
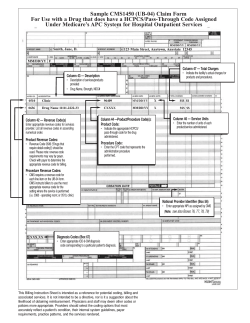
Sample UB-04 (also known as CMS 1450) Claim Form for... Department Billing: KEYTRUDA (pembrolizumab) for Injection 50 mg
Sample UB-04 (also known as CMS 1450) Claim Form for Hospital Outpatient Department Billing: KEYTRUDA® (pembrolizumab) for Injection 50 mg __ Note: for questions on billing if a portion of a package __ is wasted, consult the applicable payor’s policy regarding wastage. __ 1 4 3a PAT. CNTL # b. MED. REC. # 2 6 5 FED. TAX NO. 8 PATIENT NAME 9 PATIENT ADDRESS a Locator 42 b 10 BIRTHDATE 11 SEX DATE ADMISSION 13 HR 14 TYPE 15 SRC 16 DHR 17 STAT • E nter appropriate revenue code for each line item. • Drugs that are billed with HCPCS codes usually require revenue code 0636—Drugs requiring detailed coding. 31 OCCURRENCE CODE DATE 32 OCCURRENCE CODE DATE 33 OCCURRENCE DATE CODE a b 38 18 7 STATEMENT COVERS PERIOD FROM THROUGH a b 12 TYPE OF BILL 19 20 21 Locator 43 c CONDITION CODES 24 22 23 25 26 27 • F or each line item, enter the description of the revenue code used. • F or the KEYTRUDA line item, also enter the drug’s branda and generic names. 34 OCCURRENCE CODE DATE 35 CODE 36 CODE OCCURRENCE SPAN FROM THROUGH 39 CODE 40 CODE VALUE CODES AMOUNT Locator 46 d 28 e 29 ACDT 30 STATE • W hen using an unspecified HCPCS code, enter only 1 unit in this field. 37 OCCURRENCE SPAN FROM THROUGH a b 41 CODE VALUE CODES AMOUNT VALUE CODES AMOUNT b c d 42 REV. CD. 44 HCPCS / RATE / HIPPS CODE 43 DESCRIPTION 45 SERV. DATE 46 SERV. UNITS 47 TOTAL CHARGES 48 NON-COVERED CHARGES 49 1 1 2 2 3 3 4 4 5 5 6 6 7 7 Locator 44 8 9 8 • U se the appropriate unspecified HCPCS code to bill for KEYTRUDA. • The infusion time corresponds to CPT code 96413. 10 11 12 13 9 10 11 12 13 14 14 15 15 16 16 17 17 18 18 19 19 20 20 21 21 22 22 PAGE 23 OF TOTALS CREATION DATE 50 PAYER NAME 52 REL. INFO 51 HEALTH PLAN ID 53 ASG. BEN. 23 55 EST. AMOUNT DUE 54 PRIOR PAYMENTS 56 NPI A 57 A B OTHER B PRV ID C Locator 66 C 58 INSURED’S NAME • E nter appropriate ICD-9-CM diagnosis code(s). A B C 62 INSURANCE GROUP NO. 61 GROUP NAME 59 P. REL 60 INSURED’S UNIQUE ID A B C 65 EMPLOYER NAME 64 DOCUMENT CONTROL NUMBER 63 TREATMENT AUTHORIZATION CODES A A B B C C 66 DX 67 I A J 69 ADMIT 70 PATIENT DX REASON DX PRINCIPAL PROCEDURE a. 74 CODE DATE B C D LocatorE80 F K L N O M a Enterb the following: c a • D rug name: [KEYTRUDA (pembrolizumab)] • R oute of administration • N DC: 0006-3029-02 • T he dosage provided OTHER PROCEDURE CODE DATE b. OTHER PROCEDURE CODE DATE e. 71 PPS CODE OTHER PROCEDURE CODE DATE G P b 72 ECI 75 76 ATTENDING NPI LAST c. OTHER PROCEDURE CODE DATE d. OTHER PROCEDURE CODE DATE 77 OPERATING UB-04 CMS-1450 81CC a APPROVED OMB NO. 0938-0997 78 OTHER b LAST c 79 OTHER d LAST NUBC ™ National Uniform Billing Committee 68 73 QUAL FIRST NPI LAST 80 REMARKS H Q c QUAL FIRST NPI QUAL FIRST NPI QUAL FIRST THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. The suggestions contained on this form are compiled from sources believed to be accurate for the Medicare Part B program, but Merck makes no representation that the information is accurate or that it will comply with the requirements of any particular Medicare Administrative Contractor (MAC) or payor. You are solely responsible for determining the billing and coding requirements applicable to any payor or MAC. Diagnosis codes should be selected only by a health care professional. The information provided here is not intended to be conclusive or exhaustive, and is not intended to replace the guidance of a qualified professional advisor or any instructions provided by a payor or MAC. Billing and coding requirements may vary or change over time, so it is important to regularly check these requirements with each payor or MAC. Merck makes no warranties or guarantees, expressed or implied, concerning the accuracy or appropriateness of this information for your particular use and cautions that changes in public and private payor billing requirements occur frequently. The use of this information does not guarantee payment or that any payment received will cover your costs. ONCO-1108274-0011 08/14








© Copyright 2026