
Document 5293
99 Common Questions (and more) about Palliative Care. What is pai pain? How is p assessed? What are different types of pain? Why is a history of subs substance abus relevant to pain assessment and management? How is it assessed? How is pai assessed in someone who is confused? Which opioids are preferred for use? Ho should opioids be ordered? 99 Common Questions (and more) about ab Hospice Palliative CareWhat is breakthrough pain? How should break through throug opioids b ordered? What is the maximum dose of an opioid? What is the preferred prefe route administration of opioids? What are the potential side effects of an oopioid? Wha drowsiness with op eurotoxicity? What are the interventions? How can excessive drowsin use be decreased? How are opioids used safely in persons with renal rena impairme abou What are the causes of myoclonus? 99 Common Questions (and more) m Hospice Palliative CareDoes unrelieved pain always require increasing increasi the opio ose? Should opioids ever be withheld? Should placebos ever be administered? W adm other medications are used in the management of pain? What are the nonharmaceutical interventions to control pain? How can questions rega regarding addic e managed? How is pain managed in persons with an addiction history? histo 99 Com Questions (and more) about Palliative CareWhat can be done when family fa mem ive or request opioids inappropriately? What is anorexia cachexia syndrome? W sy re the causes? How can appetite and oral intake be optimized? What can be don assist persons and their families cope with reduced nutritional intake intake? Is nutritio Common Ques pport appropriate? What is constipation? How is it assessed? 99 Com (and more) about Hospice Palliative Care What causes constipation? What are t nterventions for constipation? How is diarrhea assessed? What are th the causes? W are the interventions? What is bowel obstruction? How is it assessed? 99 Comm Questions (and more) about Hospice Palliative Care. What are the cau causes? What the interventions for bowel obstruction? What is dehydration? How is i dehydrati sessed? When is it appropriate to hydrate? When is it not appropria appropriate to hydra hydration appropriate forth a person who has edema? How should hydration h b aintained? What is nausea and vomiting? What causes nausea and vvomiting? Ho nausea and vomiting assessed? What are the interventions to contro control nausea an vomiting? 99 Common Questions (and more) about Hospice Palliative Palliativ Care Wha delirium? What are the causes of delirium? How is delirium assessed? What are nterventions for delirium? What is dyspnea? What are the causes dyspnea? dy How yspnea assessed? What are the interventions for dyspnea? What are edema, asc and lymphedema? What are the causes? How are edema, ascites and lymphede ssessed? 99 Common Questions (and more) about Hospice Palliative Care What Published by: bed-bound people be repositioned regularly? the interventions? regula What Should Edmonton PalliativeWhat Care are Program pruritis? What causes it? How isZone it assessed? the interventions? interven Wha AlbertaWhat Healthare Services, Edmonton, Canadaand sstomatitis (s ontributes to taste changes? xerostomia (dry mouth) mouth)? What causes xerostomia and stomatitis? How do you assess xerostomia x 99 Common Questions (and more) About Hospice Palliative Care A nurse’s handbook 4 edition Copyright Notice Copyright © (1997 – 2013) Alberta Health Services. This material is protected by Canadian and other international copyright laws. All rights reserved. These materials may not be copied, published, distributed or reproduced in any way in whole or in part without the express written permission of Alberta Health Services. These materials are intended for general information only and are provided on an “as is”, “where is” basis. Although reasonable efforts were made to confirm the accuracy of the information, Alberta Health Services does not make any representation or warranty, express, implied or statutory, as to the accuracy, reliability, completeness, applicability or fitness for a particular purpose of such information. These materials are not a substitute for the advice of a qualified health professional. Alberta Health Services expressly disclaims all liability for the use of these materials, and for any claims, actions, demands or suits arising from such use. To seek permission to use, modify, or adapt material that is subject to AHS copyright, contact the Edmonton Zone Palliative Care Program via telephone at 1-780-735-7834, facsimile at 1-780-735-7640, or regular mail at Room 335, St. Marguerite Health Services Centre, 1090 Youville Drive West, Edmonton, Alberta, Canada, T6L 0A3. ISBN 978-0-929064-53-6 The Authors Editors Fourth Edition Jacquie Peden RN MN, Consultant Independent Practice, Westerose, AB Sandra K. Young, MScN, RN, CHPCN(C), Clinical Nurse Specialist, Edmonton Zone Palliative Care Program, Edmonton, AB Ursula Bohn RN, MN, CHPCN(C), Clinical Nurse Specialist, Palliative/End-of-Life – Calgary Zone, AB Arlene McDonald RN, BN, Nurse Consultant, Edmonton Zone Palliative Care Program, Edmonton, AB. Reviewers Fourth Edition Pablo Amigo MD, MCFP. Palliative Medicine Physician, Tertiary Palliative Care Unit, Grey Nuns Community Hospital, Edmonton, AB. Darcee Bidgood MSN RN CHPCN(C) President, CHPC Nurses Group, Victoria, BC Carmel Collins RN BN NP-PHC, CHPCN(C), Nurse Practitioner, Regional Palliative Care Leadership Team Rehabilitation, Continuing & Palliative Care Program, Eastern Health, St. John’s, NL Connie Doucet RN CHPCN(C), Palliative Care Coordinator, Extra Mural Program, Miramichi, NB Joan Faily BMSc, MBBS, CCFP, Palliative Medicine Physician, Palliative Community Consult Team, Edmonton Zone, Edmonton, AB Ruth Herbert BScN RN CHPCN(C), Palliative/End-of Life Care Integrated Home Care Team, Calgary, AB Juliana Howes RN MN CHPCN(C), Clinical Nurse Consultant, Hospice Palliative Care Teams for Central LHIN, Newmarket, ON Julia Johnston RN (EC) MN NP-Adult, CHPCN(C), Advanced Practice Nurse, Mississauga Halton Palliative Care Initiative, Mississauga, ON Charlotte Koso RN BN CHPCN(C), Senior Manager Program Planning & Service Integration CarePartners, Mississauga, ON iii Lawrence Lee MD, CCFP, Palliative Medicine Physician, Palliative Community Consult Team, Edmonton Zone, Edmonton, AB Deanna Makortoff BScOT(c), Occupational Therapist, Innisfail Community Health Center, Innisfail, AB Kathryn McGovern RN CHPCN(C), Home Care Nurse, North Zone, Grande Prairie, AB Joanne Mills RN MSc(A) CHPCN(C), Clinical Nurse Specialist, Palliative Care, St Boniface Hospital Palliative Care Service, Winnipeg, MB Jacki Morgan RN BScN CHPCN(C), Clinical Practice Coordinator, Central Okanagan Hospice Palliative Care Program, Kelowna, BC Cheryl Nekolaichuk PhD R Psych, Psychologist, Tertiary Palliative Care, Grey Nuns Community Hospital, Edmonton, AB Doreen Oneschuk MD, CCFP, Palliative Medicine Physician, Palliative Community Consult Team, Edmonton Zone, Edmonton, Alberta Larissa Podilsky BScN RN, Palliative Care Nurse Consultant, University of Alberta Hospital, Edmonton, AB Krista Rawson RN MN, NP-Adult, Nurse Practitioner, Central Alberta Cancer Centre, Red Deer, AB Heather Skinner RN CHPCN(C), Home/Hospital Consult Nurse, Cape Breton District Health Authority, Sydney, NS Margot Sondermann BScPT, MEd, Palliative Consultant for End Stage Lung Disease, Palliative / End of Life Care - Calgary Zone, Calgary, AB Simone Stenekes RN MN CHPCN(C), Clinical Nurse Specialist Pediatric Symptom Management and Palliative Care Service, Palliative Care Program, Winnipeg Regional Health Authority - Winnipeg, MB Merle Teetaert RN CHPCN(C), Regional Palliative Care Coordinator, Assiniboine Regional Health Authority, Deloraine, MB Coby Tschanz RN PhD(c), Senior Instructor, University of Victoria, School of Nursing, Victoria, BC Beth Tupala RN CHPCN(C), Clinical Nurse Educator, Covenant Health, Tertiary Palliative Care, Grey Nuns Community Hospital, Edmonton, AB Loretta Ward RN CHPCN(C), Program Manager, Emmanuel House, Hamilton ON Nathalie Warmerdam RN, Eganville, ON iv Sharon Watanabe, MD, FRCPC, Director, Department of Symptom Control and Palliative Care, Cross Cancer Institute, Edmonton, AB Debbie Watt RN CHPCN(C), Director Clinical Management, Bayshore Home Health, Ottawa, ON Erik Williams BA, Health Promotion Facilitator, Comprehensive Tissue Centre, Edmonton, AB Terri Woytkiw RN MN CHPCN(C), Lead-Clinical Support, Seniors Health North Zone, Onoway, AB Shari Young RN BScN CHPCN(C), Manager, Palliative Community Consult Team, Edmonton Zone, Edmonton, AB Production Support, Fourth Edition Publishing Advice and Pre-press Louise Ziola BA, some production! Editors Third Edition Jacquie Peden RN MN, Consultant Independent Practice, Edmonton, AB Donna deMoissac BScN MN CON(c) CHPCN (c), Nurse Practitioner, Royal Alexandra Hospital, Edmonton, AB Karen MacMillan RN BScN, Manager Unit 43, Grey Nuns Hospital, Edmonton, AB Tayreez Mushani-Kanji RN BScN CON(c) CHPCN(C), Community Liaison, Cross Cancer Institute, Edmonton, AB Reviewers Third Edition Darcee Bidgood RN MSN CHPCN(C), Clinical Nurse Specialist, Palliative Care, Vancouver Island Health Authority, BC Maryse Bouvette RN BScN MEd CON(c) CHPCN (c), Coordinator Pain and Symptom Team/Community Consult, SCO Health Service, Ottawa, ON Anna Maria Buhr MSW, Palliative Care Social Worker, St. Paul’s Hospital, Saskatoon, SK Carleen Brenneis(3) RN MHSA, Program Director, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Barbara Campbell RN, Manager of Nursing and Inner City Health, VON Ottawa Branch, Ottawa, ON Pat Clark RN, Palliative Home Care, Saskatoon Health Region, Saskatoon, SK v Paul Daeninck MD MSc FRCPC DABIM, Acting Palliative Care Medical Director, WRHA Palliative Care, Winnipeg, MB Chris Emery RN MSN CON(c) CNS, Hospice Palliative Care, Fraser Health, New Westminster, BC Robin Fainsinger(2) MD, Clinical Director, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Romayne Gallagher MD CCFP, Head, Division of Residential Care and Operations Leader, Providence Health Care, Vancouver, BC Darlene Grantham MN CHPCN(C), Clinical Nurse Specialist, WRHA Palliative Care, Winnipeg, MB Debbie Gravelle RN BScN MHS(c), Advance Practice Nurse, SCO Health Service, Ottawa, ON Margaret Harris BA RN CHPCN(C), Palliative Care Unit, SCO Health Service, Ottawa, ON Georgena Haubrich RN, Palliative Home Care, Saskatoon Health Region, Saskatoon, SK Lori A. Ives-Baine RN BScN, Palliative and Bereavement Coordinator, Neonatal Intensive Care Sick Children, Toronto, ON Shelley Jolly BA RN BSN, Clinical Coordinator Palliative Care, Saskatoon City Hospital and Long Term Care, Saskatoon, SK Connie Lachapelle, Manager, Spiritual Care, St. Paul’s Hospital, Saskatoon, SK Barb Linkewich RN HBScN IBCLC CHPCN(C), Program Manager, Northwestern Ontario Pain and Symptom Management Team, Thunder Bay, ON Addie Loomes RN BScN, Clinical Coordinator, Palliative Home Care, Saskatoon Health Region, Saskatoon, SK Joan Mac Donald RN BScN MEd, National Practice Consultant, Client Services, VON Canada, Montreal, QC Rev. Michael Marshall, Anglican Chaplain, Hospital for Sick Children, Toronto, ON Mark Miller PhD, Ethicist, St. Paul’s Hospital, Saskatoon, SK Fred Nelson MSW RSW, Director of Social Work, WRHA Palliative Care Subprogram, Winnipeg, MN Christine Newman MD FRCPC, Staff Neonatologist, Palliative Care Physician, Hospital for Sick Children, Toronto, ON Daphne Powell RN BScN, Nurse Coordinator, Palliative Care, St. Paul’s Hospital, Saskatoon, SK vi Ann-Marie Primeau RN, Bereavement Coordinator, Manager Nursing and Health Service Coordinator, Hospice, VON, Halton Branch, Oakville, ON Maria Pruett RN CHPCN (c), Palliative Care Unit, SCO Health Service, Ottawa, ON Shannon Pyziak RN BN CHPCN(C), Regional Palliative Care Coordinator, Interlake Regional HA, Fisher Branch, MB Janet Ursel RN BScN, Palliative Home Care, Saskatoon Health Region, Saskatoon, SK Linda Read Paul(3) RN MN CHPCN(C) CNS, Palliative and Hospice Care Service, Calgary Health Region, Calgary, AB Maria Rugg RN MN ACNP CHPCN(C), Palliative and Bereavement Care Program, Hospital for Sick Children, Toronto, On Myrna Sawatzky RN BSN, Clinical Coordinator, Palliative Care, Royal University Hospital, Saskatoon, SK Lisa Savage-Larose RN CHPCN (c), Palliative Care Unit, SCO Health Service, Ottawa, ON Connie Sessa RN MN (c), Advanced Practice Nurse Student, Hospital for Sick Children, Toronto, ON Judy Simpson RN BN MEd CHPCN(C), Palliative and Supportive Care Coordinator, Cancer Care Nova Scotia, Halifax, NS Ken Stakiw MD CCFP FCFP, Medical Director, Palliative Service, Saskatoon Health Region, Saskatoon, SK Simone Stenekes RN MN CHPCN(C), Clinical Nurse Specialist, Pediatric Palliative Care Service, Halifax, NS Jackie Theriault RN CHPCN(C), Palliative Care Unit, SCO Health Service, Ottawa, ON Gregg Trueman NP PhD MN CHPCN(C), Nurse Practitioner, Faculty, Mount Royal University, Calgary, AB Cindy VanHalderen RSW MSW, Social Worker, Hospital for Sick Children, Toronto, ON Meredith Wild RN MN, Manager, Palliative Care Services, Saskatoon Health Region, Saskatoon, SK Brian Zimmer, Director of Mission, St. Paul’s Hospital, Saskatoon, SK vii Production Support and National Review Coordination, Third Edition (Pallium Project, Phase II) Project Oversight Michael Aherne MEd CMC Project Coordination Jacquie Peden RN MN Research Assistance Crystal Beaumont BSc Publishing Advice and Pre-press Louise Ziola BA, some production! Contributors Second Edition Beth Perry RN PhD, Editor, Associate Professor, Athabasca University, Edmonton, AB Susan Campbell RN BScN, Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Trish Clark RN MN CON(c) CNS, Palliative Care, Tom Baker Cancer Centre, Calgary, AB Janice Chobanuk RN BScN CON(c), Former Nurse Manager 9Y Edmonton General Continuing Care Centre, Edmonton, AB Gary Frank RN BEd CON(c), Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Dennie Hycha RN MN, Former Palliative Care Program Coordinator. David Thompson Health Region, Red Deer AB Sharon Hunter RN BScN, Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Kate Squires RN BScN, Clinical Educator Unit 43, Grey Nuns Hospital, Edmonton, AB Contributors First Edition Eduardo Bruera MD, Former Clinical Director, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Patsy Cantwell RN BScN, Former Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Susan MacKay RN BScN, Former Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Sandy McKinnon RN MN Former Manager Unit 43 Grey Nuns Hospital, Edmonton, AB Sally Turco RN CON(c), Former Nurse Consultant, Capital Health, Regional Palliative Care Program, Capital Health, Edmonton, AB Note: Some of these individuals contributed to all three editions of this handbook, indicated by a (3) and some have contributed to two editions, indicated by a (2). viii Introduction Who Will Use This Handbook? This handbook was written to enhance the professional caregiver’s capacity and confidence in offering Hospice Palliative Care (HPC). Professional caregivers work in a variety of settings, including urban, rural, home, hospital, hospice, and residential or continuing care. They play a key role in addressing physical, psychosocial, and spiritual needs, providing practical support, coordinating services, and accessing palliative care specialists for more complex situations. Many of these professional caregivers may have limited education and skills in HPC. Furthermore, the opportunity to provide palliative services in a primary-care practice can be sporadic, making it difficult to maintain a high-level of clinical practice, especially in the absence of reminder tools, bed-side decision supports, and resources. What is Hospice Palliative Care? The Canadian Hospice Palliative Care Association (2013) defines hospice palliative care as whole-person health care that aims to relieve suffering and improve the quality of living and dying. Hospice palliative care strives to help individuals and their families: • Address physical, psychological, social, spiritual and practical issues and associated expectations, needs, hopes and fears, • Prepare for, and manage, self-determined life closure and the dying process, and • Cope with loss and grief during the illness and bereavement. Hospice palliative care aims to: • Treat all active issues. • Prevent new issues from occurring. • Promote opportunities for meaningful and valuable experiences, personal and spiritual growth, and self-actualization. Hospice palliative care is appropriate for any patient and/or family living with, or at risk of developing, a life-threatening illness due to any diagnosis, with any prognosis, regardless of age, and at any time they have unmet expectations and/or needs, and are prepared ix to accept care. HPC may complement and enhance diseasemodifying therapy or it may become the total focus of care. Hospice palliative care is most effectively delivered by an interdisciplinary team of healthcare providers who are knowledgeable and skilled in all aspects of the caring process related to their discipline of practice. These providers are typically trained by schools or organizations that are governed by educational standards. Once licensed, providers are accountable to standards of professional conduct that are set by licensing bodies and/or professional associations. The World Health Organization (2013) defines hospice palliative care as an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Hospice Palliative Care: • Provides relief from pain and other distressing symptoms. • Affirms life and regards dying as a normal process. • Intends neither to hasten or postpone death. • Integrates the psychological and spiritual aspects of patient care. • Offers a support system to help patients live as actively as possible until death. • Offers a support system to help the family cope during the patient’s illness and in their own bereavement. • Uses a team approach to address the needs of patients and their families, including bereavement counseling, if indicated. • Will enhance quality of life, and may also positively influence the course of illness. • Is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications. (Ferris et al., 2002, p. 17-18) x Hospice Palliative Care: Canadian Hospice Palliative Care Association (CHPCA) Model Illness trajectory • More predictable in cancer and ALS • Less predictable in AIDS, lung & heart diseases End of Life Care Terminal Phase Therapy to cure or control disease Palliative Care Approach Diagnosis made of life-limiting illness Bereavement Care Death Illness Trajectory Pereira, J.L. & Associates. (2008). Reprinted with permission. This diagram illustrates how the illness trajectory may be more predictable in some illnesses (e.g. advanced cancer) than in others (AIDS, end-stage heart, or end-stage lung disease). These unpredictable trajectories are often characterized by gradual deterioration combined with acute crises or episodes during which the individual appears to be in the terminal phase, only to rebound again. There is risk in assuming that an acute episode is a terminal event. How Was the Handbook Developed? This 4th national edition was published in 2013 by the Edmonton Zone Palliative Care Program, Alberta Health Services, following a review by hospice palliative care (HPC) professionals from across Canada. Heavily revised in 2006 by experienced HPC clinicians from across Canada, the 3rd edition was published by the former Capital Health’s Regional Palliative Care Program in collaboration with The Pallium Project and the Canadian Hospice Palliative Care Association (CHPCA). The book is part of a joint commitment to ensure HPC is current and well-integrated within Canada’s primary health care renewal efforts. A national review was undertaken to ensure the handbook continued to reflect the diversity of safe, ethical, and effective HPC practices across Canada. Experienced HPC practitioners from various primary, secondary and tertiary practice settings across Canada reviewed the 3rd edition, through a structured review process to validate the appropriateness and evidence of existing questions, identify xi additional questions, and identify additional or new evidencebased interventions or practices. Questions and appendices with similiar themes were organized into 11 groups of 5-10 questions. Each group of questions was assigned to 2 or 3 reviewers from different provinces. Revisions were made to the handbook based on suggestions from the national review process. Subsequently, an editorial committee reviewed and integrated the revisions into the handbook while considering the national commitment to align practices with the principles and norms outlined in the CHPCA Model to Guide Hospice Palliative Care and the Canadian HPC Nursing Standards of Practice. The Canadian Hospice Palliative Care Nursing Standards of Practice define the standard of nursing care expected by all those who are living with, and dying from an advanced illness; establish requisite knowledge for the nursing care of persons and families with advanced illness; and support on-going development of hospice palliative care nursing. The 2009 Canadian HPC nursing standards, aligned with the Ferris et al. (2002) CHPCA Model to Guide Hospice Palliative Care, are: 1) Quality of Living-Dying, 2) Comfort, 3) Transitions, 4) Quality and Safety, 5) Leadership, and 6) Personal and Professional Growth. What is the Scope of the Handbook? The handbook is intended as a “field guide” for the general practice nurse and not as a textbook on palliative care nursing. It can be read from cover to cover or it may be used as a resource to answer a particular question. The handbook has limited the explanations for each question in order to keep it compact and “user friendly.” Key references are included following each topic for readers who are seeking more complete knowledge of a specific subject. A list of books that have a general focus as well as pertinent web sites can be found at the end of the handbook. Some information has been organized under the headings of Nursing Alert or Clinical Tip. Nursing Alert Information found under the heading Nursing Alert is extremely important and needs to be considered prior to providing care. xii Clinical Tip Information found under the heading Clinical Tip assists with the implementation of care. The handbook contains guidelines and general suggestions for treatment and care that must be individualized to the specific person and family. Suggested drugs and drug doses have been reviewed by hospice palliative care physicians and pharmacists. Information is provided about the maximum daily dose for the drugs that have a definite maximum dose. However, drugs such as opioids do not have a specific maximum dose and should be titrated to best analgesia with the fewest side effects. The drugs and drug doses were included in this handbook to assist nurses when consulting with the primary-care or attending physician about symptom management. When possible, the interventions in this handbook are evidencebased, but at times, the interventions are based on best practice standards or protocols. Since some nursing practices vary between provinces and even sites, some of the interventions are only suggestions and it is recommended that a nurse follows the standard or protocol provided by the place of practice. The suggestions for care in this handbook can often be applied to people who are facing life-limiting illnesses other than cancer. The intention of this handbook is to serve as a resource for all nurses who provide palliative care regardless of diagnosis or practice setting. Content, particularly discussion of possible pharmacological interventions, is specific to an adult population, and if caring for a child, it is important to consult a pediatric specialist. Disclaimer Care has been taken in the preparation of the information provided. Nonetheless, any person seeking to apply or consult these guidelines is expected to use independent clinical judgment in the context of individual clinical circumstances, or seek out the supervision of a qualified clinician. Alberta Health Services and the parties for whom it is legally responsible, makes no representations or warranties about the accuracy, reliability, completeness, currency, or timeliness of this document and specifically disclaims any such representations and warranties. xiii This handbook is not a substitute for, and does not provide medical advice. The material contained herein is for educational and informational purposes only, and is not to be used for the direction of care of individual patients. It is general in nature and is not intended in any way to be a substitute for medical examination or professional medical or nursing advice, diagnosis or treatment. Always seek the advice of appropriately qualified and regulated health care providers with any questions you may have with regard to a specific medical condition that transcends your specific scope of regulated practice or professional competence. Never disregard or delay seeking consultative advice because of something you have read or viewed in the course of using this handbook. Medication Conventions For ease of reference, the convention which has been used throughout is to list the generic name of medications and give, as examples, common brand names used in Canada. You are advised to always verify the items discussed in this book against your approved local formulary. Funding Acknowledgement The Edmonton Zone Palliative Care Program, Alberta Health Services, provided the funding to publish the previous editions of the Handbook and recoups this cost from sales of the Handbook. In-kind support for this project was provided by the employers of the editors and reviewers. References Canadian Hospice Palliative Care Association (2013) What is hospice palliative care? Retrieved from http://www.chpca.net/Home CHPCA Nursing Standards Committee (2009). Canadian Hospice Palliative Care Nursing Standards of Practice. Ottawa, ON: Canadian Hospice Palliative Care Association. Retrieved from www.chpca.net Ferris, F.D., Balfour, H.M., Bowen, K., Farley, J., Hardwick, M., Lamontagne, C., Lundy, M., Syme, A., & West, P. (2002). A model to guide hospice palliative care. Ottawa, ON: Canadian Hospice Palliative Care Association. Retrieved from www.chpca.net Pereira, J.L. & Associates. (2008). The Pallium palliative pocketbook: a peer-reviewed referenced resource. 1st Cdn. ed., Edmonton, Canada. The Pallium Project. World Health Organization. (2013). WHO Definition of Palliative Care. Retrieved from www.who.int/cancer/palliative/definition/en/ xiv Contents The Authors................................................................................. iii Introduction................................................................................ ix Part I. Physical Symptoms............................................... 1 Pain............................................................................................... 2 1. What is pain? How is pain assessed?..................................2 2. What are the different causes and types of pain? ...........7 3. Why is a history of substance use relevant to pain assessment and management? How is it assessed?.........9 4. How is pain assessed in someone who is confused?.....10 5. Which opioids are preferred for use?...............................11 6. How should opioids be ordered?......................................14 7. What is breakthrough pain? How should breakthrough opioids be ordered? ..................................15 8. What is the maximum dose of an opioid?.......................16 9. What are the preferred routes for administration of opioids?............................................................................ 17 10. What are the potential side effects of an opioid?...........18 11. What is opioid neurotoxicity?............................................19 12. What are the interventions for opioid neurotoxicity?....21 13. How can excessive drowsiness with opioid use be decreased?............................................................................22 14. How are opioids used safely in persons with renal impairment?.........................................................................22 15. What are the causes of myoclonus?.................................23 16. Does unrelieved pain always require increasing the opioid dose? .................................................................23 17. Should opioids ever be withheld? ....................................24 18. Should placebos ever be administered?..........................25 19. What other medications are used in the management of pain?.........................................................25 20. What are the non-pharmacological interventions to control pain?....................................................................27 21. How can fears regarding addiction be managed?..........28 22. How is pain managed in persons with an addiction history?..................................................................................29 xv 23. What can be done when family members give or request opioids inappropriately? .....................................30 Anorexia and Cachexia............................................................. 33 24. What is cancer associated anorexia/cachexia syndrome (CACS)? What are the causes? .........................................33 25. How can appetite and oral intake be optimized?...........34 26. What can be done to assist persons and their families cope with reduced nutritional intake? ..............36 27. Is nutritional support beneficial?.......................................38 Constipation, Diarrhea and Bowel Obstruction............................................................... 41 28. What is constipation? How is it assessed? ......................41 29 What causes constipation? ................................................42 30. What are the complications of constipation?..................43 31. What are the interventions for constipation? .................44 32. How is diarrhea assessed? What are the causes?..........................................................47 33. What are the interventions for diarrhea?.........................48 34. What is bowel obstruction? What are the causes? .........................................................49 35. What are the signs and symptoms of bowel obstruction? How is it assessed?.......................................50 36. What are the interventions for bowel obstruction?........51 Dehydration............................................................................... 55 37. What is dehydration? How is dehydration assessed? ..........................................55 38. When is it beneficial to hydrate?.......................................55 39. When is it not beneficial to hydrate?................................56 40. Is hydration appropriate for a person who has edema?.................................................................................57 41. How can hydration be maintained?.................................57 Nausea and Vomiting................................................................ 59 42. What are nausea and vomiting? What are the causes?..........................................................59 43. How are nausea and vomiting assessed?........................60 44. What are the interventions to control nausea and vomiting?..............................................................................61 xvi Delirium...................................................................................... 65 45. What is delirium? What are the causes of delirium? .....65 46. How is delirium assessed? ................................................67 47. What are the interventions for delirium?.........................68 48. What are the interventions for supporting family when a person is delirious? ..............................................69 Dyspnea.......................................................................................71 49. What is dyspnea? What are the causes of dyspnea?.....................................71 50. How is dyspnea assessed?.................................................72 51. What are the interventions for dyspnea? ........................74 Edema, Ascites, and Lymphedema........................................... 77 52. What are edema, ascites, and lymphedema? What are the causes? .........................................................77 53. How are edema, ascites, and lymphedema assessed? .............................................................................78 54. What are the interventions for edema, ascites, and lymphedema?......................................................................79 Care of the Integument ............................................................ 82 55. Should bed-bound people be repositioned regularly?..............................................................................82 56. What is pruritis? What causes it? ......................................83 57. How is pruritis assessed? What are the interventions?...............................................84 58. What is a malignant wound? How is it assessed? .............................................................85 59. What are the interventions for a malignant wound?.....86 Oral Conditions.......................................................................... 88 60. What contributes to taste changes? What are the dietary interventions?.................................88 61. What are xerostomia (dry mouth) and stomatitis (sore mouth)? What are the causes? ...............................88 62. How are xerostomia and stomatitis assessed? What are the interventions?................................................................89 xvii Fatigue........................................................................................ 92 63. What is fatigue? What are the causes?.............................92 64 How is fatigue assessed? What are the interventions?...............................................92 Circulatory Conditions.............................................................. 94 65. What are the causes of hemorrhage? .............................94 66. What are the interventions for hemorrhage?..................95 67. What are thrombi and emboli? What are the causes? .........................................................97 68. How are thrombi and emboli assessed? What are the interventions?.........................................................97 Spinal Cord Compression......................................................... 99 69. What is spinal cord compression? What are the causes? How is it assessed? ......................99 70. What are the interventions for spinal cord compression? ...................................................................100 Superior Vena Cava Syndrome................................................101 71. What is superior vena cava syndrome? What are the causes? How is it assessed? ....................101 72. What are the interventions for superior vena cava syndrome?.......................................................102 Seizures ................................................................................... 103 73. What are seizures? What are the causes? How are seizures assessed? ............................................103 74. What are the interventions for seizures?.......................104 Alternative and Complementary Therapies.......................... 105 75. What are alternative and complementary therapies? What are the nursing responsibilities? .........105 Palliative Sedation....................................................................107 76. What is palliative sedation? What needs to be considered? ......................................................................107 xviii Part II. Psychosocial, Spiritual, Ethical, and Legal Issues....................................................................111 Family and Coping....................................................................112 77. What is helpful to know about the person’s family? ...112 78. What is coping? What are coping strategies? ..............113 79. Which persons may be at risk for coping poorly?........114 80. How can support be offered to family members?........114 81. How is loss of control expressed by persons and their families? How can they be assisted to maintain a sense of control?............................................116 Psychosocial..............................................................................117 82. What is anxiety? How does the person express anxiety? What are the interventions?............................. 117 83. How is depression expressed? What are the interventions?.............................................118 84. What interventions are used when dealing with anger?.................................................................................119 85. What are the interventions for supporting the person who is crying? ......................................................120 86. How is denial expressed? What are the interventions?.............................................120 87. What is a child’s understanding of death? .................... 121 88. How can children be prepared?......................................122 Spirituality and Hope.............................................................. 124 89. What are spirituality and religion? How are spirituality and religion assessed? .................................124 90. What interventions support the person’s spirituality and religion?......................................................................126 91. What is hope? How is it assessed? What are the interventions?.............................................127 Culture...................................................................................... 129 92. What is cultural competence? How is it applied to practice? ..........................................129 93. How does culture influence the dying process?........... 131 xix Euthanasia and Suicide........................................................... 132 94. What are euthanasia and assisted suicide? What are the nursing responsibilities?......................................132 95. What are the risk factors for suicide? What are the interventions? ............................................133 Goals of Care........................................................................... 134 96. What influences Goals of Care and Advanced Care Planning? ..........................................................................134 97. How are goals of care discussed? ..................................135 Organ and Tissue Donation.................................................... 136 98. Can an individual with terminal illness, advanced disease, or cancer donate? Is an open-casket funeral possible after organ and tissue donation?.......136 99. What is the health care professional’s role in organ and tissue donation?.............................................137 Last Days ................................................................................. 137 100. How can nurses prepare families for the last days of life?........................................................................137 101. What are the indicators of imminent death? ................138 102. What are the interventions in the last days of life?......139 Grief and Bereavement........................................................... 140 103. What is grief? What are the immediate interventions?.........................140 104. What are some interventions for bereavement follow-up? ..........................................................................141 Care for the Caregiver............................................................. 142 105. What strategies can a nurse take to reduce his or her stress?................................................................142 106. What might be warning signs of inappropriate boundaries? .......................................................................144 General References...................................................... 145 Appendix A. ESAS-r................................................................. 148 Appendix B. Faces Pain Scale – revised ............................... 152 Appendix C. CAGE Questionnaire.......................................... 154 Appendix D. Table of Equianalgesic Doses of Opioids ....... 157 Appendix E. Strategies for Energy Conservation ................. 159 xx Part I Physical Symptoms 1 Pain 1. What is pain? How is pain assessed? Pain is a subjective, multidimensional experience. Each person’s experience of pain is unique. The perception, expression and relief of pain are influenced by physical, psychological, social, cultural and spiritual factors. Conversely, the experience of pain will influence how a person functions within each of these dimensions. Therefore, a complete pain assessment and treatment plan must also be multidimensional. It is important to consider an interdisciplinary approach to pain assessment and management. Clinical Tip A systematic approach to questions for assessment and the use of tools such as the ESAS-r (Edmonton Symptom Assessment System–revised, see Appendix A) or Faces Pain Scale (see Appendix B) will facilitate communication and consistency in pain assessment. The following is just one example of a systematic approach to a pain assessment. Components of a Multidimensional Pain Assessment I. Identify pain characteristics through use of questions and physical exam. The acronym PQRSTU may facilitate a thorough, systematic assessment: P: Palliating and Provoking Factors • What makes the pain better or worse? • What brings on the pain? • Include physical exam to determine if pain produced or altered with palpation, movement or positioning (e.g. psychological, social, spiritual, environmental and/or cultural factors). • Include a multi-dimensional focus e.g. psychological, social, spiritual, environmental and/or cultural factors that make the pain better or worse e.g. pain worse at night when alone. 2 • Include medication and treatment history: – What medications are currently being taken for pain relief? – Was the medication used as prescribed? – What medications and treatments have been used in the past? – What other treatments are being/have been used for pain relief? – How effective have these medications and treatments been? Q – Quality • What does the pain feel like? (e.g. aching, stabbing, burning, numbness, tingling). • What would you have to do to me to make me feel the pain you are feeling? R – Radiating Pain • Does the pain move or travel anywhere? S – Site • Show me where you hurt. • Include a physical exam to help identify specific pain location. Clinical Tip Asking a person to show you, rather than tell you, where it hurts can reveal whether the pain is localized or diffuse, stationary or moving. This information can provide important clues as to the etiology of the pain that might be missed with a simple verbal response. Use a body diagram and have the person identify the location of each pain with either a letter or a number (See Appendix A). When people have more than one pain, it is important to conduct a comprehensive assessment of each pain separately, as well as the relationship between the different pains. 3 S – Severity • How much does it hurt? Clinical Tip Visual analogue scales (VAS), numerical scales (0-10), verbal rating scales or face scales can be used to provide valid measures of pain severity or intensity (See Appendix A and B). – Symptoms • Are there any symptoms that accompany the pain? (e.g. nausea, sweating) T – Timing • Onset: When did the pain start? • Duration: How long does the pain last? • Frequency: How often do you feel the pain? When are you in pain? Is the pain there all the time or does it come and go? – Tolerance • What amount of pain can you tolerate/live with? (use 0-10 scale) (See Appendix A) U – Impact on you • How has the pain affected your ability to function? • What do you believe is causing the pain? II. Further explore non-physical dimensions to see how these factors may influence and be influenced by the pain experience: Behavioural • What behaviours does the person exhibit when in pain? (e.g. rocking, pacing, guarding or withdrawing) • How does the person express pain? • Are there behaviours or actions that make the pain worse? 4 Clinical Tip Chronic pain may exist without any overt behavioural expression of pain. The reliance on visual inspection can lead to an underestimation of pain severity and possible poor pain control. Psychological • How does the person’s mood affect the pain? • How does the pain affect the mood? • Does the person feel angry, depressed and afraid or a combination of these? • How has the pain experience impacted the person’s self-image or self-esteem? • Is the person cognitively impaired or delirious? Use screening tools such as the Molloy Standardized Mini-Mental State Examination (SMMSE) or the Confusion Assessment Method (CAM). • Is the person experiencing major psychological distress? Look for total pain (See Question 2). • How has the person coped with pain and other stressors in the past? • Does the person have a history of drug or alcohol use? (See Appendix C) Social • • • • How does the pain influence the person’s daily living? How effective is the person’s social support network? What effect does significant others have on pain? How has the pain influenced the person’s relationships and roles at home and/or work? • What effect has the pain had on sexuality? • Are there financial concerns? Cultural • What are the cultural traditions, customs, beliefs and values that influence the expression, meaning and treatment of pain? 5 Spiritual • What is the meaning of pain to the person? • What does the person think is causing the pain? • How has the pain influenced the person’s hope, meaning and purpose in life? • Are there other spiritual issues affecting the pain experience? Environmental • How does the environment affect the person’s pain (e.g. loud noises, bright lights)? • What environmental conditions increase or decrease the person’s pain? When to Assess Pain • • • • On initial contact and at regular intervals, After report of a new pain, After change in existing pain, To evaluate pain interventions. Assess the intensity and impact of the person’s pain before the intervention and after the intervention has had sufficient time to take effect, noting any improvement (e.g. for most pain medications, effectiveness should be evaluated 20-30 minutes after administration). Similarly, assess pain within 24 hours of starting a new medication or new dose, to determine whether there is a sustainable effect. Nursing Alert Escalating back pain that radiates and increases with straight leg raise or banded pain around chest or torso may indicate spinal cord compression. It is important to perform a neurological assessment, including bladder and bowel function, as impairment in these may also indicate spinal cord compression (see Questions 69 and 70). Report immediately and take action so that permanent, irreversible damage from the compression can be minimized. 6 2. What are the different causes and types of pain? Almost all persons with a life-limiting illness will have several different factors contributing to their pain experience. In a person expressing a pain intensity of 8/10, the mechanism may be almost completely physical. In another person with the same pain rating, fear, depression or confusion may be responsible for the majority of the pain expression and therefore, analgesics may not result in improvement. It is important to assess the characteristics, treatment history and impact of each pain separately, as well as the relationship between the different pains. The pain experience is rarely, if ever, purely spiritual or physical or the result of a single factor in a single dimension. Physical Pain Syndromes I. Nociceptive Pain Pain caused by on-going activation of pain fibres by a noxious stimulus. Two sub-types: a) Somatic Pain (e.g. bone metastases, muscle or soft tissue damage). This is described as pain that is well-localized, gnawing, dull, boring, aching or occasionally cramping. It may be constant or intermittent. Pressing over the affected area elicits pain or makes it worse. It is also usually worse with movement. b) Visceral Pain (e.g. liver metastases, GI infection). This is described as a constant deep aching, squeezing or cramping pain that is usually poorly localized or diffuse. It can be referred (e.g. to sacral or perineal area). It is often associated with autonomic symptoms including sweating and pallor. II. Neuropathic Pain This type of pain is caused by the destruction, infiltration or compression of nerve tissue. Pain perception may continue in the absence of persistent noxious stimulus. There are 2 sub-types often differentiated by the characteristics used to describe them: 7 a) Dysesthetic or deafferent pain (e.g. peripheral vascular disease, peripheral neuropathy). This is a constant pain that occasionally radiates and is often characterized by heat, burning, numbness or tingling over the area. Light pressure from non-painful stimuli (e.g. clothing or light touch) can produce severe pain. b) Neuralgic pain (e.g. post-herpetic pain, sciatica). This is described as paroxysms of lancinating pain that can be sharp, shooting or electrical in nature that can follow nerve roots or dermatomes. Nociceptive and neuropathic pain may have different components that reflect the timing of the pain experience. • Baseline pain is described as a constant pain state experienced for greater than half the day. • Breakthrough pain is described as an intermittent flare of pain that exceeds the intensity of the baseline pain and “breaks through” the baseline analgesia. • Incident pain (subtype of breakthrough pain) is described as a severe transitory increase in pain of varying intensity that occurs suddenly in response to a trigger, such as toileting, repositioning, coughing, hiccups and/or dressing changes. Total Pain Refers to the multidimensional nature of pain, which includes the physical, psychological, social, and spiritual domains. This pain has a large psychosocial or spiritual component. Total pain is also known as total suffering or existential pain. Persons experiencing this type of pain often feel overwhelmed. They may not have the ability or insight to accurately describe the complex characteristics of their total pain experience and may perceive and/or express their suffering as physical pain. Consider total pain if: • Sgnificant psychosocial or spiritual issues are identified, • The person describes pain as all over, in absence of a physical cause for this pain, and/or • Escalating doses of analgesics produce toxicity with little or no pain relief. 8 Nursing Alert Involvement of the interdisciplinary team is essential in the assessment and management of the total pain experience. Psychosocial or spiritual interventions are often more effective than analgesics in these complex situations. 3. Why is a history of substance use relevant to pain assessment and management? How is it assessed? People with a history of substance use may: • Require higher doses of opioids to control pain and/or • Use opioids inappropriately as a means of coping with the psychosocial or spiritual distress inherent in their illness experience. The following signs indicate the likelihood of substance use or chemical coping: • Rapidly escalating doses of opioids with little or no pain relief and the development of toxicity (e.g. delirium, hallucinations, myoclonus), • Taking opioids for reasons other than pain control (e.g. to calm nerves or to sleep), • Losing prescriptions or medications, • Seeking opioids from multiple providers, • Failing to fulfill work, school or home obligations and/or • Experiencing legal problems with substances. Clinical Tip A history of alcohol use may be assessed using the CAGE Questionnaire (See Appendix C). A new version of the CAGE called the CAGE AID has been modified to screen for both alcohol and drug addiction; however, reliability and validity testing have not yet been completed. The caregiver should be sensitive and tactful when asking questions regarding the overuse of alcohol or prescription and illegal drugs. 9 For those persons who are in recovery from a substance use disorder/addiction, it may be challenging to get the person and/or family’s to agree to use opioids for pain due to fear of potentially developing another addiction. This would interfere with adherence to pain management treatment and the ability to optimize pain control. Reassure the person that pain control is achievable despite previous substance use through the development of an honest and trusting relationship with the health care team. Support the person’s efforts to participate in recovery efforts considering functional ability and interest (See Questions 21 and 22). 4. How is pain assessed in someone who is confused? In someone who is cognitively impaired, such as a person with dementia or delirium, it becomes even more challenging to assess pain. It may be helpful to confer with primary caregivers and family members to identify changes in behaviour. When assessing for pain in such situations, look for the following changes: • Vocalizations (e.g. crying or moaning). • Facial expression (e.g. furrowed brow or grimacing). • Body movements (e.g. tense body language, guarding behaviour, rocking or pacing). • Interpersonal interactions (e.g. aggression, resisting care or withdrawing). • Activity patterns or routines (e.g. changes in appetite, sleep or increased wandering). • Mental status (e.g. increasing confusion or irritability). • Agitation or restlessness (e.g. crawling out of bed or picking at the air). Statements such as “Show me where it hurts” are helpful as the ability to pinpoint the pain can be considered a confirmation of pain, especially if pathology is known. However, describing pain as “all over” or an inability to pinpoint the pain may mean the person is expressing general distress or some other discomfort. 10 Clinical Tip When unsure if a confused person is in pain, administer a trial dose of pain medication. If the problem is physical pain, the presumed pain behaviours should diminish. However, note that the sedative effect of the pain medication can also relieve agitation for a while. Inform the family of this possibility. If the person had no pain or the pain control was good before the onset of confusion, it is likely that the person’s agitation is not due to increased pain. Administer a trial dose of a neuroleptic (e.g. Haloperidol) and evaluate its effect. A decrease in agitated behaviours is an indication that they are more likely a result of delirium than pain (See Question 23). Nursing Alert Restlessness, agitation, moaning and/or grimacing can be an expression of delirium and not necessarily indicative of pain. Moaning may also be simply the sound of air moving through relaxed or weakened muscles of the vocal cords as the person breathes. Discuss this with family to alleviate their concerns. 5. Which opioids are preferred for use? Codeine, Fentanyl, Hydromorphone, Methadone, Morphine, Oxycodone, Sufentanil, and Tramadol are commonly used opioids. Opioids may be classified into weak and strong. “Weak” opioids, such as codeine and tramadol, have a ceiling effect, meaning that there is a maximum dose above which there is no further increase in analgesia. “Strong” opioids, such as morphine, hydromorphone, and oxycodone, are not subject to a ceiling effect and have no maximum dose. The opioids mentioned above are short acting formulations and are more appropriate for individuals who have not received opioids before (are opioid naïve) and/or have pain that is unstable. Because of their shorter half-life, short acting formulations allow for safer and more rapid titration. 11 Nursing Alert Some individuals lack the enzyme that converts Codeine to Morphine; therefore, Codeine is ineffective for pain control for these individuals. Long acting opioids should be considered when pain control is stable and minimal amounts of short-acting breakthrough medication are required. Long acting opioids include: Codeine Contin®, Hydromorph Contin®, Oxyneo, M Eslon®, and MS Contin®. These analgesics are usually administered every 12 hours. Do not administer more frequently than every 8 hours. Kadian® is a long acting Morphine that is given once every 24 hours. Methadone and Transdermal Fentanyl are opioids with a longer duration of action. Their half-life varies from one person to another as they are fat soluble. Methadone has to be titrated carefully under the guidance of a palliative care physician or pain specialist who is licensed to prescribe this medication. Methadone’s variability may result in an accumulation which is potentially toxic, even lethal. Methadone acts on the NMDA receptor and is used for the treatment of neuropathic and/or severe pain refractory to other opioids. Nursing Alert Long acting oral analgesics CANNOT be crushed or altered and MUST be swallowed intact. One exception is M Eslon® which is a capsule that can be opened and the contents sprinkled on soft food. Swallow the soft food (like pudding, yogurt, and applesauce) without chewing. Fentanyl is very short acting in one form (injectable/buccal) and very long acting in another form (transdermal). It is not a good choice for regular 4 hour or prn dosing. The transdermal Fentanyl patch is a long-acting controlled-release opioid preparation that offers a convenient, non-invasive method of delivering analgesia medication slowly into the bloodstream through the skin. Transdermal Fentanyl patches are indicated for persons who: • Are opioid tolerant for the management of chronic, persistent, 12 moderate to severe pain that requires continuous, around the clock opioid administration. • Are already receiving opioid therapy at a total daily dose of at least 45 mg of an oral Morphine equivalent per day. Transdermal Fentanyl is contraindicated in persons: • With acute, unstable or postoperative pain, as the dosage cannot be adjusted quickly. • With mild, intermittent or short duration pain. • Who are opioid-naïve. Over a period of 12 – 24 hours following application of a transdermal Fentanyl patch, a deposit of medication begins to accumulate in the intradermal layer of the skin. When initiating a Fentanyl patch, overlap it with the existing opioid for the first 12 hours. Medication will continue to be delivered via the intradermal reservoir 12–24 hours following patch removal. Transdermal Fentanyl products must be used with caution in elderly, cachectic or debilitated persons. Persons should be cautioned to avoid exposure to external heat sources when using a transdermal Fentanyl product. When selecting the site for application, choose a flat surface such as the upper chest, back, flank, upper arm or thigh where skin movement is limited. Select a new site different from the previous location to minimize changes in blood levels due to build-ups of subcutaneous deposits and skin discomfort. Do not apply the patch to broken, irritated or scarred skin, or to areas that have received treatment with radiation as this can affect drug absorption. Do not cut or damage the patch before applying. Wear gloves to prevent your hands from absorbing medication. Nursing Alert Merperidine (Demerol) should not be used for the following reasons: • It rapidly accumulates, potentially causing delirium and/or seizures, • Its duration of action is only 2 to 3 hours, necessitating more frequent administration and • Its active metabolites are more neurotoxic than the metabolites of other opioids. 13 6. How should opioids be ordered? Opioids may be ordered as needed (PRN) in situations where the pain is not severe or constant. Opioids for moderate to severe, constant pain (baseline) should be given on a fixed schedule around the clock (ATC). For people requiring ATC dosing, there should also be a provision for PRN opioids for breakthrough pain (See Question 7). A useful guideline is the “three rules of three”: 1. Greater than 3 PRN doses/24h – assess need for ATC administration. 2. Greater than 3 BTA (Breakthrough Analgesia)/24h – may need to increase ATC baseline dose. 3. Greater than 3 BTA in a row with little effect – immediate reassessment needed, contact a physician. When initiating ATC dosing, start with immediate release (shortacting) formulations to make dosage titration safe and effective. Avoid the use of a long acting opioid until the person’s opioid requirements are established. Nursing Alert The above rules do not apply to people with severe renal failure (See Question 14). If the person is requiring ATC opioids for adequate pain control, it is important to awaken the person for every scheduled dose to maintain a therapeutic level of analgesia in the bloodstream. However, if the person feels it is very important to have an uninterrupted night’s sleep, he or she may try any of the following, with a physician’s order. • Double the ATC short acting bedtime dose and omit the duringthe-night dose; then resume with the regular early morning dose. • Omit the during-the-night dose and resume with the regular early morning dose. • Take either the ATC short acting or breakthrough dose whenever he or she wakes up during the night. 14 Remember: Most people only need to use ATC short acting opioids for a short time period. Once the pain management is stable and no dosage change has been needed for at least 4-7 days, the opioid can be switched to a long acting preparation, eliminating the need to wake up during the night for regular dosages. 7. What is breakthrough pain? How should breakthrough opioids be ordered? Breakthrough pain is a flare of pain that exceeds the intensity of the baseline pain and “breaks through” the analgesia provided by ATC analgesics. Breakthrough analgesia (BTA) is medication used to relieve this type of pain. In general: • BTA should be the same opioid as the ATC (an exception is Transdermal Fentanyl). • BTA is ordered at 10%-15% of the person’s total 24 hour dose, every hour as needed, or 50% of a single ATC dose every hour as needed when a short acting opioid is being used. • BTA should be given when needed regardless of when the next regular dose is due. Incident pain is a distinct type of breakthrough pain. It is pain that directly results from an action or activity. Incident pain can be experienced by persons with bone metastases, rib fractures or myofascial involvement of a tumour. Circumstances in which incident pain can occur include repositioning, bathing or changing clothes, transfers, wound management, catheterization or disimpaction, and ambulation. Management of incident pain requires the use of a short-acting opioid, which can be administered by oral, subcutaneous, sublingual, or bucal routes. The oral route may take up to 30 minutes to reach effect. The other routes result in quicker analgesia. Fentanyl or Sufentanil can be administered sublingually 10-15 minutes prior to the activity. These injectable formulations are administered via the transmucosal route due to rapid absorption through the mucous membranes. The onset of action is about 5-6 minutes and the duration of analgesia 20-30 minutes. Use caution with Fentanyl and Sufentanil preparations as they are extremely potent opioids. Fentanyl is approximately 100 times more potent than Morphine and Sufentanil is 1000 times more potent than Morphine. 15 Nursing Alert Timing of the ATC analgesic dose should never be changed due to administration of a BTA (e.g. if BTA was administered at 1330 and the next ATC dose is due at 1400), the ATC dose remains due at 1400. 8. What is the maximum dose of an opioid? “Weak” opioids (e.g. codeine and tramadol) have a ceiling dose, which means the analgesic effect of the drug does not continue as the dose is increased. Other drugs, such Tylenol # 3®, Percocet®, and Percodan® have a maximum dose due to the addition of acetaminophen and acetylsalicylic acid, which have a daily dose limit. “Strong” opioids such as Morphine, Hydromorphone, Oxycodone, Fentanyl, and Methadone are not subject to a ceiling effect and have no maximum dose. Treatment with opioids involves a balance between sufficient analgesia and the typical side effects (see Question 10). Side effects such as sedation and nausea diminish over time because of tolerance. Constipation may be prophylactically treated with good results. Opioid toxicity causing delirium can be easily missed. A comprehensive assessment and ongoing reassessment of cognitive function is therefore important (see Questions 45–48). Nursing Alert If opioids are started at low doses and increased slowly, there is less risk of respiratory depression and delirium. 16 9. What are the preferred routes for administration of opioids? The oral route is the preferred route for the following reasons: • It is the most natural and non-invasive. • It can be self-administered. • It has a variety of formulations. • It is the most cost effective. The transmucosal route (e.g. sublingual, buccal or intranasal), is useful when managing incident pain because this route allows for rapid absorption. It is important to use small amounts, so that the medication can be absorbed through the mucosa. Usually a volume of less than 1 mL is recommended. If the medication volume is larger than 1 mL, then administer the medication about 5–10 minutes apart in order to allow for proper absorption. Examples of medications administered using this route are Fentanyl and Sufentanil. It is often anticipated at end of life (or with any condition that impacts swallowing) that the oral or transmucosal route may no longer be possible. When this occurs, other routes should be considered. The subcutaneous (subcut) route is the preferred parenteral route. This route can be used, through a hypodermoclysis site, to give medication or hydration. The intravenous (IV) route is an acceptable route if there is an established IV site or central venous access or if rapid administration of fluids is required. It can be uncomfortable, reduces the person’s independence, is no more effective than the subcutaneous route, and is associated with more complications. The transdermal route is non-invasive and convenient. A transdermal patch (e.g. Transdermal Fentanyl, also known as a Duragesic Patch) slowly releases the drug beneath the skin into the subcutaneous tissue where it enters the circulation over the course of 3 days. This option is only suitable for persons whose pain is well controlled with a stable dose of an opioid and whose previous opioid needs were the equivalent of at least 45mg of oral Morphine per day. The rectal route is safe, inexpensive and effective, but its absorption can be variable. It is not suitable for people with anal or rectal 17 lesions, constipation, diarrhea, or severe thrombocytopenia. This route may not be acceptable for some people. The intramuscular route should not be used in the palliative setting as it causes unnecessary discomfort and absorption is erratic. The spinal route (e.g. epidural or intrathecal) is the most invasive route and is commonly reserved for severe intractable pain or when systemic opioids are causing unacceptable side effects. The use of this route may impact the ability for people to be cared for outside a tertiary centre. Nursing Alert When converting opioids from one route to another, it is important to recognize that potency is not equivalent (e.g. Morphine 10mg oral or rectal = Morphine 5mg parenteral). (See Appendix D). 10. What are the potential side effects of an opioid? One or more of the following side effects may be experienced by persons on initiation, titration, or rotation of an opioid. Common Side Effects • Constipation occurs in almost 100% of persons; therefore, a regular bowel regime is essential (See Question 31). • Nausea may be prevalent for the first the 2–3 days but usually resolves within 24-72 hours. Nausea that persists requires medical management (See Question 44). • Somnolence may be present for the first 2-4 days but usually resolves with continual use of an opioid. (For persistent somnolence or drowsiness, see Question 13). • Xerostomia (Dry mouth) is common and occurs with variable intensity (See Question 62). 18 Less Common Side Effects • Pruritis (Itchiness) is less common with the administration of oral and parenteral opioids and more common with the administration of epidural and spinal opioids (See Question 57). • Urinary retention is most common with spinal opioids and in persons with prostatism or urethral stricture. • Neurotoxicity (See Question 12). Rare Side Effects • Respiratory depression can occur if the initial dose is too high, doses are increased too rapidly, long-acting opioids have been inappropriately used as breakthrough medication, and/or there has been incautious use of multiple opioids at the same time. Persons and their families should be taught about the possibility of opioid side effects and advised to alert a health care professional immediately if any such effects are experienced. Nursing Alert Older adults may experience a prolongation of side effects and increased sensitivity due to their decreased metabolism and excretion of medications. A good rule for using opioids is to ‘start low and go slow’. 11. What is opioid neurotoxicity? Opioid neurotoxicity or opioid toxicity is hyperexcitation of the nervous system secondary to the accumulation of active opioid metabolites (by-products of drug breakdown in the liver). The risk of opioid metabolite accumulation and subsequent opioid neurotoxicity is increased in persons with renal impairment. This risk seems to be highest with Morphine, Codeine and Oxycodone and seems lowest with the use of Hydromorphone, Fentanyl and Methadone. 19 Factors that place persons at higher risk of developing opioid neurotoxicity include: • Being frail and/or elderly, • Impaired renal and/or hepatic function, • Rapid dose escalation, • Use of the same opioid for a prolonged period of time, and/or • Dehydration. Manifestations of opioid neurotoxicity include: • Nightmares or vivid dreams causing distress, that may progress to visual or tactile hallucinations, and less commonly, auditory hallucinations. Nursing Alert People experiencing hallucinations may withhold this information as they are often afraid that they are “losing their minds”. It is important to normalize the experience and ask direct questions. If pain is described as all over and accompanied by myoclonus and hallucinations, suspect that opioid metabolite accumulation is occurring. • Myoclonus is bilateral jerking or seizure-like activity of limbs or facial muscles which can progress to seizures if not treated. • Hyperalgesia and allodynia are increased pain responses to a mildly painful stimulus (hyperalgesia) or pain perceived after a stimulus that would not normally cause pain (allodynia) such as a light touch, or being covered with clothing or bed linen. • Delirium is an alteration in cognitive functioning that has a sudden onset and includes fluctuating disturbances in one’s level of consciousness, attention, perception, psychomotor behaviour and/or emotional state (See Questions 45-48). 20 12. What are the interventions for opioid neurotoxicity? • Hydration helps to maintain kidney function and flush the opioid metabolites out of the system. • Opioid rotation, as different opioids produce different metabolites. By rotating or switching from one opioid to another, the body is able to eliminate the offending metabolites that are causing neurotoxic side effects. Nursing Alert When switching from one opioid to another, beware of incomplete cross tolerance. With extended use, people may build up tolerance to the effects of one opioid, requiring increasing dosages to achieve the same analgesic effect. When switching to another opioid, this same level of tolerance will not exist; therefore, the same analgesic effect can usually be maintained using a 20-30% decrease in the dose of the new opioid. If the pain is wellcontrolled prior to the rotation, the dose reduction would be higher than if the pain is poorly controlled, in which case the reduction would be lower in order to gain more analgesic effect. A neuroleptic (e.g. Haloperidol), may be used to control hallucinations, nightmares or agitated behaviour until the offending metabolites are eliminated. Counsel the family regarding the nature of the condition and provide support during this distressing experience. Reassure them that 24–48 hours is usually required for reversal of opioid toxicity symptoms. Non-pharmacologic measures include providing structure and routine, a quiet room, a visible clock and calendar, simple explanations, a calm, respectful attitude, and familiar objects and people. 21 13. How can excessive drowsiness with opioid use be decreased? Minor sedation may be experienced by most persons when opioids are initiated or a dose is increased. Education and reassurance are required as this symptom will usually clear within a few days. If the drowsiness continues for longer than 2-4 days and the person is in good pain control, dose reduction can be trialed. If the current dose of an opioid or a higher dose is required to achieve optimal pain relief, a psychostimulant to relieve day time somnolence could be trialed. However, drowsiness could be due to other medication(s) such as antidepressants, tranquilizers and antiemetics and/or metabolic disturbances such as hypercalcemia. Similarly, end stage disease can also contribute to drowsiness. 14. How are opioids used safely in persons with renal impairment? Opioids and their metabolites are excreted via the kidneys. In the presence of renal impairment, the administration of opioids and accumulation of their metabolites may result in neurotoxic side effects (See Question 11). The risk of opioid neurotoxicity can be reduced by: • Early recognition of renal impairment, • Gradually decreasing the opioid dose as renal failure occurs and/or progresses, • Administering opioids less frequently (e.g. every 6-8 hours ATC instead of every 4 hours) or administering PRN doses only and/ or • Using short acting formulations only. When there is renal impairment, opioid reduction usually does not result in a pain increase because opioids are retained in the body longer and some opioid metabolites have analgesic properties. Opioid reduction may not be necessary if the person has no undue side effects. The decision to alter the opioid dose depends on the goals of care and stage in the illness trajectory. 22 Nursing Alert In persons with renal impairment, the risk of opioid neurotoxicity seems to be lowest with the use of Fentanyl (due to rapid metabolism and excretion), Methadone (due to minimal active metabolites and fecal elimination) and Hydromorphone. The risk seems to be highest with the use of Morphine and Codeine, as well as with slow-release opioids, due to prolonged clearance times. 15. What are the causes of myoclonus? Myoclonus is often associated with opioid metabolite accumulation, but can also be caused by the following: • Other medications with neurotoxic side effects (e.g. neuroleptics, anti-depressants or NSAIDs), • Some neurological disorders, • Infection and/or • Metabolic disorders. The occasional myoclonic jerk, especially when sleeping, is common even in healthy persons. 16. Does unrelieved pain always require increasing the opioid dose? The experience of pain is multi-factorial, and the person may respond to interventions other than dose increases. Pain assessments must be done regularly, as the pain mechanism (nociceptive or neuropathic), pain sites, and acuity may change with disease progression. Adjuvant medication, radiation therapy, and surgery are other options that may be required to achieve pain control. “Total pain”, where psychological, social and spiritual suffering is expressed as pain, must be considered in order to address underlying issues. 23 Unrelieved or escalating pain with increased opioid use is a “red flag” for opioid toxicity. Increasing the opioid dosage in this situation may exacerbate the pain and other symptoms caused by opioid metabolite accumulation. Opioid rotation, rather than opioid dose increase, would be appropriate in this case. Depending on the type of pain and the factors influencing the pain experience, the pain may respond better to: • The addition of an adjuvant, • A non-pharmacological intervention and/or • An alternate route of medication delivery. Nursing Alert It is important to recognize that unrelieved or escalating pain may be caused by an accumulation of opioid metabolites. Paradoxically, an increase in the opioid dosage in this situation may exacerbate the pain or the person’s perception of pain, rather than relieve it. This is known as opioid neurotoxicity, which requires urgent medical treatment (See Question 11). 17. Should opioids ever be withheld? Yes, in certain situations. Doses may need to be withheld temporarily when there is evidence of severe side effects such as abrupt onset of decreased level of consciousness, marked sedation, respiratory depression (less than 8 breaths per minute) and/or pinpoint pupils (miosis). This can occur when the dose of an opioid is rapidly escalated. Regular doses should continue to be held until these side effects are reversed. Nursing Alert Respiratory depression and neurotoxic manifestations may result from other centrally acting drugs and many other causes (e.g. brain tumour). Nursing Alert If a person receiving oral opioids is required to be NPO for a procedure, it is important to administer the opioid using a different route at an equivalent dose. 24 18. Should placebos ever be administered? No. This approach to pain management is destructive to the caregiver-person relationship, proves nothing about the reality of the pain, and should not be used. If you suspect there may be a psychosocial or spiritual component to the pain, honest discussion and counselling is the most effective approach. If a physiological cause for the pain cannot be found and/or the pain is not relieved by opioids, do not assume that the pain is purely psychosocial or spiritual in origin. Pain is rarely one-dimensional. 19. What other medications are used in the management of pain? Adjuvants are medications that are not primarily indicated for pain control but may provide analgesic effects in some painful conditions. Some adjuvants may also potentiate the effect of an opioid. Adjuvants include the following: • Anticonvulsants for neuropathic pains (e.g. Gabapentin 100–300mg PO 3-4 times daily titrating up to the most effective analgesia or intolerable side effects, maximum dose 3600mg in 24 hours). • Bisphosphonates for control of bone pain (e.g. Clodronate 1500mg IV/subcut, Pamidronate 60-90mg IV or Zoledronate 4-8mg IV as single doses). These drugs may be repeated every 2-6 weeks depending on the medication and effect. • Chemotherapy agents for control of pain through reduction of tumour bulk. • Corticosteroids for lymphatic obstruction, cerebral edema, cord compression, bowel obstruction, bone pain and liver capsular pain (e.g. Dexamethasone 4-16 mg PO/subcut per day in one single daily dose or divided doses). Nursing Alert Corticosteroids have the potential to cause night time insomnia; therefore, divided doses should not be administered later than 1600 hours. After therapeutic effect is achieved, gradually taper to lowest effective dose. 25 • Muscle relaxants and antispasmodics for control of pain related to skeletal muscle spasm (e.g. Baclofen 5mg PO 2 to 3 times daily) and smooth muscle spasm (e.g. Hyoscine Butylbromide [Buscopan ®] 10mg PO/subcut as needed every 4 hours). • Non-steroidal anti-inflammatory drugs (NSAID) have a limited role in the control of bone pain and should be used with caution or avoided in persons with renal failure, known history of gastrointestinal ulcers and/or cardiac history (e.g. Diclofenac 50mg PO 3 times daily, with a maximum dose of 150mg PO in 24 hours, Naproxen 250-500mg PO twice daily, with a maximum dose of 1000mg in 24 hours). • NMDA antagonists used for neuropathic pain, especially in those with a hyperalgesic component (e.g. Ketamine 0.5mg/ kg IV per day in 3 divided doses). Due to the potential for significant psychotic effects, Ketamine should be initiated and titrated under guidance of a palliative care physician or pain specialist. • Topical local anesthetics used for control of some forms of dysesthetic neuropathic pain such as post-herpetic neuralgia (e.g. EMLA cream for topical use) or pain from stomatitis (e.g. Viscous Lidocaine for mucous membranes). • Tricyclic antidepressants (e.g. Amitriptyline or Nortriptyline 10–25mg PO at bedtime titrating up to a maximum daily dose of 150mg in 24 hours). • Epidural or spinal anesthetic usually administered in conjunction with an opioid for selected persons with difficult to control pain (e.g. Bupivicaine). It is also important to optimize the disease-specific drugs related to the management of non-malignant pain in end-stage chronic illnesses (e.g. optimize cardiac drugs such as diuretics, ACE inhibitors, beta blockers, vasodilators and Nitroglycerine in individuals with end-stage heart failure). Nursing Alert Benzodiazepines (e.g. Lorazepam) have no analgesic properties and are extremely sedating. These drugs have been implicated as one of the most common causes of falls in acute care settings. 26 Clinical Tip Reinforce safe medication practices such as keeping medication out of children’s reach and emphasize that medications are prescribed for a particular person and are not intended for use by others. For safety, the person should exercise discretion with whom information is disclosed regarding their opioids. Also consider safe disposal for patches as they may continue to hold active ingredients. 20. What are the non-pharmacological interventions to control pain? Cognitive strategies that may facilitate relief of pain include distraction, diversion and education. Expressive supportive therapy can be a powerful tool especially for people who have a large psychosocial or spiritual component to their pain. Allow persons to express their feelings (e.g. fear or anger). Emotive and/or spiritual interventions that can improve pain control include humor, art, music, religious rituals (e.g. prayer), acts of forgiveness, reconciliation, and reminiscence. Environmental factors may play a significant role in pain management. Ask the person what helps. Dimmed lights, soft music, a quiet room, and presence of others may reduce the experience of pain. Complementary therapies are especially useful for people who have high locus of control and are comfortable with these therapies. People who wish to use complementary therapies are encouraged to discuss their choices with the health care team to avoid unintended or harmful interactions with medical treatments. Therapies may include herbs, Reiki, therapeutic touch, meditation, hypnosis, imagery, and acupuncture. Occupational and physical therapy pain control techniques include transcutaneous electronic nerve stimulation (TENS), massage or relaxation therapy, supports (e.g. collars, brace and slings) and heat and/or cold application. 27 Palliative radiotherapy is used for control of bone pain and other types of pain caused by tumour infiltration. Radiotherapy can provide relief from bone pain in up to 70% of recipients, with the full benefit often not realized for up to 10-14 days following treatment. Radiotherapy may be provided as a single large dose or multiple fractionated doses. Orthopedic procedures such as internal fixation of an actual or impending pathologic fracture or spinal instrumentation for deteriorating vertebrae can significantly improve pain relief and function. Surgical resection is used for removal of painful bulky tumours and to relieve obstructions. Neurolytic procedures are used for interruption of the transmission of pain signals when other interventions have proven ineffective (e.g. celiac plexus block for pain related to pancreatic cancer). Clinical Tip The Interdisciplinary Team including the person and family play an important role in developing individual pain management strategies. Remember to involve other disciplines in the plan of care and to include strategies identified by the person and family. 21. How can fears regarding addiction be managed? Addiction is not the same as physical dependence or opioid tolerance. Reassure the person that as long as the medication is taken to relieve physical pain and not to experience its psychological effects, he or she is not addicted. Problems occur if the opioid is taken to experience its psychological effects (e.g. to relieve anxiety, or to address emotional and/or spiritual pain). Assess and address the person’s and family’s fears regarding addiction. The differences between physical dependence, addiction and tolerance are as follows: • Physical dependence is a normal physiological response to chronic opioid use. The body adapts to the presence of the opioid and the person experiences withdrawal symptoms if the 28 opioid is suddenly stopped or an antagonist such as Naloxone is administered. • Addiction (psychological dependence) is a pathologic psychological condition that includes a compulsion to take a specific drug to experience its psychic effects (e.g. euphoria, feeling of being high or spaced out). • Tolerance is a normal physiological phenomenon in which larger doses of an opioid are required over time to maintain the same level of analgesia. 22. How is pain managed in persons with an addiction history? Follow all the basic principles of opioid therapy as already outlined (See Question 5-13). Discuss the addiction history in an open, honest and non-judgmental manner. Commit to working together to control the pain. Expect that the person may require higher dosages of opioid to control the pain given the possibility of tolerance. Monitor carefully for signs that the person may be using the opioid to cope with problems other than the pain (See Question 3). Reassure the person that addiction is rarely an issue when opioids are used for the reason they are prescribed. Consider developing and signing a therapeutic agreement with the person, wherein the person agrees to: • Take opioids only for relief of physical pain not to “get high”, to sleep or to calm nerves, • Adhere to prescribed dosage and frequency, • Obtain opioids from a single provider • Refrain from sharing or selling opioids, • Recognize that lost prescriptions or medications will not be replaced. If the person is at home, recommend short dispensing intervals so that the person does not have large quantities of opioids in their possession at any given time. Provide information about and facilitate connection with appropriate counselling and support personnel. Teach the person and family how to use assessment tools (See Appendix A and B) and encourage them to monitor the intensity of pain and the use of BTA. 29 23. What can be done when family members give or request opioids inappropriately? A life-limiting illness affects the family as well as the person. It is therefore important to develop a therapeutic relationship with the family so that you can communicate and understand their perspectives. Nursing Alert Family members may give or request pain medication because they misinterpret the ill person’s behaviour as pain. This is more common when the ill person is unable to clearly express his or her needs. Should this scenario occur, ask the family what they are seeing that leads them to believe the person is having pain and explain what you are seeing that leads you to think differently. Explain to the family that: • Moaning, grimacing, restlessness and agitation may indicate delirium rather than pain. Delirium may actually be worsened, rather than be relieved, by the administration of opioids. • Moaning may simply be air moving over vocal cords as they relax. • Opioid toxicity may lead to significant discomfort (e.g. hallucinations, agitated delirium, myoclonus and/or hyperalgesia). • Ask family members to record medication administration and to note the events around the administration. • Teach family members non-pharmacological means to comfort the ill person (e.g. relaxation, massage, touch or music). Acknowledge the emotional pain experienced by the family and commend them on their efforts to comfort the ill person. It is important to involve other team members to include the family and offer support to address their emotional pain. Family members often feel powerless and helpless in the face of advancing disease and can feel more empowered through the provision of interdisciplinary support. 30 References Altilio, T. (2004). Pain and symptom management: An essential role for social workers. In J. Berzoff & P. Silverman (Eds.), Living with dying (pp. 380-408). New York: Columbia University Press. Black, F., Wilde, J., & Downing, G.M. (2006) Pain – Principles and titration. In G. M. Downing, and W. Wainwright (Eds.). Medical care of the dying (4th ed.) (pp. 159-188). Victoria Hospice Society Learning for Palliative Care. Dean, M. (2004). Opioids in renal failure and dialysis patients. Journal of Pain and Symptom Management, 28(5), 497-504. Ferro, C., Chambers, J., & Davison, S. (2004). Management of pain in renal failure. In E. Chambers, M. Germain, & E. Brown (Eds.), Supportive Care for the Renal Person (pp. 103-113). New York, NY: Oxford University Press. Good, P., Jackson, K., Brumley, D., & Ashby, M. (2009). Intranasal Sufentanil for cancer-associated breakthrough pain. Palliative Medicine, 23, 54-58. Harlos, M. (2002). Palliative care incident pain and incident dyspnea protocol. Retrieved from http://palliative.info/Incident Pain Herr, K. A., Spratt, K., Mobily, P .R., & Richardson, G. (2004). Pain intensity assessment in older adults: Use of experimental pain to compare psychometric properties and usability of selected pain scales with younger adults. Clinical Journal of Pain, 20(4), 207-219. Janssen-Ortho Inc. (2009). Product monograph: Duragesic. Retrieved from http://www.janssen-ortho.com/JOI/pdf_files/ Duragesic_E.pdf Jovey, R. (2002). Managing pain: The Canadian healthcare professional’s reference. Toronto, ON: Healthcare & Financial Publishing, Rogers Media. Librach, S. L., & Squires, B. P. (2001). The pain manual: Principles and issues in cancer pain and management (5th ed.). Montreal: Pegasus Healthcare International in association with Canadian Cancer Society/CANO. Molony, S., Kobayash, M., Holleran, E., & Mezey, M. (2005). Assessing pain as a fifth vital sign in long-term care facilities: Recommendations from the field. Journal of Gerontological Nursing, 31(3), 16-25. 31 Muijsers, R. B. R., & Wagstaff, A. J. (2001). Transdermal Fentanyl: An updated review of its pharmacological properties and therapeutic efficacy in chronic cancer pain control. Drugs, 61(15), 2289-2307. National Opioid Use Guideline Group. (2010). Canadian guideline for safe and effective use of opioids for chronic no-cancer pain. Retrieved from http://nationalpaincenter.mcmcaster.ca/opioid/ Pereira, J. L. & Associates. (2008). The Pallium palliative pocketbook: A peer-reviewed, referenced resource. (1st Cdn. Ed.) Edmonton, Canada: The Pallium Project. Pereira, J., Lawlor, P., Vigano, A., Dorgan, M., & Bruera, E. (2001). Equianalgesic dose ratios for opioids: A critical review and proposal for long-term dosing. Journal of Pain and Symptom Management, 22, 672-687. Reisfield, G. M., Paulian, G. D., & Wilson, G. R. (2009, Aug 31). #127 Substance use disorders in the palliative care patient, (2nd ed.) Medical College of Wisconsin. Retrieved from http://www.eperc.mcw.edu/fastFact/ff_127.htm Rhiner, M., Palos, G., & Termini, M. (2004). Managing breakthrough pain: A clinical review with three case studies using oral transmucosal Fentanyl citrate. Clinical Journal of Oncology Nursing, 8(5), 507-512. Sager, G. (2012). Pain assessment and management. In D. Oneschuk, N. Hagen & N. MacDonald (Eds.), Palliative Medicine: A Cased-Based Manual (pp 27-49). Oxford: Oxford University Press. Sargent, C. (2002). Naloxone: How well do you know this drug? Clinical Journal of Oncology Nursing, 6(1), 1-2. Schlisio, B. (2010). Profiles, Doses, and Side Effects of Drugs Used in Pain Management. Pain. In Kopf, A., & Patel, N. (Eds.), Guide to Pain Management in Low-Resource Settings (pp.351-358). Seattle: IASP. Schofield, P. (2010). ‘It’s your age’: The assessment and management of pain in older adults. Continuing Education in Anaesthesia, Critical Care & Pain 10(3), 93-95. Thai, V., & Fainsinger, R.L. (2011). Pain. In L.L. Emanuel & S.L. Librach (Ed.), Palliative care: Core skills and clinical competencies (2nd ed.) (pp.95-114). St. Louis, Missouri: Saunders. 32 Anorexia and Cachexia 24. What is cancer associated anorexia/cachexia syndrome (CACS)? What are the causes? CACS is a hypercatabolic state. Anorexia (loss of appetite) and cachexia (loss of weight and catabolism of adipose tissue and skeletal muscle) will occur in 80-90% of people with advanced cancer. Anorexia cachexia occurs in many other non-cancers advanced illnesses. These problems are often accompanied by asthenia, a constellation of symptoms including severe lethargy, generalized weakness, decreased immune response and profound fatigue. The syndrome may also include chronic nausea. Causes Primary anorexia and cachexia is a result of three processes that prevent normal metabolism of nutrients and is associated with an altered inflammatory state: • Complex metabolic alterations resulting in muscle wasting and loss of fat. • Neuroendocrine alterations resulting in loss of appetite, early satiety, and chronic nausea. • Metabolic modifications resulting in decreased muscle building and asthenia. There are three types of secondary anorexia and cachexia: 1. Starvation or malnutrition caused by: – Decreased oral intake secondary to a number of factors, – Impaired GI absorption (e.g. malabsorption, exocrine pancreatic insufficiency and/or chronic severe diarrhea), – Loss of proteins through body fluids (e.g. frequent drainage of ascites or pleural fluid and nephritic syndrome). 2. Catabolic states unrelated to cancer (e.g. infections or chronic heart failure). 3. Loss of muscle in the absence of cachexia and wasting due to decreased muscle activity secondary to limited mobility. 33 Decreased oral intake can be due to stomatitis, taste alterations, zinc deficiency, dry mouth, dehydration, dysphagia, severe constipation, bowel obstruction, vomiting, severe pain, severe dyspnea, depression, cognitive impairment, social or financial obstacles, and anxiety. 25. How can appetite and oral intake be optimized? Managing early satiety is important because after eating a small amount, a person may feel full and/or nauseated, and may vomit food that was eaten several hours earlier. Early satiety often results from gastric stasis (delayed emptying of the stomach) and/or slowed peristalsis. Specific causes of gastric stasis include medications, autonomic dysfunction, hepatomegaly, tumour of upper gastrointestinal tract, or ascites. Assessment 1. History – appetite, weight change, bowel habits, dietary intake, food habits, food aversion or intolerance, symptoms affecting nutrition, medication, change in body image, and emotional impact on person and family. 2. Physical examination – measures of nutritional status (e.g. weight and height ratio (BMI), functional status, oral assessment). 3. Investigations – blood work (e.g. albumin and/or serum transferrin), professional to assess dysphagia and oral intake. 34 Non-Pharmacological Interventions Consult speech and language pathologists for management of dysphagia. Consult occupational therapists for help with energy conservation strategies (see Appendix E) and the actual physical process of eating. Specific interventions may include: • Completing oral care prior to eating • Eating small frequent meals that are high calorie, low volume, and culturally appropriate • Eating when hungry rather than at typical meal times • Experimenting with texture, temperature, and seasonings • Increasing activity as tolerated. Pharmacological Interventions • Review potentially offensive medications (e.g. opioids, anticholinergics, and antispasmodics). • Promotility agents may stimulate gastrointestinal peristalsis and reduce early satiety (e.g. Metoclopramide 5-20mg PO/ subcut or Domperidone 5-20mg PO four times daily, maximum dose 120mg in 24 hours). • Progestational agents may stimulate the appetite resulting in increased caloric intake, body weight (mostly water) and sense of well-being, but there is a risk of thromboembolic complications (e.g. Megestrol acetate 400-800mg PO per day in divided doses, maximum dose 800mg in 24 hour). • Corticosteroids may improve appetite resulting in increased food intake, performance, and quality of life, with no change in muscle mass. They have a short term benefit of approximately three weeks. Other possible benefits are the control of coexisting nausea and possible relief of any obstruction (e.g. Dexamethasone 4-8mg PO/subcut twice daily or Prednisone 5-25mg PO per day). 35 26. What can be done to assist persons and their families cope with reduced nutritional intake? Eating is commonly associated with health and well-being. When people are no longer able to eat or drink, this change can often cause distress to families. Intervention Strategies • Provide adequate education and counselling that address the family’s anxiety and concerns. Explain that cachexia is not the same as starving to death, but instead is the result of metabolic abnormalities caused from cancer. Giving the person more food will not result in fat or muscle mass gain. • Explain that forcing a person to eat will have no impact on wellbeing or survival, but instead may result in increased distress, discomfort and nausea. • Reassure the family that the decrease in food and fluid intake is because of the illness and not because the person is giving up. • Encourage family members to think of food as a comfort measure. Suggest offering culturally appropriate and favourite foods without worrying about nutritional value. • Emphasize the importance of fluids over solids to maintain hydration. • Encourage the family to try to preserve the social benefits of meal times (e.g. have the ill person join the table at mealtime even if intake is minimal). • Help create the best conditions for eating, address nausea and pain, provide good mouth care, ensure a pleasant setting for meals, and offer frequent small meals according to the person’s preferences. • Encourage family to provide other methods of caring such as moistening the person’s lips and oral cavity, providing light massage, and/or reading or playing music. 36 Nutritional Tips Add extra calories for energy. • Spread plenty of butter/margarine on toast, muffins, rolls, potatoes, and rice. • Add peanut butter, jam, and honey to bread. • Pour sauces or gravies over potatoes, meat ,and vegetables. • Add sour cream or mayonnaise to vegetables, salads, and sandwiches. • Spread cream cheese on bread, muffins, fresh fruit, and crackers. • Melt cheese over bread, vegetables, or potatoes. • Scoop ice cream on desserts or into carbonated beverages. • Drink homogenized milk. • Drink milkshakes or hot chocolate made with whole milk. • Add cream to cereals, hot beverages, and fresh fruit. • Top desserts or fruit with whipped cream or yogurt. Add protein for strength. • Grate cheese onto vegetables, pasta, bread, casseroles, and soup. • Dice fish, chicken or beef into casseroles, soup, and sauces. • Eat yogurt or cottage cheese alone or added to recipes. • Add eggs into sauces and soups, bake in puddings, sponge cakes, and custards. • Add 3-4 tablespoons of skim milk powder to each cup of milk. This fortified milk can be added to soup, sauces, scrambled eggs, casseroles, hot cereals, puddings, custards, and milkshakes. • Use milk instead of water to make soup, sauces, hot cereal, and cocoa. • Blend eggs into sauces and soups; bake eggs in puddings. Other ideas • Check your recipe books for foods that may appeal to the person. • Vary the colour of food served on the plate (e.g. arrange food attractively or add a slice of tomato, orange, or a sprig of parsley). • Eat small amounts of nutritious foods six to eight times each day. • Keep nutritious snacks such as raisins, nuts, fruits, and yogurt close at hand. 37 • Eat the main meal at the time when the person feels the best during the day. • Alcohol may increase appetite (e.g. include a glass of wine or a cocktail before the meal). • An eating schedule may be necessary to remind the person to eat. • Chew foods slowly to prevent the stomach from becoming too full too quickly. • Make sure fluids are nutritious such as juices, milk, or milkshakes. • Rely on food the person really loves during times when he or she is not hungry. • Concentrate on making the meal more enjoyable with attractive settings, bright surroundings, and good company. • If appetite is reduced by nausea, eat small portions of dry foods like crackers, pretzels, or toast. • Limit procedures, treatments, or other stresses immediately prior to meals. 27. Is nutritional support beneficial? [Nutritional support may include vitamins, calorie dense drinks, enteral formulas, and total parenteral nutrition (TPN).] Not necessarily. When a person has anorexia cachexia syndrome, feeding by any route will not improve his or her nutritional status, as the metabolic and tumour-related factors causing this syndrome cannot be changed. There is no evidence that nutritional supplements will reverse cachexia. Further research is needed to determine whether supplements will improve energy levels and an overall sense of well-being. Some people will find that liquid supplements (e.g. Boost ®, Ensure ®, Resource ® or Carnation Instant Breakfast®) are easier to ingest than full meals. The use of supplements to increase protein, vitamins, and caloric intake at a time when the person has an appetite can be encouraged. 38 Nursing Alert Tube feeding and TPN are not beneficial in most palliative situations. As with other forms of nutritional intake, these nutritional therapies have not been shown to improve survival. With parenteral nutrition in particular, research has shown low potential benefit and high risk for serious side effects (e.g. septicemia or electrolyte imbalances). In persons for whom loss of weight and muscle may be primarily attributed to factors other than advanced anorexia and cachexia, there may be a temporary benefit from nutritional support. People who may potentially benefit from tube feeding or TPN include those persons with: • Head and neck cancer that interferes with ingestion and swallowing, • Hastrointestinal obstruction from intra-abdominal disease, • Severe depression, • Abnormalities of taste, • Chronic nausea and/or vomiting and/or • Malabsorption secondary to pancreatic insufficiency, short gut syndrome, fistula formation or late effects of radiation therapy to the abdomen. When a decision is made to commence nutritional support, this decision should be accompanied with criteria by which to measure the benefit (e.g. weight gain, improved energy, and/or improved quality of life as guided by the goals of care). Prior to initiating these interventions, decisions related to when and if to discontinue nutritional support would therefore be clearly understood by the person, family members, and health care professionals. When this type of nutritional support is not indicated, an explanation of the lack of proven benefit and associated morbidity is essential. The provision of nutritional support to the person is indicated especially if he or she still has an appetite. Expected benefits may include improved energy, slowed weight loss, and relief of symptomatic distress from hunger. In a person with irreversible altered mental status, these subjective benefits may not be realized and, hence, the initiation of this type of nutritional support would be inappropriate. 39 References Brown, J. K. (2002). A systematic review of the evidence on symptom management of cancer-related anorexia and cachexia. Oncology Nursing Forum, 29(3), 517-532. Downing, M. G. & Wainwright, W. (2006). Cachexia-Anorexia Syndrome (CAS). Medical Care of the Dying, (4th ed., pp. 307309). Victoria, BC: Friesens Corporation, Canada. Grant M., & Kravits, K. (2000). Symptoms and their impact on nutrition. Seminars in Oncology Nursing, 16(2),113-121. Holmes, S. (2009). A difficult clinical problem: Diagnosis, impact and clinical management of cachexia in palliative care. International Journal of Palliative Nursing, 14(7), 320-326. Laviano, A., Meguid, M. M., Inui, A., Muscaritoli, M., & Rossi-Fanelli, F. (2005). Therapy insight: Cancer anorexia−cachexia syndromewhen all you can eat is yourself. Nature Clinical Practice Oncology, 2(3), 158-165. MacDonald, N. (2003). Is there evidence for earlier intervention in cancer-associated weight loss? The Journal of Supportive Oncology, 1(4), 279-286. Ross, D., & Alexander, C. (2001). Management of common symptoms in terminally ill patients: Part I. Fatigue, anorexia, cachexia, nausea and vomiting. American Family Physician, 64(5), 807-814. Sarhill, N., Mahmoud, F. A., Christie, R., & Tahir, A. (2003). Assessment of nutritional status and fluid deficits in advanced cancer. American Journal of Hospice and Palliative Care, 20(6), 465-473. Strasser, F. (2003). Eating-related disorders in patients with advanced cancer. Supportive Care in Cancer, 11(1), 11-20. Strasser, F., & Bruera, E. (2002). Update on anorexia and cachexia. Hematology Oncology Clinics of North America, 16(3), 589-617. UpToDate. (2011, February 11). End of life care: Overview of symptom control. Retrieved from http://www.uptodate.com/ store UpToDate. (2011, January). Pharmacologic management of cancer related anorexia/cachexia. Retrieved from http://www.uptodate. com/store. 40 Constipation, Diarrhea and Bowel Obstruction 28. What is constipation? How is it assessed? Constipation is the passage of small, hard stools that may be painful or difficult to pass and/or a prolonged interval between bowel movements (normal range is 1 in 3 days to 3 in 1 day) and/ or incomplete evacuation of stool. Suspect constipation in any person who presents with one or more of the following: • Irregular bowel movements (especially if no bowel movement for 3 or more days), • Firm or hard stools, • Bypass diarrhea (liquid stool oozing around a constipated mass), • Anorexia, nausea, and/or emesis, • Abdominal distension/discomfort and/or bloating, • Bowel obstruction • Regular opioid use. Assessment 1. History – Include the person’s normal bowel pattern, date of last bowel movement, quality, quantity and frequency of stools, feeling of abdominal discomfort, bloating or rectal fullness, sense that bowels are not moving often enough, difficulty/ pain with passing stools, onset of the problem, nausea, and/or vomiting. Review medications, as medications such as opioids can contribute to constipation. Assess food and fluid intake. 2. Physical assessment Abdominal assessment – Inspect the abdomen for bloating, distension, and/or bulges. Auscultate to assess bowel sounds. Palpate to evaluate abdominal tenderness and/or stool especially in the left colon. Digital rectal exam – Assess the amount and consistency of stool in the rectum. 41 3. Investigations – Abdominal flat plate to quantitatively assess the amount and location of stool in the colon. The amount of stool in each of the ascending, transverse, descending, and sigmoid colon is scored on a scale of 0 to 3, where: 0 = no stool 1 = stool fills <50% of lumen 2 = stool fills >50% of lumen 3 = stool completely fills lumen The total score yields a “constipation score” out of 12. A score of 7/12 or more indicates severe constipation and requires aggressive intervention to empty the colon. 29 What causes constipation? Causes The most important causes of constipation are medications and systemic effects of terminal disease. Contributing factors: • Dehydration (e.g. reduced fluid intake and/or increased insensible losses), • Poor gut motility (e.g. increased fluid absorption due to prolonged transit time), • Medications (e.g. Opioids, Anticholinergics, 5-HT3 Antagonists, Antidepressants, Antiepileptics, Iron supplements, Antacids), • Metabolic disturbances (e.g. hypercalcemia, uremia, hypothyroidism, diabetes), • Neurological Disorders (e.g. cerebral tumours, spinal cord involvement, sacral nerve involvement, autonomic nerve failure such as MS, Parkinsons, motor neuron disease ), • Structural abnormalities (e.g. malignant ascites pelvic tumour masses, radiation fibrosis, anal rectal conditions such as fissures, abscess, hemorrhoids), • Other (e.g. inattention to normal body functions secondary to altered mental status, inactivity and weakness, advanced age, depression, decreased mobility, lack of privacy). 42 30. What are the complications of constipation? Complications • • • • • • • • Increased pain, Abdominal distension or discomfort, Anorexia, nausea, and/or vomiting, Hemorrhoids or anal fissures, Bowel obstruction, Urinary retention, Agitation and restlessness, Exacerbation of confusion. Nursing Alert Overflow diarrhea is liquid stool oozing around a constipated mass. Before holding laxatives or treating with antidiarrheals, the possibility of significant constipation with bypassing stool must be ruled out. People with advanced cancer are far more likely to experience constipation than diarrhea; suspect overflow diarrhea in this population. Nursing Alert Constipation may be an early sign of spinal cord compression when accompanied by decreased perianal sensation and decreased rectal tone. 43 31. What are the interventions for constipation? In the absence of oral intake, the body continues to produce 2-3 ounces of stool per day. The bowel lining is continually renewing itself. Sloughed cells, along with bacteria and digestive juices, comprise much of the stool. A person can easily become constipated even when he or she is not eating. Prevent Constipation • Encourage increased fluid intake. • Ensure all people on regular opioids are on a bowel routine and bowel function is assessed daily. • Although fibre may be effective, bulk laxatives (e.g. Metamucil®), are not recommended, as the inability to drink enough fluid will make stool extremely hard and may result in or add to an obstruction. • Encourage physical activity as tolerated as this increases peristalsis. • Provide adequate time and privacy to defecate. Pharmacological Interventions Oral bowel stimulants are started simultaneously with opioids. Examples include: • Senna, usual starting dose is 1-2 tabs orally at bedtime but can be increased to 2-4 tabs twice daily and up to 4 times daily as needed. • Lactulose, usual dose 30 mL 1-3 times daily orally. Lactulose may, however, be poorly tolerated due to its sweet taste, abdominal bloating and/or cramping effect. • Polyethylene glycol 3350 (PEG 3350), usual dose 17 grams daily by mouth, up to 75 g/day. Adjust dosages and frequencies of oral bowel stimulants as needed to ensure the person has a soft, formed bowel movement every 1-2 days. Rectal laxatives are useful if there is stool in the rectum or if the person does not tolerate oral laxatives. If there is no soft bowel movement at least every 3 days, give a stimulant suppository (e.g. Bisacodyl) and, if ineffective, give a micro or sodium phosphate enema. 44 Methylnaltrexone (Relistor®) is an injectable laxative given subcutaneously. This laxative is generally not used as a first-line therapy, but rather for acute management when other methods have failed, and/or for maintenance when oral laxatives have been ineffective. The dosage is based on the person’s weight (e.g. weight 8-62 kg give 8mg subcut; 63kg-114kg give 12 mg subcut). Relistor® is not effective for every person but it can work within 30 minutes or sometimes a bit longer. If the above interventions are ineffective, further action is guided by results of a digital rectal exam. • If there is soft stool in rectum, repeat the stimulant suppository and/or sodium phosphate enema. If ineffective, try larger volume enema (e.g. soap suds). • If there is firm stool in the rectum, soften stool with a mineral oil enema followed by a stimulant suppository and/ or micro or sodium phosphate enema. If ineffective, try a high mineral oil enema followed by a large volume enema to clear the mineral oil from the bowel. If the rectum is empty but other symptoms indicate probable impaction, consider a flat plate of the abdomen to assess the amount and location of stool within the colon and treat accordingly. • If there is stool in the ascending or transverse colon, the oral route may be the most effective; a bottle of Magnesium Citrate may be required. • If there is stool in the descending or sigmoid colon or rectum, the rectal route is more likely to be effective. A larger volume enema may be required. • If there is overflow diarrhea, continue to administer laxatives to expel the constipated mass. Nursing Alert Before initiating aggressive laxative and/or enema administration, rule out possible bowel obstruction. Such therapies are contraindicated in the presence of bowel obstruction, unless the obstruction is due to constipated stool. One good response to a laxative or enema doesn’t mean that constipation is resolved. The sigmoid colon may be clear but the remaining colon may still be full of stool. 45 Rectal procedures are invasive and carry some risk in certain circumstances. As with any procedure, they should not be performed when the potential benefits do not clearly outweigh the risks. Contraindications include: • Rectal bleeding – if only mild bleeding, enemas can usually be given safely, • Rectal tumours – are often very vascular and these people are at greater risk of tissue injury, • Heart problems – arrhythmias can be triggered by vagal stimulation, • Leukothrombocytopenia – people with decreased cell counts are at increased risk of infection and bleeding with any invasive procedure. People with painful hemorrhoids may avoid defecating and become constipated. Use of local anaesthetic creams or ointments may reduce local discomfort with defecation and also aid the use of suppositories or enemas. Keeping stools soft and easily evacuated is important for reduction of rectal pain and prevention of constipation for persons with rectal tumours or hemorrhoids. Prevention of constipation is also important for persons with intraabdominal tumours or malignant ascites so abdominal distention and discomfort are not exacerbated by an excessive stool burden. 46 32. How is diarrhea assessed? What are the causes? Diarrhea is an increase in stool volume and liquidity resulting in 3 or more bowel movements per day. Associated symptoms may include abdominal cramping, anxiety, general malaise, dehydration, electrolyte abnormalities, excoriated perineum or ostomy site, and pain. Assessment 1. History – onset, duration, frequency, aggravating and alleviating factors, stool volume and description, fluid and diet intake, presence of nausea, vomiting and/or pain. Review medications, imaging and surgical history. 2. Physical assessment – examine perineum or ostomy site, perform abdominal and digital rectal exam, and observe for signs of dehydration. 3. Investigations – stool specimens including C. difficile, Vancomycin Resistant Enterococci (VRE), Methicillin-resistant Staphylococcus aureus (MRSA) and/or ova and parasites (O&P). Causes • Fecal impaction with overflow diarrhea, • Overuse of laxative therapy, dietary fibre and/or hyperosmolar preparations (e.g. enteral feeds), • Pelvic or lower abdominal radiation therapy, • Malabsorption (e.g. pancreatic disease, gastrectomy, ileal resection or colectomy), • Enterocolic fistula, • Infection by intestinal or other organisms. If recent or frequent hospital stay(s) consider C. difficile, MRSA, E. coli and/or VRE. If HIV positive, consider infections common to HIV/AIDS that cause diarrhea, such as cryptosporidiosis. • Surgical shortening of the bowel, • Tumour type (e.g. carcinoid tumours or villous adenomas), • Medications (e.g. antacids, antibiotics, certain NSAIDs) in susceptible people or sorbitol (found in “sugar-free” elixirs and tube feeds), 47 • Concurrent diseases (e.g. inflammatory or irritable bowel syndromes, diabetes or hyperthyroidism), • Metabolic abnormalities (e.g. hypomagnesemia and hypocalcemia). 33. What are the interventions for diarrhea? Non-Pharmacological Interventions • • • • Provide psychosocial support. Monitor skin for breakdown and treat appropriately. Maintain hydration and electrolyte balance. Consider dietary measures such as small frequent bland meals, a low residue or potassium rich diet (e.g. “Brat” – Bananas, Rice, peeled Apples and Toast). • Treat any reversible causes (e.g. rule out constipation, manage infections or reassess medications). Pharmacological Interventions • Anti-diarrheal agents such as non-opioid (Imodium®, Kaopectate® or selective use of Metamucil®) or opioids (Lomotil® or Codeine). • Octreotide (Sandostatin ®) 50-200mcg subcut 3 times daily, maximum dose 600mcg in 24 hours. • Cholestyramine capsules prior to meals, if pancreatic insufficiency or cystic fibrosis. Nursing Alert If overflow diarrhea is suspected, refer to pharmacological interventions for constipation (See Question 31). 48 34. What is bowel obstruction? What are the causes? Bowel obstruction occurs when the intestinal contents fail to propel forward through the lumen, either as a result of mechanical blockage or impaired motility secondary to the loss of propulsive peristalsis or paralytic ileus (sometimes called functional or pseudo-obstruction). Partial or complete malignant bowel obstruction is common in persons with advanced intra-abdominal or pelvic, colorectal, and ovarian cancers. Bowel obstruction occurs less commonly in other cancers such as cervical, gastric, pancreatic, uterine, and lymphomas. Causes Mechanical obstruction from: • External tumour or nodal mass compressing small or large bowel, rarely from tumour within the bowel, • Malignant adhesions or strictures resulting from carcinomatosis or peritoneal seeding within the abdominal cavity, often resulting in multiple sites of obstruction. Adhesions or strictures may also be secondary to intestinal surgery or radiation therapy • Impacted feces (obstipation). Functional obstruction from: • Carcinomatosis, peritoneal seeding, bowel wall invasion, or malignant adhesions within the abdominal cavity, • Diabetic neuropathy, • Peritonitis or prolonged intestinal inflammation, • Autonomic dysfunction secondary to: – Medication (e.g. opioids), – Metabolic abnormalities (e.g. hypokalemia or hypercalcemia), – Spinal cord injury, or – Post-operative ileus, ischemia or intestinal edema. 49 35. What are the signs and symptoms of bowel obstruction? How is it assessed? Signs and Symptoms Nausea and vomiting will occur in 100% of people with an obstruction. Presentation varies depending on the site of the obstruction: • Gastric outlet obstruction is associated with large volume projectile emesis that often occurs without warning. • Small bowel obstruction is associated with early onset emesis, can be large in volume, and is common shortly after oral intake. • Large bowel obstruction is associated with emesis that develops later on and may include fecal content. Abdominal pain is described as colicky or cramping pain and is often located near the site of obstruction. Prior to the onset of vomiting, pain will often occur in the majority of people with an obstruction. Abdominal distension is more significant in cases of obstruction of the large bowel versus the small bowel. Changes in bowel sounds may include: • Hyperactive and high-pitched tinkling sounds suggesting intestinal fluid and air under tension in a dilated bowel (rushes of high-pitched sounds coinciding with abdominal cramping indicate intestinal obstruction and are more common in partial obstruction), • A succussion splash, which is a sloshing sound of retained gastric contents audible during rocking of the upper abdomen, • Diminished or absent bowel sounds, which usually indicate complete obstruction. Changes in bowel movements may include: • Infrequent bowel movements, • Bowel movements normal in frequency but reduced calibre (pencil-like stools), • Incomplete emptying secondary to overflow diarrhea. Absence of flatus is associated with complete obstruction. Evidence of air/fluid levels on abdominal x-ray is associated with obstruction. 50 Nursing Alert Regular bowel assessments are necessary in order to detect bowel obstruction. Signs and symptoms of bowel obstruction may be acute with nausea, vomiting, and abdominal pain; however, it is often a slow, insidious process which may progress from partial to complete obstruction. 36. What are the interventions for bowel obstruction? Non-Pharmacological Interventions • Reduce intake and promote bowel rest. • Continue with small amounts of liquids or soft diet in the presence of an incomplete or distal obstruction, if tolerated. • Provide good mouth care. Assess and treat oral candidiasis especially for persons on medications that cause immunosuppression. Use ice chips or artificial saliva, especially if the person is NPO. • Prevent dehydration through administration of 1-2 litres of fluid per day via hypodermoclysis or intravenous. Nursing Alert In the presence of an incomplete bowel obstruction, some persons may tolerate a soft diet to facilitate movement through narrowed bowel lumen. Pharmacological Interventions • Decrease painful peristalsis (e.g. Hyoscine butylbromide [Buscopan ®] 10-20mg subcut every 4-6 hours, maximum dose 120mg in 24 hours). • Reduce GI secretions and bowel wall edema (e.g. Octreotide 50-200mcg subcut every 8 hours). • If tumour or tumour related edema is suspected, give antinflammatory medications (e.g. Dexamethasone 4-20mg PO/subcut per day in one single daily dose or divided doses). May provide relief of symptoms and/or possibly transform a complete obstruction to a partial one. 51 • Control nausea and vomiting without stimulating peristalsis, use antiemetics with no promotility effect (e.g. Haloperidol 0.5–5mg PO/subcut every 6-8 hours, maximum dose 20mg in 24 hours). • Control visceral pain by giving opioids via a non-oral route. • Correct electrolyte imbalances, if appropriate • If the obstruction is due to fecal impaction, aggressive administration of enemas and oral laxatives is indicated. Nursing Alert In the event of a partial bowel obstruction, prokinetic agents such as Metoclopramide or Motilium ® and vigorous use of enemas and oral laxatives may prevent progression to a complete obstruction. However, there is a relative contraindication to the use of prokinetic agents such as Metoclopramide and oral laxatives in the presence of complete bowel obstruction as they may exacerbate pain, nausea, and vomiting and could lead to bowel perforation, particularly if they occur higher in the bowel. Invasive Interventions • Decompress the GI tract when there is persistent, significant nausea, vomiting, and abdominal distension despite optimal medical management. Use a nasogastric (NG) tube for this purpose on a temporary basis. • Consult Gastrointestinal specialist to determine appropriateness of a percutaneous venting procedure that may provide longer term symptom management. • If there is a well-defined locus of mechanical intestinal obstruction secondary to malignancy, consider correction via surgical resection or stent insertion. If the obstruction is at the level of the esophagus, stent insertion or dilatation procedures could be effective. Factors such as extent of disease, prognosis, goals of care, and quality of life must be taken into account when considering the appropriateness of the surgical intervention. Clinical Tip Liquid to soft nutrients may still be enjoyed by persons with NG or venting decompression tubes as what is swallowed will be eliminated via the drainage system. 52 References Abernethy, A., Wheeler, J., & Zafar, Y. (2009). Detailing of gastrointestinal symptoms in cancer patients with advanced disease: New methodologies, new insights, and a proposed approach. Current Opinion in Supportive and Palliative Care, 3(1), 41-49. Candy, B., Jones, L., Goodman, M. L., Drake, R., & Tookman, A. (2001). Laxatives or Methylnaltrexone for the management of constipation in palliative care persons. Retrieved from http://www.cochranejournalclub.com/management-ofconstipation-clinical/pdf/CD003448.pdf Chamberlain, B. H., Cross, K., Winston, J. L., Thomas, J., Wang, W., Su, C., & Israel, R. J. (2009). Methylnaltrexone treatment of opioid induced constipation in patients with advanced illness. Journal of Pain and Symptom Management, 38(5), 683-690. Clemens, K. E., & Klaschik, E. (2008). Management of constipation in palliative care patients. Current Opinion in Supportive and Palliative Care, 2(1), 22-27. Economou, D.C. (2005). Bowel management: Constipation, diarrhea, obstruction, and ascites. In B. Ferrell & N. Coyle (eds.), Textbook of palliative nursing (2nd ed., pp. 219-238). New York: Oxford University Press. Feuer D.J., Broadley, K.E., Shepherd, J.H., & Barton, D.P. (2000). Surgery for the resolution of symptoms in malignant bowel obstruction in advanced gynaecological and gastrointestinal cancer. Cochrane Database of Systematic Reviews [Computer File],(4):CD002764. Fraser Health. (2006). Bowel care. Retrieved from http://www. fraserhealth.ca/media/04FHSymptomGuidelinesBowelCare.pdf Fraser Health. (2006). Malignant bowel obstruction. Retrieved from http://www.fraserhealth.ca/media/13FHSymptom GuidelinesMalignantBowelObstruction.pdf Friedrichsen, M., & Erichsen, E. (2004). The lived experience of constipation in cancer patients in palliative hospital-based home care. International Journal of Palliative Nursing, 10(7), 321-32. Larkin, P. J., Sykes, N., Centeno, C., Ellershaw, J., Elsner, F., Eugene, B., Gootjes, J., Nabal, M., Noguera, A., Ripamonti, C., Zucco, F., & Zuurmond, W. (2008). The management of constipation in 53 palliative care: Clinical practice recommendations. Palliative Medicine, 22, 796-807. Librach, S. L., Bouvette, M., De Angelis, C., Farley, J., Oneschuk, D., Pereira, J. L., & Syme, A. (2010). Consensus recommendations for the management of constipation in patients with advanced, progressive illness. Journal of Pain & Symptom Management, 40(5), 761-773. McMillan S.C. (2002). Presence and severity of constipation in hospice patients with advanced cancer. American Journal of Hospice and Palliative Care, 19(6), 426-430. Peate, I. (2003). Nursing role in the management of constipation: Use of laxatives. British Journal of Nursing, 12(19), 1130-1136. Ramkumar, D., & Satish, S. S. C. (2005). Efficacy and safety of traditional medical therapies for chronic constipation: Systematic review. American Journal of Gastroenterology, 100, 936-971. doi:10.1111/j.1572-0241.2005.40925.x Ripamonti, C., & Mercadanta, S. (2004). How to use octreotide for malignant bowel obstructions. Supportive Oncology, 2(4), 357-365. Ripamonti, C., Easson, A., & Gerdes, H. (2008). Management of malignant bowel obstruction. European Journal of Cancer, 44, 1105-1115. Thomas, J., Karver, S., Cooney, G. A., Chamberlain, B. H., Watt, C. K., Slatkin, N. E., Stambler, N., Kremmer, A. B., & Israel, R.J. (2008). Methylnaltrexone for opioid-induced constipation in advanced illness. The New England Journal of Medicine, 358(22), 2332-2343. Woolery, M., Bisanz, A., Lyons, H. F., Gaido, L., Yenulevich, M., Fulton, S., McMillan, S. C. (2008). Putting evidence into practice: Evidence-based interventions for the prevention and management of constipation in patients with cancer. Clinical Journal of Oncology Nursing, 12(2), 317-337. 54 Dehydration 37. What is dehydration? How is dehydration assessed? Dehydration is a loss of normal body water. Unfortunately, it is often difficult to assess hydration in people with advanced illness. Therefore, findings from a variety of assessments are most reliable. Assessment 1. History – Assess appetite, oral intake, associated symptoms (e.g. nausea, vomiting, diarrhea, drowsiness, fatigue, and confusion). 2. Physical Examination – Assess skin and oral cavity, dry mucous membranes, jugular venous pressure (JVP), blood pressure, pulse, temperature, ascites, muscle weakness. 3. Investigation – Serum urea, creatinine, sodium, hematocrit. Nursing Alert In severe cachexia, the skin turgor is hard to assess and is often not reliable. Similarly, thirst and edema are not good indicators of hydration status. 38. When is it beneficial to hydrate? As persons become increasingly debilitated, they will be at greater risk for dehydration. Treating dehydration can be a controversial topic. Decisions related to hydration need to be person and family focused and guided by goals of care. Different palliative care programs have varying philosophies regarding hydration. Treating dehydration that appears to be contributing to symptom distress could be considered reasonable. For example, in cases of dehydration, kidneys cannot effectively eliminate metabolites and body waste. As these metabolites accumulate, they may cause distressing symptoms such as nausea, constipation, confusion, 55 restlessness, agitation, hallucinations, nightmares, vivid dreams, hyperalgesia, allodynia, myoclonus, and seizures. In addition, dehydration can also result in dry, cracked lips and viscous secretions. Consider parenteral hydration as a therapeutic option aimed at achieving a specified clinical goal. The resolution of symptoms may depend in part on the volume or rate of parenteral fluids administered. For example, if: • Hydration is ineffective in achieving the desired goal within a pre-established time frame, it is reasonable to reassess the rate of infusion or consider discontinuing it. • The desired goal is achieved and the person is able to drink fluids, hydration may be discontinued or the volume reduced. • The desired goal is achieved and the person is unable to drink fluids, it may be necessary to continue with hydration. • The hydration seems to be causing more distress (e.g. increased respiratory secretions), it is reasonable to re-evaluate the rate or discontinue it completely. 39. When is it not beneficial to hydrate? In general, hydration may not be recommended or useful in the following situations: • The person is able to maintain an adequate oral intake (usually one litre per day is sufficient). • The person is unable to drink, or has limited oral intake and is not taking medications that are eliminated by the kidneys, and/or is not experiencing distressing symptoms. If a person is unable to drink or has limited oral intake, consider a reduction in the dose of medications (e.g. opioids may prevent metabolite accumulation caused by impaired renal function). • Supportive interventions (e.g. ice chips, artificial saliva or lip lubricants) are effective for symptom relief. • The person and/or family do not wish to have hydration. 56 40. Is hydration appropriate for a person who has edema? A person with edema has excessive fluid in the interstitial spaces but may have inadequate fluid in the intravascular and/or intracellular spaces and therefore, may be in need of additional fluids. Edema, especially of the lower extremities, is not a good indicator of hydration status. Edema can be a concern in the terminal phase of many diseases, i.e. up to last couple of months. Common causes of edema can be attributed to: • Reduced physical function, • Low serum albumin related to cachexia, which causes a decrease in vascular osmotic pressure and a shift of fluid from the vascular system into the interstitial tissues, or • Tumour blockage in the venous or lymphatic systems which causes an increase in back pressure and subsequent movement of fluid into the interstitial tissues. 41. How can hydration be maintained? Oral intake is the preferred route as long as it is well tolerated. Popsicles, frozen yogurt, ice chips made from water or fruit juice, and commercial instant breakfast drinks or milkshakes can be offered. Bendable straws and sports bottles can also be helpful. Hypodermoclysis (HDC), the subcutaneous administration of fluid via continuous, intermittent or bolus infusion is possible when the oral route cannot be used. Subcutaneous fluids may offer advantages over the intravenous route unless venous access has already been established. Intravenous infusions may be utilized in an in-person or community setting if central venous access is already in place. Advantages of hypodermoclysis over intravenous include: • Easier access, • Increased comfort, 57 • • • • Decreased cost, Decreased risk of systemic infection and other complications, Increased ease and safety to administer at home, and Increased patency of administration site (HDC sites can last up to 7 days or longer). Clinical Tip For specific guidelines on how to initiate parenteral hydration, refer to your agency policy. Clinical Tip If the individual is too weak to sip fluids up the entire length of the straw, cut the straw in half. References Downing, M. G., & Wainwright, W. (2006). Artificial hydration and hypodermoclysis guideline. Medical Care of the Dying, (4th ed., pp. 311-317). Victoria, BC: Friesens Corporation, Canada. Ferrell, B. R., & Coyle, N. (2010). Oxford textbook of palliative nursing, (3rd ed.). New York: Oxford University Press. Hodgkinson, B., Evans, D., & Wood, J. (2003). Maintaining oral hydration in older adults: A systematic review. International Journal of Nursing Practice, 9(3):S19-S28. MacMillan, K., Peden, J., Hopkinson, J., & Hycha, D. (2000). A caregiver’s guide: A handbook about end of life care. The Palliative Care Association of Alberta and Military and Hospitaler Order of St. Lazarus of Jerusalem. Sarhill, N., Walsh, D., Nelson, K., & Davis, M. (2001). Evaluation and treatment of cancer-related fluid deficits: Volume depletion and dehydration. Supportive Care in Cancer, 9(6):408-419. 58 Nausea and Vomiting 42. What are nausea and vomiting? What are the causes? Nausea is a subjective symptom involving an unpleasant feeling experienced at the back of the throat and/or the stomach. Vomiting is a mechanism whereby the body tries to purge itself of noxious substances involving expulsion of gastric contents by forceful contractions of abdominal muscles. Vomiting may or may not be associated with nausea. Nausea and vomiting are common at the end of life particularly among persons with cancer, AIDS, renal and hepatic failure. These symptoms are prevalent because they have multiple etiologies, several of which may be present at the same time. Causes Chemical and/or mechanical • Metabolic abnormalities (e.g. hypercalcemia, renal or hepatic failure and/or electrolyte imbalance), • Dehydration, • Medication toxicity/side effects (e.g. opioids, NSAIDs, antibiotics, selective serotonin reuptake inhibitors (SSRIs), chemotherapy, anticholinergics and/or Digoxin), • Decreased gastrointestinal motility (e.g. secondary to gastric stasis, autonomic insufficiency or intra-abdominal disease), • Constipation, obstipation or bowel obstruction, • Gastrointestinal pathology (e.g. tumour, ascites, gastroesophageal reflux disease, esophagitis or gastritis, peptic ulceration), • Liver metastasis, • Infection, • Chronic cough, • Retroperitoneal disease, • Radiation therapy. 59 Central Nervous System (CNS) Increased intracranial pressure secondary to: • Tumour-induced brain and skull metastasis or leptomeningeal disease • Cerebral edema • Cerebral infection • Cerebral hemorrhage. Vestibular Movement – associated nausea/vomiting secondary to vestibular disturbance caused by tumour or vestibular nerve invasion. Psychological • Anxiety • Fear • Anticipatory nausea • Pain. 43. How are nausea and vomiting assessed? Assessment 1. History • Intensity: How severe is the nausea? 0-10 rating scale or visual analogue scale such as that used in the ESAS-r (see Appendix A). • Onset: When did it start? • Duration: How long has the problem existed? How long does each episode of nausea and/or vomiting last? • Frequency: How often does nausea and/or vomiting occur? • Impact: How does the nausea/vomiting impact ability to function and quality of life? • Aggravation: What makes it worse? • Alleviation: What makes it better? • Associated symptoms: Are there other symptoms (e.g. constipation)? • Person’s perception: What is thought to be the cause of nausea or vomiting? • Environmental factors: What in the environment triggers nausea or vomiting? 60 • Emesis: How much emesis is there? What does it look like (colour, consistency)? What does it contain? 2. Physical assessment • Abdominal assessment: inspect, auscultate, percuss and palpate. Findings may include distention, ascites, abnormal bowel sounds, flatus, masses and/or tenderness. • Rectal exam: if constipation is suspected. • Oral assessment: findings may include infection (e.g. oral candida infection, stomatitis dryness, halitosis, poor oral hygiene and/or ill-fitting dentures). • Assess other systems as indicated (e.g. neurological for CNS induced nausea). 3. Investigations • Three views of the abdomen, electrolytes, renal and liver function tests. Consider other tests as indicated by the person’s history (e.g. flat plate of the abdomen to assess fecal load or CT of the head to rule out metastasis). 44. What are the interventions to control nausea and vomiting? Treat reversible causes: • Evacuate the bowels, • Reassess medications, • Correct metabolic imbalances, • Consider oncologic options (e.g. chemotherapy, radiation therapy and/or steroids), • Consider paracentesis as it may provide relief of nausea secondary to ascites, • Treat esophagitis, gastritis, peptic ulceration, • Rehydrate, • Treat vestibular disturbances. 61 Pharmacological Interventions The selection of an anti-emetic is guided by the etiology of the nausea and the potential toxicities of the drug. When people have advanced disease there are often multiple causes of nausea and therefore multiple strategies are often needed. • Metoclopramide (Maxeran®) 5-20mg PO/subcut/IV 4-6 times daily and every 1-2 hours as needed, maximum daily dose 120mg in 24 hours. Metoclopramide can also be given in continuous subcutaneous infusion of 60-120mg per day for persistent nausea. Metoclopramide is the drug of choice for mechanical and/or chemical causes of nausea because of its anti-emetic effects on the gastrointestinal and chemoreceptor trigger zone. Metoclopramide may be contraindicated if the person has a complete bowel obstruction due to its prokinetic effect. • Dexamethasone (Decadron®) 4-20mg PO/subcut in one daily dose or divided doses, taper to minimal effective dose as soon as response observed. Dexamethasone may be added to Metoclopramide if nausea persists. Dexamethasone is known to reduce swelling and inflammation potentially contributing to nausea; however, other mechanisms of action have been suggested. • Haloperidol (Haldol®) 0.5 -2mg PO/subcut every 4-12 hours and 0.5-2mg every 1 hour as needed, maximum dose 20mg in 24 hours. Haloperidol is also effective for mechanical and/or chemical causes of nausea and it may be used in the presence of bowel obstruction due to its lack of prokinetic activity on the gastrointestinal tract. Nursing Alert When using Metoclopramide and Haloperidol, monitor for infrequent but possible extrapyramidal side effects, such as restlessness, stiffness of the neck or jaw, tremours and/ or rigid muscles. There is evidence that prochlorperazine or methotrimeprazine can also cause extrapyramidal side effects. 62 • Domperidone (Motilium®) 5-20mg PO four times daily and 5-10mg every hour as needed, maximum dose 120mg per day. Domperidone is useful for its prokinetic effect. • Ondansetron hydrochloride (Zofran®) or Granisetron hydrochloride (Kytril®) 8mg PO/subcut every 8 hours, maximum dose 24mg in 24 hours. These medications may be especially helpful for chemotherapy induced nausea and vomiting. Remember that this drug causes constipation. • Prochlorperazine (Stemetil®) 2.5-10mg subcut every 4-8 hours, maximum dose 40mg in 24 hours. • Dimenhydrinate (Gravol®) 50-100mg PO/subcut every 4-6 hours, maximum dose 400mg in 24 hours. • Methotrimeprazine (Nozinan®) 2.5mg to 25mg PO/subcut every 4-6 hours, maximum dose 200mg in 24 hours. Nursing Alert Prochlorperazine, Dimenhydrinate, and Methotrimeprazine may cause significant sedation. Their use as antiemetics in hospice palliative care is infrequent. • Cannabinoids (Dronabinol, Nabilone) dosages vary. Further research is needed to determine the value of this drug group in advanced disease. • Octreotide (Sandostatin®) 50-200mcg subcut every 8 hours reduces gastric secretions and potentially bowel wall edema. • Hyoscine Butylbromide (Buscopan®) 10-20mg subcut every 4-8 hours and every hour as needed, maximum dose 120mg in 24 hours. Use as a last resort as it paralyzes the bowel. Non-Pharmacological Interventions • • • • Provide good oral hygiene. Apply a cool damp cloth to forehead and nape of neck. Manage associated symptoms (e.g. pain or constipation). Minimize noxious stimuli including: – Aromas in the hospital (remove the lid from the meal tray outside the person’s room to allow some of the food odour to dissipate, offer non-aromatic cold foods such as sandwiches), 63 • • • • – Avoid foods that are greasy, spicy or excessively sweet, – Avoid other smells (e.g. perfume, smoke), – Eat in a pleasant environment. Eat or drink small amounts often. Include foods such as lemonade, juices, soft drinks, popsicles, sherbet, crackers, pretzels, plain cookies, and toast. Avoid dehydration. Position the person in an upright position after eating to facilitate digestion. Provide loose fitting clothing. Consider complementary therapies such as relaxation, imagery, acupressure, and acupuncture. References Alexander, C. (2001). Management of common symptoms in terminally ill patients: Part I. Fatigue, anorexia, cachexia, nausea and vomiting. American Family Physician, 64(5), 807-814. Campbell, T., & Hately, J. (2000). The management of nausea and vomiting in advanced cancer. International Journal of Palliative Nursing, 6(1), 18-25. Downing, M. G., & Wainwright, W. (2006). Nausea and vomiting. Medical Care of the Dying (4th ed., pp. 317-333). Victoria, BC: Friesens Corporation, Canada. Ferrell, B. R., & Coyle, N. (2010). Oxford textbook of palliative nursing, (3rd ed.). New York: Oxford University Press. Parkman, H.P. (2002) New advances in the diagnosis and management of nausea and vomiting. Case Manager, 13(2), 83-86. Rhodes, V.A., & McDaniel, R.W. (2001). Nausea, vomiting, and retching: Complex problems in palliative care. Cancer: A Cancer Journal for Clinicians, 51(4), 232-248. 64 Delirium 45. What is delirium? What are the causes of delirium? Delirium is a cognitive impairment with a sudden onset and fluctuating level of consciousness. Dementia is differentiated from delirium in that dementia has a gradual onset, the person’s level of consciousness is unimpaired, and it does not fluctuate. It is important to distinguish delirium from dementia because the diagnosis provides an indication of the likelihood of restoration of cognitive function. Approximately 25-45% of episodes of delirium are reversible, whereas dementia is usually chronic and irreversible. It is possible for a person with delirium to have a preexisting dementia. Hence, reversing the delirium in those people will not completely restore cognitive function. Features of delirium include disturbances in: • Level of consciousness that ranges from hyperalert to somnolent, • Attention with decreased ability to focus, sustain, or shift attention, • Cognition and/or perception including paranoia and hallucinations, • Sleep-wake cycle, • Psychomotor behaviour with changes ranging from withdrawal to agitation and • Emotional state with manifestations such as anxiety, anger, depression, apathy and/or irritability. Emotions are often labile. There are three main types of delirium: 1. Hypoactive hypoalert is a calm somnolent state often manifested when a person is actively dying or is associated with dementia, depression, and somnolence. As long as it is not of sudden onset and reversible causes have been ruled out, no treatment is necessary. Attention to comfort is all that is required. 2. Hyperactive hypoalert (mixed) is a restless somnolent state; however, the person can fluctuate between somnolence and agitation. 65 3. Agitated or hyperactive hyperalert is an agitated, restless state with sudden onset and a fluctuating level of consciousness that may or may not include hallucinations, delusions, disorientation, memory impairment, distractibility, day/night reversal, inappropriate communication, incoherent speech, an increase in psychomotor activity, anxiety and/or emotional lability. All of these symptoms can result in obvious behavioural changes. Causes An acronym that may assist with identification of multifactorial causes is “DELIRIUM”: D – Drugs e.g. opioids, benzodiazepines, antidepressants, nonsteriodal anti-inflammatory agents, ACE inhibitors, Digoxin, anticholinergics and diuretics. Dehydration. E – ETOH (alcohol) and/or drug use, misuse or withdrawal. L – Liver impairment. I – Infection. R – Respiratory impairment (e.g. hypoxemia). I – Intracranial pathology (e.g. brain tumour or head injury). U – Uremia (e.g., renal impairment). M – Metabolic abnormalities (e.g. hypercalcemia or hyponatremia). Nursing Alert Urinary retention and constipation do not cause delirium but may exacerbate agitation in cognitively impaired individuals. 66 46. How is delirium assessed? Episodes of early delirium are easily missed. A comprehensive assessment and ongoing reassessment of cognitive function is therefore important. Assessment 1. History – clarify the following with family and/or caregivers: • Speed of onset, • Timing of symptoms (e.g. when is the delirium better and/or worse), • Changes in behaviour, level of consciousness, attention, sleep wake cycles, cognition/perception, and emotions, • Alleviating and aggravating factors, • Effect on daily functioning and activities of daily living, history of drug or alcohol use. Review medications to identify potential causes. 2. Physical Examination – assess for signs and symptoms of possible causes (e.g. opioid toxicity, infection, dehydration, metabolic abnormalities, and/or hypoxemia). 3. Investigations – review screening blood work and other investigations to help identify cause(s) (e.g. CBC, blood culture, electrolytes, calcium and albumin, liver and renal function tests, metabolic screening, urinalysis, CT of head, chest x-ray and/or oxygen saturation). Use a screening tool [e.g. Molloy Standardized Mini-Mental State Examination (SMMSE), Confusion Assessment Method (CAM) and Confusion Rating Scale (CRS)] to help detect and monitor delirium. Nursing Alert Orientation questions (to the person, place, and time) alone do not provide an accurate assessment of a person’s cognitive status. To normalize and reduce stigma associated with the use of any screening tool for cognitive impairment, provide the following type of explanation, “Illnesses and medications can affect the way your mind works and interfere with your memory, concentration, and ability to think clearly. I have a set of questions I ask all people to see if these problems are occurring and to monitor changes over time. If you are experiencing these kinds of problems, I hope to find ways to improve things for you. Is it okay if I ask you the questions?” 67 47. What are the interventions for delirium? Non-Pharmacologic Interventions • Surround the person with familiar objects and people including family members and consistent caregivers if possible. • Be calm and respectful. • Provide structure and routine with simple explanations. • Provide a quiet, well-lit room, night light, visible clock, and calendar. • Do not try to re-orientate agitated persons or correct them, as this tends to increase agitation. Identify and treat reversible causes including: • Infection (e.g. antibiotics), • Opioid neurotoxicity (e.g. hydration and opioid rotation), • Cerebral tumour (e.g. steroids and/or radiation therapy), • Metabolic abnormalities (e.g. correct imbalances), and/or • Medications (e.g. change or discontinue as indicated) Pharmacological Interventions If the person is agitated, control the agitation as follows: Haloperidol (Haldol®) 0.5-2mg PO/subcut every 4-6 hours and every hour as needed, titrate upward to maximum dose of 20mg in 24 hours. Haloperidol has antipsychotic properties effective for controlling hallucinations, restlessness, and agitation, and for this reason it is the drug of choice. Methotrimeprazine (Nozinan®) 2.5mg to 25mg PO/subcut every 8-12 hours and every hour as needed, maximum dose 200mg in 24 hours. Methotrimeprazine is a sedating neuroleptic that can be used if there is no improvement (after 36-48 hours) after optimal titration of Haloperidol. Nursing Alert In rare instances of agitated delirium intractable to all measures, consider palliative sedation (See Question 76). 68 Lorazepam (Ativan®) Some centres use Lorazepam as an infusion. Midazolam (Versed®) is a quick acting benzodiazepine that can be used to produce sedation for cases of intractable agitated delirium. A common starting dose is 1mg per hour via continuous subcut/IV infusion. Titrate upward to achieve the desired level of sedation that relieves the distress of intractable delirium. Midazolam 2.5-5.0mg subcut may be given as a loading dose while the infusion is being prepared (see Question 76 on Palliative Sedation). Nursing Alert Any of these medications may have a paradoxical effect and worsen the delirium. If this occurs, refer to a palliative care specialist. 48. What are the interventions for supporting family when a person is delirious? Family Counselling It can be very distressing for family members to witness hyperactive delirium. It is important to acknowledge the loss experienced by the family as they struggle to cope with someone who has changed dramatically. The following explanations may help the family cope: • Symptoms of delirium such as moaning and agitation are an indication of brain malfunction and not an expression of pain or suffering. • If the person had no pain or the pain control was good before the onset of delirium, it is likely that the person’s behaviour is not due to increased pain. • Increasing the dose of opioids can worsen the agitation and potentially escalate distressing toxic side effects. • Medications are available for treating the symptoms. The goal of treatment is comfort. • People who recover usually have little or no recollection of this symptom after the episode of agitated delirium resolves. 69 • The person is not in control of what he or she is doing or saying. • The person may be comforted by having family members present at all times. However, because it can be exhausting to be with a hyperactive delirious person, it may be advisable for the family to take turns, if possible, so they can maintain their own rest and well-being. • Attempt to provide a quiet, restful, calm environment that minimizes sensory stimulation to help reduce the person’s agitation. Nursing Alert Misinterpretation of the symptoms of agitated delirium (e.g. restlessness, grimacing, and/or moaning as uncontrolled pain) and the consequent administration of more opioids can result in aggravation of the agitation and possibly contribute to opioid toxicity. Advise family that moaning and/or agitation may be due to confusion and not necessarily pain. References Breitbart, W., & Cohen, K. (2000). Delirium in the terminally ill. In H.M. Chochinov and W. Breitbart (Eds.), Handbook of psychiatry in palliative medicine (pp. 75-90). New York, NY: Oxford University Press. Brown, S., & Degner, L. F. (2001). Delirium in the terminallyill cancer patient: Aetiology, symptoms and management. International Journal of Palliative Nursing, 7(6), 266-268, 270-272. Lawlor, P., Fainsinger, R., & Bruera, E. (2001). Delirium at the end of life: Critical issues in clinical practice and research. JAMA, 284, 2427-2429. Friedlander, M.M., Brayman, Y., & Breitbart, W. S. (2004). Delirium in palliative care. Oncology (Williston.Park), 18, 1541-1550. Gaudreau, J., Gagnon, P., Harel, F., Trembley, A., & Roy, M. (2005, April). Fast, systematic, and continuous delirium assessment in hospitalized patients: The nursing delirium screening scale. Journal of Pain and Symptom Management 29(4), 368-375. 70 Gagnon, P., Allard, P., Masse, B., & DeSerres, M. (2000). Delirium in terminal cancer: A prospective study using daily screening, early diagnosis, and continuous monitoring. Journal of Pain and Symptom Management, 19(6), 412-426. Grealish, L. (2000). Mini-Mental State Questionnaire: Problems with its use in palliative care. International Journal of Palliative Nursing, 6(6), 298-302. Dyspnea 49. What is dyspnea? What are the causes of dyspnea? Dyspnea is a subjective discomfort related to breathing involving the perception of breathlessness and the person’s reaction to it. Dyspnea is not the same as tachypnea or hypoxia. A person’s expression of dyspnea may not necessarily correlate with his or her respiratory rate or oxygen saturation. Breathing can be compromised by problems with inhalation, ventilation, perfusion, transportation, diffusion, utilization, and/or metabolism. Dyspnea can be a very distressing symptom for the ill person and his/her family. Causes The causes of dyspnea can be multifactorial including any of the following: Pulmonary causes • Obstruction (e.g. tumour blockage, COPD, emphysema, or chronic bronchitis), • Restriction (e.g. pulmonary fibrosis), • Consolidation of lung tissue (e.g. pulmonary parenchymal lesion, pneumonia or cystic fibrosis), • Collapsed lung or atelectasis, • Pleural effusion(s), • Pleural-based tumour, • Lymphangitic carcinomatosis, 71 • Lung damage secondary to treatment (e.g. chemotherapy or radiation therapy), • Lobectomy or pneumonectomy. Cardiovascular causes • Obstruction of pulmonary blood vessels (e.g. pulmonary embolus, pulmonary edema or superior vena cava syndrome), • Pericardial effusion, • Anemia, • Heart failure, • Cardiomyopathy. Other causes • Myopathy (e.g. multiple sclerosis, muscular dystrophy, or amyotrophic lateral sclerosis), • Anorexia cachexia syndrome (e.g. persons with advanced cancer, renal or cardiac failure, or AIDs), • Elevated diaphragm (e.g. secondary to ascites, liver metastases, or a collapsed lung), • Emotional distress (e.g. anxiety, panic attacks, and/or depression). 50. How is dyspnea assessed? Assessment 1. History Ask the person the following questions: – Intensity: How severe is the shortness of breath? Use a 0-10 rating scale or visual analogue scale, such as that used in the ESAS-r (see Appendix A). How distressing is it at rest? At worst? At best? – Quality: Describe how it feels (e.g. is it tightness in the chest, not getting enough air like suffocating or drowning)? – Onset: When did the breathlessness start? Is it related to activity? – Duration: When did the dyspnea start? How long does each episode of breathlessness last? – Frequency: How often is shortness of breath experienced? 72 – Aggravation: What makes it worse? What activities cause shortness of breath? – Alleviation: What makes it better? How is it managed? – Impact: Is there suffering when breathing? How has the breathlessness affected the ability to function? Quality of life? 2. Physical assessment: Identify objective signs of respiratory impairment. Although they are not necessarily indicative of dyspnea, they may help identify the etiology. Observe for the following: – Signs including increased respiratory rate, respiratory pattern (abdominal or apical chest movement), cyanosis (central and/or peripheral), restlessness, facial expression, nasal flaring, use of accessory muscles, intercostal/suprasternal/ supraclavicular indrawing, tracheal tug, an inability to complete full sentences, gasping during eating and possible gagging, coughing and/or expectorating. – Palpate bony structures to detect bone metastasis or fractures, pain over chest wall, equal chest wall movement bilaterally. – Percuss lung fields to detect consolidation, effusion, or collapse. – Auscultate to assess for alterations in air entry and/or adventitious breath sounds (e.g. crackles, wheezes, and/or rubs). 3. Investigations: Oxygen saturation, blood work (e.g. hemoglobin, WBC), diagnostic procedures (e.g. chest x-ray, CT of chest, ECG, VQ scan, ABGs, and pulmonary function tests). 73 51. What are the interventions for dyspnea? Non-Pharmacological Interventions • Provide reassurance (e.g. calm environment and information). • Allow person to assume any body position which provides relief, usually leaning forward sitting with arms supported on a table. High Fowler’s position works well for fatigued or unconscious persons (be sure elbows are supported). • Allow person to breathe as quickly as they feel they need to through mouth or nose, regardless of presence of supplementary oxygen. Once their breathing begins to slow down and becomes more relaxed, encourage diaphragmatic breathing and/or pursed lip breathing. • Increase ventilation (e.g. a fan blowing across the face or over a bowl of ice, open a window) • Provide relaxation therapy, massage to upper back and arms, or distraction. • Provide oxygen therapy if the person is hypoxemic or has a low oxygen saturation (i.e. titrate oxygen to relieve symptoms as oppposed to achieving a particular oxygen saturation level). Be cautious of providing high flow oxygen to people with chronic obstructive pulmonary disease (COPD) as the drive to breathe may depend on their carbon dioxide level. • Provide cool mist humidity. • Maintain good oral hygiene. • Teach energy conservation strategies (See Appendix E). • Offer chest physiotherapy – may be useful in persons with chest congestion to help mobilize sputum. Use caution in persons with compromised bone structure (e.g. bone metastases or osteoporosis). • Consider radiation therapy – may help relieve obstruction or inflammation secondary to tumour. • Transfuse packed red blood cells – may alleviate anemia. • Consider thoracentesis/pleurodesis – may reduce the work of breathing secondary to pleural effusion(s). 74 Nursing Alert Suctioning has a limited role and potential benefits need to be weighed against the risks (e.g. stimulating further secretions). Pharmacological Interventions The following interventions target the cause of dyspnea: • Antibiotics may relieve symptoms associated with chest infection. • Bronchodilators (e.g. Salbutamol sulphate (Ventolin ®) 2.5-5mg via nebulization every 4 hours as needed, maximum dose 6 inhalations in 24 hours). May alleviate obstructive bronchoconstriction secondary to COPD or asthma. • Cough suppressants (e.g. Dextromethorphan 10–20mg PO every 4 hours, maximum dose 120mg in 24 hours; Codeine 1560mg PO/subcut every 4 hours; or Morphine 1.5-5mg PO/subcut every 4 hours as needed). Cough suppressants are useful for relief of a persistent dry cough. • Diuretics are useful if dyspnea is caused by pulmonary or hepatic congestion. However, diuretics must be used cautiously in most palliative persons as the risk of dehydration may outweigh any potential benefit. • Expectorants (e.g. Guanifesin 200-400mg PO every 4 hours, maximum dose 2400mg in 24 hours). Expectorants are useful for dyspnea associated with a productive cough. • Steroids (e.g. Dexamethasone (Decadron ®) 4-10mg PO/subcut 1 to 4 times daily or Prednisone 10-40mg PO daily). Steroids may prove useful when dyspnea is secondary to obstruction (e.g. superior vena cava syndrome, radiation therapy fibrosis, lymphangitic carcinomatosis, or COPD exacerbation). • Chemotherapy may help relieve dyspnea associated with obstruction or inflammation by shrinking tumour bulk. • Anticoagulants may reduce dyspnea if caused by pulmonary emboli. 75 Symptomatic Pharmacological Interventions • Opioids may help decrease the perception of breathlessness. If the person is receiving opioids regularly for pain, breakthrough doses of the same opioid can be given for dyspnea. In the absence of opioids for analgesia, Morphine 2-10mg PO or 1-5mg subcut every hour as needed may be ordered for dyspnea. Titrate to effect. For the opioid naïve or frail person, opioids should be started at a lower dose and titrated based on response. If 3 or more doses are required in a 24-hour period, a regular dose around the clock (ATC) is recommended (see Question 6). If a more rapid onset of action is required, use Fentanyl SL/subcut 12.5 - 25 mcg every hour as needed. This opioid can ease dyspnea quickly as it acts within 5 minutes to reduce the perception of dyspnea and is metabolized within 30 minutes. Fentanyl is useful if given prior to activity-related dyspnea or for breakthrough dyspnea. Avoid nebulized opioids as research has not proven effect. • Anxiolytics are rarely needed for dyspnea if the underlying cause has been treated. Many times the cause cannot be treated, thus an anxiolytic can be effective when used in conjunction with an opioid to reduce dyspnea. With severe dyspnea, methotrimeprazine (Nozinan®) may be effective. If dyspnea continues or is considered intractable, palliative sedation may be appropriate (See Question 76). Nursing Alert When a person has become unresponsive and appears to be actively dying, it is appropriate to speak to family about discontinuing life-prolonging measures, including oxygen. 76 References Galbraith, S., Fagan, P., Perkins, P., Lynch, A., Booth, S. (2010). Does the use of a handheld fan improve chronic dyspnea? A randomized, controlled crossover trial. Journal of Pain and Symptom Management, 39(5), 831-838. Gauna, A. A., Kang, S. K., Triano, M. L., Swatko, E. R., & Vanston, V. J. (2008). Oral transmucosal fentanyl citrate for dyspnea in terminally ill patients: An observational case series. Journal of Palliative Medicine, 11(4), 643-648. Jennings, A. L., Davies, A. N., Higgins, J. P. T., & Broadley, K. (2001). Opioids for the palliation of breathlessness in terminal illness. The Cochrane Database of Systemic Research. Payne, D. K., & Massie, M. J. (2000) Anxiety in palliative care. In H. M. Chochinov and W. Breitbart (Eds.), Handbook of Psychiatry in Palliative Medicine (pp. 63-74) New York: NY. Pinna, M., Vargas, R., Moralo, M., Correas, M., & Blanco, G. (2009). Dyspnea - a bad prognosis symptom at the end of life. American Journal of Hospice and Palliative Care, 26(2), 89-97. Rocker, G. M., Sinuff, T., Horton, R., & Hernandez, P. (2010). Advanced chronic obstructive pulmonary disease: Innovative approaches to palliation. Journal of Palliative Medicine, 10(3), 783-797. Edema, Ascites, and Lymphedema 52. What are edema, ascites, and lymphedema? What are the causes? Edema, ascites, and lymphedema are abnormal accumulations of excess fluid within soft tissue or cavities secondary to obstruction, loss of protein, and/or organ failure (e.g. hepatic, renal, and/or cardiac failure). In the final stage of an illness, a large percentage of people will experience problems associated with fluid accumulation. Edema is an accumulation of fluid within soft tissue that typically presents in dependent areas (e.g. lower extremities in mobile persons, the sacrum, and/or scrotum in bed-ridden persons). 77 The causes of edema are multifactorial including loss of protein, compression of vascular or lymphatic systems, and organ failure. There is a risk of infection because of the composition and stagnant nature of the fluid. Lymphedema is an accumulation of fluid within soft tissue characteristically found in limbs affected by disease and/or treatment, and is not necessarily dependent on position. Prevention is vital. Although the resolution of lymphedema is possible, once it occurs, it tends to be a chronic condition. If detected early, it is possible to reverse the progression of lymphedema. Clinical signs are discomfort, heaviness and weakness of limbs, a sensation of tightness, and lack of flexibility. The cause of lymphedema is usually multifactorial; any of the following may obstruct or interrupt the lymph channels: • Surgery (e.g. node dissection), • Radiation therapy, • Infection and/or • Obstruction secondary to tumour or ascites. Ascites is the accumulation of excess fluid within the abdominal cavity. Ascites can be caused by tumour cells in the abdomen, tumour invasion resulting in compression of the portal and venous lymphatic systems, decreased protein in the bloodstream, liver disease, or congestive heart failure. Severe ascites is associated with poor prognosis. 53. How are edema, ascites, and lymphedema assessed? Assessment Assessment of edema, ascites, and lymphedema may include any of the following: 1. History – onset, severity, alleviating and aggravating factors, associated symptoms (e.g. dyspnea, constipation, anorexia, early satiety, nausea, vomiting or esophageal reflux), significance to person including concerns about body image and sexuality, altered functional abilities, and psychological concerns such as depression and social isolation. 78 2. Physical Examination − Observe the affected area for alterations in skin and tissue including skin integrity, colour and moisture, signs of infection, distortion of shape, weight gain, and fit of clothing. − Assess temperature. Risk of infection especially with repeated paracentesis is high. − Inspect the abdomen for bloating, distension or bulging flanks. Auscultate for bowel sounds. Percuss to determine the presence and volume of fluid. With ascites, there must be at least 1500 mls of fluid before dullness occurs with percussion. Palpate for abdominal tenderness. − Test for function, range of motion, and mobility. 3. Investigations – CBC and differential, protein and albumin (prealbumin), cardiac and/or liver enzymes, renal function, total bilirubin, chest x-ray, venous doppler, abdominal ultrasound, and/or CT scans. 54. What are the interventions for edema, ascites, and lymphedema? Interventions for edema, ascites, and lymphedema may include any of the following: General Interventions • Determine goals of care with the person and family. • Educate the person and family: explain diagnosis, etiology, and self-care activities. • Provide supportive care and counselling. • Make referrals to rehabilitation therapists. • Provide skin care and attend to positioning. • Reduce the risk of falls as fluid shifts and excessive weight associated with fluid accumulation may cause orthostatic hypotension, as well as alter the person’s centre of gravity. • Avoid insertion of IV or subcutaneous devices in the affected limb or an edematous abdomen. • Avoid blood pressure measurement on affected limbs. • Avoid diuretics as they are often of little value in the treatment of fluid accumulation (e.g. ineffective in shifting fluids in the 79 presence of hypoproteinemia and/or obstruction). A trial of diuretic may be useful in fluid accumulation due to organ failure (e.g. cardiac and portal hypertension). If diuretics are indicated, suggest Spironolactone 25-50mg PO daily in divided doses titrating up to 200mg daily depending on the person’s response and renal function. Edema Interventions • Restrict fluid and sodium if appropriate [e.g. in persons with cardiac related edema or syndrome of inappropriate antidiuretic hormone secretion (SIADH)]. • Elevate limbs. • Use compression stockings (up to 30mmHg for mild edema). Greater compression requires appropriate assessment. Compression stockings and bandages should be discontinued in the event of cellulitis. Tubular supports or antiembolism stockings are too weak and may roll down producing a tourniquet effect. • Mobilize if possible, including passive range of motion and ankle pumps while seated or lying in bed. Lymphedema Interventions • Use of exercise, vibration, massage, manual lymphatic drainage, and/or use of intermittent compression pump (Lymphapress). Intermittent compression pumps may cause rapid diffusion of fluid elsewhere in the body and in conjunction to the pump, the patient will still need to use a compression garment. Pump use may not benefit the person any more than the use of a compression garment alone, and is contraindicated in the presence of infection or thrombosis. • Use a compression garment, a low pressure sleeve, or multilayered compression bandages. Compression bandaging is strongly recommended in the presence of lymphorrhea. Multilayer lymphedema bandaging (MLLB) should not be used in patients with severe arterial insufficiency (ABI <0.5), uncontrolled heart failure, and/or severe peripheral neuropathy. • Provide adequate pain management. 80 Nursing Alert Long term neglected edema such as with venous insufficiency can develop into chronic lymphedema. Ascites Interventions • Manage related symptoms such as constipation (See Question 31), nausea (See Question 44) and/or dyspnea (See Question 51). • Provide paracentesis for recurrent ascites. Despite the potential for fluid volume depletion, protein loss, and the possibility of rapid fluid re-accumulation, symptomatic relief takes priority. Persons who require frequent paracentesis may benefit from the insertion of a permanent catheter. References Dean, M., Harris, J., Regnard, C., & Hockley, J. (2006). Symptom relief in palliative care. United Kingdom: Radcliff Publishing Ltd. Economou, D. (2010) Bowel management: Constipation, diarrhea, obstruction and ascites. In B. Ferrell & N. Coyle (Eds.), Oxford textbook of palliative nursing (3rd edition, pp. 269-289). New York, NY: Oxford University Press. Fu, M., & Smith, J. (2010). Lymphedema management. In B. Ferrell & N. Coyle (Eds.), Oxford textbook of palliative nursing (3rd edition, pp. 341-358). New York, NY: Oxford University Press. Hospital Pharmacists’ Special Interest Group in Palliative Care. (2009). Care beyond cure: Management of pain and other symptoms (4th ed.) Ottawa, Canada: Canadian Society of Hospital Pharmacists. Mason, W. (2000).Exploring rehabilitation within lymphedema management. International Journal of Palliative Nursing, 6(6), 265-273. McNamara, P. (2000). Paracentesis – An effective method of symptom control in the palliative care setting? Palliative Medicine, 14, 62-64. Pereira, J. L. & Associates. (2008). The Pallium palliative pocketbook: A peer-reviewed, referenced resource. (1st Cdn. Ed.) Edmonton, Canada: The Pallium Project. Smith, S. (2000). Hospice concept: A guide to palliative care in terminal illness. Champaign, Il: Research Press. 81 Care of the Integument 55. Should bed-bound people be repositioned regularly? Yes. Repositioning and providing skin care remain important comfort measures throughout the last days, or even hours, of life. A person with advanced disease, limited mobility, and cachexia is at risk for developing, or may have already developed, bedsores, particularly if he or she is immobile. Repositioning reduces this risk, lessens the discomfort of bedsores, and can also help to prevent stiff joints and muscles. Identify persons at risk for pressure ulcers by using a risk assessment tool (e.g. Braden or Norton Scale for predicting pressure sore risk). Implement strategies to reduce this risk (e.g. use pressure relieving surfaces for beds and chairs, manage incontinence, avoid infection, and educate caregivers). Interventions • Reposition the person very gently, a few inches at a time. A draw sheet under a bed-bound person can be used to turn or lift. With the person lying on his or her back, “cradle” them by placing pillows under the draw sheet along each side, thus providing just enough lift to keep the bones of the spine and hips from resting fully on the bed. • Administering regular or breakthrough analgesic before repositioning may minimize discomfort on movement. • Explore the use of specialty mattresses and/or beds that may decrease the potential for skin breakdown and reduce discomfort with movement. Nursing Alert If repositioning causes a person pain, consider giving pain medications prior to turning. 82 56. What is pruritis? What causes it? Pruritis is the cutaneous sensation of itchiness that can be fleeting, intermittent, or constant. It can be multifactorial. Causes Dermatological • Psoriasis, • Infectious processes (e.g. mycosis fungoides or parasitic infections). Systemic • Biliary and/or hepatic diseases (e.g. primary biliary cirrhosis or extrahepatic biliary obstruction, resulting in deposition of bile salts in the skin), • Renal diseases (e.g. chronic or end-stage renal disease, resulting in deposition of urea in the skin), • Hematologic diseases (e.g. lymphoma or multiple myeloma), • Infectious processes (e.g. HIV or syphilis), • Endocrine or metabolic processes (e.g. diabetes, thyroid insufficiency or vitamin and mineral deficiency), • Neurological diseases (e.g. herpes zoster or peripheral neuropathies), • Connective tissue disorders (e.g. lupus or graft versus host disease). Iatrogenic • Medication side effects (e.g. opioids, antibiotics, allergies), • Treatment side effects (e.g. radiation therapy). Psychological • Anxiety or nervousness. 83 57. How is pruritis assessed? What are the interventions? Assessment 1. History – location, quality, intensity, timing (onset, duration, and constancy), associated symptoms, aggravating, alleviating and environmental factors (e.g. use of new products), and significance to person. Medication and allergy review. 2. Physical Examination – assess affected areas for the presence and distribution of rashes, skin integrity, infection, bleeding, serous fluid leakage, and colour changes. 3. Investigations – CBC and differential; total bilirubin; blood glucose; renal, hepatic and thyroid function tests; fungal, bacterial and viral swabs; and possibly a skin biopsy. Non-Pharmacological Interventions • Maintain good hygiene as perspiration and accumulation of waste on the skin increases itchiness. Tepid baths are usually best tolerated; avoid soap and other drying agents. • Dress in loose fitting, cotton clothing. • Maintain cooler rather than warmer room temperature. • Apply oatmeal-colloidal lotions (e.g. Aveeno®). • Apply moisturizers (e.g. Menthol in aqueous cream or Sarna cream). • Use TENS for neurological causes. Pharmacological Interventions • Antihistamines such as Cetrizine (Reactine®) 5-10mg PO every day, maximum dose is 20mg in 24 hours; Diphenhydramine (Benadryl®) 25-50mg PO every 4-6 hours, maximum dose is 400mg in 24 hours; or Hydroxyzine (Atarax®) 10-25mg PO 3-4 times daily, maximum dose 100mg in 24 hours. Note Benadryl ® and Atarax ® are more sedating. • Topical or systemic steroids such as Dexamethasone (Decadron®) 2-4mg PO/subcut daily if pruritis is intractable. • Doxepin (Sinequan®) 10-30mg PO at bedtime. Doxepin topical may be applied thinly 4 times daily for uremic pruritis. 84 • Cholestyramine (Questran®) 4 grams PO daily up to 1- 4 times daily (titrate), maximum dose is 24 grams in 24 hours. May relieve pruritus secondary to partial biliary obstruction or uremia. • Erythropoietin, Ultraviolet B phototherapy, or Gabapentin (Neurontin®) 125-300mg PO daily. Typically given post-dialysis for uremic pruritus. • Ondansetron has been shown to be very effective when given IV followed by PO. • Stent insertion with internal or external drainage and/or Dexamethasone (Decadron®) 12-16mg PO/subcut daily for pruritus due to biliary obstruction. • Other disease-specific drugs and therapies for pruritus caused by specific systemic or dermatologic diseases e.g. treatment for lymphoma or psoriasis. • Discontinuation or adjustment of medications for pruritus caused by medications. 58. What is a malignant wound? How is it assessed? A malignant wound is a break in the epidermal integrity caused by the infiltration of malignant cells. Persons with cutaneous lesions are at highest risk for developing malignant wounds. Radiation therapy, surgery, and chemotherapy can also contribute to malignant wound formation. Assessment 1. History – location, quality, radiation therapy, severity, timing (onset, duration, constancy), associated symptoms, aggravating and alleviating factors in relation to wound pain/discomfort; significance of wound and wound discomfort to person, therapies/treatments used in past and presently as well as their effectiveness. Complete a review of medications. 2. Physical Examination – assess the location, size and depth of the wound, condition of surrounding skin, appearance of the wound bed and margins, the type of tissue present (necrotic, 85 sloughing, granulating, epithelializing), amount and quality of drainage, episodes of bleeding, signs of infection, presence of odour, and presence of subcutaneous masses. 3. Investigations – CBC and differential, swabs for culture and sensitivity, blood culture, and possibly a biopsy. Nursing Alert A malignant wound can change rapidly. Regular assessment using valid and reliable tools is therefore essential. Consider a referral to an Enterostomal Therapist or a nurse specializing in wound management. 59. What are the interventions for a malignant wound? Interventions • Treat infection with systemic antibiotics. • The goal in malignant wound care is to minimize the associated symptoms including: pain, odour, exudate, and/or bleeding. The goal is not necessarily to heal the wound. − Managing the individual’s pain related to the wound and during dressing changes is very important. Since the pain may be deep in nature or neuropathic, it should be managed by systemic therapy. However, procedural pain caused by dressing changes may require additional treatment of mixing an opioid analgesic into a topical gel. − Metronidazole 0.75% gel has been shown to be very effective in controlling odour caused by anaerobic bacteria when applied in a thin layer to the wound. Alternatively, a solution made from crushed metronidazole tablets and sterile water (e.g. 0.5% solution/5mg/mL or 1% solution10mg/mL) can be used to irrigate the wound, or to soak gauze to be placed on or packed into the wound cavity. − Managing exudates and controlling bleeding is critical in caring for these wounds, and can be achieved through the use of specialized wound products. 86 • Consider radiation therapy to reduce tumour bulk and/or stop bleeding. • Avoid commercial deodorizers. Essential oils such as oil of clove and environmental filters may provide some odour control. Odour absorbing dressings (e.g. charcoal), as well as odour absorbing materials (e.g. pumice stones or cat litter) placed in the room may also be effective in reducing odour. • Emotional support to the person and his or her caregiver is vital as the impact of odour and pain can interfere with the selfesteem of the person and his or her relationships. Nursing Alert Refer to your organization’s procedures and policies for site specific interventions for wound care. References Chaplin, J. (2004). Wound management in palliative care. Nursing Standard, 19(1), 39-42. Naylor, W. (2003). Palliative management of fungating wounds. European Journal of Palliative Care, 10(3), 95 Ferrell, B. R., & Coyle, N. (2010). Oxford textbook of palliative nursing, (3rd ed.). New York: Oxford University Press. 87 Oral Conditions 60. What contributes to taste changes? What are the dietary interventions? Changes in taste may result from disease, malnutrition (e.g. protein, vitamins, or zinc deficiencies), and/or mouth complications (e.g. candidiasis, xerostomia, neurological damage dental pathology, medications, chemoradiotherapy, or surgical interventions). Dietary Interventions Suggestions for changes in taste: • Try foods that leave their own taste (e.g. fresh fruit and mints). • Add spices or sauces to enhance the food flavour if taste sensation is decreased. • Experiment with tart foods such as citrus juices, lemonade, cranberry juice, and/or pickles. 61. What are xerostomia (dry mouth) and stomatitis (sore mouth)? What are the causes? Xerostomia is the subjective feeling of dryness of the mouth, lips, gums, tongue, and/or palate dryness. If these symptoms are left untreated, xerostomia may lead to stomatitis. Stomatitis is the inflammation of the mouth characterized by red, shiny, and edematous gums, tongue, and palate. Advanced stages of stomatitis are frequently characterized by shallow ulcerative lesions with white plaques. Predisposing factors of xerostomia and stomatitis include: • Decrease in saliva. • Dehydration secondary to diarrhea, anorexia, oxygen therapy, vomiting, and decreased fluid intake. • Poor oral hygiene, mouth breathing, and poor fitting dentures. 88 Causes • Treatment such as radiotherapy, medications (e.g. opioids, tricyclic antidepressants, anticholinergics, diuretics, and chemotherapy). • Tumour infiltration. • Erosion of the buccal mucosa by disease or treatment. • Infection – Fungal (e.g. candidiasis) – Bacterial (e.g. gingivitis) – Viral (e.g. herpes simplex) 62. How are xerostomia and stomatitis assessed? What are the interventions? Assessment 1. History – oral dryness, pain or discomfort including intensity, timing (onset, duration, constancy), associated symptoms, aggravating and alleviating factors, and significance to person. Complete a medication review. 2. Physical Examination – examine the oral pharyngeal cavity including gums, palate, tongue, buccal mucosa, dentition, and lips. 3. Investigations – CBC and differential, bacterial, fungal and viral swabs, and possibly a biopsy. General Interventions • Maintain clean, moist mouth and lips. When appropriate, use an ultra-soft toothbrush (child’s size least traumatic) or sponge tipped swab dipped in carbonated soda water for regular mouth care. Be sure to brush all surfaces of the tongue, roof of the mouth, gums, and inside of the cheeks, in addition to all surfaces of the teeth. If a toothbrush is not available, use gauze wrapped around a finger and dipped in carbonated soda water. Toothpaste is not essential, but, if desired, a mild formulation works best. • Provide mouth care before and after meals, at bedtime or routinely with other nursing care, such as regular repositioning. 89 • Offer frequent sips of water, small ice chips, ice cubes made with club soda, frozen fruit chunks such as pineapple or grapes, frozen juice, and/or popsicles. • Suggest sugarless gum, mints, or hard candy to stimulate production of saliva. • Avoid the use of petroleum products and glycerine products; use water-soluble lubricants or lip balms. • Avoid mouthwashes containing alcohol, baking soda, or hydrogen peroxide as they can be dehydrating, abrasive, and/or damaging to the oral mucosa. Use “soda water” with carbonation or sodium chloride as a cleansing rinse. Chlorhexidene 0.12% oral rinse may also be used, especially if the person is at high risk for oral infection. • Ensure dentures are properly fitted. Remove dentures for cleaning and possibly overnight. • Provide humidification in the person’s room. Nursing Alert These interventions and dietary suggestions may only be effective for the milder form of these oral conditions. General Dietary Interventions • Offer soft foods such as cooked cereal, pancakes, soft pasta dishes, soft fruit, puddings, ice cream, well-cooked vegetables, eggs, fish, casseroles, and milkshakes. • Add butter, margarine, gravy, sauces, or soups to help soften and moisten foods. • Drink soups or beverages with meals. • Exercise caution with food and fluid temperature. • Avoid tobacco and alcohol products. Dietary Interventions • Avoid acidic, spicy, salty, and rough textured foods. • Avoid tart foods such as citrus juices, lemonade, cranberry juice or pickles. 90 Pharmacological Interventions • Artificial saliva sprays. • Pilocarpine (Salagen®) 5-10mg PO 3-4 times daily, maximum dose of 30mg per day. • Viscous Xylocaine or Pink Lady (Viscous Xylocaine 2% and Maalox®). • Tantum oral rinse (15ml swish for 1-3 min every 4 hours ATC). • Antifungal such as Nystatin (Mycostatin ®) mouth rinse 500,000 units swish and swallow after meals and at bedtime (QID). Fluconazole 100mg PO/IV daily for 5-7 days. Ketoconazole 200mg PO twice daily for 5-7 days. • Antivirals such as Acyclovir 200mg PO q4h 4-6 times daily for 10 days. Famcyclovir 500mg PO 3 times daily for 7 to 10 days. • Antibiotics (e.g. Clindamycin, Amoxicillin or Metronidazole). • Systemic analgesics may be appropriate in the setting of severe stomatitis. Nursing Alert Be cautious of the risk of aspiration with the use of viscous Xylocaine before eating. The throat may be anesthetized and the ability to swallow safely impaired. Encourage the person to sit upright with the chin tucked down when eating or drinking and observe closely for signs of aspiration. References Chalmers, J., & Johnson, V. (2004). Evidence-based protocol: Oral hygiene care for the functionally dependent and cognitively impaired older adult. Journal of Gerontological Nursing, 30(11), 5-12. Langhorne, M., Fulton, J. & Otto, S. (2007) Oncology Nursing (5th ed.) St. Louis, Mosby. Sweeney, M. P., & Bagg, J. (2000). The mouth and palliative care. American Journal of Hospice and Palliative Care, 17(2), 118-124. 91 Fatigue 63. What is fatigue? What are the causes? Fatigue is a complex multifactorial syndrome that develops over time and is characterized by physical, mental, and psychological effects that reduce capacity and impact quality of life. The prevalence of fatigue in patients with cancer is 70-100%, but it is also very common in persons with other advanced illnesses such as renal failure, HIV/AIDS, and advanced cardiac disease. Causes • Effects of disease (e.g. cancer, HIV/AIDS or COPD), • Medical treatments and their related side-effects, • Underlying medical conditions (e.g. infections, anemia, and/or hypoxia), • Metabolic and/or electrolyte imbalances, • Sleep disturbances, • Inactivity or immobility, • Poor symptom management, • Psychosocial and spiritual distress, • Anorexia cachexia syndrome (See Question 24). 64 How is fatigue assessed? What are the interventions? Assessment 1. History – physical and mental fatigue, quality (e.g. tiredness or exhaustion), severity, timing (onset, duration, constancy, daily pattern), sleep history, psychosocial or spiritual distress, associated symptoms, aggravating and alleviating factors, and significance to person (distress or impact). Review the medications. 2. Physical Examination – general appearance, level of alertness, vital signs, strength, tone, and reflexes in extremities, and ability to complete activities of daily living. 3. Investigations – CBC and differential, glucose, thyroid function, metabolic and electrolyte screen. 92 Non-Pharmacological Interventions • • • • • • • • Referral to physiotherapist and/or occupational therapist, Education, Energy conservation and restoration (see Appendix E), Balance between activity and rest, Sleep hygiene, Nutrition and hydration management, Stress management, Cognitive and behavioural strategies (e.g. relaxation therapy, hypnosis, delegating, and setting limits), • Psychosocial and/or spiritual counselling and support. Pharmacological Interventions • Manage the underlying medical conditions (e.g. infections, anemia, hypoxia, anorexia cachexia syndrome, and metabolic abnormalities). • Minimize medication side effects (e.g. early morning administration of steroids and diuretics). • Manage symptoms that can increase fatigue (e.g. pain, nausea, shortness of breath). • Use medications such as Progestogens, Methylphenidate, and Modafinil when non-pharmacological methods are ineffective. References Bender, C., Kramer, P., & Mraskowski, C. (2002). Cognitive Impairment, In New directions in the management of cancerrelated cognitive impairment, fatigue, and pain. Bridgewater, NH: Ortho Biotech. Dean, M., Harris, J., Regnard, C., & Hockley, J. (2006). Symptom relief in palliative care. United Kingdom: Radcliff Publishing Ltd. Hospital Pharmacists’ Special Interest Group in Palliative Care. (2009). Care beyond cure: Management of pain and other symptoms (4th ed.) Ottawa, Canada: Canadian Society of Hospital Pharmacists. Larsen, D., & Mallett, L. (2010). Gastrointestinal symptoms. In M. Matzo & D. Witt Sherman (Eds.), Palliative care nursing: Palliative care to the end of life (3rd edition, pp. 463-487). New York, NY: Springer Publishing Company LLG. Nail, L. N. (2002). Fatigue in patients with cancer. CLOR, 29(3), 537542. Stone, P., Richardson, A., Ream, E., Smith, A. G., Kerr, D.J., & Kearney, N. (2000). Cancer-related fatigue: Inevitable, unimportant and untreatable? Results of a multi-centre patient survey. Cancer Fatigue Forum. Annals of Oncology, 11(8), 971- 975. 93 Circulatory Conditions 65. What are the causes of hemorrhage? Hemorrhage and exsanguination are rare complications for the person living with life-limiting illness. Significant bleeding occurs in 6% to 10% of persons with advanced cancer. Terminal massive hemoptysis occurs in 3% of persons with lung cancer. Causes • Direct tumour invasion of major vessels in the head, neck, lungs, and gynecological regions are most commonly associated with massive hemorrhage. Metastatic involvement from tumour eroding into major vessels also has the potential to cause massive hemorrhage. • Thrombocytopenia is an abnormally low platelet count. Causes of thrombocytopenia include: low platelet production in the bone marrow, increased platelet breakdown in the bloodstream, and increased platelet breakdown in the spleen or liver. Thrombocytopenia may be found in persons with aplastic anemia, cancer in the bone marrow, cirrhosis, folate deficiency, infections in bone marrow, myelodysplasia, and Vitamin B12 deficiency. Use of certain drugs (e.g. chemotherapy) may cause a reduction in platelet production. Symptoms include bruising, nosebleed, bleeding mouth and gums, and petechiae. • Disseminated intravascular coagulation (DIC) is a disturbance in the blood clotting mechanism characterized by concurrent coagulation and hemorrhage triggered by such factors as transfusion reactions, septicemia, chemotherapy, and substances released by malignant cells. • Liver failure results in disturbances in blood coagulation. It also can interfere with portal circulation contributing to esophageal varicies that are prone to bleeding. 94 66. What are the interventions for hemorrhage? Identifying the underlying cause of hemorrhage is essential in order to determine the appropriate intervention(s). Identify persons with a potential for bleeding (e.g. an ulcerating neck tumour, a tumour in close proximity to large neck arteries, recurrent episodes of bleeding, recurrent rectal or upper GI bleeds or underlying anticoagulation problems). Bleeding is a traumatic experience for the person, family, and staff. Discuss the possibility of hemorrhage with the person and/or family and develop a plan of care. Pharmacological Interventions • Midazolam (Versed®) 5mg subcut repeat every 5 minutes for 3 doses. This may be used for sedation in the event of a massive hemorrhage. • Transexamic acid (Cyklokapron®) 500mg PO 4 times daily may reduce the risk of bleeding. Clinical Tip If bleeding is anticipated, have medications pre-drawn and accessible. The use of a prefilled syringe of midazolam stored near the person will facilitate rapid response. Parenteral midazolam may be stored at room temperature in a dark place for up to 30 days. Non-Pharmacological Interventions • Have a supply of dark coloured towels or blankets ready in or near the person’s room to absorb the blood. Use simple hygiene measures and the dark towels to minimize the visual impact of bleeding. • Provide continuous support to the person and family using a calm and reassuring approach. • Assist the person into a comfortable position. • Consider the goals of care. Hydration may be initiated, especially if bleeding is slow and progressive. 95 • Apply direct pressure to the site if bleeding is external. • Pack the area using an absorbable hemostatic product if the bleeding originates from the nose, vagina, or rectum. • Suction the oropharyngeal area with a soft suction catheter and low suction pressure if gagging becomes a problem. Take care not to exacerbate bleeding or pain. • Give regular analgesics using an appropriate route. Clinical Tip Occasionally the infusion of platelets may be indicated for the person with critically low platelet levels who is actively bleeding (petechiae, hemoptysis). Nursing Alert In event of massive hemorrhage in persons with advanced disease, aggressive treatment to alleviate the cause of bleeding is rarely indicated. Family members and caregivers need to be sensitively informed and prepared for the possibility of a massive hemorrhage. Establish common goals of care with all those involved. 96 67. What are thrombi and emboli? What are the causes? Thrombi are blood clots that form in a vessel or within the heart and remain there. Emboli are obstructions in a blood vessel that travel from vessels or heart chambers to other vascular locations. Emboli and obstructing materials may develop from various causes, including air, blood, fat, tissue, and/or bacteria. Causes Coagulopathy is common in cancer and may often be the presenting symptom of cancer. Causes of thrombus formation include abnormalities related to any of the following: • Blood flow due to bed rest, vascular compression by tumours, or hyperviscosity of blood. • Vessel wall damage due to tumour invasion or trauma. • Blood composition due to elevated serum levels of coagulation factors and increased circulating activated coagulation factors. 68. How are thrombi and emboli assessed? What are the interventions? Assessment 1. History – consider cough, location of clot, pain, and dyspnea (e.g. including quality, intensity, onset, associated symptoms, aggravating and alleviating factors). Review medications. 2. Physical Examination – observe the circulation to affected limbs, signs of edema, temperature, colour, vital signs, mobility, and respiratory function. 3. Investigations –- CBC and differential, PT or INR, PTT, D-dimer, electrolytes, renal and hepatic function, doppler, and/or spiral CT scan. 97 Non-Pharmacological Interventions • Encourage frequent position changes to prevent the development of thrombi and emboli. • Encourage bed rest initially (e.g. high Fowler’s for persons with pulmonary emboli). • Immobilize affected limbs initially. • Avoid warm compresses and massaging the affected area(s). • Consider compression stockings. • Address associated symptoms (e.g. provide oxygen and/or analgesic as required). • Consider the insertion of an IVC filter. • Consider invasive surgery as last resort. Pharmacological Interventions • Consider anticoagulant therapy for an existing clot and prophylaxis for persons with decreased mobility. The choice of an anticoagulant depends on the ease of administration and minimizing the burden of blood monitoring. References Harris, D. G., & Noble, S. I. R. (2009). Management of terminal hemorrhage in persons with advanced cancer: A systematic review. Journal of Pain and Symptom Management, 38(6), 913-926. Pereira, J. (2004). Management of bleeding in person with advanced cancer. The Oncologist, Symptom Management and Supportive Care, 9, 561-570. Prommer, E. (2005, June). Management of bleeding in the terminally ill person. Hematology, 10(3), 167-175. Sarhill, N., Walsh, D., Nelson, K., & Davis, M. (2001). Evaluation and treatment of cancer-related fluid deficits: Volume depletion and dehydration. Supportive Care in Cancer, 9(6), 408-419. 98 Spinal Cord Compression 69. What is spinal cord compression? What are the causes? How is it assessed? Spinal cord compression (SCC) is a serious neurological problem and considered a palliative emergency. SCC occurs when a spinal cord tumour or metastatic tumour grows in the spine and destroys the bony vertebral body that surrounds the cord, or wraps around the spinal cord and its nerve roots. If the vertebral body collapses, it puts pressure on and compresses the spinal cord, leading to swelling, cord injury, and possibly permanent paralysis. With early detection and treatment, paralysis may be prevented. Causes Spinal cord compression is most often associated with cancers that tend to spread (metastasize) to the bone, including breast, lung, prostate, kidney, multiple myeloma, and lymphoma. Clinical Tip Early recognition and diagnosis of spinal cord compression before neurological deficits occur results in the best treatment outcomes. Assessment 1. History Back pain, include location, quality, intensity, and onset. The most common presenting symptom is steady and progressive back pain that may radiate from the cervical spine, down the arms, and/ or around the thorax creating a band-like pressure. It may also radiate from the lumbar or sacral area resulting in pain in the lower extremities. The pain may be aggravated by movement, coughing, straining, or lying down. It may also be provoked by gentle neck flexion or straight leg raises. Complete a medication review. 2. Physical Examination • Palpate the spine for point tenderness. • Complete a neurological examination including muscle strength (often reduced), deep tendon reflexes (may be or ), sensation, rectal tone – Sensory changes include numbness, tingling, and coldness in the affected extremities. 99 – Motor changes may include weakness and ataxia. – Autonomic dysfunction including urinary hesitancy or incontinence, constipation, reduced rectal tone, sexual dysfunction. 3. Investigations – Urgent MRI is the investigation of choice. If an MRI cannot be done, CT scan. 70. What are the interventions for spinal cord compression? Interventions • Dexamethasone (Decadron®) 8-10mg PO/subcut 2-4 times daily. Reduce rapidly to lowest effective dose. • Consult neurosurgery for spinal decompression and stabilization. • Consult radiation oncology. Radiation may alleviate pressure on the spinal cord from the tumour to prevent progression resulting in permanent paralysis. The full pain-relieving benefits of RT may not be achieved until about 10-14 days following treatment. Nursing Alert Delay in treatment may leave the person paralyzed and without bowel and bladder control. Action may not result in the prolongation of life; however, it can impact the person’s quality of life. References Canadian Cancer Society. (2013). Spinal Cord Compression. Retrieved from www.cancer.ca. Drudge-Coates, L. & Rajbabu, K. (2008). Diagnosis and management of malignant spinal cord compression: Part 1. International Journal of Palliative Nursing, 14(3), 110-112, 114-5. Drudge-Coates, L. & Rajbabu, K. (2008). Diagnosis and management of malignant spinal cord compression: Part 2. International Journal of Palliative Nursing, 14(4), 175-180. Schulmeister, L. & Gatlin, C. G. (2008) Spinal cord compression. In Gates, R. A. & Fink, R. M. (Eds.) Oncology Nursing Secrets (3rd ed., pp.546-550). St Louis: Mosby Elsevier. 100 Superior Vena Cava Syndrome 71. What is superior vena cava syndrome? What are the causes? How is it assessed? Superior Vena Cava (SVC) Syndrome is compression of the superior vena cava resulting in the reduction of blood flow from the head, neck, arms, and thorax to the heart. Causes • The most common cause is cancer. Cancers of the lung, lymphoma, or metastases to the mediastinum can cause compression of the superior vena cava. • Another cause, although uncommon, is thrombi formation within the superior vena cava. Assessment 1. History – quality, severity, intensity and onset, associated cardiac/pulmonary symptoms, and aggravating and alleviating factors. Complete a review of medications. Consider the following symptoms: • Upper extremities and/or tightness of throat, • Shortness of breath and orthopnea, • Chest pain, tachycardia, and/or cough, • Feeling of fullness in the head or headache, dizziness, visual disturbances and/or nausea. These may worsen when leaning forward. 2. Physical Assessment – examine head, chest, upper extremities, and respiratory/cardiac function. Take note of the following signs: • Flushing of the face, and swelling/edema of the face, neck, or arms, dilatation of the neck and chest veins, • Hoarseness, stridor, nasal congestion, cough, increased respiratory rate. 2. Investigations – chest x-ray, thoracic CT scan, Doppler, venography, or MRI imaging. 101 72. What are the interventions for superior vena cava syndrome? Interventions • • • • Provide information and support, Position to relieve dyspnea, Provide oxygen therapy, Administer dexamethasone (decadron®) 8-10mg po/subcut 2-4 times daily. Reduce rapidly to lowest effective dose. • Consider radiation and/or chemotherapy, • Administer opioids for pain or dyspnea as required, • Avoid insertion of IV or subcut devices in affected limbs or chest. References Wan, J. F. & Bezjak, A. (2009). Superior vena cava syndrome. Emergency Medical Clinics of North America, 27, 243-255. Wilson, L. D., Detterbeck, F. C., Yahalom, J. (2007). Superior vena cava syndrome with malignant causes. New England Journal of Medicine, 356(18), 1862-1869. 102 Seizures 73. What are seizures? What are the causes? How are seizures assessed? Seizures are characterized by involuntary muscle twitching that result from an abnormal discharge of neurons. Seizures are considered a palliative emergency. Causes Causes of seizures include primary or metastatic cerebral tumours, meningeal malignancy, paraneoplastic syndromes, medications, withdrawal from medications or alcohol, metabolic disturbances, infection, intracerebral hemorrhage, and stroke. Assessment 1. History – initial focus of seizure activity, frequency and extent of motor involvement, intensity, timing (onset, duration, constancy), associated symptoms, aggravating and alleviating factors, history of alcohol or drug misuse. Complete a review of medications (e.g. Phenytoin levels are sensitive to a number of other medications, as well as available protein stores in the body). 2. Physical Examination – consider level of consciousness, incontinence of urine or stool, hypoxemia, motor and sensory changes. 3. Investigations – CBC and differential, glucose, thyroid, metabolic and electrolyte screen, kidney and liver function studies, drug levels and/or toxicology screen, CT head, MRI brain and/or spine, and lumbar puncture. 103 74. What are the interventions for seizures? Interventions • Provide information and support. • Attend to positioning. Place the person in the recovery position; move any objects that might cause injury • Provide oxygen therapy as needed. • Reverse and/or correct identified causes. • Consider seizure prophylaxis including anticonvulsant therapy (e.g. Phenytoin 200-1200mg PO/IV per day in divided doses; Carbamazepine – maximum daily dose is 800-1200mg PO in divided doses; Valproic Acid 1000-2500mg PO per day). All these doses are dependent on the serum level of the drug. If the oral route is not possible, Phenobarbital 30-120mg can be given subcutaneously 2-3 times daily. These drugs may be very sedating. • Manage active seizures with Midazolam (Versed ®) 5 mg subcut/ IV every 5 minutes as needed, Lorazepam (Ativan®) 2mg subcut/IV every 15 minutes as needed, or Diazepam (Valium ®) 2 mg bolus doses up to 10mg IV every 15 minutes as needed. These medications should be given for seizures lasting longer than 2 minutes. References Currow, D., & Clark, K. (2006). Emergencies on Palliative and Supportive Care. Oxford: Oxford University Press. Simonetti, F., & Carcini, A. (2006). Seizures. In E. Bruera, I. J. Higginson, C. Ripamonti, & C. F. VonGunten (Eds.), Textbook of Palliative Medicine (pp. 841-848). Philadelphia: London: Hodder Arnold. Walsh, D., Caracini, A., Fainsinger, R., Foley, K., Glare, P., Goh, C., Lloyd-Williams, M., Nunez Olatre, J., Radbruch, L. (2009). Palliative Medicine. Philadelphia: Saunders Elsevier. Watson, M. S., Lucas, C. F., Hoy, A. M., Block, I. N. (2005). Oxford Handbook of Palliative Care. Oxford: Oxford University Press. 104 Alternative and Complementary Therapies 75. What are alternative and complementary therapies? What are the nursing responsibilities? Alternative therapies are therapies that may be used instead of conventional care. Complementary therapies are therapies used in addition to conventional therapies. Although grouped together, complementary and alternative therapies have some significant differences. Goals of complementary therapies may be to promote relaxation, to reduce stress and anxiety, to relieve pain and other symptoms, to reduce adverse effects of conventional therapies, and to improve sleep. Evidence based complementary therapies have been shown to affect physical, emotional, and spiritual well-being in beneficial ways. Alternative therapies are sometimes considered in place of mainstream cancer therapies such as surgery, chemotherapy and radiation therapies. These therapies are often based on anecdotal rather than research-based evidence and can misguide, raise false hopes, and financially exploit. Alternate therapies may be associated with significant risks. Complementary and alternative therapies are sought for a variety of reasons including: • Enhancing self-care and sense of well-being, • Controlling symptoms, • Reducing fear and anxiety, • Improving quality of life, • Maintaining hope, • Increasing a sense of control, • Yielding to family pressure, • Mistrust of the medical system, and/or • Convenience of accessing information about alternative therapy options on the internet. 105 Nursing Responsibilities • Recognizing the person’s autonomy in decision-making, • Providing information to ensure awareness of evidence-based health care treatment, • Supporting the person’s exploration of therapy in a nonjudgmental manner, • Assisting and encouraging the person to obtain accurate information (e.g. potential risks, benefits, and limitations) and/or potential interactions with other medications or therapies, • Reviewing policies and procedures specific to these therapies, • Encouraging the person to maintain openness with his or her physician regarding the use of these therapies. References Kravats, K., & Berenson, S. (2010). Complementary and alternative therapies in palliative care. In B. Ferrell & N. Coyle (Eds.), Oxford textbook of palliative nursing (3rd edition, pp. 545-565). New York, NY: Oxford University Press. 106 Palliative Sedation 76. What is palliative sedation? What needs to be considered? Palliative sedation is the process of inducing various degrees of unconscious through the use of medications. Palliative sedation can be considered when the person is in the final hours to days of life, and is experiencing severe suffering caused by one or more intractable symptoms. Symptoms are considered intractable when all appropriate interventions have failed to bring adequate symptom relief. The purpose or intent is not to hasten death but to provide comfort and relieve suffering of refractory symptoms. The most common refractory symptoms include refractory dyspnea and agitated delirium. It is less commonly used for refractory pain and vomiting. Use for purely existential/spiritual symptoms is controversial, and should only be initiated in rare cases. Palliative sedation is also known as controlled sedation, continuous deep sedation, prolonged sedation, or sedation for intractable distress in the dying person. The level of palliative sedation can be superficial or deep; intermittent or continuous. Continuous palliative sedation should be considered only in persons with a prognosis of two weeks or less. While palliative sedation is ethically justified based on precepts of dignity, autonomy, beneficence, fidelity, non-maleficence, and the rule of double effect, it can be a complex issue with ethical, emotional, cultural legal, and technical considerations. Palliative sedation is not to be confused with euthanasia (see Question 94). Palliative sedation should only be administered in exceptional cases where refractory suffering is evident and for the person who is close to end of life. 107 Nursing Alert Palliative sedation is used to relieve intolerable and refractory symptoms only when all other therapeutic measures have failed. The expertise required to assess for the suitability of palliative sedation is a specialized skill set requiring advanced education and experience in hospice palliative care medicine. When considering palliative sedation, the following must be addressed: • A terminal disease exists. • A thorough assessment has been conducted to treat reversible symptoms. • The person is suffering from refractory symptom(s). • Pharmacologic and non-pharmacologic approaches to symptom control have been maximized (e.g. titration of opioids for dyspnea and pain, appropriate dosing of neuroleptics for delirium, distraction or relaxation techniques, and counselling in the case of anxiety or dyspnea). • Consultations have been made with Palliative Care Specialists to ensure symptom control strategies have been exhausted. • Goals of care indicate no resuscitation measures to be undertaken. • Prognosis – Is death imminent (hours to days)? Prior to initiating palliative sedation, it is essential to: • Discuss palliative sedation with the person, family, or agent/ proxy named in an advance directive, and the primary physician. • Document the rationale for palliative sedation and the process of consent. • Provide the family with time and opportunity for private conversation before the person enters a deep sleep. • Provide psychosocial support to the family. 108 Clinical Tip The induction and maintenance of sedation is most often achieved through use of a continuous subcutaneous or IV infusion of Midazolam (Versed ®). The Richmond Agitation Sedation Scale (RASS) can be used to assess and titrate sedation. A common starting dose is 1mg per hour, titrated upward to achieve the desired level of sedation. Midazolam 2.5-5 mg subcut may be given as a loading dose. Clinical Tip The minimum dosage required to control the intolerable and refractory symptom(s) should be used (i.e. titrate to clinical effect). If comfort cannot be achieved with one drug, another drug with minimally overlapping disadvantages may be trialed (e.g. methotrimeprazine, phenobarbital). Nursing Alert Opioid analgesics should be continued even when palliative sedation is used. Palliative sedation is reversible by discontinuing the sedating medication. References Beel, A., McClement, S. E., & Harlos, M. (2002). Palliative sedation therapy: A review of definitions and usage. International Journal of Palliative Nursing, 8, 190-199. Cherny, N. I., & Radbruch, L. (2009). European Association for Palliative Care (EAPC) recommended framework for the use of sedation in palliative care. Palliative Medicine, 23(7), 581-593. De Graeff, A., & Dean, M. (2007). Palliative sedation therapy in the last weeks of life: A literature review and recommendations for standards. Journal of Palliative Medicine, 10(1), 67-85. Knight, P. & Epiosa, L. A. (2010). Sedation for refractory symptoms and terminal weaning. In B. R. Ferrell & N. Coyle (Eds.). Palliative Nursing (3rd ed., pp 527-528). New York: Oxford Press Inc. 109 Mercadante, S., Intravaia, G., Villari, P., Ferrera, P., David, F., & Casuccio, A. (2009). Controlled sedation for refractory symptoms in dying persons. Journal of Pain and Symptom Management, 37(5), 771-779. Morita, T. (2004) palliative sedation to relieve psycho-existential suffering of terminally ill cancer patients. Journal of Pain and Symptom Management, 28(5), 445-450. Vogel, L. (2011). Framework urges physicians to proceed with caution on palliative care. Canadian Medical Association Journal, 183(2), 174-175. Walsh,D., Carceni, A.T., Fainsinger, R., Foley, K., Glare, P., Goh, C., Lloyd-Williams, M., Nunez Olarte, J., Radbruch, L. (2009). Palliative Medicine. Philadelphia: Saunders. 110 Part II Psychosocial, Spiritual, Cultural, Ethical, and Legal Issues A NOTE TO CAREGIVERS Although controlling pain and other physical symptoms can be difficult, addressing the emotional and spiritual concerns of the terminally ill person, family, and other caregivers can be equally if not more challenging. Self-awareness for the health professional is important when interacting with persons and families with psychosocial, spiritual, cultural issues, ethical, and legal issues. 111 Family and Coping A family consists of a group of persons emotionally connected with one another. 77. What is helpful to know about the person’s family? Assessment Identify the following: • Individuals the person considers to be family, • Family’s awareness and understanding of medical and other information, amount and type of additional information desired, • Family’s concerns about the illness, • Family’s ability and willingness to participate in care, • Age and developmental stages of family members, • Family rules, values, beliefs, styles, and past experiences that may influence quality of life and the health/illness experience, • Patterns of family communication and methods of decisionmaking, and ability/willingness of family members to openly share information, thoughts, and feelings about the illness experience, • Cultural beliefs and practices that may influence roles, communication or decision making , • Concurrent stressors and coping strategies among individual family members, • Nature of the relationships of each family member with the person since diagnosis and any points of strength or conflict, • Success of role changes within the family, • Availability of social and other support systems, • Strengths identified by the family. Nursing Alert Be careful not to make judgments based on your assumptions of an “ideal” or “normal” family. 112 78. What is coping? What are coping strategies? Coping refers to the cognitive and behavioural strategies used to manage stressful situations and is a multi-factorial adaptation process. Coping is affected by personality traits, personal coping skills, and emotional and cognitive development. It is commonly believed that coping mechanisms used previously by persons and their families will likely be used when faced with life-limiting illness. Some coping strategies might appear less useful, but the person and family may have used them successfully in the past. Common Coping Strategies • Seeking information, • Maintaining a “normal” life, for example, a caregiver continuing to work, • An attitude of “living with instead of dying from” a life-limiting illness, • Disengaging from life or relationships (e.g. withdrawing, becoming depressed or apathetic), • Expressing anger, hostility, guilt, or denial, • Using food, non-prescription medications, or alcohol, • Focusing on the positive and forcing painful thoughts into the unconscious, • Allowing or asking others to make decisions, • Finding meaning in the terminal diagnosis, • Intellectualizing by focusing on facts, • Striving for control. 113 79. Which persons may be at risk for coping poorly? Persons at high risk for coping poorly and/or developing a major psychological disturbance in response to a life-limiting illness may include those persons with: • Limited family or social support, • Unresolved family issues (e.g. estrangement or conflict in relationships), • Recent losses or unresolved grief, • Current or past history of alcohol or drug use, • History of mental or physical illness, • Overwhelming feelings of apathy, hopelessness, despair or helplessness, • Concurrent life crises or situational stressors (e.g. multiple losses or loss of income). 80. How can support be offered to family members? Interventions • Determine how family members have coped with illness in the past. • Explore the person’s and family’s concerns and expectations regarding illness, dying, and death. • Correct misinformation and explore concerns. • Facilitate access to and understanding of medical and other information. Allow time for information to be processed. • Be prepared to provide information several times as families under stress may not be able to comprehend and remember details. Ensure all members of the health care team are providing consistent information to the family. • Help family members differentiate their beliefs and needs from those of the dying person, and if possible, provide assistance in meeting those needs. • Encourage family members to make time to look after their own health. 114 • Facilitate communication between family members and the dying person, if desired. • Assist family members in finding ways to be present as the dying person becomes less able to interact with them. • Provide families with practical information about topics such as the physical process of dying, making funeral arrangements, and accessing insurance benefits. • Teach family members about the physical, emotional, and spiritual effects of grief (e.g. loss of appetite, sadness, and difficulty sleeping). • Explain that feelings such as shock, numbness, anger, ambivalence, sadness, and fear may or may not be part of grieving and that the intensity of feelings may fluctuate. • Help family members understand that individuals may have very different experiences and ways of coping. • Explain to the family that role reallocation and family reorganization may be necessary. • Facilitate access to needed resources (e.g. pharmacy that delivers, equipment, supplies, and volunteer help). • Facilitate referral to a psychosocial professional as needed. Nursing Alert Be realistic. Recognize that this is not the time to change the family’s communication style or a lifetime of established coping skills. 115 81. How is loss of control expressed by persons and their families? How can they be assisted to maintain a sense of control? Loss of control can be a significant source of distress for persons and their families. The ill person may experience progressive dependency, family role disruption, and alteration of future plans. Those struggling with loss of control may seek detailed medical information, insist on maintenance of a consistent routine, make frequent requests of caregivers and criticize care provided, direct anger or frustration toward caregivers, or insist on doing activities that risk injury. Interventions • Reinforce that the person and family are an important part of the team. Demonstrate this by including them in decisions and assisting them to participate in care in which they wish to be involved. • Provide opportunities for the person and family to discuss what is important to them. • Provide information as requested; allow time for it to be processed. • Support existing strategies for maintaining control (e.g. being assertive, directing care). • Encourage maintenance of usual routines. • If hospitalized, encourage the family to make the environment home-like (e.g. display family photos and bring in the person’s clothes). • Facilitate referral to spiritual and religious leaders as desired. • Respect the choices made by the person or family. Recognize the difference between personal opinions and what the person or family believe is important. 116 Psychosocial 82. What is anxiety? How does the person express anxiety? What are the interventions? Anxiety is a non-specific subjective feeling of uneasiness, stress, and insecurity. Anxiety can range from mild to severe depending on the perceived threat. The expression of anxiety can include restlessness, irritability, jitteriness, agitation, and panic. Interventions • Expressive-supportive therapies (e.g. listen to the person, encourage expression of feelings). • Relaxation exercises (e.g. massage, imagery, soothing music, slow rhythmic breathing exercises). • Complementary therapies (e.g. aromatherapy, therapeutic touch, Reiki, acupuncture, meditation). • Referral to a social worker, psychologist, or spiritual care provider for counselling. • Pharmacological modalities: benzodiazepines, nonbenzodiazepines, and neuroleptics may be considered. Nursing Alert People with advanced cancer are vulnerable to the side effects of psychoactive medications. Monitor for delirium. Suggest discontinuing any anxiolytic if delirium is suspected. 117 83. How is depression expressed? What are the interventions? Depression in advanced disease may be under diagnosed. Nevertheless, sadness and depressed mood are normal responses to a diagnosis of a life-limiting illness and depressed mood may not indicate depression. Conditions that may mimic depression include: hypoactive delirium, hypercalcemia, hypothyroidism, and the side effects of some medications. Somatic symptoms of depression, such as anorexia, weight loss, and fatigue, are of little value in diagnosing depression in a person as they are common in advanced disease. Assessment A 0–10 rating scale can be used to screen for the possibility of depression (see Appendix A). It is important to assess for psychological indicators of depression including: profound feelings of worthlessness, guilt, hopelessness, anhedonia (inability to experience pleasure in normally pleasurable acts), thoughts of “wishing for death”, and thoughts of suicide. Interventions • Facilitate referral to a psychosocial professional. • Respectfully acknowledge the person’s sadness or depressed feelings. • Encourage the person’s expression of feelings or emotions. • Involve the person in aspects of their care and provide choices. • Involve the person in normal social conversation. • Help the person set achievable and realistic goals. • Review and reinforce realistic ideas and expectations. • Focus on the person’s strengths. • Establish rapport by frequent short visits. • Resist giving false reassurances. Nursing Alert Antidepressants should be considered for treatment when the person expresses ongoing psychological indicators of depression, especially feelings of being a burden, wishing for death, and/or expressing suicidal ideations. 118 84. What interventions are used when dealing with anger? Anger is a common emotion. Feelings of anger may be directed at the caregiver, the health care professional/system, family members, or spiritual deities. Anger often results from perceived feelings of powerlessness, anxiety, and fear. Interventions • • • • • • • • • Validate the person’s feelings of anger. Attempt to identify the source of anger. Respond to the feeling, not the words. Realize that the anger is not directed at you. Keep your voice level low, even if the other person becomes loud and aggressive. Sit down at eye level with the individual. Let the person know that s/he has been heard. Take responsibility for any of your actions that would be legitimately upsetting and apologize as appropriate. Do not provide excuses for the actions of others. Provide examples of how anger can be constructively vented. 119 85. What are the interventions for supporting the person who is crying? Crying is a common reaction in many situations. People express emotions along a continuum. While some only express their feelings in private, others express their feelings in public. Be sensitive to these individual differences. Your comfort level with other’s emotions will impact your ability to support them. Interventions • Provide a supportive, non-judgmental environment in which the person feels safe and comfortable to express feelings. • Do not try to stop someone from crying. • Acknowledge emotions in a reflective, non-threatening manner. • If appropriate, ask why they are crying; do not assume you know the reason for the emotion. • Do not provide false hope or lessen the reality of devastating news. Use therapeutic silence when warranted. • Ask questions (e.g. “What kind of support system do you have?”) If supports are inadequate, offer suggestions for providing support. 86. How is denial expressed? What are the interventions? Assess the degree of denial. Denial can be displayed on a continuum ranging from selective focusing, when the person makes the conscious choice not to acknowledge the illness and its implications, to a complete lack of awareness of the facts of the illness. Selective focusing can be beneficial because it provides necessary respite from preoccupation with death and allows time for information to be absorbed and for alternate coping mechanisms to be mobilized. If the person and/or family completely deny the medical condition, there can be detrimental effects, such as ignoring medical advice or failure to use the remaining time to organize their affairs, resolve family issues, or leave a legacy. 120 Nursing Alert Be cautious in your use of the label “denial.” It is often perceived as a negative term that implies poor coping. In fact, behaviour labelled as denial can be a very positive means of living with a terminal disease. Whether or not to live in denial, accept treatment, and/or prepare for death are all personal choices. Interventions • Determine what the person and family have been told and their understanding of the illness. • Acknowledge the rights of the person and family to make future plans. • Do not provide false hope or attempt to break down the denial. • Be aware that the person and family may not be experiencing the same level of denial. 87. What is a child’s understanding of death? A child’s understanding of death is influenced by age related developmental stages. Ages 0-2 Years: This age group has no understanding of death and they are unlikely to be able to differentiate death from temporary separation. Ages 3-5 Years: Children 3-5 years of age are very concrete thinkers and do not fully understand the permanency of death as they view death as a temporary departure or separation. They may forget the person has died and can confuse death with sleep. They are able to connect death with events (beginning to understand cause-effect), but may attribute life to inanimate objects. Ages 6-8 Years: This age group often experiences much confusion and misunderstanding with death. They are magical thinkers, who may see death as external and avoidable. They understand death as linear – that individuals die when they are old. This group may personify death (e.g. a ghost, shadow, or a skeleton), and could feel some responsibility for a death, that has occurred and may see death as punishment. 121 Ages 9-12 Years: Abstract thinking is developing in children 9-12 years of age and they are beginning to understand that death is universal, inevitable, and permanent. Children in this age group are beginning to inquire about what happens to the body and spirit after death. They are socially concerned and able to acknowledge the feelings of people around them. Ages 13-17 Years: Teenagers are able to understand the implications of death and may be overwhelmed by intense emotion when someone has died. They may feel invincible, but death shatters this belief. When a death has occurred, they may be shocked and confused about their reactions. 88. How can children be prepared? Children often perceive that something is wrong even if they are not told. Routines are disrupted and people close to them may look and act differently. It is best to tell children what is wrong rather than allowing them to fantasize. Talking with Children • Provide a comfortable environment early in the day when there is time to listen. Avoid times before bed, school, or important events. • Allow time for children to express feelings. • Answer questions simply and honestly. Use words children understand. Pace information to give the child time to assimilate and process. • Ask children what they understand or think about the illness and the future (e.g. Do you know what kind of sickness Daddy has? What do you think happens when someone gets sick? Have you ever thought that Mommy may not get better?). • It is important to explain to children what caused the illness. If the cause is not known, tell children this and reassure them that the person’s illness is not their fault. • Explain what has happened and what may happen next (e.g. Daddy’s body is getting weaker every day. Sometimes when a person gets this sick, they can’t get well again). 122 • Relate the situation to a previous experience of death such as the loss of a grandparent or the loss of an animal, using nature as the cycle of life. • Use dolls or draw pictures. • Ask children to explain back to you what they understand from your conversation so that you can clarify confusion. • Go back later and ask if there are any questions. Repeat information as often as needed. • Read or provide books that discuss life and death. • Access grief programs for children. Specific Actions to Take with Children Suggest that families reassure children that they will be supported, cared for, and loved. Provide extra hugs, kisses, and spend time together when possible. Encourage families to normalize the routine by maintaining usual structure and boundaries. Nursing Alert It is okay for adults to cry in front of children and to tell them how they are feeling. However, adults must be careful not to overwhelm children with the intensity of their own emotions. References Cairns, M., Thompson, M., & Wainwright, W. (2003). Transitions in dying and bereavement: A psychosocial guide for hospice and palliative care (pp. 61-62). Baltimore: Health Professions Press. Chochinov, H. (2002). Dignity-conserving care – A new model for palliative care, JAMA, 287, 2253-2260. Kreicbergs, U., Valdimarsdottir, U., Onelov, E., Henter, J. I., & Steineck, G. (2004). Talking about death with children who have severe malignant disease. New England Journal of Medicine, 351(12), 1175-86. Faulkner, K.W. (2001). Children’s understanding of death. In A. Armstrong-Dailey & S. Zarbrock Goltzer (Eds.) Hospice care for children (2nd ed., pp. 9-22). New York: Oxford University Press. Pereira, J. L. & Associates. (2008). The Pallium palliative pocketbook: A peer-reviewed, referenced resource. (1st Cdn. Ed.) Edmonton, Canada: The Pallium Project. 123 Spirituality and Hope 89. What are spirituality and religion? How are spirituality and religion assessed? For many individuals, spirituality is expressed through religious means. Spirituality refers both to the essence of what it means to be human, such as our sense of who we are, and to a connection to a transcendent domain. Spirituality encompasses how we seek meaning in life and how we experience ourselves in relationship with other people and possibly with a Higher Power. Religion is associated with an organized system of faith, beliefs, worship, rituals, and relationship with a divine being. Religions are belief systems that can provide a framework for spirituality. Religious rites, writings, and rituals can provide concrete ways of expressing and fostering spirituality for believers. Assessment Identify the following: • Personal meaning of illness, • Relationships with others and/or a higher being, • Ways in which spirituality and/or religious beliefs influence care decisions at the end of life, • Personal history of loss, grief, and style of coping, • Sources of meaning and purpose in life, • Sources and targets of hope, • Need to give or receive forgiveness or acceptance, • Need to reconcile, and/or • Significant religious or spiritual practices. 124 A tool that can aid in your spiritual assessment is the FICA Spiritual Assessment Tool©: The FICA Spiritual Assessment Tool© was developed by Dr. Puchalski and a group of primary care physicians to help health care professionals address spiritual issues with patients. The acronym FICA can help structure questions when taking a spiritual history in the clinical setting. F – Faith and Belief Do you consider yourself spiritual or religious?” or “Do you have spiritual beliefs that help you cope with stress?” If the patient responds “No,” the health care provider might ask, “What gives your life meaning?” Sometimes patients respond with answers such as family, career, or nature?” I –Importance “What importance does your faith or belief have in our life? Have your beliefs influenced how you take care of yourself in this illness? What role do your beliefs play in regaining your health?” C –Community “Are you part of a spiritual or religious community? Is this of support to you and how? Is there a group of people you really love or who are important to you?” Communities such as churches, temples, and mosques, or a group of likeminded friends can serve as strong support systems for some patients. A – Address in Care “How would you like me, your health care provider, to address these issues in your healthcare?” Reprinted with permission from Dr. Puchalski, The George Washington Institute for Spirituality & Health. Available online at www.gwish.org 125 Signs that may indicate spiritual distress include: • Questioning of religious faith and beliefs such as, “Why would God allow this to happen to me? Why am I being punished? What did I do wrong?” • Other difficult questions, such as, “What does this mean? Is it too late to turn to God?” • Expressions of anxiety, hopelessness, worthlessness, guilt, shame, failure, remorse, regret, and/or sense of meaninglessness. • Feelings of abandonment. • Physical symptoms, which may be a manifestation of spiritual pain and despair. 90. What interventions support the person’s spirituality and religion? Interventions • Acknowledge and respect the beliefs and views of the person. • Be present for people as they experience suffering and struggle with difficult questions. Being present involves being with the person physically, psychologically, and spiritually, often without words. It also involves having the courage to face your own and others’ suffering, helplessness, fear, and despair. • Be available to listen actively, non-judgmentally, and with acceptance. • Explore spiritual beliefs, issues and concerns with the person and his or her family. • Arrange for time, space, privacy, and resources to facilitate significant religious or spiritual practices as requested by the person (e.g. prayer, meditation, administration of sacraments, and/or reading of religious writings). • Acknowledge your limitations as a clinician and arrange for appropriate supports (with person’s approval) based on the person’s belief system. Nursing Alert People may find meaning or purpose from a life-limiting illness that supports them to endure suffering, accept dying, and realize value in the present. The search for meaning can provide an opportunity for growth and self-reflection. 126 91. What is hope? How is it assessed? What are the interventions? Hope has been described as an inner power or a life force. It is essential to the human experience and is closely associated with human suffering. Hope enables people to move forward and engage in life and protects them from being engulfed by suffering and negativity. Hope can be a generalized state of being within the self or it can be specifically focused on a valued goal or outcome (e.g. the person hopes to live until Christmas). The target or intensity of hope may change as an illness progresses. Redefining hope is an ongoing process. Nursing Alert Ensuring that hope is realistic is not a nursing resposibility. If we challenge what we consider to be unrealistic, we run the risk of stripping a person of important ways of coping. When tempted to label hope as unrealistic, we need to ask ourselves, “Whose reality are we talking about, mine or the person’s?” Each person has the right to choose what to hope for in keeping with his or her own perceptions, beliefs, and attitudes toward reality. Assessment Identify the following: • Effect of illness on sense of hope, • Factors that enhance or diminish hope, • Meaning and sources of hope, • Targets of hope (e.g. attending a daughter’s wedding or leaving a legacy), • Values, beliefs, information that support the person’s hopes. Interventions Assist the person to: • Focus on personal strengths and abilities, • Lead a normal life (as much as possible), without constantly focusing on the illness, • Reflect on past accomplishments, positive memories, and significant milestones, 127 • Create a personal legacy (e.g. photo album for children or letters), • Maintain meaningful relationships with family and significant others, • Identify personal goals and hopes, and find opportunities to achieve them, • If old hopes are unattainable, replace with new hopes, • Identify images, symbols, or rituals that foster hope. Sustain your own hope. Use humour and be positive in your interactions with others. Be honest and clear in the delivery of information, while respecting each individual’s “need to know” (too much information and/or unsolicited information can destroy hope). Remind people that prognosis predictions can be inaccurate. A person may have future hopes and goals that are unlikely to be realized. Focusing on these hopes could prevent the person from taking important actions or completing preparations for death. Encouraging the person to complete these actions or preparations, without destroying hope, may be facilitated by the following approaches: • A “what if” approach – invites the person and family to reflect upon what they would do differently if things don’t turn out as they hope (e.g. What if the treatment doesn’t cure you?) • A “just in case” approach – encourages the person and his or her family to hope for the best while planning for the worst, just in case it happens (e.g. Just in case you don’t live until the wedding, is there anything you’d like to do now)? • A “normalizing” approach – encourages the person to complete end of life planning and finish business because it’s something we all should do. Nursing Alert Remember that some people can accept and prepare for death while also holding onto hope. For example, a person may already have planned a funeral and completed a will, yet adamantly maintains hope for a cure and focuses on living life fully to the end. Other people will not accept or prepare for death – and that is their right. 128 References Borneman, T., Ferrell, B., & Pulchalski, C. (2010). Evaluation of the FICA Tool for Spiritual Assessment. Journal of Pain and Symptom Management, 40(2), 163-173. Pereira, J. L. & Associates. (2008). The Pallium palliative pocketbook: A peer-reviewed, referenced resource. (1st Cdn. Ed.) Edmonton, Canada: The Pallium Project. Puchalski, C. (2006). Spiritual Assessment in Clinical Practice. Psychiatric Annals, 36(3), 150-155. Puchalski, C. & Romer, A. (2000). Taking a Spiritual History Allows Clinicians to Understand Patients More Fully. Journal of Palliative Medicine, 3(1), 129-137. Sherman, D. W. (2001). Spiritually and culturally competent palliative care. In M.L. Matzo & D.W. Sherman (Eds.), Palliative care nursing: Quality care to the end of life (pp. 3-47). New York: Springer. Sinclair, S. (2012). Spiritual care. In D. Oneschuk, N. Hagen & N. MacDonald (Eds.), Palliative Medicine: A Cased-Based Manual (pp 209-220). Oxford: Oxford University Press. Wright, L. (2005). Spirituality, suffering, and illness: Ideas for healing. Philadelphia: Davis. Culture 92. What is cultural competence? How is it applied to practice? The goal in providing “culturally competent” care is to be sensitive and aware of the beliefs, values, practices, and traditions of others, and respect them when providing care. Cultural experience includes self-awareness, cultural knowledge about illness and healing practices, communication skills, and behavioural flexibility. Culturally competent behaviours include: • Self-awareness: Be aware of your cultural beliefs and values and how they influence the care you give. It is important that you do not impose your values on others. 129 • Breaking down stereotypes: Judgments can be easily formed about those who are different from us. To eliminate misinformation and bias, dialogue and comunication are important to help us learn more about each other. • Exploration of cultural values and beliefs: Discover the uniqueness of each person by asking questions about such things as family lifestyle, patterns of authority and communication, and expectations of caregivers. • Facilitation of meaningful practices: Support and make referrals to appropriate persons, groups, or institutions who can facilitate the practice of specific rituals, customs, or traditions • Determine the person’s preference for disclosure: The desire to tell or know the truth about illness or death is a cultural value that is not shared by everyone. Remember that people have the right “not to know” if this is their wish. Some families or cultural groups may wish to shield a dying person from knowing he or she has a life-limiting illness (e.g. some cultures may prefer to shield the person from knowing his or her diagnosis because the knowledge of a life-limiting illness may result in loss of hope and the will to live). Clinical Tip To determine a person’s preference for information disclosure, ask “Besides yourself, is there anyone else that you would like us to talk to about your medical information?” Possible preferences include the person alone, the person and family, or a designated family member only. Nursing Alert When using a family member as a translator, be mindful that the intended message may be altered. Explore if your organization has translation services available. 130 93. How does culture influence the dying process? A person’s culture may influence: • Expression and meaning of pain and suffering, • Attitude toward disclosure and awareness, • Beliefs about the cause and meaning of illness, • The choice of healer and treatment regimen, • Attitudes toward death and dying, • Beliefs about the afterlife, and the value of human life and the body, • Expressions of loss and grief, • Death rituals, including preparation for death, burial, funeral or memorial services, customs for disposal of the body, and mourning rites. References Cloutier, K. (2000). Customs and traditions in times of death and bereavement (4th ed.). Calgary, AB: McInnis & Holloway Funeral Homes. Elliot, G. (2011). Cracking the cultural competency code. Canadian Nursing Home. 22(1), 27-31. 131 Euthanasia and Suicide 94. What are euthanasia and assisted suicide? What are the nursing responsibilities? Euthanasia means knowingly and intentionally performing an act that is explicitly intended to end the life of a person who has an incurable illness, and doing so with empathy and compassion and without personal gain. Assisted suicide means knowingly and intentionally providing a person with the knowledge or means or both required to commit suicide, including counseling about lethal doses of drugs, prescribing such lethal doses or supplying the drugs. Euthanasia and assisted suicide are often regarded as morally equivalent, although there is a clear practical distinction, as well as a legal distinction, between them. Persistent requests for euthanasia, once physical symptoms are controlled, are usually due to psychosocial and/or spiritual distress (e.g. hopelessness, a loss of meaning and purpose in life, a feeling of being a burden to others, isolation or abandonment, depression). Nursing Responsibilities • • • • • • Be non-judgmental and reflective, Explore the reason(s) for the request, Identify fears and sources of suffering, Ensure physical symptoms are adequately controlled, Take measures to alleviate psychosocial and spiritual distress, Discuss with the person and family their choices regarding treatment, (e.g. medications for chronic illness, high flow oxygen, hydration), • Refer to a social worker, psychologist, spiritual care provider, or ethics consultant for further support 132 Nursing Alert There will be a very small number of people who continue to request euthanasia or assisted suicide despite interventions. At the time of publication, euthanasia and assisted suicide are illegal in Canada. Politely and non-judgmentally decline this request, and explore possible underlying reasons. It is important that the individual does not feel abandoned. Make sure you have support and an opportunity to express your own feelings about these challenging situations 95. What are the risk factors for suicide? What are the interventions? Suicide risk factors include: • Verbal and behavioural clues (e.g. isolation or withdrawal, communicating death wishes, statements reflecting a sense of hopelessness, or resistance to care), • A detailed suicide plan including method and time frame, with no precautions for rescue, • Lack of social support, • Social isolation, • Significant losses, • Fear of being or becoming a burden, • Significant life stressors (e.g. serious or debilitating illness of a loved one and/or financial concerns), • Depression, • Prior suicide attempts, • Being between 15-24 years of age or over 50. Interventions To reduce the risk of suicide, consider the following: • Determine the extent of depression, • Facilitate the person’s expression of feelings, • Provide a safe environment, • Provide symptom management, • Inform members of the interdisciplinary team about suicide risk, • Refer to psychosocial resources, 133 • Connect with family and significant others to develop a support plan, • If the person expresses suicidal ideation – Explore the person’s suicide plan, including method, plan for rescue, timing, and organizational detail. – Immediately notify the person’s attending physician. – Refer immediately to a professional trained in suicide intervention. Reference Canadian Medical Association (2007). CMA Policy: Euthanasia and Assisted Suicide. Ottawa: Canadian Medical Association. Goals of Care 96. What influences Goals of Care and Advanced Care Planning? There are a number of different terms that are used when referring to goals of care, including preferences for comfort, medical, and resuscitative interventions. Current recommendations focus on advance care planning and use of terms that direct care such as Allow Natural Death, Comfort Measures, and Provision of Comfort Care. Influencing factors regarding interventions, including resuscitation are: • Extent of disease, • Quality of life (defined by the person), • Current goals of care and perception of interventions, • Values and beliefs of the person and family that align with the goals of care, • Medically appropriate interventions, • Individual consideration of benefits and burdens of treatment, • Potential causes of cardiac arrest and the likelihood of recovery. 134 Some people have Advance Directives (Living Wills) or Advanced Care Planning documents that guide decision-making. These documents provide an opportunity for discussion of the goals of care, and outline a person’s wishes in the event that he or she is unable to make decisions. If a person has an Advance Directive, read it and become familiar with the contents. Consult your organization’s policies and procedures related to Advance Directives. Legislation varies regarding Advance Directives across provinces/territories. 97. How are goals of care discussed? When discussing goals of care with a person and family: • Ensure a comfortable, quiet, and private setting. • Explore knowledge of illness and prognosis. • Address their misconceptions; be cautious when denial, unrealistic hope, or a preference for non-disclosure are present. • Discuss the goals of care and examples of interventions. • Use the terminology Allow Natural Death, rather than Do Not Resuscitate. • Assure that each goal is intended to optimize care. Reversible complications may still be treated if desired and symptoms will continue to be aggressively managed. • Emphasize that the goal of hospice palliative care is to provide comfort, alleviate suffering, enhance quality of life, and promote a peaceful death. • Explain that if the disease progresses and the person’s heart or breathing stops, efforts at resuscitation are unlikely to succeed. • If the heart does resume beating, the person may remain unresponsive and will usually die shortly afterwards. • Resuscitation efforts usually inflict needless suffering for persons and families and are not recommended. • The nurse should be prepared to initiate the conversation and discuss goals of care with the patient and family. 135 Resources for the public and health care professionals are available from a variety of sources, including The Advance Care Planning National Task Group at www.advancecareplanning.ca/about-advancecare-planning/advance-care-planning-national-task-group.aspx. Organ and Tissue Donation 98. Can an individual with terminal illness, advanced disease, or cancer donate? Is an open-casket funeral possible after organ and tissue donation? Yes, individuals 80 years of age or younger with a terminal illness, advanced disease or certain cancers may be eligible for eye and tissue donation. Organ donation may also be possible when a terminally ill person is being cared for in an intensive care unit. All potential organ and tissue donors are assessed on a case by case basis. Tissues which can be donated include: • Eyes – for sight-restoring surgeries • Skin – to help burn patients • Bone and Tendons – to aid bone repair or restore joint mobility • Heart for valves – for life-saving heart repair procedures Open casket funerals are possible after organ and tissue donation. All efforts are made to ensure that there are no visible signs that donation has occurred. Donation should not interfere with any funeral arrangements that are made. 136 99. What is the health care professional’s role in organ and tissue donation? Offering the option of tissue donation empowers patients and families to make choices in keeping with their own wishes and goals of care at the end of life. In order to support patients and families to make these decisions, it is important for health care professionals to facilitate and respond to conversations about donation. If the health care professional does not ask about donation wishes, the discussion may not happen. After the window of opportunity to donate is closed, families can feel regret. Discussing donation prior to determining an individual’s eligibility to donate can create false hope. When possible, screening for initial eligibility before approaching patients and families may help eliminate false expectations. Health care professionals can work with their local organ and tissue donation program to develop a process for initial screening. For more information on organ and tissue donation, contact the donation/transplantation program in your region. Last Days 100.How can nurses prepare families for the last days of life? Nurses can help families prepare by: • Letting them know that predicting the time of death is difficult. Time frame can be described in general terms, such as “hours to days”, “days to weeks”, “weeks to months” or “months to years”. If family is concerned about prognosis, ask what would be done differently if time was short. • Being proactive and trying to anticipate family concerns, fears, and feelings about dying and death. • Exploring their fears openly and non-judgmentally, correcting distorted expectations, and addressing concerns. • Assessing their ability to cope. 137 • Supporting them in coming to terms with impending death. • Teaching them the indicators of imminent death (See Question 101). • Teaching them about comfort measures. • Facilitating timely access to appropriate services and resources. • Giving a copy of the book A Caregiver’s Guide: A handbook about end of life care, available from the Canadian Hospice Palliative Care Association http://www.chpca.net. • Encouraging them to carry out family and/or religious rituals as desired. • Exploring the appropriateness and importance of contacting out of town family member(s). Answers to the following questions may facilitate the family’s decision: – How soon is the person likely to die (e.g. hours to days, days to weeks, or weeks to months)? – Does the ill person want these persons to be informed of his or her condition? – Is it important that the family member visits? – Is there an issue that needs to be resolved? • Helping family members understand that the person’s progressive withdrawal and detachment does not indicate rejection. 101.What are the indicators of imminent death? Explain to family members that as the body’s functions shut down, changes occur. Reassure family members that observed changes, especially changes in breathing, are usually more distressing for family than for the dying person. Physiological changes or signs may include: • Reduced urine output and/or concentrated urine, • Changes in pattern and sounds of breathing such as periods of apnea (Cheyne-Stokes) or sounds of congestion, • Progressive coldness, discolouration, and mottling of skin, • Weakening pulse, • Fluctuating level of consciousness with a gradual decline, accompanied by decreased awareness, dysphagia, and flaccid muscles. 138 Nursing Alert Anxiety, restlessness, confusion, and hallucinations may not be indications of imminent death but instead may be poorly controlled symptoms. Further assessment and management are needed. 102.What are the interventions in the last days of life? Interventions The following strategies are intended to facilitate a peaceful and dignified death: • Provide privacy, • Maintain the person’s sense of identity and dignity, • Provide gentle, respectful care, • Provide optimal symptom management, • Help fulfill a final wish or resolve a pressing concern (e.g. help restore important relationships), • Encourage family members to talk to the person even if he or she appears not to hear or respond, • Suggest family members say their good-byes, • Demonstrate how to talk to and care for the person with your own words and actions, • Encourage family to take care of themselves and not to neglect their need for sleep and food, • Provide emotional support, • After the death, offer the family private time with the deceased; remain with them if requested. • Ask if there is anything you can do (e.g. make phone calls to relatives, arrange a visit by clergy), • To the extent possible, honour special requests regarding treatment of the body after death (e.g. some cultures or religions call for the body to not be left alone). 139 Nursing Alert Discuss with family their wishes regarding being present at the time of death. If their hope is to be present, they may not want to take time away from their loved one. Grief and Bereavement 103.What is grief? What are the immediate interventions? Grief is a personal emotional response to a loss, and impacts every aspect of a person’s being. Grieving may start with the diagnosis of a life-limiting illness and can continue until well after the death. Nurses can support families in their grieving process. Interventions • Show your genuine concern and emotions. • Avoid clichés (e.g. You need to be strong now. It’s God’s will. I know how you feel). Such responses can make survivors feel angry, misunderstood, or unsupported. Every person’s experience is unique. • Use touch when appropriate. • Allow for silence; often your presence is appreciated. • Don’t be afraid to say, “I don’t know what to say”. • Facilitate expression of feelings or conversation about the person who has died. • As appropriate, share your memories of the deceased and talk about his or her special qualities. • Assist with rituals at the time of death. • Contact spiritual or religious leaders if desired by the family. • If family members are not present at the time of death, ask them what this means to them. They may be interested or reassured to know it is not uncommon for people to die when their family is not present. 140 Be especially involved in the following situations: • There is limited support from relatives, friends, or the community, • The death is of a child or young adult, • The death was sudden, • There are significant questions or concerns about the cause of death, • There are significant questions or concerns about the location of death (e.g. home vs. hospital vs. hospice vs. alternate level of care). 104.What are some interventions for bereavement follow-up? Coping during bereavement fluctuates over time (e.g. a person may need to be told that it is common to move between feeling sad and laughing with friends). The brain and body can only sustain intensity of emotion for short periods. Healthy bereavement is the ability to continue to thrive despite the loss. While grief is a normal process, those who are grieving may experience higher rates of medical and psychiatric events, including depression in the first year after a death. Critical times for bereavement follow-up: • 2 weeks to 1 month – it is important to make initial contact, • 3 months – often the first crisis occurs at this stage as extended family leave and people begin to believe the person who is grieving “should be over it”, • 6 months, • Anniversary of the death, • Holidays, birthdays, and other anniversaries. Interventions Interventions for bereavement follow up may include: • Providing a card with contact numbers and resources, including formal grief support programs, • Arranging home visits, • Assisting with family rituals, 141 • Providing opportunities for the family caregivers to review their experience, • Commending the family on what they did for the person (e.g. advocating for individual throughout illness), • Making phone calls at critical times. References Aranda, S., & Milne, D. (2000). Guidelines for the assessment of complicated bereavement risk in family members of people receiving palliative care. Melbourne: Centre for Palliative Care. Cairns, M., Thompson, M., & Wainwright, W, (2003). Transitions in dying and bereavement. Baltimore: Health Professions Press. Corless, I. B., (2010). Bereavement. In B. R. Ferrell & N. Coyle (Eds.), Oxford book of palliative nursing (3rd ed., pp. 597-611), New York, NY: Oxford University Press. Grief, C. (2002, August). Bereavement in the elderly: Clinical considerations. CPA Bulletin, 29-33. Care for the Caregiver 105.What strategies can a nurse take to reduce his or her stress? Caring for terminally ill persons and their families can be challenging. Some strategies that professional caregivers can use to support self-care include: • Acknowledging times of difficult or intense emotions or questioning. • Seeking assistance to work through recurring or ongoing grief and loss in your personal life. • Focusing on potential rewards and opportunities inherent in caring for the dying: – Connecting in a meaningful way. – Transforming a difficult and painful time into a time of comfort, meaning, and hope, as well as an opportunity for personal and spiritual growth. – Identifying meaning and purpose in one’s own life. 142 • • • • • • • • • • • • Using humour appropriately and with sensitivity. Adopting a healthy, balanced lifestyle. Holding a memorial service for families at your place of work. Debriefing or conducting rituals to honour others and your work after experiencing death(s) (e.g. lighting a candle or saying a prayer in memory of the deceased). Attending the funeral, if appropriate. Celebrating the happiness in your own life. Requesting assistance or time-out at work without feeling guilty. Setting realistic goals and limits, looking for small victories, and celebrating success. Seeking the support of a skilled mentor. Participating in continuing education activities. Joining or forming support groups, bereavement groups, or palliative care associations. Engaging in self-awareness activities that help you understand your own emotional responses to persons and families as well as death and mortality. Nursing Alert Health care professionals need to be careful not to hold inappropriate or unrealistic expectations to ensure “a good death”. While a death can be considered good if all suffering is alleviated, death is openly discussed and accepted, all business is finished, good-byes are well-articulated, and the exit is made gracefully, in some cases, death is neither good nor graceful. Many of the problems and issues confronting dying people cannot be resolved, despite the care providers doing all the “right” things. 143 106.What might be warning signs of inappropriate boundaries? Caregivers can develop a high level of concern for those they are looking after. Sometimes it is challenging to maintain appropriate boundaries. Families and ill persons often desperately need and welcome professional support. If boundaries are inappropriate, the person or family may not seek or receive the support that they need (e.g. the caregiver is too distant or too intimate). The following may be signs of inappropriate boundaries: • Giving out your home number. • Telling ill people or their families to call you anytime. • Avoiding difficult questions or avoiding engaging in discussions about concerns or issues (e.g., euthanasia, changing treatment plans, feelings of abandonment or anger). • Socializing with persons or families in your care. • Conducting home visits that are more social than professional. • Being treated or behaving like a family member. • Becoming involved in family decisions. • Receiving comfort from the person or family. • Favouring one person‘s care at the expense of others. • Being seen as the favourite or preferred nurse for a person. • Giving and receiving inappropriate gifts. Nursing Alert It is normal to develop a thorough knowledge of some families in your care. Be careful not to confuse professional familiarity with personal closeness. Remember that you are not a family member nor a friend. Reference DeAngelis, R. (2004, September). Professional nursing boundaries: Is crossing the line helpful or hurtful? (juried concurrent presentation). Proceedings of the 15th International Congress on Care of the Terminally Ill, Montreal. 144 General References The following is a list of books and websites that may be of assistance if further resources are sought. 145 Textbooks Cairns, M., Thompson, M., & Wainwright, W. (2003). Transitions in dying and bereavement: A psychosocial guide for hospice and palliative care. Baltimore: Health Professional Press. Hanks, G., Cherney, N., Christakis, N., Fallon, M., Kaasa, S., & Portenoy, R. (2010). Oxford textbook of palliative medicine, 4th edition. New York, NY: Oxford University Press. Ferrell, B., & Coyle, N. (2010). Oxford textbook of palliative care nursing. New York, NY: Oxford University Press. Hospital Pharmacists’ Special Interest Group in Palliative Care. (2009). Care beyond cure: Management of pain and other symptoms (4th ed.) Ottawa, Canada: Canadian Society of Hospital Pharmacists. Oneschuk, D., Hagen, N., & MacDonald, N. (Eds.) (2012). Palliative medicine: A case-based manual (3rd ed.). New York: Oxford University Press. Otto, S.E. (2001). Oncology nursing (4th ed.). St. Louis: Mosby. Pereira, J. L. & Associates. (2008). The Pallium palliative pocketbook: A peer-reviewed, referenced resource. (1st Cdn. Ed.) Edmonton, Canada: The Pallium Project. Victoria Hospice Society. (2006). Medical care of the dying (4th ed.) Victoria, B.C.: Victoria Hospice Society. Waller, A. & Caroline, N. (2000). Handbook of palliative care in cancer (2nd ed.). Boston: Butterwort and Heinemann. Wrede-Seaman, L. (2005). Pediatric pain and symptom management algorithms for palliative care, (1st ed.). Washington: Intellicard, Inc. General Reference Websites Canadian Hospice Palliative Care Association http://www.chpca.net Canadian Network of Palliative Care for Children http://cnpcc.ca Canadian Virtual Hospice www.virtualhospice.ca National Cancer Institute http://www.cancer.gov Palliative Care Links and Resources http://palliative.info Edmonton Zone Palliative Care Program in Edmonton, Alberta http://www.palliative.org The Pallium Project http://www.pallium.ca/ 146 Appendices A. Edmonton Symptom Assessment System – Revised (ESAS-r) B. Faces Pain Scale - Revised (FPS-R) C. CAGE Questionnaire D. Table of Equianalgesic Doses of Opioids E. Suggested Strategies for Energy Conservation 147 Appendix A Edmonton Symptom Assessment System – Revised (ESAS-r) This tool is designed to assist in the assessment of nine symptoms common in palliative care: pain, tiredness, drowsiness, nausea, lack of appetite, shortness of breath, depression, anxiety, and wellbeing (there is also a line labelled “Other Problem”). The severity at the time of assessment of each symptom is rated from 0 to 10 on a numerical scale, 0 meaning that the symptom is absent and 10 meaning the worst possible severity. The person and family should be taught how to complete the scales. It is the person’s opinion of the severity of the symptoms that is the “gold standard” for symptom assessment. The ESAS-r provides a clinical profile of symptom severity over time. It provides a context within which symptoms can begin to be understood. However, it is not a complete symptom assessment in itself. For good symptom management to be attained, the ESAS-r must be used as just one part of a holistic clinical assessment. The ESAS-r is completed regularly, preferably at least once a day (depending on the setting), and the score is then transferred to a bar graph. The graphic representation allows the staff to visualize patterns of symptom control and symptom expression over time. Individuals can either complete the ESAS-r alone or with the assistance of a caregiver, depending on their ability. If the person is unable to complete the ESAS-r, then proxy ratings may be provided by a caregiver. The ESAS-r tool and bar graph, with more detailed guidelines for use, can be accessed via the Edmonton Zone Palliative Care Program website www.palliative.org. 148 Edmonton Symptom Assessment System (ESAS-r) Edmonton Symptom Assessment System: (revised version) (ESAS-r) Please circle the number that best describes how you feel NOW: No Pain 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Pain No Tiredness 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Tiredness 1 2 3 4 5 6 7 8 9 10 Worst Possible Drowsiness (Tiredness = lack of energy) No Drowsiness 0 (Drowsiness = feeling sleepy) No Nausea 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Nausea No Lack of Appetite 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Lack of Appetite No Shortness of Breath 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Shortness of Breath No Depression 0 1 2 3 4 5 6 7 8 9 10 Worst Possible Depression 1 2 3 4 5 6 7 8 9 10 Worst Possible Anxiety 1 2 3 4 5 6 7 8 9 10 Worst Possible Wellbeing No __________ 0 1 2 3 Other Problem (for example constipation) 4 5 6 7 8 9 10 Worst Possible _______________ (Depression = feeling sad) No Anxiety 0 (Anxiety = feeling nervous) Best Wellbeing 0 (Wellbeing = how you feel overall) Patient’s Name __________________________________________ Date _____________________ Time ______________________ Completed by (check one): Patient Family caregiver Health care professional caregiver Caregiver-assisted BODY DIAGRAM ON REVERSE SIDE ESAS-r Revised: November 2010 149 Please mark on these pictures where it is that you hurt: 150 References Bruera, E., Kuehn, N., Miller, M. J., Selmser, P., & Macmillan K. (1991). The Edmonton Symptom Assessment System (ESAS): A simple method of the assessment of palliative care patients. Journal of Palliative Care, 1(7), 6-9. Nekolaichuk, C, Watanabe, S, Beaumont, C. (2008). The Edmonton Symptom Assessment System: A 15-year retrospective review of validation studies (1991-2006). Palliative Medicine, 22, 111-122. Watanabe, S. M., Nekolaichuk, C., Beaumont, C., Johnson, L., Myers, J., Strasser, F. (2011). A multi-centre comparison of two numerical versions of the Edmonton Symptom Assessment System in palliative care patients Journal of Pain and Symptom Management, 41, 456-468. 151 Appendix B Faces Pain Scale – Revised (FPS-R) 0 2 4 6 8 10 Numbers are not shown to the child. Instructions to the child are: “These faces show how much something can hurt. This face [point to left-most face] shows no pain [or hurt]. The faces show more and more pain [point to each from left to right] up to this one [point to right-most face] – it shows very much pain. Point to the face that shows how much you hurt [right now].” Do not use words like ‘happy’ or ‘sad’. This scale is intended to measure how children feel inside, not how their face looks. Numbers are not shown to children; they are shown here only for reference. Copyright ©2001 International Association for the Study of Pain (IASP). 152 The full-size version of the Faces Pain Scale (FPS-R), together with instructions for administration, are freely available for noncommercial clinical and research use from www.iasp-pain.org References Hicks, C.L., von Baeyer, C.L., Spafford, P., van Korlaar, I., & Goodenough, B. (2001). The Faces Pain Scale – Revised: Toward a common metric in pediatric pain measurement. Pain, 93, 173-183. International Association for the Study of Pain. (2001). Faces Pain Scale – Revised. Retrieved from www.iasp-pain.org. Scale adapted from: Bieri, D., Reeve, R., Champio, G., Addicoat, L., & Ziegler, J. (1990). The Faces Pain Scale for the selfassessment of the severity of pain experienced by children: Development, initial validation and preliminary investigation for ratio scale properties. Pain, 41, 139-150. 153 Appendix C CAGE Questionnaire The CAGE Questionnaire was developed in 1970 by Dr. John A. Ewing as a screening test for problem drinking and potential alcohol problems. It consists of four simple questions which, when administered properly, have been shown to be a valid and reliable screening tool for detection of problem alcohol use. The term “CAGE” is an acronym derived from the four questions that make up the tool. The questionnaire should be completed once as part of an initial multidimensional assessment. When the CAGE questions are included as part of a baseline assessment, they become a natural part of the medical history and there is less chance of eliciting a defensive response from the patient. The CAGE questionnaire screens for problem alcohol use only. It is not designed to screen for other types of substance use. The CAGE questions pertain to the whole life of the patient. It is important that the interviewer make this clear to the patient. Questions related to alcohol use that are not part of the CAGE questionnaire should be asked after the CAGE questions have been completed. For example, questions regarding volume of alcohol consumed, date of last alcohol consumption, and periods of abstinence are important parts of a thorough assessment, but should be asked after the CAGE questions so as not affect the validity of the CAGE questionnaire. 154 Administering the CAGE Questionnaire Ask the following questions in the order in which they are listed. Score one point for each affirmative answer (Yes = 1, No = 0). Do not ask any other questions about alcohol use prior to asking these questions. 1. Have you ever felt you should cut down on your drinking? (Cut down) 2. Have people annoyed you by criticizing your drinking? (Annoyed) 3. Have you ever felt bad or guilty about your drinking? (Guilty) 4. Have you ever had a drink first thing in the morning or (Eye-opener) to get rid of a hangover? Score: _____ /4 2/4 or greater = positive CAGE and suggests increased risk for coping with alcohol or chemical substances Screening for Problem Alcohol Use: The CAGE Questionnaire in Palliative Care Tips for Use and Interpretation of the CAGE in Palliative Care: 1. Uncertainty exists regarding the significance of the date of last alcohol consumption. Though even remote problem alcohol use may complicate current symptom management, it should be kept in mind that some patients may have developed more effective coping skills since an earlier period of problem alcohol use. In these patients, a positive CAGE score may not necessarily indicate complicated symptom management. 2. Most individuals with a positive CAGE score do achieve stable pain control. However, in the positive CAGE group, this occurs at higher opioid doses than in those with negative CAGE scores. The CAGE-AID Questionnaire is a combination of four simple questions that can be used to screen individuals for a history of alcoholism and/or drug addiction (this tool has not had reliability and validity testing). 155 CAGE-AID Questions In the past, have you ever: 1. Tried to Cut down or Change your pattern of drinking or drug use? 2.Been Annoyed by others’ concerns about your drinking or drug use? 3.Felt Guilty about the consequences of your drinking or drug use? 4. Had a drink or used a drug first thing in the morning (Eye-opener) to decrease hangover or withdrawal symptoms? References Aertgeerts, B., Buntinx, F., & Kester, A. (2002). The value of the CAGE in screening for alcohol abuse and alcohol dependence in general clinical populations: A diagnostic meta-analysis, Journal of Clinical Epidemiology, 57(1), 30-39. Delgado-Guay, M.O., & Bruera, E. (2008). Management of pain in the older person with cancer Part 1. Oncology, 22(1), 56-61. Lawlor, P. G., Quan, H., Hanson, J., & Bruera, E. (2000). Screening for alcohol abuse in an advanced cancer population. Supportive Care in Cancer, 8(3), 253. Visit the Edmonton Zone Palliative Care Program website www.palliative.org for further information. 156 Appendix D Table of Equianalgesic Doses of Opioids PO Dose PO:subcut/ IV Ratio Subcut/IV Dose Morphine 10mg 2:1 5mg Codeine 100mg 2:1 50mg Oxycodone 5-7.5mg 2:1 2.5 – 3.75mg* Tramadol 100mg -- -- Hydromorphone 2mg 2:1 1mg Methadone** 1mg -- may not be readily available Fentanyl*** -- -- 50mcg Fentanyl Patch use chart supplied by manufacturer Drug Morphine 10mg po = Hydromorphone 2mg po Morphine 10mg po = Oxycodone 5 – 7.5mg po Morphine 10mg po = Codeine 100mg po Morphine 10mg po = Methadone 1mg po * Oxycodone subcut formulation may not be readily available and may require compounding pharmacy to produce. ** Because of the poor correlation between methadone’s metabolic half-life and the duration of analgesic effect, initiation of Methadone should be undertaken by a physician with expertise. The equianalgesic ratio of Methadone to other opioids changes according to the dose of the previous opioid, making rotation to Methadone a complex undertaking. *** There is some debate as to exact morphine-fentanyl equivalency. The ratio appears to be approximately 100:1. For example, 10mcg parenteral Fentanyl is equivalent to 1mg parenteral Morphine. The equianalgesic ratio between parenteral Fentanyl and transdermal Fentanyl (patch) is 1:1. For example, 25 mcg/h transdermal Fentanyl is equivalent to 25mcg/h IV Fentanyl. 157 Nursing Alert These tables are guidelines. There exists considerable variation in the dose ratio due to inter-individual variability in response to opioids. When switching opioids, doses should be decreased by 25–30% or more to compensate for incomplete cross tolerance, depending on severity of pain and adverse effects. Incomplete cross-tolerance refers to tolerance to the current opioid that does not extend completely to other opioids, thus typically lowering the required dose of the second opioid. Nursing Alert Methadone should be started and titrated under the guidance of a palliative care physician or pain specialist. Administering and managing Methadone is more complex than other opioids and serious complications can result if prescribed incorrectly. A special license is required to prescribe and/or titrate Methadone. Reference Saiger, G. (2012). Pain assessment and management. In D. Oneschuk, N. Hagen & N. MacDonald (Eds.), Palliative Medicine: A Case-Based Manual (pp 27-49). Oxford: Oxford University Press. 158 Appendix E Suggested Stategies for Energy Conservation An Occupational Therapist can assess the person’s functional ability and safety in the home, as well as provide recommendations regarding equipment, and techniques to conserve energy, and maximize independence. Discuss the benefits of Occupational Therapy involvement and refer as needed. Strategies that the person can use include: Activities of Daily Living • • • • Sitting down to bathe. Wear a terry bathrobe to dry off. Installing grab rails in the bathroom. Using an elevated toilet seat. Placing chairs in strategic places in your home to allow rest stops. • Wearing slip-on shoes and button or zipper front shirts. Housekeeping • Scheduling and pacing household tasks throughout the week. • Doing housework sitting down if possible, such as ironing. Using long-handled dust mops may be helpful. • Delegating heavy chores such as shopping and laundry. • Dragging or sliding objects rather than lifting. • Stopping work before becoming tired. • Organizing kitchen items in easy to reach locations (i.e. between shoulder and hip height). Shopping • • • • Organizing list by aisle. Using a grocery cart. Shopping at less busy times. Requesting assistance to the car. 159 Meal Preparation • • • • • Using convenience foods and easy-to-prepare foods. Preparing meals sitting down. Soaking dishes instead of scrubbing and let dishes air-dry. Preparing double portions and freeze half. Arranging your environment so you can easily access frequently used items. Child Care • Plan activities that can be done while sitting down (e.g. drawing, playing computer and board games, reading). • Teach children to climb up on your lap instead of lifting them. • Make a game of household chores so that children will want to help. • Delegate childcare when possible. Workplace • Plan workload to take advantage of peak energy times. Alternate physically demanding tasks with sedentary ones. • Arrange the work environment so you can easily access commonly used equipment and supplies. Leisure • Do activities with a companion. • Select activities that match your energy level. • Balance activity and rest to avoid exertion. Reference Hospital Pharmacists’ Special Interest Group in Palliative Care. (2009). Care beyond cure: Management of pain and other symptoms (4th ed.) Ottawa, Canada: Canadian Society of Hospital Pharmacists. Donovan, E. (1995). Energy conservation. Educational program sponsored by Oncology Nursing Society and Ortho Biotech Inc. (used with permission). 160 Common Questions (and more) about Palliative Care. What is pain? How is pain ssessed? What are different types of pain? Why is a history of substance substa abuse elevant to pain assessment and management? How is it assessed? How H is pain sessed in someone who is confused? Which opioids are preferred fo for use? How hould opioids be ordered? 99 Common Questions (and more) about abou Hospice alliative CareWhat is breakthrough pain? How should break through opioids be dered? What is the maximum dose of an opioid? What is the preferred preferr route for opioid? What is ministration of opioids? What are the potential side effects of an opi drowsiness with opioi rotoxicity? What are the interventions? How can excessive drowsine e be decreased? How are opioids used safely in persons with renal impairment? i What are the causes of myoclonus? 99 Common Questions (and more) mo about ospice Palliative CareDoes unrelieved pain always require increasing the opioid e? Should opioids ever be withheld? Should placebos ever be admin administered? Wh other medications are used in the management of pain? What are the t nonmaceutical interventions to control pain? How can questions regard regarding addictio anaged? How is pain managed in persons with an addiction history? history 99 Commo stions (and more) about Palliative CareWhat can be done when family fam member or request opioids inappropriately? What is anorexia cachexia syn syndrome? Wha he causes? How can appetite and oral intake be optimized? What can c be done t ist persons and their families cope with reduced nutritional intake? Is nutritiona ort appropriate? What is constipation? How is it assessed? 99 Comm Common Questio nd more) about Hospice Palliative Care What causes constipation? What W are the rventions for constipation? How is diarrhea assessed? What are the causes? Wha e the interventions? What is bowel obstruction? How is it assessed? 99 9 Common estions (and more) about Hospice Palliative Care. What are the caus causes? What ar e interventions for bowel obstruction? What is dehydration? How is dehydration ssed? When is it appropriate to hydrate? When is it not appropriate to hydrate? hydration appropriate for a person who has edema? How should hydration hy be ntained? What is nausea and vomiting? What causes nausea and vomiting? vom How usea and vomiting assessed? What are the interventions to control nausea and miting? 99 Common Questions (and more) about Hospice Palliative Care What is irium? What are the causes of delirium? How is delirium assessed? What W are the erventions for delirium? What is dyspnea? What are the causes dysp dyspnea? How is pnea assessed? What are the interventions for dyspnea? What are eedema, ascite d lymphedema? What are the causes? How are edema, ascites and lymphedema l ssed? 99 Common4th Questions (and more) about Hospice Palliative C Care What ar edition developed in collaboration with: he interventions? Should bed-bound people be repositioned regularly? regular What is Edmonton Zone Care Program pruritis? What causes it? How is itPalliative assessed? What are the interventions? interventio What Health Services, Edmonton,(dry Canada tributes to tasteAlberta changes? What are xerostomia mouth) and sto stomatitis (sore 162 uth)? What causes xerostomia and stomatitis? How do you assess xe xerostomia an





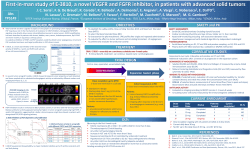


© Copyright 2026