall having any problems learning to read, write, calculate or perform fine sensorimotor tasks. She does not believe that she was ever told that she had a developmental, congenital, familial, genetic or sensorimotor disorder. SOCIAL HISTORY: She comments that her interests and hobbies include bible studies and karaoke. She has not been able to go to church since her disability; however, she watches services at home. She states her two divorces were difficult for her. She filed a Workers' Compensation claim in 1983 for a low back injury and another claim in 2007 for a right shoulder injury. She underwent right shoulder surgery and both cases are settled. She denies ever filing a Personal Injury claim. Ms. Marie Perriott November 9, 2012 Page 11 She denies any problems with alcohol, illicit drugs, or gambling. Furthermore, she has never had any criminal charges placed against her. MENTAL STATUS EXAMINATION: Behavior/Demeanor: Casually attired, Ms. Perriott shows no evidence of psychomotor retardation or agitation. There is no suggestion of any abnormalities of manner. She relates well to the examiner and is cooperative throughout the interview. Speech/Language: Ms. Perriott is articulate. Her speech is fluent, and has good prosody, repetition and spontaneity. There is no suggestion of aphasia, apraxia, anomia or agnosia. Affect/Mood: Her mood is bland and her affect blunted. Cognition: There are no signs of hallucinations, delusions, tangentiality, circumstantiality, autism, or ideas of reference. There are no manifestations of loose associations, pressured speech, obsessive ruminations or flight of ideas. Ms. Perriott is oriented to time, place, and person, and her memory for recent and remote events is intact. Ms. Perriott's insight into herself is fair and her judgment is fair. Her intelligence is average. Physiologic: There is no suggestion of conversion reaction or excessive autonomic discharge in Ms. Perriott. There is no manifestation of marked diaphoresis, pallor or flushing of the skin. Ms. Marie Perriott November 9, 2012 Page 12 RESULTS OF PSYCHOLOGICAL TESTING: Ms. Perriott was administered the Hamilton Depression Rating Scale, the Hamilton Anxiety Rating Scale, the Rey 15-Item Memorization Test and the Rey Dot Counting Test. Hamilton Depression Rating Scale: On the Hamilton Depression Rating Scale, Ms. Perriott received a score of 8 out of a possible 61 points, indicating slight symptomatology indicative of a possible depressive disorder. Hamilton Anxiety Rating Scale: On the Hamilton Anxiety Rating Scale, Ms. Perriott obtained a score of 4 out of a possible 56 points, indicating minimal symptomatology suggestive of a possible anxiety disorder. Rey 15-Item Memorization Test and Rey Dot Counting Test: The Rey 15-Item Memorization Test and the Rey Dot Counting Test were scored and interpreted by Carla Back-Madruga, Ph.D., Clinical and Neuropsychologist. These tests are designed to evaluate the veracity of claims by patients that their cognitive ability is decreased. Research has indicated that individuals who fake or exaggerate memory or other impairments tend to display responses which are quantitatively and qualitatively different from those of actual brain-injured individuals with true cognitive impairment. The use of these two tests in conjunction with other tests designed to evaluate malingering have been fruitful in identifying patients who were not truly impaired cognitively, and were either exaggerating or fabricating their symptoms. Boone KB, Savodnik I, Ghaffarian S, Lee A, Freeman D, Berman N. Rey 15Item Memorization and Dot Counting scores in a "stress" claim Workers' Compensation population: Relationship to personality (MCMI) scores. Journal of Clinical Psychology, May 1995, Vol. 51, No. 3. Ms. Marie Perriott November 9, 2012 Page 13 Ms. Perriott passed the measures, suggesting that she probably was not attempting to malinger cognitive deficits. REVIEW OF MEDICAL RECORDS: 1) Various Dates: Series of Doctor’s First Report of Occupational Injury or Illness by Various Providers. The records were dated from [Undated] to 7/08/09. [Undated] by [illegible], Galloni Enterprises Medical Group, Inc.: Date of Injury: 2/19/09. Ms. Perriott had an automobile accident while working with Rose Hills. She injured her low back, right hip, left shoulder, and right groin area. She complained of pain in the right hip and left shoulder. DIAGNOSIS: 1. OA AC joint. 2. OA LS severe. 3. OA right hip [illegible]. She was to have hip surgery on 3/06/12. 7/08/09 by Hamid Rahman, M.D., F.A.C.S.: Date of Injury: 2/12/09. Ms. Perriott was involved in a motor vehicle accident while returning to her place of employment. She complained of constant aching pain in her low back and right hip. Ms. Marie Perriott November 9, 2012 Page 14 DIAGNOSIS: 1. Musculoligamentous strain/sprain lumbar spine. 2. Right hip strain. 3. Greater trochanteric bursitis. 4. Insomnia. Authorization was requested for MRI of the lumbar spine and right hip. She was referred for physical therapy and acupuncture. 2) 2/23/91: Emergency Room Record by [illegible], Queen of the Valley Hospital. Ms. Perriott had an industrial injury to her back in 1983. Apparently she was injured while wrestling at work. She worked for the LAPD as a recruit officer. She was eventually placed on partial permanent disability of 80%. She later returned to work as a medical office manager. She was doing relatively well until approximately one week ago when she began having back muscle spasms after cleaning a bathtub. She was at a friend’s house last night when she experienced very severe muscle spasms and was not able to get out of the car. The paramedics had to take her out of the car and bring her here by ambulance. She was unable to be ambulated and was admitted at this time for analgesia. ASSESSMENT: 1. Acute lumbar spasm. Rule out herniated disk. She was admitted for bedrest, MRI scan, and analgesia. She was to be gradually ambulated as tolerated and discharged when able to ambulate. Ms. Marie Perriott November 9, 2012 Page 15 3) Various Dates: Series of MRI Reports by Various Providers. The records were dated from 2/23/91 to 10/19/10. 2/23/91 by Robert Cohen, M.D., Valley Imaging Partnership: STUDY: MRI of the Lumbar Spine. IMPRESSION: 1. There are degenerative changes in the lower four lumbar discs. A combination of diffuse disc bulges and endplate osteophytes cause slight narrowing of the central canal and moderate narrowing of the neural foramina. There does not appear to be focal disc herniation on nerve root compression. 12/11/97 by Thomas R. Sanders, M.D., Valley Imaging Partnership: STUDY: MRI of the Lumbar Spine. IMPRESSION: 1. Slight to moderate disc bulges centrally at L2-3 and L3-4 with slight to moderate compression of the thecal sac. 2. Slight disc bulge at L4-5 and L5-S1 with slight compression of the thecal sac. 3. The disc bulges are slightly larger than on previous examination. Ms. Marie Perriott November 9, 2012 Page 16 1/28/99 by Gregory M. Henzie, M.D., Medical Diagnostic Associates: STUDY: MRI of the Lumbar Spine. IMPRESSION: 1. Disk dessication at L4-L5 with an approximately 2 mm disk bulge, most pronounced posterolaterally, left greater than right. There is mild to moderate foraminal narrowing bilaterally, left greater than right. 2. Disk desiccation and narrowing at L3-L4 with a small posterior osteophyte and minimal retrolisthesis of L3 on L4. There is mild foraminal narrowing bilaterally. 3. Mild to moderate disk desiccation at L5-S1 with mild facet hypertrophy. No central canal or foraminal stenosis is identified. 12/08/06 by James Shelby, M.D., San Gabriel Valley MRI: STUDY: MRI of the Shoulder without contrast. IMPRESSION: 1. Nonspecific tendinosis of the supraspinatus tendon. 2. A partial thickness type I SLAP lesion is suspected. 3. Possible small joint body within the subcoracoid recess measuring 3-4 mm. 4. Small joint effusion. Ms. Marie Perriott November 9, 2012 Page 17 STUDY: MRI of the Cervical Spine without contrast. IMPRESSION: 1. Areas of disc desiccation and degenerative change results in mild-to-moderate foraminal stenosis, particularly at C6-7, asymmetric to the left. 10/11/07 by Agustinus Suhardja, M.D., Medical Imaging Center of Huntington Beach: STUDY: MRI Arthrogram Right Shoulder. IMPRESSION: 1. Partial-thickness tear of the articular surface of the supraspinatus tendon 1.5 cm from the insertion site. 2. Amorphous partial tear of the superior labrum, posterior to the biceps labral anchor. The biceps labral anchor is intact. 3. Mild degenerative changes of the AC joint without significant impingement. 7/27/09 by Sim C. Hoffman, M.D., Diplomate, American Board of Radiology, Certified Specialist, American Board of Nuclear Medicine, Advanced Professional Imaging Medical Group: STUDY: Open MRI of the Lumbar Spine. Ms. Marie Perriott November 9, 2012 Page 18 IMPRESSION: 1. L2-L3 disc level shows a 2 to 3 mm posterior disc protrusion present. Hypertrophic facet changes are present. The neural foramina appear patent. There is no evidence of spinal stenosis. 2. L4-L5 disc level shows a 4 to 5 mm posterior disc protrusion present. Moderate hypertrophic facet changes are present. Lateral recess stenosis is present. 3. L5-S1 disc level shows a 2 mm posterior disc protrusion present. Spondylosis is present. Mild hypertrophic facet changes are present. The neural foramina appear patent. There is no evidence of spinal stenosis. STUDY: Open MRI of the Right Hip. IMPRESSION: 1. There is narrowing at the superior margin of the acetabularfemoral joint space. 2. There is no evidence of fracture or avascular necrosis. 9/29/09 by Scott Goldman, M.D.: STUDY: MRI of the Lumbar Spine. IMPRESSION: 1. Severe disc space narrowing at the L3-L4 level with a 4-5 mm disc protrusion at the L4-5 level. Ms. Marie Perriott November 9, 2012 Page 19 10/19/10 by David Dang, M.D., McKesson: STUDY: MRI of the Lumbar Spine without contrast. IMPRESSION: 1. Mild L2-L3 degenerative disc and moderate facet arthrosis with mild central and foraminal narrowing without significant nerve root compression. 2. Severe L3-L4 degenerative disc disease with chronic endplate changes and facet arthrosis. Moderate bilateral neural foraminal narrowings with deflection of the nerve roots. 3. Moderate to severe L4-L5 degenerative disc disease with facet arthrosis and moderate foraminal narrowing with deflection of exiting nerve roots. 4. Question 8-mm left renal cyst. Ultrasound evaluation is recommended. 4) Various Dates: Series of Reports by Thomas O. Bryan, M.D., Diplomate, American Board of Orthopaedic Surgery, Clinical Assistant Professor of Orthopaedics, University of Southern California School of Medicine, Metcalf Orthopaedic Medical Group, Inc. The records were dated from 3/08/91 to 4/22/08. 3/08/91: Orthopaedic Consultation. A history was obtained. A physical examination was performed. Ms. Perriott complained of mild low back muscle spasm and pain. Ms. Marie Perriott November 9, 2012 Page 20 DIAGNOSIS: 1. Spinal stenosis with degenerative changes of the lower four lumbar discs. Dr. Bryan felt Ms. Perriott had an exacerbation of her ongoing low back problem. The recommended treatment was for her to be continued on physical therapy and also continue the Naprosyn. She was to take Vicodin only as needed. She may continue to work at her usual job as a medical office manager. 4/16/91: Supplemental Report. Ms. Perriott stated that she was doing quite well overall. She had been going to therapy as needed. She was going three times a week but now had only gone once in the past two weeks. She had a near normal physical examination. She was to go to physical therapy only if needed. 10/29/91: Supplemental Report. Ms. Perriott reported for renewal of Darvocet and Naprosyn due to some increased low back discomfort. Medications were renewed. 11/18/91: Supplemental Report. Ms. Perriott reported that she was doing significantly better. The back was less tender and she had been able to work at her job as a medical office manager. It was felt she had resolution of the acute exacerbation of her low back pain. 5/19/93: Supplemental Report. Ms. Perriott reported that she had a flare-up over the past several days. She had been wearing a back brace which she had at home and had been using a heating pad. Most of the pain was in the left side of her back and also the left thigh felt “funny” when she went up stairs. She reported that she had not worked since June of 1992. Apparently she had been taking care of her nephew and received some Ms. Marie Perriott November 9, 2012 Page 21 compensation for this. She reported that this latest flare up of back pain occurred when she was getting ready for a birthday party and was doing a lot of bending, stooping, and lifting. DIAGNOSTIC IMPRESSION: 1. Recurrent lumbar strain. Recommended treatment was for her to begin a physical therapy treatment program. She was given medication refills. 2/02/94: Supplemental Report. Ms. Perriott reported she was doing well for approximately six months but now had a “flare up” for several days. She was uncertain what caused it. Upon physical examination, she appeared quite uncomfortable. DIAGNOSTIC IMPRESSION: 1. Acute flare up of chronic low back pain. Recommended treatment was for her to begin a short course of physical therapy for symptomatic relief. Medications were refilled. She was fitted with a lumbar corset. 11/29/06: Progress Report. Ms. Perriott complained of shoulder pain secondary to carrying a heavy briefcase over her shoulder for long periods of time. Physical therapy helped the shoulder a bit but exercises made the pain go down the left arm to the fingers. DIAGNOSES: 1. Rule out rotator cuff tear right shoulder. Ms. Marie Perriott November 9, 2012 Page 22 2. Rule out cervical disc syndrome. She was referred for an MRI of the right shoulder. She was returned to regular duty. 12/13/06: Progress Report. Ms. Perriott was here to go over the MRI results. She complained of right shoulder pain. DIAGNOSES: 1. Cervical disc bulges with foraminal stenosis. 2. Glenoid labral tear with impingement. She was referred for physical therapy. She was returned to modified work with restrictions of limited use of the right shoulder. 2/22/07: Letter to Angela Singh, Senior Claims Representative, Gallagher Bassett. Dr. Bryan was in receipt of the denial letter dated 2/15/07 regarding his authorization request for shoulder arthroscopy with debridement of glenoid labral tear and subacromial decompression. Ms. Perriott was treated conservatively initially, however she had continued pain and impingement. Dr. Bryan recommended that she undergo surgery to debride the torn labrum and also a subacromial decompression. Dr. Bryan noted that he would be happy to discuss Ms. Perriott’s case with a board-certified orthopedic surgeon. He felt that Ms. Perriott was an appropriate candidate for arthroscopic subacromial decompression and debridement of the torn glenoid labrum. She had physical therapy for her neck which had led to some improvement with the pain localizing more to the shoulder. Dr. Bryan felt that a steroid injection was unlikely to be of any benefit Ms. Marie Perriott November 9, 2012 Page 23 to Ms. Perriott and she did not want to have an injection performed. Dr. Bryan saw no reason to further delay or deny the surgery. 5/02/07: Progress Report. Ms. Perriott complained of increased fatigue and weakness. The pain to her shoulder had subsided. DIAGNOSIS: 1. Status post arthroscopy right shoulder debridement of torn glenoid labrum. 2. Chondroplasty of humeral head. She was referred for physical therapy. She remained off work for four weeks. 4/22/08: Primary Treating Physician’s Permanent and Stationary Report. Postoperatively, Ms. Perriott had continued to have some acromioclavicular joint pain and consideration at one point was given to performing an arthrocopic Mumford procedure. However, she had made some improvement. She still had some limitations. She used her other arm for most overhead activities as well as for repetitive pushing and pulling. DIAGNOSIS: 1. Status post arthroscopic surgery right shoulder with debridement of torn glenoid labrum, chondroplasty of the humeral head and arthroscopic subacromial decompression. There was no rateable disability by AMA Guidelines. It was Dr. Bryan’s medical opinion that Ms. Perriott injured her shoulder when she repetitively carried a heavy briefcase in the course of her duties at work. Apportionment did not appear to be a significant issue as she had no rateable disability at this time. Ms. Marie Perriott November 9, 2012 Page 24 She was returned to full, unrestricted duty. Future medical care may be required. She had significant chondroplasty of the humeral head and may require further evaluation including injections, MRI scans, and operative debridement. 5) Various Dates: Series of Operative Reports by Various Providers. The records were dated from 2/19/99 to 3/06/12. 2/19/99 by Richard Kennedy, M.D., Citrus Valley Medical Center: Preoperative diagnosis: 1. Lumbar disc disease with left-sided radiculopathy. Operation performed: 1. Selective left L4 foraminal block and selective left L5 foraminal block using fluoroscopy. The postoperative diagnosis was the same as the preoperative diagnosis. 4/23/07 by Thomas Bryan, M.D., Citrus Valley Medical Center: Preoperative diagnosis: 1. Torn glenoid labrum, right shoulder with impingement syndrome. Operation performed: 1. Arthroscopy of the right shoulder with debridement of torn glenoid labrum, chondroplasty of humeral head, arthroscopic subacromial decompression. Ms. Marie Perriott November 9, 2012 Page 25 Postoperative diagnosis: 1. Torn glenoid labrum, right shoulder, with dissecting chondromalacia of the humeral head and impingement syndrome with rotator cuff tendintis. 3/06/12 by Thomas K. Donaldson, M.D.: Preoperative diagnosis: 1. Degenerative arthritis of the right hip. Operation performed: 1. Right total hip arthroplasty. The postoperative diagnosis was the same as the preoperative diagnosis. 6) Various Dates: Series of Progress Notes by Various Providers, Bergman Medical. (Handwritten, Partially Illegible) The records were dated from 2000 to 2009. The assessments included: bronchitis; muscle spasm; asthma; right hip pain; acute pharyngitis. 7) Various Dates: Series of Radiology Reports by Various Providers. The records were dated from 5/11/04 to 3/29/12. Ms. Marie Perriott November 9, 2012 Page 26 5/11/04 by Andrea Mallet Reece, M.D., Diplomate, American Board of Radiology, Diagnostic Medical Group of Southern California: STUDY: Bilateral Mammogram. IMPRESSION: 1. Questionable visualization of an ill-defined left 3 o’clock nodule. 2. Recommend EFT compression mammography for any palpable abnormality involving either breast, ultrasound is recommended. 9/21/04 by Andrea Mallet Reece, M.D., Diagnostic Medical Group of Southern California: STUDY: Left Focal Compression Mammography and Left Breast Ultrasound. IMPRESSION: 1. The asymmetric 3 o’clock density seen in mammograms dated 5/11/04 appears stable and exhibits no ominous features in focal compression images. Suspect normal variation. 2. Incidental finding of an approximately 5 mm sized upper left breast nodule seen in the mediolateral oblique focal compression image, which was not seen in mammograms dated 5/11/04. This probably represents a 5 mm sized cyst seen by ultrasound dated 9/21/04. A 9 mm sized 2 o’clock cyst seen by ultrasound was occult by mammography. 3. ACR category: 2 (benign). Ms. Marie Perriott November 9, 2012 Page 27 8/07/06 by Andrea Mallet Reece, M.D., Diagnostic Medical Group of Southern California: STUDY: X-ray of the Right Shoulder. IMPRESSION: 1. No acute abnormalities are identified. Mild degenerative joint disease is noted. Soft tissues are unremarkable with no evidence of calcific tendonitis. 9/01/06 by Andrea Mallet Reece, M.D., Diagnostic Medical Group of Southern California: STUDY: Pelvic Ultrasound, Transabdominal. IMPRESSION: 1. Suboptimal study due to gas. 2. Normal uterus. 3. Nonvisualization of the ovaries. 10/12/06 by Merton L. Shew, M.D., Presbyterian Intercommunity Hospital: STUDY: X-ray of the Right Shoulder. IMPRESSION: 1. `` Normal right shoulder study. Ms. Marie Perriott November 9, 2012 Page 28 4/21/07 by Shaya Ghazinoor, M.D., Citrus Valley Medical Center: STUDY: X-ray of the Chest. IMPRESSION: 1. No acute cardiopulmonary process. 11/07/08 by Tan Tran, M.D., Whittier Imaging Center: STUDY: X-ray of the Chest. IMPRESSION: 1. Normal chest x-ray. 12/09/08 by Aldric Shim, M.D., Diplomate, American Board of Radiology, Diagnostic Medical Group of Southern California: STUDY: Mammography Bilateral Diagnostic. IMPRESSION: 1. BI-RADS Category 2 (benign finding). 5/11/09 by Spencer Silverback, M.D., Grove Diagnostic Imaging: STUDY: X-ray of the Lumbar Spine. Ms. Marie Perriott November 9, 2012 Page 29 IMPRESSION: 1. Multifocal disc degeneration with spondylosis. STUDY: X-ray of the Right Hip. IMPRESSION: 1. Negative study. 9/30/09 by Scott Goldman, M.D.: STUDY: X-ray of the Right Hip. IMPRESSION: 1. Mild osteoarthritis. 3/29/12 by Wayne R. Boyd, M.D.: STUDY: X-ray of the Right Hip. IMPRESSION: 1. Satisfactory total hip prosthesis. 8) Various Dates: Series of PR-2 Progress Report/Industrial Records by Philip Baily, M.D., Presbyterian Intercommunity Hospital. The records were dated from 9/21/06 to 10/24/06. Ms. Marie Perriott November 9, 2012 Page 30 9/21/06: Ms. Perriott stated that she had some improvement in her symptoms. She had started attending regular therapy sessions. She had been attempting to perform her regular duties at work, which were essentially sedentary in nature. DIAGNOSIS: 1. Status post right upper back strain (trapezius musculature). 2. Status post right upper arm strain. The plan was to continue with medications and cold pack. She was to continue physical therapy three times a week for the next two weeks. 10/12/06: Ms. Perriott stated that she had made some progress with regard to her right upper back complaints in that she was having only minimal complaints in that area at this time. She remained symptomatic, however, with regard to pain in the right arm and shoulder. It appeared in taking history from her that her right shoulder appeared to be more symptomatic than noted on the previous examination, where her right upper arm appeared to be the focus of her symptoms. DIAGNOSIS: 1. Status post right shoulder/upper arm strain. She was to continue with medications and the cold pack. She was to continue with her physical therapy treatment program three times a week for the next two weeks. 10/24/06: Ms. Perriott stated that she remained symptomatic with regard to pain in the area of the right shoulder. Current pain levels had actually increased to 6/10. For the past couple of weeks she had not been Ms. Marie Perriott November 9, 2012 Page 31 taking the Flexeril due to some family issues where she had to be available to help another family member at night. She had started back on the Flexeril in the last couple of days. DIAGNOSIS: 1. Status post right shoulder sprain (rule out rotator cuff injury). She was to continue with medications and physical therapy. She was referred to be seen by an orthopedic specialist with regard to her ongoing right shoulder complaints. Dr. Baily was concerned that there was a good possibility that she may have suffered an injury to her right rotator cuff. This was a transfer of care. 9) Various Dates: Series of Non-Certification Letters by Various Providers, Concentra. The documents were dated from 2007 to 2009. The following were listed as non-certified: home health aid; physical therapy for the lumbar & right hip; physical therapy for the right shoulder. 10) 11/07/07: Agreed Medical Reexamination by Lawrence A. Feiwell, M.D., Diplomate of the American Board of Orthopaedic Surgery, Fellow of the American Academy of Orthopaedic Surgery, The Greater Long Beach Orthopaedic Surgical and Medical Group. Ms. Perriott was initially evaluated on 10/03/07. An interim history was obtained. A physical examination was performed. Ms. Perriott reported that the MR arthrogram of the right shoulder increased symptoms of shoulder pain. DIAGNOSES: 1. Impingement syndrome right shoulder. Ms. Marie Perriott November 9, 2012 Page 32 2. Acromioclavicular degenerative joint disease with residual stiffness and pain. 3. Degenerative disc disease cervical spine. Dr. Feiwell believed Ms. Perriott required further treatment which should consist of a subacromial injection of cortisone and he believed she required another two months of physical therapy consisting of range of motion and strengthening. If her symptoms did not improve, he believed she would be a candidate for revision arthroscopy with debridement and resection of the distal clavicle. She may continue to perform her usual and customary duties. 11) Various Dates: Series of Office Notes by Various Providers, Inland Region Medical Group. The records were dated 2009. The assessments included: sprain and strain of unspecified site of hip and thigh; acute nasopharyngitis; unspecified asthma. 12) Various Dates: Series of Application for Adjudication of Claim. The records were dated from 6/18/09 to 5/09/11. 6/18/09: Date of Injury: 2/12/09. Ms. Perriott, while employed as Sales with Rose Hills Company, sustained injury as follows: to the back, right hip, and right leg, due to an auto accident.. An Employee’s Claim for Workers’ Compensation Benefits of the same date contained information consistent with the Application for Adjudication of Claim. Also, a Workers’ Compensation Claim Form dated 5/29/09 also contained information consistent with the Application for Adjudication of Claim. Ms. Marie Perriott November 9, 2012 Page 33 3/28/11: Amended. Right shoulder and right arm were added as a compensable consequence to industrial injuries. 4/27/11: Amended. Left shoulder and left upper extremities were added as a compensable consequence of industrial injuries (not right arm or right shoulder). 5/09/11: Amended. Psyche, left shoulder, and left upper extremities were added as a compensable consequence of industrial injuries (not right arm or right shoulder). 13) Various Dates: Series of Reports by Hamid Rahman, M.D., Orthopedic Sports & Spine Medical Group. The records were dated from 7/08/09 to 8/05/09. 7/08/09: Authorized Initial Orthopedic Consultation. A history was obtained. Medical records and radiology reports were reviewed. A physical examination was performed. Ms. Perriott complained of constant aching pain to the right side of the low back that radiated into the hip and leg. There was a lot of stiffness of the low back that radiated downward. There had been an increase in urinary frequency and bowel movements. There was a popping of the low back with pressing down on the abdomen, and she stated this relieved some of the pain. The pain was increased with bending, pulling, pushing, lifting, twisting, prolonged standing, sitting and driving. There was a constant aching pain with stiffness of her right hip. She stated she felt like she had a strain of the hamstring region of her leg. There was weakness and instability to the right hip and leg. The pain was increased with standing, walking, driving, and ascending/descending stairs. Ms. Marie Perriott November 9, 2012 Page 34 DIAGNOSES: 1. Musculoligamentous strain/sprain lumbar spine. 2. Right lower extremity radiculitis, rule out herniated nucleus pulposus. 3. Right greater trochanteric bursitis. 4. Insomnia. Medications were dispensed. Authorization was requested for MRI of the lumbar spine and MRI of the right hip, EMG/NCV studies, interferential stimulator, and physical therapy twice a week for 6 weeks. Also recommended was a trial of acupuncture treatment with Dr. Hing for six sessions. Ms. Perriott was temporarily totally disabled. 8/05/09: Orthopedic Reevaluation. Ms. Perriott was still complaining of significant low back pain. She was attending chiropractic and physiotherapy with Dr. McClellan and had improved somewhat with therapy. Additional therapy had been recommended for at least five visits. There was pain radiating into the right groin area. The diagnoses remained the same. She had a negative EMG/Nerve Conduction Study and a progress report from Dr. McClellan showed that although the symptoms persisted she had improved range of motion and increased strength. She was referred to pain management for trial lumbar spine epidural steroid injection. Darvocet was refilled. She was temporarily totally disabled. 14) 7/15/09: Electrodiagnostic Studies Report by Aaron Coppelson, M.D., Diplomate of the American Board of Electrodiagnostic Medicine, Physical Medicine & Rehabilitation, & Pain Management, Restore Medical Group. Ms. Marie Perriott November 9, 2012 Page 35 Ms. Perriott was referred by Dr. Rahman for electrodiagnostic testing of the bilateral lower extremities. STUDIES: Nerve Conduction Studies and Electromyogram. IMPRESSION: 1. Normal NCS. 2. Normal EMG. 15) Various Dates: Series of Depositions of Marie Perriott. The depositions were dated from 9/14/09 to 1/31/12. 9/14/09: Volume I. Ms. Perriott was currently taking medication which consisted of Darvocet and over-the-counter Extra Strength Tylenol. The Darvocet was prescribed by Dr. Ramon [sic], and she took it for pain in her lower back and right leg. Marie Antoinette Perriott stated her full name. She had also been known by the names of Marie Antoinette Lara and Marie Antoinette Para. She had a nickname of Melly. She was born on 5/19/50 in Los Angeles, California. She lived in Michigan for one year, in 1979. She lived with her son, who was an adult. She had one other child, a daughter who lived in Upland. Her current physician was Dr. Jennifer Boozer, who had been her doctor since May of 2009. Prior to this, she saw Dr. Rosario Cecilio in Whittier. She was previously a member of Kaiser, but could not recall the period of time in which she was a member. She was hospitalized six years ago due to respiratory problems. She Ms. Marie Perriott November 9, 2012 Page 36 was also hospitalized due to her low back, which she believed was as a result of using a TENS unit for her lower back. She had injured her lower back in 1983 due to combat wrestling/police training. She received treatment from Dr. Bryan who had been her doctor since 1991 for her back. She had been involved in two car accidents, most recently six years ago while backing out her driveway and scratching another car; there were no injuries. The other accident occurred approximately 15 years ago when she was rear-ended on the street. She recalled a stiffness in her neck. She had her deposition taken in 2007 for a work-related injury while employed with Rose Hills, her current employer. She injured herself due to the weight of her briefcase on her shoulder which caused a tear in her right shoulder rotator cuff. She had surgery performed by Dr. Bryan, and underwent therapy. The pain in her right leg would sometimes travel all the way down to her toes. She denied left leg pain. 1/31/12: Volume II. Ms. Perriott had been involved in another automobile accident since the prior deposition. She stated that she was rear-ended last week in Rancho Cucamonga; she did not sustain any injuries. She spent her days at home “most of the time” and reclined the majority of the time. She tried to do a little bit of housework, but she had to recline in between activities due to her right leg pain. Her current source of income was EDD disability. She lived with her adult son who was working and helping out with the rent. She was behind with her electric bill and gas bill. Her rent was on time. She had a total of two children and one grandchild. She had been married twice; the first time to David Belara in 1969. The marriage lasted three years; she wanted a divorce because she was not happy with him. She described him as jealous. She recalled seeking Ms. Marie Perriott November 9, 2012 Page 37 counseling with the Air Force chaplain; maybe two sessions. He was the father of her son. Her second husband was Mark Perriott; they were married in 1975 for a year and a half. He was the father of her daughter. She initiated the divorce because she wanted to work and he did not want her to work. She stated that he was verbally abusive sometimes, and had hit her a couple of times. The abuse caused her a little bit of stress. She described the relationship with her first husband as “cordial”and the relationship with her second husband as “very good.” She recalled her injury in 2009 in which she injured her upper back, right hip into her groin, and her right leg. She was claiming injury to additional parts of her body: her left shoulder and arm. She stated that the symptoms in her left shoulder had happened slowly. She stated, “Because of the problem in my right hip and lower back, I have difficulty sleeping too long on my back and/or on my right side. So I spend a lot of time when I sleep on my left side of my body.” As a result of her work at Rose Hills, she claimed she had injured the following parts of her body: lower back, right hip, leg, and groin, left shoulder and arm. She started to feel symptoms of depression when she went to CedarsSinai, and then went back to Dr. Goldman’s office and was told there was nothing that could be done for her, that her “back was going to be like that.” She felt like she wanted to cry, and wondered what kind of life she was going to have.” She felt symptoms of anxiety, which she described as “feeling nervous, hopeless, trapped.” She had seen Dr. Donaldson twice. She wished to have right hip surgery, but did not want back surgery. Ms. Perriott stated that she no longer socialized with friends. She had not had a boyfriend in the last ten years. She had crying spells a couple of times a week. Her mother passed away in January 1998 from leukemia. She described the relationship with her mother as “very loving.” Her Ms. Marie Perriott November 9, 2012 Page 38 mother had been given fourteen days to two months to live, and she passed away in fourteen days. She had nine siblings and said she was close to all of them. Her father died from complications of pneumonia in 2002. She stated that she was “very” close to her father, and her parents were still together up until her mother’s passing. Her father had Alzheimer’s. She had a brother who died at age 49 and had cerebral palsy. After her parents died, she sought counseling from her pastor. 16) Various Dates: Series of Reports by Scott Goldman, M.D., Board Certified Orthopedic Surgeon. The records were dated from 9/30/09 to 1/13/12. 9/30/09: Initial Orthopedic Evaluation Report. A history was obtained. Diagnostic studies were reviewed. A physical examination was performed. Ms. Perriott had a painful condition affecting the lower back, with radiation of pain into the right lower extremity. She sustained injury to her lower back with right-sided sciatica as a result of a motor vehicle accident that occurred on 2/12/09 while working in sales for Rose Hills Company. At the time of injury, she was stopped in her vehicle when another vehicle struck her vehicle on the front passenger side, resulting in injury to her lower back and right leg. She had a previous history of work-related injury to the lower back in 1982. ASSESSMENT: 1. Disc protrusion, L4-5, with spinal stenosis, L3-4, and rightsided sciatica. Medications were prescribed. She was referred for physical therapy with spinal decompression, 3 times a week for 4 weeks for the lower back. Recommendation was made for ambulation with cane to left Ms. Marie Perriott November 9, 2012 Page 39 hand, as she had significant pain in the right leg. She was temporarily totally disabled. 10/14/11: Primary Treating Physician’s Progress Report. Ms. Perriott had severely painful conditions affecting the lower back and right hip. As a result, she slept on the left side of her body. This had resulted in traumatic injury to the left shoulder. Repeated sleeping on the left shoulder had injured her rotator cuff. Authorization was requested to evaluate and treat the left shoulder at this time. X-ray of the right hip was reviewed. ASSESSMENT: 1. Disc protrusion, lumbar spine. 2. Osteoarthritis, right hip, severe. Authorization was requested for total right hip replacement with Dr. Donaldson. Medication was prescribed. The treatment plan included a home exercise program for the lower back. Ms. Perriott was permanent and stationary status under Future Medical Care. 12/12/11: Primary Treating Physician’s Progress Report. Ms. Perriott had severe osteoarthritis affecting the lumbar spine and right hip. ASSESSMENT: 1. Osteoarthritis, lumbar spine. 2. Osteoarthritis, right hip. Authorization was requested for cardiac clearance followed by joint replacement of the right hip by Dr. Donaldson. Anaprox was dispensed. 1/13/12: Primary Treating Physician’s Progress Report. Ms. Marie Perriott November 9, 2012 Page 40 Ms. Perriott had seen Dr. Donaldson, who recommended total hip replacement. A repeat EKG was performed and according to Ms. Perriott, this was normal. However, Dr. Goldman did not have the results to verify this. ASSESSMENT: 1. Osteoarthritis, lumbar spine. 2. Osteoarthritis, right hip. Authorization was requested for cardiology clearance for right total hip replacement and right total hip replacement with Dr. Donaldson. 17) 7/11/11: Notification of Non-Certification by Rosalyn Beaty, M.D., Coventry. The request for right hip MR arthrogram and MRI of the lumbar spine at San Antonio Community Hospital was not certified. 18) Various Dates: Series of Secondary Treating Physician’s Progress Reports by Thomas K. Donaldson, M.D. The records were dated from 10/27/11 to 4/12/12. 10/27/11: Ms. Perriott reported for pre-operative examination in anticipation of a right total hip arthroplasty. DIAGNOSES: 1. Hip degenerative joint disease. 2. Hip pelvis pain. The treatment plan included right total hip arthroplasty. Ms. Marie Perriott November 9, 2012 Page 41 3/16/12: Ms. Perriott was here for her first post op of the right total hip arthroplasty performed on 3/06/12. She currently was not having any pain or major complications at this time. DIAGNOSIS: 1. Hip joint replacement. She was to continue the home exercise program and start out-patient physical therapy. Activity modification was as tolerated. 4/12/12: Ms. Perriott was doing well. She was awaiting approval for physical therapy. She requested transportation to and from doctor’s office as she was still not cleared to drive yet. DIAGNOSIS: 1. Hip joint replacement. 2. Hip pelvis pain. Authorization was requested to provide transportation to and from doctor’s office for 6 weeks. Authorization was requested for x-rays of the right hip and ultrasound of the right lower extremity. 19) Various Dates: Series of Clinic Notes by Gail Maloff, L.M.F.T., Perry Maloff, M.D., & Associates. The records were dated from 12/20/11 to 2/23/12. 12/20/11: Ms. Perriott received psychotherapy on 10/18/11 and 12/05/11. Her mood was depressed; affect was congruent to mood. She complained Ms. Marie Perriott November 9, 2012 Page 42 of back and hip pain. She stated, “I don’t do anything. I have to recline.” She was anxious. She reported going to emergency room fearing she was having a “heart attack.” There was improvement in sleep. She described stopping “all medication” and experiencing improvement in symptoms. 2/23/12: Ms. Perriott was scheduled for hip surgery on 3/06/12. She reported her mood was better with the knowledge that she was cleared for surgery. She had lost a few pounds. She acknowledged she would be on her own after surgery as her daughter had to work and her son underwent surgery. She had numerous somatic complaints. She did not go out “so much.” 6/25/12: Ms. Perriott was status post surgery. Her mood was irritable and depressed with congruent affect. She was highly frustrated with denials following surgery for physical therapy. She was dependent upon others for transportation. She felt isolated and socially withdrawn. There were negative thought processes. She had numerous complaints regarding navigation through workers’ compensation system. 20) Various Dates: Series of Reports by Luigi F. Galloni, M.D. The records were dated from 2/24/12 to 9/27/12. 2/24/12: Primary Treating Physician’s Initial Orthopedic Evaluation. A history was obtained. Diagnostic studies were reviewed. A physical examination was performed. Ms. Perriott complained of pain and discomfort in the left shoulder, with radiation to the fingers. The pain was associated with numbness and tingling. The pain came and went and was constant in frequency. Ms. Marie Perriott November 9, 2012 Page 43 She complained of pain in the low back, with radiation to the coccyx. The pain was constant in frequency. She complained of pain in the right hip, with radiation to the right groin area. The pain was on and off in frequency. DIAGNOSES: 1. Osteoarthritis of the acromioclavicular joint with possible impingement syndrome of the left shoulder. 2. Severe osteoarthritis of the lumbosacral spine. 3. Moderate osteoarthritis of the right hip. Ms. Perriott was scheduled for a total hip replacement on 3/06/12. She was also here for a change of primary treating physician. She was temporarily totally disabled. 3/01/12: Review of Medical Records. Numerous medical records were reviewed with regard to Ms. Perriott’s injury to her right hip and lumbosacral spine. Dr. Galloni found the information contained in the records to be consistent with the information Ms. Perriott provided to him. He found nothing to cause him to change any of his prior opinions, conclusions or recommendations. 4/27/12: Follow-Up Orthopaedic Evaluation. Ms. Perriott had lower lumbar problems. She was post-op right hip replacement. She was not able to drive and therefore needed transportation to several doctor’s appointments. She was in need of a cane. She had also been denied physical therapy which was an important part of post operative care. She was to be seen by Dr. Donaldson in May and was to follow-up here in four to six weeks. She remained temporarily totally disabled. 5/25/12: Follow-Up Orthopaedic Evaluation. Ms. Marie Perriott November 9, 2012 Page 44 Ms. Perriott complained of pain in the lower back. She related that she was receiving therapy for the right hip, three times a week. The diagnoses remained the same as on 2/24/12. She was to continue with her physical therapy two times a week for the next six weeks. She remained temporarily totally disabled. 5/29/12: Review of Medical Records. Additional medical records were reviewed. Dr. Galloni found nothing to cause him to change any of his prior opinions, conclusions or recommendations. 6/28/12: Follow-Up Consultation. Ms. Perriott continued to complain of neck pain radiating to both shoulders, lower back pain, and left wrist pain. DIAGNOSES: 1. Acromioclavicular arthrosis, left shoulder. 2. Impingement syndrome, left shoulder. 3. Tendinitis/bursitis, left shoulder. 4. DeQuervain’s, left wrist. 5. Tenosynovitis, left 1st carpometacarpal joint. A course of shockwave treatment to the left shoulder and left wrists. was recommended. If this failed, Dr. Galloni felt the only other option was surgical, in the form of a decompression to the left shoulder. It was recommended she continue with her splinting. 6/29/12: Follow-Up Orthopaedic Evaluation. Ms. Marie Perriott November 9, 2012 Page 45 Ms. Perriott continued to complain of right hip pain, as well as lower back pain. DIAGNOSES: 1. Osteoarthritis of the acromioclavicular joint with possible impingement syndrome of the left shoulder. 2. Severe osteoarthritis of the lumbosacral spine. 3. Moderate osteoarthritis of the right hip. 4. Status post right total hip replacement. She continued to need postoperative rehabilitation for the right total hip replacement. She remained temporarily totally disabled. 9/27/12: Follow-Up Orthopaedic Evaluation. Ms. Perriott complained of dull aching pain in the right hip. She also complained of severe low back pain. She stated that she was unable to stand or walk for any significant amount of time. Additional medical records were reviewed. DIAGNOSES: 1. Osteoarthritis of the acromioclavicular joint with possible impingement syndrome of the left shoulder. 2. Severe osteoarthritis of the lumbar spine. 3. Severe lumbar discogenic disease. 4. Central and foraminal narrowing, L3-L4 and L4-L5. 5. Post total hip replacement on the right. It was recommended that Ms. Perriott see a pain management doctor in view of the severe degree of pain in her lower back which was Ms. Marie Perriott November 9, 2012 Page 46 confirmed by MRI scan. She needed to continue to follow up with Dr. Donaldson for the hip replacement procedure performed by him. It was also recommended that the pain management doctor manager her pharmcologically. She was to be started on a course of physical therapy for her lumbar spine, two times a week for 6 weeks. She was recommended to perform home exercises for her hip. She remained temporarily totally disabled. 21) Various Dates: Series of Secondary Treating Physician’s Progress Reports by Thomas K. Donaldson, M.D., Empire Orthopedic Center. The records were dated from 7/25/12 to 9/13/12. 7/25/12: Ms. Perriott reported for a recheck of the right total hip arthroplasty, performed on 3/16/12. She stated that her right hip was doing well, but that she was having difficulty driving. She was currently taking Vicodin for pain. She was in physical therap and had completed 12 sessions. Overall she felt that she was progressing. DIAGNOSIS: 1. Hip joint replacement. She was to continue the home exercise program and start out-patient physical therapy, 2 times a week for the next 6 weeks. She was to perform activity modification as tolerated. 9/13/12: Ms. Perriott stated that she had been experiencing an ache in her right hip and groin, and had also noticed that she had been limping for the past six months. Overall, she was satisfied with her progress. The diagnosis remained the same. She was to continue with her home exercises and activity modification as tolerated. Ms. Marie Perriott November 9, 2012 Page 47 DIAGNOSIS: On the basis of Ms. Perriott's history, mental status examination, review of medical records, and the results of psychological testing, the following diagnoses are offered in accordance with the Diagnostic and Statistical Manual-IV of the American Psychiatric Association: AXIS I: DEPRESSIVE DISORDER NOT OTHERWISE SPECIFIED (INDUSTRIALLY RELATED) [311]. AXIS II: NO PERSONALITY DISORDER. AXIS III: OA AC JOINT. OA LS SEVERE. OA RIGHT HIP. MUSCULOLIGAMENTOUS STRAIN/SPRAIN LUMBAR SPINE. RIGHT HIP STRAIN. GREATER TROCHANTERIC BURSITIS. INSOMNIA. RECURRENT LUMBAR STRAIN. MILD OSTEOARTHRITIS. IMPINGEMENT SHOULDER. SYNDROME RIGHT ACROMIOCLAVICULAR DEGENERATIVE JOINT DISEASE WITH RESIDUAL STIFFNESS AND PAIN. Ms. Marie Perriott November 9, 2012 Page 48 DEGENERATIVE DISC DISEASE CERVICAL SPINE. HIP DEGENERATIVE JOINT DISEASE. HIP PELVIS PAIN. AXIS IV: DEFERRED. AXIS V: GAF SCORE OF 61 CORRESPONDING TO A WHOLE PERSON IMPAIRMENT (WPI) SCORE OF 14. SUMMARY AND CONCLUSIONS: Ms. Marie Perriott began working for Rose Hills Co. as a memorial service counselor on October 6, 2003. She reports that she injured herself at work on February 12, 2009, when she was driving back to the office from a presentation and was hit on front end of the passenger side by a van. She injured her lower back and right hip.” Ms. Perriott reported the job injury to her supervisor. She was later sent to Presbyterian Intercommunity Hospital emergency room on May 29, 2009, where she saw a physician assistant, who prescribed pain medication and treated her with physical therapy. Ms. Perriott went back to work with job restrictions. Subsequently, she consulted an attorney and was sent to Dr. Rahman, who took her off work. Her last day of work was on May 7, 2012. She was treated with physical therapy and various medications. She was told by two different doctors that they did not recommend back surgery, which put Ms. Perriott in a depression because she felt there was nothing they could do for her back pain. She was sent to a psychiatrist because she was depressed. She received individual psychotherapy sessions. Ms. Marie Perriott November 9, 2012 Page 49 According to Ms. Perriott, she went to San Antonio Hospital emergency room due to shortness of breath, hot flashes, and lightheadedness. She was told that she was “okay.” She later got an MRI on her right hip and underwent a total right hip replacement surgery on March 6, 2012. She was then sent to a nursing home for three weeks and was treated with postoperative physical therapy. In regard to her current physical complaints, Ms. Perriott reports right hip pain, headaches and lower back pain that radiates down her right leg. She is taking the following medications: 1. Hydrocodone. 2. Naproxen. 3. Amitriptyline. 4. Flurbiprofen. 5. Mometasone. 6. Desonide. Having considered the evidence gained from Ms. Perriott's history, her mental status examination, the review of medical records, and the psychological testing, an assessment of DEPRESSIVE DISORDER NOT OTHERWISE SPECIFIED (INDUSTRIALLY RELATED) is offered on Axis I. Ms. Perriott is permanent and stationary. Ms. Marie Perriott November 9, 2012 Page 50 On the basis of these considerations, the following statements are offered: TEMPORARY DISABILITY: Ms. Perriott is not temporarily disabled psychiatrically on an industrial basis. PERMANENT AND STATIONARY: Ms. Perriott is permanent and stationary with a GAF score of 61 corresponding to a Whole Person Impairment (WPI) score of 14. CAUSATION: Ms. Perriott’s work injury contributed at least 51% to her psychiatric condition and was the predominant cause of her disability. MEDICAL CARE: Ms. Perriott should have access to psychiatric care should she experience an exacerbation or recurrence of her present condition. ABILITY TO WORK: Ms. Perriott’s ability to work is diminished in proportion to her GAF score and WPI ratings. DISCUSSION OF APPORTIONMENT: 5% History of abuse by spouse. Any or all of the diagnoses and conclusions contained herein are subject to revision based upon the receipt and review of additional medical records. Ms. Marie Perriott November 9, 2012 Page 51 RESEARCH FINDINGS Ms. Perriott has a diagnosis of Depressive Disorder NOS. According to Kessler, Berglund et al have concluded, “major depressive disorder is a common disorder, widely distributed in the population, and usually associated with substantial symptom severity and role impairment. While the recent increase in treatment is encouraging, inadequate treatment is a serious concern.” In a related study, Kessler, Nelson et al found “most cases of lifetime MDD are secondary. In the sense that they occur in people with a prior history of another DSM-III-R disorder. Anxiety disorders are the most common primary disorders. The time-lagged effects of most primary disorders on the risk of subsequent MDD continue for many years without change in magnitude. Secondary MDD is, in general, more persistent and severe than pure or primary MDD.” However, Kessler sounded a moderating note to his warning in a later study with Chiu et al, which concluded, “Although mental disorders are widespread, serious cases are concentrated among a relatively small proportion of cases with high comorbidity.” This conclusion was backed by the Netherlands study of Bijl et al, which reported “Some 41.2% of the adult population under 65 had experienced at least one DSM-III-R disorder in their lifetime, among them 23.3% within the preceding year. No gender differences were found in overall morbidity. Depression, anxiety, and alcohol abuse and dependence were most prevalent, and there was a high degree of comorbidity between them.” The need for adequate treatment of depression was further underlined by Judd et al, who concluded “resolution of major depressive episodes with residual subthreshold depressive symptoms, even the first lifetime episode, appears to be the first step of a more severe, relapsing, and chronic future course. When ongoing subthreshold symptoms continue after major depressive episodes, the illness is still active, and continued treatment is strongly recommended.” Cassem had this take on the relationship between depression and physical Ms. Marie Perriott November 9, 2012 Page 52 illness: “Depressive disorders are far more serious than most people realize, and depressive disorders are disabling affected persons progressively earlier in life. Heavy utilization of medical services, extensive disability and morbidity, and high suicide risk exact a staggering economic toll in the United States annually. Depressive illness is, like pneumonia and septic shock, a dread complication of major medical illness, and depressive illness appears more frequently as the medical illness worsens . . .” Rost et al seconded this conclusion in their study, which found, “Ongoing intervention increased remission rates and improved indicators of emotional and physical functioning. Studies are needed to compare the cost effectiveness of ongoing depression management with other chronic disease treatment routinely undertaken by primary care.” Underscoring the seriousness of inadequate treatment of MDD, Stewart et al concluded, “A majority of the LPT [lost production time] costs that employers face from employee depression is invisible and explained by reduced performance while at work. Use of treatments for depression appears to be relatively low. The combined LPT burden among those with depression and the low level of treatment suggests that there may be cost-effective opportunities for improving depression-related outcomes in the US workforce.” Greco et al indicated the tenacity of physical symptoms in depression: “Physical symptoms are prevalent in depressed patients and initially improve in the first month of SSRI treatment. Unlike depression, however, improvement in physical symptoms typically plateaus with minimal resolution in subsequent months.” Finally, Bair et al reported “Pain is present in two-thirds of depressed primary care patients begun on antidepressant therapy, and the severity of pain is a strong predictor of poor depression and health-related quality of life outcomes at 3 months.” JAMA, the Journal of the American Medical Association ISSN 0098-7484 2003, vol. 289, no23, pp. 3095-3105 [11 page(s) (article)] (80 ref.) Ms. Marie Perriott November 9, 2012 Page 53 THE EPIDEMIOLOGY OF MAJOR DEPRESSIVE DISORDER: RESULTS FROM THE NATIONAL COMORBIDITY SURVEY REPLICATION (NCS-R) Kessler RC (1) ; Berglund P (2) ; Demler O (1) ; Jin R (1) ; Koretz D(3) ; Merikangas KR (4) ; Rush AJ (5) ; Walters EE (1) ; Wang PS. (1, 6) (1) Department of Health Care Policy, Harvard Medical School, Boston, Mass, ETATS-UNIS (2) Institute for Social Research, University of Michigan, Ann Arbor, ETATS-UNIS (3) Division of Mental Disorders, Behavioral Research and AIDS National Institute of Mental Health, Rockville, Md, ETATS-UNIS (4) Intramural Research Program, National Institute of Mental Health, Rockville, Md, ETATS-UNIS (5) Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, ETATS-UNIS (6) Brigham and Womens'Hospital, Harvard Medical School, ETATS-UNIS CONTEXT: Uncertainties exist about prevalence and correlates of major depressive disorder (MDD). OBJECTIVE: To present nationally representative data on prevalence and correlates of MDD by Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria, and on study patterns and correlates of treatment and treatment adequacy from the recently completed National Comorbidity Survey Replication (NCS-R). DESIGN: Face-to-face household survey conducted from February 2001 to December 2002. SETTING: The 48 contiguous United States. PARTICIPANTS: Household residents ages 18 years or older (N =9,090) who responded to the NCS-R survey. MAIN OUTCOME MEASURES: Prevalence and correlates of MDD using the World Health Organization's (WHO) Composite International Diagnostic Interview (CIDI), 12-month severity with the Quick Inventory of Depressive Ms. Marie Perriott November 9, 2012 Page 54 Symptomatology Self-Report (QIDS-SR), the Sheehan Disability Scale (SDS), and the WHO disability assessment scale (WHO-DAS). Clinical reinterviews used the Structured Clinical Interview for DSM-IV. RESULTS: The prevalence of CIDI MDD for lifetime was 16.2% (95% confidence interval [Cl], 15.1-17.3) (32.6-35.1 million US adults) and for 12-month was 6.6% (95% CI, 5.9-7.3) (13.1-14.2 million US adults). Virtually all CIDI 12-month cases were independently classified as clinically significant using the QIDS-SR, with 10.4% mild, 38.6% moderate, 38.0% severe, and 12.9% very severe. Mean episode duration was 16 weeks (95% CI, 15.1-17.3). Role impairment as measured by SDS was substantial as indicated by 59.3% of 12-month cases with severe or very severe role impairment. Most lifetime (72.1%) and 12-month (78.5%) cases had comorbid CIDI/DSM-IV disorders, with MDD only rarely primary. Although 51.6% (95% CI, 46.1-57.2) of 12-month cases received health care treatment for MDD, treatment was adequate in only 41.9% (95% CI, 35.9-47.9) of these cases, resulting in 21.7% (95% CI, 18.1-25.2) of 12-month MDD being adequately treated. Sociodemographic correlates of treatment were far less numerous than those of prevalence. CONCLUSIONS: Major depressive disorder is a common disorder, widely distributed in the population, and usually associated with substantial symptom severity and role impairment. While the recent increase in treatment is encouraging, inadequate treatment is a serious concern. Emphasis on screening and expansion of treatment needs to be accompanied by a parallel emphasis on treatment quality improvement. Br J Psychiatry Suppl. 1996 Jun;(30):17-30. Comment in: Br J Psychiatry. 1997 Nov;171:487-8. COMORBIDITY OF DSM-III-R MAJOR DEPRESSIVE DISORDER IN THE GENERAL POPULATION: RESULTS FROM THE US NATIONAL COMORBIDITY SURVEY. Kessler RC, Nelson CB, McGonagle KA, Liu J, Swartz M, Blazer DG. Institute for Social Research, University of Michigan, Ann Arbor Ms. Marie Perriott November 9, 2012 Page 55 48106-1248, USA. General population data are presented on the prevalence and correlates of comorbidity between DSM-III-R major depressive disorder (MDD) and other DSM-III-R disorders. The data come from the US National Comorbidity Survey, a large general population survey of persons aged 15-54 years in the non-institutionalised civilian population. Diagnoses are based on a modified version of the Composite International Diagnostic Interview (CIDI). The analysis shows that most cases of lifetime MDD are secondary. In the sense that they occur in people with a prior history of another DSM-III-R disorder. Anxiety disorders are the most common primary disorders. The time-lagged effects of most primary disorders on the risk of subsequent MDD continue for many years without change in magnitude. Secondary MDD is, in general, more persistent and severe than pure or primary MDD. This has special public health significance because lifetime prevalence of secondary MDD has increased in recent cohorts, while the prevalence of pure and primary depression has remained unchanged. Arch Gen Psychiatry. 2005 Jun;62(6):617-27. Erratum in: Arch Gen Psychiatry. 2005 Jul;62(7):709. Merikangas, Kathleen R [added]. Comment in: Arch Gen Psychiatry. 2005 Jun;62(6):590-2. Arch Gen Psychiatry. 2007 Mar;64(3):379-80; author reply 381-2. Arch Gen Psychiatry. 2007 Mar;64(3):380-1; author reply 381-2. Evid Based Ment Health. 2006 Feb;9(1):27. PREVALENCE, SEVERITY, AND COMORBIDITY OF 12-MONTH DSM-IV DISORDERS IN THE NATIONAL COMORBIDITY SURVEY REPLICATION. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Department of Health Care Policy, Harvard Medical School, Boston, Massachusetts 02115, USA. [email protected] BACKGROUND: Little is known about the general population prevalence or severity of DSM-IV mental disorders. Ms. Marie Perriott November 9, 2012 Page 56 OBJECTIVE: To estimate 12-month prevalence, severity, and comorbidity of DSM-IV anxiety, mood, impulse control, and substance disorders in the recently completed US National Comorbidity Survey Replication. DESIGN AND SETTING: Nationally representative face-to-face household survey conducted between February 2001 and April 2003 using a fully structured diagnostic interview, the World Health Organization World Mental Health Survey Initiative version of the Composite International Diagnostic Interview. PARTICIPANTS: Nine thousand two hundred eighty-two English-speaking respondents 18 years and older. MAIN OUTCOME MEASURES: Twelve-month DSM-IV disorders. RESULTS: Twelve-month prevalence estimates were anxiety, 18.1%; mood, 9.5%; impulse control, 8.9%; substance, 3.8%; and any disorder, 26.2%. Of 12-month cases, 22.3% were classified as serious; 37.3%, moderate; and 40.4%, mild. Fifty-five percent carried only a single diagnosis; 22%, 2 diagnoses; and 23%, 3 or more diagnoses. Latent class analysis detected 7 multivariate disorder classes, including 3 highly comorbid classes representing 7% of the population. CONCLUSION: Although mental disorders are widespread, serious cases are concentrated among a relatively small proportion of cases with high comorbidity. Soc Psychiatry Psychiatr Epidemiol. 1998 Dec;33(12):587-95. PREVALENCE OF PSYCHIATRIC DISORDER IN THE GENERAL POPULATION: RESULTS OF THE NETHERLANDS MENTAL HEALTH SURVEY AND INCIDENCE STUDY (NEMESIS). Bijl RV, Ravelli A, van Zessen G. Netherlands Institute of Mental Health and Addiction, Trimbos-Instituut, Utrecht, The Netherlands. This article reports the initial results of a prospective study on the prevalence Ms. Marie Perriott November 9, 2012 Page 57 of psychiatric disorders in the Dutch population aged 18-64. The objectives and the design of the study are described elsewhere in this issue. A total of 7,076 people were interviewed in person in 1996. The presence of the following disorders was determined by means of the CIDI: mood disorders, anxiety disorders, eating disorders, schizophrenia and other non-affective psychoses, and substance use disorders. Psychiatric disorders were found to be quite common. Some 41.2% of the adult population under 65 had experienced at least one DSM-III-R disorder in their lifetime, among them 23.3% within the preceding year. No gender differences were found in overall morbidity. Depression, anxiety, and alcohol abuse and dependence were most prevalent, and there was a high degree of comorbidity between them. The prevalence rate encountered for schizophrenia was lower (0.4% lifetime) than generally presumed. A comparison with findings from other countries is made. Relevant determinants of psychiatric morbidity were analysed. Am J Psychiatry. 2000 Sep;157(9):1501-4. DOES INCOMPLETE RECOVERY FROM FIRST LIFETIME MAJOR DEPRESSIVE EPISODE HERALD A CHRONIC COURSE OF ILLNESS? Judd LL, Paulus MJ, Schettler PJ, Akiskal HS, Endicott J, Leon AC, Maser JD, Mueller T, Solomon DA, Keller MB. Department of Psychiatry, University of California at San Diego, La Jolla, CA 92093-0603, USA. [email protected] OBJECTIVE: This study investigated the influence of incomplete recovery from first lifetime major depressive episodes on long-term outcome. METHOD: After their first lifetime major depressive episode, patients were divided into asymptomatic (N=70) and residual subthreshold depressive symptom (N=26) recovery groups and compared on longitudinal course during up to 12 years of prospective naturalistic follow-up. RESULTS: Patients with residual subthreshold depressive symptoms during recovery had significantly more severe and chronic future courses. Those with residual symptoms relapsed to major and minor depressive episodes faster and had more recurrences, shorter well intervals, and fewer Ms. Marie Perriott November 9, 2012 Page 58 symptom-free weeks during follow-up than asymptomatic patients. CONCLUSIONS: Resolution of major depressive episodes with residual subthreshold depressive symptoms, even the first lifetime episode, appears to be the first step of a more severe, relapsing, and chronic future course. When ongoing subthreshold symptoms continue after major depressive episodes, the illness is still active, and continued treatment is strongly recommended. Psychosomatics ISSN 0033-3182 1995, vol. 36, no2, pp. S2-S10 (45 ref.) DEPRESSIVE DISORDERS IN THE MEDICALLY ILL: AN OVERVIEW: DEPRESSIVE DISORDERS IN THE MEDICALLY ILL: EXPANDING OPTIONS FOR THE CONSULTATION-LIAISON PSYCHIATRIST. Cassem EH. Massachusetts Gen. Hosp., Dep. Psychiatry, Boston MA 02114, ETATS-UNIS Depressive disorders are far more serious than most people realize, and depressive disorders are disabling affected persons progressively earlier in life. Heavy utilization of medical services, extensive disability and morbidity, and high suicide risk exact a staggering economic toll in the United States annually. Depressive illness is, like pneumonia and septic shock, a dread complication of major medical illness, and depressive illness appears more frequently as the medical illness worsens; diseases affecting the brain may have the highest rates of depressive symptoms. Correctly diagnosing a depressive disorder in a medically ill patient is a clinical challenge that requires systematic, persistent clinical scrutiny. Compassion demands that depressive disorders, when diagnosed, be treated aggressively. BMJ. 2002 Oct 26;325(7370):934. Comment in: BMJ. 2003 Feb 8;326(7384):338. Evid Based Ment Health. 2003 May;6(2):47; author reply 47. Ms. Marie Perriott November 9, 2012 Page 59 Evid Based Nurs. 2003 Jul;6(3):86. MANAGING DEPRESSION AS A CHRONIC DISEASE: A RANDOMISED TRIAL OF ONGOING TREATMENT IN PRIMARY CARE. Rost K, Nutting P, Smith JL, Elliott CE, Dickinson M. Center for Studies in Family Medicine, Department of Family Medicine, University of Colorado Health Sciences Center, UCHSC at Fitzsimons, Aurora, CO 80045-0508, USA. [email protected] OBJECTIVES: To evaluate the long term effect of ongoing intervention to improve treatment of depression in primary care. DESIGN: Randomised controlled trial. SETTING: Twelve primary care practices across the United States. PARTICIPANTS: 211 adults beginning a new treatment episode for major depression; 94% of patients assigned to ongoing intervention participated. INTERVENTION: Practices assigned to ongoing intervention encouraged participating patients to engage in active treatment, using practice nurses to provide care management over 24 months. MAIN OUTCOME MEASURES: Patients' report of remission and functioning. RESULTS: Ongoing intervention significantly improved both symptoms and functioning at 24 months, increasing remission by 33 percentage points (95% confidence interval 7% to 46%), improving emotional functioning by 24 points (11 to 38) and physical functioning by 17 points (6 to 28). By 24 months, 74% of patients in enhanced care reported remission, with emotional functioning exceeding 90% of population norms and physical functioning approaching 75% of population norms. CONCLUSIONS: Ongoing intervention increased remission rates and improved indicators of emotional and physical functioning. Studies are Ms. Marie Perriott November 9, 2012 Page 60 needed to compare the cost effectiveness of ongoing depression management with other chronic disease treatment routinely undertaken by primary care. JAMA. 2003 Jun 18;289(23):3135-44. Erratum in: JAMA. 2003 Oct 22;290(16):2218. COST OF LOST PRODUCTIVE WORK TIME AMONG US WORKERS WITH DEPRESSION. Stewart WF, Ricci JA, Chee E, Hahn SR, Morganstein D. AdvancePCS Center for Work and Health, Hunt Valley, MD, USA. [email protected] CONTEXT: Evidence consistently indicates that depression has adversely affected work productivity. Estimates of the cost impact in lost labor time in the US workforce, however, are scarce and dated. OBJECTIVE: To estimate the impact of depression on labor costs (i.e., work absence and reduced performance while at work) in the US workforce. DESIGN, SETTING, AND PARTICIPANTS: All employed individuals who participated in the American Productivity Audit (conducted August 1, 2001-July 31, 2002) between May 20 and July 11, 2002, were eligible for the Depressive Disorders Study. Those who responded affirmatively to 2 depression-screening questions (n = 692), as well as a 1:4 stratified random sample of those responding in the negative (n = 435), were recruited for and completed a supplemental interview using the Primary Care Evaluation of Mental Disorders Mood Module for depression, the Somatic Symptom Inventory, and a medical and treatment history for depression. Excess lost productive time (LPT) costs from depression were derived as the difference in LPT among individuals with depression minus the expected LPT in the absence of depression projected to the US workforce. MAIN OUTCOME MEASURE: Estimated LPT and associated labor costs (work absence and reduced performance while at work) due to depression. Ms. Marie Perriott November 9, 2012 Page 61 RESULTS: Workers with depression reported significantly more total health-related LPT than those without depression (mean, 5.6 h/wk vs. an expected 1.5 h/wk, respectively). Eighty-one percent of the LPT costs are explained by reduced performance while at work. Major depression accounts for 48% of the LPT among those with depression, again with a majority of the cost explained by reduced performance while at work. Self-reported use of antidepressants in the previous 12 months among those with depression was low (<33%) and the mean reported treatment effectiveness was only moderate. Extrapolation of these survey results and self-reported annual incomes to the population of US workers suggests that US workers with depression employed in the previous week cost employers an estimated 44 billion dollars per year in LPT, an excess of 31 billion dollars per year compared with peers without depression. This estimate does not include labor costs associated with short- and long-term disability. CONCLUSIONS: A majority of the LPT costs that employers face from employee depression is invisible and explained by reduced performance while at work. Use of treatments for depression appears to be relatively low. The combined LPT burden among those with depression and the low level of treatment suggests that there may be cost-effective opportunities for improving depression-related outcomes in the US workforce. J Gen Intern Med. 2004 Aug;19(8):813-8. Comment in: J Gen Intern Med. 2004 Aug;19(8):893-5. THE OUTCOME OF PHYSICAL SYMPTOMS WITH TREATMENT OF DEPRESSION. Greco T, Eckert G, Kroenke K. Department of Medicine, Indiana University School of Medicine, Indianapolis, USA. OBJECTIVE: This study examined the prevalence, impact on health-related quality of life (HRQoL), and outcome of physical symptoms in depressed patients during 9 months of antidepressant therapy. Ms. Marie Perriott November 9, 2012 Page 62 DESIGN: Open-label, randomized, intention-to-treat trial with enrollment occurring April through November 1999. SETTING: Thirty-seven primary care clinics within a research network. PATIENTS: Five hundred seventy-three depressed patients started on one of three selective serotonin reuptake inhibitors (SSRIs) by their primary care physician and who completed a baseline interview. INTERVENTIONS: Patients were randomized to receive fluoxetine, paroxetine, or sertraline. MEASUREMENTS AND MAIN RESULTS: Outcomes assessed included physical symptoms, depression, and multiple domains of HRQoL. Prevalence of physical symptoms was determined at baseline and after 1, 3, 6, and 9 months of treatment. Stepwise linear regression models were used to determine the independent effects of physical symptoms and depression on HRQoL domains. Of the 14 physical symptoms assessed, 13 were present in at least a third to half of the patients at baseline. Each symptom showed the greatest improvement during the initial month of treatment. In contrast, depression continued to show gradual improvement over a 9-month period. Physical symptoms had a predominant effect on pain (explaining 17% to 18% of the variance), physical functioning (13%), and overall health perceptions (13% to 15%). Depression had the greatest impact on mental (26% to 45%), social (14% to 32%), and work functioning (9% to 32%). CONCLUSIONS: Physical symptoms are prevalent in depressed patients and initially improve in the first month of SSRI treatment. Unlike depression, however, improvement in physical symptoms typically plateaus with minimal resolution in subsequent months. Psychosom Med. 2004 Jan-Feb;66(1):17-22. IMPACT OF PAIN ON DEPRESSION TREATMENT RESPONSE IN PRIMARY CARE. Bair MJ, Robinson RL, Eckert GJ, Stang PE, Croghan TW, Kroenke K. Regenstrief Institute and the Department of Medicine, Indiana University Ms. Marie Perriott November 9, 2012 Page 63 School of Medicine, [email protected] Indianapolis, Indiana 46202, USA. OBJECTIVE: Pain commonly coexists with depression, but its impact on treatment outcomes has not been well studied. Therefore, we prospectively evaluated the impact of comorbid pain on depression treatment response and health-related quality of life. METHODS: We analyzed data from the ARTIST study, a randomized controlled trial with naturalistic follow-up conducted in 37 primary care clinics. Participants were 573 clinically depressed patients randomized to one of three selective serotonin reuptake inhibitor (SSRI) antidepressants: fluoxetine, paroxetine, or sertraline. Depression as assessed by the Symptom Checklist-20 (SCL-20) was the primary outcome. Secondary outcomes included pain and health-related quality of life. RESULTS: Pain was reported by more than two-thirds of depressed patients at baseline, with the severity of pain mild in 25% of patients, moderate in 30%, and severe in 14%. After 3 months of antidepressant therapy, 24% of patients had a poor depression treatment response (i.e., SCL-20 >1.3). Multivariate odds ratios for poor treatment response were 1.5 (95% confidence interval, 0.8-3.2) for mild pain, 2.0 (1.1-4.0) for moderate pain, and 4.1 (1.9-8.8) for severe pain compared with those without pain. Increasing pain severity also had an adverse impact on outcomes in multiple domains of health-related quality of life. CONCLUSIONS: Pain is present in two-thirds of depressed primary care patients begun on antidepressant therapy, and the severity of pain is a strong predictor of poor depression and health-related quality of life outcomes at 3 months. Better recognition, assessment, and treatment of comorbid pain may enhance outcomes of depression therapy. Ms. Marie Perriott November 9, 2012 Page 64 MEDICAL-LEGAL DISCLOSURE INFORMATION PATIENT'S NAME: Ms. Marie Perriott DATE THE EVALUATION WAS PERFORMED, LOCATION OF EVALUATION, AND TIME SPENT BY PHYSICIAN INTERVIEWING PATIENT: The evaluation was performed on October 24, 2012 at my Riverside office. Ms. Perriott was evaluated for a full session, which lasted approximately one hour, during which I obtained all of the information in the report, including current complaints, history of present illness, past history, mental status examination, and psychological testing. When Ms. Perriott left, it was explicit and apparent that she had provided a full account of the substance of her alleged problems, which is contained in my comprehensive report. DATE OF REPORT: November 9, 2012 PHYSICIAN PERFORMING THE EVALUATION AND PHYSICIAN'S QUALIFICATIONS: The evaluation was solely conducted by Barbara J. Strong, M.D., Qualified Medical Examiner in Psychiatry and Neurology. MEDICAL TECHNICIAN: Not applicable LABORATORY TESTS DONE BY: Not applicable OTHER PSYCHOLOGICAL TESTING: The Rey 15-Item Memorization Test, and the Rey Dot Counting Test. INTERPRETER/INTERPRETING SERVICE: Not applicable "I declare under penalty of perjury that the information contained in this report and its attachments, if any, is true and correct to the best of my knowledge and belief, except as to information that I have indicated I received from others. As to that information, I declare under penalty of perjury that the information accurately describes the information provided to me and, except as noted herein, that I believe it to be true." "I further declare under penalty of perjury that I personally performed the evaluation of the patient on October 24, 2012 at Riverside, California, and that, except as otherwise stated herein, the evaluation was performed and the time spent performing the evaluation was in compliance with the guidelines, if any, established by the Industrial Medical Council or the administrative director Ms. Marie Perriott November 9, 2012 Page 65 pursuant to paragraph (5) of subdivision (j) of Section 139.2 or Section 5307.6 of the California Labor Code." "I further declare under penalty of perjury that I have not violated the provisions of California Labor Code Section 139.3 with regard to the evaluation of this patient or the preparation of this report." "I further declare under penalty of perjury that the name and qualifications of each person who performed any services in connection with the report, including diagnostic studies, other than clerical preparation, are as follows:" Name Qualifications Carla Back-Madruga The Rey 15-Item Memorization Test and the Rey Dot Counting Test were scored and interpreted by Carla Back-Madruga, Ph.D. Dr. Back-Madruga obtained her doctorate in Clinical Psychology at California School of Professional Psychology in 1994. She completed her post-doctoral fellowship in clinical neuropsychology at Harbor-UCLA Medical Center and UCLA Neuropsychiatric Institute and Hospital, UCLA Center for the Health Sciences from 1994 to 1995. She is currently the director of Neuropsychology Service at Rand Schrader Health and Research Center, USC Keck School of Medicine, in Los Angeles, California; instructor of Psychology Assessment Seminar at USC Keck School of Medicine; and supervisor of psychology graduate students’ neuropsychological evaluations at USC School of Medicine. Dr. Back-Madruga has a private practice as a clinical neuropsychologist in Los Angeles, California. She has co-authored many journal articles. Along with Kyle Boone, Ph.D., she has reviewed research articles in The Clinical Neuropsychologist. Dr. Back-Madruga is licensed as a psychologist within the state of California and is the Associate Professor of Clinical Psychiatry and Behavioral Sciences, University of Southern California Keck School of Medicine, Los Angeles, California. Ms. Marie Perriott November 9, 2012 Page 66 Date of Report: Signed this day of at Los Angeles County, California. , 20 , Barbara J. Strong, M.D., Q.M.E. BS:as/cb Copyright © 2013 by Irwin Savodnik, M.D., and Medical Associates, Inc. National Assessment Specialists Ms. Marie Perriott November 9, 2012 Page 67 Dr. Caper conducted the research for this report. This research consisted of a lengthy literature search, a comparison with existing research and the integration of the appropriated clinical information with these research results. The goal of this work was to maximize the scientific foundations for the findings and conclusions of this report. Date of Report: Signed this day of at Los Angeles County, California. , 20 , Robert Caper, M.D. RC/as/cb Copyright © 2013 by Irwin Savodnik, M.D., and Medical Associates, Inc. National Assessment Specialists




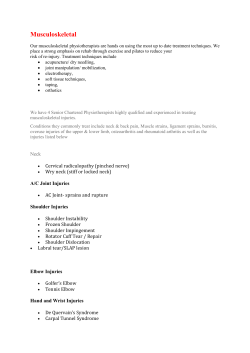




© Copyright 2026