
Document 307117
Clinic Intern Manual Fall 2014 1 CLINIC MANUAL Clinic Guidelines National University of Health Sciences 200 E. Roosevelt Road Lombard, Illinois 60148 www.nuhs.edu Revised: August 2014 by: Theodore L. Johnson, Jr., DC, MS Disclaimer: The university reserves the right to make changes as required in course offerings, curricula, academic policies, and other rules and regulations affecting students. Although this manual intends to reflect current policies, rules and regulations, students are cautioned that changes or additions may have become effective since the publication of this material. 2 Table of Contents NUHS Mission and Goals .............................................................................................................. 5 Introduction .....................................................................................................................................7 Chapter 1: Rules and Regulations ...................................................................................................9 Chapter 2: General Clinic Rules ...................................................................................................19 Chapter 3: Charting .......................................................................................................................29 Chapter 4: Phlebotomy Procedure ................................................................................................39 Chapter 5: Patient Care .................................................................................................................47 Chapter 6: Outcome Disability Questionnaires ............................................................................57 Chapter 7: Clinic Disciplinary Protocols ......................................................................................59 Chapter 8: Incident/Accident Report Procedure ...........................................................................63 Chapter 9: OSHA Training and Compliance ................................................................................65 Chapter 10: HIPAA Training and Compliance .............................................................................79 Chapter 11: Business Office Procedures .......................................................................................85 Chapter 12: Clinic Community Outreach Events ..........................................................................87 Chapter 13: Clinical Clerkship Program ........................................................................................91 Appendix .......................................................................................................................................95 A – CCE Standard H: Educational Requirements for DC Program .............................................97 B – College of Professional Studies Competencies ....................................................................105 C – Quantitative Requirements for Graduation ..........................................................................107 D – Clinic Internship I Syllabus .................................................................................................109 E – Clinic Internship II Syllabus..................................................................................................115 F – Clinic Internship III Syllabus ...............................................................................................121 G – Abbreviations .......................................................................................................................127 H – DC Intern Weekly Tally Sheet .............................................................................................129 I – Equipment Damage and Repair Form ...................................................................................131 J – Clinic Outreach Record .........................................................................................................133 K – Clinic Community Outreach Hours Form ............................................................................135 L – Accident / Incident Report.....................................................................................................137 M – Supervisor’s Accident / Incident Report ..............................................................................139 N– Clinical Clerkship Qualifications & Application Requirements ..........................................141 O– Ancillary Clinical Experience (ACE) Basics ........................................................................143 P – Clinical Based Internship (CBI) Basics ................................................................................145 Q – Request for Independent Clinic Observation .......................................................................147 Student Intern Non-Solicitation Agreement ...............................................................................149 Signature Page ............................................................................................................................151 3 4 Mission Statement Because: • We value students as unique individuals seeking quality health sciences education through our service and support; • We value being progressive, knowledgeable, adaptable, original, and academically sound in our academic programs; • We value the substantive quality of our curricula through emphasis upon academic excellence; • We value progress achieved by the development of new knowledge and its importance to chiropractic medicine and other complementary healing arts and sciences; • We value quality training and practice in the clinical skills of all relevant programs with particular emphasis upon the physician/patient relationship within the first professional programs; • We value complementary and alternative care for its emphasis upon holism and use of the least invasive therapeutic procedures necessary for optimizing human health; • We value collegiality and cooperation among all members of the University community, the related professions, other health care systems, and the community; Therefore: The mission of National University of Health Sciences is to provide and promote the necessary leadership, management and resources for the advancement of education, new knowledge, outreach, and the ethical practice of the healing arts and sciences as taught within the programs of this University. Institutional Goals I. By 2015, to continue development of a stronger financial position for the University. II. By 2015, to develop and graduate physicians and other health care practitioners who, because of the NUHS integrative education model, enthusiastically, confidently and collegially promote integrative practice in their respective healing art and science. III. By 2015, to continue expansion of educational program diversity. IV. By 2015, to strengthen our position as a recognized, dynamic leader in education and research germane to the primary care, “whole health healing” role of natural medicine physicians and other health care providers. V. By 2015, to develop, expand and promote greater cultural authority for our graduates. Approved by the NUHS Board of Trustees, November 2011 5 6 Introduction The Clinic Manual is the resource for general information regarding clinic activities, rules and regulations that affects everyone. In order to maintain consistent behavior, appearance and service, we ask that all students and clinicians abide with the standards provided in this manual. During the last three trimesters at National University of Health Sciences, interns will receive mentoring in a clinical setting. This is where students integrate the classes they have taken to date. Through direct patient contact, interns grow into the role of a chiropractic physician. This period is divided into three trimesters of outpatient operations. The outpatient clinics are clinical settings under the authority of the Dean of Clinics and directly overseen by the Chair of Clinical Practice. They are staffed by chiropractic physicians chosen for their years of experience in a variety of settings. Students entering the 8th trimester are gradually integrated into the clinic system and are stepwise given increasing levels of patient care responsibilities, as determined by their supervision clinician. They are rewarded with the inherent satisfaction of applying their learned basic and clinical science knowledge and skills to patient care, while at the same time learning to shoulder the concomitant responsibilities, in the role of student doctor. Even though the 8th Trimester Clinic Internship is the first clinical setting in which the student doctor will function, the demands and responsibilities are no less than in any of the subsequent internships in which the student doctor or intern will have duty. Every effort must be made to develop the proper attitudes, habits and skills necessary to effectively deliver health care. During the 9th and 10th trimester internships, those skills developed during the prior trimester will be used to treat patients from a broader spectrum of the general public. The clinicians will continue to work to enhance and deepen the interns’ understanding and challenge them to continue their growth. National University of Health Sciences wants its students to graduate with the confidence that they have what it takes to be a successful doctor of chiropractic in every sense. The clinics give interns that opportunity. In the Appendixes of this document will be found the parameters of intern assessment, requirements for graduation and the respective syllabi for the last three trimesters at National University of Health Sciences. 7 8 Chapter 1 Rules and Regulations These rules and regulations are designed to help the NUHS clinics run smoothly and efficiently. Always remember that the clinics represent the largest area of public relations in the University. The impressions that patients carry away about the University and the profession are determined to a large extent by their experiences within the clinics and their environs. These impressions are based in large part on personal interactions with interns, attending clinicians and office staff. Attempts must be made to make these experiences as pleasant as possible. Everyone involved in the clinic is expected to adhere strictly to clinic rules and regulations. Professional Attitude A positive professional attitude is an integral part of a chiropractic physician’s “armamentarium” or tool kit, and it is essential that it matures during the intern’s time in the clinic. Professional attitude is composed of many things, and is judged collectively under the category of professional conduct. Attitudes: • • • • Toward colleagues and other professionals Toward the patient/client Toward the support staff Toward other professional programs Personal Hygiene Keep the use of cologne or perfume to a minimum. Dress Patients prefer conservative rather than contemporary avant-garde styles. Male interns are expected to wear a shirt, tie and clean well-pressed dress pants. Dress shoes or boots are acceptable; sandals or sports shoes are not. Hairstyle and beard should be conservative, clean and tidy. Beards can be grown on vacation, but should not be started while the intern is assigned to clinic duties. Long hair must be pulled back and secured so as not to fall into the eyes or interfere with rendering of treatment to the patients. Body piercing jewelry should be removed when on duty, if possible. Otherwise, they must not be dangling or otherwise interfering with patient care. 9 Female interns are expected to be dressed neatly; no jean style pants are permitted. Hem lengths between mid-calf and 1" above the knee are acceptable. Spandex or other body-conforming clothing is unprofessional and inappropriate in the clinics. Conservative necklines are expected. Makeup should not be excessive. Hair should be clean and neat. If long, it must be tied back or pinned up. Body piercing jewelry that is visible is to be of a conservative nature with no dangling items. All interns are expected to wear a clean, well-pressed, white, long-sleeved clinic jacket that displays the intern’s name. The clinic jacket must be worn at all times when within the confines of the clinic, and may be removed only when in a treatment room rendering treatment. The jacket must be worn in any area where patients or the public may see the intern. Well-trimmed and clean nails are essential. Jeans, denim outfits, stretch pants, sweat-pants/shirts, and fleece materials, shorts, Spandex, and similar outerwear are unacceptable. The intern must follow all the dress code rules and it is the decision of the attending clinician if the intern is appropriately attired for clinical duties. If not, the intern will be sent home immediately and must make up the clinic shift at another time when they comply with the dress code rules. Smoking and Alcohol Smoking is not permitted within the confines of the clinic. Interns shall not smoke immediately prior to working with a patient. Alcoholic beverages are not permitted in the clinic. Interns shall not consume alcohol prior to working with patients; clinicians are authorized to suspend interns with alcohol on their breath from patient care. For further information, refer to the NUHS “Alcohol and Drug Policy.” Weapons Weapons of any variety are not permitted in any part of the clinic. Use of Telephone Because of the large number of employees and interns using clinic facilities, it is necessary to restrict telephone access for personal use. Personal calls on clinic phones for or by interns will not be permitted except in emergency situations. Calls to patients concerning clinic business can be made using a clinician’s telephone line, providing the clinician has authorized this. All clinic phone lines have detailed logs, which track all calls. Any call on a clinic phone that is not directly verifiable to patient care will be billed to the intern. Nametags Nametags are worn by all clinic personnel, including interns, so that all personnel are readily identifiable. Intern nametags must not include the term Dr., DC, ND, or LAc. Acceptable nametags include picture identification attached to the clinic jacket or an intern tag engraved by an outside supplier. 10 Manners of Address When speaking to a clinician, use appropriate speech for the nature of the relationship between an intern and the doctor overseeing the care you provide. Use the more formal title when asking a question of a clinician, i.e., “Dr. Smith, do I have your permission to treat my patient John as we discussed?” Informal or more causal expressions are discouraged, i.e., “Hey Doc, what day is the final?” The clinicians are not your peers, so the nature of your speech should reflect that fact. When addressing an older or senior patient for the first time, it is respectful to address them with “Ms., Mrs. or Mr.,” rather than “Jane or John.” Ask patients that you are seeing for the first time what their address preference would be. This simple gesture could save you a lot of embarrassment. Business Cards Since interns are working under the licensure of their clinician, the University provides clinicians with business cards to distribute to their interns. The front of the cards contain the clinic name, phone and fax numbers, the clinician’s name, and a line on which the intern can write their name; the reverse side lists the NUHS clinics and addresses. These cards also serve as a tool for the interns to use in patient recruitment. The University does not allow the use of any other business cards by interns. Any questions regarding business cards should be directed to the clinician and/or the dean of clinics. Advertising The University grants limited use of its logo, name and identifying information. This information may not be used in any advertising without the expressed consent of the University. The Office of the Dean of Clinics grants this consent. Each clinician must review all proposed advertising and forward said copy to the Dean for approval. At no time will consent be given for individual interns to advertise their services to any outside party, without the consent of the University. The University will promote clinics within its system and not individual interns. Interns are not allowed to advertise individually. Patient Recruitment Each intern is required to recruit patients to the attending clinician’s practice. The University does not guarantee that each intern will see the same quantity or quality of patient. The recruitment of patients by the intern is a valuable experience to be gained. The clinic system will experience fluctuations in patient volume depending on economic factors, weather and normal patterns, generally seen in private practice. It is imperative that interns learn techniques to recruit patients throughout their internship. No one can guarantee what the marketplace will present at any given time and the intern must be adaptable to those changes. The University will teach and guide the intern through proper patient recruitment techniques. Cellular Telephones The University recognizes the need and convenience of cellular telephones. However, during the duty shift, an intern may not have their cellular telephones turned on within the confines of the clinic. They may use them outside of the clinical treatment room and most preferably, outside the clinic building. Students should not talk on their cellular telephones in any clinic hallway nor 11 bring cellular telephones into treatment rooms with patients, to avoid them ringing/vibrating and disrupting normal clinic activities. Cellular telephones must be turned off and/or not brought to clinic preview and review sessions. NUHS Whole Health Center - Lombard Dean of Clinics: Theodore L. Johnson, Jr., DC, MS 630-889-6513 [email protected] Chair of Clinical Practice: Manuel Duarte, DC, MS, MSAc, DACBSP, DABCO 630-889-6525 [email protected] Clinicians: Brian Anderson, DC Denise Piombo, DC Anna Jurik, DC Tari Reinke, DC Angie Skokos, DC 630-889-6464 630-889-6443 630-889-6823 630-889-6662 630-889-6459 [email protected] [email protected] [email protected] [email protected] [email protected] 630-889-6851 [email protected] Clinic Services Manager: Jean Fairbank Clinic Hours: Monday-Friday: 7:00 a.m. - 7:00 p.m. Monday-Friday (mid-shift): 9:00 a.m. - 3:00 p.m. Saturdays: 7:00 a.m. - 12:00 p.m. Clinic Phone: 630-629-9664 Clinic Website: http://clinicalinfo.nuhs.edu You will find forms of documents you will use in the clinic and an online Student Manual. New Patient Visits—Lombard Chiropractic AM Shift The last appointment for which new or re-examination patients can be scheduled is 11:45 a.m., Monday-Friday. The front desk is to inform the new or re-examination patient that the paperwork can be completed PRIOR to the initial visit (forms can be obtained online at www.nuhs.edu); or, the new patient must be informed to arrive at the clinic 15-20 minutes prior to their set appointment for the purpose of completing the paperwork. By having the paperwork ready prior to the set appointment, more time will be made readily available for the patient and clinician/intern. 12 During the initial visit, an intake will be obtained which will include a consultation and physical exam. Depending on time constraints, lab and/or imaging may be performed as well. Any report of findings and treatment will be discussed on the next visit. Chiropractic Mid-Shift The last appointment for which new or re-examination patients can be scheduled is 1:45 a.m., Monday-Friday. The front desk is to inform the new or re-examination patient that the paperwork can be completed PRIOR to the initial visit (forms can be obtained online at www.nuhs.edu); or, the new patient must be informed to arrive at the clinic 15-20 minutes prior to their set appointment for the purpose of completing the paperwork. By having the paperwork ready prior to the set appointment, more time will be made readily available for the patient and clinician/intern. During the initial visit, an intake will be obtained which will include a consultation and physical exam. Depending on time constraints, lab and/or imaging may be performed as well. Any report of findings and treatment will be discussed on the next visit. Chiropractic PM Shift The last appointment for which new or re-examination patients can be scheduled is 5:45 p.m., Monday-Friday. The front desk is to inform the new or re-examination patient that the paperwork can be completed PRIOR to the initial visit (forms can be obtained online at www.nuhs.edu); or, the new patient must be informed that he/she can arrive at the clinic 15-20 minutes prior to their set appointment for the purpose of completing the paperwork. By having the paperwork ready prior to the set appointment, more time will be made readily available for the patient and clinician/intern. During the initial visit, an intake will be obtained which will include a consultation and physical exam. Depending on time availability, lab and/or imaging may be performed as well. Any report of findings and treatment will be discussed on the next visit. Snow Schedule The “Snow Schedule” applies in cases of inclement weather. Please check the website www.EmergencyClosings.com or go directly to the University website: www.nuhs.edu where information regarding a change in University and clinic hours will be posted on the homepage. Emergencies If an urgent need for care arises, the student should call the front desk in the Lombard Clinic at 630-629-9664 to make an appointment. The student will be seen in the clinic and an attending physician will assess the need for care. Under no circumstances can the intern treat a patient without the supervision of a clinician. • IF YOU HAVE WHAT YOU BELIEVE IS AN EMERGENCY – CALL 911 — OR GO TO THE NEAREST EMERGENCY ROOM * 13 Caruth Health Education Center (Florida) Dean of Clinics: Theodore L. Johnson, Jr., DC, MS 630-889-6513 [email protected] Chair of Clinical Practice: Manuel Duarte, DC, MS, MSAc, DACBSP, DABCO 630- 889-6525 [email protected] Clinician: W. Scott Harrison, DC 727-341-3769 Clinic Phone: 727-341-3760 [email protected] Clinic Services Manager: Jean Fairbank 630-889-6851 [email protected] Clinic Hours: Monday: 8:00 a.m. - 4:00 p.m. Tuesday: Noon - 7:00 p.m. Wednesday: 8:00 a.m. - 3:00 p.m. Thursday: Noon - 7:00 p.m. Friday: 8:00 a.m. - 2:00 p.m. Saturday & Sunday: Closed NUHS Whole Health Center - Pinellas Park Clinic (Florida) Dean of Clinics: Theodore L. Johnson, Jr., DC, MS 630-889-6513 [email protected] Chair of Clinical Practice: Manuel Duarte, DC, MS, MSAc, DACBSP, DABCO 630- 889-6525 [email protected] Clinician: Mohsen Radpasand, MD (Iran), DC 727-873-7870 [email protected] Clinic Hours: Monday: 11:00 a.m. - 6:00 p.m. Tuesday: 8:00 a.m. - 3:00 p.m. Wednesday: 11:00 a.m. - 7:00 p.m. Thursday: 8:00 a.m. - 3:00 p.m. Friday: Noon - 6:00 p.m. Saturday & Sunday: Closed Weather Emergencies Weather radios have been provided to each SPC college site to alert employees and students that severe weather (thunderstorms, high winds and tornadoes) may be approaching. This system is 14 designed for early evacuation of portable buildings and similar vulnerable areas before the approach of high winds, tornadoes or other severe weather. The radios receive weather warnings and emergency broadcasts from the National Weather Service. Tornado Safety Tornado Watch: Conditions are favorable for tornados to form. If you are in a portable building or trailer, prepare to relocate to a permanent building. Tornado Warning: A tornado has been spotted in your area. Tornado warnings will be announced by e-mail and verbal communications. When a tornado warning is issued, all attention should be directed toward protecting life, not property. 1. If you are in a portable building or trailer, move to a permanent building. 2. Do not seek shelter in a gymnasium, auditorium or similar type of building with a freespa roof. 3. If you are on an upper level of a multi-story building, move to a lower level. 4. Stay away from exterior walls, doors, windows and items that might fall from above. 5. Move to an interior area of the building and take cover under a sturdy object or next to an interior wall. Cover your head and face with your hands and arms. Tropical Storm / Flood Threat / Hurricane Threat When St. Petersburg College closes because of a tropical storm, rain or flooding, or hurricane threat, the following activities must be completed by each department before releasing faculty and staff: 1. Monitor the radio/television for additional information or call the college information number at 727-341-4772 or 866-822-3978. Additional information can be found at the SPC disaster preparedness site — www.spcemergency.wordpress.com. 2. Back up computer hard drives. Secure disks, CDs and DVDs in zip-lock bags or move off site. 3. Unplug computers, printers and other electrical appliances. 4. Move contents from bottom drawers of desks and file cabinets in case of flooding. 5. Move all equipment, books, papers and other valuables off the floor in case of flooding. 6. If necessary, relocate equipment, books, papers and other valuables off the floor in case of flooding. 7. If relocation to a higher floor is difficult or impossible, cover and/or seal equipment and other valuables with plastic. 8. In lab areas subject to flooding, store sensitive apparatus and glassware. 9. Attend to critical utility-dependent processes and make arrangements for back-up supply. 10. Ensure all hazardous chemicals and biohazard materials and wastes are properly protected. 11. Check contents of refrigerators and set to coldest settings. 12. Empty trash receptacles of items likely to rot. 13. Take home all personal items of value. 14. Close and latch all windows. Close and lock all doors. 15 In addition, in case of a hurricane threat: 15. Move all equipment, books, papers and other valuables away from windows, off the floor and to interior areas of the building. Be sure that equipment and other valuables that are moved outside your office are tagged for easy identification and retrieval. 16. Clear desktops, tables and exposed horizontal surfaces of materials subject to damage. 17. Close and latch all filing cabinets. Time Off Each intern is allowed three (3) days per trimester of “release time.” The release time is not cumulative and is forfeited at the end of each trimester if it is not used. This release time may be used for any reason, such as: 1) personal time, 2) illness, or 3) licensure examinations. If emergency or sickness occurs, it is the intern’s responsibility to either email or phone their clinician and inform them of their absence. In this manner, appropriate accommodations can be made or arranged for their scheduled patients. Contact with the clinician must be made within 15 minutes of the start of the intern’s shift. If the intern who will be absent that day does not notify the clinician within this allowed time, this will be considered an “unexcused absence.” An unexcused absence requires 2 make-up shifts for every 1 clinic shift that has been missed and considered unexcused. Furthermore, a shift must be made up in its entirety from the beginning until the end, i.e., 7 a.m. to 1 pm. or 1-7 p.m., and during a non-assigned shift. No partial hours will be allowed to be made up on various clinic shifts. Finally only 1 missed seminar is allowed throughout the trimester. If the clinician is not notified within the 15 minutes allowed time by the intern who will be absent that day, this will be considered an “unexcused absence” and will require 2 hours make-up time. Again, make-up time for seminars must be made up during a shift for which the intern is not scheduled. Release time must be requested and signed off in advance by filling out a “Request for Time Off” form. The forms are available from the clinician. The form must clearly identify the intern, the date(s) requested, and make-up time (if required). Both the intern and clinician must sign the form and a copy must be filed in the intern’s clinic performance file. When the make-up shift is completed, the clinician must sign off next to the make-up date. Make-up shifts must be completed within two weeks of the missed clinic shift. These personal days must be made up by serving shifts at times other than those regularly assigned to that intern. Additional time beyond the three non-personal days per trimester must be made up after the Saturday prior to “Pink Slip Day,” unless other arrangements have been approved by the Chair of Clinical Practice or Dean of Clinics. Pink slips indicating completion of requirements for exiting the clinics (graduation) will be withheld until the additional duty is served. Extended absence for military duty must be arranged with the Dean of Clinics or his designee. Absences in access of the policies noted above will be reflected in the portion of the intern’s clinic grade that addresses participation. Frankly, clinic is a “hands-on” experience that requires interns to be present. It is contact with patients that makes the doctor, hence the strict rules regarding attendance. More information concerning the participation section of the respective syllabus for each trimester can be found at the end of this manual in the Appendix. 16 Special Clinic Support Assignments The operation of a professional practice requires attention to a number of mundane daily tasks that impact upon the public image and impression of the clinic. Support functions of this kind are generally carried out at the beginning or end of each business day. At the discretion of the clinic director, various support tasks may be distributed among all interns including laundry (washing, folding and storing gowns and towels), discarding face paper after treating a patient, replacing the face paper once it empties, etc. Your willingness to carry out these functions will also be reflected in the degree to which you will be graded on participation. Lombard Clinic Internship I Interns Only A mandatory all-day trip and tour of the factory of Standard Process Inc. is scheduled for 8th Tri students. The date will be announced to the class once it has been finalized. The bus ride between Lombard and Palmyra, Wisconsin, takes approximately two hours each way. The bus is equipped with a bathroom and air conditioning. Standard Process will provide lunch. • • • • All students must ride the bus both ways. All students must be on time for the bus, as the bus will leave at the designated time. The bus will not pick up late students at any other location on the way to Wisconsin. Dress is business casual, no shorts or tank tops. While at Standard Process, professional decorum is expected. Students must attend the Standard Process tour when their class is scheduled. If they do not attend, they must make it up as an absence. If they attend the following trimester, they are forgiven the absence. If they refuse to sign the waiver, they will sit in the cafeteria of the Lombard clinic for the entire duration of the trip or be counted absent. Florida Interns Only NUHS/SPC interns participate in clinic lectures. Intern Observations Interns may choose to go on observations with doctors of their choice for a total of up to 10 days. They may do so in their 10th trimester after all their clinical requirements for graduation are completed, submitted and approved by their Clinician, the Clinic Services Manager, and the Dean of Clinics. Interns must complete the “Request for Independent Clinic Observation” form, which can be found on the website: http://clinicalinfo.nuhs.edu or obtained from Clinic Services Manager Jean Fairbank. A copy of the doctor’s license must be attached to the form. Deadline for completion of observation paperwork must be completed by the third Thursday prior to graduation. See Appendix R. Pink Slip Day Pink Slip Day is the same day as graduation rehearsal. Students must present their Pink Slip at graduation rehearsal. 17 One week prior to Pink Slip Day, all graduating 10th Trimester students must check in with Clinic Services Manager Jean Fairbank to make sure all Quantitative Requirements for Graduation have been completed and received, and that all clinic accounts have been paid. Note: Just because the ECQES requirements have been met does not mean that the hard copy has been received by Jean Fairbank. Pink slips will not be issued until all requirements have been met and paperwork received. 18 Chapter 2 General Clinic Rules General Rules The Clinic is the primary health care service for the students of NUHS. Eighth, ninth and tenth trimester interns render care, acting at all times under the supervision and license of the attending physicians. The Lombard Clinic is located on the main floor of Building B, the Howard-Schulze Building and Clinic. The Florida SPC Clinic is located on the main floor of the Orthotics and Prosthetics Building of the SPC Caruth Health Education Center. Eligibility All registered students of National are eligible for care in the Clinic. Additionally, the student’s spouse and children are eligible to receive care. If the spouse or child of a student cannot come to the Clinic during its normal hours of operation, they may be referred to the main clinic. Students of NUHS and student dependents are eligible for complimentary treatment including chiropractic adjustments and therapies and the first pair of orthotics. However, these individuals will be charged for any procedures involving diagnostic imaging (i.e., X-rays are $5.00/film) and lab work. Services and Fees A full scope of diagnostic and therapeutic services is available in the main clinic. Any patients being seen in main clinic will be charged the normal fee schedule either directly or to their insurance. See Route Slips in each location for details on services and fees. Clinic Freshman Physicals – Lombard A physical examination is required of all first trimester DC, ND and MT students. DC and ND students must complete all aspects of this examination prior to registration for Trimester Two. MT students may schedule an appointment in the main clinic with the approval of the Massage Therapy Clinic supervisor. Part-time students in the Prerequisite Program or Bachelor’s Program do not require a freshman physical. First trimester students presenting to the clinic are not required to have completed the physical prior to care being instituted. They should be advised that they need to complete the freshman physical in a timely manner, but they will receive care, if needed. The freshman physical examination consists of a comprehensive health history, a physical examination (vitals, head, neck, eyes, ears, nose, throat, chest, abdomen, neurological, male 19 genitalia, female pelvic exam, and chiropractic spinal analysis) and a report of findings. A urinalysis and complete blood count is required for student in the Doctor of Chiropractic Medicine Program. Any CBC and UA performed for the purpose of the freshman physical is at no charge; any additional lab work or X-rays may be recommended, if clinically indicated, at the student’s expense. For female students, a breast examination and genital/pelvic examination are part of the routine freshman physical, however, a Pap smear is not unless clinically indicated. (Pap smears are available if requested at University cost). If the student has had a breast and genital/pelvic examination within the last year, or chooses to see another physician to have it completed, she must have the doctor fax copies of the medical records including findings to the attention of the Clinic at 630-889-6800. Freshman Physicals – Florida A physical examination is required of all first trimester DC students. DC students must complete all aspects of this examination prior to registration for Trimester Two. The freshman physical examination consists of a comprehensive health history, a physical examination (vitals, head, neck, eyes, ears, nose, throat, chest, abdomen, neurological, male genitalia, female pelvic exam, and chiropractic spinal analysis) and a report of findings. A urinalysis and complete blood count is required for student in the Doctor of Chiropractic Medicine Program. Any CBC and UA performed for the purpose of the freshman physical is at no charge; any additional lab work or X-rays may be recommended, if clinically indicated, at the student’s expense. For female students, a breast examination and genital/pelvic examination are part of the routine freshman physical, however, a Pap smear is not unless clinically indicated. (Pap smears are available if requested at University cost). If the student has had a breast and genital/pelvic examination within the last year, or chooses to see another physician to have it completed, she must have the doctor fax copies of the medical records including findings to the attention of SPC Clinic at 727-302-6610. Supervision The attending physicians at the University clinic are responsible for all decisions relating to the care provided to the patients. The interns are under the constant and close supervision of the attending and are permitted to perform only those procedures approved by the attending physician. In addition, a detailed treatment plan must be completed within the same visit and signed by the physician/clinician on shift. This insures continuity of care over the various physicians who serve in the main clinic. Any questions regarding health issues or management should be discussed with the attending physician. Interns in the eighth, ninth and tenth trimesters are to provide recommendations and care only under the attending physician and only in the University clinics. Care should not be rendered in the dormitories, classrooms or any other sites. 20 Clinic Rules and Regulations Clinic interns work under the attending clinician’s license. The patients are the responsibility of the licensed physician. On initial presentation with the patient, interns should bring a single sentence S (subjective) in writing, on the progress note, to the clinician to begin the patient visit. For example: Patient returns for continuing care of his elbow complaint and states that he is doing much better. More history may be obtained and included in the subjective after the initial presentation to the clinician. Interns SHOULD NOT complete an extensive history or start examination or treatment without consulting with the clinician. A Treatment Plan (green sheet) is needed in order to treat any condition. Therapies performed are to be ONLY those listed on the Treatment Plan including manipulation to a specific area, physiotherapy per the settings recommended and rehabilitation as recommended, and patient education. Perform ONLY those things and everything listed on the Treatment Plan. Should the plans need to be modified they should be discussed first with the clinician and changed on the Treatment Plan. Before commencing with treatment, patients should be informed of the condition being treated and the treatment plan, and must consent to treatment. This is referred to as “report of findings.” Prior to instituting therapy, the patient should be advised of the treating diagnosis, the treatment plans, and goals. The benefits, alternatives and risks to care also should be discussed. Patients should be asked if they have any questions. Finally, the patient must be formally asked they consent to care. This whole process of informed consent must be completed prior to starting care and should be recorded on the progress note and appropriate check boxes on the Treatment Plan. If any time plans are changed, they should be recorded. Patients should not be discharged without the clinician’s approval. The clinician needs to know the status of the patient prior to discharge. Interns should not write on the Treatment Plan unless instructed to do so by the attending clinician. These issues should be discussed prior to writing in the patient’s file. On the progress note, interns should record the EXACT treatment performed for that visit under the Treatment Plan. Included should be: areas adjusted and techniques used; physiotherapy applied with the specific setting used; specific rehab performed; any patient education given to the patient during the visit or those to be explained in the future. Essential HIPAA Compliance On the initial visit to the clinic, the student must fill out a Financial/Treatment Consent form and be provided a copy of the Practice Privacy Policy. The student must initial the portion of the Financial/Treatment Consent form that states they have been provided with a copy of the Practice Privacy Policy. The student should not be seen unless this has been accomplished. A copy (yellow) of the Practice Privacy Policy is to be delivered to the main clinic desk at the end of the shift, with the white copy placed in the patient’s file. 21 It is not appropriate for an intern to read a patient’s file if they are not involved in the case. Do not discuss information with those not involved in clinic care. Do not discuss information outside of clinic, or in classes where the patient’s right to privacy may be violated. Disciplinary actions may result if the intern fails to comply. Intern Reminders • Do not leave patient files unattended (especially in the patient’s room). • Do not examine or treat a patient through street clothes. • Clinic Route Slip – Lombard: An NUHS routing sheet must be filled out with each patient visit. (See example in Appendix.) The main clinic desk will note the patient’s name and date at the top of the sheet. The intern’s name and the clinician’s name must added. Please record the therapy procedures rendered (CPT codes) and the diagnostic code (ICD). Include the patient’s next recommended visit (NPV). The attending clinician must sign. The intern should escort the patient to the front desk after the visit. The patient must turn in the NUHS route slip at the main clinic desk at the end of each visit, and if any services were rendered that require payment, handle prior to leaving. • Clinic Route Slip – Florida: An NUHS routing sheet must be filled out with each patient visit. (See example in Appendix.) The intern needs to note the patient’s name and date at the top of the sheet. The intern’s name and the clinician’s name must be included. Please record the therapy procedures rendered (CPT codes) and the diagnostic code (ICD). Include the patient’s next recommended visit (NPV). The attending clinician must sign. The intern should escort the patient to the front desk after the visit. The patient must turn in the NUHS route slip at the main clinic desk at the end of each visit, and if any services were rendered that require payment, handle prior to leaving. • Outcome Assessment Form: Patients must fill out the appropriate outcome assessment form(s) prior to beginning the history and exam. This must also be done at every reevaluation and with a new chief complaint, which will then go into the patient’s file. • Intern Tally Sheets: Intern All NUHS interns are required to keep their clinic numbers recorded on Tally Sheets. Tally Sheet forms can be found on http://clinicalinfo.nuhs.edu. All Tally Sheets must be readable, and all back-up paperwork needed to support the work done must be attached. Back-up paperwork cannot be handed in after the Tally Sheet has been entered into ECQES. See Appendix G. The intern is responsible for the accuracy of this record, and entering the data from the tally sheet into ECQES on a weekly basis. After the intern has entered the data, they should submit their tally sheet to their clinician. The clinician will electronically review, modify, and except the tally sheets weekly. After the clinician has accepted the tally sheet, it will be submitted to the Clinic Services Manager, Jean Fairbank, for record storage. Periodic audits of intern tally sheets will be performed to ensure accuracy of ECQES data. 22 All NUHS interns will receive the information on how to enter their tally sheet data into ECQES at the beginning of Clinic Internship I (eighth trimester). This will be the same logon information, as they will need for the Audit system. Protocols • Only those techniques taught in the core curriculum at the National University of Health Sciences are to be used in this clinic. • Universal Precautions are to be exercised at all times. (Please refer to Infection Control Procedures in the Clinic Manual or check with the NUHS OSHA compliance officer.) • Interns should not leave the clinic area without notifying the attending clinician. • Interns should not leave the clinic until the patient’s file(s) has been completed. • Interns should sign out under THEIR OWN NAME at the end of the shift with the clinician’s approval. • Interns should not treat any patients without informing the attending clinician. • Interns should be prompt for their scheduled shift and arrive a few minutes early, if possible. Patients can be seen more promptly if the intern is prepared for the visit. Intern evaluation sheets may reflect tardiness as an unacceptable behavior. • Interns should not attempt to erase or “scratch out” any item in a patient’s file. Items to be deleted should have a single line placed through them and initialed. Anything that may have been “forgotten” may be added after the initialed SOAP note as an “addendum.” Interns should be sure to complete the SOAPs in a timely manner, the same day of the visit, preferably before the end of the shift. • Interns should remember when writing progress notes: if it is not recorded in the file you didn’t ask it, test for it, or do it. Duty Intern A Duty Intern is scheduled daily, Monday through Saturday, for each shift during clinic hours. The primary responsibility of the Duty Intern is to help promote positive relations between the patient and clinic. It is also felt that exposure to front desk operations will provide interns with valuable experience when it comes time to organizing the front desk area in their own offices and help them understand the need for orderly patient flow. Duty Interns cannot see nor treat patients that day. Duty Intern responsibilities include: 1. Arriving 10 minutes early; 2. Locating patient charts in Medical Records, and asking for the charts from the assistants in medical records; 23 3. Annotating any special equipment or treatment room needs (flexion/distraction table, etc.); 4. Greeting each patient in reception area; 5. Escorting the patient to the appropriate room; 6. Telling the patient to open the door slightly when gowned and ready; 7. Notifying clinician of patient’s arrival; 8. Being available to assist Front Desk/Support Staff when not escorting patients; 9. Noting in the medical file if a patient reschedules or did not keep his/her appointment and producing a Recall List at the end of the shift; 10. Bringing phone messages and rescheduling notes to a clinician as soon as possible; 11. Checking the intern room for neatness at the end of shift, sanitizing tables between patient visits and reminding colleagues to clean, if necessary, for the next shift. 12. Checking the patient rooms to be sure that there is lotion, gloves, tongue depressors, and any other pertinent supplies that may be required for use by the treating intern, and making sure the supplies have not expired. 13. Returning all charts to medical records at the end of the shift. Making sure that all charts are printed and signed by the treating intern, followed by a signature of the clinician. Making sure that the charts of patients who did not keep their appointments have been documented and signed by the clinician. 14. AM Duty Interns will pull all laboratory reports from the printer in the lab and sort by clinic and physician. A copy of each report is kept in the lab and filed in the appropriate clinic's folder. The Duty Intern will place all lab reports in the clinic mailbox and deliver reports to each Lombard clinician. 15. Anytime during the shift, the Duty Intern is to go to the lab, and each and every one of the treatment rooms located in the DC, ND, and AOM rooms of the clinic, and replace any filled biohazard red bins with new, clean bins, which are found in the storage room. The filled red biohazard containers should be sealed shut and placed into the biohazard boxes found in the lab. Be sure to ask the assistant(s) in Medical Records to unlock the room for the new biohazard bins, which are to be replaced in the room that had the previously filled biohazard bin. Remember: The primary role of a Duty Intern is to ensure maximum convenience to the patient. Courtesy is paramount. When greeting patients, the Duty Intern should use the following script: “Mrs./Mr. (etc.), I am intern _________. Dr.__________ will be able to see you in a moment. Please follow me.” If for any reason there is a disturbance, direct the patient to an available empty consultation room and summon the clinician or business supervisor immediately. The Duty Intern must not discuss the patient’s clinical condition. (Do not start a conversation with "How are you?" for example.) The Duty Intern must not discuss patients with staff; patient information is confidential. The Duty Intern must not make comments about patients, staff, interns, NUHS, policies, etc., in public areas. 24 Laundry Duties – Lombard Student Clinic has been given the responsibility of doing the clinic laundry on Mondays and Wednesdays. Main clinic performs this task on Tuesdays, Thursdays and Fridays. Laundry duties include washing, drying and folding any laundry from these days on both shifts. This applies to folding laundry found in dryers on Wednesday and Friday morning. Below are instructions for the clinic laundry. • Use the grocery carts or gown and towel carts to gather all gowns and towels located in the bins in the hallway by the PT room. • Take the dirty laundry to the basement. Turn left out of the elevator and go to the laundry room #102. To wash laundry, there are three washers. Two are silver commercial washers (first and third in the line of machines). For these two washers, just place laundry in the washers and press Start. Soap is automatically added! • For the standard washer (white washer in the middle of the line of machines), add one teaspoon of soap. The soap is in a 50-gallon drum on the right when you first walk in the room. Push the pump on the drum until the soap comes out. Be careful in case the blue soap splashes. Do not wear your white coat when dispensing soap! The washers all take about 20 minutes. Never leave wet laundry in the washers at the end of your shift! • To dry laundry, set the drying time to 50 or so minutes and set the cooling time to 15 minutes to prevent overheating! Dry the gowns and towels separately. • Fold the laundry when it’s done and put towels and gowns back in the spaces provided in the clinic halls. • Note: Massage Therapy and AOM are responsible for their own laundry and responsible for returning their sheets or blankets to their hallways. Laundry Duties – Florida The Florida clinic uses an outside laundry service. Interns need to sort used laundry into separate bags for gowns and towels. After laundry is returned, interns must restock the rooms with items. Working with Medical Records Lab work: • • • Interns must have a route slip for the student initialed by the clinician. If the student has never had lab work done previously, the intern will need their birth date. The intern must go to Medical Records first to pick-up the labels and requisition form before they begin any lab work on the student. 25 • • • The intern will need to know the name(s) for the test(s) they want to conduct. Medical Records can look up the price and CPT code. o If a test is not found, Medical Records or clinicians can check with the lab. Interns may not call the lab. o On the route slip, the Medical Records will always write the full amount. o Students pay half. If supplies are running low in the lab, interns must inform Medical Records. If there is a test that needs specific supplies, they can be ordered and should be arrive in about two days. Interns must inform the clinician and Medical Records. Supplements – Dispensary: • • • • • Supplements can only be purchased by students, who are under a clinician’s care and currently being seen in the clinic. The dispensary is now on an electronic scanning system. All supplements need to be scanned by a designated dispensary clerk or someone from Medical Records. NO SUPPLEMENTS MAY LEAVE THE ROOM WITHOUT BEING SCANNED. SUPPLEMENTS CANNOT BE TAKEN FROM THE DISPENSARY TO SHOW TO A PATIENT OR CLNICIAN. After the supplements are scanned, the name, price and quantity of each supplement will be written on the route slip. Refunds are given only on non-refrigerated items if they are returned within 7 days from the date of purchase. Refunds cannot be given on refrigerated items. Make sure the patient is willing to try the supplement before selling it to them. Multiple refunds to an individual patient will not be tolerated. Should an intern require a special supplement that is not in the dispensary inventory: o Their clinician must give approval to order the supplement; o Pre-payment must be received from the patient before the supplement is ordered; o The clinician is the only person who can give the special supplement to the person who orders the supplements. Files: • • • • • The Duty Intern picks up all files for their shift. If someone adds to the schedule, the Duty Intern will need to complete an Out-Guide slip. o The file number is the student/patient’s last name first, then the first name. o Their clinician is the clinician for that day. o The intern is the name of the intern who is seeing the student. o The date is the day the file is being removed. Some students go by different first and/or last names. If a student’s chart cannot be found, look under a married name or maiden name. If a student patient is a student dependent, Medical Records must be informed. Should a patient request copy of their X-ray report, lab work, or any part of their file, they must sign a Medical Release form that can be found at the front desk. Please refer to the front desk receptionist for such a form prior to giving out the requested documents. This also applies to any medical information to be sent to any other individual requesting medical records. 26 Equipment: • • • • All equipment must be signed out at the Medical Records window. The Equipment Sign-out sheet includes: o Date o Equipment removed o Intern/clinician’s name o Time removed When finished with equipment, it must be returned and the return time noted on the sheet. This applies to things such as the male/female models for proctologic or gynecology mock exams, icthemol, ear lavage equipment, acupuncture electric stimulation units, and anything that is found in Medical Records that requires signing out. If a piece of equipment does not work properly, you must do the following: o Tell Medical Records the piece of equipment is not working. Fill out an “Equipment Damage & Repair Form” found on http://clinicalinfo.nuhs.edu. See Appendix I. Have your clinician sign the form and put the original in the mailbox of the Administrative Assistant to the Dean of Clinics, Vicki Shargo. 27 28 Chapter 3 Charting Integral to good patient care is a system of record keeping which insures that all aspects of a clinical encounter is notated and consistent care can be rendered visit to visit. There is also the medical/legal aspect to documentation. This chapter reflects the evolution of charting at National University of Health Sciences, with an emphasis on a “whole person” concept of primary health care. With this in mind, here are the essential components of a chart: • History • Chief Complaint / Presenting Illness • Family History • Review of Systems / Past Medical History • Physical Exam • Laboratory Evaluation • Treatment Plan, including diagnosis • Report of Findings: A report on the patient’s overall health status • Progress Notes (SOAP) Here are some examples of the components noted above being considered in a variety of scenarios: • A family history of CV disease & a poor diet, which may generate a need for some life style changes. • A history of chronic mid-scapular pain and thoracic postural abnormalities noted on physical exam, which may be amenable to chiropractic care. • A family history of thyroid disease, history of chronic fatigue, and intolerance to cold may generate thoughts for further evaluation of the patient’s thyroid. • A history of fatigue, and glucose noted on the urinalysis should generate some thoughts for further evaluation. o A report on the lab work that was done should include a brief description of the test and what was learned. (Results should not to be reported as, “Your blood and urine are OK.” Consider reporting results in the following manner. “CBC: “These results rule out anemia and infection.” UA: “ These results speak against bladder, kidney problems.” 29 Abnormal findings may generate an entry on the Treatment Plan and/or the Chronic Problem sheet to address prevention of disease and care for conditions. In some case, the information gathered may trigger an entry on the Contraindications sheet (the top half of the Chronic Problem sheet). An example of this would be: • The patient is wearing a cardiac pacemaker. Interferential current would be deleterious in the extreme to this patient. • A DEXA scan shows that the patient has marked osteoporosis. High velocity manual manipulation would in all likelihood cause a fracture and therefore should not be performed. Incomplete Data Base: Once the incoming student has begun the evaluation, it is noted in the SOAP note for that date that the patient has an Incomplete Data Base (IDB). Until the report of findings has been given, this status will be in effect. When the IDB has been resolved, there will be another note in the record to reflect that fact. In all likelihood, the patient may be given a report of findings following the completion of the database. A patient presenting for a freshman physical that does not have a CC/PI will only need one sentence on the progress note stating: “Pt. presents for Freshman Physical, denies CC/PI.” When a patient has presented for a physical exam and also has an active problem for which they are seeking care, a precise description of that problem is written on this page. Use complete sentences, writing in paragraph form. Place the data in chronological order. Include the following: • Description of the onset and course of the problem • Location of the primary discomfort/problem and any radiation/referral of pain • Type of discomfort • Aggravating and relieving factors • Associated manifestations or constitutional symptoms • Previous treatment, including efficacy THE HISTORY Before beginning, insure the patient completes the Comprehensive Medical History form. Then in person, explore the details of their chief complaint, prioritizing from the most pressing concern and working towards those items with which they have less perceived unease. This is all documented on the front of the Chief Complaint/Hx of Present Illness form. Site Notice that on this form there is a small text box. This list of the various Intensity types of inquiries should act as both a starting point and give a checklist to Quality insure that an essential line of questioning is not missed. On the other hand, Onset this list alone does not constitute all that is required to complete an in-depth Radiation Aggravating Factors history. Remember that each answer the patient gives opens up a whole Alleviating Factors Associated Manifestations realm of other associated questions. An example would be asking the patient about an injury that occurred at work, which should then evoke a detailed description of the nature of their occupation and the challenges inherent in that work. 30 Once this is completed, move on to covering every positive response to the questions framed by the Comprehensive Medical History form, item by item. This gives you a chance to “connect the dots,” for not only do you need to follow up on any marked item, but also question in more depth those areas where, as a physician, you perceive a connection between a set of symptoms and possibly systemic dysfunctions. . There are also named items on the backside of this sheet to look at other general health related questions. If the patient is coming in for a freshman physical and presents with no chief complaint, first explore their lifestyle choices. This includes diet, exercise and sleep, how they are handling stress, and recent major life changes in enough detail to understand ways that you might improve their health during their tenure at the University. When you go onto the Comprehensive Medical History form, you may find that they indeed do have a recurrent or chronic complaint, but have become so acclimatized to its possible low-grade presence that they do not think to mention this issue in a health care setting. On the other hand, for at least half of our students, the care they receive from one of our interns is the first time they have been under chiropractic care. They may be unaware of the broad scope of what we treat as a profession, therefore discount health concerns, not knowing what might fall within the chiropractic scope of practice. Lastly, there is the Adult Preventive Health Record (APHR)form. This form allows you to record key examination procedures, which regardless of which profession is providing health care, should be checked on a regular basis as indicated. This form also includes various risk factors and the time you as the provider asked about them. Education is an essential element of the service we provide. A “whole person” approach to health care must include informing the patient of practices and behavior that could prove deleterious to them. The front of the chart should be stamped with the APHR grid, and the date of each exploration of this topic should be noted. THE PHYSICAL EXAMINATION When completing the physical examination, use the Comprehensive Exam 1 & 2 sheet to keep track of your findings. Remember to minimize patient movement. The form has been laid out to insure you are efficient in time management. You do not want your patient to have to stand-up, sit down, roll over, and then stand up again! It is disrespectful of the patient, they may be in pain and cannot tolerate all this movement, and your behavior will make you look like a disorganized amateur. When you have completed the examination you can take the information which you collect on the Comprehensive Exam 1 & 2 and write notes in the O: section of the SOAP note for this visit, outlining the highlights or positive findings of this process in summary. An example of this might be as follows: S: PP for initial visit evaluation for LBP of several years duration. See Hx form dated today for more details. Pt complete pain chart with analog pain scale. VAS=3-5/10, Oswestry LB=54 O: Performed both physical exam and lumbar regional (see forms dated today for details). Exam findings significant for the following: decreased L/S ROM; increase BP at 135/98 31 right; decreased gluteal strength both maximus and medius 4/5 b/L; provocative Kemp’s with non-radiating to the L4-S1 region; pain, palpable and tender b/L psoas muscle; and, mild Trendelenburg hip drop during gait. A: Based upon Pt’s symptoms and physical exam findings, Pt’s distress arising from facet syndrome, psoas myofascial pain syndrome, gluteal muscle weakness, and segmental dysfunction L/S. P: See treatment plan dated today for details of care. Presence of osteoporosis as noted on DEXA scan from Jan 11, 2006, dictates low force technique be used with no HVLA. If you were not able to complete the examination on a given day it is still important that you complete the objective portion of your SOAP note for that visit, showing what you did accomplished. From a medical / legal standpoint, if you pick up the examination on another day, show which sections of the Physical or Regional Examination form(s) were completed when. Draw a line, date it and indicate that all material that followed afterwards was completed at another time. Of course, the Physical and/or Regional Examination form(s) remain part of the record. Correct File Order The various parts of the patient’s file are placed in a specific order. Following is a diagram showing the correct placement of clinic forms. Note: When the file is opened, the two files that should be immediately visible are the Problem List on the left side and the latest Daily Progress Note (SOAP) on the right side. 32 THE PHYSICAL EXAMINATION When completing the physical examination, use the General Examination Findings sheet to keep track of your findings. Remember to minimize patient movement. The form has been laid out to insure you are efficient in time management. You do not want your patient to have to stand-up, sit down, roll over, and then stand up again! It is disrespectful of the patient, they may be in pain and cannot tolerate all this movement, and your behavior will make you look like a disorganized amateur. When you have completed the examination you can take the information which you collect on the General Examination Findings and write notes in the O: section of the SOAP note for this visit, outlining the highlights or positive findings of this process in summary. An example of this might be as follows: S: PP for initial visit evaluation for LBP of several years duration. See Hx form dated today for more details. Pt complete pain chart with analog pain scale. VAS=3-5/10, Oswestry LB=54 O: Performed both physical exam and lumbar regional (see forms dated today for details). Exam findings significant for the following: decreased L/S ROM; increase BP at 135/98 right; decreased gluteal strength both maximus and medius 4/5 b/L; provocative Kemp’s with non-radiating to the L4-S1 region; pain, palpable and tender b/L psoas muscle; and, mild Trendelenburg hip drop during gait. A: Based upon Pt’s symptoms and physical exam findings, Pt’s distress arising from facet syndrome, psoas myofascial pain syndrome, gluteal muscle weakness, and segmental dysfunction L/S. P: See treatment plan dated today for details of care. Presence of osteoporosis as noted on DEXA scan from Jan 11, 2006, dictates low force technique be used with no HVLA. If you were not able to complete the examination on a given day it is still important that you complete the objective portion of your SOAP note for that visit, showing what you did accomplished. From a medical / legal standpoint, if you pick up the examination on another day, show which sections of the Physical or Regional Examination form(s) were completed when. Draw a line, date it and indicate that all material that followed afterwards was completed at another time. Of course, the Physical and/or Regional Examination form(s) remain part of the record. Correct File Order The various parts of the patient’s file are placed in a specific order. Following is a diagram showing the correct placement of clinic forms. Note: When the file is opened, the two files that should be immediately visible are the Problem List on the left side and the latest Daily Progress Note (SOAP) on the right side. 33 LEFT SIDE TOP OF FILE RIGHT SIDE TOP OF FILE Problem List SOAP APHR Exam Med List CC/PI (Hx/pink form) Problem Management / Treatment Plan Hx Follow-up Miscellaneous Forms: Labs Imaging Release form Demographics Consent Copy of Insurance Card Patient Information Form Comprehensive Hx Outcome Assessment Forms including SF-12 The right side of the chart is grouped by date, NOT BY COLOR. Example: SOAP 11/5/13, Outcome Assessment Forms + SF-13 dated 11/5/13. Subsequent visits would include SOAP 11/7/13 on top of the SOAP dated 11/5/13 (latest date is placed on top). Charts are to be updated with the most current paperwork and placed in the correct order. Problem Management ICD #: In the codebook, find the appropriate number that corresponds to the patient’s issues. Each set of orders / plans applies only to the problem under which it is listed. For instance, prescribing the use of ultrasound for a neck problem doesn’t authorize the use of ultrasound for a low back disorder. Once a therapy is discontinued, it cannot be used again on that patient without new orders by the clinician on the Treatment Plan sheet. PROGRESS NOTES (aka “S.O.A.P.” Notes) Throughout your clinical career, you will be noting in detail the interactions you have with your patient. The most common and accepted format is called a “SOAP” note. The initials stand for Subjective, Objective, Assessment, and Plan. A SOAP note is a type of narrative called a Problem Oriented Medical Record (POMR). The assumption here is that you lead with the patient’s chief complaint. In general, the orientation of the record is geared to monitoring the chief complaint, not only in the subjective section but also as a flow seen in all areas. 34 Below you will find both explanations of the chief components of these notes and examples of the text. S: Subjective: This is the story that is told in the patient’s own words. It also can be their response to a specific question. Minimally this section should include: • History of the chief complaint or current status of symptoms • Interim history – how well has the patient done since the last time they were in for care? • How has the pain changed? • ADL’s (Activities of Daily Living) – how have these been affected? • Are they following your recommendations? • Review of Systems – heart, lungs, fever, cold, cough, weight loss, difficulty breathing, bladder function Example: Since the last visit, the patient has experienced a decrease in her low back pain. She reports that the pain continues to be achy but is more localized to the region of the right PSIS. She is no longer experiencing the diffuse pain that was extending down her right leg. When questioned about her exercise program, she admits that she has been doing the last taught set of Swiss ball exercises only once per day, instead of the twice per day as was recommended. There has been no change in her health or medical status since her last visit to this office. O: Objective: Record here the results of all examinations. The yardstick for objective findings is those procedures for the purpose of uncovering the nature of a patient’s condition that could be replicated by another physician of similar training. If a regional or physical examination was performed, carry over any positive findings from the exam sheet over to the SOAP note. This allows the SOAP note to be a stand-alone document. Even if the regional examination was lost, you could still replicate the determining factors from the examination. Record what you found during inspection: symmetrical, tonicity or swelling. How was palpation performed, motion or static, and what was uncovered? If you have completed the regional examinations, consider what high yield screening procedures you might do to uncover the worse case scenarios in your patient population. For example, vital signs, active observed range of motion (with or without pain) for the area of manipulation, mechanical or orthopedic tests for the area to be treated such as Kemp’s, cervical compression, Schepleman’s, etc. Finish with an explanation of your chiropractic findings, with a brief note concerning the method used to determine these listings. Example: Vitals: pulse = 72 bpm, BP = 120/72 right, respiration = 12/m, temperature = 98.6 F (these results would be written in the margin below the date). The following orthopedic tests were performed and found to be negative: cervical compression and depression, Kemp’s seated and Lewin’s tests. Gross ROM in the cervical and thoracic spine was observed and was full and pain free. Motion palpation detected loss of: right rotation - C3 & L3, extension - L4, left rotation - C2. The right upper cervical paravertebral musculature was found to be moderately tender to moderate palpation pressure, markedly taut with a small involuntary twitch noted during palpation. 35 A: Assessment: Make a commitment to what you think is going on with the patient. Record here your differential diagnosis, working diagnosis, and steps you might take to confirm or deny each item. You can also discuss the patient’s progress by weighing in on factors such as the degree of subjective improvement that the patient reports and how much your objective findings have changed. Some doctors use a percentage to describe the amount of improvement realized. Since chiropractic physicians often deal with various biomechanical problems that do not lend themselves very well to “sprain/strain,” a more complex language showing the interplay of factors can be appropriate in this realm. Here are a couple of examples: Chronic recurrent segmental dysfunction of the right sacral iliac joint secondary to bilateral foot pronation and an anatomical right lower extremity limb length discrepancy. In this example you have actually three diagnoses, yet the narrative shows the causal relationship between these various factors and how they relate to the first diagnosis, the primary concern causing the patient’s chief complaint. Thoracic outlet syndrome with radial nerve neuralgia primarily arising from hypertonicity of the right pectoralis minor. This is with an overlay of myofascial pain referral from the right anterior scalene muscles and associated segmental dysfunction of the upper thoracic and lower cervical spine. In this second example, again you see there is a primary diagnosis, yet the various principle players that contribute to the malady are also featured. Broken down into components, there are four different diagnoses running together here in addition to the regions of spinal dysfunction. In practical terms, on both the problem sheet and your treatment plan, you would list each item separately. Note: After the first visit, when you have established the diagnosis, it is no longer necessary to repeatedly state the diagnosis. By this point, it should be noted in the treatment plan. Once a treatment plan has begun, it is far more important that you monitor the patient progress and make comments concerning your outcomes. The example immediately below outlines the second component of the assessment section of a SOAP note. It is here that you summarize the patient's response. Notice that reference is made to both the subjective and objective aspects of the patient’s status. Since starting care three weeks ago, the patient has shown a noticeable improvement in both her symptoms and objective findings, especially the degree of fixation and number of levels involved. Current treatment appears to be effective and no modification of the treatment plan is required at this time. P: It is helpful to break down the explanation of treatment into what was done today versus what will be done at the next or future visits. Here is an example of that: 36 Today the patient received supine cervical manipulation for the above noted segments. This was performed while maintaining the neck in slight flexion and minimizing rotation and lateral flexion. Soft tissue release was performed using a thumb contact into the right upper trapezius muscle to patient’s tolerance until a relative degree of muscle relaxation was achieved. Instruction was given both by example, the patient’s own demonstration and in written format (see Swiss ball exercise sheet) in a new sitting Swiss ball exercise: one-leg lift. She is to perform this exercise 20 times (10 per each side) twice per day. If she continues to show good stability on the ball while performing this and other exercise, we will add the contralateral puppet at the next visit, in addition to the program outlined in the treatment plan. The next visit is scheduled for__________. If you have a high level of detail in your treatment plan, it is acceptable to make reference to the treatment plan in both the A: and P: sections of the SOAP note for a given day. This reference would include the actual date of the treatment plan under which you are working. In the A: section, you still have a responsibility to weigh in on the patient’s status. In other words, in light of the S: and O: how is the patient proceeding? It is not enough that the patient is feeling better. Are there also objective changes that support the subjective changes? Remember that S + O = A -> P. Subjective plus objective adds up to a diagnosis or status report leading to a given mode or course of treatment. In addition, for the P: section, specific treatment settings, nutritional supplements and types of manipulation must be stated. This would also include the teaching of therapeutic exercises, spelling out frequency, number of repetitions, and the name or description of the actual exercise taught. Formulate a detailed and thoughtful treatment plan and you will have the necessary road map for the best treatment possible for your patient. Use the examples on the next page to guide you. Referral of a Patient In the course of management with a given patient, you always have three choices before you: treat, co-manage or refer. In either co-management or referral, there is a need to let the other physician know the status of the case. Whether the referral is made internally (within the National campus) or externally (to a physician outside the campus), a letter of referral is required. Here are the basic components of a good referral: • Identify the patient • Date of the letter of referral • Brief description of the chief complaint, pertinent PE/laboratory findings and reason for making the referral • Very Important – Let the physician know if you are referring the patient for transfer of care or for co-management of the case!!! • If co-management, let the other physician know that the patient is still under your care. • Bring to the other physician’s attention any current issues and lab reports, radiographic findings, etc. that might help them in their attempts to help the patient • Print your name with a space above to sign • Clinician’s name with a space above to sign 37 Filing Laboratory, X-Ray, And Other Reports Reports from the clinical laboratory, radiology, outside physician’s reports, and consultations return to the clinic and must be entered in the patient’s file. Do not simply place the reports in the file. Instead record the results on a progress note and place the results in the appropriate place in the file. Do not search through the reports without permission of the attending. An attending clinician will review the report and initial it, and make it available to the intern. Carefully study the report and review any abnormalities. Enter the results on the progress note. The results may necessitate a change in the diagnosis or creation of a new problem (such thoughts should be reflected under the “A” portion). Should the report necessitate further work or education to the patient, record this under the Plan on the progress note. A new Treatment Plan may need to be created if the report modifies or creates a new problem for the patient. Use the example below of an “OAP” note following review of reports: O: Pt brought to initial visit labs collected on 7/31/09 yielding the following results: Cbc/diff: MCH <H> @ 32.5 pg (N=27.0-32.0 pg); MPV <L> @ 6.7 FL (N=7.4-10.3 FL). Other values within reference ranges. CMP: Glucose <H> @ 106 mg/dL (N=65-99 mg/dL). BUN/CREA ratio <L> @ 7.2 (N=10.0-20.0. ALT <H> @ 64 u/L (N=17-63 u/L). All other values within normal reference ranges. Lipid Panel: HLD <L> @ 29 mg/dL (N=40-60 mg/dL); triglyceride <H> @ 159 mg/dL (N=1-149 mg/dL). GFR within normal reference ranges, all other values within normal reference ranges. TSH=0.54 UIU/ML (N=0.34-5.60 UIU/mL). Bone Mass Calculation for DEX scan performed on 1/11/06 yielded the following results: distal BMD T-score= -3.0 and Distal BMC T score= -2.6. A: ICD 277.7 Metabolic Syndrome; 733.0 Generalized Osteoporosis 59 YOWF presents to learn of lab results. Based upon above findings including hyperglycemia and hyperlipidemia, and previous Dx of HTN (done by her GP) metabolic syndrome fits her current presentation. In addition, her bone density rating falls within the category for osteoporotic. P: Pt will follow-up for treatment plan on 5/1/14. 38 Chapter 4 Phlebotomy Procedure Phlebotomy Procedure • • • • • • • • • • • • • • • • • • • • • • • • • • • Show pt that the needle is sealed and open it in front of them Insert it into needle holder Put gloves on Open alcohol swab, Band-Aid, make sure appropriate tubes are available as well as cotton ball/gauze pad Place tourniquet on one arm 2 inches above antecubital fossa Palpate for adequate vein Release tourniquet Repeat tourniquet and vein palpation on opposite arm Once adequate vein in chosen, set supplies on paper towel next to patient (either lying down or sitting is fine) Apply tourniquet 2 inches above antecubital fossa Clean area in a bull’s eye fashion with a folded alcohol prep pad, clean traction hand with opposite side of alcohol pad (that didn’t clean pt arm) Make sure bevel is up and cotton ball is ready Traction above and below area, insert needle at 15-20 degree angle quickly and smoothly Insert tube with equal and opposite pressure (gold, blue, green, lavender) Remove tube with equal and opposite pressure (if don’t, the needle will slide farther into arm) Repeat if necessary (depending on the number of tubes) Remove tourniquet when last tube is halfway full. (Make sure tourniquet is released before pulling needle out because blood will spurt out and hematoma could form.) Let last tube fill up and remove tube from holder with equal and opposite pressure. Place cotton ball over the area of the needle. (Don’t press down until needle is out of arm.) CAP NEEDLE ON EDGE OF TABLE IMMEDIATELY!!!!! Have pt hold cotton ball with arm straight and preferably elevated above heart level Dispose of needle into sharps container Mix tubes with any additive, if necessary Apply bandage to arm Dispose of cotton ball, alcohol pad into gloves. Remove gloves with proper technique. Dispose of glove package into biohazard. All other waste without blood on it is regular trash. Process samples as directed by clinician 39 Considerations • • • • • • • Never draw from an arm or leg with a shunt or fistula Avoid drawing from the affected side of a pt with a stroke or radical mastectomy Never draw above an IV site With a Pt on anticoagulants (coumadin, heparin) take extra care to stop the bleeding and apply pressure bandage Most common site and best site to draw is the Median antecubital (cephalic) vein. This is the most stable, as there is not much to damage to this area. Lateral vein is next best. Medial side should be avoided if possible. There are tendons and the brachial artery is in the area. Alternate drawing sites, i.e., dorsum of the hand. To be done only by the clinician or a phlebotomist • Dorsum of hand, lateral wrist, dorsum of the foot Ordering Labs From Elmhurst Memorial Hospital – Lombard Ordering Labs From Quest Diagnostics – Florida • • • • • • • • • • • Take the completed route slip with all labs that you want run for each patient to your respective Medical Records department. Be sure any lab tests are approved and signed off by the attending clinician. The route slip needs to have the patient’s last and first name with correct spelling and the patient’s birth date listed at the bottom of the route slip. Lombard Medical Records will enter the labs into the Elmhurst Hospital ordering system. Florida Medical Records will enter the labs into the Quest Diagnostics ordering system. After the labs have been completed, the Requisition form and the labels that go on the specimens will print out. The intern/doctor will take the labels and put them on the specimen(s). One extra label will be placed in the patient’s file on the progress note. Take the requisition and specimen(s) with the printed labels and put them into specimen bag. Before placing the specimen(s) into the refrigerator, put the barcode label on the outside of the bag as you currently do. Now you may put the specimen(s) into the refrigerator. Finally, enter patient’s name and the ordering doctor’s name into the big lab book with the second bar code label as you have been doing. All labs will print out in Medical Records when they have been completed. Medical Records will give the lab results to the ordering doctor. Elmhurst does not automatically pick up orders on Saturdays. YOU MUST CALL TO REQUEST PICK-UP ON SATURDAYS. Addendum to EMH Labs • For ABO Blood Group – label the tube with your name and date If the samples are not obtained on that patient visit, for whatever reason, please notify medical records and the order will be cancelled. 40 ****Student results will be placed into the Student Clinic mailbox or in the box of the attending physician by medical records. Lombard Medical Records is open from 7 a.m. to 8 p.m., Monday through Friday, and 7 a.m. to 12 p.m. on Saturday. Florida Medical Records is open from 8 a.m. to 6 p.m., Monday and Thursday, from 1 p.m. to 6 p.m. on Tuesday, from 8 a.m. to 4:45 p.m. on Wednesday, and from 8 a.m. to 1 p.m. on Friday. Lombard Clinic Only All laboratory samples are sent to Elmhurst Memorial Hospital reference labs (unless specifically advised otherwise by the attending clinician). Note: An improperly processed sample may be rejected by the lab and result in a redraw of your patient. CBC: (Purple top) After the specimen has been obtained, place the label on tube. Enter the patient’s name into the clinic laboratory logbook (located in clinic lab), as indicated in Table I below. Then record the logbook number onto the patient’s requisition. Affix one label to the CBC tube, one label in the logbook, and one label in the margin of the progress note for that patient visit. Place the CBC tube into the Ziplock portion of the same bag and seal it closed. Using a set of the paired EMH tracking labels, place one label on the specimen bag and the other next to the patient’s label in the logbook. Place the bag and its entire contents into the refrigerator in the lab. Urinalysis: After the patient has collected the sample into the plastic urine transport container, collect the sample from the patient while wearing gloves. Check to confirm that the cap of the tube is securely in place and immediately identify the container with the patient’s name. If the sample is going to EMH labs, take the vacutainer tube and siphon off urine to the tube with preservative. Place label on specimen. You will complete the logbook, requisition, labeling, and packaging of the sample using the same procedure as above for the CBC. Metabolic/chemistry panels (SST, PST tubes): After collecting the SERUM (gold tubes) specimen from the patient, make sure you have attached the label to the specimen. The sample must then sit upright in the tube for 15-30 minutes to allow the blood to clot. Once the specimen has solidified, it is then placed in a BALANCED centrifuge and spun down for 15 minutes. NEVER – leave an unlabeled specimen to clot or place it into the centrifuge. While the blood is clotting and spinning, fill out the logbook following the procedures outlined above for the CBC. The specimen is now packaged as previously described above and placed in the refrigerator for pick-up. PST (light green) tubes are handled the same as above, although no clotting time is required (i.e., they can be spun down immediately after drawing). 41 Pink tubes are processed the same as CBC tubes. Remember that the requisition must include the patient SS#; the SS# and your initials must be on the label. The testing will NOT be done without this info. There are special labels in the lab for this sample. NOTE: When more than one type of sample is obtained from the same patient (i.e., UA and CBC), they are all included on the same EMH requisition, the same line of the logbook, and sent in the same transport bag. If in doubt, check with the EMH reference lab or supervising clinician. Ordering Labs from Cleveland HeartLab – Lombard • All supplies are in the ND chief clinician’s office (Currently Dr. Liebich) • Locate the Cleveland HeartLab Shipping Supplies binder. • In this binder you will find several supplies you will need, including: o Requisition form Complete the Patient Information section: First and last name, date of birth and gender are REQUIRED. All other information is helpful. Please check Yes or No under “Fasting”. “Other patient ID” is the patient’s chart number. Fill in the corresponding box of the lab(s) you wish to run, or manually write them in under “Other”. Have the appropriate clinician sign the requisition form. (The clinician legally allowed to sign this form will be listed under “Practitioner information”). Fill in the yellow highlighted section on the left side of this form: Draw date, time and your initials. The back of this form also has instructions. o UPS labels Tear off the next label (do not peel off the backing!) and take with you. o Tube labels Obtain the appropriate number of blank tube labels for each tube you will be using. Information needed on each tube includes: • Patient’s first and last name • Patient’s date of birth • If you are using a Sample Tube – the label must also include the sample type o NUHS Cleveland HeartLab Test Pricing Form Obtain one of these forms • Do NOT take the last form without making copies Highlight each test run on this form, as well as appropriate COST (paying patient or Emp/Stu cost) o Cleveland HeartLab Test Menu This is in the outside pocket of the binder; please return this form once you have found the required tubes. 42 Read over this form to determine which tube is required for each test • NOTE: A serum tube is the tiger top tube (dark grey/orange) • NOTE: the red/yellow tiger top is a URINE SPECIMEN tube The reverse side of this form describes how each tube is to be processed and the minimum amount required for each test to be run • Locate the “Labs Ordered” Folder in your attending clinician’s office. o Write down the date the test was drawn, the patient’s name and the lab running the test (i.e. 4/17/2014 Ennsmann, Michelle Cleveland) • Locate other supplies in the chief clinician’s office: o Styrofoam box o UPS Laboratory Shipping Pak mailer o One biohazard bag o Applicable tubes (if there is more than one bag of the same type of tubes, please grab the ones closest to the top or front – these have the most recent expiration date) or urine cup, sample tube or pipette • Go to Medical Records to obtain a needle and barrel • Draw blood/collect urine • Label tubes • Prepare blood as required • Place cold or frozen sample(s) (as indicated per sample directions) in the biohazard bag • Place completed requisition for each sample in the pouch of the biohazard bag • Place biohazard bag(s) (with sample(s) and requisition form) in the styrofoam box • Place a frozen ice pack on top of the samples in the styrofoam box o You will find several of these in the freezer in the lab • Check with other clinicians to see if anyone else is performing Cleveland labs the same day, as numerous samples can be packaged and sent together in the same styrofoam box and UPS bag • Place the styrofoam box into the UPS laboratory Shipping Pak • Place sticky label on outside of UPS laboratory Shipping Pak • Call UPS at (800) 742-5877 to schedule a “Return Service Labeled” pick-up o Have the tracking number from the label available o Provide the closing time of clinic as 6 p.m. CHECKING OUT PATIENT: • Fill out information for front desk for proper billing • Staple NUHS Cleveland HeartLab Test Pricing form (with test(s) highlighted) to the back of the route slip • On the front of the route slip, you must write “extra labs” so the front desk will know to check the back of the slip. It may help to highlight this or underline it. • On the back of the route slip write “Cleveland Heartlab” o List test name(s) o CPT code(s) o BOTH Emp/Stu cost and patient cost; CIRCLE appropriate cost (Emp/Stu or patient) 43 SAMPLE REJECTION POLICY Samples will be rejected for any of the following reasons: • Sample types were incorrect or samples were received in damaged condition (i.e. tube open or cracked, sample not shipped at correct temperature). • Sample tube is not properly labeled with first and last name and date of birth. In addition, transport tubes must also be labeled with tube type and sample type. • Samples that are beyond their stability limits. • Requisition form is incomplete. First and last name, date of birth and gender are required. • Physician signature is missing. • Any additional rejection criteria for a test, beyond the above standard criteria, will be listed on the individual test’s page on our test menu. Ordering Labs from Genova Diagnostic Labs – Lombard • All supplies are in the ND chief clinician’s office (Currently Dr. Liebich) • Locate the “Genova & SpectraCell” binder. • In this binder you will find information about the tests, and: o NUHS Genova Diagnostics Lab Pricing form Obtain one of these forms • Do NOT take the last form without making copies Highlight each test run on this form, as well as appropriate COST (paying patient or Emp/Stu cost) • Obtain the appropriate testing box from the top of the bookshelf. This box should include: o Styrofoam box – for frozen or refrigerated samples only o Instruction form Each kit will have a detailed instruction form, please follow this CLOSELY Assure that the box includes all of the indicated supplies (many times items are missing) Each box will have different testing/sampling supplies • Follow the instruction form carefully to assure the testing will be done properly Every box should have the following supplies: o Requisition form Carefully follow all of the instructions on the form Complete the date of sample collection at the top of the form Check the appropriate tests that you would like to run Assure that the appropriate clinician signs the form (this is the clinician whose name is printed on the form) Billing options: • Check “Bill Healthcare Practitioner Account” Check the appropriate ICD-9 Code(s) or add them in if necessary Have the patient complete the purple highlighted Patient Information section. The labs will NOT be run if this section is incomplete. The Medicare Information Section and Payment Information Section do not need to be completed 44 • • • • • • • • • • • • • • Have the patient read, sign and date the yellow highlighted Patient/Responsible Party Acknowledgement section. The labs will NOT be run if this section is incomplete. o Advance Beneficiary Notice of Noncoverage (ABN) Because we cannot bill Medicare for our services, this form is N/A and can be thrown away o Prepaid FedEx Bag with Label Locate the “Labs Ordered” Folder in your attending clinician’s office. o Write down the date the test was drawn, the patient’s name and the lab running the test (i.e. 4/17/2014 Ennsmann, Michelle Genova) Go to medical records to obtain a needle and barrel Draw blood/collect urine Label tubes Prepare blood as required Place samples(s) in the biohazard bags The individual test will include instructions on how to properly package the sample for shipment. This will change depending on if the sample is refrigerated/frozen or stored at room temperature. Place completed requisition on top of the test box. Do NOT staple or tape the box. Place the complete box in the FedEx envelope Call FedEx at (800) 463-3339 to schedule shipping o Say “Return a Package” o Tell the FedEx representative “I am using a billable stamp” and they will walk you through the process. o Provide the closing time as 6 p.m. Fill out information for front desk for proper billing Staple NUHS Genova Diagnostics Lab Pricing form (with test(s) highlighted) to the back of the route slip On the front of the route slip, you must write “extra labs” so the front desk will know to check the back of the slip. It may help to highlight this or underline it. On the back of the route slip write “Genova” o List test name(s) o CPT code(s) o BOTH Emp/Stu cost and patient cost and CIRCLE the appropriate one 45 46 Chapter 5 Patient Care Patient Care Elective Care The delivery of health care is both a responsibility and a privilege. At each patient visit, therapeutic necessity is judged based on the current findings and the history of the patient’s health. Therapeutic necessity for continuing treatment diminishes as the patient reaches maximum therapeutic improvement. With that judgment, the patient is usually discharged from active care for that episode. On occasion, the patient may ask to continue care on an n elective basis. It is the policy of the University that a patient has the right to seek elective care from any source including our clinic facilities. Elective care may be administered to any patient who requests it, provided that the patient is informed that fees for services rendered may not be reimbursed by a third party payer. The attending clinician or the office manager will undertake discussion of the specifics of each case. The attending clinician will make a decision on the appropriateness for elective care. The clinic director may assume this task on behalf of the attending clinician, if necessary. The business office manager shall discuss all payment options and inform the clinician and patient if the services will be reimbursed by the third party payer. The intern is not authorized to discuss the patient’s method of payment or make financial decisions for the patient’s care. Walk-In or Emergency Patients Patients requesting services without an appointment will be given the option of waiting for an appointment to open or schedule another appointment time. If, in the judgment of the patient, an emergency situation exists, the front desk will contact the attending physician serving as Emergency Officer of the Day (EOD). The EOD will determine if a true emergency exists or if the patient may be made comfortable until the next available appointment time. It is the policy of the clinic system of National University of Health Sciences to permit unscheduled patients to supersede the appointments of scheduled care ONLY if a true emergency exists. A person presenting for treatment without an appointment and determined to not be a medical emergency will be required to wait to avoid inconvenience of those who have made previous appointments. 47 Treatment of Minor Patients In the course of practicing in the clinics, the issue of treatment of minor children will come up. There are legal requirements that must be met to be sure all parties involved in the encounter are protected and informed. A child is defined as anyone under the age of 18 who has not been legally emancipated. Emancipation is declared for children under age 18 by a court of law, which legally pronounces the child as an adult for purposes of entering contracts, undergoing informed medical procedures and signing binding contractual agreements. Most of the minor patients who will be encountered in the NUHS Health System will be living with their parents, guardians or another adult with the legal status of being able to give consent for treatment. The adult must be present at the initial visit to give written authorization for examination and treatment. On all patient information sheets used in the NUHS system, a signature line is present for the adult to give permission to treat the minor. The signature must be affixed prior to the minor patient entering the examination room. Failure to obtain the authorization leaves the physician and intern vulnerable to charges of battery later. Battery is the unauthorized or unwelcome physical touching of another person. Without authorization by a consenting adult for the minor child, the act of examining a patient constitutes the legal description of battery. After the initial visit, and with the clinical decision of the attending physician, the adult giving consent may not need to be physically present for continuing treatment. The adult must be informed of the treatment plan and give authorization for carrying out the diagnostic workup and treatment before the minor will be examined, X-rayed or treated. All risks and benefits must be outlined to the child, depending on age and ability to comprehend, and the adult giving consent. If the minor is of an age where they are unable to be left alone or unwilling to be away from the adult giving consent, that adult must be present. If the minor is able to comprehend and give historical information, then the attending physician can allow the minor to be seen without the adult accompanying them. Although there is no legal requirement to have written informed consent in the patient’s chart, it is a requirement of the NUHS Health System to have a signed copy of the form obtained and filed in the chart. A copy of the appropriate Informed Consent Form may be obtained from your attending physician. Be sure you are familiar with the contents before giving it to the adult for signing. Witness the signature and have the attending physician countersign the adult’s signature. This form should be photocopied and one copy given to the adult, the original going into the patient’s chart. The outside of the chart will be identified by the word “MINOR.” As with all issues of providing care, the attending physician must be consulted in every issue of the course of history, physical examination, diagnostic testing, and treatment plans. No minor patient may be seen in any clinical setting without a signed authorization. Patient’s Bill of Rights If the patient lacks decision-making capacity, is legally incompetent, or is a minor, these rights can be exercised on the patient’s behalf by a designated surrogate or proxy decision-maker. The patient has the right to considerate and respectful care. The patient has the right to and is encouraged to obtain from physicians and other direct caregivers relevant, current and understandable information concerning diagnosis, treatment and prognosis. 48 Patients have the right to know the identity of physicians, nurses, residents, interns, or other trainees. The patient also has the right to know the immediate and long term financial implications of treatment choices, insofar as they are known. The patient has the right to make decisions about the plan of care prior to and during the course of treatment and to refuse a recommended treatment or plan of care to the extent permitted by law and clinic policy and to be informed of the medical consequences of this action. In case of such refusal, the patient is entitled to other appropriate care and services that the clinic provides or transfer to another health care provider. The clinic should notify patients of any policy that might affect patient choice within the institution. The patient has the right to have an advance directive (such as a living will, health care proxy, or durable power of attorney for health care) concerning treatment or designating a surrogate decision-maker with the expectation that the clinic will honor the intent of that directive to the extent permitted by law. The patient has the right to every consideration of privacy. Case discussion, consultation, examination, and treatment should be conducted so as to protect each patient’s privacy. The patient has the right to expect that all communications and records pertaining to his/her care will be treated as confidential by the clinic, except in cases such as suspected abuse and public health hazards when reporting is permitted or required by law. The patient has the right to expect that the clinic will emphasize the confidentiality of this information when it releases it to any other parties entitled to review information in those records. The patient has the right to review the records pertaining to his/her medical care and to have the information explained or interpreted as necessary, except when restricted by law. The patient has the right to expect that, within its capacity and policies, the clinic will make reasonable response to the request of a patient for appropriate and medically indicated care and services. The clinic must provide evaluation, service, and/or referral as indicated by the urgency of the case. The patient has the right to ask and be informed of the existence of business relationships among the clinic, educational institutions, other health care providers, or payers that may influence the patient’s treatment and care. The patient has the right to consent to or decline to participate in proposed research studies or human experimentation affecting care and treatment or requiring direct patient involvement, and to have those studies fully explained prior to consent. A patient who declines to participate in research or experimentation is entitled to the most effective care that the clinic can otherwise provide. The patient has the right to expect reasonable continuity of care when appropriate and to be informed by physicians and other caregivers if available and realistic patient care is no longer appropriate. 49 The patient has the right to be informed of clinic policies and practices that relate to patient care, treatment and responsibilities. The patient has the right to be informed of available resources for resolving disputes, grievances and conflicts, such as ethics committees, patient representatives or other mechanisms available in the institution. The patient has the right to be informed of the clinic’s charges for services and available payment methods. The patient has an obligation to follow the treatment plan agreed to and make every effort to cooperate in the progression of their treatment to help ensure the desired outcome. Clinic Fees and Patient Accounts Patients occasionally have questions regarding their accounts or clinic financial policy. Since these matters can be construed as verbal contracts, it is important that all such questions be referred to the attending clinician and business office manager for response. The business office manager will make financial arrangements with the patient depending on the circumstances of the case. Do not discuss these matters with the patient yourself. The intern is responsible for properly recording all services rendered on the route slip. Failure to indicate services provided to a patient is considered violation of the code of conduct of the clinics and will result in the intern being charged personally for the services that were not recorded correctly. In addition, the attending clinician may take further disciplinary action against the intern. On the surface, it may seem kind or compassionate to supply treatment (or other services) without writing it on the route slip or by altering the route slip to obtain a reduced fee for a patient. However this results in increasing clinic costs that must be absorbed by the University and by its students. Moreover, should a case be challenged, the financial record is often compared to the physician’s orders and daily progress notes to test veracity. If these do not agree, the patient can lose benefits of third party payment. It may further place the clinic in violation of federally controlled programs and lead to fines and sanctions. Billing Categories Charity Treatment All discounts, charity case decision requests, etc. may be initiated only by the attending physician in close conference with the business office manager. The business office manager may make the financial decisions in concert with the Dean of Clinics. No clinician or intern may make the offer of charity treatment without clearing the matter through the business office. If it is discovered that charity treatment has been extended without authorization, the intern and/or clinician will be financially responsible for all charges. Extenuating circumstances can be explained by a letter co-signed by the supervising clinician and clinic director and should be forwarded to the business office manager of the clinics who will consult with the Dean of Clinics. Treatment of Interns If an intern wishes to be treated at the clinic, an Intern Treatment Only route slip must be obtained and all services must be appropriately recorded on that slip. All patient record protocols must also be adhered to. Interns are reminded that all procedures counted towards graduation 50 requirements must be verifiable in the medical records. Intern treatments must not be recorded on regular patient route slips (yellow routing slip). All fees that normally apply to students, also apply to the intern being treated (i.e., lab fees, X-rays, free adjustments, and therapy). Procedure for Intern Treatment • Notify your clinician that you wish to treat an intern. Obtain the clinician’s permission and get a yellow routing slip. • Complete the section of the slip indicating the intern’s file number and name, your clinician’s name, and the date. • Check the intern’s file out of Medical Records. • Provide the services ordered by the clinician. • Complete the route slip, recording your intern number next to the services you provided and listing the proper diagnosis(es) for the visit. • Obtain your clinician’s signature on the completed route slip. • Take the completed route slip to the cashier. • Complete your charting of the visit in the medical record, then have your clinician sign the progress note and return the file to Medical Records. Any intern credits recorded on the weekly Intern Tally Sheet that DO NOT have corresponding entries in the clinic computer system or medical record will be denied and the disciplinary code penalties for claiming false credit on clinical services will apply. Diagnostic Imaging Guidelines General Guidelines • • • • • Food is not permitted in the department. Drinks are allowed only if in a spill-proof container. X-ray or MRI files must be signed out before the can be removed from the department. X-ray or MRI files must be signed back into the department. Patients must wear shoes or socks while in Radiology. Professional behavior is expected at all times while in Radiology. X-ray Positioning and Factoring (P&F) and Report Writing Procedures • • You must complete 30 P&Fs prior to graduation. Your best opportunity to meet this requirement occurs during the course of your internship while radiographing the patients that you are treating. You will receive one credit per correctly performed radiograph (i.e. seven credits possible from a Davis series). Be prepared to perform the studies yourself (no “cheat sheets” allowed in radiography suite) or you will receive no credit. Five credits are awarded to all interns at the start of their Eighth Trimester for the successful completion of the P&F class in Seventh Trimester. 51 • Procedures for earning P&F credits and for performing radiographic studies on patients vary according to the clinic at which you are stationed. Please consult the technologist or your supervising clinician for details. NUHS Clinic System Diagnostic Imaging Procedures – Illinois • • • • • • Record the patient’s name, date, series, and the doctor’s name in the X-ray log book. Type the patient information on the ID/flash card. (Aurora only) Make sure that the patient is gowned (if appropriate) and that jewelry, dentures or clothing (ex. bra, belts, pants with rivets, buttons, or zippers, or any body piercings, etc.) that may generate artifacts are removed. Be prepared to position the patient for the study and calculate the factors to be used. Have the clinician or resident check your technique and make the exposure. Interns are not permitted to “push the button” and make exposures. Make sure that your name, the views you performed, and either a clinician or a resident signature is recorded on the Radiology Positioning Credit forms located in the radiology suite. (Lombard clinic) NUHS Clinic System Diagnostic Imaging Procedure – Florida • • • • Make sure that the patient is gowned (if appropriate) and that jewelry, dentures or clothing (ex. bra, belts, pants with rivets, buttons, or zippers, or any body piercings, etc.) that may generate artifacts are removed. Be prepared to position the patient for the study and calculate the factors to be used. Interns are required to bring their own Supertech calculator and laterality markers. Have the clinician or resident check your technique and make the exposure. Interns are not permitted to “push the button” and make exposures. Make sure that your name, the views you performed, and either a clinician or a resident signature is recorded on the Radiology Positioning Credit forms located in the radiology suite. (Lombard clinic) This must be turned in the same day as the radiology procedure. Indications for X-ray Examination It is understood that X-ray studies should be performed only when it is believed that they will significantly contribute to case management and diagnosis. It is, however, ultimately left to the discretion of the clinician when to proceed with X-ray evaluation. As an intern involved in the management of any particular case, please be prepared to discuss the rationale for ordering radiographs with radiology personnel. The decision to take radiographs should be based upon information gathered from the case history, physical examination, and lab data (when available). Below is a table taken from Essentials of Skeletal Radiology, by Yochum and Rowe, p.7, Table 7.2 that illustrates the guidelines for obtaining skeletal radiographs: 52 Table 4.1 Guidelines for Obtaining Skeletal Radiographs Probable Indicators Recent trauma Neurologic deficit Inflammatory arthritis History or suspected malignancy Fever of unknown origin (>100 °F) Deformity (scoliosis, congenital) Recent surgery Failure to respond to therapy Possible Indicators >50 years of age Drug or alcohol abuse Corticosteroid use Unavailability of alternate imaging Unavailable/lost technically inadequate studies Constitutional/systemic disease How to Order Radiographic Studies at NUHS Clinics • Call Radiology (ext. 6832) before bringing your patient back for X-rays. This helps prevent unnecessary waiting in the department. (Lombard clinic only) • A requisition form must be completed legibly and signed by the referring physician. Xrays will not be taken without a completed and signed requisition form. • Make sure that your female patients are within the first 10 days of their menstrual cycle (10-day rule) and have them sign and date a pregnancy release form. • Inform the clinician/resident that your patient is ready and what radiographs are to be obtained. • Please remain with your patient while they are in X-ray. It is important that your patient be attended while receiving procedures. • It is the intern’s responsibility to present the patient’s route slip to the clinician/resident for completion. If the service rendered is not on the route slip, the patient cannot be charged. Failure to complete the route slip is a common error that often results in misunderstanding, inconvenience, accounting dilemmas, embarrassment, loss of revenue, and loss of intern credit. The intern will be responsible for paying for any procedure that they performed but did not charge the patient for. • Interns must be prepared to correctly position and calculate technical factors for the studies being performed. • Once the study has been reviewed and approved by a clinician, resident or radiologist, interns are expected to escort patients from radiology after successful completion of the procedure. 53 Radiological Studies (By Region) **Some studies will be performed recumbent unless standing radiographs are specifically ordered and factors do not exceed tube limits. Cervical Spine Limited Medicare series: on patients over age 65, APOM, APLC and Lateral Limited series: APOM, APLC, Lateral 5 view series: APOM, APLC, Lateral, Obliques Davis series: 5 views plus flexion and extension views Special views: as needed by radiologist: pillar arch views. Oblique odontoid views, swimmers lateral view Thoracic Spine Limited Medicare series: AP, Lateral & PA Chest Routine series: AP, Lateral & PA Chest Special views: as needed by radiologist Ribs Routine series: PA chest & Oblique Special views: as needed by radiologist: Swimmers lateral Chest Routine series: PA chest and Lateral Chest Special views: as needed by radiologist: Apical lordotic, Full Chest Lordotic, obliques Lumbar Spine: Medicare series: AP, Lateral, AP angulated lumbosacral spot Routine: AP, Lateral, AP angulated lumbosacral spot Full series: AP, Lateral, AP angulated spot, Obliques Special views: as needed by radiologist: AP angulated spot, Lateral Spot Projection, Angulated Oblique, Flexion & Extension Lateral Full Spine 14x17 Bucky AP & Lateral Sectional Views (Lumbar, Thoracic & Cervical) Pelvis Routine series: AP Pelvis Hip Routine series: AP Pelvis, AP Spot, Frog Lateral of involved hip Coccyx Routine series: AP & Lateral 54 Knee Routine series: AP, Lateral. Tunnel, Tangential Patella Patients over 40: Replace AP with bilateral AP weight-bearing study Special views: as needed by radiologist Ankle Routine series: AP Mortise, Lateral & Medial Oblique Special views: as needed by the radiologist: Eversion & Inversion Stress Foot Routine series: Dorsoplantar, Lateral & Medial Oblique Special views: as needed by the radiologist Tibia/Fibula Routine series: AP & Lateral Special views: as needed by the radiologist Femur Routine series: AP & Lateral Special views: as needed by the radiologist Shoulder Routine series: Internal rotation, External rotation & Baby Arm Special views: as needed by the radiologist: Transthoracic, Scapular “Y” Acromioclavicular Joints routine series: AP weighted and AP non-weighted Elbow Routine series: AP, Lateral, Internal Oblique & Jones Special views: as needed by the radiologist: External Oblique Wrist Routine series: PA, Medial Oblique, Lateral & Ulnar Deviation Special views: as needed by the radiologist Hand Routine series: Dorsopalmar, Medial Oblique & Lateral Special views: as needed by the radiologist Fingers Routine series: PA Hand, Medial Oblique and Lateral of involved finger 55 Radius/Ulna Routine series: AP & Lateral Special views: as needed by the radiologist Humerus Routine series: AP & Lateral Special views: as needed by the radiologist Abdomen Routine series: Supine KUB Special views: as needed by the radiologist: PA & lateral (upright and/or recumbent) Functional Radiography Standing Lateral Bending The standing lateral bending examination of the lumbar spine is performed with the patient initially in the AP lumbar position. The patient bends as far as possible with the ipsilateral hand sliding along the lateral aspect of the thigh and hip. Effort must be made to discourage rotation at the pelvis and shoulders. There are three exposures made: Neutral, Left Lateral Bending and Right Lateral Bending. Lumbar Standing Flexion and Extension The patient stands with their legs straight and shoulder width apart. For flexion, the patient bends forward at the waist as far as possible with care taken to avoid rotation. For extension, the patient bends backward as far as possible. There are three exposures made: Neutral, Flexion and Extension. Special Intern Study Program (Radiology) Special study opportunities are available to interested interns in the Radiology Department during the Tenth Trimester. The special study rotation will include reading radiographs with the residents and radiologists, assisting in special procedures, and preparing for state board examinations by utilizing the ACR pathology file and audiovisual material in the department. Interns are expected to stay in the department at all times during this special rotation. Sessions run daily for two weeks from 8:00 a.m. to 2:00 p.m. If the number of applicants outnumbers the number of slots available, the department will select participants based upon performance during the regular rotation and classroom setting. Requirements are as follows: • Completion of all graduation requirements at your main clinic • A completed application with the signatures from the Radiology department head, clinic director and Dean of Clinics. (See special study request form at the end of this manual.) This form should be submitted at least two weeks before the desired session is to begin. On the application, please select three choices for dates of attendance 56 Chapter 6 Outcome Disability Questionnaires A variety of questionnaires are utilized by the physician to diagnose a patient’s area and level of disability. Back Pain Questionnaire Patients are asked to indicate how back pain affects their daily life in such areas as lifting, walking, sleeping, social life, traveling, employment, etc. Diet Diary On this chart, patients record the type of food, quantity and method of preparation for a four-day period. Disabilities of the Arm, Shoulder and Hand (DASH) Patients are asked to describe their ability to perform certain activities utilizing the arm, shoulder and hand. Headache Diary Patients are asked to record headache pain including timing, warning signs, type and intensity of pain, etc. Lower Extremity Functional Scale Patients are asked to rate their inability to perform specific activities due to lower limb problems from extreme difficulty to no difficulty. Modified Zung Depression Index Patients are asked to respond to a variety of positive and negatively worded statements ranging from “rarely or none” to “most of the time.” Neck Disability Index Patients are asked to indicate the statements that most closely describe their inability to perform specific activities due to neck pain. Oswestry Low Back Pain Disability Questionnaire Patients are asked to rate their ability to perform a variety of activities on a 0-5 scale. 57 Pain Chart On drawings of the front and back of the human body, patients are asked to use designated symbols to indicate their type and area of pain from numbness to stabbing. Patient Specific Functional and Pain Scales (PSFS) On this follow-up form, patients are asked to indicate whether or not they are still having difficulty with activities they indicated in a previous visit. TMD Disability Index Patients are asked to rate their ability to perform a variety of activities that would be indicative of temporomandibular disorders (TMD). TMJ/TMD Outcome Assessment Form Patients are asked to check a series of symptoms indicative of temporomandibular joint disorder (TMJ) / temporomandibular disorders (TMD). Visual Analog Scale On a horizontal line ranging from “no pain” to “worst pain imaginable,” patients are asked to mark the point that they feel represents their perception of their current state for various regions of the body. 58 Chapter 7 Clinic Disciplinary Protocols During the internship phase of the curriculum, clinicians assume the primary role of supervisor/instructor to the interns assigned to them. Clinicians are faculty members tasked with the responsibility of evaluating an intern’s skill at distilling all the information acquired from their academic coursework into useful clinical knowledge. At the same time, clinicians are also evaluating an intern’s development of non-cognitive skills, character traits and personal attributes that are just as important as clinical knowledge. An intern’s trainee status dictates restriction of full practice privileges, but it does not diminish their obligation to cultivate and demonstrate the habits and mannerisms of professional conduct far in advance of graduation. These skills are revealed over time through acts of compassion, trustworthiness, sound judgment, personal accountability, respect for others, and the capacity to exceed mere compliance with rules or avoiding prohibited behavior. Monitoring the progress of each intern’s personal development relies upon a carefully fostered, mentoring relationship between each intern and their attending clinician. This important relationship involves more subtle, interactive assessment of a student than the limited revelations of a multiple-choice exam. Ultimately, it provides the most effective learning platform for interns to strengthen any areas of weakness and refine their competence, personal integrity, selfdiscipline, and confidence prior to graduation, and afterward, to assuming their role as a healthcare professional. There are numerous expectations that must be met and competencies that must be mastered during a clinical internship. Intern training within the NUHS clinic system begins with a week of orientation and the issuance of the NUHS Clinic Intern Manual. The NUHS Clinic Intern Manual is used to orient interns to the NUHS clinic system of rules, regulations and office protocols. Copies of the clinic system business forms are reviewed, and several state and federal laws that are enforced within the clinic system are explained. At the conclusion of orientation, every intern submits a signed and dated form acknowledging having read and understood the contents of their NUHS Clinic Intern Manual. Interns are also informed that failure to comply with the NUHS clinic system rules or procedures described within the NUHS Clinic Intern Manual may have automatic penalties ordered by their supervising clinician when specific infractions (listed below) occur. These measures are used to help an intern correct a deficiency in competence or rectify a conduct infraction without interrupting: 1. The quality or continuity of patient care; and/or 2. The timely completion of internship; and/or 3. The degree completion credit an intern may have earned toward graduation requirements. 59 Automatic Penalties For Clinic Infractions Clinicians may impose an automatic penalty upon an intern who has committed any of the infractions listed below. Repeat occurrences of the same infraction or commission of other infractions on a different occasion may be managed by increasing the severity (quantity) of the penalty after consulting with the Chair of Clinical Practice. If, however, an intern fails to complete a penalty, decides to dispute an assigned penalty, or the supervising clinician and the Chair of Clinical Practice deem the nature or severity of an intern’s infractions to merit additional administrative review or referral for disciplinary sanctions that may result in suspension or expulsion of the intern, then the matter shall be referred to the Dean of Clinics. The infractions and penalties are listed below: • Infraction: Unauthorized performance of clinical service on any person, withholding clinical information on a patient’s condition, or withholding services that were ordered by the clinician. Penalty: Intern will not be allowed to count that patient toward their new patient/college service requirement. All treatments carried out during the course of the patient visit will be disallowed. Intern will be suspended from patient care for three days and must complete an appropriately referenced 10-page paper on a topic chosen by the clinician or the Chair of Clinical Practice. • Infraction: Unauthorized use or possession of clinic equipment or facilities, including being present in clinic after their attending clinician has left the building. Penalty: Suspension from patient care for two weeks. Unauthorized use of copy machine will result in confiscation of copy materials and/or charge for copies and use of equipment. Clinic records, equipment, furniture, office supplies and patient files are the property of NUHS. Removal, attempted removal, and/or duplication of clinic records (without authorization), through the use of copy machines or any electronic device (e.g., camera, handheld scanner, smart phone, laptop/tablet with camera, flash drive) will result in suspension for 2 weeks and may be referred to law enforcement authorities as property theft. • Infraction: Unauthorized absence from clinic, including failure to notify clinician in a timely fashion of inability to be present at clinic shift due to illness, emergency or habitual tardiness. Interns must notify their clinician within 20 minutes of the start of their regular shift or rotation if they have an illness or emergency. Penalty: May range from making up one or more days per absence to repeating the entire trimester. • Infraction: Unsatisfactory dress/appearance or poor personal hygiene, as indicated by attending clinician. Penalty: Exclusion from clinic until the situation is rectified. Absence must be made up and additional days may be added at the clinician’s discretion. • Infraction: Failure to complete charting of patient visit, including having the record signed by attending clinician at the end of the visit, and failure to return the record to Medical Records by the end of the shift. Penalty: The intern(s) involved in the patient care for the date in question will not receive credit for the visit or services rendered. An additional two duty shifts will be made up. 60 • Infraction: Failure to record/carry out services ordered by the attending clinician. Penalty: Exclusion from patient care for two days and loss of credit for the patient service on the date in question. The intern will also be personally responsible for all services rendered but not recorded on the route slip. • Infraction: False claim for credit on clinical services or other internship (graduation) requirements. Penalty: Deduction of the falsified credit plus an additional 10 University Service Credits and an additional 40 non-student CMTs to be completed prior to graduation. • Infraction: Failure to have a professional attitude toward colleagues, other professionals, patients, clients, support staff, and professionals from other programs. If, for any reason, an intern acts with deliberate disregard of the authority of the attending clinician, the intern may be referred, by the Dean of Clinics, to the Committee on Discipline for a formal hearing where the intern’s misconduct shall be subject to the full range of disciplinary sanctions cited within the NUHS Student Code of Conduct. Penalty: Ranges from loss of patient credits to suspension from clinic duties. Depending on the nature, severity and potential for the misconduct to adversely affecting the interests or reputation of the clinic or University. Penalty may range from loss of patient credits to suspension from clinic duties for a specified period of time by the clinician. Lombard Only • Infraction: Failure to attend the mandatory trip to Standard Process Inc. Penalty: Two-for-one make-up shifts and attendance on the next trip. NOTE: Any make-up shifts ordered as a result of an infraction will be served at a time and place approved in advance by the clinic director. Under no circumstances shall such time be served prior to the beginning of “Pink Slip Week.” Pink slips will be withheld and diplomas will not be awarded until all necessary time has been completed. Hearing Procedures If an intern fails to complete a penalty, decides to dispute an assigned penalty, or the supervising clinician and the Chair of Clinical Practice deem the nature or severity of an intern’s infractions to merit additional administrative review or referral for disciplinary sanctions that may result in suspension or expulsion of the intern, then the matter shall be referred to the Dean of Clinics. The Dean of Clinics shall confer with the Dean of Students to discern which hearing procedure is best suited to address the issues resulting from the infractions while safeguarding the interests of the student and the institution. (Under the aegis of the University President, the Dean of Students functions as the primary university official responsible for the administration of the NUHS Student Code of Conduct. The Dean is also the arbiter of procedural interpretations or disputes related to intern conduct and discipline arising from alleged violations of the NUHS Clinic Intern Manual.) The hearing procedures used to conduct a formal or informal hearing are derived from the NUHS Student Code of Conduct (full text version available online at: http://www.nuhs.edu/media/175591/code_of_conduct.pdf). 61 The University system that is used to manage student conduct and discipline is not analogous to, is not equivalent to, and does not conform to, the criminal or civil law process. The NUHS Student Code of Conduct is designed, in part, to determine individual or group responsibility, or lack thereof, for violations of the NUHS Student Code of Conduct or Clinic Intern Manual only – not guilt or innocence under federal, state, or municipal laws. Disciplinary hearings shall be carried out in a manner that ensures that fairness is observed and shall not be restricted by the formal rules of evidence governing criminal and civil proceedings nor shall minor deviations from the described hearing procedures necessarily invalidate a disciplinary decision, unless significant prejudice to a student or the University may result. Informal Hearing If the Dean of Clinics elects to manage the matter through the use of an informal hearing, the intern shall be notified in writing of the issue(s) that prompted the referral and a meeting shall be scheduled for the intern to meet with the Dean. The date of the meeting shall allow the intern a reasonable time to prepare a response/explanation for committing the infraction(s). The Dean may tape record this meeting and admit record(s), witness(es), written statement(s) or exhibit(s) deemed contributory or important to a fair hearing. An advisor or an attorney shall not assist the intern. After the meeting, the Dean of Clinics shall write a brief summary report that will include a final decision (reduce or uphold the penalties assigned by the attending clinician and/or Chair of Clinical Practice and take no further action, or impose an additional disciplinary sanction). The report shall be the property of the University. This report shall be on file with the Dean of Clinics. The decision of the Dean of Clinics shall be final pending an appeal based upon the criteria set forth in the Appeal Process section of the NUHS Student Code of Conduct. Formal rules of process, procedure, and/or technical rules of evidence, such as are applied in criminal or civil court, are not used in student disciplinary proceedings. Any change in status of the intern with the University resulting from the Dean’s decision shall be transmitted in writing to the VP for Academic Services, the VP for Administrative Services, the Dean of Students, the Chair of Clinical Practice, the Attending Clinician, the Director of the Business Office, the Director of Financial Aid, and the Registrar. Formal Hearing If the Dean of Clinics elects to manage the matter through the use of a formal hearing, the Dean of Students shall notify the intern in writing and a copy of this notification shall also be forwarded to the Committee on Discipline. A formal hearing shall follow the guidelines set forth in the Hearing Procedures section of the NUHS Student Code of Conduct. Any change in status of the intern with the University resulting from the Committee’s decision shall be transmitted in writing to the VP for Academic Services, the VP for Administrative Services, the Dean of Clinics, the Dean of Students, the Chair of Clinical Practice, the Attending Clinician, the Director of the Business Office, the Director of Financial Aid, and the Registrar. 62 Chapter 8 Incident/Accident Report Procedure The following procedure must be followed whenever any accident or incident takes place in which one of our patients, students, interns, employees, or visitors is injured in any manner and from any cause while in the facilities of the National University of Health Sciences. 1. Attend to the immediate needs of the person as competently and as quickly as possible. Call for help. Make sure that the person is protected from further injury and make the site as safe as possible. If the injury is of a nature that cannot be handled by the Whole Health Center, arrangements must be made for immediate emergency medical transportation to another facility that is capable of handling trauma. No employee, student, intern, or visitor shall transport an injured person in their private vehicles. 2. Report the accident or incident immediately to the Emergency Officer of the Day (EOD). The EOD is the clinical faculty member assigned for the duration of the shift. This is a rotating position. The EOD will generate the initial Accident/Incident Report. This form is filled out in detail. See Appendix L. 3. If the Accident/Incident Report refers to a patient, a copy must be put in the patient’s medical records file. 4. The Attending Clinician or Staff Member completing the Accident/Incident Report will forward the original to their Immediate Supervisor (Chair for Clinical Practice or Clinics Business Services Coordinator). The Immediate Supervisor completes a Supervisor’s Report (See Appendix M) for the accident/incident. Both reports are forwarded to the Dean of Clinics. The Dean of Clinic’s Administrative Assistant will keep a copy of both completed forms, prior to sending the originals to Human Resources. 5. The Dean of Clinics will report the incident to the Clinic Risk Management Committee. 6. The Dean of Clinics will advise the Vice President for Academic Services of the incident and any additional information that has been found on further investigation. FLORIDA ONLY: 7. Special note for incidents/accidents that occur at the Health Education Center (HEC) of SPC, in addition to above steps: a. Contact SPC security, 727-341-3654 b. Contact the SPC Provost’s Office, 727-341-3664 c. Contact the Dean of the College of Professional Studies’ office, 727-394-6058 63 64 Chapter 9 OSHA Training and Compliance The University has an OSHA training program for the academic clinical faculty and the clinical faculty. The OSHA compliance officer is located in the clinical offices. Basic information is provided below. For information regarding the official OSHA manual and training material call extension 6851. Universal Precautions and Infection Control Barrier Precautions Barrier precautions, including gloves, should be taken to prevent contact of skin and mucous membranes with the patient’s blood or other body fluids. During venipuncture and emergency procedures, gowns, aprons and other body coverings should be worn. This covering should be able to be removed and prevent penetration of body fluids if contaminated. Gloves should be worn whenever doing venipuncture, examinations where body fluids may be contacted, or processing specimens for laboratory analysis. Precautions While Handling Sharp Devices, e.g. Needles All disposable needles, scalpels or sharp devices from invasive procedures (acupuncture, venipuncture) must immediately be placed in puncture-proof containers for disposal. No sharp device shall be left on a tabletop, examination table, or countertop. UNDER NO CIRCUMSTANCES SHOULD A SYRINGE OR NEEDLE BE RECAPPED OR LEFT UNATTENDED. PLEASE PROPERLY DISCARD OF ALL NEEDLES IN THE BIOHAZARD BINS. For the University’s purpose, all needles are disposed of properly and not autoclaved for reusable purposes. First Aid After Needle Stick If a needle stick or injury occurs in which the skin is scratched or pierced with a potentially infected device, the following procedures must be followed: • Immediate attention to the wound for decontamination must be carried out. This includes allowing bleeding if it is bleeding at the time. 65 • • • • • Wash with an antiseptic soap or other germicidal agent approved for wound management. Report incident to Infection Control Committee with the Report of Injury form available from clinical faculty or Dean of Clinics. Draw blood from individual whose body fluid is in question for possible HIV/HepB testing (with consent). Offer blood testing to injured party (with consent). Advise to watch for signs of infection and care of wound. Additional Infection Control Measures Hands and Other Skin Surfaces • Hands must be thoroughly washed before and after examining the patient and doing procedures such as acupuncture, venipuncture, gynecological and proctological examinations. • Hands and other skin surfaces that have been accidentally contaminated with blood and other body fluids must be scrubbed immediately with germicidal soap. • Hands must be washed after removing masks, gloves or other barrier devices. Mouth-to-Mouth Resuscitations (CPR) • A barrier must be used to prevent transmission of infection by saliva or blood in the mouth and/or nose. • Anyone with an active, draining skin or mucous membrane lesion must not handle the patients or equipment that will come in contact with the patient. INFECTION CONTROL PROCEDURES Prevention of Transmission of Infectious Disease The following section addresses the prevention of transmission of bloodborne pathogens, and is adapted from the NUHS Exposure Control Plan (5/92). It is in conformance with, and supplements, the CDC guidelines (“Update: Universal Precautions for Prevention of Transmission of Human immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Other Bloodbome Pathogens in Health Care Settings,” June 24, 1988) Definitions (adapted from OSHA): Blood means human blood, human blood components, and products made from human blood. 66 Bloodborne Pathogens means pathogenic microorganisms that are present in human blood and can cause disease in human. These pathogens include, but are not limited to, hepatitis B virus (HBV) and human immunodeficiency virus (HIV). Contaminated means the presence or the reasonably anticipated presence of blood or other potentially infectious materials on an item or surface. Contaminated Laundry means laundry, which has been soiled with blood or other potentially infectious materials or may contain sharps. Contaminated Sharps means any contaminated object that can penetrate the skin including but not limited to needles, scalpels, broken glass, and broken capillary tubes. Hand Washing Facilities means a facility providing an adequate supply of running potable water, soap, and single use towels, or hot air drying machines. HBV means hepatitis B virus. HIV means human immunodeficiency virus. Occupational Exposure means reasonably anticipated skin, eye, mucous membrane, or parenteral contact with blood or other potentially infectious materials that may result from duties. Other Potentially Infectious Materials means: 1. The following human body fluids: semen, vaginal secretions, synovial fluid, amniotic fluid, and any body fluids in situations where it is difficult or impossible to differentiate between body fluid; 2. Any unfixed tissue or organ (other than intact skin) from a human (living or dead); and 3. HIV-containing cells or tissue cultures, organ cultures, and HIV or HBV-containing culture medium or other tissues from experimental animals infected with HIV or HBV. Parenteral means piercing mucous membranes or the skin barrier through such events as needle sticks, human bites, cuts, and abrasions. Personal Protective Equipment is specialized clothing or equipment worn by a student or employee for protection against a hazard. General work clothes (e.g., uniforms, pants, shirts, or blouses) not intended to function as protection against a hazard are not considered to be personal protective equipment. Source Individual means any individual, living or dead, whose blood or other potentially infectious materials may be a source of occupational exposure to the intern. Examples include, but are not limited to: hospital and clinic patients; clients in institutions for the developmentally disabled; trauma victims; clients of drug and alcohol treatment facilities; 67 residents of hospices and nursing homes; human remains; and individuals who donate to sell blood or blood components. Sterilize means to use physical or chemical procedures to destroy all microbial life including highly resistant bacterial endospores. Universal Precautions is an approach to infection control. According to the concept of Universal Precautions, all human blood and certain human body fluids are treated as if known to be infectious for HIV, HBV and other bloodborne pathogens. Universal precautions have been recommended by the CDC to protect health care workers from bloodborne diseases and should be consistently used for all patients. The update specifies the body fluids that universal precautions apply to: • blood • any body fluid containing visible blood • semen • vaginal secretions • tissues Universal precautions do not apply to feces, nasal secretions, sputum, sweat, tears, urine, and vomitus unless they contain visible blood. Some special settings may require protective barriers such as health care workers wearing gloves in breast milk banks or dental workers wearing gloves, masks and protective eyewear during dental procedures. As stated by the CDC, “Blood is the single most important source of HIV, HBV and other bloodborne pathogens in the occupational setting. Infection control efforts for HIV, HBV and other bloodborne pathogens must focus on preventing exposures to blood as well as delivery of HBV immunization.” Universal precautions are meant to complement routine infection control practices in health care facilities, such as hand washing and using protective barriers in other situations of gross microbial contamination. The judgment of the health care worker must be depended upon for specific clinical situations. The university formally adopts the use of Universal Precautions, and all human blood and certain human body fluids shall be treated as if known to be infectious for HIV, HBV and other bloodborne pathogens. Proper Needle Use and Disposal Self-sheathing needles will be used whenever possible. Contaminated needles are to be immediately disposed of in a sharps device located in the room. Recapping of needles is not permitted. In the unforeseen event that a needle has been used but no sharps container is available or operational in the room, a one-handed scoop method of recapping 68 (the cap lays on a flat surface) shall be used; such occurrences are to be reported to the intern’s supervisor verbally and by a written incident report form. Needles are to be removed from vacutainer holders only by the device on the lid of the sharps container; removal of needles by hand is not permitted. Containers Containers used for disposal of contaminated sharps will be closable, puncture-resistant, and leak proof on the sides and bottom. The containers will be red in color or labeled with the biohazard symbol. Cardboard sharps containers are not permitted. Sharps containers will be located in the rooms where sharps are used. It is not acceptable to have to transport a sharp into another room for disposal. In the clinics, sharps containers will be located in the following areas: patient examination rooms, clinical laboratory, electrodiagnosis room, and acupuncture rooms. Additionally, each portable phlebotomy tray shall have a sharps container. Sharps containers shall be monitored on a bi-weekly basis and changed as needed to prevent overfilling. Small (hand-sized) containers shall be disposed of when no more than half (50%) full. Large (pint and larger) containers shall be disposed of when no more than three-quarters (75%) full. Monitoring of the containers shall be done by the clinic director/supervisor or their designee; such person shall be named at the beginning of each academic trimester, as well as the alternate in case of vacation. A log of inspection and replacement of sharps containers shall be kept. Any intern who discovers a sharps container, which is overfilled, shall report such to the clinic director/supervisor. Sharps containers in patient rooms shall be kept out of the reach of small children. Sharps containers shall be transported in an upright position and provided with support to prevent tipping during transport. Management of Broken Glassware and Spills Only mechanical means (tongs, brush and dust pan) shall be used to clean up broken glassware. The use of bare or gloved hands to directly pick up broken glass is not permitted. Tools used in cleanup of contaminated broken glass should be disinfected after use. Broken glassware shall be placed in sharps containers. Spills of blood and potentially contaminated fluids shall be wiped up with absorbable material, which shall then be placed into biohazard containers. The spill area shall be decontaminated with a tuberculocidal germicidal disinfectant. Hand Washing Hand washing facilities are also available to the interns who incur exposure to blood or other potentially infectious materials. OSHA requires that these facilities be readily accessible after 69 incurring exposure. At this facility, hand washing facilities are located in patient examination and treatment rooms, laboratories, and restrooms. Interns shall wash hands with soap and water when gloves are removed and as soon as possible after any contact with blood or other potentially infectious materials. At locations where hand washing facilities are not reasonably accessible (for example, offcampus health screening activities), antiseptic towelettes or antiseptic hand cleaners may be used until the hands can be washed with soap and running water. If interns incur exposure to their skin or mucous membranes, then those areas shall be washed or flushed with water as soon as feasible following contact. Eating and Personal Care Interns may not eat, drink, apply cosmetics or lip balm, or handle contact lenses in contaminated work areas. Food and beverages may not be kept in refrigerators, cabinets, shelves, countertops, or other areas with blood and other potentially infectious materials. Food and drink may not be temporarily placed on any surface, which may be contaminated, or near any device that may generate splashes, sprays, or droplets of blood or other potentially infectious materials. All procedures will be conducted in a manner that will minimize splashing, spraying splattering, and generation of droplets of blood or other potentially infectious materials. The method that will be employed at this facility to accomplish this goal is to have covers on all centrifuges used in the laboratory. Decontamination of Laboratory Equipment Prior to Servicing Any contaminated laboratory equipment, or other equipment that may come into contact with blood or other potentially infectious materials, being transferred or shipped for servicing shall be decontaminated prior to transport. In the case of highly technical or sensitive equipment and/or equipment with limited access to contaminated parts, at least partial decontamination shall be performed. Transportation of Specimens and Other Potentially Infectious Materials Blood samples and other potentially infectious materials being transported between clinics or other campus locations shall be placed in a container that prevents leakage during transport. The container shall be red or red-orange or labeled with the biohazard symbol. If the materials are capable of puncturing their container, the primary container shall be placed within a secondary, puncture-resistant container. Blood-contaminated waste and other potentially infectious materials being disposed of in any location shall be placed in a biohazard container that prevents leakage during storage. The container shall be red or red-orange or labeled with the biohazard symbol. If a container shows 70 evidence of contamination on the outside of the container, or if leakage of contents has occurred, the primary container should be placed in a secondary container and removed for proper disposal. Infectious waste shall not be placed in ordinary waste disposal containers. Any contaminated sharps shall be disposed of as described previously in this plan. Mouth Pipetting / Suctioning Mouth pipetting or suctioning of specimens is strictly prohibited. Personal Protective Equipment All garments that are penetrated by blood shall be removed immediately or as soon as feasible. All personal protective equipment will be removed prior to leaving the work area. The following protocol has been developed to facilitate leaving the equipment at the work area: Personal Protective Equipment Storage Site Gloves (laboratory) Single-use gloves are disposed after use Lab Coat (Clinic Lab) Clinic Laboratory Janse Hall Phlebotomy (Lab Diagnosis) Laboratory Interdisciplinary Research Laboratory Protective eyewear With endoscopic kits Clinic Laboratory Interdisciplinary Research Laboratory Utility Gloves Clinic Laundry Maintenance Department Examination Gloves Single-use gloves are disposed after use Use of Gloves Disposable (single-use) gloves shall be worn when performing venipuncture, acupuncture, when in contact with blood, mucous membranes, non-intact skin, or potentially infectious materials is anticipated, or when handling or touching contaminated items or surfaces. Gloves shall be available in the following sites: patient examination rooms, clinical laboratory, patient records/dispensary, electrodiagnosis room, colonic irrigation room, radiology suites, Interdisciplinary Research Laboratory, Janse Hall Phlebotomy (Laboratory Diagnosis) Laboratory, Physiology Laboratory, Biochemistry Laboratory, chiropractic technique and anatomical laboratories. Disposable (single-use) gloves may not be reused. Powderless gloves or hypoallergenic gloves will be available in each facility for use by interns who need them. Reusable (utility) gloves shall be used by laundry personnel when handling potentially contaminated linens. These should be decontaminated after each use and discarded if they show 71 signs of cracking, peeling, tearing, puncturing, deterioration, or failure to provide a protective barrier. Disinfectants shall be germicidal and tuberculocidal. Disposable Patient Gowns for Colonic Irrigation Patients receiving colonic irrigation or enemas shall be gowned in paper, disposable gowns. These gowns are to be placed in biohazard containers after use. Regular linen gowns shall not be used on these patients, however if a linen gown is accidentally used, it shall be placed in a red biohazard bag and taken to be autoclaved prior to being taken to the laundry. Decontamination of Work Surfaces Contaminated work surfaces must be decontaminated with a germicidal tuberculocidal disinfectant upon completion of procedures or when contaminated by splashes, spills, or contact with blood, other potentially infectious materials, and at the end of the work shift. Countertops may be protected with nonabsorbent materials, however these must be inspected frequently for contamination and changed when found to be contaminated. Waste Cans and Pails Waste cans and pails must be inspected and decontaminated on a regularly scheduled basis. Waste cans and pails in patient rooms are to be used only for disposal of non-contaminated materials; visibly contaminated materials are to be placed in biohazard containers. Biohazard Labeling Refrigerators and freezers that contain blood or other potentially infectious materials shall be clearly labeled with the universal biohazard symbol. Only the OSHA-approved universal biohazard symbol shall be used for labeling blood and potentially infectious material containers at NUHS. That symbol must be black (or very dark) on a red or orange-red background. Existing non-approved symbols will be replaced with the approved label. There will be no biohazard labeling of patients’ charts or laboratory specimens. Resuscitation Equipment One-use emergency airway resuscitation equipment will be available in each clinic. Mouth-to-mouth resuscitation should not be performed if one-use resuscitation equipment is available. Patient Examination Equipment Disinfection High-level disinfection is required for re-usable items that come in contact with mucous membranes (e.g., reusable specula, endoscopes) 72 Approved types of disinfectants include: • Gluteraldehydes (10 minutes minimum contact) • Phenols or Iodophors (1 minute minimum contact) Management of Exposure Incident The following section has been taken from the NUHS Policy on Management of Employees and Students Accidentally Exposed to Blood or Other Potentially Infectious Materials. Upon any accidental percutaneous (needle stick, laceration, abraded or inflamed skin, or bite), or permucosal (ocular or mucous membrane) exposure to blood and other potentially infectious materials, the following steps shall be taken: • Clean the site of exposure as soon as possible. In the case of percutaneous exposure, the area should be irrigated thoroughly with soap and water, while encouraging bleeding of the site by squeezing the area. A topical disinfectant (Betadine) should then be applied for at least one minute (exposed persons should be questioned about iodine sensitivity prior to Betadine application). In the case of permucosal exposure, the surface should be irrigated with water for at least 15 minutes. • Notify the exposed person’s supervisor and fill out an incident report form. • Obtain a blood sample from the person who was the source of exposure and test for HBsAg (Hepatitis B surface antigen) and antibodies to HIV. Testing may be done on existing blood samples without the patient’s consent in situations involving accidental exposure of a health care worker in Illinois. The source patient’s name should be included on the incident report form. The order for the test should not appear in the patient’s medical record. • Determine if source patient is at high risk of HIV or HBV infectious (i.e., history of homosexual or bisexual contact, IV drug abuser, hemophiliac, etc.). • If the source patient is seronegative for HBV and HIV, no further action is necessary unless the source patient was determined to be at high risk of HBV or HIV. In this case, HIV and HBV testing should be performed on the exposed persons at the time of the exposure and in twelve (12) weeks. Written consent from the exposed person must be obtained for HIV testing. Additionally, the exposed person should be advised to report any acute febrile illness that occurs within 12 weeks after exposure. • If the source patient refuses to allow a sample of blood to be collected, if the source patient has AIDS, if the source patient is positive for HIV, or if the source is unknown: o Counseling should be arranged for the exposed person o HIV testing should be performed as soon as possible, with written consent, and repeated at 6 weeks, 12 weeks, 6 months, and 12 months after exposure. 73 o For at least the first 12 weeks, the exposed person should be advised on prevention of transmission of bloodborne diseases (i.e., practice safe sexual practices, refrain from blood donations, etc.) • If the source patient refuses to allow a sample of blood to be collected, if the source patient has Hepatitis B, if the source patient is positive for HBsAg, or if the source is unknown: o Counseling should be arranged for the exposed person. o The hepatitis B vaccination and anti-HBs (antibody to HB surface antigen) status (if known) of the exposed person should be reviewed. If the exposed person has not been vaccinated (or has not finished the vaccination series) against HBV, they will be immediately referred for vaccination and administration of HB immune globulin. If the exposed person has previously been vaccinated, testing for anti-HBs should be done; if there is adequate antibody, no further treatment is necessary; however, if the antibody level is inadequate, referral for HBIG and vaccination booster should be performed. o For at least the first 12 weeks, the exposed person should be advised on prevention of transmission of bloodborne diseases (i.e., practice safe sexual practices, refrain from blood donations, etc.) Protocol for HIV Test-Positive Patients: Salvation Army Clinics This protocol has been developed to assure that each patient is handled in a professional and consistent manner. Every effort will be made to assure that each patient receives appropriate medical follow-up and counseling and that each case is handled individually and confidentially. 1. Patients receiving physical examinations at the Salvation Army chiropractic clinics will be questioned on current and previous drug use history and sexual contacts as well as other factors that may predispose to AIDS. 2. All patients that test HIV-positive will be confirmed by the Western Blot before the patient is informed of a test-positive. 3. Upon confirmation of the Western Blot, the patient will be informed that a positive test has been received. At this time, the patient will be informed of the confidentiality and reporting policies of the chiropractic clinic as they relate to the Salvation Army administration. 4. Every effort will be made at this point to assure that the patient receives the appropriate follow-up and counseling needed to assist in dealing with psychological and medical problems that may arise. 5. Personnel will be identified within the staff at Salvation Army to assist the patient. 74 6. The patient will also be referred to either Freedom Center or the Sacred Heart Hospital for medical evaluation. 7. If a diagnosis of AIDS is established, the patient will be referred to Howard Brown Memorial Clinic or another appropriate facility for care. 8. If there are no symptoms to suggest AIDS, the patient will be referred to TPAN (test positive awareness network) or another facility for appropriate follow-up care. 9. Every effort will be made to assign patients that test positive, but have not yet contracted AIDS, to tasks that are not at risk for immune compromise. These policies will be reviewed periodically and updated as new data become available. 75 NATIONAL UNIVERSITY OF HEALTH SCIENCES Request and Consent for Testing for Antibodies to the Human Immunodeficiency Virus Last Name First Name Middle Name Address City Patient Number Day Telephone State Sex Zip Code Race Evening Telephone Birthdate Date of Request 1. I am requesting a blood test to detect the presence of antibodies to the Human Immunodeficiency Virus (HIV), the virus that causes Acquired Immunodeficiency Syndrome (AIDS). I have been advised that the procedure, which involves the withdrawal by needle of a small amount of blood for laboratory testing (about 1-1/2 Tablespoons), may cause some slight discomfort at the site of entry of the needle, and that the procedure has minimal risks, such as bruising, soreness, and a slight risk of infection. 2. I have been provided with information about the test for antibodies to the HIV virus, about the HIV virus, and about AIDS, and I have been given the opportunity to ask questions regarding this information and have my questions answered. 3. I have been informed that both my request for the HIV virus test and the test results are considered confidential and will be released only to me except as required by law. This request form and the laboratory report represent the only records that will be maintained on my test and its results by National University of Health Sciences. 4. Personnel handling these records have been carefully selected and trained to ensure that procedures for maintaining my privacy are followed without exception. The request form is maintained apart from the laboratory report and both will be destroyed by shredding within from the date of the test, which is the retention period established in conformance with state law. 5. I will be solely responsible for seeking any further care that I might require, including immunization when such a breakthrough occurs. 6. I understand that if the test results are positive that I will be provided information on counseling services available to those infected with HIV virus and I will be advised to see a physician both for my own health care and so that I might take adequate precautions to prevent transmission of the virus to others. 7. I understand that if the test results are positive and that if I do not collect my test results within one month of the date of this request, a diligent effort will be made to locate me. In order not to violate my privacy, National University of Health Sciences will not identify itself in correspondence or its staff will not identify themselves in any telephoned contact, but will simply request that I call the number of the facility. I agree to assume all risks that may result if I do not collect my test results. 8. Because DuPage County law requires reporting of individuals with antibodies to the HIV virus, I understand that if the test results are positive and after ensuring the accuracy of the test results, they will be submitted to the DuPage County Health Department. Signature of Individual Date 76 Note: The following forms relating to HIV are subject to change because of revisions in public health regulations. NATIONAL UNIVERSITY OF HEALTH SCIENCES Patient’s Billing Consent for HIV Testing I consent to allow the disclosure of my name, address, birthdate, name of the test(s), and the charge to Medicaid or other medical assistance programs. Patient’s Full Name: Birthdate: Address: City: State: Zip Code: Medicaid Number: I do not give my consent to release the name of the test(s) to my insurance company, or medical assistance program. I will pay the bill myself. Signature: I also authorize the following persons or agencies access to my HIV antibody test results: Name of Person/Agency To Date Valid Name of Person/Agency To Date Valid 77 OSHA Compliance Acknowledgement of Training I acknowledge that I have watched the training program. I have completed the quiz and reviewed any areas where I felt I needed more training or information. Student Printed Name: Student Signature: Date of Completion: Clinician’s Printed Name: Clinician’s Signature: 78 Chapter 10 HIPAA Training and Compliance Health Insurance Portability and Accountability Act USES AND DISCLOSURES FOR TREATMENT, PAYMENT, AND HEALTH CARE OPERATIONS [45 CFR 164.506] Background The HIPAA Privacy Rule establishes a foundation of Federal protection for personal health information, carefully balanced to avoid creating unnecessary barriers to the delivery of quality health care. As such, the Rule generally prohibits a covered entity from using or disclosing protected health information unless authorized by patients, except where this prohibition would result in unnecessary interference with access to quality health care or with certain other important public benefits or national priorities. Ready access to treatment and efficient payment for health care, both of which require use and disclosure of protected health information, are essential to the effective operation of the health care system. In addition, certain health care operations—such as administrative, financial, legal, and quality improvement activities—conducted by or for health care providers and health plans, are essential to support treatment and payment. Many individuals expect that their health information will be used and disclosed as necessary to treat them, bill for treatment, and, to some extent, operate the covered entity’s health care business. To avoid interfering with an individual’s access to quality health care or the efficient payment for such health care, the Privacy Rule permits a covered entity to use and disclose protected health information, with certain limits and protections, for treatment, payment, and health care operations activities. How the Rule Works What are Treatment, Payment, and Health Care Operations? The core health care activities of “Treatment,” “Payment,” and “Health Care Operations” are defined in the Privacy Rule at 45 CFR 164.501. • “Treatment” generally means the provision, coordination, or management of health care and related services among health care providers or by a health care provider with a third party, consultation between health care providers regarding a patient, or the referral of a patient from one health care provider to another. • “Payment” encompasses the various activities of health care providers to obtain payment or be reimbursed for their services and of a health plan to obtain premiums, to fulfill their 79 coverage responsibilities and provide benefits under the plan, and to obtain or provide reimbursement for the provision of health care. In addition to the general definition, the Privacy Rule provides examples of common payment activities, which include, but are not limited to: o o o o Determining eligibility or coverage under a plan and adjudicating claims; Risk adjustments; Billing and collection activities; Reviewing health care services for medical necessity, coverage, justification of charges, and the like; o Utilization review activities; and o Disclosures to consumer reporting agencies (limited to specified identifying information about the individual, his or her payment history, and identifying information about the covered entity). • “Health care operations” are certain administrative, financial, legal, and quality improvement activities of a covered entity that are necessary to run its business and to support the core functions of treatment and payment. These activities, which are limited to the activities listed in the definition of “health care operations” at 45 CFR 164.501, include: o Conducting quality assessment and improvement activities, population-based activities relating to improving health or reducing health care costs, and case management and care coordination; o Reviewing the competence or qualifications of health care professionals, evaluating provider and health plan performance, training health care and non-health care professionals, accreditation, certification, licensing, or credentialing activities; o Underwriting and other activities relating to the creation, renewal, or replacement of a contract of health insurance or health benefits, and ceding, securing, or placing a contract for reinsurance of risk relating to health care claims o Conducting or arranging for medical review, legal, and auditing services, including fraud and abuse detection and compliance programs; o Business planning and development, such as conducting cost-management and planning analyses related to managing and operating the entity; and o Business management and general administrative activities, including those related to implementing and complying with the Privacy Rule and other Administrative Simplification Rules, customer service, resolution of internal grievances, sale or transfer of assets, creating de-identified health information or a limited data set, and fundraising for the benefit of the covered entity. General Provisions at 45 CFR 164.506. A covered entity may, without the individual’s authorization: • Use or disclose protected health information for its own treatment, payment, and health care operations activities. For example: 80 o A hospital may use protected health information about an individual to provide health care to the individual and may consult with other health care providers about the individual’s treatment. o A health care provider may disclose protected health information about an individual as part of a claim for payment to a health plan. o A health plan may use protected health information to provide customer service to its enrollees. • A covered entity may disclose protected health information for the treatment activities of any health care provider (including providers not covered by the Privacy Rule). For example: o A primary care provider may send a copy of an individual’s medical record to a specialist who needs the information to treat the individual. o A hospital may send a patient’s health care instructions to a nursing home to which the patient is transferred. • A covered entity may disclose protected health information to another covered entity or a health care provider (including providers not covered by the Privacy Rule) for the payment activities of the entity that receives the information. For example: o A physician may send an individual’s health plan coverage information to a laboratory that needs the information to bill for services it provided to the physician with respect to the individual. o A hospital emergency department may give a patient’s payment information to an ambulance service provider that transported the patient to the hospital in order for the ambulance provider to bill for its treatment. • A covered entity may disclose protected health information to another covered entity for certain health care operation activities of the entity that receives the information if: o Each entity either has or had a relationship with the individual who is the subject of the information, and the protected health information pertains to the relationship; and o The disclosure is for a quality-related health care operations activity (i.e., the activities listed in paragraphs (1) and (2) of the definition of “health care operations” at 45 CFR 164.501) or for the purpose of health care fraud and abuse detection or compliance. For example: < A health care provider may disclose protected health information to a health plan for the plan’s Health Plan Employer Data and Information Set (HEDIS) purposes, provided that the health plan has or had a relationship with the individual who is the subject of the information. • A covered entity that participates in an organized health care arrangement (OHCA) may disclose protected health information about an individual to another covered entity that participates in the OHCA for any joint health care operations of the OHCA. For example: o The physicians with staff privileges at a hospital may participate in the hospital’s training of medical students. Uses and Disclosures of Psychotherapy Notes. Except when psychotherapy notes are used by the originator to carry out treatment, or by the covered entity for certain other limited health care operations, uses and disclosures of psychotherapy notes for treatment, payment, and health care operations require the individual’s authorization. See 45 CFR 164.508(a)(2). 81 Minimum Necessary. A covered entity must develop policies and procedures that reasonably limit its disclosures of, and requests for, protected health information for payment and health care operations to the minimum necessary. A covered entity also is required to develop rolebased access policies and procedures that limit which members of its workforce may have access to protected health information for treatment, payment, and health care operations, based on those who need access to the information to do their jobs. However, covered entities are not required to apply the minimum necessary standard to disclosures to or requests by a health care provider for treatment purposes. Consent. A covered entity may voluntarily choose, but is not required, to obtain the individual’s consent for it to use and disclose information about him or her for treatment, payment, and health care operations. A covered entity that chooses to have a consent process has complete discretion under the Privacy Rule to design a process that works best for its business and consumers. A “consent” document is not a valid permission to use or disclose protected health information for a purpose that requires an “authorization” under the Privacy Rule (see 45 CFR 164.508), or where other requirements or conditions exist under the Rule for the use or disclosure of protected health information. Right to Request Privacy Protection. Individuals have the right to request restrictions on how a covered entity will use and disclose protected health information about them for treatment, payment, and health care operations. A covered entity is not required to agree to an individual’s request for a restriction, but is bound by any restrictions to which it agrees. See 45 CFR 164.522(a). Individuals also may request to receive confidential communications from the covered entity, either at alternative locations or by alternative means. For example, an individual may request that her health care provider call her at her office, rather than her home. A health care provider must accommodate an individual’s reasonable request for such confidential communications. A health plan must accommodate an individual’s reasonable request for confidential communications, if the individual clearly states that not doing so could endanger him or her. See 45 CFR 164.522(b). Notice. Any use or disclosure of protected health information for treatment, payment, or health care operations must be consistent with the covered entity’s notice of privacy practices. A covered entity is required to provide the individual with adequate notice of its privacy practices, including the uses or disclosures the covered entity may make of the individual’s information and the individual’s rights with respect to that information. HIPAA Frequently Asked Questions: Search FAQs by category at: http://www.hhs.gov/ocr/privacy/hipaa/faq/index.html OCR HIPAA Privacy December 3, 2002 Revised April 3, 2003 82 HIPAA Privacy Compliance Acknowledgement of Training I acknowledge that I have watched the training program. I have completed the quiz and reviewed any areas where I felt I needed more training or information. Student Printed Name: Student Signature: Date of Completion: Trainer’s Printed Name: Trainer’s Signature: 83 84 Chapter 11 Business Office Procedures Photocopying • Photocopying is restricted to materials from the patient record and is done during normal business office hours. • No personal materials are to be photocopied on business office copiers. • A fee for photocopying is charged to the patient. • Only the clinic business office manager can authorize copying to be done by interns. A request must be filed that contains the name of the patient requesting copies, data submitted and number of copies needed. • Copies needed for the patient will be made immediately if approved by an attending clinician and submitted with a current completed release form signed by the patient. • Other materials require the approval of the clinic director and business office manager and will incur a copying fee payable at the time copies are made. New Patients New patients are scheduled at any convenient time for the attending clinician. Only the attending clinician will authorize the overbooking of a schedule. All calls will be directed to the attending clinician by the front desk. The attending clinician will direct the front desk to either overbook or not and the patient will then be given the next most convenient appointment time. A maximum of 120 minutes will be considered acceptable for the time needed to attend to the usual new patient’s needs on the first visit. Emergency situations may alter this time span. To assure the most equitable distribution of patient load across the clinical practices, the following procedure for scheduling will be followed: • The new patient calling to schedule an appointment will be asked if they have been referred to a specific doctor. If they have been directly referred to a specific attending clinician, the appointment is made with that doctor. 85 • If no direct referral is indicated, the patient will be asked if they have a time preference for the morning or afternoon. • Once the shift preference has been determined, a rotation system of scheduling is in place to distribute the new patients across the clinic system. Patient Appointments All appointments and/or rescheduling of appointments must be done by the patient through the front desk personnel. Return visits are scheduled from the information entered at the top right hand corner of the route slip by authorization of the attending physician. An entry in the upper right corner of the route slip designated "d/c" means the patient is not to be rescheduled and treatment is to be discontinued. If a patient reschedules or does not keep their appointment, the front desk personnel will call the patient to determine the circumstances of the missed appointment and reschedule them for a future date, if appropriate. The front desk will forward all questions regarding care to the attending physician for follow-up. Interns MUST note in the medical record that a patient has rescheduled or missed an appointment. Each medical file date stamp must have an entry next to it indicating what took place on that date. Notation of reason for missing the appointment and date rescheduled should be entered. The clinician must sign such entries. Routing of Patients After signing in, the Duty Intern escorts the patient to the treatment room and places the folded route slip into the holder on the door. After the treatment is finished, the patient goes to the cashier. The completed route slip MUST accompany the patient to the cashier station. File entries are NOT to be made at the cashier’s station or the business office area. The next appointment time should be listed in the upper right hand corner of the route slip. Correct completion of the route slip includes making sure that all procedures carried out at the treatment are listed on the route slip. Failure to list a service that was carried out will result in the intern being personally financially responsible for the charge. The intern must write their threedigit intern number in the box to the left of the charged service. This will enable proper credit to be granted. The date of the next visit must be listed in the upper right hand corner. The attending physician must sign all route slips. The intern must not list fees for the services rendered, as this is the responsibility of the cashier/business office. All financial arrangements are made by the business office ONLY. No intern is to discuss or otherwise indicate payment arrangements for patients. This is not the privilege of the intern. Direct all financial questions to the business office and/or clinic director. 86 Chapter 12 Clinic Community Outreach Events Clinic Community Outreach Hours Needed to Graduate – 20 Hours All forms can be found at: http://clinicalinfo.nuhs.edu (See Appendix J & K) • The Dean of Clinics approves all events. The completed paperwork/forms need to be submitted at least 2 weeks in advance of the event. • “Observed/assessed” CMT credits can be acquired only in the clinic setting. Interns can still acquire “CMT” credits by providing manual services to participants at outreach events. • When the event is approved, a Clinician or the Administrative Assistant to the Dean of Clinics will communicate with the contact person for the event, not the intern. Interns may research the event, event dates and event coordinator, but must then give the information to the Clinician or Administrative Assistant to the Dean of Clinics. • Having a Clinician or Administrative Assistant to the Dean of Clinics as the contact person will accomplish three things: 1. There will be one NUHS representative contacting all outside event coordinators. 2. The Clinician or Administrative Assistant to the Dean of Clinics will be more knowledgeable as to what NUHS has to offer in all programs and can promote NUHS appropriately. 3. Event information will be kept on file by the Clinician or Administrative Assistant to the Dean of Clinics for future years and not lost when interns graduate. COMMUNITY OUTREACH EVENT PROCEDURE STEP 1: GET APPROVAL To get approval to attend an outreach event, fill out the boxed part of the Outreach Record sheet and give to the Administrative Assistant to the Dean of Clinics, Room 535. (Aurora, Chicago and Florida, may email the records sheet to [email protected]) Please include the location of the event and the event’s start and end times. Remember, NUHS does not attend events where there is a monetary charge to participate. The Administrative Assistant will give the form to the Dean of Clinics to approve or deny. This will get the event on the books and reserve one of the three Outreach Storage Bins, which contains materials that will be needed for the event. This also will get the 87 event on the calendar and eventually on the Outreach report that is sent monthly to the NUHS vice presidents. SIMULTANEOULY– STEP 2: FIND A CLINICIAN If an intern submitted the Outreach Record or the Clinician who submitted the event cannot attend: Find a Clinician who is available to attend and supervise group. If intern cannot find a Clinician, the Administrative Assistant will try to find one. Remember, without a clinician in attendance, no treatments can be given; only marketing materials can be handed out. SIMULTANEOUSLY STEP 3: CONTACT WITH EVENT COORDINATOR If the Clinician has already confirmed attendance at the event with the event’s coordinator, then this step is not needed. While the Administrative Assistant is finding a Clinician to supervise the event, she will make contact with the event’s coordinator (per the Dean’s request) to determine if NUHS is acceptable for participation. If there are any specific questions regarding the event, note them on the initial paperwork before it is submitted so the Administrative Assistant, who will then get the answers while contacting the event’s coordinator to determine NUHS’ acceptability for participation. STEP 4: RECRUIT OTHER INTERNS Recruit other interns to attend. In some cases, the Clinician will offer the event to his interns first, but make sure there are enough interns to run the event. STEP 5: A WEEK BEFORE THE EVENT Stop by the Administrative Assistant’s office in Room 535 to remind her that an Outreach Storage Bin or tent(s) has been reserved and that she has the paperwork and storage bin in reserve for your event. STEP 6: A DAY BEFORE THE EVENT A day before the event, pick up the storage bin and/or tent(s) in Room 533. Inside the storage bin you will find all that you will need for the event, but you will still need to provide your own business cards. There are three Outreach Storage Bins for Lombard. Florida, Aurora and Chicago have their own bins, but Chicago and Aurora will need to make an appointment with the Administrative Assistant to pick-up their tent(s). Outreach Storage Bin Contents: • NUHS table cover • Table wipes • Rubber gloves • Pens to write with. No pens for giving away! Phone # is incorrect! 88 • • • • • • • Clipboards with Intake Forms Weekly Outreach Tally Sheets Table paper Hand antiseptic Samples of Bio Freeze 2 different NUHS brochures Garbage bags Tent(s) • There are three tents – (two black and a red). • Tents must be reserved one week in advance when verifying paperwork with the Administrative Assistant. First come, first served basis. • Two buckets of sand are also needed to weigh down the tents. Each bucket of sand is 50 pounds in weight. It is mandatory to use the sand buckets due to a previous accident. STEP 7: ATTEND THE EVENT AND HAVE PAPERWORK PROPERLY SIGNED • • • Make sure to get patient signatures and Clinician’s approval signature. Print names of patients on Tally Sheet. Copies of all paperwork can also be found at: http://clinicalinfo.nuhs.edu If this event is only for marketing or presentation purposes, different paperwork asking for Credit Hours needs to be completed and approved by the Dean of Clinics. This paperwork can also be found at: http://clinicalinfo.nuhs.edu STEP 8: EVENT COMPLETED • If paperwork is filled out correctly and submitted for credit or record maintenance, the event is closed and can be reported and Tally Credits entered. • Return Outreach Storage Bin and/or tents to Room 533, the day after the event or the next business day. STEP 9: AFTER EVENT The Clinician who attends the event must grade the event from 1 to 5; 1 being an excellent event that we should do again. Also there is a comment section, for making notes about the event. Grades and comments can be sent by email to the Administrative Assistant after the event. FINAL NOTES • In addition to earning outreach numbers needed to graduate, the main reason for OUTREACH is to encourage more patients to visit our clinics AND to promote NUHS and our services to the public. 89 • • • Attending events that are more than 15 to 20 miles away from one of our clinics defeats the purpose of getting more patients into those facilities. Attending events during clinic hours needs special approval by the Dean of Clinics. No “observed/assessed” CMT credits are allowed during outreach events. They are only allowed within the clinic hours. 90 Chapter 13 NUHS Clinical Clerkship Program Note: Appendices N, O, P and Q refer to this chapter. NUHS is responsible for ALL education that is given to its students from beginning to commencement and the outcomes of that education must be reflected on the NUHS student transcript. This is a responsibility that mandates that all individuals who teach our students, whether here or in our clinic system or elsewhere are of a caliber that meets NUHS Academic Standards and the NUHS Mission and Goals. This means that: 1. All people who teach our students must be approved faculty members. 2. All faculty members must be teaching from the same set of academic principles that are guided by the “Programmatic Purpose Statements,” and the Institutional Mission and Goals. 3. All instruction must meet the test of being broad scope primary care oriented (as required by the CCE and CNME Standards). Since January 2010 and in consequence of these factors, all doctors who function as adjunct faculty, whether in the Ancillary Clinical Education (ACE) clerkship, the Community-Based Internship (CBI), or the Clinical Clerkship Rotations (such as the VA program at Danville) are chosen by the University. Any intern who wishes to serve part or all of an internship in an offcampus setting will first need to obtain a form from the Clinic Services Manager will need to be approved by the respective clinician and the Dean of Clinics prior to taking the next step. Each such intern will need to meet certain academic standards as well. Upon approval the intern will be assigned to an appropriate clerkship. The prerequisite steps needed for students to apply to work with an approved adjunct faculty member can be found in Appendix N entitled “Clinical Clerkship Qualifications and Application Requirements.” The process for participating in a clinical clerkship can be found in Appendix O entitled “Ancillary Clinical Experience (ACE) Basics” and in Appendix P entitled “Clinical Based Internship (CBI) Basics.” 91 Clerkship Frequently Asked Questions Students should be sure to read the following information before contacting the Administrative Assistant to the Dean of Clinics, Vicki Shargo, with any questions or requests for application forms. Answers to the most commonly asked questions can be found here. Once interns are in their 9th trimester and have completed the prerequisites, they should follow the following steps: Step 1 – Interns Read the three definition sheets (“Clinical Clerkship Qualifications and Application Requirements,” “Ancillary Clinical Experience (ACE) Basics” and “Clinical Based Internship (CBI) Basics”) and become familiar with all the prerequisites. Step 2 – Interns When interns reach their 9th trimester and have met all of the prerequisites, they will need to contact the Administrative Assistant to the Dean of Clinics, Vicki Shargo, for the “NUHS Clinical Clerkship Program – Intern Eligibility Form.” After the Registrar and all the other necessary individuals have signed the form, the intern will be given the appropriate application to complete. Once the intern returns the completed application and requested paperwork to the Administrative Assistant to the Dean of Clinics, the intern will be told when he has been approved and is available to start the clerkship. The intern will then be asked to fill out the “Clinical Clerkship Program Assignment Request Form,” which will give the starting and ending dates and times for the clerkship. This form must be signed by the following: • Adjunct faculty member doctor • Intern’s attending clinician • Chair of Clinical Practice • Clinic Services Manager • Dean of Clinics • Intern Once this form is completed and returned to the Clinic Services Manager, the clerkship can begin on the agreed upon start date. In some cases, an intern may want to carry out their clerkship with a specific doctor who has not been formally approved by the university’s Clinical Clerkship Committee. To allow enough time for the doctor to complete the application process, the doctor can apply during the intern’s 8th trimester to early 9th trimester. A CBI clerkship doctor needs to be located within 75 miles of any of the NUHS clinics and have radiology equipment on site, so the intern is able to complete his numbers needed to graduate. In an ACE clerkship, the intern must have all their numbers needed to graduate completed and approved by the Clinic Services Manager before they are allowed to begin their clerkship. 92 The doctor must complete the following steps in sufficient time for their application to be processed through committee: Step 1 – Interested Doctors 1. Send a letter of interest on practice letterhead addressed to: Dr. Theodore L. Johnson, Jr., Dean of Clinics. If they have a specific intern in mind, the intern’s name should be mentioned in the letter of interest. 2. Send a current CV. 3. Both the letter and CV Both documents can be emailed to [email protected] Step 2 – Applying Doctors Once the letter and CV are received, the appropriate application will be sent to the doctor to complete and return with the additional paperwork requested in the application. Please note: If the doctor has other doctors in his practice that will also be teaching the intern, they, too, must fill out their own application form and be approved. Step 3 – Approval of Applicants 1. Once the doctor has returned the application and additional paperwork, the application file is sent to the Clinical Clerkship Committee, a group of five faculty members, who will review the application. 2. Once all five members have graded the application, they will give their recommendation to the Dean of Clinics, who can agree or disagree with the committee. 3. Next, the application and recommendation is given to the Vice President for Academic Services (VPAS), who can agree and disagree. 4. The committee recommendation plus the recommendation of the VPAS is then given to the President, who can agree or disagree with the committee, dean and VPAS. 5. The President then gives the final decision to the Dean of Clinics who will then notify the doctor whether he has been approved or denied. If the doctor is approved, he stays on the approved list as long as his license, malpractice insurance policy and CV are current. Intern Observations If interns are not eligible to go on a clerkship, interns may choose to go on observations with doctors of their choice for a total of up to 10 days. They may do so in their 10th trimester after all their clinical requirements to graduate are completed, turned in, and approved by the Clinic Services Manager. There is a form to fill out titled “Request for Independent Clinic Observation” which can be found on the inner web site: http://clinicalinfo.nuhs.edu, or can be obtained from Clinic Services Manager Jean Fairbank. A copy of the doctor’s license must be attached to the form. However, the deadline for completion of observation paperwork must be completed by the third Thursday prior to graduation. See Appendix Q. 93 94 Appendix 95 96 Appendix A CCE Standard H: Educational Requirements for Doctor of Chiropractic Program CCE Meta-Competencies & Guidelines (Appendix 1) (Effective 1/1/12) Manual of Policies of The Council on Chiropractic Education January 2011 The DCP is required to demonstrate that its students have achieved the mandatory meta-competencies and their required components and outcomes noted below. Within the constraints of the meta-competencies and evidence-informed assessment techniques, each DCP is free to determine its own method of metacompetency delivery and assessment. Ultimately, the DCP is accountable for the quality and quantity of its evidence of compliance with the meta-competencies and their required components and outcomes. A meta-competency assessment guide, Guidelines for DCP Assessment of Meta-Competencies, is attached to this policy. The guide is designed to provide insight into several options for documenting success in achieving the competency requirements. The guidelines are not meant to be all inclusive or prescriptive with respect to the evidence necessary to demonstrate compliance. CCE Clinical Education Meta-Competencies A graduate of a CCE accredited DCP is competent in the areas of: META-COMPETENCY 1 - ASSESSMENT & DIAGNOSIS An assessment and diagnosis requires developed clinical reasoning skills. Clinical reasoning consists of data gathering and interpretation, hypothesis generation and testing, and critical evaluation of diagnostic strategies. It is a dynamic process that occurs before, during, and after the collection of data through history, physical examination, imaging, and laboratory tests. REQUIRED COMPONENTS: A. Compiling a case-appropriate history that involves a process focused on patients’ health status, including a history of any present illness, systems review, and review of past, family and psychosocial histories for the purpose of directing clinical decision-making. B. Determining the need for and availability of external health records. C. Performing case-appropriate physical examinations that include evaluations of body regions and organ systems, including the spine and any subluxation/neuro-biomechanical dysfunction that assist the clinician in developing the clinical diagnosis(es). D. Utilizing diagnostic studies and consultation when appropriate, inclusive of imaging, clinical laboratory, and specialized testing procedures, to obtain objective clinical data. E. Formulating a diagnosis (es) supported by information gathered from the history, examination, and diagnostic studies. OUTCOMES: 1. Documentation of a list of differential diagnosis (es) and corresponding exams from a case-appropriate health history and review of external health records. 97 2. Determination and documentation of the significance of physical findings and thereby the need for follow-up through a physical examination, application of diagnostic and/or confirmatory tests and tools, and any consultations. 3. Generation of a problem list with diagnoses after synthesizing and correlating data from the history, physical exam, diagnostic tests, and any consultations. META-COMPETENCY 2 - MANAGEMENT PLAN Management involves the development, implementation and documentation of a patient care plan for positively impacting a patient’s health and well-being, including specific therapeutic goals and prognoses. It may include case follow-up, referral, and/or collaborative care. REQUIRED COMPONENTS: A. Establishing a management plan appropriate for the diagnosis and the patient’s health status, including specific therapeutic goals and prognoses. B. Determining the need for emergency care, referral and/or collaborative care. C. Providing information to patients of risks, benefits, natural history and alternatives to care regarding the proposed management plan. D. Obtaining informed consent. E. Determining the need for chiropractic adjustment and/or manipulation procedures, or other forms of passive care. F. Determining the need for active care. G. Determining the need for changes in patient behavior and activities of daily living. H. Monitoring patient progress and altering management plans accordingly. I. Recognizing the point of a patient’s maximum therapeutic benefit and release of the patient from corrective care, and communicating rationales for any ongoing care. J. Incorporating patient values and expectations of care in the management plan. OUTCOMES: 1. Formulation and documentation of an evidence-informed management plan appropriate to the diagnosis, inclusive of measureable therapeutic goals and prognoses in consideration of bio-psychosocial factors, natural history and alternatives to care. 2. Documentation of informing the patient of any need for emergency care, referral and/or collaborative care. 3. Documentation of informed consent. 4. Deliverance and documentation of appropriate chiropractic adjustments/manipulations, and/or other forms of passive care as identified in the management plan. 5. Deliverance and documentation of appropriate active care as identified in the management plan. 6. Documentation of patient counseling regarding recommended changes in the life style behaviors and activities of daily living. 7. Documentation of modifying the management plan as new clinical information becomes available. 98 8. Documentation of end points of care. META-COMPETENCY 3 - HEALTH PROMOTION AND DISEASE PREVENTION Health promotion and disease prevention requires an understanding and application of epidemiological principles regarding the nature and identification of health issues in diverse populations and recognizes the impact of biological, chemical, behavioral, structural, psychosocial and environmental factors on general health. REQUIRED COMPONENTS: A. Assessing the patient’s health and determining areas of potential health improvement (e.g. disease screening, ergonomics, nutrition, fitness, posture, smoking cessation, and risk factor reduction.) B. Addressing appropriate hygiene in a clinical environment. C. Coordinating health improvement strategies with other health care professionals. D. Identifying public health issues relevant to patients. OUTCOMES: 1. Documentation of management of health risks and public health issues, including reporting, as required. 2. Explanation of health risk factors, leading health indicators and public health issues to patients. 3. Provision of recommendations regarding patient’s health status, behavior and life style. 4. Recommendation or provision of resources (educational, community-based, etc.) and instruction designed to encourage a patient to pursue change. 5. Recommendation of dietary habits and/or nutritional approaches designed to restore, maintain or improve the patient’s health. 6. Implementation of appropriate hygiene practices in the clinical environment. 7. Communication of health improvement strategies with other treating health professionals. META-COMPETENCY 4 - COMMUNICATION AND RECORD KEEPING Effective communication includes oral, written and nonverbal skills with appropriate sensitivity, clarity and control for a wide range of healthcare related activities, to include patient care, professional communication, health education, and record keeping and reporting. REQUIRED COMPONENTS: A. Communicating effectively, accurately and appropriately, in writing and interpersonally with diverse audiences (e.g. patients, their relatives and others involved in their care; regulatory agencies, third party payers and employers; and doctors of chiropractic and other healthcare professionals). B. Acknowledging the existence and nature of different value systems of patients and others. C. Creating and maintaining accurate and legible records. D. Complying with regulatory ethical standards and responsibilities involving patient and business records. 99 OUTCOMES: 1. Provision of accurate and understandable explanations of health issues and management options considering the patient’s health care needs and goals. 2. Documentation of any health risks and management options considering the patient’s health care needs and goals. 3. Generation of patient records, narrative reports and correspondences that are accurate, concise and legible. 4. Evidence of safeguarding the patient’s protected health and financial information. META-COMPETENCY 5 - PROFESSIONAL ETHICS AND JURISPRUDENCE Professionals comply with the law and exhibit ethical behavior. REQUIRED COMPONENTS: A. Applying knowledge of ethical principles and boundaries. B. Applying knowledge of health care law. C. Applying knowledge of expected professional conduct. OUTCOMES: 1. Maintenance of appropriate physical communication (verbal and non-verbal) and emotional boundaries with patients. 2. Maintenance of professional conduct with patients, peers, staff, and faculty in accordance with established policies. 3. Compliance with the ethical and legal dimensions of clinical practice. 4. Generation of patient records and diagnostic and billing codes in compliance with federal and state law. META-COMPETENCY 6 - INFORMATION AND TECHNOLOGY LITERACY Information and technology literacy are manifested in an ability to locate, evaluate and integrate research and other types of evidence, including clinical experience, to explain and manage health-related issues and use emerging technologies appropriately. REQUIRED COMPONENTS: A. Demonstrating knowledge of relevant research methodologies and ability to critically appraise and apply the literature to clinical cases. B. Using health informatics to access information. OUTCOMES: 1. Critical appraisal of scientific literature and other information sources. 2. Incorporation of health care informatics into patient care. META-COMPETENCY 7 - INTELLECTUAL AND PROFESSIONAL DEVELOPMENT Intellectual and professional development is characterized by maturing values and skills in clinical practice; the seeking and application of new knowledge; and the ability to adapt to change. 100 REQUIRED COMPONENTS: A. Demonstrating knowledge of basic, social and clinical sciences sufficient to promote intellectual development and effective patient care. B. Reflecting on and addressing personal and professional learning issues. C. Providing evidence of critical thinking skills. OUTCOMES: 1. Satisfactory performance on licensing board exams and other assessments of student learning. 2. Use of appropriate self-evaluation and other feedback for personal and professional development. 3. Incorporation of critical thinking and clinical experience into patient care. CCE Guidelines Guideline for DCP Assessment of Learning of Meta-Competencies CCE Meta-Competencies are assessable learning outcomes to be measured at the student and program levels. The DCP utilizes a system of student assessment and evaluation that is based on the goals, objectives, competencies and learning outcomes established by the DCP, as well as the Meta-Competencies defined by the CCE Standards and appropriate to entry-level chiropractic practice. The system must clearly identify the level of performance expected of students in the achievement of these objectives, competencies, and outcomes. As a component of its assessment plan, the DCP develops and carries out program assessment activities to collect information about the attainment of Meta-Competencies and the other DCP competencies, which are desired student-learning outcomes. The assessment activities employ a variety of valid and reliable direct and indirect measures, systematically and sequentially throughout the professional degree program. At the program level, it is suggested that learning is assessed using a minimum of two direct measures and one indirect measure that reflect learning close to or at the end of the program. Assessment methods and tools are appropriate for the type of learning that is assessed. Direct measures include student products or performances that demonstrate that specific learning has taken place, including reports, exams, demonstrations, performances, and completed works. Indirect measures may imply that learning has taken place (e.g., student perceptions of learning), but do not specifically demonstrate that learning or skill. Such perceptions can come from many perspectives, including students, faculty, internship supervisors, alumni, transfer institutions, and employers. Because each method has its limitations, an ideal assessment program would combine direct and indirect measures from a variety of sources. Examples of direct measures of student learning relative to the knowledge component of taking a patient history include student performance on a course written exam and relevant NBCE sub scores on Patient History found in the Part II & III exams. Direct measures of student performance relative to taking a patient history include Objective Structured Clinical Exams (OSCEs), clinical Qualitative Evaluations (QE) and Part IV scores related to history taking. Examples of indirect measures of student learning relative to the knowledge and performance components of taking a patient history include student surveys of their perception of their knowledge and ability, employer surveys, and course evaluations. 101 Results obtained through assessment of student learning are made available to appropriate constituencies, including students themselves. The DCP uses the analysis of assessment measures to improve student learning and the achievement of the Meta-Competencies. Examples of Direct Measures of Learning of Meta-‐Competencies -‐ Performance scores on Standardized Tests (sub scores on NBCE exams related to specific meta-‐ competencies) -‐ Course written & Practical exams related to meta-‐ competencies -‐ Graded patient file audits -‐ Clinical OSCEs -‐ Direct observations in a clinical setting -‐ Case Studies -‐ Relevant internships/clinical experiences with evaluation -‐ Performance based projects w ith evaluation -‐ Graded presentations (individual or group) -‐ Portfolio evaluation -‐ Research and o ther published papers -‐Progressive disclosure case studies Examples of Indirect Measures of Learning of Meta-‐Competencies -‐ Student Satisfaction relative to their perception of their knowledge/ability regarding a given meta-‐ competency -‐ Global Rating Scales -‐ Preceptor surveys -‐ Classroom assessment techniques -‐ Clinical mentor evaluations CCE Guideline for Measuring Program Effectiveness Along with assessment of learning of Meta-Competencies, each DCP provides evidence of overall program effectiveness through a variety of valid and reliable measures that assess the impact of the curriculum and co-curriculum on learning. Measures include data with thresholds for success. Examples of measures are found in the table below. Results obtained through program assessment are made available to appropriate constituencies. The DCP uses the analysis of assessment measures for continuous improvement of its curriculum and cocurriculum. 102 Examples of Direct Measures of the DCP Examples of Indirect Measures of the DCP -‐ NBCE pass rates -‐ CCEB pass rates -‐ OSCE pass rates -‐ Student publication counts -‐ Evaluation of off-‐site clinical experiences -‐ Student portfolio evaluations -‐ External accreditation reviews -‐ Course pass rates -‐ Clinical qualitative evaluation scores -‐ Patient quality assurance data/analyses -‐ Progressive disclosure case studies Approved: 1/14/11 Revised: N/A -‐ Satisfaction (Student, Patient, Alumni, Employer) -‐ Preceptorship rates -‐ Title IV Loan default rates -‐ Graduating class GPA -‐ Graduate placement -‐ Licensure rates -‐ Enrollment percentage -‐ Diversity of student and staff populations -‐ Retention rates -‐ First year completion rates -‐ Graduation rates -‐ Transfer ratios -‐ Community services (clinical care) -‐ Community partnerships -‐ Extramural grants -‐ Faculty publications/presentations -‐ Student complaint percentage -‐ Articulation agreements w ith o ther colleges -‐ Faculty publication rates -‐ Faculty retention 103 104 Appendix B The NUHS College of Professional Studies Competencies NUHS Competency Domain Description of Performance Standard I. Medical Knowledge The competent graduate employs evidence informed practices, demonstrating good clinical care and developing medical expertise. II. Interpersonal and Communication Skills The competent graduate develops and assesses communication skills, developing an ability to work in health care teams. III. Patient Care The competent graduate fosters the ability to deliver patient-centered care, develops the doctor’s ability to teach, train, appraise, and assess, and develops collaborator skills. IV. Professionalism The competent graduate develops and assesses appropriate ethical relationships with patients, peers and subordinates, and develops and assesses the doctor’s ability to present themselves in a professional manner both in appearances and actions. V. Practice-Based Learning and Improvement The competent graduate develops the ability to apply quality improvement methods both through self and peer assessments. VI. Systems-Based Practice The competent graduate develops the ability to understand roles in current health care models (medical, home, multidisciplinary practice, hospital-based practice). 105 106 Appendix C Quantitative Requirements for Graduation Amount Skill or task Specific Criteria 350 Patient encounter (patient visit) 20 History 25 Examination 10 Gynecological Examination 10 20 Proctological Examination Hematology (i.e., CBC) – Interpretations on all 20 procedures and/or profiles performed 20 Chem/Micro/Immuno – Interpretations on all 20 procedures and/or profiles performed 25 Urinalysis (UA) – Interpretations on all 25 procedures performed 25 Venipuncture – 10 are required for graduation 30 Radiographic Studies 20 Diagnosis 250 CMT 75 Observed CMT 35 PT/Rehab 35 Evaluation & Management5 15 File Audits 20 Case Reports/Narratives 20 hours Clinic Community Outreach 20 hours University Service Credit 1350 hrs Minimum Practical Clinical Experience Mandatory Pink slips must be presented at graduation rehearsal. – Performed on 20 different patients – 80% must be on non-student patients1 – Performed on 20 different patients – 80% must be on non-student patients – 15 different case types2 – All 30 must be evaluated for the technical component (Diagnostic Imaging Dept.) – All 30 must be evaluated for the interpretive component (OAP note) – 15 different case types3 – Performed on 20 different patients – 80% must be on non-student patients each w/ defined case management plans – 15 different case types each w/ defined case management plans4 – 80% must be spinal adjustments provided during 250 separate encounters – 80% must be non-student patients of which 75 are assessed (see below) – Assessed through direct observation of non-student spinal adjustments – 20 cases must be live-patient cases6 – 80% must be non-student patients – 15 File Audits are required for graduation – 5 narratives required in Clinic Internship I – 10 narratives required in Clinic Internship II – 5 narratives required in Clinic Internship III – Must complete requirement while enrolled in Clinic Internship I and/or II – Clinician must be present for credit – Administered by the Office of the Dean of Clinics – See Appendices J & K – Must complete requirement prior to graduation – Administered by the Office of the Registrar – 350 hours, Clinic Internship I – 525 hours, Clinic Internship II – 525 hours, Clinic Internship III One week prior to Pink Slip Day, all graduating 10th Trimester students must check in with Clinic Services Manager Jean Fairbank to make sure all Quantitative Requirements for Graduation have been completed and received, and that all clinic accounts have been paid. Pink slips will be issued once are requirements have been met. See Footnotes on next page 107 Appendix C Footnotes: 1 A non-student patient is any patient that is not a student of the DC program and a student intern’s spouse, parents or children. 2 Which may be included among the 20 different patients, or in which the student may assist, observe, or participate in live, paper-based, computer-based, distance-learning, or other reasonable alternative. Case types = diagnostic entities (i.e., lumbar disc herniation, hypertension), patient presentations (i.e., woman with fatigue, patient over 50 w/ insidious low back pain, patient w/ radiating arm pain & nerve root deficits), and/or functional articular lesions (i.e., Maigne’s syndrome, upper cervical joint dysfunction causing cervicogenic headache). 3 Which may be included among the 30 radiographic studies, or in which the student may assist, observe, or participate in live, paper-based, computer-based, distance-learning, or other reasonable alternative. 4 Which may be included among the 20 different patients, or in which the student may assist, observe, or participate in live, paper-based, computer-based, distance-learning, or other reasonable alternative. 5 These cases, due to their complexity, require a higher order of clinical thinking and integration of data. This would include cases, which demand the application of imaging, lab procedures or other ancillary studies in determining a course of care, or cases in which multiple conditions, risk factors, or psychosocial factors have to be considered. 6 In the remaining cases, the student may assist, observe, or participate in live, paper-based, computer-based, distance-learning, or other reasonable alternative. 108 Appendix D Clinic Internship I Syllabus COURSE TITLE: Clinic Internship I TIME REQUIREMENT: (hrs/week) COURSE NUMBER: IC700 Course Credits: 11 Laboratory: 18 hours x 15 weeks & 30 hours x 2 weeks Total Clock Hours: 330 PREREQUISITES: Completion of Phase I; Current CPR Certification; EC6303; FR6307; RA6302 COREQUISITES: EM6403, RA6409, RA6408 COMPETENCIES GUIDING THE COURSE: 1. Medical Knowledge 2. Interpersonal and Communication Skills 3. Patient Care 4. Professionalism 5. Practice-based Learning and Improvement 6. Systems-based Practice Given the particular needs of assessment within the clinical setting, some of these core competences are evaluated in a targeted manner during the course of patient encounters. Below are listed the various areas where the Clinic Internship I student must show an appropriate introductory level of mastery before being allowed to work without a senior intern mentor. These are further described in Intern Manual Appendix A - CCE Standard H: Educational Requirements for Doctor of Chiropractic Program META-COMPETENCY 1 - ASSESSMENT & DIAGNOSIS An assessment and diagnosis requires developed clinical reasoning skills. Clinical reasoning consists of data gathering and interpretation, hypothesis generation and testing, and critical evaluation of diagnostic strategies. It is a dynamic process that occurs before, during, and after the collection of data through history, physical examination, imaging, and laboratory tests. META-COMPETENCY 2 - MANAGEMENT PLAN Management involves the development, implementation and documentation of a patient care plan for positively impacting a patient’s health and well-being, including specific therapeutic goals and prognoses. It may include case follow-up, referral, and/or collaborative care. META-COMPETENCY 3 - HEALTH PROMOTION AND DISEASE PREVENTION Health promotion and disease prevention requires an understanding and application of epidemiological principles regarding the nature and identification of health issues in diverse populations and recognizes the impact of biological, chemical, behavioral, structural, psychosocial and environmental factors on general health. META-COMPETENCY 4 - COMMUNICATION AND RECORD KEEPING Effective communication includes oral, written and nonverbal skills with appropriate sensitivity, clarity and control for a wide range of healthcare related activities, to include patient care, professional communication, health education, and record keeping and reporting. META-COMPETENCY 5 - PROFESSIONAL ETHICS AND JURISPRUDENCE Professionals comply with the law and exhibit ethical behavior. 109 META-COMPETENCY 6 - INFORMATION AND TECHNOLOGY LITERACY Information and technology literacy are manifested in an ability to locate, evaluate and integrate research and other types of evidence, including clinical experience, to explain and manage health-related issues and use emerging technologies appropriately. META-COMPETENCY 7 - INTELLECTUAL AND PROFESSIONAL DEVELOPMENT Intellectual and professional development is characterized by maturing values and skills in clinical practice, the seeking and application of new knowledge, and the ability to adapt to change. GENERAL COURSE DESCRIPTION: IC7000 Clinic Internship I - Credits 11:Clinic Internship I, although designated as a laboratory in a curricular sense, marks the advent of the student's practical application of the basic and clinical sciences in a clinical setting. Students will receive close supervision, guidance and instruction in the delivery of health care by licensed clinical personnel as well as mentoring by senior interns. Students participating in clinical experiences are expected to exhibit clinical competence and professionalism (including knowledge of and strict adherence to confidentiality and privacy policies). Clinic Internship I operations will closely mirror the experiences of Clinic Internship II and III, including but not limited to clinic forms, diagnostic and therapeutic procedures. In each clinical experience (I, II, III), responsibilities are granted interns based upon the clinician’s assessment that patient care competencies have been mastered. Clinical competencies relating to the skills of historical interviewing, medical record documentation, physical examination (general, regional and specialty), laboratory testing (selection, performance and interpretation), evidence-based therapeutics, differential diagnoses development, ethics, professionalism, and interpersonal communication will be assessed (Competencies 1-7). Prerequisites: Completion of Phase I, Current CPR Certification; EC6303; FR6307; RA6302 Corequisites: EM6403, RA6408, RA6409 COURSE OBJECTIVES: Upon completion of the course the student will be able to: 1. Assess the completeness of the initial patient intake information. 2. Interview patients to discover the parameters of their presentation and any other contributing factors. 3. Select the appropriate examination procedures that would result in robust data concerning the patient’s presentation. 4. Record history and examination findings utilizing the proper forms in the patient’s file. 5. Determine the working diagnosis as a result of the subjective and objective findings. 6. Design a treatment plan that is within the best practices as supported by current research. 7. Apply the procedures as outlined in the patient’s treatment plan. 8. Monitor the patient’s progress as they receive treatments according to the set treatment plan. 9. Detect inappropriate reactions to the set treatment protocols. 10. Revise the treatment plan for further care based upon the patient’s progress and know when to discharge a patient from care. INSTRUCTIONAL MATERIALS: Required Texts: All previously utilized texts required for the previous clinical sciences courses will be considered required and will be referred to on a regular basis in the course of patient evaluation and management. Recommended/Supplemental Texts: Muscles: Testing and Function, with Posture and Pain By Florence Peterson Kendall (Editor), Elizabeth Kendall McCreary (Author), Patricia Geise Provance, Mary McIntyre Rodgers, William Anthony Romani Publisher: Lippincott Williams & Wilkins; Fifth Edition (February 1, 2005) ISBN-10: 0781747805 110 Myofascial Pain and Dysfunction: The Trigger Point Manual; Vol. 1. The Upper Half of Body by Janet G. Travel & Lois S. Simons Publisher: Lippincott Williams & Wilkins; 2nd edition (November 1, 1998) # ISBN-10: 0683083635 Myofascial Pain and Dysfunction: The Trigger Point Manual; Vol. 2; The Lower Extremities ISBN-10: 0683083678 Other Required/Recommended Instructional Materials: In addition, the kit of diagnostic equipment given to students at the beginning of their career at National University of Health Sciences should be with them every day. If they are found to be without these essential tools, they will receive an unexcused absence for each day they are present without this gear. Orientation During the first week of classes, Clinic Internship I interns will not be seeing patients in clinic. This period is given over to ensuring that a set of basic practical skills and/or administrative functions has been covered. Be it appropriate forms, procedures or constructs for understanding the “flow” of a patient within the clinic or the ordering of radiographic images or laboratory studies, exposure prior to undertaking patient care lays the foundation for effective care and the efficient use of time. During this week, the normal clinic dress code is suspended. Self-Study It has been the experience of successful doctors that nearly every patient encounter triggers some degree of additional study, especially early in their careers. This course is patient case driven, and self-directed study outside of the clinic is expected. The cases will originate from the patients that interns treat within the clinic and those which are presented during the regular case discussions. EVALUATION OF STUDENT’S ACHIEVEMENT: Compared to the rest of a student’s career at National, entrance into the clinic system, starting with Clinic Internship I marks a definitive change. Students are now responsible for the health and well being of the patients under their care. This is a simple but profound statement, underlying the added charge being laid upon the student. With this in mind, the bar is set higher for passing in this setting. Grading Procedure: Course grade is Pass/Fail (70%). Assessment will be based on: • Evaluations generated for intern performance while in the clinic will be performed by the clinicians using ECQES (40% of the grade). The interns will need to be assessed by the staff clinicians in the following categories with different patients. It will be the student’s responsibility to seek out a clinician to observe their activities in the following categories: o Manipulative Therapy (the adjustment) – from a minimum of 5 patient contacts o RIME – 5 assessments • Written entrance examinations covering material presented during Orientation Week (Week 1) and the Intern Manual. The breakdown of this grading is as follows: A brief written exam will be given in Week 1 of the trimester. A re-exam will be offered again that week. This written exam will serve as an “entrance exam” and the intern must successfully pass with 70% in order to be allowed to partake in patient care in Clinic Internship I. • 50% of the grade in this course will be determined by participation. This will be measured, but not limited to, the number of patients seen, active involvement in case round table discussions, and seminars. Another perimeter of participation will depend upon how readily interns bring a clinician for observation at key points during the course of patient care, especially as measured against the class as a whole. In addition, there are a myriad of ways in which an intern can participate in the daily educational life of the clinic to their and other team members’ betterment, and determination of this involvement is not limited to the few examples noted above. Determination of participation is at the discretion of the faculty running the twiceweekly case discussions or observing an intern’s activities within this course in any clinic setting. Finally, a determination of participation remains under the discretion of the department chair. 111 • • • Interns will be expected to successfully complete the following: o Filing of lab results to include at least one each o CBC o UA o Comprehensive Metabolic profile Individual assignments may be given by a duty clinician or by the department chair if in their judgment such activity would be educational in nature. 10% of an intern’s grade is determined through assessment of the degree of professionalism, interpersonal skills, ability to work under any of the clinicians assigned to oversee operations and instruction. Attitudinal attributes such as enthusiasm, cooperativeness and efficiency all play a role in this determination. Factors such as timeliness for shift, preparedness for the patient encounter, interactions with staff, interns and clinicians are considered and are those interactions appropriate and commensurate with an intern’s status in the clinic? Clinicians will be also looking for to what degree the intern displays independence? Are they needy, complainers, or are they problem solvers and self-starters? Failure to complete these requirements, attendance policy, intern conduct, as well as performance of Duty Intern duties will be reflected on clinic evaluation forms. Grading Course grade is on a Pass/Fail basis. 70% is considered passing. The College of Professional Studies’ policy regarding final examinations, as published in the most recent National University of Health Sciences Bulletin, will be followed. Missed Assessment(s): o Missed entrance examination may be made up if the Chair of Clinical Practice has granted an excused absence. o The make-up examination must be made up within two weeks of the missed entrance examination unless the Chair of Clinical Practice grants some special accommodation. Students will not be allowed to engage in clinic activities until the examination is passed. o Interns may be failed for lack of academic progress in the course, including failure to complete the entrance examination in a timely manner, failure to engage in patient care, as well as failure to successfully demonstrate competence in that care, and for other reasons outlined in the Intern Manual and other University documents. o Standard Process Field Trip to Palmyra, Wisconsin, is mandatory for the Illinois DC and ND students. Every student is expected to attend this field trip with his class during his time in 8th trimester. Failure to attend the field trip will require the student to make up the field trip with the next incoming 8th trimester class. Review of Grades and Assessments: As noted above, information concerning assessment will be collected through the use of ECQES. This data will be reviewed and sent out as individual emails biweekly to each intern in the program. All other grades from quizzes, midterms and the like will be posted on CygNET and/or available as an individual email sent to the intern’s current account. Each student has 10 calendar days from the date that a test or course grade is made available to review the grade. Failure to discuss the grade or make an appointment to discuss the grade within that allotted time frame will result in forfeiture of the right to question the grade. Questions regarding the course should be directed to Manuel Duarte, DC, chair of clinical practice. If the grades and assessments are below the passing grade but the intern has shown substantial participation in clinic activities, it will be up to the discretion of the Chair of Clinical Practice to determine if the intern will receive an incomplete versus a failure. If circumstances do come to this point, an exit exam may be administered. The intern will be allowed one month from the last day of finals for the course to take this special exam. Prior to the commencement of this one-month period, the intern will be required to outline a course of remediation, which will be discussed and approved by the Chair. 112 The special examination to be administered will be generated by a committee composed of the Chair, the intern’s clinician and another clinician. This same committee will also grade the finished exam separately, and then compare their scores for the exam to ensure consistency. If there is a serious difference in the scoring of any given exam question, the Dean of Clinics will provide the necessary determination for the final reconciled scoring. During the period of this remediation and study the intern may attend their assigned outpatient clinic, but not participate in patient care. If the intern successfully passes the special exit exam, all restrictions will be removed from their activities in the outpatient setting. Failure to pass at 70% or above will ensure that the intern will repeat Clinic Internship I. Mentoring: It is the natural and customary manner of such a clinical laboratory course that mentoring will be part of the daily activities. Each member of the clinical staff will be available for consultation concerning the care of the student patients and their family members under the interns’ care. TEACHING METHODS AND ACTIVITIES: Teaching methods within this clinician setting consist of oversight of patient care from the moment that the history is obtained, guiding of which exams might be applicable, and development of the diagnosis and treatment plan through to overseeing the actual care. In other words, a one-on-one encounter with the staff clinicians serving a given shift is the principle method of instruction. There are opportunities for mentoring and small group tutorials, especially pertaining to material presented in the case discussions, workshops and seminars connected with this class. COURSE OUTLINE (May be subject to change): Course Outline: Will be given out during the first week of class (Orientation) LABORATORY ATTIRE AND REQUIREMENTS: The interns are expected to not only show up early for their shifts but also be properly attired for a clinical environment. The details of what constitutes proper attire are clearly spelled out in the Intern Manual. It will be up to the discretion of the duty clinician or Chair of Clinical Practice to make any judgment call in this realm. An intern may be asked to leave the shift over this issue. The missed shift will be need to be made up within two weeks or will count as an unexcused absence, which would need to be made up at a two-for-one ratio. Repeat offenses in this area will be handled by the campus disciplinary committee. PROFESSIONAL RESPONSIBILITY: The College of Professional Studies' policy on code of conduct, as published in the most recent National University of Health Sciences Student Handbook, will be followed. ATTENDANCE POLICY: Clinic attendance: If an intern knows in advance that they will miss a clinic assignment, 3 days notice should be given to their clinician. Two excused absences are allowed during Clinic Internship I without being made up. Beyond that, excused absence make-up shifts will be done on a one-to-one basis and should be scheduled and completed within two weeks and upon approval of the make-up date by the department chair or a clinician. If illness or an unforeseen event prevents attendance, interns should contact the clinic directly or by voice mail (630-889-6525) PRIOR to their shift, or email their clinician and copy Dr. Duarte at: [email protected]. Non-reported missed shifts (or other unexcused absences) will be made up on a two-for-one basis. Scheduled make-ups must be scheduled with at least 24 hours notice prior to presenting to the clinic. A maximum of two absences is allowed per trimester. Excess absences must be approved by the Chair of Clinical Practice. There is no “banking” of absences in anticipation of time missed from clinic without prior approval from the Chair of Clinical Practice. Attendance at professional seminars does not constitute time spent in clinic nor an excused absence. Travel time to and from a seminar or for National Boards is also considered an absence from the total of three “release days” an intern is allowed. 113 An intern must be in the clinic and prepared for shift on time. If an intern is going to be late, they must contact their clinician and inform them of the lateness. An intern who arrives 15 minutes late without notifying their clinician will make up the shift on a two-to-one basis. If arriving less than 15 minutes late three times, the intern will be required to make up the shift. DISABILITY SUPPORT SERVICES: Please refer to the most recently published National University of Health Sciences Student Handbook for further information regarding disability disclosure and support services. SYLLABUS INFORMATION: Syllabus prepared by: Manuel Duarte, DC Date: 31 December 2012 Modified 11 June, 2014, Drs. Duarte, Cohen Curriculum Committee Approval Date: NUHS President Approval Date: Proposed changes to the course title and identification number, time requirement, prerequisites, general course description, competencies, and objectives as described at the beginning of the syllabus, must be presented to the appropriate department chair. The department chair, in conjunction with the assistant dean(s), may submit the proposed changes to National University of Health Sciences Curriculum Committee. If approved, the curriculum committee will submit the proposed changes to the president of National University of Health Sciences. 114 Appendix E Clinic Internship II Syllabus COURSE TITLE: Clinic Internship II TIME REQUIREMENT: (hrs/week) COURSE NUMBER: IC7100 Lecture: 0 Laboratory: 525 Total Clock Hours: 525 Course Credits: 17 PREREQUISITES: Successful completion of IC7000; American Heart Association BLS for Health Care Professionals with AED CPR certification COMPETENCIES GUIDING THE COURSE: 1. Medical Knowledge 2. Interpersonal and Communication Skills 3. Patient Care 4. Professionalism 5. Practice-based Learning and Improvement 6. Systems-based Practice Given the particular needs of assessment within the clinical setting, some of these core competences are evaluated in a targeted manner during the course of patient encounters. Below are listed the various areas where the Clinic Internship I student must show an appropriate introductory level of mastery before being allowed to work without a senior intern mentor. These are further described in Intern Manual Appendix A - CCE Standard H: Educational Requirements for Doctor of Chiropractic Program META-COMPETENCY 1 - ASSESSMENT & DIAGNOSIS An assessment and diagnosis requires developed clinical reasoning skills. Clinical reasoning consists of data gathering and interpretation, hypothesis generation and testing, and critical evaluation of diagnostic strategies. It is a dynamic process that occurs before, during, and after the collection of data through history, physical examination, imaging, and laboratory tests. META-COMPETENCY 2 - MANAGEMENT PLAN Management involves the development, implementation and documentation of a patient care plan for positively impacting a patient’s health and well-being, including specific therapeutic goals and prognoses. It may include case follow-up, referral, and/or collaborative care. META-COMPETENCY 3 - HEALTH PROMOTION AND DISEASE PREVENTION Health promotion and disease prevention requires an understanding and application of epidemiological principles regarding the nature and identification of health issues in diverse populations and recognizes the impact of biological, chemical, behavioral, structural, psychosocial and environmental factors on general health. META-COMPETENCY 4 - COMMUNICATION AND RECORD KEEPING Effective communication includes oral, written and nonverbal skills with appropriate sensitivity, clarity and control for a wide range of healthcare related activities, to include patient care, professional communication, health education, and record keeping and reporting. META-COMPETENCY 5 - PROFESSIONAL ETHICS AND JURISPRUDENCE Professionals comply with the law and exhibit ethical behavior. 115 META-COMPETENCY 6 - INFORMATION AND TECHNOLOGY LITERACY Information and technology literacy are manifested in an ability to locate, evaluate and integrate research and other types of evidence, including clinical experience, to explain and manage health-related issues and use emerging technologies appropriately. META-COMPETENCY 7 - INTELLECTUAL AND PROFESSIONAL DEVELOPMENT Intellectual and professional development is characterized by maturing values and skills in clinical practice, the seeking and application of new knowledge, and the ability to adapt to change. GENERAL COURSE DESCRIPTION: Students will further develop skills needed for successful management of patients and their conditions. Students will participate in off-campus rotations to expand their experience and knowledge base. All students will be evaluated for skill development, adjustive technique and case management. Students must provide a written case narrative on at least 10 cases that they have managed or co-managed in the clinics. Students will participate in Quality Assurance activities to ensure that the patient chart is in compliance with the University’s Quality Assurance program. Inservice training will be given in personnel issues for the practice, OSHA compliance issues for the private practice office, provisional credentialing of the chiropractic intern, and Medicare issues for the private practice. COURSE OBJECTIVES: 1. Demonstrate the basic to intermediate skills of patient care to the clinician on staff for your shift or clinic. These skills are outlined in the course objectives in DC7043L. 2. Interact professionally with the clinician and upper trimester interns, focusing on primary care. 3. Design rehabilitation programs for a variety of physical ailments focusing on musculoskeletal conditions. 4. Have an increasing awareness of business procedures used in a successful practice. 5. Competently write referral letters, narrative reports, and requests to other health care professionals and businesses related to the health care field. 6. Construct defensible replies to insurance denials utilizing EBP articles. 7. Generate 5 new patients to the clinic before graduation. INSTRUCTOR INFORMATION AND OFFICE HOURS: Regardless of the location of the clinic, Outpatient Clinical Internship is overseen by Manuel Duarte, DC, chair of clinical practice. His office is located off the main clinic hallway overlooking the back outdoor courtyard, Room 311. Aside from when he has clinic shifts, generally he can be found in this office from 9:00 AM to 5:00 PM. The extension for this office is 6525, although the best way to reach him is by email: [email protected]. It is strongly suggested that if you wish to meet with him you make an appointment by email at least a week prior. INSTRUCTIONAL MATERIALS: Required Texts: All previously utilized texts required for the previous clinical sciences courses will be considered required and will be referred to on a regular basis. Recommended/Supplemental Texts: There are no recommended or supplemental texts. Other Required/Recommended Instructional Materials: In addition, the kit of diagnostic equipment given to students at the beginning of their career at National University of Health Sciences should be with them every day. If they are found to be without these essential tools, they will receive an unexcused absence for each day they are present without this gear. EVALUATION OF STUDENT’S ACHIEVEMENT: Compared to the rest of a student’s career at National, entrance into the clinic system, starting with Clinic Internship I, marks a definitive change. Students are now responsible for the health and well-being of the patients under their care. This is a simple but profound statement, underlying the added charge being laid upon the student. With this in mind, the bar is set higher for passing in this setting. 116 Grading Procedure: Course grade is Pass/Fail (70%). Assessment will be based on: • Evaluations generated for intern performance while in the clinic will be performed by the clinicians using ECQES or a web browser based assessment tool (60% of the grade). The interns will need to be assessed by the staff clinicians in the following categories over at least four different patients. It will be the student’s responsibility to seek out a clinician to observe their activities in the following categories: o History Taking – from 20 assessments o Physical Exam Procedures – from 20 assessments o Diagnosis – from 20 assessments o Case Management – from 20 assessments o Patient Education – from 20 assessments o Manipulative Therapy (the adjustment) – from a minimum of 80 patient contacts o RIME – 20 assessments (between 9th and 10th trimesters) Special note: Interns must show a passing grade (70%) for each section noted above. If an intern falls below 70%, they will be given an opportunity for remediation in the topic in question. Interns will be allowed two extra clinician observed assessments to attempt to bring their grade up to a passing level. If an intern shows a score below 70% in two or more categories, even after attempted remediation, they will be required to repeat the course. In addition the intern may be asked to complete assignments for further educational need, as deemed necessary by clinician. • 20% of an intern’s grade is determined through assessment of the degree of professionalism, interpersonal skills, ability to work under any of the clinicians assigned to oversee operations and instruction. Attitudinal attributes such as enthusiasm, cooperativeness and efficiency all play a role in this determination. Factors such as timeliness for shift, preparedness for the patient encounter, interactions with staff, interns and clinicians are considered, and are those interactions appropriate and commensurate with an intern’s status in the clinic? Clinicians will be also looking for to what degree the intern displays independence? Are they needy, complainers, or are they problem solvers and self-starters? • Given the unique nature of clinic, participation is critical to the learning process; therefore this aspect of the clinical experience is given a high priority. 20% of the grade in this course will be determined by participation. This will be measured, but not limited to, the number of patients seen, active involvement in case discussions. Another perimeter of participation will depend upon how readily interns bring a clinician for observation at key points during the course of patient care, especially as measured against the class as a whole. In addition, there are a myriad of ways in which an intern can participate in the daily educational life of the clinic to their and other team members’ betterment, and determination of this involvement is not limited to the few examples noted above. Determination of participation is at the discretion of the clinician. Finally, a determination of participation remains under the discretion of the department chair. Failure to complete these requirements, attendance policy, intern conduct, as well as performance of DI duties may be reflected on clinic evaluation forms. Grading As noted above, course grade is on a Pass/Fail basis. 70% is considered passing. Special Note: Given that trimesters 8 through 10 make up the direct patient care clinical experience, there is a defined set of requirements for graduation that need to be completed over the course of these trimesters. These requirements are spelled out in detail in Appendix C of this document. The College of Professional Studies’ policy regarding final examinations, as published in the most recent National University of Health Sciences Bulletin, will be followed. Missed Assessment(s): o Missed final examinations may be made up if an excused absence has been granted by the appropriate dean. o The make-up examination will be scheduled by the faculty member within two weeks of the missed final 117 examination but never later than the first day of class of the following trimester. o If examinees are not present at the scheduled make-up exam time, they will receive the grade of F for the course or lab unless the grade of I is reissued. Enrollment in any new courses will not be continued if students have not converted the grade of I to a regular passing grade by the first calendar day of the second calendar week of the next trimester of attendance. The removal of the I must be accomplished within the maximum of one calendar year. Otherwise, the I becomes an F automatically. The College of Professional Studies’ policy regarding make-up final examinations, as published in the most recent National University of Health Sciences Bulletin, will be followed. Review of Grades and Assessments: As noted above, information concerning assessment will be collected through the use of ECQES or an Internet browser based database system and updated by the clinician(s). This data will be reviewed and sent out as individual emails biweekly to each intern in the program. Each student has 10 calendar days from the date that a test or course grade is made available to review the grade. Failure to discuss the grade or make an appointment to discuss the grade within that allotted time frame will result in forfeiture of the right to question the grade. Questions regarding the course should be directed to Manuel Duarte, DC, chair of clinical practice. Mentoring: It is the natural and customary manner of such a clinical laboratory course that mentoring will be part of the daily activities. Each member of the clinical staff will be available for consultation concerning the care of the student patients and their family members under the interns care. TEACHING METHODS AND ACTIVITIES: Teaching methods within this clinician setting consist of oversight of patient care from the moment that the history is obtained, guiding of which exams might be applicable, and development of the diagnosis and treatment plan through to overseeing the actual care. In other words, one-on-one encounters with the staff clinicians serving a given shift are the principle method of instruction. There are opportunities for mentoring and small group tutorials, especially pertaining to material presented in the seminars connected with this class. ADDITIONAL COURSE CONTENT: There is no additional course content. LABORATORY ATTIRE AND REQUIREMENTS: The interns are expected to not only show up early for their shifts but also be properly attired for a clinical environment. The details of what constitutes proper attire is clearly spelled out in the Clinic Intern Manual. It will be up to the discretion of the duty clinician to make any judgment call in this realm. Repeat offenses in this area will be handled by the campus disciplinary committee. PROFESSIONAL RESPONSIBILITY: The College of Professional Studies’ policy on code of conduct, as published in the most recent National University of Health Science Student Handbook, will be followed. ATTENDANCE POLICY: Attendance at in-services or seminars is mandatory. Roll is taken by the clinician to whom the intern has been assigned, with the window for not receiving a tardy closed out 10 minutes after the clinic shift starts. Two tardies will constitute an absence. If the intern has a patient scheduled and they are not there prior to the patient’s arrival, they will receive a tardy and no credit for their activities in the clinic that shift. If the intern totally misses the appointment through non-attendance and the case must be passed to another intern, this is not only an absence but they will be suspended from receiving credit for patient care for a week. Clinic attendance: If an intern knows in advance that they will miss a clinic assignment, 3 days notice should be given to their clinician. Make-up shifts will be done on a one-to-one basis and should be scheduled within a week. If illness or an unforeseen event prevents attendance, interns should contact their clinician directly or by voice mail 118 PRIOR to their shift. Non-reported missed shifts will be made up on a two-for-one basis. Scheduled make-ups must be scheduled with at least 24 hours notice prior to presenting to the clinic. A maximum of three absences is allowed per trimester. Excess absences must be approved by the Chair of Clinical Practice and will be made in consultation by the clinician overseeing the intern. If deemed appropriate, absences in excess of the three allowed will be made up shift-for-shift at a two-to-one ratio after notification of completion (“pink slips”) of requirements for graduation have been given out at the end of Trimester 10. Release of an intern’s diploma will be held back until these shifts have been completed. There is no “banking” of absences in anticipation of time missed from clinic without prior approval from the chair of clinical practice. Interns are expected to show up early for their shifts for patients will be present from the moment the shift starts. An intern must be in the clinic and prepared for their shift on time. If an intern is going to be late, they must contact their clinician and inform them of the lateness. An intern who arrives 20 minutes late without notifying their clinician will make up the shift on a two-for-one basis. If arriving less than 20 minutes late three times, the intern will be required to make up the shift. Attendance at off-campus professional seminars does not constitute time spent in clinic nor an excused absence. Travel time to and from a seminar or the National Boards also falls into the same category. DISABILITY SUPPORT SERVICES: Please refer to the most recently published National University of Health Sciences Student Handbook for further information regarding disability disclosure and support services. SYLLABUS INFORMATION: Syllabus prepared by: Manuel Duarte, DC Date: 31 December 2012 Curriculum Committee Approval Date: NUHS President Approval Date: Proposed changes to the course title and identification number, time requirement, prerequisites, general course description, competencies, and objectives as described at the beginning of the syllabus, must be presented to the appropriate department chair. The department chair, in conjunction with the assistant dean(s), may submit the proposed changes to National University of Health Sciences’ Curriculum Committee. If approved, the curriculum committee will submit the proposed changes to the president of National University of Health Sciences. 119 120 Appendix F Clinic Internship III Syllabus COURSE TITLE: Clinic Internship III TIME REQUIREMENT: (hrs/week) COURSE NUMBER: IC7200 Lecture: 0 Laboratory: 525 Total Clock Hours: 525 Course Credits: 17 PREREQUISITES: Successful completion of IC7100, American Heart Association BLS for Health Care Professionals with AED CPR certification. COMPETENCIES GUIDING THE COURSE: 1. Medical Knowledge 2. Interpersonal and Communication Skills 3. Patient Care 4. Professionalism 5. Practice-based Learning and Improvement 6. Systems-based Practice Given the particular needs of assessment within the clinical setting, some of these core competences are evaluated in a targeted manner during the course of patient encounters. Below are listed the various areas where the Clinic Internship I student must show an appropriate introductory level of mastery before being allowed to work without a senior intern mentor. These are further described in Intern Manual Appendix A - CCE Standard H: Educational Requirements for Doctor of Chiropractic Program META-COMPETENCY 1 - ASSESSMENT & DIAGNOSIS An assessment and diagnosis requires developed clinical reasoning skills. Clinical reasoning consists of data gathering and interpretation, hypothesis generation and testing, and critical evaluation of diagnostic strategies. It is a dynamic process that occurs before, during, and after the collection of data through history, physical examination, imaging, and laboratory tests. META-COMPETENCY 2 - MANAGEMENT PLAN Management involves the development, implementation and documentation of a patient care plan for positively impacting a patient’s health and well-being, including specific therapeutic goals and prognoses. It may include case follow-up, referral, and/or collaborative care. META-COMPETENCY 3 - HEALTH PROMOTION AND DISEASE PREVENTION Health promotion and disease prevention requires an understanding and application of epidemiological principles regarding the nature and identification of health issues in diverse populations and recognizes the impact of biological, chemical, behavioral, structural, psychosocial and environmental factors on general health. META-COMPETENCY 4 - COMMUNICATION AND RECORD KEEPING Effective communication includes oral, written and nonverbal skills with appropriate sensitivity, clarity and control for a wide range of healthcare related activities, to include patient care, professional communication, health education, and record keeping and reporting. META-COMPETENCY 5 - PROFESSIONAL ETHICS AND JURISPRUDENCE Professionals comply with the law and exhibit ethical behavior. 121 META-COMPETENCY 6 - INFORMATION AND TECHNOLOGY LITERACY Information and technology literacy are manifested in an ability to locate, evaluate and integrate research and other types of evidence, including clinical experience, to explain and manage health-related issues and use emerging technologies appropriately. META-COMPETENCY 7 - INTELLECTUAL AND PROFESSIONAL DEVELOPMENT Intellectual and professional development is characterized by maturing values and skills in clinical practice, the seeking and application of new knowledge, and the ability to adapt to change. GENERAL COURSE DESCRIPTION: Students enter the senior intern phase of training when skill development and evaluation continues until graduation. Students will participate in the development of junior interns and begin advanced technique electives. Students will explore off-campus observations and assignments to expand their knowledge base and obtain exposure to private practice via mentoring with a licensed field doctor. In-service training will consist of advanced diagnostic procedures such as EMG, MRI, ultrasonography, etc. There will be a continuation of rehabilitation training and advanced treatment techniques to help refine the skill levels of the intern prior to graduation. Business office rotations and insurance submission experience is offered. COURSE OBJECTIVES: At the end of this course the student will be able to: 1. Demonstrate the basic skills of patient care to a junior intern. These skills are outlined in the course objectives in DC7043L. 2. Interact professionally with chiropractic field doctors as well as other specialties focusing on primary care. 3. Design comprehensive rehabilitation programs for a variety of physical ailments focusing on musculoskeletal conditions. 4. Assess the appropriateness of business procedures in a successful practice. 5. Complete third party payment criteria for a spectrum of primary care conditions. 6. Competently write referral letters, narrative reports, and requests to other health care professionals and businesses related to the health care field. 7. Construct defensible replies to insurance denials utilizing EBP articles. 8. Each intern is required to generate 5 new patients to the clinic before graduation. INSTRUCTOR INFORMATION AND OFFICE HOURS: Instruction and mentoring is provided to the intern by the clinician who is on staff or covering the clinic on a given day or shift. Their office hours generally will be the hours that the clinic is open. Regardless of the location of the clinic, Outpatient Clinical Internship is overseen by Manuel Duarte, DC, chair of clinical practice. His office is located off the main clinic hallway overlooking the back outdoor courtyard, Room 311. Aside from when he has clinic shifts, generally he can be found in this office from 9:00 a.m. to 5:00 p.m. The extension for this office is 6525, although the best way to reach him is by email: [email protected]. It is strongly suggested that if you wish to meet with him you make an appointment by email at least a week prior. INSTRUCTIONAL MATERIALS: Required Texts: All previously utilized texts required for the previous clinical sciences courses will be considered required and will be referred to on a regular basis Recommended/Supplemental Texts: There are no recommended or supplemental texts. Other Required/Recommended Instructional Materials: In addition, the kit of diagnostic equipment given to students at the beginning of their career at National University of Health Sciences should be with them every day. If they are found to be without these essential tools, they will receive an unexcused absence for each day they are present without this gear. 122 EVALUATION OF STUDENT'S ACHIEVEMENT: Compared to the rest of a student’s career at National, entrance into the clinic system, starting with Clinic Internship I, marks a definitive change. Students are now responsible for the health and well-being of the patients under their care. This is a simple but profound statement, underlying the added charge being laid upon the student. With this in mind, the bar is set higher for passing in this setting. Grading Procedure: Course grade is Pass/Fail (70%). Assessment will be based on: • Evaluations generated for intern performance while in the clinic will be performed by the clinicians using ECQES or a web browser based assessment tool. (60% of the grade). The interns will need to be assessed by the staff clinicians in the following categories over at least four different patients. It will be your responsibility to seek out a clinician to observe your activities in the following categories: o History Taking – from 20 assessments Physical Exam Procedures – from 20 assessments o Diagnosis – from 20 assessments o Case Management – from 20 assessments o Patient Education – from 20 assessments o Manipulative Therapy (the adjustment) – from a minimum of 80 patient contacts o RIME – 20 assessments (between 9th and 10th trimesters) Special note: You must show a passing grade (70%) for each section noted above. If you fall below 70% you will be given an opportunity for remediation in the topic in question. You will be allowed two extra clinician observed assessments to attempt to bring your grade up to a passing level. If the intern shows a score below 70% in two or more categories, even after attempted remediation, they will be required to repeat the course. In addition the intern may be asked to complete assignments for further educational need, as deemed necessary by the clinician. • 20% of an intern’s grade is determined through assessment of the degree of professionalism, interpersonal skills, ability to work under any of the clinicians assigned to oversee operations and instruction. Attitudinal attributes such as enthusiasm, cooperativeness and efficiency all play a role in this determination. Factors such as timeliness for shift, preparedness for the patient encounter, interactions with staff, interns and clinicians are considered, and are those interactions appropriate and commensurate with an intern’s status in the clinic? Clinicians will be also looking for to what degree the intern displays independence? Are they needy, complainers, or are they problem solvers and self-starters? • Given the unique nature of clinic, participation is critical to the learning process, therefore this aspect of the clinical experience is given a high priority. 20% of the grade in this course will be determined by participation. This will be measured, but not limited to, the number of patients seen, active involvement in case discussions. Another perimeter of participation will depend upon how readily interns bring a clinician for observation at key points during the course of patient care, especially as measured against the class as a whole. In addition, there are a myriad number of ways in which an intern can participate in the daily educational life of the clinic to their and other team members’ betterment, and determination of this involvement is not limited to the few examples noted above. Determination of participation is at the discretion of the clinician. Finally, a determination of participation remains under the discretion of the department chair. Failure to complete these requirements, attendance policy, intern conduct, as well as performance of DI duties may be reflected on clinic evaluation forms. Grading As noted above, course grade is on a Pass/Fail basis. 70% is considered passing. Special Note: Given that trimesters 8 through 10 make up the direct patient care clinical experience, there is a defined set of requirements that need to be completed over the course of these semesters required for graduation. These requirements are spelled out in detail in Appendix C in this document. 123 The College of Professional Studies’ policy regarding final examinations, as published in the most recent National University of Health Sciences Bulletin, will be followed. Missed Assessment(s): Since this is a clinical course, based upon direct patient care, the issue of missed assessments will not arise. This is especially true given that there are not written examinations associated with this course. Review of Grades and Assessments: As noted above, information concerning assessment will be collected through the use of PDAs or an Internet browser based database system and updated by the clinician(s). This data will be reviewed and sent out as individual emails biweekly to each intern in the program. Each student has 10 calendar days from the date that a test or course grade is made available to review the grade. Failure to discuss the grade or make an appointment to discuss the grade within that allotted time frame will result in forfeiture of the right to question the grade. Questions regarding the course should be directed to Manuel Duarte, DC, chair of clinical practice. Mentoring: It is the natural and customary manner of such a clinical laboratory course that mentoring will be part of the daily activities. Each member of the clinical staff will be available for consultation concerning the care of the student patients and their family members under the interns’ care. TEACHING METHODS AND ACTIVITIES: Teaching methods within this clinician setting consists of oversight of patient care from the moment that the history is obtained, guiding of which exams might be applicable, and development of the diagnosis and treatment plan through to overseeing the actual care. In other words, one-on-one encounters with the staff clinicians serving a given shift are the principle method of instruction. There are opportunities for mentoring and small group tutorials, especially pertaining to material presented in the seminars connected with this class. ADDITIONAL COURSE CONTENT: There is no additional course content. LABORATORY ATTIRE AND REQUIREMENTS: The interns are expected to not only show up early for their shifts but also be properly attired for a clinical environment. The details of what constitutes proper attire is clearly spell out in the Clinic Intern Manual. It will be up to the discretion of the duty clinician to make any judgment call in this realm. Repeat offenses in this area will be handled by the campus disciplinary committee. PROFESSIONAL RESPONSIBILITY: The College of Professional Studies’ policy on code of conduct, as published in the most recent National University of Health Sciences Student Handbook, will be followed. ATTENDANCE POLICY: Attendance at in-services or seminars is mandatory. Roll is taken in the form of a sign-in sheet in the clinic lounge, with the window for not receiving a tardy closed out 15 minutes after the clinic shift starts. Two tardies will constitute an absence. If the intern has a patient scheduled and they are not there prior to the patient’s arrival they will receive a tardy and no credit for their activities in the clinic that shift. If the intern totally misses the appointment through nonattendance and the case must be passed to another intern, this is not only an absence but they will be suspended from receiving credit for patient care for a week. Seminar attendance is handled by roll call at the beginning of a given session. An excuse is given for tardiness when patient care comes first, but only upon the approval of the duty clinician. Interns will still be responsible for the content of the seminar or workshop. Like attendance in clinic, interns are allowed up to four absences from seminar. Clinic attendance: If an intern knows in advance that they will miss a clinic assignment, 3 days notice should be given to their clinician. Make-up shifts will be done on a one-to-one basis and should be scheduled within a week. If illness 124 or an unforeseen event prevents attendance, interns should contact their clinician directly or by voice mail PRIOR to their shift. Non-reported missed shifts will be made up on a two-to-one basis. Scheduled make-ups must be scheduled with at least 24 hours notice prior to presenting to the clinic. A maximum of three absences is allowed per trimester. Excess absences must be approved by the Chair of Clinical Practice and will be made in consultation by the clinician overseeing the intern. If deemed appropriate, absences in excess of the three allowed will be made up shift-for-shift at a two-to-one ratio after notification of completion (“pink slips”) of requirements for graduation have been given out at the end of Trimester 10. Release of an intern’s diploma will be held back until these shifts have been completed. There is no “banking” of absences in anticipation of time missed from clinic without prior approval from the chair of clinical practice. Interns are expected to show up early for their shifts for patients will be present from the moment the shift starts. An intern must be in the clinic and prepared for their shift on time. If an intern is going to be late, they must contact their clinician and inform them of the lateness. An intern who arrives 20 minutes late without notifying their clinician will make up the shift on a two-to-one basis. If arriving less than 20 minutes late three times, the intern will be required to make up the shift. Attendance at off-campus professional seminars does not constitute time spent in clinic nor an excused absence. Travel time to and from a seminar or the National Boards also falls into the same category. DISABILITY SUPPORT SERVICES: Please refer to the most recently published National University of Health Sciences Student Handbook for further information regarding disability disclosure and support services. SYLLABUS INFORMATION: Syllabus prepared by: Manuel Duarte, DC Date: 17 December 2012 Curriculum Committee Approval Date: NUHS President Approval Date: Proposed changes to the course title and identification number, time requirement, prerequisites, general course description, competencies, and objectives as described at the beginning of the syllabus, must be presented to the appropriate department chair. The department chair, in conjunction with the assistant dean(s), may submit the proposed changes to National University of Health Sciences’ Curriculum Committee. If approved, the curriculum committee will submit the proposed changes to the president of National University of Health Sciences. 125 126 Appendix G Abbreviations Abbreviations A a.c. ad feb. ad int. ad lib. BCP b.i.d. BM Before Before Meals Fever Present In the interim As Wanted Birth Control Pill Twice per day Bowel Movement n/1 n.p.o. OB/GYN OC OTC p p PERLA BP Bx C CA CBC CBR CMT COPD CP CVA CVP D/C DD Dx ECG or EKG EEG HEENT or EENT EMS ESR FBC/FBS FUO FX GI GU HA Hb or HgB Hct HMP HTN HVG Hx IF or FC IUD JVP LLQ LUQ MCB MI MVA Blood pressure Biopsy With Cancer Complete Blood Count Complete Bed Rest Chiropractic Manipulative Therapy Chronic Obstructive Pulmonary Disease Cold Packs Cerebrovascular Accident Central Venous Pressure Discontinue Differential Diagnosis Diagnosis Electrocardiogram Electroencephalogram Head/Eyes/Ears/Nose/Throat Electrical Muscle Stimulation Erythrocyte Sedimentation Rate Fasting Blood Glucose/Sugar Fever of Unknown Origin Fracture Gastrointestinal Genitourinary Headache Hemoglobin Hematocrit Hot Moist Packs Hypertension High Volt Galvanism History Interferential Therapy Intrauterine Device Jugular Venous Pressure Left Lower Quadrant Left Upper Quadrant Mean Corpuscular Volume Myocardial Infarction Motor Vehicle Accident pt. Pt Ed. PT Pap p.c. PMI p.r.n. PVC Px q.a.m. q.d. q.h. q.i.d. q.o.d. q.p.m. R R/O RLQ ROM RUQ Rx s SOB Stat. STM SWD Sx Sy T t.i.d. TPT tx T.O. Tx U/A URI US UTI WNL 127 Normal Limits Nothing by Mouth Obstetrics and Gynecology Oral Contraceptive Over the Counter After Pulse Pupils Equally Reactive to Light and Accommodation Patient Patient Education Physical Therapy Papanicolaou Smear After Meals Point of Maximum Intensity As Needed Premature Ventricular Contraction Physical Exam Every Morning Every Day Every Hour Four Times Per Day Every Other Day Every Afternoon/Evening Respirations Rule Out Right Lower Quadrant Range of Motion Right Upper Quadrant Therapy/prescription Without Shortness of Breath Immediately Soft Tissue Massage Shortwave Diathermy Surgery Symptoms Temperature Three Times Per Day Trigger Point Therapy Traction Telephone Order Treatment Urinalysis Upper Respiratory Infection Ultrasound Urinary Tract Infection Within Normal Limits 128 Appendix H DC Intern Weekly Tally Sheet 129 130 Appendix I Equipment Damage and Repair Form 131 132 Appendix J Clinic Outreach Record 133 134 Appendix K Clinic Community Outreach Hours Form 135 136 Appendix L Accident / Incident Report Accident / Incident Report Form FOR A CLINIC ACCIDENT / INCIDENT, IMMEDIATELY SEND THIS REPORT TO HUMAN RESOURCES AND SEND A COPY TO THE DEAN OF CLINICS. This is an ! Accident Report ! Incident Report Date of Report Employee ! Student ! Student Emp. ! Athlete ! Visitor ! Patient ! Time Reported a.m. / p.m. Person Involved Home Phone Social Security # Address Street ! Male City ! Female ! Single State ! Married Department Title Date Time ! Zip Code Divorced ! Widowed a.m. / p.m. Location What Happened Individual in Charge Administrative Information Person in charge when accident/incident occurred Staff member(s) witnessing accident Names and addresses of other witnesses Treatment Recommendation Sent to Doctor/Hospital By whom Who was notified? ! Ambulance ! Security ! Police Describe any other actions Your Signature Date Use Back of Sheet for Other Information 137 Revised - 12/12/2011 138 Appendix M Supervisor’s Accident / Incident Report ! This is an Supervisor’s Accident/Incident Report ☐ Accident Report ☐ Incident Report Date of Accident/Incident_________________ Time of Accident/Incident____________ a.m./p.m. Personnel in Charge_____________________________________________________ Person Involved_________________________________________________________ Location_______________________________________________________________ Description of Accident/Incident____________________________________________ Interventions Taken______________________________________________________ Outcome of Interventions__________________________________________________ Was Emergency Personnel Notified?________________________________________ Was Emergency Transport Needed?________________________________________ Is Follow-up Needed?______________ If so, when?____________________________ By whom?_____________________________________________ Supervisor’s Signature_______________________________ Date ________________ Created'08/07/2013' 139 140 Appendix N Clinical Clerkship Qualifications & Application Requirements Clinical Clerkship Qualifications and Application Requirements To Quality you must have the following prerequisites: • Grade Point Average of at least 2.75 or better • Currently in or starting the correct Trimester depending on Clinic’s requirements and stated within the body of information on each clinic To Apply: Filled out 4 page application form – Application forms are obtained from Jean Fairbank, Student Coordinator. Can only request application in person from Jean her office is on the second floor of the clinic room 533. Mandatory documents that need to be supplied along with application form are: • Copies of all Immunization records • Current yearly TB test results • Proof of HEP B, 3 shot series • Current Curriculum Vitae • Copy of your most recent NBCE exam scores letter • Official NUHS transcripts must be sent directly to the Dean of Clinics in an envelope sealed by the registrar • Letter to Clerkship Program titled: “Why I would be a good Candidate for the Clerkship” ADDED PREREQUISITES FOR BETHESDA CLERKSHIP • Must be a U.S. Citizen • More extensive background check – DOCUMENTS SUBMITTED 40 DAYS IN ADVANCE • All trainees will complete the SAAR-N upon arrival to NNMC NNMC SECURITY PROCEDURES Trainees Rotating at NNMC over 30 days: The NNMC Clinical Champion (or GME Office if a clinical champion is not identified) will send Standard Forms 85P and 306 to the trainees. Trainees must submit completed these two forms with a fingerprint card to the Clinical Champion 30 Days prior to the first day of training. The three forms (SF85P, SF306, and finger print card) will be forwarded to the command security manager. At least two weeks prior to the start of training, each trainee must submit a Base Access Form to the clinical champion. This form will be forwarded to the Pass and ID office. Location: Bethesda - National Naval Medical Center (NNMC) 8901 Wisconsin Avenue Bethesda MD 20889 Dr. Bill Morgan Availability: 1 Student Length of Program: 6 Months – January and June Apply: Beginning of 9th and or 10th Trimester Housing: Not provided – must find own housing Note: Open to other college applications 141 Two Sided http://clinicalinfo.nuhs.edu Location: Veterans Administration 1900 E Main Danville, IL 61832 Dr. Don Owens Availability: 1 Student Length of Program: 1 Month Apply: End of 8th Trimester to Beginning of 9th Trimester Application Deadline: No later than the fourth Friday of Trimester 9 Housing: Provided Note: We are the only college who applies Location: Cancer Treatment Centers of America (CTCA) Midwestern Regional Medical Center Inc. 2520 Elisha Ave. Zion, IL 60099 Dr. Jim Rosenburg Availability: 1 Student Length of Program: 1 Month Apply: Beginning of 9th or 10th Trimester Application Deadline: No later than the fourth Friday of Trimester 9 Housing: Not provided – must find own housing ON HOLD UNTIL 2016 DUE TO A RESEARCH PROJECT Location: Naval Air Station – Clinic- Pensacola 6000 W. Hwy 98 Pensacola, Fl 32512 Dr. Greg Lillie Availability: 1 Student Length of Program: 6 Months – January and June Apply: Beginning of 9th or 10th Trimester Application Deadline: No later than the fourth Friday of Trimester 9 Housing: Not provided – Must find own housing Note: Open to other college applications – at this time 142 Appendix O Ancillary Clinical Experience (ACE) Basics NUHS – Clinical Clerkship Program (CCP) Ancillary Clinical Experience (ACE) Basics National University of Health Sciences (NUHS) Ancillary Clinical Experience (ACE) is designed to offer senior chiropractic/naturopathic interns the opportunity to gain valuable clinical experience in a private practice setting under the close supervision and guidance of an experienced, ethical and successful physician (adjunct faculty physician). The program functions within the parameters established by the Council on Chiropractic Education (CCE) for DC interns and the parameters established by the Council on Naturopathic Medical Education (CNME) for ND interns, as well as the state licensing board of the respective state in which the adjunct faculty clinician is located. The program allows eligible interns to spend part of their clinical training in an off-campus educational experience. The supervising practitioners are adjunct faculty clinicians of National University of Health Sciences. CLINICAL CLERKSHIP PROGRAM ORGANIZATION AND THE CLINICAL CLERKSHIP PROGRAM COMMITTEE The Clinical Clerkship Program (CCP) is under the authority of the Dean of Clinics. The Dean of Clinics oversees the activities of the CCP and has the day-to-day responsibility for the program. The CCP Committee, chaired by the Dean of Clinics, is responsible for reviewing applications from interns and preceptors, making recommendations to the Dean of Clinics regarding program participants, reviewing the progress and performance of participants, and advising the Dean of Clinics on matters concerning the operation and effectiveness of the program. The Dean of Clinics submits recommendations to the Vice President for Academic Services and final approval of the preceptor must be obtained from the President or his/her designee. The Dean of Clinics, in conjunction with his/her chosen advisors, will determine the number of interns assigned to a CCP. Each clinician at the University clinics, with the exception of those at the Salvation Army Clinics, must have a minimum of 5 interns per shift. If this number is not met, then the CCP request may not be approved. INTERN QUALIFICATIONS – ACE To be eligible for selection for participation in the ACE, an intern must meet the following criteria: 1. Successful completion of Phase 3, Term 1 (9th trimester) internship of DC/ND programs. 2. Successful completion of all of the University’s academic and clinical requirements for graduation, except for the required number of internship clock hours. 3. Be in good academic standing and making satisfactory academic progress. A 2.75 GPA average is required. 4. Recommended for participation by the supervising attending clinician and the Chair of Clinical Practice (and the Assistant Dean of Naturopathic Medicine – ND interns only). 5. Passed Part I and II of the examinations of the NBCE. (DC Interns only) 6. Must not be the subject of any University or clinic disciplinary action. 7. Completed all assigned patient care records and related forms including narratives and insurance forms to the satisfaction of the supervising attending clinician. 8. Submitted a completed application form to the Vice President for Administrative Services accompanied by a current curriculum vita. 9. Agree, as evidenced by a signed affidavit, to abide by the law(s) governing adjunct faculty clinicians in the jurisdiction in which the applicant seeks to participate and to abide by the provisions of the NUHS CCP. http://clinicalinfo.nuhs.edu 143 144 Appendix P Clinical Based Internship (CBI) Basics NUHS – Clinical Clerkship Program (CCP) Clinical Based Internship (CBI) Basics National University of Health Sciences (NUHS) is designed to offer chiropractic interns the opportunity to gain valuable clinical experience in a private practice setting under the close supervision and guidance of an experienced, ethical and successful adjunct faculty clinician. The program functions within the parameters established by the Council on Chiropractic Education (CCE) for DC interns, as well as the state licensing board of the respective state in which the adjunct faculty clinician is located. The program allows eligible interns to spend part of their clinical training in an off-campus educational experience. The supervising practitioners are adjunct faculty clinicians of National University of Health Sciences. CLINICAL CLERKSHIP PROGRAM ORGANIZATION AND THE CLINICAL CLERKSHIP PROGRAM COMMITTEE The Clinical Clerkship Program (CCP) is under the authority of the Dean of Clinics. The Dean of Clinics oversees the activities of the CCP and has the day-to-day responsibility for the program. The CCP Committee, chaired by the Dean of Clinics, is responsible for reviewing applications from interns and preceptors, making recommendations to the Dean of Clinics regarding program participants, reviewing the progress and performance of participants, and advising the Dean of Clinics on matters concerning the operation and effectiveness of the program. The Dean of Clinics submits recommendations to the Vice President for Academic Services and final approval of the preceptor must be obtained from the President or his/her designee. The Dean of Clinics, in conjunction with his/her chosen advisors, will determine the number of interns assigned to a CCP. Each clinician, with the exception of those at the Salvation Army Clinics, must have a minimum of 5 interns per shift. If this number is not met, then the CCP request may not be approved. INTERN QUALIFICATIONS – CBI To be eligible for selection for participation in the CBI, an intern must meet the following criteria: 1. Successful completion of the didactic components of the first professional program. 2. Be in good academic standing and making satisfactory academic progress. A 2.75 GPA average is required. 3. Recommended for participation by the supervising attending clinician and the Chair of Clinical Practice. 4. Passed Part I and II of the examinations of the NBCE. 5. Must not be the subject of any University or clinic disciplinary action. 6. Completed all assigned patient care records and related forms including narratives and insurance forms to the satisfaction of the supervising attending clinician. 7. Submitted a completed application form to the Vice President for Administrative Services accompanied by a current curriculum vita. 8. Agree, as evidenced by a signed affidavit, to abide by the law(s) governing adjunct faculty clinicians in the jurisdiction in which the applicant seeks to participate and to abide by the provisions of the NUHS CCP. http://clinicalinfo.nuhs.edu 145 146 Appendix Q Request for Independent Clinic Observation REQUEST FOR INDEPENDENT CLINIC OBSERVATION Date of Request _________________ Current Trimester (Circle) Intern Name ______________________ Clinician _____________________ 9 10 I wish to request time off from my regular clinic shift in order to observe at the clinic listed below. I understand that I am at no time authorized to render any form of care to any patient during this observation. Doctor’s Name ____________________________________________________________ Clinic Name: ______________________________________________________________ Address:__________________________________________________________________ Phone #: _________________________ Dates of Observation:_____________________ Hours student will be at Doctor’s Office: ________________________________________ Intern’s Signature: ________________________ Total # of Hrs. at Doctor’s: ___________ Cell Number: __________________________ Date: ____________________________ DOCTOR’S ACKNOWLEDGMENT Signature below indicates that the above-named doctor acknowledges this request and agrees to accept the student, on an observation only basis for the date(s) and hours listed above. Approval of this observation shall no way imply a relationship between the doctor and National University of Health Sciences. The doctor is not to be considered as faculty of the University and therefore is prohibited from allowing the observing student to render any form of health care on his/her patients. Doctor’s Signature _______________________________________________ A copy of your Doctor’s License must be attached to this form. Please print name _______________________________________________ APPROVAL OF OBSERVATION Clinician’s Signature__________________________________ Date_______________ Dean of Clinic’s Signature_____________________________ Date________________ Clinic Services Mgr. _______________________ Verified Requirements are met Observations may be for a maximum of 10 days total (with no "renewal" of the 10 days allowed) and the student needs to be done with his/her numbers before an observation.) The observation in no way constitutes or serves as a prelude to a preceptorship agreement. Paperwork deadline: paperwork must be completed no later than the third Thursday prior to graduation date. Revised: 7/28/14 147 148 SIGNATURE PAGE NATIONAL UNIVERSITY OF HEALTH SCIENCES NON-SOLICITATION OF PATIENTS AGREEMENT Student Intern (Print Name) ___________________________________ The parties agree that the treatment of patients/clients is a valuable and integral part of the University’s operation and that the University has spent valuable time, effort and expense in securing patients/clients and in developing and maintaining data, records, information and services associated with same. Therefore, during the term of this Clinical Rotation Agreement and for a period of two years following graduation from the University, the Student shall not, either directly or indirectly, perform any act or make any statement which would tend to divert any current patients/clients away from the University or solicit any current patients/clients of any University Clinic, wherever located, either for him/herself for any other person, firm, corporation or health care practice without prior permission, in writing, from the Dean of Clinics or his designee. This shall not limit the intern (with clinician approval) in the clinics from making appropriate and documented patient referrals for diagnostic or therapeutic care. A current patient/client is any individual who, during the clinical enrollment or the year immediately prior to the effective date of this Clinical Rotation contract, visited any University Clinic for the purpose of receiving health care, counsel or treatment. In the event that a Student violates this provision, said violation will be cause for immediate action up to and including expulsion. ________________________________________________________ Signature of Intern ________________________________________________________ Date (mm/dd/yyyy) This form must be on file with the office of the Dean of Clinics before you may see clients in the clinics. Please make a copy for yourself. 149 150 SIGNATURE PAGE I, _____________________________________ acknowledge that I have read and understand the contents of the National University of Health Sciences’ Clinic Intern Manual for the class entering clinic in the _________________________ Trimester. I further acknowledge that I will respect and follow any modifications made and communicated to me by the office of the Dean of Clinics including any updated revisions of the Clinic Intern Manual or sections thereof. I recognize and will respect the University ownership of property, equipment and client related information with which I may come in contact during the course of my 2nd and 3rd trimester training. By affixing my signature below, I agree to abide by all policies and procedures set forth in this manual and I agree to the following Statement on Confidentiality: Confidentially of the medical record is critical. All health care personnel shall uphold the client’s right to privacy. Violation of the confidentiality of client information shall be cause for immediate termination of access to further data and shall be considered Unprofessional Conduct, subject to disciplinary action as set forth in this manual. Penalties for this misconduct may result in expulsion form the National University of Health Sciences. ________________________________________________________ Signature of Intern ________________________________________________________ Date (mm/dd/yyyy) This form must be on file with the office of the Dean of Clinics before you may see clients in the clinics. Please make a copy for yourself. 151






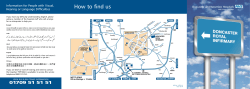



© Copyright 2026