
Walsall Safeguarding Children Board W4 Serious Case Review
Better Together for Children JANUARY 2015 WALSALL SAFEGUARDING CHILDREN BOARD W4 SERIOUS CASE REVIEW Reported by: Gill Baker, OBE, BA (Hons) Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review GLOSSARY ADHD Attention Deficit and Hyperactivity Disorder CAF Common Assessment Framework CAFCASS Children and Family Court Advisory and Support Service CAMHS Child and Adolescent Mental Health Service CCG Clinical Commissioning Group CLR Critical Learning Review COG Children with Complex Needs Operational Group Panel CPR Cardiopulmonary resuscitation EPP External Placements Panel (formerly COG) IMR Individual Management Review LAC Looked After Children LACCP Looked After Child Care Plan LADO Local Authority Designated Officer Ofsted Office for standards in Education, Children’s Services and Skills OR Overview Report POT Position of Trust RCP Residential Care Provider and owner of 3 of the Children’s Homes referenced within this review SAFS Safeguarding & Family Support Service SCR Serious Case Review SQIFA Screening Questionnaire Interview for Adolescents WSCB Walsall Safeguarding Children Board YJB Youth Justice Board YJS Youth Justice System YOS Youth Offending Service Note: Prior to a service design in Autumn 2012 West Mercia YOS was known as Shropshire, Telford & Wrekin YOS (S,T & W YOS) 1 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review CONTENTS Page Introduction 4-5 Purpose, Scope and Terms of Reference 4-8 Process 8-10 Serious Case Review Panel Members 10-11 Individual Management Reviews and Information Reports 11-14 Ethnicity, Diversity and Cultural Issues 14-15 Background 15-17 Chronological sequence of events 17-32 Family Engagement 32-34 Analysis and Recommendations 34-43 Good Practice 43 Changes/Improvements to Service Delivery actioned prior to this SCR 43-44 Single Agency Recommendations 44 Lessons Learnt & Conclusion 44-45 Appendix A - WSCB Recommendations Appendix B - Single Agency Recommendations and Action Plan Appendix B - Bibliography 2 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 1. Introduction 1.1 At approximately 2335 hours on 15 December 2012, two separate ‘999’ emergency calls were received to report a house fire with a person trapped inside. Fire, Ambulance and Police officers attended the scene and the Young Person, who had made one of the 999 calls, was located trapped in an upstairs bedroom. She was carried out of the premises by fire officers who commenced CPR which was continued by paramedics but resuscitation proved unsuccessful and the Young Person was pronounced dead at 0025 hours on 16 December 2012. The Young Person had been in the care of Walsall Children’s Social Care for one year and 10 months during which time she had been resident in several homes in West Midlands, Cambridgeshire and in Shropshire. The scene of the fire was at a care home in Ellesmere, Shropshire where she was the only resident with two adult carers. During her time in care it was found that the Young Person had complex needs and continually exhibited challenging, disruptive and risk-taking behaviour. 1.2 A police investigation was commenced regarding the fire, which revealed that the Young Person had barricaded herself into her bedroom by placing a mattress against the door which she locked from the inside and she then set fire to the mattress. This action followed a dispute with her carers when she was denied continued access to the internet for that night. Despite unlocking the bedroom door with a master key the carers were unable to gain access to the bedroom due to the barricade and whilst one of the carers phoned the emergency services, the other unsuccessfully attempted to extinguish the flames. The police concluded that all available evidence indicated that the Young Person had deliberately set the fire. A report was submitted to the Coroner and at an Inquest Hearing on 6 August 2013, it was concluded that the cause of death was accidental and that the Young Person had died as a result of inhalation of products of combustion. 3 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 1.3 The case was subsequently discussed at the Walsall Safeguarding Children Board (WSCB) when it was agreed to await the findings of the Inquest and of initial scoping of agency involvement before deciding whether a serious case review should be undertaken. After receipt of information and of the conclusion of the Coroner’s proceedings, Robert Lake, the Independent Chair of the WSCB, agreed on 9 April 2014 that a serious case review should be undertaken as the case met the following criteria: Working Together to Safeguard Children March 2013 ‘A serious case is one where: (a) abuse or neglect of a child is known or suspected; and (b) either — (i) the child has died; or (ii) the child has been seriously harmed and there is cause for concern as to the way in which the authority, their Board partners or other relevant persons have worked together to safeguard the child’ 1.4 Due to the involvement of agencies in Shropshire liaison was made with Shropshire Safeguarding Children Board who provided information, assistance and panel membership for this SCR. 2. Purpose, Scope and Terms of Reference 2.1 The purpose of this serious case review, is as outlined in the government document ‘Working Together to Safeguard Children’. The aim being to: • review the circumstances leading to the incident that caused the death of the Young Person, establish why professionals took the decisions they did and establish what lessons are to be learned from the case about the way in which local professionals and organisations work individually and across the system to safeguard and promote the safety and welfare of children. • identify clearly what those lessons are both within and between agencies, how and within what timescales they will be acted on and 4 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review what is expected to change as a result. To apply these lessons to service responses including changes to the policies and procedures as appropriate. • improve intra and inter-agency working and better safeguard and promote the welfare of children. 2.2 It was determined that this review should focus on the period between 15 February 2011 until 15 January 2013. However it was stipulated that should agencies identify information prior to or post that period, which is relevant to the findings of the SCR then that should be included. This review should include contact with extended members of the family and any other significant persons only in so much as it is relevant to the decision making and safeguarding of the Young Person. 2.3 The most important issues to be addressed by agencies, in trying to learn from this case were identified in the Terms of Reference as: Generic Issues Were practitioners aware of and sensitive to the needs of the children in their work, and knowledgeable both about potential indicators of abuse or neglect and about what to do if they had concerns about a child’s welfare? When, and in what way, were the child(ren)’s wishes and feelings ascertained and taken account of when making decisions about the provision of children’s services? Was this information recorded? 5 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Did the organisation have in place policies and procedures for safeguarding and promoting the welfare of children and acting on concerns about their welfare? What were the key relevant points/opportunities for assessment and decision making in this case in relation to the child and family? Do assessments and decisions appear to have been reached in an informed and professional way? Did actions accord with assessments and decisions made? Were appropriate services offered/provided, or relevant enquiries made, in the light of assessments? Were there any issues, in communication, information sharing or service delivery, between those with responsibilities for work during normal office hours and others providing out of hours services? Where relevant, were appropriate child protection or care plans in place, and child protection and/or looked after reviewing processes complied with? Was practice sensitive to the racial, cultural, linguistic and religious identity and any issues of disability of the child and family, and were they explored and recorded? Were senior managers or other organisations and professionals involved at points in the case where they should have been? Was the work in this case consistent with each organisation’s and the LSCB’s policy and procedures for safeguarding and promoting the welfare of children, and with wider professional standards? Were there organisational difficulties being experienced within or between agencies? Were these due to a lack of capacity in one or more 6 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review organisations? Was there an adequate number of staff in post? Did any resourcing issues such as vacant posts or staff on sick leave have an impact on the case? Was there sufficient management accountability for decision making? Specific Issues 1. Were the multi-agencies involved in the Young Person’s care fully aware of the risk issues and if so, were they subject to appropriate and robust reviewing arrangements including the role of the IRO? a. Were the thresholds around her behaviour clearly understood within the context of meeting the criteria for alternative care provision and subject to regular review? b. To what degree did the Young Person’s contact with her family impact significantly on her behaviour and the management of this and were the issues clearly understood and reviewed? c. Taking in to account the Young Person’s behaviour, were the staff caring for her appropriately informed of the associated risk issues and able to care for her accordingly? Where appropriate, identify any positive protection factors. d. To what extent were the repeat missing episodes fully considered in line with the developing risk assessment in relation to the Young Person? 2. Is there evidence that staff within individual organisations used any processes or procedures to escalate concerns relating to the Young Person’s behaviour and the day to day management of this? 7 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 3. Was the fact that the Young Person was placed out of Borough and ‘a distance away from home’ detrimental to her care and the oversight of her care provision by the professionals involved in her care planning arrangements? a. Was there evidence of detailed oversight and monitoring within the commissioning arrangements of the placement and the delivery of integrated care planning for the Young Person? b. Is there evidence within the care provided to the Young Person of senior management oversight given the nature of her vulnerabilities by the various agencies including West Mercia Police, CAMHS, Youth Justice and Children’s Social Care? 4. Was the Mental Health Service provision provided to the Young Person fully aware of her needs and is there evidence of a coordinated and joint approach to the delivery of her care including the monitoring of her medication? 5. Taking into account the allegations made by the Young Person against staff, was the LADO appropriately informed and the allegations managed and reviewed in line with the Young Person’s needs? 6. Was Ofsted notified and involved appropriately of the incidents that were taking place and were these reported appropriately in line with the regulations and guidance? 3. Process 3.1 Notification of this serious case review was sent to agencies with a request to undertake a management review of any contact with the Young Person and her family. The agencies were requested to look critically and openly at individual and organisational practice to ascertain whether changes could and should be made and, if so, how this should be achieved. It was requested that 8 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review a senior member of staff who had no involvement with the case, complete the management review. Guidance notes which included a template for the review report were provided to each agency. It was requested that upon completion, each individual management review (IMR) be agreed by that organisation’s senior managers who would be responsible for ensuring that their single agency recommendations are acted upon. If agencies had no contact with the Young Person or her family they were asked to complete a ‘nil’ return. Those agencies which had minimal involvement provided an information report. 3.2 A Serious Case Review Panel was established to actively manage the serious case review process and to obtain all relevant information from agencies and any parallel processes. The panel’s role was to ensure robust analysis of IMRs and that the overview report accurately reflected agency contributions and met the ‘Working Together’ guidance. The panel was set up with an Independent Reviewer/Chair, an Independent Reviewer/Author and representatives from a range of agencies relevant to this case. 3.3 On 12 June 2014 a briefing session was held for IMR authors which was facilitated by the independent reviewer (chair) and the independent reviewer (author). The requirements of up to date ‘Working Together’ guidance was disseminated to all of those present to ensure that IMR authors were aware of the developments in review processes, particularly focusing on establishing why actions were or were not taken by professionals. 3.4 At the first meeting of the Serious Case Review panel, the terms of reference provided by Walsall SCB, were reviewed and agreed. 3.5 Upon receipt of IMRs from agencies, a composite chronology of events was produced. The IMRs and integrated chronology were discussed by the review panel and any discrepancies or need for further information was resolved by either written communication and/or invitation to a SCR Panel meeting. As a result amended final IMRs were received from the agencies as indicated in paragraph 5.1. 9 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 3.6 The SCR Panel met on seven occasions to consider all of the IMRs, information reports and to progress the Overview Report. 3.7 The Overview Report was presented to Walsall SCB on 19 November 2014 and the action was discussed and agreed at a subsequent meeting held on 17 December 2014. 4. Serious Case Review Panel Members 4.1 Independent Reviewer/Chair: Martin Banks The independent reviewer/chair is a qualified social worker with almost 40 years’ experience in child protection as a social worker and manager. He is employed by Cafcass as a service manager and although a member of Walsall Safeguarding Children Board, he has had no previous involvement in the case of the Young Person including the recommendation that a serious case review should be held. Cafcass has not had involvement with the Young Person and her family since family court proceedings in 2001. 4.2 Independent Reviewer/Overview Author: Gill Baker OBE The author of the overview report is a retired police officer and is independent of all the local agencies and professionals involved in the case and of the Walsall SCB. During the last ten years of her thirty year police service she was a Detective Inspector specialising in child protection, domestic violence, sexual offences, sex offender management and vulnerable adult protection. Within her role she was responsible for compiling police individual management reviews and was a member of many serious case review panels across the West Midlands area. She was involved in the development of local, national and international multi-agency projects and initiatives as well as 10 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review policy and procedures for the police service. Her work in this field was recognised when she was awarded an OBE in 2006 for services to the police. Since retirement she has been an independent chair and/or author of several serious case reviews, domestic homicide reviews and MAPPA reviews. 4.3 The members of the panel are senior managers from the key statutory agencies who had no direct contact or management involvement with the case and were not the authors of Individual Management Reviews. 4.4 Panel Members: • Health, Well-being & Citizenship Manager – Walsall Children’s Services, School Improvement • Consultant Child & Adolescent Psychiatrist – Dudley & Walsall Mental Health Trust • Strategic Lead - Targeted Youth Support and Youth Justice Services • Designated Nurse Safeguarding Children – Walsall CCG • Solicitor -Walsall Council • Detective Chief Inspector Protecting Vulnerable People - West Mercia Police • Board Manager – Walsall Safeguarding Children Board • Development Officer - Shropshire Safeguarding Children Board It should be noted that a request was made to Walsall Children’s Social Care to provide a senior manager to be a Panel member. Unfortunately that agency was unable to provide a representative but the WSCB have been assured Walsall Children’s Social Care will be a member agency in the event of any future serious case review panels. 5 Individual Management Reviews 5.1 Agencies were asked to provide an IMR, an information report or a nil return, i.e. no contact with the Young Person or family. As a result IMRs were received from the following agencies: 11 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Residential Care Provider (RCP) - Children’s Homes 5, 6 and 7 Shrewsbury & Telford Hospital NHS Trust Shropshire CCG Shropshire Community Health NHS Trust (CAMHS) Shropshire Doctors Co-operative Limited (Shropdoc) Shropshire Social Care Walsall Healthcare NHS Trust Walsall Children’s Social Care Walsall Youth Justice System/West Mercia Youth Offending Service West Mercia Police West Midlands Police 5.2 Information Reports Information reports rather than IMRs, were obtained from the following agencies due to relatively minimal involvement with the Young Person and her family. Cambridgeshire Police Children’s Home 1 Children’s Home 2 Children’s Home 4 Shropshire Fire & Rescue Service Walsall Commissioning Services (Walsall CCG and Walsall Children’s Services) West Midlands Ambulance Service NHS Foundation Trust An information report was requested from Children’s Home 3 but was not forthcoming despite a second request. However information regarding this placement was contained within the Walsall Social Care IMR and the information report from Cambridgeshire Police. 12 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 5.3 Independent Management Reviews/information Reports Process Agencies reviewed their computer and paper records, details of which are itemised within their respective IMRs. Each of the agencies, conducted interviews of their staff to enhance the quality of their IMRs and to try and get an understanding of not only what happened but why something did or did not happen. Guidance was also provided to IMR authors regarding the interviewing of staff. Contextual information relating to volume of work, staff turnover, training, sickness, organisational change management and supervisory practice is contained within each IMR. 5.4 The Panel robustly scrutinised and quality assured each IMR and information report. When clarification was needed, specific issues in written form were raised with IMR authors, some of whom were invited to and attended a panel meeting for detailed discussion. Amendments and additions were subsequently made to the relevant IMRs. There was a timely response from all of the agencies involved to the issues raised. 5.5 A ‘Reflective Learning’ event facilitated by the independent chair and the independent author was held on 25 September 2014, which was intended for practitioners who directly worked with the Young Person. The purpose was to provide practitioners with an opportunity to maximise and share learning to contribute their perspectives of the case with a view to understanding practice from their viewpoint. Unfortunately, there was little availability of individuals who had worked with the Young Person which was partly due to the length of time since the death of the Young Person. However agency representatives, some of whom were IMR authors or who had had some limited involvement with the Young Person did attend. Nevertheless, this learning event served to increase an understanding of not only what happened but why actions were or were not taken in an effort to identity any systemic failings, as well as giving an insight into the progress made by agencies in changes to practice from lessons learnt to date in respect of this case. 13 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 5.6 A total of 52 single agency recommendations were contained in the IMRs, which were scrutinised by the Panel and are considered appropriate. Agencies were requested to progress their single agency recommendations in a timely manner prior to the publication of the serious case review. A common feature of these recommendations was actions to improve record keeping and communication. These single agency recommendations and action plan are detailed in Appendix B of this review. 6. Ethnicity, Diversity and Cultural Issues 6.1 Commissioning arrangements for IMR reports required agencies to specifically consider whether practice was sensitive to racial, cultural, disability, linguistic and religious identity of the child and family subject of the serious case review, and the impact on service delivery. 6.2 Walsall is a geographically small urban area with a population in 2012 of 271,000, and the proportion of children was 23.4% (63,300). There were 534 Looked After Children, 236 of whom were placed outside of Walsall Borough. There were 245 Looked After Children placed in Walsall by other Local Authorities. By comparison Shropshire is a mostly rural and a sparsely populated large geographical county with a population in 2012 of 291,000, of which 22.4% (68,100) were children. There were 225 Looked After Children, 50 of whom were placed in residential care. There are 65 residential children’s homes in Shropshire, only three of which are run by the Local Authority. Most of the residential placements in Shropshire are from other Local Authority areas. 6.3 The Young Person was of white British ethnicity and no specific issues relating ethnicity, diversity or cultural issues which impacted upon service delivery were identified during this review. However a factor to be borne in mind is the change in environment for the Young Person when she was accommodated in isolated rural settings which contrasted greatly to the urban environment that she had been used to. 14 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 7. Background 7.1 The parents of the Young Person had two other children, aged 3 years and 2 years when the Young Person was born. The parents were aged 19 and 20 years when they had their first child. They had another child three years after the birth of the Young Person and all four of the children were removed from the care of their parents due to neglect when the Young Person was only three years of age. The family at that time lived in Wolverhampton and unfortunately there is no detail available including the conditions in which the children were living at that time. Care proceedings followed and the Young Person and her three siblings were placed with their paternal uncle and aunt to whom residence orders were granted. There was supervised contact with the birth parents. 7.2 The children remained living with the paternal uncle after his marriage broke up but as the Young Person entered adolescence behavioural difficulties were encountered. The Young Person made allegations of physical abuse against her uncle and she went missing on several occasions. She lived with her parents for a short period but also had a strained relationship with them and police were called out on a number of occasions to domestic disputes, allegations of assault against her mother and criminal damage. She was arrested during this period but no further action was taken when complaints were withdrawn. She returned to the care of her uncle but went missing after an argument and refused to return to either her uncle or her parents. At the age of 15 years, the Young Person then became a Looked After Child (LAC) in the care of Walsall Children’s Services. 7.3 The Young Person was described as ‘a stocky young woman, 5’4” tall who could be pleasant, laughed a lot, was a chatty and bubbly character with a good sense of humour. She took a pride in her appearance and would often change the colour and style of her hair’. She received positive reports from her education providers both in regard to attainment and attitude, and was noted to have a strong work ethic. There is evidence that she got on well with some professionals who worked with her and her family. On the other hand she was 15 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review often extremely aggressive and had a lot of anger. She was physically very strong and over one hundred incident reports are recorded where she reportedly displayed extremely verbal and/or physically aggressive behaviour towards professionals, police officers, her family and members of the public. She often had to be restrained and there were incidents when she put herself and others in risky or life threatening situations which included fire setting. 7.4 During the time that the Young Person was a Looked After Child she was arrested on numerous occasions and convicted of offences relating to her aggressive behaviour whilst living in several care homes which were in the main sited in rural areas a distance away from her family. However, she consistently spoke of a desire to be closer to her family and spoke fondly of her siblings. 8. Summary of Chronological Sequence of Events 8.1 Each agency was required to collate a sequence of events of their organisation’s professional involvement with the Young Person and her family, and this information was merged to create an integrated chronology to enhance learning. Primarily this concentrates upon the date from when the Young Person went into care at the age of 15 years, but does contain relevant prior information. Prior to Entering the Care System as a Looked After Child 8.2. On 1 June 1999 the Young Person, together with three siblings, was placed in the care of her paternal uncle due to parental neglect. There is a record of an initial referral to Walsall Children’s Social care in May 2004 which indicates that the case was allocated and closed. No detail of this referral or subsequent action is known. 8.3 On 9 June 2008 the Young Person, aged 12 years, disclosed at school that her uncle hit her on a regular basis. A strategy discussion took place between police and social workers when it was decided that children’s social care would 16 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review conduct a single agency enquiry despite a criminal offence being alleged. No lateral checks were made with any other agency and the Young Person was not spoken to until the following day when she gave a detailed account of physical abuse against her and her siblings. She was reluctant for her uncle to be spoken to and believed that a consequence would be further physical abuse. However the team manager advised the social worker to discuss the referral with the uncle and put a written agreement in place whereby he agreed to stop physically chastising the children. The siblings were not spoken to and the referral was closed without further action, apart from referrals for counselling for the children which relied upon the uncle following these up. 8.4 Four months later on 16 October 2008, the Young Person, now 13 years of age, made another disclosure at school that she had been physically assaulted by her uncle. This was referred to children’s social care but no child protection enquiry was initiated. The Young Person was spoken to over the telephone when she reported that everything was now ‘fine’ and she did not want the uncle spoken to. However four days later she failed to return home from school and was reported as missing by her uncle. She was later found at a friend’s house by the police when she again reported being physically assaulted by her uncle. The police liaised by telephone with children’s social care when it was stated that the matter had been ‘investigated’ and had been unsubstantiated. The Young Person was returned to her uncle’s care but was visited the following day by a social worker. She alleged that she had been assaulted again by her uncle and provided details. Again no child protection enquiry was initiated and instead an initial assessment was completed. There is no evidence that the siblings were seen or spoken to. The outcome was a referral to Spurgeons 1 for the Young Person and the case was transferred to the Safeguarding and Family Support Service (SAFS). This meant that there was no continued social work involvement. It was reported though that the uncle would not allow direct work to be undertaken by Spurgeons at the school and he was always present when the Young Person was seen at home. The case 1 Spurgeons were commissioned by Walsall Children’s Services to work with children subject to Child In Need or Child Protection plans. The focus of their work was rebuilding family relationships with a particular focus on challenge to care. They provided frequent and targeted direct work with children and their families. 17 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review was closed in March 2009 when it was reported that the Young Person was settled and was moving schools as her uncle felt that she was being negatively influenced by peers at school. 8.5 On 31 October 2010, the Young Person, now aged 15 years, was reported as missing from home when her uncle explained this was a result of an incident the previous day when he had confiscated her mobile phone as she had been sending messages of a sexual nature to a male. The Young Person was found at a friend’s home by her uncle and police officers who attended were informed that when she had tried to run off her uncle had grabbed hold of her and dragged her a short distance over grass. She did not have any injuries and refused to return to her uncle’s care. The incident was recorded and an immediate referral made to children’s social care. It was agreed that she could stay at the friends with the uncle’s agreement and a private fostering assessment commenced. The Young Person made a further allegation concerning the uncle which was not pursued and also there was no investigation into the alleged mobile phone messages of a sexual nature. The friend was only willing to care for the Young Person for a short period until a long term placement could be identified. The Young Person then indicated that she wanted to live with her parents with whom she had been staying at weekends. A risk assessment was completed and the Young Person returned to her parents care on 3 December 2010. 8.6 However, the Young Person’s placement with her parents broke down following a number of incidents which took place and on 10 January 2011 she returned to her uncle’s care. Her parents were unable to manage her behaviour and the police were called to six incidents. She was detained for theft from a shop, which was resolved by a community resolution. She assaulted her mother on two occasions and was arrested but no further action was taken after advice from the Crown Prosecution Service (CPS) and a withdrawal of the complaints by her mother. 8.7 On 14 February 2011, the Young Person failed to return home after school and was reported as missing by her uncle. When she was located later that day, 18 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review she refused to stay with her uncle or with her parents and became ‘uncontrollable’. The children’s social care emergency duty team were contacted, and after spending the night at a police station, the Young Person was accommodated at Children’s Home 1 in Walsall. In the Care of Walsall as a Looked After Child First Placement (15.02.2011 – 22.03.2011) Children’s Home 1 Walsall 8.8 The Young Person was placed in an emergency placement at Children’s Home 1 in Walsall in accordance with Section 20 of the Children Act 1989. Staff at the home were immediately concerned about the Young Person’s high level of anxiety and lack of regard for her personal safety. She would: • refuse to sleep in her bedroom, preferring to sleep on the landing as she stated that she had always shared a room with a sibling, • climb trees as this was something she had always done to ‘get away from things’, • climb onto the roof of the children’s unit and when challenged by staff she would climb higher into more dangerous positions. The Young Person also repeated her allegation of long term physical abuse by her uncle adding that he also abused her younger sibling. This allegation was not investigated and the Young Person’s sibling was not seen. 8.9 On 24 February 2011 a Looked After Child (LAC) review took place in respect of the Young Person. Actions from the Review were: • Health – her GP to remain the same, a LAC health assessment to be set up and for her to be registered at a dentist and optician • Social worker to make a referral to CAMHS • A transitional analyst psychotherapist assigned to the Children’s Home 1 to develop a treatment plan together with Unit staff based upon the 19 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Young Person’s needs • Liaison to be made with the Young Person’s school to update them of the current situation • Practical matters, i.e. collection of clothing, provision of school uniform to be undertaken • Contact with family to be planned and arranged with a view to supporting the Young Person At this time a core assessment was undertaken by a children’s services support officer (an unqualified social worker) which concluded that the Young Person should remain a Looked After Child with the rationale being that a return to her family would result in a further breakdown. 8.10 The treatment plan recommended by the psychotherapist was followed by staff but deterioration in the Young Person’s behaviour escalated. This included flooding her room by turning on taps, burning the carpet with electric hair tongs. She would not attend education and would regularly verbally abuse another resident and night staff at Children’s Home 1. The Young Person would also barricade herself in different rooms, breaking into the loft space and the kitchen. On three occasions police officers attended and on one occasion the Young Person was arrested for assault for which she eventually received a reprimand and a referral to the youth offending team. 8.11 On 9 March 2011 a professionals meeting took place which involved the allocated social worker, team manager and the team manager of the Children’s Unit. The purpose of the meeting being to plan how the Young Person could be supported in the placement. The recommendations were clarification of whether Spurgeons could continue work with the Young Person and for CAMHS to begin a mental health assessment (which did not take place as the Young Person was placed out of Borough shortly thereafter). The Young Person did not receive a statutory LAC visit from her social worker until 14 March 2011. 20 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 8.12 The police attended a further seven incidents relating to aggressive behaviour by the Young Person, one of which occurred at her birth family’s home and she was arrested on three occasions and was twice charged with offences of assault and/or criminal damage and it was noted by police officers that she had self-harm marks on her arms. One of the incidents involved the Young Person barricading herself into her bedroom with the use of a wardrobe, a bed and a chest of drawers. After the final incident on 22 March 2011 the placement broke down. Second Placement (22.03.2011 – 06.06.2011) Children’s Home 2 Shropshire 8.13 After the first placement broke down the Young Person was accommodated at an independent residential children’s home (Children’s Home 2) in Shropshire on an emergency basis for a short term 12 week assessment to assess her needs. This organisation included the use of adventurous activities and outdoor pursuits. During this placement 35 incidents were recorded which included assaults on both staff and residents, damage to property and self-harm. One of these incidents on 28 May 2011 involved the Young Person setting fire to a plastic coat in a tent after which she was admitted to hospital for smoke inhalation. She was seen by a consultant child psychiatrist who diagnosed her with a longstanding behavioural disturbance and at risk of developing a personality disorder. She was prescribed medication (0.25 milligrams Risperidone twice a day as required) to improve her impulse control and mood regulation. During her time in hospital she repeatedly tried to abscond and had also managed to get onto a ledge and threatened to jump. Also during her placement police were called on three occasions and she was arrested and charged once, resulting in a 12 month referral order after being convicted of common assault and assault police. The Young Person’s behaviour at this placement reflected similar behaviour displayed at the previous placement, i.e. placing herself at risk, assaulting staff and attempting self-harm. However she also built up some good relationships with some members of staff, had a good sense of humour and was able to interact well with some other young people. She also had regular contact with her uncle and had several phone calls, home visits and visits from her uncle and siblings. During this placement a second 21 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review LAC review took place and it is recorded that five statutory LAC visits took place but the Young Person was not actually seen on three occasions and she was seen alone only once. Two visits did not take place due to her behaviour and two as she was out on an activity. Third Placement (06.06.2011 – 20.07.2011) Children’s Home 3 Cambridgeshire 8.14 The Young Person was moved to a third placement in Children’s Home 3 in Cambridgeshire on 6 June 2011 after the assessment period at Children’s Home 2 came to an end. There were seven incidents reported which mirrored previous behaviour, i.e. climbing trees, assaults on staff, damage to property and self-harming. Staff at the home quickly felt that they could not manage the Young Person’s behaviour and 28 days’ notice was given. The Young Person was admitted to hospital on 10 June 2011 after an overdose of Resperidone. She was seen by a child psychiatrist and psychotherapist when it was concluded that she showed no sign of mental illness or suicidal ideation. She was discharged from the CAMHS service as it was felt that her needs could be better served by the Youth Offender Service(YOS) and a referral was made by the Young Person’s social worker to the YOS psychologist in Peterborough as a matter of urgency but there is no trace that this was received or actioned. The Young Person was arrested on three occasions and on 26 June 2011 she made an allegation of sexually inappropriate behaviour towards her by a member of staff. She subsequently withdrew her allegations. During this placement the Young Person received four statutory LAC visits and was seen alone during three of them. Fourth Placement (20.07.11 – 05.09.2011) Children’s Home 4 Birmingham 8.15 The Young Person was placed at Children’s Home 4 in Birmingham on 20 July 2011 and a Behaviour Management plan and a risk assessment were compiled and agreed in consultation with the Young Person’s social worker. Information was exchanged regarding her history and behaviour during previous placements. The Behaviour Management plan focussed on safety and included 22 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review strategies to be used by staff to ensure consistency of practice. At first the Young Person appeared to be a very friendly individual who was helpful around the home and it was believed that she would be able to engage with the other occupants of the home. However, during this placement 22 incident reports were received by Walsall Social Care of a similar nature to those reported previously. The Young Person was arrested on two occasions and incidents were occurring on almost a daily basis. These included assaults on staff, setting off fire alarms, setting light to paper and pushing through a letter box, attempting to set fire to a tea towel, causing damage and going missing. Within five days of the commencement of this placement staff were reporting that her behaviour was difficult to manage and they were unsure about being able to continue with the placement. The most challenging behaviour occurred at bed times when the Young Person would be reluctant to go to bed and often left the home late at night returning in the early hours. Indeed at first she repeated a refusal to sleep in her bedroom preferring to sleep on the landing. During this placement she did not attend school but she benefitted from one to one tuition with a personal tutor (a qualified teacher) who was employed by the home. It was recorded that the Young Person was able to make a positive contribution to the home and was able to engage in activities, became involved in group meeting to plan activities, helped with weekly shopping and showed an interest in her personal care. 8.16 A second risk assessment was conducted on 2 August 2011 which concluded that the Young Person posed a high risk of being physically and verbally abusive to staff and peers and also of self-harm and smoking. Legal advice was sought to determine whether the threshold was met for a Secure Order under Section 25 of the Children Act 1989 in respect of the Young Person. It is recorded that the threshold was met for a secure placement under welfare grounds. An application was not made and she remained at this placement for a further six weeks. 8.17 During this placement three statutory LAC visits took place and it was noted on one visit that the Young Person was allowed to stay up late and sleep late in the morning. This was one of the strategies taken by staff to avoid escalation of 23 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review further incidents. A professionals meeting took place to discuss the number of missing episodes taking place by the Young Person and other residents and as a result extra funding was provided to provide additional staff. There was no detail of the discussion recorded and it is not known whether there was any investigation as to reasons why or where she was going missing to, or detail of any contingency planning. A third LAC review was undertaken when it was agreed that the Young Person should remain at the home for assessments and options explored for her education, registration with a GP, arrangements for a health assessment, her attendance at court, the involvement of the Youth Offending Team in completing a pre-sentence report, liaison with CAMHS, and contact with the birth family. 8.18 On 17 August 2011 the Young Person reported that she was pregnant but there is no record of a pregnancy test having been taken or any discussion around sexual health and keeping safe. 8.19 Due to the amount of incidents recorded an unannounced visit was made to the Home by representatives of COG (Children with Complex needs Operational Group) Funding Panel who commissioned the placement. As a result of the visit and concerns raised the home gave 28 days’ notice on 18 August 2011 to end the placement. Five further incidents occurred which involved police being called to the home and on 3 September 2011 the Young Person was arrested and charged with assault upon two police officers and she remained in custody until a court appearance on 5 September 2011 when the placement ended. Fifth Placement (05.09.2011 – 16.12.2012) (RCP) • 05.09.2011 - 11.09.2011 Crisis Response Assessment Centre • 12.09.2011 - 06.11.2011 Children’s Home 5 • 07.11.2011 - 14.10.2012 Children’s Home 6 • 15.10.2012 – 16.12.2012 Children’s Home 7 8.20 The Young Person was then placed in the care of RCP, an independent provider of therapeutic residential care for young people between the ages of 24 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 10 to 18 years. The Young Person was now two days short of her sixteenth birthday. She spent one week in a transitional placement in a crisis response centre for assessment. During this week she took two pregnancy tests and she was not pregnant. There is no record of whether any discussion regarding sexual health or sexual exploitation took place between the Young Person and her carers. She was then moved to Children’s Home 5 where there was only one other child resident. However her pattern of behaviour continued and during her time at this home there were 14 incidents reported. Police were contacted a total of 16 times either by the home, by the Young Person herself, by the ambulance service, by hospital staff or by others in respect of the Young Person. During this placement she did not get along with the other resident. She was arrested on two occasions for breach of the peace. Incidents included barricading herself in her room, smashing a mirror and holding a shard of glass to her throat threatening to self-harm. She also made an allegation of sexual assault against a member of staff. She was taken to hospital after it was suspected she had taken an overdose of Paracetamol but later absconded from the hospital and had to be returned to the home by police. She also assaulted members of staff and damaged property. 8.21 On 16 September 2011 a meeting took place by Walsall Social Workers with the Young Person as there was a change of her social worker. At that time it was recorded that the transition to the house had ‘gone smoothly’ but the first incident occurred the following day. A statutory LAC visit did not take place until 10 October 2011 five weeks after she had begun the placement. 8.22 In respect of the allegation of sexual assault a Child Protection Enquiry was initiated but after strategy discussion between the police and social care no further action was taken. The Shropshire Local Authority Designated Officer (LADO) was contacted and a strategy meeting did take place and the decision to take no further action was reiterated. 8.23 On 7 November 2011 the Young Person was moved to Children’s Home 6 which was run by RCP. This was a solo placement as it was agreed between the providers and the commissioners that it was necessary due to her high level 25 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review of violent behaviour which was reportedly exacerbated by the other resident in the previous Home. The initial staffing of one to one was increased to two to one. During this placement there were 32 incidents reported to Walsall Children’s Social Care, over 40 calls to the police and the Young Person’s behaviour became more difficult. She displayed more defiance and her aggression became more extreme. There were more attempts at self-harming by overdoses, jumping out of cars or trying to stop cars whilst in motion. 8.24 During this placement six weekly statutory visits took place and the Young Person was seen alone and with carers. Three LAC Reviews took place and it was noted in February 2012 that an ‘in house’ psychiatric assessment had diagnosed that the Young Person had ADHD combined with Conduct disorder. There had been referrals to CAMHS discussed at each LAC meeting and when the Young Person was in hospital, but she had not been assessed as there was an issue over funding and also a refusal by her to attend an appointment given. Funding was eventually approved on 26 April 2012. The Young Person was to miss two appointments for a CAMHS mental health assessment but was actually seen on 27 July 2012 by a consultant child psychiatrist who reviewed the diagnosis of ADHD. During this consultation the Young Person repeated her allegations of physical abuse by her uncle and that no-one believed her. She also showed no remorse for her offending and felt her actions were fully justified. She went on to say that she did not think things through before acting and did sometimes regret not doing so. The consultant explained what the treatment entailed stating that it would need to be carefully planned. The Young Person expressed a concern that given medication she may get angry and take it all at once. The Consultant psychiatrist agreed to send her information about ADHD with copies to her social worker and the home Manager. 8.25 On 5 August 2012 the Young Person was taken into police protection as the children’s home staff were unable to control her but she was later returned to the home. A strategy discussion was to take place the next day to discuss more suitable accommodation for her. It appears that what actually took place was a LAC Review but the record of that review is not available. A report was 26 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review available from the care home which indicated that the Young Person had successfully completed a BTec qualification in food technology but she did not want to remain at the home and wanted to live nearer to her family. 8.26 On 13 September 2012 28 days’ notice was given by the Commissioners to RCP to terminate the Young Person’s placement as more suitable accommodation was needed for her. However no alternative provider could be found and she remained in the care of RCP. 8.27 On 21 September 2012 the Young Person and the children’s home manager met with the consultant child psychiatrist and the Young Person agreed to start medication and was prescribed 18mg of Atomoxetine daily which was to be reviewed on 23 October 2012 but that appointment was subsequently cancelled. 8.28 On 15 October 2012 the Young Person moved to Children’s Home 7 home run by RCP. It was planned that the Young Person would move into a multibedded unit as a preparation for independence as she was now 17 years of age. This home had recently been redecorated due to a fire caused by a previous resident and although there was accommodation for two children, the Young Person was the only resident. The staffing ratio was one to one but from the onset her behaviour proved difficult and the staffing ratio had to be increased to two to one. Four incident reports were received by Walsall Social Care, the police received nine calls from staff reporting the Young Person missing or reporting assaults on staff or from the Young Person asking to be returned to the home or reporting being left alone in the home. On 17 October 2012 she had visited her sibling and refused to return to the home but after being told by her parents that she could not live with them as they could not cope with her behaviour, she returned to the home the following day. At this point the social worker was told by the children’s home manager that the Young Person had been prescribed medication but there was no improvement in her behaviour. It appears this was the first time that the social worker was aware of medication being prescribed to the Young Person. 27 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 8.29 On 20 October 2012 the Young Person punched a care worker in the face after being told that she could not have any Paracetamol as there was none in the medicine cabinet. She was arrested and later released on police bail pending advice from the Crown Prosecution Service. The following day she ran away from the home but later asked police to be taken back. On 22 October 2012 a LAC statutory visit took place by the social worker but the Young Person would not see the social worker alone stating that she would have her say at the LAC review which was planned on 12 November 2012. The social worker was shown around the home but the Young Person would not allow entry into her room. She was told that her uncle had agreed that she could see her younger sibling every two months. In the early hours of the next day an incident occurred whereby a new member of staff at the home was the sole carer of the Young Person who forced her way into the office and was verbally abusive. The member of staff fled from the home after being afraid of being physically assaulted. The Young Person then telephoned the police stating that she was alone in the home and was afraid. The police attended and insisted on another worker being present in the home. The Young Person apologised for her behaviour and stated that she was at fault. From this point on the staffing ratio was two to one. 8.30 There was a missed appointment with her YOS officer for which there was no explanation, a missed appointment with CAMHS which probably was due to an incident which had occurred on that day. There were telephone consultations with an out of hours GP service regarding pain to her wrist which may have been due her being restrained during an incident. She was also registered with a GP whom she saw, her medication (Atomoxetine) was noted, as well as the fact that she had another appointment with CAMHS on 11 December 2012. The Young Person did attend two appointments with the YOS team which involved a decision making session and a reparation session of 6 hours in length, during which she was able to demonstrate that she was able to engage and follow instruction without incidences of aggressive behaviour. On 8 November 2012 a meeting in respect of the Young Person was held by the Walsall YJS (Youth Justice Service) Risk and Vulnerability panel with the aim of enabling additional management oversight for cases deemed at high risk of 28 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review serious harm and/or vulnerability. Concerns were raised in relation to the electronic file not reflecting up to date information about her. Also she had not been seen by the Walsall YJS supervising officer. Contact made the same day with West Mercia YOS provided information about the extent of change experienced by the Young Person with a new placement, changes to care staff and a change of YOS case manager. Information in respect of the assaults against staff was also exchanged. A review meeting was scheduled to take place on 22 November 2012 but records do not indicate that this took place. The Young person attended a further reparation session when it was recorded that she showed a good work ethic and was willing to try new things. 8.31 On 12 November 2012, a seventh LAC Review was held when it was recorded that the purpose of the meeting was to prepare the Young Person with independent living skills. It was agreed that she would remain at the placement, staffing levels were to be discussed, she was to continue to engage in anger management/therapy and weekly updates were required from the therapist. Her medication was to be reviewed, further work to be undertaken regarding her independence skills, she was to continue in education and be given opportunity for day release and work experience. The unit was to support and encourage contact with her family. Updates were to be made to the funding panel and the pathway plan in place. She was to attend court and cooperate with any sentence and rehabilitation order. A review of risk was undertaken by the West Mercia YOS officer which deemed that the Young Person was at high risk of re-offending, medium level of vulnerability and a high risk of causing serious harm to others. At the same time a mental health screening form (SQIFA) 2 was undertaken with the Young Person who was asked a series of questions with a view to determining whether a referral to a mental health specialist was required. Her score indicated that she required a full assessment but a referral was not needed as she was already receiving a CAMHS service. There was no YOS officer in attendance at the LAC review meeting and there is 2 SQIFA - A questionnaire used as part of the Asset Assessment where mental health is being assessed. The ASSET Assessment is a common, structured, assessment tool used across the youth justice system in England and Wales. The purpose of an ASSET Assessment is for making a comprehensive and holistic assessment; identifying the needs of a young person; identifying factors contributing to offending behaviour; identifying risk and vulnerability and identifying positive factors as well as problems 29 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review no evidence that YOS were aware it was to take place. 8.32 There was a period of six days of relative calm during which risk assessments were conducted by the children’s home in respect of the Young Person’s behaviour and strategies put in place in respect of fire setting, aggressive behaviour, self-harm and absenting. She appeared at court when she pleaded guilty to two offences of assault against care workers and was granted bail with a condition that she cooperate with YOS in the preparation of a pre-sentence report. She went missing again on 19 November 2012 after an incident where damage was caused to a staff car. She contacted the police herself and returned to the home in the early hours of the next day. On the same day the LAC named nurse attended the care home with a view to conducting a health assessment but the Young Person refused to be seen and locked herself in the bathroom. Also on that day she was arrested by police for the criminal damage and assault on care staff. She was charged and kept in custody to appear before the court from where she was bailed back to the home. Information was exchanged between the police, care home, social worker and YOS worker. It was noted that the Young Person was struggling with changes in staff at the care home but failed to recognise that her behaviour had resulted in five members of the care home team going off on sick leave. 8.33 She attended a further reparation session with YOS. It is noted by the Walsall social worker that the Young Person faced four charges of assault by kicking and biting and two charges of criminal damage. It was likely that if she committed any further offences before the trial date that it was likely that she would be kept in custody and a psychiatric report had been requested by the prosecution. At this time the LAC named nurse also raised concerns about the Young Person’s refusal to go to the dentist, her psychological health, emotional vulnerability and lack of uncertainty about the future. 8.34 She attended a further YOS appointment which was described as positive but she expressed anger about her carers. She also related an incident which occurred at the weekend whereby she was ‘targeted’ and became involved in a fight with a girl in a nearby town. The police attended that incident but no 30 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review further action was taken. 8.35 On 1 December 2012 the Young Person was assigned to different YJS worker in Walsall but there is no evidence that West Mercia YOS were informed of this change. A further appointment with her West Mercia YOS worker indicated that the Young Person had a good week but she was still ‘bitter’ towards her carers who were now all male due to the fact that female staff were unwilling to work with her. On 7 December 2012 the Walsall social worker submitted a report to the effect that the Young Person had remained in her current placement as no alternative could be found. She now refused to meet with her social worker for statutory meeting. However she was engaging well with education and making good progress in that respect. Weekly updates had not been received from the care home but would be forthcoming from this point on. 8.36 On 10 December 2012 the Young Person was reported as missing by care staff as she had walked away during an activity in Birmingham. It was felt that she may be at danger of sexual exploitation. However she was contacted by telephone and stated that she was staying with her sibling. There was a report from her family that she was with them, she was drunk but she could stay there. She was due to attend a CAMHS appointment the next day which was cancelled but it is not recorded by whom. 8.37 Members of staff at the home showed a reluctance to pursue any complaint against the Young Person. However on 12 December 2012 she bit a member of staff three times and punched another in the face. Police were called and she was arrested but was given police bail with conditions that she did not directly or indirectly contact the staff members she had assaulted. She also made allegations of assault against her by a carer but did not wish to pursue this. Information was exchanged between Walsall Social Care, West Mercia YOS and Shropshire Social Care. 8.38 On 16 December 2012 the Young Person died in a fire at the Care Home. It transpired that following a dispute with carers about continued use of the internet, that she had barricaded herself in her bedroom and had then set fire to 31 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review a mattress which had been placed against the door. She had previously posted a message on a social networking site about setting fire to her room. 9 Family Engagement 9.1 At the commencement of this review the Young Person’s family were informed about the serious case review by letter and by a personal visit by the independent chair of this review and the WSCB Board Manager. Her parents and her uncle were seen and the purpose and process of the review was explained to them. However they were, perhaps understandably, focused upon the circumstances and cause of the Young Person’s death and initially seemed to lack an understanding of the purpose of the serious case review. It was subsequently reiterated to them by the WSCB Board Manager during a telephone conversation that the cause of death was a matter for the Coroner but the focus of the SCR was around the involvement of agencies prior to the Young Person’s death. A second visit took place on 5 August 2014 when the parents and the uncle were seen by the independent overview author and the WSCB Board Manager. They were a little hesitant and uncertain about contributing to the review which of course meant them having to relive the loss of the Young Person. Nevertheless they did express a wish to contribute to the review process. 9.2 The family described the Young Person as caring and adventurous enjoying outdoor activities, swimming and tenpin bowling. The birth parents spoke fondly of the Young Person who was physically very strong and who did get involved in fights at school. When younger she was respectful and always apologised if she was in the wrong. Her uncle said that he believed in the children being in a routine as he had looked after her and her three siblings from such a young age, had children of his own and had to cope alone when his marriage broke up. He began to experience difficulties managing the Young Person’s behaviour when she entered adolescence and that is when she made the allegations of physical abuse against him. She had contact with her parents but they too had problems in coping with her, she argued with them, assaulted her mother and the police had to be called to their home on a number of occasions. The family were of the 32 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review opinion that the Young Person had ‘got away’ with her offending and as a result was not made to understand the serious implications of her behaviour and actions. They believed that she should have been placed in secure accommodation for her own safety. 10. ANALYSIS OF AGENCIES INVOLVEMENT 10.1 The Young Person and her family had a great deal of involvement with agencies which intensified after she made allegations of physical abuse by her uncle in whose care she had been since a young child. She repeatedly made these allegations to a number of different professionals and child protection procedures were initiated but there was never a thorough investigation and initially a reliance on a written working agreement. She also alleged that her siblings had been physically abused by her uncle but they were never spoken to. At the age of 15 years the Young Person became a Looked After Child. During the 22 months that she was in the care of Walsall Local Authority, she was accommodated in seven different children’s homes. She expressed a desire to be near to her family home but five of those homes were located a distance away in rural areas. Walsall Children’s Social Care were notified of 112 incidents concerning disruptive behaviour. The police were called on 130 occasions concerning incidents involving the Young Person and she was arrested on 31 occasions. In respect of her offending, within an eighteen month period she was sentenced on six different occasions for a total of twenty eight offences. She repeatedly went missing, assaulted care home staff members, placed herself in vulnerable and dangerous situations and took overdoses of medication or stated that she had with the aim of being taken to hospital from where she could abscond. 10.2 There was information exchange between agencies and professionals within and outside of Walsall Borough and statutory LAC Review meetings and visits took place. However some visits were late and some actions from meetings were repeated and not followed through. There was a considerable delay in the provision of a CAMHS assessment, and a failure to provide sufficient general health assessment and care, albeit 33 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review this was due in part to a refusal by the Young Person to co-operate. There were communication difficulties encountered across county boundaries, confusion in respect of commissioning and provision of funding which resulted in services not being available. There was a lack of a holistic assessment with little evidence of exploration into the causes of the Young Person’s behaviour, of listening to her, and of the escalation of the frequency and extent of her increased aggression, violence and absconding. It was evident that she had complex needs which required a proactive multi agency coordinated response which was lacking. KEY ISSUES • Allegations of Abuse 10.3 Prior to becoming a Looked After Child, the Young Person made four allegations of physical abuse by her uncle against her and her siblings. On the first occasion a strategy discussion took place between police and social care when it was agreed that a single agency enquiry would be conducted by social care but no lateral checks were made with other agencies and although the Young Person gave a detailed account of her allegations, there is no recorded evidence that her siblings were seen or spoken to on their own. The matter was discussed with the uncle and reliance was placed upon a written agreement with him to stop physically chastising the children and no further action was taken apart from referrals for counselling for the children which the uncle was left to follow up. A failure to thoroughly investigate these allegations resulted in the Young Person’s feelings of never being believed which she claimed when she repeated her allegations to various professionals. This belief could have been a factor contributing to her anger and extreme behaviour. Potentially the Young Person’s siblings may have been left at risk of significant harm. The failure to speak with the siblings is the subject of a recommendation made by Walsall children’s social care. It is understood that written ‘working’ agreements are still utilised in Walsall as part of care planning but it is of concern that in this case such an agreement, which has no legal standing, seemed to replace a thorough investigation into 34 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review allegations repeatedly made. 10.4 The Young Person went on to make allegations against staff at care homes of sexually inappropriate behaviour and of physical assault. Although she withdrew complaints there was no robust enquiry into any of the incidents, with no POT (Position of Trust) meetings being held. This is usual practice when an allegation has been made against a person who works with children. It should be noted that there is no known evidence which would have substantiated any of the allegations. However, these incidents served to reinforce the view that the Young Person made false allegations and her credibility was undermined. • Commissioning Arrangements 10.5 The circumstances of children placed in residential care are presented to a funding panel. Initially when a child or young person was placed in a residential unit, the funding panel was referred to as Children with Complex Needs Operational Group Panel (COG) and this was later replaced by External Placements Panel (EPP). The Panels meet to decide on coordinated actions by partner agencies to meet the needs of children with complex needs. The partners are the local authority, education and health. Funding for placements is agreed by either two or all three of the partners involved. The first two placements for the Young Person were sourced by a placements officer and decisions with regard to establishing whether residential placements were single agency or jointly funded were not defined. There is evidence of systemic delay and lack of challenge of partners in reaching a decision and obtaining contributory funding was problematic and hence tripartite funding was not agreed until January 2012. 10.6 A lack of holistic assessment provided to the panel from Walsall Children’s Social Care resulted in the panel members being unable to fully appraise the Young Person’s needs and plan interventions and resources needed. Hence the decisions appeared to be reactive rather than proactive. There was a lack 35 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review of governance of compliance with the recommendations or actions made with considerable delay in the completion of tasks. Agreement for funding of the CAMHS service is an example of unacceptable delay. The focus of the panels appeared to be on costs rather than upon quality assurance of planning to seek the best outcomes for her. 10.7 As a result of a request by the SCR Panel, two reviews were made on commissioning arrangements, one by Walsall children’s social care and the other by Walsall CCG. These reviews have resulted in five recommendations which relate to a review of terms of reference, emergency placements, recording, requests for CAMHS assessment, escalation processes and quality assurance framework. These recommendations are detailed within Appendix A of this review. • Health and General Well Being 10.8 The Young Person took a pride in her appearance but was reluctant to attend appointments relating to her health, the majority of which were cancelled. At the first LAC review when she entered care her health was a priority and it was actioned that she undergo a LAC health assessment and be registered at a dentist and optician. Obviously difficulties arose in a continuity of health services due to her moving accommodation seven times during her time in care. However a LAC health assessment was never achieved which was in the main due to her refusal to attend. It has been identified by health that when there is a refusal to undergo a health assessment that the LAC nurse should visit the young person in placement and this is the subject of a single agency recommendation. It was also identified at an early stage that a treatment plan be developed in respect of the Young Person’s mental health and whilst she did benefit from some input from psychotherapists and counselling, it was only at crisis points, i.e. admission to hospital, that any input from CAMHS was provided. A referral to CAMHS was made in the first LAC review and was repeated in subsequent reviews and was discussed in the funding panels. It is unclear at what point a diagnosis of ADHD was made and appears to have been identified by an in-house psychiatrist when the 36 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Young Person was resident and in the care of RCP. The delay in the provision of CAMHS was due to an unacceptable delay in funding and a final diagnosis which resulted in the provision of the appropriate therapeutic intervention came 20 months after she became a Looked After Child. It is understood that CAMHS will now provide a service prior to the agreement of funding. 10.9 There is also some confusion around medication that was prescribed for the Young Person. It is known that in May 2011 she was prescribed Risperidone by a consultant child psychiatrist after she was admitted to hospital suffering from smoke inhalation. At that time she was diagnosed with longstanding behavioural disturbance and was at risk of developing a personality disorder. However after her admission to hospital a month later when she had taken an overdose of the prescribed medication it was concluded that she showed no sign of mental illness and she was discharged at that point from CAMHS as it was felt that her needs could be better served by the Youth Offending Service. She went on to take or allegedly take overdoses of Paracetamol which had been prescribed by GPs. Whilst a pattern emerged of these overdoses being in order to be taken to hospital so that it would give her an opportunity to abscond, it is not evident that the danger of her actions were fully recognised by professionals and there is little evidence that her medication was sufficiently monitored. Indeed she herself highlighted that she was hesitant about the treatment plan for ADHD which was discussed with the consultant child psychiatrist in July 2012 as she may be tempted, when angry, to take the medication (18mg of Atomoxetine daily) in one go. The Young Person agreed to the treatment plan and the medication was prescribed in September 2012 and was known to the children’s home manager who was present during the consultations with the consultant child psychiatrist. However, the Young Person was to move children’s homes once more and it appears that her medication was not monitored, despite a children’s home manager reporting to the Young Person’s social worker that there had been no improvement in her behaviour after being prescribed the medication. It is possible that she had not taken the medication and her appointment with CAMHS on 23 October 2012 was cancelled. Enquiries made with the children’s home 37 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review providers after the death of the Young Person indicated that they had no record of any medication prescribed to her which does indeed indicate that her medication had not been monitored. 10.10 In addition to her physical and mental health, there is little evidence of professionals from any agency being aware of or acknowledging important events in her life, such as birthdays, Christmas, achievements in her education. Issues that within a family setting would usually promote some form of celebration. Some attention to these issues may have boosted her self-esteem and promoted her well-being. The Young Person spoke of a boyfriend which related to incidents in July 2012 but there is no further information recorded. There is also no mention of any friendship groups that she belonged to which may in part be due to limited opportunities to socialise with other young people due to the isolation of her placements. However it should be noted that on one hand she demonstrated positive behaviour whilst working with other young people in YOS reparation sessions but would also adopt an anti-social persona with peers on other occasions. 10.11 The Young Person indicated to care staff that she may be pregnant which she was found not to be but there is no record of any discussion about sexual health, safety and the risk of her being vulnerable to sexual exploitation was not identified. • Reviews, Planning and Risk Assessment 10.12 Whilst statutory LAC reviews and visits took place, agencies did not coordinate sufficiently and there was no holistic approach taken in relation to identifying the Young Person’s needs. Professionals meetings took place on four occasions and at the point where she was approaching independent living it was decided that these would be held every six weeks but this did not occur. The lack of Professionals meetings was a missed opportunity to consider a coordinated response to her escalating behaviour and it is apparent that the approach taken by Walsall children’s social care was 38 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review reactive rather than proactive. There seemed to be scant probing of why the Young Person was acting in such an aggressive and violent manner and lack of identification of triggers and communication of patterns of behaviour to carers. For example her tendency to barricade herself into rooms started very early in her placements. There was a lack of robust risk assessment. The Young Person went missing on numerous occasions but there was a lack of focus on her absconding and adherence to joint protocols in place in respect of missing children and young people, particularly in respect of prevention strategies. Unusually for a young person already in the care of a local authority, the police resorted to placing the Young Person in police protection after several incidents when she was found to be uncontrollable by care staff. The use of police protection should result in a Section 47 Children Act 1989 enquiry following a strategy meeting but in this instance these procedures were not followed. Instead a planned LAC review took place and in the absence of a record of that particular meeting it is not known why a Section 47 enquiry was not pursued. This was a missed opportunity to achieve a coordinated multi agency care plan for the Young Person. 10.13 In two of the placements there was very early identification by staff that they felt unable to manage the Young Person’s behaviour and legal advice was sought in respect of secure accommodation. In August 2011 it was deemed that the threshold was met and whilst secure accommodation for a Looked After Child is indeed a last resort, this option although mentioned did not seem to be fully considered when there was an escalation of the frequency of absconding and an increase in the level of aggression. Indeed the Young Person also faced the possibility of a custodial sentence in view of the high level of offending. There was an understandable reluctance by carers to pursue complaints of assault against her but it was obvious that she posed a high risk of harm to others and to herself. Her behaviour could not be controlled and she was indeed unmanageable in her placements. The ultimate option of secure accommodation where her needs could be 39 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review comprehensively assessed in a safe environment should have been regularly reviewed. 10.14 When placements for the Young Person crossed county boundaries information was not fully exchanged despite processes and procedures being in place. When she moved to Cambridgeshire, information was transferred from Shropshire CAMHS and from the West Mercia YOS but there is little recording of any action taken by those agencies, albeit the Young Person was only there for a relatively short period. Indeed there were no assessments or interventions conducted by YOS whilst she was resident in Cambridgeshire or in Birmingham which resulted in missed opportunities for early planning. There were delays in case transfer information which resulted in the Young Person actually not receiving YOS interventions for a period of six months. • Placements 10.15 The Young Person consistently expressed a desire to be placed nearer to her family home and it was apparent that she valued time spent with her family. She frequently absconded from her placements to return to her family who found difficulty in managing her behaviour and who were therefore unable to accommodate her. As previously stated the response to the challenges presented by the Young Person were reactive rather than proactive and as a result she faced constant change and isolation in the placements, five out of seven being in remote rural areas which was a strong contrast to the urban environment she was used to. The lack of coordinated holistic robust multi agency planning in respect of the Young Person indicated an almost ‘out of sight, out of mind’ culture. This issue has been highlighted nationally when concern was raised about the high number of children being placed many miles away from their home community. As a result Ofsted conducted a thematic inspection (From a Distance – looked after children living away from their home area – April 2014). A number of the issues identified in that thematic inspection mirror the findings of this SCR. There were several 40 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review recommendations for Local Authorities (LAs) which include; discharging responsibilities as corporate parents; ensuring appropriate health and education services are immediately available; provision to carers of timely and comprehensive information about LAC children and young people; establishing full agreement for the funding of health provision. A recommendation is included for LSCB’s in relation to monitoring the performance of their local authority and partners in meeting the needs of all looked after children living in and out of the local authority area. It is understood that this recommendation has not to date been adopted by Walsall SCB, and therefore a recommendation has been made. 11 Good Practice 11.1 There are no items of good practice over and above the expected level of service identified in this review. 12 Changes/Improvements to Service Delivery actioned prior to this SCR • Fire Service 12.1 There had been a previous fire at the care home where the Young Person died. In August 2012, a resident had set fire to linen and clothes in a bedroom and on that occasion no-one was injured. It is probable that the Young Person knew of this as the home had been refurbished and she knew the resident responsible. In September 2012 a post fire audit inspection was carried out which identified minor alterations to the premises which involved safe storage of materials and fire protection adaptations, i.e. internal timber doors were replaced with fire doors and fire alarms were fitted. Following the fire in which the Young Person died the fire service brought forward all of its fire audit inspections for children’s homes in Shropshire and each home was reviewed over a period of six months. Prior to 2006 inspections were conducted on a yearly basis but that had been changed to every five years as a result of the introduction of revised legislation. Standards have been raised and involves sign-posting for fire setting 41 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review behaviours and enquiries are made about risk profiles of young people. When a resident is known to present a risk of fire setting additional safety measures, e.g. installation of a sprinkler system, could be utilised. • Youth Offending Service/Youth Justice Service 12.2 After the death of the Young Person Walsall Youth Justice Service was required to complete a Critical Learning Review (CLR) as part of the Youth Justice Board’s (YJB) Serious Incident reporting procedures. As a result both Walsall YJS and West Mercia YOS reissued staff guidance on assessing and managing issues in relation to child safeguarding and vulnerability management, Training audits to ensure that all staff attend mandatory LSCB training and changes to quality assurance processes and staff supervision were actioned to ensure that policy was embedded. 13 Single Agency Recommendations 13.1 All agencies that had had significant involvement with the Young Person were required to compile an individual management review to provide an independent, open and critical analysis on individual and organisational practice, which resulted in a total of 52 recommendations focused on improving practice. These recommendations and action plan are detailed in Appendix B of this review. 13.2 Walsall SCB and Shropshire SCB require that organisations provide direct feedback of the key learning to the professionals involved in the case and where individual practice, supervision or management has fallen below the expected standards, appropriate action is taken by the organisation concerned. 42 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 14 Lessons Learnt • There was a failure to take a holistic, proactive co-ordinated multi agency approach to meet the complex needs of this Young Person • There was no robust challenge or review of care plans • Communication and information sharing amongst professionals and across county boundaries need to be improved to ensure that carers in placements are fully aware of risk factors and triggers to incidents • Actions taken were generally reactive rather than proactive • More risk assessments should have been conducted into the level of risk of harm posed to the Young Person and to others • There was an unacceptable delay in provision and funding of services in respect of the Young Person’s mental health needs. • Medication prescribed was not sufficiently monitored to reduce the risk of overdose and to assess effectiveness • There must be more enquiry and probing into the root cause of a Young Person’s aggression, risk taking, disruptive behaviour and absconding • The option of secure accommodation must be reviewed and reconsidered when there is an escalation of intensity and frequency of violent, aggressive and absconding behaviour 15 Conclusion 15.1 In view of the aggressive, violent, fire setting and risk taking behaviour which was consistently displayed by the Young Person it was predictable that she would eventually cause serious harm to herself and/or to others. Immense difficulties were encountered by all professionals working with or caring for the Young Person. The failure to adequately address the escalation of her unmanageable behaviour may in part be due to issues of gender, carers being afraid of physical assault or of allegations being made against them. However, it is concluded that a more co-ordinated robust holistic multi-agency approach, an earlier and full mental health assessment and formulation, monitoring and reviewing of treatment for ADHD, plus utilising the option of 43 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review secure accommodation would have provided an opportunity to fully assess and meet her needs in a safe environment which may have contributed to potentially preventing her death. 44 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review APPENDIX A WSCB Serious Case Review – W4 LSCB Recommendations 1) The use of written working agreements relating to the safety and wellbeing of children in Walsall be analysed and steps taken to ensure clarity of purpose. When used such agreements must not replace a thorough investigation when allegations of abuse are received and should form part of an overall care plan. Such agreements must be regularly reviewed and monitored. 2) When commissioning placements for Looked After Children it must be specified that any medication prescribed to individual children/young people must be documented and monitored to ensure their safety. There needs to be a clear handover from one set of staff to another especially when there are frequent moves and changeover of staff. The Social Worker and LAC Nurse need to have a copy of all the letters so that all information relating to the child/Young Person’s health can be held in one place. 3) The option of Secure Accommodation for a Young Person must be regularly and robustly considered when the frequency and intensity of violent, aggressive behaviour and absconding reaches a point whereby the Young Person or others cannot be kept safe. 4) WSCB to consider the findings of the Ofsted thematic inspection –‘From a Distance’ and adopt the recommendation to LSCBs as outlined: ‘Monitor the performance of Walsall LA and partners in meeting the needs of all Looked After Children living in and out of the local authority area, paying particular attention to: 45 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review ⎯ the extent to which specialist services are available ⎯ the sufficiency of education and health resources ⎯ the risk to children missing from care ⎯ the effectiveness of the local authority sufficiency strategy in reducing the number of children placed out of the area’. 46 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review APPENDIX B WSCB Serious Case Review W4 Individual Single Agency Recommendations Walsall Children’s Services 1) Where an allegation of abuse has been alleged all children in the household should be seen and spoken to alone 2) All information relating to a child should be held on the electronic case file. 3) All management decisions must be recorded on the electronic case file as an evidence trail for decision making 4) Visits should not be recorded as statutory visits where the young person has not been seen or seen alone 5) Core Assessments should be updated at a minimum of 6 months 6) There is a need to reinforce the need for case recording to be uploaded within the prescribed timescale of 3 days from the event. 7) Early LAC Review’s should be convened if there are significant concerns about a child and or placement. 8) IRO Recommendations at Review should be child specific and should not repeatedly use blanket statements. 9) Disruption Meetings must take place when at the point where it becomes evident that a placement is likely to break down. 10) Where young people are refusing to undergo a health assessment the Looked After Nurse should be engaged to visit them in placement. West Mercia Police 1) Police should be more proactive in challenging agencies with regards appropriateness of care facilities should such issues as this particular case arise again. 2) Police supervisors should be encouraged to be more intrusive in debriefing incidents involving child safeguarding. 3) The use and availability of restorative intervention should be more widely considered when dealing with similar cases such as this in the future. 47 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Walsall Healthcare NHS Trust 1) Review of Safeguarding Supervision Policy to ensure minimum standards of supervision for LAC team. 2) Review of self-harm policy to ensure clear guidance regarding management of client following A&E attendance. 3) All breaches against the self-harm policy to be reported through the Incident Reporting Process. 4) Audit of actions against all self-harm attendances in A&E against self-harm policy 5) Review of organisational structure of LAC and Safeguarding services to ensure appropriate and adequate management and clinical leadership arrangements 6) Revision of policy for the management of A&E notifications to ensure effective identification and follow up for Young People who self harm. Shropshire CCG 1) GP surgeries to routinely check on receipt of receiving a new young person as a patient, that pertinent information is included within their records. To include: -Whether a LAC/CIN or subject of a CP plan -Next of kin details - Name and contact details for named social worker - As well as the medical history, information on any significant social, emotional or educational needs that may impact on their care 2) GP surgeries to routinely ensure all the above relevant history is included within medical records and available to be forwarded to the next GP practice when a young person leaves their care. 3) All GP practice staff to receive suicide prevention and self-harm toolkits to increase understanding and awareness of the vulnerabilities and needs of these young people. 4) Encourage and share across Shropshire GP practices the good practice achieved through practice staff using the ‘Blue Stream Academy’ on line elearning tool for accessing training and development for Care Quality Commission (CQC) compliance 5) If young people don’t attend CAMHS appointments, GP’s to be informed to review if required to ensure continuation of medication and treatment 6) Ensure that all LAC children have their mental health and well-being routinely screened using the SDQ as required by government. Ensuring that these results are available to inform the need for a full psychological mental assessment by CAMHS in order to secure the appropriate response/intervention and medication is implemented accordingly. 48 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review Shrewsbury & Telford NHS Trust 1) Wards to inform Social Workers of attendance at hospital 2) Flow chart to be devised for Managing Looked After Children in Hospital 3) Discharge summaries for Looked After Children to also be sent to Social Worker 4) The Trust to work with commissioners and CAMHS to gain further knowledge in managing challenging behaviour in young people. Learning Review of a local case to be shared with senior nurses across the Trust. 5) Annual safeguarding audit 6) Retrospectively flagging ‘looked after children’ on computer system, until CP-IS is in place Shropshire Community NHS Trust 1) A review of CAMHS documentation to ensure that, patient name, date of birth and NHS number are on each page, that there is a place for printed name, signature, date and designation. Labels to be used with patients PID to be used. 2) An evaluation of out of area placements to ensure that robust processes are in place to ensure that funding is in place to avoid delaying service provision to a child. 3) When a request for information is sent this is followed up within 2 weeks if no response has been received. 4) A system to be developed to ensure that when a review of CAMHS records to ensure that all copies of correspondence are signed and clearly identified as being a file copy, to consider removing excess copies. 5) Message forms to be redesigned to incorporate patients name, date of birth, NHS number and signature of person taking message also date and time of the message, who the message is from and where appropriate who the message is for. Walsall YJS and West Mercia YOS 1) The YOS’s to explore the merits of implementing an Integrated Action Plan to replace the use of three asset plans 2) Complete a training needs analysis to identify any staff that require child and adolescent development training 3) Management review of risk management processes, including the RMVP and CPF 4) Safeguarding policy to be finalised and issued to all staff 5) LSCB to consider greater involvement of YOS files in their multi agency themed audits 49 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review 6) To explore the possibility of IRO’s being included into the joint audits between Walsall YJS and Walsall LAC Teams 7) Staff to be issued with guidance regarding the need to undertake parenting assessments in Court reports where family members continue to be involved in the care of LAC 8) To develop written working agreements with children’s care homes 9) The indentified good practice in W4’s case to be disseminated to all staff 10) Walsall YJS to consult with the YJB regarding issues of cross boundary involvement in CLR’s, with an expectation that the YJB considers setting standards for YOS’s collaboration 11) Further consideration to be given to the secondment of a Social Worker into the YOS/YJS Shropshire Children’s Social Care 1) Shropshire Children’s Social Care to continue to ensure that where there are escalating concerns about a child placed in their area, appropriate challenge will be made to the placing authority regarding what action they are taking to manage the risk. 2) The child protection procedures to be reviewed and revisions made as necessary to include the direction given in the point above as well as arrangements for cross-border escalation should concerns not be dealt with in a satisfactory manner. 3) The review of the Joint Protocol for Missing Children (West Mercia LSCB Consortium – Shropshire, Telford and Wrekin, Herefordshire, and Worcestershire) to be completed by autumn/winter 2014 and the revision should take into account the relevant matters raised by this case. 4) Shropshire to continue to ensure that where there are referrals which indicate significant harm either suspected or occurring to a looked after child placed in Shropshire by another local authority - a Strategy Meeting involving key agencies should be convened as per child protection procedures. West Midlands Police 1) Identification of vulnerability and suitable recording and referral for children within children’s homes/care facilities. 50 Walsall Safeguarding Children Board (WSCB) W4 Serious Case Review APPENDIX C Bibliography From a Distance – Looked After Children living away from their Home Area – Ofsted Thematic Inspection – April 2014 Joint Protocol for Reporting Missing Children & Young People – West Mercia Police & West Mercia Local Authorities – October 2011 Learning Lessons from Serious Case Reviews: interim report 2009-10 Ofsted’s evaluation of serious case reviews 1 April – 30 September 2009 Learning Lessons from Serious Case Reviews: year 2 Ofsted’s second year of evaluating serious case reviews. April 2008 – March 2009 Standing on my own two feet – research report NSPCC - 2011 Working Together to Safeguard Children – a guide to interagency working to safeguard and promote the welfare of Children – March 2013 51

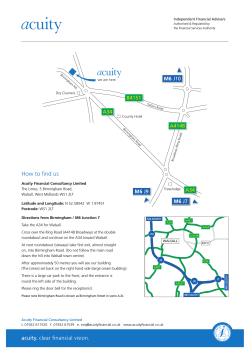








© Copyright 2026