
Communiqué
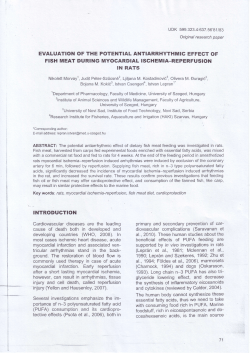
January 2002 Communiqué A Volume 27 Number 1 Features Fluorescence In Situ Hybridization for the Detection of Urothelial Carcinoma Inside Ask Us Abstracts of Interest Calendar Test Updates: • Clostridium difficile Toxin Kit Change • Human Immunodeficiency Virus Type 1 Genotyping Information Requirement • Cystic Fibrosis Test Method Change • Growth Hormone Method Change • Monoclonal Protein Urine Study Introduced W New Test Announcements EBV PCR Quantitative CMV DNA by PCR Communiqué Stabile Building 150 Third Street SW Rochester, Minnesota 55902 1-800-533-1710 [email protected] A M a y o R e f e r e n c e S e r v i c e s P u b l i c a t i o n Fluorescence In Situ Hybridization for the Detection of Urothelial Carcinoma Each year, in the United States, there are approximately 50,000 new cases of urothelial carcinoma (cancer that arises from the lining of the bladder, ureters, renal pelvis, and proximal urethra). Most urothelial carcinomas (UC) originate in the bladder. Early detection of UC recurrence is key to longterm survival. Unfortunately, UC can be difficult to detect. Early symptoms include blood in the urine, or a frequent need to void that may be accompanied by an inability to void. However, these symptoms also are associated with bladder stones, infections, or other benign conditions. Pathology There are 2 main types of UC, papillary and "flat." Approximately 80% of UC are papillary tumors and approximately 20% are flat tumors. Papillary UCs are visible by cystoscopy. They tend to recur but not progress to invasive cancer. Flat UC do not form an easily visible tumor mass, are often clinically aggressive, and tend to progress to invasive cancer. When a UC is surgically removed, it is staged and graded by the pathologist. Staging refers to the extent of tumor spread, namely how deeply it has invaded into the bladder wall (or ureters or renal pelvis) and whether or not lymph node or distant metastases have occurred. (See Table 1.) Grading refers to how differentiated the tumor cells appear when viewed under the microscope. Pathologists’ assign a grade of 1, 2, or 3 to the tumor, based on histologic criteria. Grade 3 tumors (poorly differentiated) have a tendency to recur and progress from a lower to higher stage. Most flat and invasive UC are grade 3 tumors, while most non-invasive papillary tumors are grade 1 and 2. Higher stages and grades are associated with a worse prognosis. Stage and grade help determine the therapeutic approach for individual patients. Urine Cytology Historically, the standard methods employed for the detection and monitoring of UC have been cystoscopy (where a urologist examines the lining of the bladder with a cystoscope) and cytology (where a pathologist examines cells that are voided in the urine). With regard to UC detection in urine specimens, cytology has excellent specificity but suffers from inadequate sensitivity. (See Table 2.) The high specificity of urine cytology means that a diagnosis of UC on urine cytology is almost always correct (a low percentage of false Ta Tis T1 T2 T3 T4 Table 1: Staging of Urothelial Carcinoma non-invasive papillary tumor carcinoma in situ Extension into lamina propria Extension into muscle layer of bladder, ureters, or renal pelvis Extension through the muscle layer Extension through muscle layer and into surrounding organs Figure 1 Abnormal urine specimen. Trisomy 7, visible as 3 green probe signals. CEP 3 (red); CEP 7 (green). Table 2: Sensitivity and Specificity of Urine Cytology1 Sensitivity of Cytology by Grade Specificity Grade 1 Grade 2 Grade 3 21% 53% 78% 96% positives are seen). In contrast, its suboptimal sensitivity for UC means that a negative result is not always correct (eg, tumors are present, but not detected, and thus the result is falsely negative). Because patients with bladder cancer typically are monitored for recurrence by urine cytology at periodic intervals, false-negative test results may allow the patient’s tumor 3 or more months to progress to a higher (potentially incurable) stage. Assays for Urothelial Carcinoma Detection chromosomes or loci. (Note: loci simply means location on a chromosome and does not always imply that a gene is present at that site.) Centromeric probes are useful mainly for determining how many copies of a chromosome are present in a cell. Normal cells have 2 copies of each chromosome. (See Figure 2.) Malignant cells frequently have more than 2 copies of the various chromosomes. Cells that have additional copies of 2 or more different chromosomes are very likely to be malignant. Locus-specific probes provide information about whether genes are amplified or deleted and this information may be of prognostic or therapeutic importance (eg, Her-2/neu amplification in breast cancer). Figure 2 Normal Urine Specimen: CEP 3 (red); CEP 7 (green); CEP 17 (aqua); LSI 9p21 (gold) The suboptimal sensitivity of urine cytology has prompted medical scientists to develop new tests with improved sensitivity for UC detection. Many of these tests, such as BTA-stat and NMP-22, are based on the detection of antigens that are seen at increased levels in the urine of patients with UC. While some of these assays significantly improve sensitivity for UC detection, they all have poorer specificity than cytology (a higher percentage of false positives). The lower specificity is related directly to the fact that antigen levels also may be increased as a result of inflammatory states. Typical specificities for these new assays are approximately 70% (approximately 30% of the positive results are false-positives). Based on these specificities, even with these newer tests, urologists often must perform cystoscopy on these patients to determine if UC truly is present. Fluorescence In Situ Hybridization Most solid tumors are characterized by chromosomal abnormalities. Fluorescence in situ hybridization (FISH) is a technique that utilizes fluorescently-labeled DNA probes to detect chromosomal abnormalities. FISH has applications in many areas including medical genetics, obstetrics, hematology, and oncology. (See Figure 1.) There are 2 general types of FISH probes, centromeric and locus specific probes. A centromere is a constriction point found in all chromosomes. Centromeric probes (CEP) hybridize (attach) to the centromeres of the target chromosomes, while locus-specific probes (LSI) are directed to loci on specific chromosomes. Different colors can be used to probe different chromosomes or loci, allowing the laboratory to enumerate specific 2 FISH for Urothelial Carcinoma Detection Mayo's Cytogenetics Laboratory began development of a FISH assay for the detection of UC in 1998. The laboratory tested 10 different probes for individual and combined sensitivity of urothelial cancer detection. Of the 10 probes, 9 were CEP probes (CEP 3, 7, 8, 9, 11, 15, 17, 18, and X) and 1 was a 9p21 LSI probe. The 9p21 LSI probe hybridizes to a region on the short arm of chromosome 9 where the P16 tumor suppressor gene resides. Genetic alterations that interfere with the function of the P16 tumor suppressor gene (eg, deletion of the gene) play an important role in the formation of 01/02 many UC. It was determined that a combination of CEP 3, CEP7, CEP17, and LSI 9p21 had the highest sensitivity for UC detection. The CEP3, CEP7, CEP17, and LSI 9p21 probes were labeled with red, green, aqua, and yellow fluorophores (the fluorescent molecule that is attached to the DNA probe), respectively and combined into a single, multiprobe mixture. (See Figure 3.) This multitarget, multicolor probe set is now known as UroVysionTM (Abbott Laboratories, Waukegan, IL). UroVysion received FDA approval for monitoring UC patients for tumor recurrence in July 2001. Figure 3 Abnormal cell utilizing UroVysion probe set. A subsequent study compared the sensitivity and specificity of FISH to the FDA approved BTA-stat assay.3 This study demonstrated that the sensitivity of FISH and BTA-stat were not significantly different statistically (81% vs 78%, P=0.63), but that FISH was significantly more specific than BTA-stat (96% vs 74%, P=0.0001). The recently conducted FDA trial to evaluate UroVysion found that FISH was more sensitive than cytology or BTA-stat for UC detection, and more specific than BTAstat for UC detection. Based on these and other studies, FISH has demonstrated the best combination of high sensitivity and high specificity of any test available for the detection of UC. This improved analytic performance (fewer false negative or false positive assays) should improve the clinical management of patients who are being monitored for UC recurrence. Method Sensitivity and Specificity of FISH for Urothelial Carcinoma Detection Combining the 4 probes improved the sensitivity and specificity of the assay compared to just 1 or 2 probes in a mix. Fluorescence In Situ Hybridization (FISH) For Urothelial Cancer, Urine (#81975) offers the high specificity of urine cytology, but is significantly more sensitive than cytology for the detection of UC.1,2 In a study performed at Mayo using the UroVysion probe set, the overall sensitivity of FISH and cytology were 81% and 59% (P=0.001), respectively in 75 patients with biopsy-proven UC.1 When analyzed by grade against cytology, FISH was significantly more sensitive for grade 3 tumors, approached a statistically significant difference for grade 2, and showed no statistical difference for grade 1 tumors. (See Table 3.) The low sensitivity of both FISH and cytology for grade 1 tumors Table 3: Sensitivity and Specificity of FISH for UC1 Sensitivity of Cytology by Grade Specificity Grade 1 Grade 2 Grade 3 36% 76% 97% 96% is not surprising since grade 1 tumors tend to be diploid. Bubendorf et al also have found that FISH using the UroVysion probe set is just as specific as urine cytology, but significantly more sensitive. 2 3 The FISH assay is performed by isolating cells from the urine by centrifugation, fixing the cells, placing the cells on a slide, doing the FISH hybridization and then interpreting the slide with a fluorescence microscope. The slide is scanned primarily, but not exclusively, for cells that have abnormal cytologic features when viewed with the DAPI nuclear counterstain. (See Figure 4.) These features include nuclear enlargement, nuclear irregularity, and mottled staining. The FISH signal pattern is assessed primarily in cells with these features because these cells have a much higher probability of having genetic abnormalities indicative of malignancy. Scanning significantly reduces the time required to evaluate the slide, as some cells visualized with the DAPI stain (eg, neutrophils) are clearly not neoplastic and can be excluded from the evaluation. Scanning also increases the sensitivity of the assay because the technologist scans the entire slide and all cells on the slide, instead of evaluating only a certain number (eg, 100) of consecutive cells. The main type of abnormality that malignant urothelial cells exhibit is "polysomy," where cells have gains of 2 or more chromosomes. A case is considered positive for malignancy if 5 or more cells exhibit polysomy. The cutoff of 5 or more cells with polysomy was based on receiver-operator curves that determined this cutoff gave the best combination of high sensitivity and specificity. Some cases will have numerous abnormal cells. Other cases will have few or no abnormal cells. If a case is positive for cancer because it has 5 or more abnormal cells, the percentage of cells that are abnormal 01/02 Figure 4 Polysomy usually results in an increased nuclear size. Cells can be screened for abnormal morphology with DAPI stain, then assayed with FISH to identify the specific abnormalities. Arrows indicate abnormal cells. copies of chromosome 9 having a deletion) with disomy of other chromosomes (referred to as "homozygous 9p21 deletion" pattern). (See Figure 5.) Figure 5 Homozygous 9p21 deletion. LSI 9p21 gold probes-note the missing gold probe signals in tumor (arrowed) cells. DAPI Specimen Requirement FISH is calculated by determining the percent of 100 consecutive urothelial cells that are abnormal by FISH. Cells that are obviously neutrophils, squamous, or other non-urothelial cells are excluded from these counts. Some cases are high level positives with 30%, 45%, or even 95% of the cells being abnormal. Other cases are low level positives with <10% of the cells being abnormal. The percent abnormal cells roughly reflects the patients tumor burden. In our experience, the vast majority of UC’s are detected because they shed polysomic cells. However, there are other less common FISH abnormalities that can be observed such as trisomy (ie, 3 copies) of one of the chromosomes and disomy (ie, 2 copies) of the other chromosomes, or homozygous 9p21 deletion (both 4 Fluorescence In Situ Hybridization (FISH) For Urothelial Cancer, Urine (#81975) can be performed on any type of urine specimen including voided urine, urine obtained by catheterization, bladder washings, stomal urine specimens, and ureteral washings. We recommend collecting at least 30 mL of urine. However, it may not be possible to obtain this volume for certain specimens, such as ureteral washings. In those situations, the laboratory will perform FISH despite the less than optimum specimen volume. An equal volume of 70%, 95%, or absolute ethanol should be added (other preservatives, such as PreservCyt, also are acceptable) to the urine submitted. The refrigerated (not frozen) specimen should be transported to Mayo Medical Laboratories (MML). The laboratory routinely provides 2-day turnaround for results. Summary Mayo currently is conducting studies to determine if FISH may have a role in screening for UC. Meanwhile, FISH offers a sensitive, specific, and non-invasive test for monitoring patients with urothelial carcinomas. 01/02 References Clostridium difficile Toxin Kit Change 1. Halling KC, King W, Sokolova IA, et al: A comparison of cytology and fluorescence in situ hybridization for the detection of urothelial carcinoma. J Urol, 2000;164(5):1768-75 2. Bubendorf L, Grilli B, Sauter G, et al: Multiprobe FISH for enhanced detection of bladder cancer in voided urine specimens and bladder washings. Am J Clin Pathol 2001;116(1):79-86 3. Halling KC, King W, Sokolova IA, et al: A comparison of BTA-Stat, hemoglobin dipstick, telomerase, and UroVysio™ assays for the detection of urothelial carcinoma in urine. J Urol (accepted for publication) Mayo has converted Clostridium difficile Toxin, Feces #8131 from the Clearview® kit for detecting C difficile toxin in feces, to a Primer® kit. The Primer kit detects both toxin A and toxin B (the Clearview kit detected only toxin A). It has been shown that some diseasecausing strains of C difficile produce only toxin B. Therefore, immunoassays which detect only toxin A will provide false-negative results for those strains. Monoclonal Protein Urine Study Mayo has implemented a new ordering strategy for detection of monoclonal proteins in urine. Monoclonal Protein Study, Urine #8823, (MPSU) provides total protein, immunofixation, and protein electrophoresis testing. This test is useful for the detection and immunotyping of abnormal protein in urine. The specimen requirement is listed below. The introduction of MPSU coincides with a method change in the urine total protein test and deletion of Immunoelectrophoresis, Urine #8179, from the test offerings. The urine total protein test method will change from a Coomassie Blue stain to a Pyrogallol Red stain. Pyrogallol Red stain can result in a higher value for some monoclonal proteins. Consequently, for patients who have previously had a positive test with Coomassie Blue stain, MML will assess the patient's next specimen with both stains to provide an individual comparison. This service will be offered until June 2002. Specimen Requirement 30 mL urine from a 24-hour collection. Although a 24-hour specimen is recommended, a random specimen will be tested if sent. Send three 10-mL specimens refrigerated in plastic 13-mL urine tubes. Preservatives: Preferred: plain Acceptable: toluene or thymol In addition, Electrophoresis, Protein, Urine #82441 preservative options have also changed: Preservatives: Preferred: plain Acceptable: toluene or thymol Human Immunodeficiency Virus Type 1 Genotyping Information Requirement Human Immunodeficiency Virus Type 1 (HIV-1) Genotyping, Plasma #82340 should be performed only on patient specimens that have a viral load ≥1000 copies/mL, as the test does not detect below this limit. MML now requires a recent viral load result (performed within 14 days of genotype draw) be included with the test request. If this information is not provided, the specimen will be held until the information is made available to MML. If the patient does not have a current viral load result, Human Immunodeficiency Virus Type 1 (HIV-1) RNA by Polymerase Chain Reaction (PCR), Quantitative, Plasma #80928 can be added to the test request and will be performed at an additional charge. If the resultant viral load is ≥1000 copies/mL, genotyping will be performed. If the viral load is <1000 copies/mL, the genotyping test will be canceled. Growth Hormone Moves to Automated Method Growth Hormone, Serum #8688 was converted to an FDA-approved automated chemiluminescent immunoenzymatic assay. This method is more sensitive and provides better precision. The new assay is calibrated against pituitary hGH 80/505* and yields results that are lower than the previous method. As a result, the reference values have been adjusted. The preferred specimen transport temperature has changed from frozen to refrigerated (frozen specimens will still be assayed). New Reference Values Males: ≤1.5 ng/mL Females: ≤4.0 ng/mL Previous Reference Values Males: ≤5 ng/mL Females: ≤10 ng/mL *World Health Organization 1st International Standard for growth hormone, derived from human pituitaries (not recombinant), given the code number 80/505 by the National Institute of Biological Standards and Control. 5 01/02 Cystic Fibrosis Test Method Change The American College of Obstetrics and Gynecology and the American College of Medical Genetics released recommendations on mutation testing for cystic fibrosis. In keeping with those recommendations, Mayo has converted Cystic Fibrosis, Diagnosis and Carrier Detection #9497 to a polymerase chain reaction-based assay using line probe (reverse blot) technology in combination with confirmation sensitive gel electrophoresis for all 25 mutations specified for population-based carrier screening. Additionally, this test also detects 2143delT, 3905insT, 394delTT, E60X, Q552X, and S1251N. Intron 8 poly T testing is performed as a reflex test when appropriate. There are related changes to the reference value and CPT codes. Additionally, the test now will be performed twice a week, on Monday and Wednesday. New Reference Values Racial or Ethnic Group Ashkenazi Jewish Mixed European Northern European Hispanic American African American Asian American Mutation Detection Rate - Using ACOG 25 mutation panel 97% 80% 90% 57% 69% Data not available Carrier risk - prior to Cystic Fibrosis Carrier Screening 1/29 1/29 1/29 1/46 1/65 1/90 Carrier risk - with a negative test result for ACOG panel ~1/930 ~1/140 ~1/280 ~1/105 ~1/207 Data not available Table adapted from the ACMG position statement of CF screening (Genetics in Medicine 2001; 3:149-154) Previous Reference Values Omitted New CPT Codes 83891 83894 83901x4 83903x4 83912 Previous CPT Codes 83891 83901x3 83903x2 83912 6 01/02 Abstracts of Interest Clostridium difficile–Associated Diarrhea and Colitis Said Fadi Yassin, MD; Tonia M. Young-Fadok, MD, MS; Nizar N. Zein, MD; And Darrell S. Pardi, MD Clostridium difficile is a spore-forming toxigenic bacterium that causes diarrhea and colitis, typically after the use of broad-spectrum antibiotics. The clinical presentation ranges from self-limited diarrhea to fulminant colitis and toxic megacolon. The incidence of this disease is increasing, resulting in major medical and economic consequences. Although most cases respond quickly to medical treatment, C difficile colitis may be serious, especially if diagnosis and treatment are delayed. Recurrent disease represents a particularly challenging problem. Prevention is best accomplished by limiting the use of broad-spectrum antibiotics and following good hygienic techniques and universal precautions to limit the transmission of bacteria. A high index of suspicion results in early diagnosis and treatment and potentially reduces the incidence of complications. Mayo Clinic Proceedings 2001;76:725-730 Meeting Calendar Interactive Satellite Program . . . February 12, 2002 Advances in the Management of Rheumatoid Arthritis Presenters: Harvinder S Luthra, MD; Alexander P Ruggieri, MD Moderator: Steven R Ytterberg, MD March 12, 2002 Diabetes Prevention and Management Presenter: Mehmood A Khan, MD Moderator: Robert M Kisabeth, MD Upcoming Education Conferences . . . March 12-13, 2002 Practical Spirometry Course Director: Paul D Scanlon, MD Rochester, Minnesota May 1-3, 2002 Integration Through Community Laboratory Insourcing: From Mission Statement to Successful Implementation Hilton in the Walt Disney World® Lake Buena Vista, Florida For additional information regarding the above programs, please contact the Mayo Reference Services Education Office at 1-800-533-1710. 7 01/02 Ask Q: A: ( US Does the new Lyme vaccine cause a positive Lyme serology test? Yes. The screening enzyme-linked fluorescent immunoassay (ELFA) may show a positive ELFA result in subjects who have received the Lyme vaccine, but who have not been exposed to Lyme disease. For this reason Lyme Disease Antibody, Confirmation, Serum #9535 includes a Western Blot test. The Western blot test is required to distinguish a vaccine response (1 band [OpsA] only) from true exposure (5 or more bands). Q: A: What is the benefit of ordering your amplified direct TB test over your routine culture method for TB? Conventional culture methods typically take 2-8 weeks to detect Mycobacterium tuberculosis, although results may be available as early as 1 week in uncommon cases. MML offers rapid detection of M tuberculosis by Mycobacterium Tuberculosis, Amplified Direct Test, #81383. The M tuberculosis Direct (MTD) test provides detection of M tuberculosis complex ribosomal ribonucleic acid (rRNA) in less than 1 hour. While the laboratory charges for the direct test are higher than the laboratory charges for traditional culture, early detection and prompt treatment is critical to reduce the spread of the disease. Rapid diagnosis also allows more appropriate use of isolation rooms and reduced hospital expenses. Communiqué Editorial Board: Communiqué Staff: Jane C Dale, MD Managing Editor: Denise Masoner Tammy Fletcher Medical Editor: Jane C Dale, MD Suzanne Leaf-Brock Denise Masoner Anita Workman Contributors: David J Brandhagen, MD; Virgil F Fairbanks, MD; Kevin C Halling, MD, PhD; Darrell S Pardi, MD; Stephen N Thibodeau, PhD The Communiqué is published by Mayo Reference Services to provide laboratorians with information on new diagnostic tests, changes in procedures or normal values, and continuing medical education programs and workshops. A complimentary subscription of the Communiqué is provided to Mayo Medical Laboratories’ clients. Mayo Reference Services Communiqué Stabile Building 150 Third Street SW Rochester, Minnesota 55902 1-800-533-1710 http://www.mayo.edu/mml © 2002, Mayo Press MAYO, MAYO CLINIC and the Mayo triple-shield logo and Mayo Reference Services are marks of Mayo Foundation for Medical Education and Research. MC2831/R0102 Printed on 50% recycled paper with 10% post-consumer waste.





















© Copyright 2026