ABC
docz
Explore
Log in
Create new account
Download
Report
No category
- Infectious Disease Clinics of North America
How to do the wiring of XM 300C, XD 312:
Insect Bites and Stings Patient and Family Education
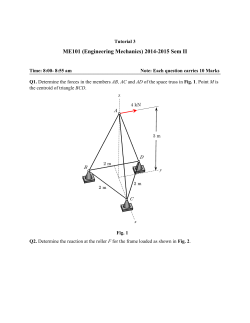
Tutorial 3 Questions
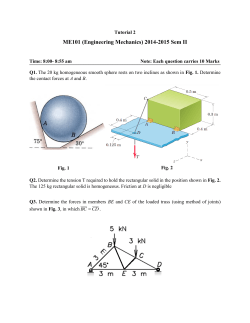
Tutorial 2 Questions
FA-1 Syllabus Class
EMS Bites and Envenomations Treatment Protocol
ME 121 Engineering Mechanics II Homework 4 Problems
PoLogCem 4.2. How to build the nonlinear regression cement plant?
Homework 8
www.TabletMod.com This guide shows how to tailor the calibration manually to... Build. This is based on the Intuos4 Large assuming...
© Copyright 2026
About abcdocz
DMCA / GDPR
Report