
Inter-Relations Among Declines in Arterial Distensibility, Baroreflex Function and Respiratory Sinus Arrhythmia
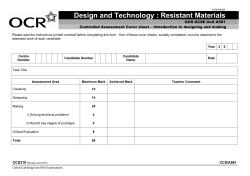
Journal of the American College of Cardiology © 2002 by the American College of Cardiology Foundation Published by Elsevier Science Inc. Vol. 39, No. 9, 2002 ISSN 0735-1097/02/$22.00 PII S0735-1097(02)01787-4 Arterial Distensibility Inter-Relations Among Declines in Arterial Distensibility, Baroreflex Function and Respiratory Sinus Arrhythmia Padmini Kaushal, BS, J. Andrew Taylor, PHD Boston, Massachusetts We hypothesized that structural and neural cardiovascular (CV) deficits may be intimately linked. Specifically, decreased carotid distensibility with age may blunt the arterial baroreflex, thereby reducing resting cardiac vagal tone. BACKGROUND Increased CV risk is associated with lower carotid distensibility, impaired baroreflex function and reduced respiratory sinus arrhythmia (RSA), possibly representing a direct path between structural and neural CV deficits. METHODS We estimated the mechanostructural and neural components of baroreflex function and examined their relation to RSA in young (20 to 31 years) and older (59 to 71 years) subjects rigorously screened for CV and autonomic diseases. RESULTS In the older subjects, RSA was ⬍ 20% of that in the younger subjects. Moreover, mechanical transduction of pressure into barosensory vessel stretch was ⬃40% lower (p ⬍ 0.05) and arterial baroreflex gain more than 60% lower (p ⬍ 0.05) in the older group. Although neural transduction of stretch into vagal outflow only tended to be less (p ⬍ 0.08), it was an important determinant of baroreflex function. A path analysis model showed comparable contributions of both the mechanical and neural components to baroreflex gain; however, lower overall baroreflex gain in the older group did not relate to lower RSA. CONCLUSIONS These data suggest that decreased carotid distensibility does reduce baroreflex function with age, but this does not lead to reduced resting vagal outflow. (J Am Coll Cardiol 2002;39: 1524 –30) © 2002 by the American College of Cardiology Foundation OBJECTIVES Cardiovascular (CV) morbidity and mortality increase with age, in part as a result of structural changes. Arterial vessels undergo age-related degeneration of the medial layer, crosslinking of elastin and collagen, and accumulation of calcium deposits (1,2) that reduce distensibility. Reduced distensibility, especially in elastic vessels such as the carotid artery, has been shown to relate directly to risk for cardiac events (3). Cardiac vagal function also demonstrates age-related deficits; tachycardic responses to cholinergic blockade decline (4), number of central vagal neurons decrease (5), and sinoatrial node muscarinic receptor density is reduced (6) with age. Respiratory sinus arrhythmia (RSA), a commonly used index for resting vagal tone, is a key prognostic indicator of cardiac health (7,8) and declines logarithmically with age (9). Although structural and neural deficits may have independent impact on CV function and health, it is possible that they are intimately linked (10). Decreased carotid distensibility may relate to CV risk by blunting arterial baroreflex function and thereby reducing cardiac vagal tone. Afferent nerves embedded in the carotid From the Laboratories for Cardiovascular Research, Hebrew Rehabilitation Center For Aged Research and Training Institute, and Harvard Medical School Division on Aging, Boston, Massachusetts. This work received research support from the National Institute on Aging, Washington, D.C. (Grant AG14376); the American Federation for Aging Research, New York, New York; Howard Hughes Medical Foundation, Washington, D.C.; and a generous contribution from the Hinda and Fred Shuman Charitable Foundation, Boston, Massachussetts. Manuscript received May 31, 2001; revised manuscript received January 28, 2002, accepted February 6, 2002. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 walls are stretch sensitive (11), and they determine baroreflex responses that buffer arterial pressure changes (12,13). Decreased distensibility would effectively desensitize these receptors and reduce baroreflex-mediated autonomic outflow in response to pressure changes. Decreased baroreflex sensitivity could lead directly to lower vagal tone as the arterial baroreflex may be a primary determinant of resting cardiac vagal outflow. Pharmacologically determined vagal tone is highly correlated to baroreflex sensitivity (13), and, in fact, RSA may derive directly from arterial baroreflex stimulation through waxing and waning arterial blood pressure at the respiratory cycle (14,15). Thus, increased CV risk associated with lower carotid distensibility (16), arterial baroreflex function (17), and RSA (18) may represent a direct path between structural and neural CV deficits. We hypothesized that the age-related decline in carotid distensibility is related to decreased resting cardiac vagal tone through blunting of the arterial baroreflex. We used our recently developed technique (19) to estimate mechanostructural and neural afferent– efferent components of arterial baroreflex function. If reduced vagal tone is related to decreased distensibility then there should be a direct path from the structural baroreflex component to RSA through arterial baroreflex gain. Therefore, we examined the relation of RSA to arterial baroreflex gain and its neural and structural components in both young and older individuals. Kaushal and Taylor Arterial Distensibility and Vagal Control JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 Abbreviations and Acronyms CV ⫽ cardiovascular ECG ⫽ electrocardiogram RSA ⫽ respiratory sinus arrhythmia METHODS Subjects. Fifteen young (20 to 31 years; 5 women) and 9 older (59 to 71 years; 2 women) volunteers were screened and selected according to these criteria: 1) no signs or symptoms of heart disease, hypertension (pressures ⬎150/90 mm Hg), diabetes, neurologic disease or cancer; 2) normal resting electrocardiogram [ECG]; 3) no recent weight change; 4) no regular tobacco use; 5) body weight within 15% of ideal; and 6) no current use of cardioactive medications. Older subjects were screened with a Brucegraded exercise test and a full carotid ultrasound examination to exclude coronary heart disease and carotid vascular disease. Subject characteristics are shown in Table 1. The study was approved by the Institutional Review Board at the Hebrew Rehabilitation Center for Aged. All subjects gave written informed consent. Protocol and measurements. Supine subjects were instrumented with 3-lead ECG for RR-interval, finger photoplethysmograph for beat-by-beat arterial pressures (Finapres, Ohmeda Medical, Baltimore, Maryland), oscillometric arm cuff for a standard measure of brachial arterial pressures to calibrate finger pressures (Dinamap, GE Medical Systems, Mount Prospect, Illinois), elastic respiratory transducer bands for breathing depth and frequency (Respitrace, NIMS, Miami Beach, Florida) and an antecubital venous catheter for drug infusions. Subjects rested quietly for at least 5 min prior to the first trial of paced breathing and pharmacologic baroreflex testing. Three paced breathing and pharmacologic baroreflex trials were performed with ⱖ15 min recovery between trials. Respiration-related RR-interval fluctuations were used to assess basal cardiac vagal outflow. Phasic vagal modulation with respiration results in RSA, an oscillation proportional to the mean level of cardiac vagal outflow (20). The ECG was recorded during 5 min of paced frequency breathing (15 breaths/min). Paced breathing avoids breathing frequency changes, which influence RSA magnitude and alter its relation to vagal outflow (13). After paced breathing, baroreflex testing was conducted using our recently developed approach (19). This technique provides robust linear gain estimates for arterial baroreflex 1525 gain and its mechanical and neural components. Arterial pressure is reduced below threshold and raised through linear and saturation regions, providing clear determination of linear relations. Moreover, acquisition of B-mode ultrasound common carotid images allows determination of carotid diameters on a near beat-by-beat basis. Briefly, we acquired the ECG, beat-by-beat arterial pressures (Finapres) and longitudinal common carotid artery images (Hewlett-Packard 7.5 MHz [Palo Alto, California]; Data Translations DT3152 Frame Grabber; Information Integrity CVI Acquisition software, Stowe, Massachusetts) immediately before and for 2 min after sequential boli of 100 g nitroprusside followed in 60 s by 150 g phenylephrine. This allowed estimation of mechanical transduction of pressure into barosensory vessel stretch (diameter/ pressure), neural transduction of stretch into vagal outflow (RR/diameter) and conventional integrated cardiovagal baroreflex gain (RR/pressure). Analysis. All waveforms were stored to computer for signal-processing and subsequent analysis (Dataq Instruments WINDAQ software [Akron, Ohio]; DSP Development DADiSP software [Newton, Massachusetts]). Digitization at 500 Hz allowed accurate measurement of RRinterval to the nearest 2 ms. The RR-intervals were derived from time difference between successive R-wave peaks. Systolic and diastolic pressures were derived from maxima and minima of the pressure waveform. Common carotid internal diameters were determined from digitized images by custom software (Information Integrity CVI Analysis software). Several points in proximity to near and far wall edges were selected, and the program fit an interpolated spline to each set of preliminary edge points and determined the best edge point from the interpolated line. Near and far wall edge points were modeled as parabolas constrained to have the same curvature, and diameter was estimated from the distance between parabolas. User-selected preliminary edge points were reused for successive images to reduce variance in the diameter time series. Respiratory sinus arrhythmia was quantitated from power spectral analysis of each 300 s RR-interval time series during paced breathing. The time series was interpolated to 4 Hz; based on the Welch algorithm (21), seven overlapping periodograms were averaged to produce the spectrum estimate for the entire time series. Power within the respiratory frequency band, defined as 0.2 to 0.3 Hz, was summed to estimate RSA. Arterial baroreflex gain and neural and mechanical com- Table 1. Subject Characteristics Young Older Age (yrs) BMI (kg/m2) Resting Heart Rate (beats/min) Resting Systolic Pressure (mm Hg) Resting Diastolic Pressure (mm Hg) Resting Systolic Carotid Diameter (mm) Resting Diastolic Carotid Diameter (mm) 25.1 ⫾ 0.7 66.5 ⫾ 1.4 22.9 ⫾ 0.5 23.5 ⫾ 0.9 59 ⫾ 2 60 ⫾ 3 115 ⫾ 3 124 ⫾ 4 66 ⫾ 2 72 ⫾ 3 6.86 ⫾ 0.18 6.98 ⫾ 0.10 6.35 ⫾ 0.18 6.70 ⫾ 0.11 BMI ⫽ body mass index. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 1526 Kaushal and Taylor Arterial Distensibility and Vagal Control JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 Figure 1. Examples of arterial baroreflex data from one young and one older volunteer. ponents were derived from the associations among RRinterval, systolic pressure and systolic carotid diameter during the drug-induced rise in arterial pressure. Beat-bybeat values for each parameter were averaged across 3 mm Hg pressure increments to account for respiration-related variations and increase confidence in the relations among variables. Three linear relations were extracted from the sigmoid relations between: systolic carotid diameter and systolic pressure, representing the mechanical baroreflex component; RR-interval and systolic pressure, representing the integrated baroflex gain; RR-interval and carotid systolic diameter, representing the neural baroreflex component. Each linear relation was independently determined; that is, saturation and threshold regions were excluded from each relation without regard to where these regions might lie in the other two. (In addition, it should be noted that no a priori mathematical dependency exists among relations derived from three independent measures.) Image consistency throughout pharmacologic interventions requires three baroreflex trials to obtain duplicate trials with adequate images for analysis on all subjects. Values were averaged across two trials or across the two best trials (highest r values) in subjects with three adequate trials. A minimum value of r ⫽ 0.65 identified significant relations among variables. Across all subjects and all trials, the three relations averaged r ⬎ 0.86. High reproducibility of these measures has been shown previously (19), and was comparable in these young and older subjects. Values for RSA were averaged from the two trials used for baroreflex assessment. Statistics. Differences were assessed by Student’s t-test with p ⬍ 0.05. To determine whether the hypothesized indirect connection of vascular distensibility to vagal tone through the arterial baroreflex existed, we used an extension of multiple regression, structural equation modeling (22). For our application, we used a path analysis, which hypoth- Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 esizes specific relations among variables and tests the model with a linear equation system. The a priori relationships among the arterial baroreflex, its components, and RSA were defined and a path diagram was constructed to represent direct and indirect effects. Path coefficients (beta weights) were calculated from structural equations reflecting defined effects. The goodness of overall model fit was determined by a nonsignificant chi-square and path coefficients were considered significant if r2 ⬎ 0.5 for the predicted variables (baroreflex gain and RSA). RESULTS Figure 1 illustrates the baroreflex gain and its mechanical and neural components in one young and one older subject. The mechanical component was somewhat less sensitive in the older subject, indicating reduced carotid distensibility. However, arterial baroreflex gain in this subject was less than half that in the younger volunteer, a difference not fully accounted for by the ⬃15% lower distensibility. Thus, the lesser sensitivity of the neural component in this older subject compared to the younger counterpart importantly contributed to the lower arterial baroreflex gain. Differences in these examples broadly applied to the groups as a whole (Fig. 2). Mechanical transduction of pressure into barosensory vessel stretch was ⬃40% lower in the older subjects. However, arterial baroreflex gain was ⬎60% lower; thus, even though differences in neural transduction of stretch into vagal outflow only approached significance, it likely played an important role in reducing baroreflex function in the older group. Figure 3 illustrates RSA in the young and older subjects from Figure 1. Respiration-related RR-interval fluctuations were profound in this young subject, resulting in large RR-interval power at the respiratory frequency. In contrast, the older subject had markedly lower RSA, despite a longer 1530 Kaushal and Taylor Arterial Distensibility and Vagal Control 26. Sa Cunha R, Pannier B, Benetos A, et al. Association between high heart rate and high arterial rigidity in normotensive and hypertensive subjects. J Hypertens 1997;15:1423–30. 27. Lage SG, Polak JF, O’Leary DH, Creager MA. Relationship of arterial compliance to baroreflex function in hypertensive patients. Am J Physiol 1993;265:H232–7. 28. Taylor JA, Eckberg DL. Fundamental relations between short-term RR interval and arterial pressure oscillations in humans. Circulation 1996;93:1527–32. 29. Taylor JA, Myers CW, Halliwill JR, Seidel H, Eckberg DL. Sympathetic restraint of respiratory sinus arrhythmia: implications for vagalcardiac tone assessment in humans. Am J Physiol Heart Circ Physiol 2001;280:H2804 –14. 30. Eckberg DL, Drabinsky M, Braunwald E. Defective cardiac parasympathetic control in patients with heart disease. N Engl J Med 1971;285:877–83. 31. Taylor JA, Carr DL, Myers CW, Eckberg DL. Mechanisms underlying very-low-frequency RR-interval oscillations in humans. Circulation 1998;98:547–55. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 32. La Rovere MT, Bigger JT, Jr, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) investigators. Lancet 1998;351:478 –84. 33. Itoh H, Bunag RD. Aging reduces cardiovascular and sympathetic responses to NTS injections of serotonin in rats. Exp Gerontol 1992;27:309 –20. 34. Dauchot P, Gravenstein JS. Effects of atropine on the electrocardiogram in different age groups. Clin Pharmacol Ther 1971;12:274 –80. 35. Tomiyama H, Kihara Y, Nishikawa E, et al. An impaired carotid sinus distensibility and baroreceptor sensitivity alter autonomic activity in patients with effort angina associated with significant coronary artery disease. Am J Cardiol 1996;78:225–7. 36. De Ferrari GM, Landolina M, Mantica M, Manfredini R, Schwartz PJ, Lotto A . Baroreflex sensitivity, but not heart rate variability, is reduced in patients with life-threatening ventricular arrhythmias long after myocardial infarction. Am Heart J 1995;130:473–80. 1528 Kaushal and Taylor Arterial Distensibility and Vagal Control JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 Figure 3. Raw and power spectral data during paced breathing in one young and one older volunteer. Effects of vagal neural deficits. Cardiac vagal outflow is crucial for both baroreflex-mediated bradycardic responses (30) and nearly all frequencies of heart rate variability (31). Both have significant prognostic value for cardiac mortality (18,32) because of the cardioprotective effects of this common vagal effector. We found that neural control of bradycardic responses was low and that it strongly determined baroreflex gain in older individuals. Moreover, we found a link between age-related reductions in our neural baroreflex component and RSA. Thus, a generalized vagal deficit may result in both lesser baroreflex-mediated bradycardia and lower RSA. Our neural baroreflex component encompasses various aspects of cardiovagal function. However, the link between this aspect of baroreflex control and RSA may indicate that significant age-related neural deficits exist beyond the afferent baroreceptive nerves. For example, there is evidence of altered central autonomic integration (33), reduced vagal outflow (34) and lower muscarinic sinoatrial node receptor density (6) with advancing age. Our findings suggest that these declines may play a direct role in age-related reductions of both resting vagal tone and cardiovagal baroreflex gain. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 Clinical implications. Although carotid distensibility correlates to baroreflex sensitivity in heart disease patients (35), Eckberg et al. (30) concluded, over 30 years ago, that reduced compliance could not fully explain the baroreflex derangement they observed. In their examination of patients with a range of heart diseases not known to involve autonomic nerves directly, they found blunted tachycardiac responses to vagal blockade and a level of baroreflex impairment related directly to the severity of cardiac symptoms. Subsequent work has made use of RSA to characterize these vagal deficits (7,9) and to assess CV risk (8,32). However, our data suggest that baroreflex gain and not RSA crucially depends upon vascular function. This could explain why baroreflex function provides a better index of risk for malignant arrhythmias (17,36) and overall cardiac mortality (18) than heart rate variability. Arterial stiffness may carry risk independent of its autonomic effects, and low baroreflex gain would encompass this risk as well as that associated with compromised vagal function. Despite the fact that both RSA and baroreflex gain are useful indices, our results suggest the information contained within them differ. Conclusions. These data provide insight to carotid arterial distensibility, arterial baroreflex sensitivity and RSA as JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 Kaushal and Taylor Arterial Distensibility and Vagal Control 1529 Figure 4. Path diagram and coefficients of the model for young and older groups of patients. n.s. ⫽ nonsignificant effect. indices for CV risk. Vascular structural declines may not impact resting vagal tone, but they do reduce baroreflex sensitivity. Moreover, because baroreflex gain encompasses both vascular stiffness and vagal function, arterial baroreflex gain may provide greater insight to CV risk than heart rate variability indices. At the least, our data suggest that baroreflex sensitivity and RSA are independent markers of autonomic function. Reprint requests and correspondence: J. Andrew Taylor, PhD, Director, Laboratories for Cardiovascular Research, HRCA Research and Training Institute, 1200 Centre Street, Boston, Massachusetts 02131. E-mail: [email protected]. REFERENCES 1. Schulman SP. Cardiovascular consequences of the aging process. Cardiol Clin 1999;17:35–49. 2. Lakatta EG. Cardiovascular regulatory mechanisms in advanced age. Physiol Rev 1993;73:413–67. 3. Riley WA, Freedman DS, Higgs NA, Barnes RW, Zinkgraf SA, Berenson GS. Decreased arterial elasticity associated with cardiovascular disease risk factors in the young. Bogalusa Heart Study. Arteriosclerosis 1986;6:378 –86. 4. Jose AD, Taylor RR. Autonomic blockade by propranolol and atropine to study intrinsic myocardial function in man. J Clin Invest 1969;48: 2019 –31. 5. Sturrock RR. A comparison of age-related changes in neuron number in the dorsal motor nucleus of the vagus and the nucleus ambiguus of the mouse. J Anat 1990;173:169 –76. 6. Brodde OE, Konschak U, Becker K, et al. Cardiac muscarinic receptors decrease with age. In vitro and in vivo studies. J Clin Invest 1998;101:471–8. 7. Casolo GC, Stroder P, Signorini C, et al. Heart rate variability during the acute phase of myocardial infarction. Circulation 1992;85:2073–9. 8. Moser M, Lehofer M, Sedminek A, et al. Heart rate variability as a prognostic tool in cardiology. A contribution to the problem from a theoretical point of view. Circulation 1994;90:1078 –82. 9. De Meersman RE. Aging as a modulator of respiratory sinus arrhythmia. J Gerontol 1993;48:B74 –8. 10. Joyner MJ. Effect of exercise on arterial compliance. Circulation 2000;102:1214 –5. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 11. Angell-James JE, Lumley JS. The effects of carotid endarterectomy on the mechanical properties of the carotid sinus and carotid sinus nerve activity in atherosclerotic patients. Br J Surg 1974;61:805–10. 12. Wallin BG, Nerhed C. Relationship between spontaneous variations of muscle sympathetic activity and succeeding changes of blood pressure in man. J Auton Nerv Syst 1982;6:293–302. 13. Kollai M, Jokkel G, Bonyhay I, Tomcsanyi J, Naszlady A. Relation between baroreflex sensitivity and cardiac vagal tone in humans. Am J Physiol 1994;266:H21–7. 14. Piepoli M, Sleight P, Leuzzi S, et al. Origin of respiratory sinus arrhythmia in conscious humans. An important role for arterial carotid baroreceptors. Circulation 1997;95:1813–21. 15. Melcher A. Respiratory sinus arrhythmia in man. A study in heart rate regulating mechanisms. Acta Physiol Scand Suppl 1976;435:1–31. 16. Arnett DK, Boland LL, Evans GW, et al. Hypertension and arterial stiffness: the Atherosclerosis Risk In Communities study. ARIC investigators. Am J Hypertens 2000;13:317–23. 17. Mortara A, La Rovere MT, Pinna GD, et al. Depressed arterial baroreflex sensitivity and not reduced heart rate variability identifies patients with chronic heart failure and nonsustained ventricular tachycardia: the effect of high ventricular filling pressure. Am Heart J 1997;134:879 –88. 18. La Rovere MT, Pinna GD, Hohnloser SH, et al. Baroreflex sensitivity and heart rate variability in the identification of patients at risk for life-threatening arrhythmias: implications for clinical trials. Circulation 2001;103:2072–7. 19. Hunt BE, Fahy LM, Farquhar WB, Taylor JA. Quantification of mechanical and neural components of the cardiac-vagal baroreflex in humans. Hypertension 2001;37:1362–8. 20. Hayano J, Sakakibara Y, Yamada A, et al. Accuracy of assessment of cardiac vagal tone by heart rate variability in normal subjects. Am J Cardiol 1991;67:199 –204. 21. Welch P. The use of fast Fourier transform for the estimation of power spectra: a method based on time averaging over short, modified periodograms. IEEE Trans Audio Electroaccoust 1967;15:70 –3. 22. Everitt B, Dunn G. Applied Multivariate Data Analysis. London: Edward Arnold, 1991. 23. Wilson PW, Kauppila LI, O’Donnell CJ, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 2001;103:1529 –34. 24. Smulyan H, Safar ME. Systolic blood pressure revisited. J Am Coll Cardiol 1997;29:1407–13. 25. Avolio AP, Deng FQ, Li WQ, et al. Effects of aging on arterial distensibility in populations with high and low prevalence of hypertension: comparison between urban and rural communities in China. Circulation 1985;71:202–10. 1530 Kaushal and Taylor Arterial Distensibility and Vagal Control 26. Sa Cunha R, Pannier B, Benetos A, et al. Association between high heart rate and high arterial rigidity in normotensive and hypertensive subjects. J Hypertens 1997;15:1423–30. 27. Lage SG, Polak JF, O’Leary DH, Creager MA. Relationship of arterial compliance to baroreflex function in hypertensive patients. Am J Physiol 1993;265:H232–7. 28. Taylor JA, Eckberg DL. Fundamental relations between short-term RR interval and arterial pressure oscillations in humans. Circulation 1996;93:1527–32. 29. Taylor JA, Myers CW, Halliwill JR, Seidel H, Eckberg DL. Sympathetic restraint of respiratory sinus arrhythmia: implications for vagalcardiac tone assessment in humans. Am J Physiol Heart Circ Physiol 2001;280:H2804 –14. 30. Eckberg DL, Drabinsky M, Braunwald E. Defective cardiac parasympathetic control in patients with heart disease. N Engl J Med 1971;285:877–83. 31. Taylor JA, Carr DL, Myers CW, Eckberg DL. Mechanisms underlying very-low-frequency RR-interval oscillations in humans. Circulation 1998;98:547–55. Downloaded From: http://interventions.onlinejacc.org/ on 10/15/2014 JACC Vol. 39, No. 9, 2002 May 1, 2002:1524–30 32. La Rovere MT, Bigger JT, Jr, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) investigators. Lancet 1998;351:478 –84. 33. Itoh H, Bunag RD. Aging reduces cardiovascular and sympathetic responses to NTS injections of serotonin in rats. Exp Gerontol 1992;27:309 –20. 34. Dauchot P, Gravenstein JS. Effects of atropine on the electrocardiogram in different age groups. Clin Pharmacol Ther 1971;12:274 –80. 35. Tomiyama H, Kihara Y, Nishikawa E, et al. An impaired carotid sinus distensibility and baroreceptor sensitivity alter autonomic activity in patients with effort angina associated with significant coronary artery disease. Am J Cardiol 1996;78:225–7. 36. De Ferrari GM, Landolina M, Mantica M, Manfredini R, Schwartz PJ, Lotto A . Baroreflex sensitivity, but not heart rate variability, is reduced in patients with life-threatening ventricular arrhythmias long after myocardial infarction. Am Heart J 1995;130:473–80.










© Copyright 2026