
At present, it is difficult to identify patients at
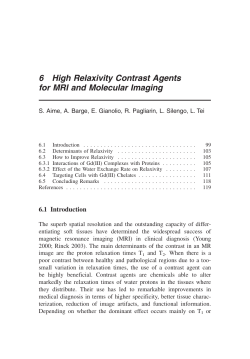
_ q g Investigations and research Advances in cardiovascular molecular imaging: the case of Annexin A5 Apoptosis helps identify patients at risk of stroke or myocardial infarction. L. Hofstra Department of Cardiology, University Hospital of Maastricht, Maastricht, the Netherlands. J. Decker Technology Officer Molecular Imaging and Diagnostics, Philips Medical Systems, Best, the Netherlands. At present, it is difficult to identify patients at risk of acute vascular events such as stroke or myocardial infarction. The inability to identify these patients results in thousands of acute vascular events every year, leading to extensive morbidity and mortality. An attractive target for the identification of patients at risk is apoptosis, which is prominent in myocardial infarction and in atherosclerotic lesions that have resulted in stroke. Another clinical problem that has not yet been solved is the need to prevent the development of heart failure following acute myocardial infarction. The heart has very limited regenerative capacity, so that cardiac cells that undergo apoptotic cell death during acute myocardial infarction are not replaced. We therefore need to develop strategies that inhibit the loss of cardiac cells, for example through pharmaceutical intervention to prevent the development of heart failure. These examples indicate that the ability to image apoptosis could improve the diagnosis and treatment of patients with cardiovascular disease. Annexin A5 is a protein which binds to cells undergoing apoptotic cell death. In this article we briefly discuss the opportunities for using Annexin A5 for the non-invasive detection of apoptosis in patients with cardiovascular disease. Molecular imaging Molecular imaging offers opportunities for early diagnosis and therapy 40 MEDICAMUNDI 49/2 2005/8 Molecular imaging is a novel and rapid emerging discipline, creating tremendous opportunities for early diagnosis and for guiding therapy [1]. In contrast to conventional imaging, such as computed tomography and/or magnetic resonance imaging, which aims to visualize the anatomical or physiological consequences of a disease, molecular imaging is focused on the visualization of the molecular defects that underlie the beginning of the disease process. The technology of molecular imaging is based on the labeling of probes that specifically target molecules that are only expressed by diseased cells. This, in theory, could be of great help in the early diagnosis of disease. Especially in cancer, where molecular changes in precancerous lesions occur years before an actual tumor develops, this information may lead to substantial diagnostic and therapeutic benefit for the patients. Molecular imaging is also of value in various cardiac diseases, as molecular events often precede clinical symptoms, offering great opportunities for the prevention of - often fatal - cardiac events. Another potential benefit of molecular imaging is providing a biological signature for detected anatomical lesions, such as tumors of unknown origin or stenotic lesions in atherosclerotic vessels. For example, it has become clear in the last decade that the biology of coronary atherosclerotic lesions is of more importance than the extent of stenosis in triggering acute vascular events. It is obvious that this information could be of great help in improving clinical decisionmaking and providing our patients with the best possible therapeutic care. Other, less well-known advantages of molecular imaging are strongly related to novel therapeutic strategies. The tremendous progress made in recent decades in understanding the fundamental changes underlying diseases has resulted in new therapeutic strategies that specifically target molecular defects in diseased cells such as cancer cells [2]. Molecular imaging could help to provide novel read-outs for the visualization of the efficacy of these targeted therapies, by imaging specific target substrates. Finally, the experience in the use of specific probes for the imaging of biological events will help us to use these probes as carriers for drugs, enabling local drug delivery. The local delivery of drugs could help to increase the local concentration of drugs and prevent side effects. This approach could be very advantageous in the treatment of atherosclerosis, where local treatment of plaques could be more efficient, with fewer unwanted side effects. _ q g One of the most promising developments in molecular imaging that has emerged in recent years, even in clinical studies, is the use of Annexin A5. Annexin A5 has the unique property of targeting and binding to cells undergoing cell death through apoptosis [3]. Apoptotic cell death is prominent in both cancer and cardiovascular diseases and, therefore, provides an attractive target for imaging these diseases. In this article we briefly describe the various aspects of molecular imaging using Annexin A5 in cardiovascular disease. We also discuss the development of various Annexin A5-based probes, their applications in animal models of cardiovascular disease and, finally, their application in patients with cardiovascular disease. Apoptosis as a molecular imaging target for imaging cardiovascular disease One of the most prominent unmet clinical needs in cardiovascular medicine is preventing the development of heart failure. Heart failure affects millions of patients in the Western world, and is associated with a poor quality of life and a high risk of mortality. An important cause of heart failure is acute myocardial infarction. In about 30% of cases myocardial infarction is followed by expansion of the infarct and dilatation of the healthy segments of the left ventricle, resulting in poor function and heart failure. The dilatation of the heart, often referred to as remodeling, is associated with changes in the extracellular matrix, cell death and fibrosis. These biological processes are targets for molecular imaging. For example, probes targeted to the formation of newly formed collagen could be of help in defining the remodeling process and for recognizing patients at risk of the development of heart failure. Furthermore, the loss of cardiomyocytes through apoptosis may be an attractive target to image, both in the acute phase of myocardial infarction and in the remodeling phase. Experimental models of disease have shown that the transition of the normal or hypertrophied heart to a dilated heart is associated with a high rate of apoptotic cell death. So far, the medical community has not succeeded in developing effective diagnostic tools for recognizing patients at risk of acute vascular events, such as acute myocardial infarction. In 90% of cases the substrate leading to myocardial infarction is rupture of an unstable atherosclerotic plaque. Rupture of unstable atherosclerotic lesions is also the main mechanism leading to stroke in patients with carotid artery lesions. Extensive research in the last two decades has shown that unstable plaques are defined by a high content of inflammatory cells such as macrophages. The current concept is that these inflammatory cells secrete cytokines, such as matrix-metallo-proteinases, which degrade the extracellular matrix and weaken the fibrous cap. Figure 1. Optical imaging showing the time course of binding of fluorescently labeled Annexin A5 following ischemia and reperfusion of the mouse heart in vivo. In addition to inflammation, cell death through apoptosis is a prominent feature of unstable plaques. Therefore, detection of apoptosis may also be of value in the identification of unstable coronary lesions. In the following sections we present pre-clinical and clinical studies demonstrating that noninvasive detection of apoptosis is feasible, and could provide us with a promising diagnostic tool. Experimental models As mentioned above, detection of cell death is potentially of great value in the assessment of cardiomyocyte loss during cardiac diseases, and MEDICAMUNDI 49/2 2005/8 41 _ q g for detection of apoptosis in the unstable atherosclerotic plaque. At the University of Maastricht in the Netherlands, we have developed a molecular imaging methodology for visualizing apoptotic cell death in vivo. This methodology is based on the recognition of specific cell membrane changes that occur during apoptosis. Annexin A5 is a specific and reliable tool for detecting apoptotic cells. We have shown the feasibility of detecting plaque instability. 42 MEDICAMUNDI 49/2 2005/8 One of the earliest events in apoptosis is the externalization of phosphatidyl serine from the inner leaflet of the plasma membrane to the outer leaflet. We and others have demonstrated that labeled Annexin A5, which has high affinity for phosphatidyl serine, is a specific and reliable tool for the detection of apoptotic cells under a variety of conditions, including ischemia and reperfusion in vivo in the murine heart [4]. These data show that the use of fluorescently labeled Annexin A5 in combination with optical imaging allows for the detailed detection of the kinetics and extent of cell death in the heart. In current studies, labeled Annexin A5 is being used for the detection of myocyte loss during development of left ventricular failure, both in experimental models and in patients. Figure 1 shows the use of fluorescently labeled Annexin A5 in combination with optical imaging to follow the time course of the binding of Oregon-Green labeled Annexin A5 following ischemia and reperfusion of the mouse heart in vivo. Ischemia is induced by ligation of the LAD, which is one of the main coronary arteries. To achieve restoration of flow (reperfusion) the ligature around the LAD is released. This model closely mimics the clinical setting of patients with acute myocardial infarction, who are treated by reperfusion. During ischemia (Figure 1a and b) slight uptake of the labeled Annexin A5 is visible in the area at risk. However, after the onset of reperfusion (Figure 1c) Annexin A5 binding to the area at risk rapidly increases. Figure 1c, d, e and f show the situation at 2, 8, 20 and 45 minutes after reperfusion respectively. There is no increase in binding of Annexin A5 after 20 minutes. These data indicate that reperfusion is a strong trigger for the induction of cell death in the heart. In close collaboration with the group of Prof. Jagat Narula we have shown the feasibility of detecting plaque instability in an animal model of atherosclerosis using radio-labeled Annexin A5 (99mTc-Annexin V) [5]. These data show that the extent of Annexin A5 uptake in the atherosclerotic lesions in the aorta of high-fat treated rabbits correlates well with the complexity of the lesions and the content of inflammatory cells. In addition, it was shown that most apoptotic cells in the atherosclerotic lesions were macrophages. These data suggest that targeting apoptotic cells and/or inflammatory cells in atherosclerotic lesions may be a way to identify patients at risk of acute vascular events. Figure 2 shows apoptosis and/or inflammation in experimentally induced atherosclerosis in the rabbit. Figure 2a-c shows the uptake of radiolabeled Annexin A5 in a high-fat treated rabbit following injury of the aorta. At the time of injection (Figure 2a) of Annexin A5 some bloodpool is visible. Two hours after injection (Figure 2b) enhanced uptake is seen in the aortic region, but is difficult to distinguish from the background signal. Ex-vivo imaging (Figure 2c) shows the enhanced uptake of Annexin A5 in the aorta. Histologic analysis confirmed the binding of Annexin A5 to the atherosclerotic lesions, mainly to apoptotic macrophages. In the corresponding stages in the control animal (Figure 2d-f ) no enhanced uptake of Annexin A5 is visible. Clinical applications of cardiovascular molecular imaging Myocardial infarction The first demonstration of molecular imaging in a clinical setting using Annexin A5 was in patients with acute myocardial infarction [6]. SPECT imaging showed extensive binding of technetium-labeled Annexin A5 in the area at risk in the left ventricle on day 1 after acute myocardial infarction. The data suggest that at least some of the heart cells in the infarct area undergo apoptotic cell death at an early stage, indicating that cell death could be prevented by timely administration of cell-death inhibiting compounds. The area of uptake of Annexin A5 correlated well with the defect found later by perfusion imaging of the heart on day 3, supporting the view that the uptake of Annexin A5 as seen on day one indeed indicates loss of cells and infarction. Figure 3 shows SPECT images of technetiumlabeled Annexin A5 in a patient with acute myocardial infarction. The image on day 1 (Figure 3a) shows enhanced uptake in the anterior wall of the heart (arrow), indicating acute cell death of heart cells in this area. Perfusion imaging of this patient on day 3 shows a defect at exactly the same site. A defect on perfusion imaging indicates myocardial infarction. Unstable plaque In a preliminary study we have shown that molecular imaging with Annexin A5 may also be able to identify plaque instability in patients [7]. _ q g Figure 2. Apoptosis and inflammation in experimentally induced atherosclerosis in the rabbit. As a clinical model, we used carotid artery disease, because of the easier accessibility of the head and neck region as compared with the heart. In addition, the contraction of the heart and ventilation of the lungs would make it difficult to exactly localize technetium-labeled Annexin A5 in the SPECT images. Two different patient groups with significant carotid artery stenosis were investigated in the atherosclerosis imaging study. The first group comprised patients with a recent transient ischemic attack (TIA), which is a sign of clinical plaque instability. The second group comprised patients with carotid artery lesions and a remote history of a TIA. In the patients with a recent TIA, enhanced uptake of Annexin A5 was observed at the site of the symptomatic carotid artery lesion, which was confirmed by histologic analysis of the surgically removed stenotic lesions (Figure 4). Furthermore, these lesions showed signs of plaque instability, including infiltration of inflammatory cells and cell death. By contrast, in the patients with carotid artery lesions and a remote history of a TIA, there was no uptake of Annexin A5, and stable atherosclerotic lesions characteristics a b were observed. These data suggest that SPECT imaging of technetium-labeled Annexin A5 could be used for clinical identification of patients at risk of undergoing a stroke and/or TIA. Figure 3. SPECT imaging of technetium-labeled Annexin A5 in a patient with acute myocardial infarction. Figure 3a. Image obtained on day 1 after the infarction, showing enhanced uptake in the anterior wall of the heart (arrow), indicating acute cell death of heart cells in this area. Figure 3b. Perfusion imaging on day 3 shows a defect at exactly the same site. Figure 4a is a SPECT image showing enhanced uptake of technetium-labeled Annexin A5 at the site of the symptomatic carotid artery (arrows) in a patient with a recent TIA. The enhanced uptake of Annexin A5 indicates cell death and/or inflammation. Figure 4b shows the histologic analysis of the unstable carotid artery plaque in the same patient, characterized by macrophage infiltration and Annexin A5 staining (brown staining). Figure 4c shows a SPECT image in a different patient, who had a TIA 3 months before imaging. In this case, no uptake of Annexin A5 is observed. Histologic analysis of the carotid artery plaque MEDICAMUNDI 49/2 2005/8 43 _ q Figure 4. Investigation of carotid artery plaque using technetium-labeled Annexin A5. Figure 4a. SPECT image in a patient with a recent TIA showing enhanced uptake (arrows). Figure 4b. Histologic analysis of the unstable carotid artery plaque in the same patient showing macrophage infiltration and Annexin A5 (brown staining). Figure 4c. SPECT image in a different patient, who had a TIA 3 months before imaging. No uptake of Annexin A5 is observed. Figure 4d. Histologic analysis of the carotid artery plaque shows a stable atherosclerotic lesion and no binding of Annexin A5. g a b c d (Figure 4b) shows a stable atherosclerotic lesion and no binding of Annexin A5. One way to use this information would be to determine which patients with significant carotid artery lesions should be scheduled for surgical removal of the stenotic lesions. In this context it is worthwhile to mention that in the USA alone 140,000 patients per year undergo carotid artery endarterectomy. Molecular imaging gives us the potential to revolutionize clinical medicine. 44 MEDICAMUNDI 49/2 2005/8 challenge here is to obtain sufficient sensitivity with the use of the MR contrast media. For instance, a widely used MR contrast agent, gadolinium, has a sensitivity equivalent to about 1% of that of radionuclide tracers such as technetium. To overcome this issue, the industry has embarked on developing the technology to either multiply the number of contrast molecules per imaging probe, or to develop liposomal formulation containing MR contrast agents. The data also supports the potential use of this technology for the detection of unstable coronary lesions. In the USA alone, 13 million patients suffer from coronary artery disease. The detection of unstable coronary artery lesions will largely depend on our ability to deal with the movement of the heart, and the relatively small size of the coronary atherosclerotic lesions. It is believed that advances in imaging equipment, such as multislice computed tomography in combination with SPECT or PET imaging (Figure 5) may provide the sensitivity and high spatial resolution needed to solve these problems. In the end, patients will benefit from the combination of innovative molecular imaging probes and advanced imaging equipment. Conclusion MR imaging is another promising technology in the molecular imaging field. By labeling imaging probes with MR contrast media, the molecular imaging information could be combined with precise anatomical information. The main The creation of successful molecular imaging tools will benefit greatly from a close interaction between various disciplines, ranging from molecular biology and clinical medicine to the development of innovative imaging techniques. Molecular imaging gives us the potential to revolutionize clinical medicine. The success of molecular imaging will largely depend on our ability to design tools that will have an impact on clinical decision-making and patient management. The fastest way to create tools that have clinical impact is to focus on technologies which have established clinical success in molecular imaging, such as SPECT technology, and to apply these diagnostic tools to unmet clinical needs in medicine. The use of combined technologies, such as SPECT/CT imaging, may provide the necessary combination of high spatial resolution and high sensitivity. _ q g Figure 5. A combined SPECT imaging and multislice CT system (Philips Precedence). Annexin A5 is an attractive candidate for molecular imaging in cardiovascular disease. Extensive clinical studies indicate that Annexin, labeled with radionuclide tracers, is a safe product. In addition, recent studies suggest that noninvasive imaging of apoptosis and inflammation using Annexin A5 offers an effective tool for detecting unstable atherosclerotic lesions. Consequently, the use of Annexin A5 imaging could help to improve diagnosis and treatment for millions of patients who are at risk for stroke and/or myocardial infarction Annexin A5 imaging could improve diagnosis and treatment for millions of patients. References 1. Weissleder R, Mahmood U. Molecular Imaging. Radiology 2001; 219(2): 316-333. 2. Weissleder R. Scaling Down Imaging: Molecular Mapping of Cancer in Mice. Nat Rev Cancer 2002; 2,1: :11-18. 3. Martin SJ, Reutelingsperger CP, McGahon AJ et al. Early Redistribution of Plasma Membrane Phosphatidylserine is a General Feature of Apoptosis Regardless of the Initiating Stimulus: Inhibition by Overexpression of Bcl-2 and Abl. J Exp Med 1995; 182,5: 1545-1556. 4. Dumont EA, Reutelingsperger CP, Smits JF et al. Real-Time Imaging of Apoptotic Cell-Membrane Changes at the Single-Cell Level in the Beating Murine Heart. Nat Med 2001; 7.12: 1352-1355. 5. Kolodgie FD, Petrov A, Virmani R et al. Targeting of Apoptotic Macrophages and Experimental Atheroma with Radiolabeled Annexin V: A Technique with Potential for Noninvasive Imaging of Vulnerable Plaque. Circulation 2003; 108,25: 3134-3139. 6. Hofstra L, Liem IH, Dumont EA et al. Visualisation of Cell Death In Vivo in Patients with Acute Myocardial Infarction. Lancet 2000; 356, 9225: 209-212. 7. Kietselaer BL, Reutelingsperger CP, Heidendal GA et al. Noninvasive Detection of Plaque Instability with use of Radiolabeled Annexin A5 in Patients with Carotid-Artery Atherosclerosis. N Engl J Med 2004; 350,14: 1472-1473. MEDICAMUNDI 49/2 2005/8 45











© Copyright 2026