
CD5+, CD11c+, CD20+ hairy cell leukemia [letter
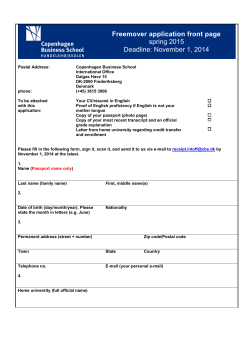
From www.bloodjournal.org by guest on December 4, 2014. For personal use only. 1991 77: 1617-1619 CD5+, CD11c+, CD20+ hairy cell leukemia [letter; comment] PS Heimann, JW Vardiman, W Stock, LC Platanias and HM Golomb Updated information and services can be found at: http://www.bloodjournal.org/content/77/7/1617.citation.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved. From www.bloodjournal.org by guest on December 4, 2014. For personal use only. CORRESPONDENCE 1617 CD5+, CDllc’, CD20’ HAIRY CELL LEUKEMIA To the Editor: In their recent report in Bloorl, Wormsley et a1 concluded that CDllc+,CD5+ B-cell chronic leukemias are subgroups of chronic lymphocytic leukemia (CLL) and prolymphocytic leukemia (PLL) rather than of hairy cell leukemia (HCL).’ We do not disagree that chronic B-cell lymphoproliferative disorders other than HCL may demonstrate CDllc’, and have previouslyreported on such cases; but we do have reservations regarding the implication that HCL should be excluded as a diagnostic possibility when the leukemic cells possess the CD5 antigen in addition to CDllc and B-cell markers. We have recently encountered a case of HCL with CD5+, CDllc+, CD20+ leukemic cells, which points out the need for cautious interpretation of immune surface markers in the context of clinical, morphologic, and cytochemicalfindings. The patient is an 85-year-old retired physician who had been in excellent health until 1985, when moderate splenomegaly was discovered on a routine physical examination at another institution. A CBC performed at that time showed a white blood cell count (wbc) of 6,70O/kL with 9% neutrophils and 37% “atypical lymphocytes,” a hemoglobin (Hgb) level of 12.3 g/dL, and a platelet count of 177,OOO/pL. A bone marrow biopsy was performed and a tentative diagnosis of HCL was made. The patient was followed with no medical intervention, but has had routine physical examinationsevery 6 months. The patient was referred to the University of Chicago for additional evaluation in July 1990. Moderate splenomegaly was present, but he had no lymphadenopathy or hepatomegaly. The wbc was 9,10O/p,L with 52% “hairy cells,” 33% small lymphocytes, 12% neutrophils, and 3% monocytes. The Hgb was 11.8 g/dL and the platelet count was 11O,OOO/pL. The “hairy cells” were large (12 to 15 p”, and had round to oval, eccentrically placed nuclei with delicate chromatin and inconspicuous nucleoli, as well as abundant cytoplasm with villous margins (Fig 1). More than one half of the Fig 1. This photomicrographillustratesthe featuresof the neoplastic cells in the peripheral blood smear of the patient (Wright‘s stain; original magnification x 1,000). hairy cells had tartrate-resistant acid phosphatase reactivity. A bone marrow biopsy specimen was only 10% cellular, but nearly one half of the marrow cells had histologic features consistent with those of HCL. Immunophenotypic studies of peripheral-blood mononuclear cells were performed by flow cytometry as well as by the alkaline-phosphatase-anti-alkalinephosphatase (APAAP)technique on peripheral blood smears. The immunophenotype of the neoplastic cells was CD5+, CDllc+, CD19+, CD20+, and CD25+. This immunophenotypewas confirmed by examination of the hairy cells on APAAP-stained peripheral blood smears. Dual staining by flow cytometry showed that CD5 and CD20 as well as CD19 and From www.bloodjournal.org by guest on December 4, 2014. For personal use only. CORRESPONDENCE 1618 C D l l c were coexpressed on the neoplastic cells. Therefore, the leukemic cells from our patient were CD5+, CDllc', CD20+, but the clinical, morphologic, and cytochemical findings were those of HCL. Although we agree with Wormsely et a1 that additional prospective studies of CDllc', CD5+ B-cell leukemias are required to show whether they are a clinically significant subgroup of lymphocytic neoplasms, we consider our case as demonstrating that this phenotype is not necessarily confined to B-CLL or B-PLL, but may, in fact, be found in HCL as well. Until additional information regarding such unusual cases is acquired, we believe that it is prudent to interpret monoclonal antibody studies cautiously, and to rely on current clinical and morphologic findings for diagnostic purposes. PRISCILLA S. HEIMANN JAMES W. VARDIMAN Department ofPathology WENDY STOCK LEONIDAS C. PLATANIAS HARVEY M. GOLOMB Department of Medicine University of Chicago Hospitals Pntzker School of Medicine Chicago, IL REFERENCES 1. Wormsley SB, Baird SM, Gadol N, Rai KR, Sobol RE: Characteristics of CDllc' CD5' B-cell leukemias and the identification of novel peripheral blood B-cell subsets with chronic lymphoid leukemia immunophenotypes. Blood 76:123,1990 2. Vardiman JW, Gilewski TA, Ratain MJ, Bitter MA, Bradlow BA, Golomb HM: Evaluation of Leu-M5 (CDllc) in hairy cell leukemia by the alkaline phosphatase anti-alkaline phosphatase technique. Am J Clin Pathol90:250,1988 RESPONSE We agree that the results of immunophenotypic analyses should be interpreted in the context of conventional morphologic, cytochemical, and clinical diagnostic criteria. However, it is well recognized that the diagnosis of a small proportion of chronic B-cell leukemias will be problematic owing to the considerable heterogeneity of these diseases and their overlap of morphologic, immunophenotypic, and clinical features. These difficulties are reflected by the case of CDS+, CDllc+ hairy cell leukemia (HCL) described by Heimann et al, our series of CD5+, CDllc' chronic lymphocytic leukemias (CLL),' and the recent report by Hanson et al' describing CDllc+ B-cell leukemias with CLL morphology and clinical characteristics associated with HCL. It should be noted that the case described by Heimann et a1 is uncommon, as CD5 is rarely expressed by leukemias with HCL m~rphology.~ In our series of 119 patients with CD5+ B-cell immunophenotypes, 26 (22%) were CDllc'and all CDllc' cases with peripheral blood smears available for review (n = 14) had CLL morphology.' Many of our cases with CD5+, CDllc' B-cell immunophenotypes were characterized by the presence of large lymphocytes with abundant cytoplasm.' Similar large lymphocyte morphologic features were reported by Hanson et alzin their study of CDllc' B-cell leukemias with CLL morphology. While our CDllc+ cases shared morphologic characteristics with those reported by Hanson et al, the presenting clinical features of our cases were different in some respects. In our patients, lymphadenopathy was common (9 of 14 cases) and splenomegaly was present in 6 of 14 patients.' In the patients studied by Hanson, et al: generalized lymphadenopathy was uncommon (1 of 14 cases) and splenomegaly was frequently obselved (11 of 14 cases). All of the patients in our study had CD5' immunophenotypes,' whereas only 7 of 14 patients evaluated by Hanson et a1 were CDS'? As the number of patients evaluated in these studies was small, definition of the morphologic, immunophenotypic, and clinical characteristics of CDllc' B-cell leukemias with CLL morphology will require assessment of a larger number of patients. Nevertheless, our results and those of others1.2,4.S indicate ' that CDllc is not restricted to cases with HCL morphology and that CDllc may be expressed by B-cell leukemias with CLL morphology.',' Prospective studies of larger numbers of patients will be necessary to determine whether CDllc' B-cell leukemias with CLL morphology represent a distinct pathologic entity of clinical significance. SUSAN B. WORMSLEY Cytometncs, Inc Division of Specialty Laboratories, Inc. San Diego, CA STEPHEN M. BAIRD Departments of Pathology and the Cancer Center University of Califomia VeteransAdministration Medical Center San Diego, CA NANCY GADOL Becton Dickinson Mountain Wew, CA KANTI R. RAI Long Island Jewish Hospital New York, NY ROBERT E. SOBOL Cancer Center University of Califomia Mercy Hospital Medical Center San Diego, CA REFERENCES 1. Wormsley SB, Baird SM, Gadol N, Rai KR, Sobol RE: Characteristics of CDllc'CDS' chronic B-cell leukemias and the identification of novel peripheral blood B-cells subsets with chronic lymphoid leukemia immunophenotypes. Blood 76:123,1990 2. Hanson CA, Gribbin TE, Schnitzer B, Schlegelmilch JA, Mitchell BS, Stoolman LM: C D l l c (LEU-M5) expression charac- terizes a B-cell chronic lymphoproliferative disorder with features of both chronic lymphocytic leukemia and hairy cell leukemia. Blood 76:2360,1990 3. Foon KA, Todd R F 111: Immunologic classification of leukemia and lymphoma. Blood 68:1,1987 4. Vardiman JW, Gilewski TA, Ratain MJ, Bitter MA, Bradlow From www.bloodjournal.org by guest on December 4, 2014. For personal use only. CORRESPONDENCE BA, Golomb HM: Evaluation of Leu-M5 (CDllc) in hairy cell leukemia by the alkaline phosphatase antialkaline phosphatase technique. Am J Clin Pathol90:250,1988 1619 5. Sheibani K, Sohn CC, Burke JS, Winberg CD, Wu AM, Rappaport H Monocytoid B-cell lymphoma: A novel B-cell neoplasm. Am J PathoI 124:310,1986











© Copyright 2026