
the widowhood effect: a comparison of jews and catholics
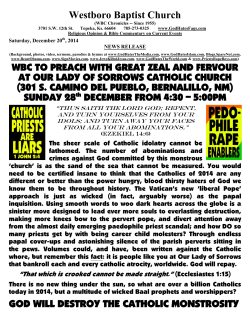
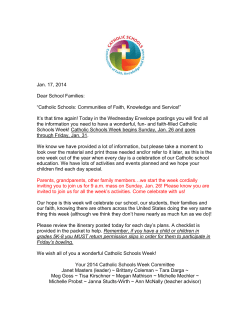
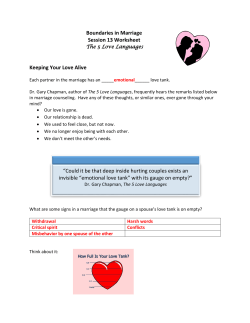
OMEGA, Vol. 59(4) 325-337, 2009 THE WIDOWHOOD EFFECT: A COMPARISON OF JEWS AND CATHOLICS ERNEST L. ABEL, PH.D. MICHAEL L. KRUGER, MS Wayne State University, Detroit, Michigan ABSTRACT Using mortality data derived from tombstones in two Midwestern cemeteries, we compared the “widowhood effect” (decreased survival following the death of a spouse) among Jews and Catholics. Jewish men and women were both more likely to die sooner after the death of their spouses compared to Catholic men and women. Life table survival analysis indicated that the median number of years of survival following widowhood for Catholic and Jewish men were 7.7 years and 5.0 years, respectively (p < .01). For Catholic and Jewish women, it was 11.0 and 9.5 years, respectively (p < .01) Interpretations were offered in terms of Bowlby’s attachment theory. INTRODUCTION Married people are more physically active, more psychologically stable, and live longer than their unmarried counterparts, and this advantage is more pronounced for men than for women (Gove, 1973; Hu & Goldman, 1990; Nock, 1995; Waite, 1995; Yanrreng & Goldman, 1990). In contrast to the beneficial effects of marriage on longevity, the bereavement associated with widowhood adversely affects physical health (Stroebe & Stroebe, 1993), and in so doing, decreases longevity for the surviving spouse, a phenomenon known as the “widowhood effect,” or 325 Ó 2009, Baywood Publishing Co., Inc. doi: 10.2190/OM.59.4.c http://baywood.com 326 / ABEL AND KRUGER “broken hearted effect” (Elwert & Christakis, 2006; Umberson, Wortman & Kessler, 1992). Mortality differences among groups within the same country can be clues to the role of different lifestyles and health-related behaviors (Rosenwaike, 1990). Examinations of mortality patterns for all causes among religious groups have a long history (Rosenwaike, 1990), but the role of religious affiliation on the “widowhood effects” has not been hitherto explored. This is the first study to show that survival of one spouse after the death of the other is related to religious affiliation. The theoretical framework in which we examined this hypothesis was Bowlby’s attachment theory (Bowlby, 1980) and the “continuing bonds” model (Waskowic & Chartier, 2003). According to attachment theory, when individuals encounter actual or potential threats to their security they automatically turn for protection and comfort to attachment figures or to internalized representations of them. When attachment figures are no longer readily available, their absence triggers memories of these attachment figures and unconscious “wishes” for reunion with them or their surrogates (Shaver & Mukulincer, 2005). Since this is not possible in the case of the death of an attachment figure, the emphasis is shifted from actual reunion to developing new and different type of “continuing bond” (Waskowic & Chartier, 2003) with the departed (Silverman & Nickman, 1996). These “continuing bonds” often take the form of visiting the grave and dreaming about and speaking to the deceased (Waskowic & Chartier, 2003). In this context, one of the ways religions may influence the reaction to the death of a spouse is by providing hope that the surviving spouse will be reunited with the departed spouse (the former attachment provider) after death. Since resurrection and reunion with a departed spouse is more integral to Christianity than Judaism (Abel, 2009; Harley & Firebaugh, 1993; Hood, Spilka, Hunsberger, & Gorsuch, 1996), the decreased belief in reunion with a spouse after death on the part of Jews may have resulted in a greater “widowhood” effect than for Christians (i.e., Jews died sooner after the death of a spouse than Christians). The data base we used to test this hypothesis was tombstones. Tombstones are death notices written in stone. These death notices contain information relating to gender, day, month, and year of death and often birth as well. If birth information is omitted, the age of death is usually included so that year of birth can be determined. Marital status and other familial relationships are often included on tombstones or can be inferred from inclusion of statements on them such as “husband of” or “wife of,” “mother,” and “father” or occurrence of male and female names incised on the same stone, or on adjacent gravestones containing the same surname and similar birth years. From such data, the date of death for each individual can be readily obtained, as well as information as to which one of a married couple died first, and the period of widowhood after the death of the other spouse (Foster & Hummel, 1995; Foster, Hummel & Adamchak, 1998; Haveman, 1999; Kephart, 1950; Young, 1960). Although some of these same data are THE WIDOWHOOD EFFECT / 327 available from vital (natality and mortality) registries, such registries were not implemented in parts of the United States before 1919 (Petersen, 1975) and were not uniformly implemented until 1933 (Petersen, 1975). Most importantly for the present purposes, religious affiliation has not been included in these data sources. For this study we operationally defined religious affiliation as burial in a Jewish or Catholic cemetery. Cemeteries for Jews and Catholics are each affiliated with and managed by related religious organizations, and restrict those who are allowed to be buried on those premises, so that only Jews are permitted to be buried in Jewish cemeteries and only Catholics are permitted to be buried in Catholic cemeteries (Abel, Kruger, & Abel, 2008). We did not include Protestants in this comparison because there are many more doctrinal distinctions within Protestantism than within Judaism or Catholicism (Xu, Hudspeth, & Bartowski, 2005). We did not attempt to compare Jews and Catholics buried in other cemeteries because most tombstones in nondenominational cemeteries do not identify Christians as Catholics or Protestants. An obvious shortcoming associated with relying on cemetery data for religious identity is that burial in a cemetery associated with a particular religion does not indicate the extent of religiosity of those interred in that cemetery. While religious belief per se is positively correlated with increased health and longevity (Goldbourt, Yaari, & Medalie, 1993; Hummer, Rogers, Nam & Ellison, 1999; Idler & Kasl, 1997; Oxman, Freeman & Manheimer, 1995), the beliefs associated with a particular religion, rather than their intensity as reflected in frequency of prayer or church attendance, are more strongly associated with health and longevity—that is, differences between religions are more important than differences within religions (Brown, Nesse, House, & Utz, 2004; Idler & Kasl, 1997). METHODS Information regarding birth and death were based on tombstones from two large cemeteries, Holy Sepulchre Catholic Cemetery and Adat Shalom Cemetery, in the Detroit, Michigan metropolitan area. These cemeteries were chosen because they are relatively large and for the pragmatic reason of proximity. According to Jewish custom, only people of Jewish faith can be buried in a Jewish cemetery and only those professing Catholicism are buried in Holy Sepulchre. Adat Shalom Cemetery is owned and operated by Adat Shalom Synagogue. Holy Sepulchre is owned and operated by the Roman Catholic Archdiocese of Detroit. Thus, all burials in each cemetery represent two distinct religious populations for comparison. Variables Digital photographs of all grave markers were obtained from Adat Shalom and from lots 15 to 20 in Holy Sepulchre Catholic Cemetery in 2007. These photographs were then transcribed into an Excel file and analyzed. For inclusion, the 328 / ABEL AND KRUGER month, day, and year of death and of birth had to be present for both husband and wife on the grave marker. To avoid selection bias arising from one of the spouses not being included because death had not occurred, we restricted our analysis to couples in which both the husband and wife were born during or before 1920. Categorial data were analyzed using the Binomial, Fisher’s Exact Test, and Wilcoxin-Mann-Whitney U-tests. Analysis of Variance and the Student’s Independent Samples “t”-test (two-sided) were used to determine differences between the two cemeteries in terms of the average year of birth for interments, age at death, age differences between spouses based on year of birth (a proxy for age differences at time of marriage), age at widowhood, and determination of the “widowhood” effect—that is, the time between death of a spouse and the death of the surviving spouse. Analysis of covariance was used to determine differences relating to religion, after controlling for the previously mentioned factors. Hierarchial multiple regression was used to examine the effects of religious affiliation by first controlling for the effects of age, gender, age difference between spouses, and birth year as the first block, followed by religion and then by the religion by age interaction. Life table survival analysis (Matthews & Farewell, 2007) was conducted to compare the year-to-year survival rates for the Catholics and conservative Jews. All statistical analyses were conducted using SPSS 15.0 for windows (SPSS, 2008). RESULTS There were 284 Jewish couples and 276 Catholic couples in our final sample. The average birth years for husbands interred in the Jewish and Catholic cemeteries were 1907 and 1904 respectively; average birth years for their wives were 1910 and 1908 respectively. The differences between Jews and Catholics were statistically significant for both males and females (t = 2.7, 2.8; df = 558, p < 0.01, respectively). As anticipated, husbands were born before their wives. The average year of birth for all women was 1909 vs. 1906 for men (F = 303.6, 0, df = 1, 559; p < .001). Overall, 76% of the women married older men (Binomial test, p < .001). On average (± S.D.), women married men who were 3.2 ± 4.3 years older. Of the 23.9% of the women who married younger men, husbands were 1.8 ± 3.0 years younger. Jewish women were much more likely to marry older men compared to Catholic women (81.8% vs. 71% respectively; Fishers exact = p < .01). However, the mean age difference between Jewish and Catholic couples was not statistically significant. For Jewish couples, the difference in age was 3.1 (± 3.6 years) compared to 3.2 (± 4.9) years for Catholic couples. Since husbands were older than their wives when they married, and men traditionally have shorter life spans than women, it was not surprising that most THE WIDOWHOOD EFFECT / 329 husbands died before their wives. Seventy percent (68.9%) of the husbands died first (p < .001, binomial test). The average age at death for men was 77.9 ± 11.4 years compared to 81.3 ± 10.2 for women. This difference was not statistically significant when corrected for birth year. The average age at death for Jews was 80.9 ± 11.1 compared to 78.3 ± 11.3 for Catholics (F = 14.4, df = 1, 556; p < .001, corrected for birth year). The interaction between gender and religion was statistically significant (F = 5.1, df = 1, 556; p < .03). The average age at death for Jewish women was 81.8 ± 9.4 compared to 80.8 ± 10.9 for Catholic women. The average age at death for Jewish men was 79.7 ± 10.4 compared to > 76.3 ± 12.1 for Catholic men indicating that the interaction occurred because Jewish men lived longer than Catholic men (p < .001), whereas Jewish and Catholic women did not differ significantly in age at death. Women who survived their husbands lived several years longer compared to husbands who survived their wives (13.4 ± 9.8 vs. 8.6 ± 8.3 years respectively; F = 6.0, df = 1, 553; p < .02; corrected for birth years of husbands and wives and age of widowhood). The main effect of religion on survival after widowhood was statistically significant (F = 5.9, df = 1, 553, p < .02, controlling for gender, age at widowhood, birth year). Both Catholic men and women lived longer than Jewish men and women after the death of a spouse. Life Table survival analysis for Jews and Catholics is shown in Figure 1. For each year after the death of a spouse, a lower percentage of Jewish widows and widowers survived the death of their spouse compared to Catholic widows and widowers. The median number of years of survival following widowhood for Jewish and Catholic men was 5.0 and 7.7 years, respectively. For Jewish and Catholic women, it was 9.5 and 11.0 years, respectively (Wilcoxin statistic = 9.3; 14.2; df = 1, p < .01 for men and women, respectively). For the first five years of widowhood, a higher percentage of Catholic men (69.7%) survived widowhood compared to Jewish men (50.0%; Fisher’s exact, p < .02, two-sided). For those men who survived the first 5 years of widowhood, 62.3% of Catholic men survived an additional 5 years compared to 59.2% for Jewish men. This difference was not statistically significant. For women, 83.0 % of Catholic women survived the first five years of widowhood compared to 71.0% for Jewish women (Fisher’s exact, p < . 01, two-sided). For those women who survived the first 5 years of widowhood, 76.5% of Catholic women survived an additional 5 years compared to 66.2% of the Jewish women. This difference was also not statistically significant. To examine the effects of religious affiliation independent of the effects of other variables associated with mortality, we also performed a hierarchical multiple regression analysis. In this analysis, we determined if survival time after the death of a spouse would still be significantly related to religious affiliation after initially controlling for the block variables of gender, birth years, age differences between husbands and wives, and age at widowhood; religion was then entered as the second step, followed by the interaction between religion × age as the third step. 330 / ABEL AND KRUGER Figure 1. Cumulative percent survival during the first ten years following widowhood for Catholic and Jewish husbands and wives. THE WIDOWHOOD EFFECT / 331 The initial block variables accounted for 49% of the variability in survival after the death of a spouse (F = 135.0, df = 4, 555, p < .001, R2 = 0.49) with age at spouse’s death, gender, and age difference between spouses all significant (p < .03). Religion was also a significant predictor of spousal survival, but accounted for only 0.5% of the variance after controlling for the variables entered at step 1 (F = 5.1, df = 1, 554, p < .03, R2 = .005). The interaction between religion and age at widowhood was not a significant predictor of spousal survival. Table 1 presents the details of the regression model. DISCUSSION In agreement with previous studies of widowhood (e.g., Elwert & Christakis, 2006; Kraus & Lilienfield, 1959; Martikainen Martelin, Nihtila, Majamaa, & Koskinen, 2005; Parkes Benjamin & Fitzgerald, 1969; Schaefer, Quesenberry, & Wi, 1995; Van-Grootheest, Beekman, Van-Groenov, & Deeg, 1999) we found that women generally survived their husbands and lived more years after the death of their spouses than vice versa. Based on Bowlby’s (1980) attachment theory, one reason for the greater impact of widowhood on men is that men derive much more of their social support from their wives than vice versa. This theory was originally developed to explain the evolutionary advantages infants derive from developing an affectionate bond for caregivers. This includes not only protection from predators, but also a sense of security. This feeling of attachment security becomes the basis for future intimate relationships with others, especially spouses. When the attachment is sundered by the death of a spouse, it can be devastating because of the loss of Table 1. Hierarchical Regression Model: Variables Predicting Survival Following Death of a Spouse STEP 1 Variable Unstand b Std. Err. Stand b t Sig. R2 0.493 Age –.596 .033 –.665 –18.2 .000 Gender 1.644 .648 .079 2.54 .012 Age difference Birth year .147 .069 .065 2.13 .034 –.021 .035 –.019 –0.60 .551 .667 –.067 –1.95 .050 .005 –.007 –.19 .850 .000 1.39 .164 2 Religion –1.297 3 Religion by age –2.38 1.25 (Constant) 94.61 67.90 332 / ABEL AND KRUGER emotional support derived from that attachment (Berado, 1970; Gove, 1973; Pihlblad, Adams & Rosencranz, 1972). This emotional loss can weaken immune function and resistance to diseases, precipitating death (Martikainen et al., 2005; Wortman and Silver, 1989). The loss of a spouse has a greater impact on men (Van-Grootheest et al., 1999) because the restraints on unhealthy behaviors—e.g., poor nutrition, alcohol consumption—provided by marriage, are greater for men than women (Umberson et al., 1992). In the present study we evaluated the role of religious affiliation, operationally defined as burial in a specific cemetery, in the context of the widowhood effect. Applications of attachment theory to religiosity (Granquist & Hagekull, 2001) propose that one of the main reasons individuals turn to religion in times of difficulty is that religions hold out the promise of being reunited (i.e., reattachment) with a loved one after death, thereby providing a source of comfort when a spouse dies. Another reason the widowhood effect has a greater impact on men may be because religion is less salient in their lives compared to women (Koenig, Hays, Larson, George, Cohen, McCullough et al., 1999), thereby diminishing the psychological comfort of a “continuing bond” that survives death (Waskowic & Chartier, 2003). Similarly, the decreased belief in reunion with a spouse after death on the part of Jews compared to Catholics (Abel, 2009; Harley & Firebaugh, 1993; Hood et al., 1996) may result in a greater negative impact on the general emotional well being of Jews. This in turn may reduce restraints on unhealthy behaviors, resulting in a significantly greater “widowhood” effect, especially in the first few years after a spouse’s death. In the present study, a higher percentage of Catholic men and women, compared to Jewish men and women survived the first 5 years of widowhood, whereas differences between Catholics and Jews were not statistically significant during the second 5 years. This is similar to other studies noting a higher incidence of stroke, heart attack, and cancer among the recently widowed (Chen, Bierhals, Prigerson, Kasl, Mazure & Jacobs, 1999; Engstrom, Gunnar, Khan, Ziab, Ijerntorpa, PessahRamussen, et al., 2004; Parkes et al., 1969), and a decreased death rate the longer the survival after the death of a spouse. Whereas interment in a cemetery managed by a religious organization does not indicate sincerity of belief in a particular religion, a study of widowed individuals found that the frequency of church/synagogue attendance was less important than an individual’s religious self-identity in coping with the loss of a spouse (Brown et al., 2004). In other words, it is not the degree of religiosity (e.g., church/synagogue attendance, frequency of prayer, or intensity of prayer) but the basic belief structure itself that influences the extent to which one relies on religion as a coping mechanism. The possible involvement of artifacts influencing gender and religious differences warrants some additional discussion. The fact that the widowhood effect is THE WIDOWHOOD EFFECT / 333 greater for men than women could simply have been the result of husbands being older than their wives, so their dying before their wives and their shorter mortalities after the death of their wives would be expected. However, even after controlling for the age factor, husbands were still more likely to have a stronger widowhood effect (i.e., they died sooner after their wives rather than vice versa), implying that other factors mediate this difference. Alternatively, gender differences may have resulted from the greater tendency of men to remarry after widowhood (Lillard & Pannis, 1996). If remarriage removes men with the highest levels of well being, those who remain unmarried would be those who experience the greatest trauma. The higher incidence of the widowhood effect among men in our study might therefore be a result of our including only couples who were buried next to one another. However, Lee, De Maris, Bavin, and Sullivan (2001) note that while more common among men than women, remarriage is still relatively uncommon among widowers, particularly those who were older when their wives died. Reports dating back to the 18th century have noted that adult mortality rates among Jews is lower than for other religious groups (Derosas, 2003; Van Straten & Snel, 2006), a finding that has continued to the present (Rosenwaike, 1990; Van Straten & Snel, 2006). We likewise found that Jews on average tended to live longer than Catholics. One reason for the aggregate lower mortality of Jews is that Jews may be more health-conscious and therefore more likely to seek medical help at an early stage of illness (Derosas, 2003). Because Jews live longer than Catholics, Jewish men may have been more likely to die sooner than Catholic men after the death of their respective spouses, simply because they were older. We eliminated this possibility by controlling for age at widowhood in our covariance and regression analyses. Even after controlling for the age difference at death, Jewish men were still more likely to die following the death of a spouse than were Catholic men. Another artifact is assortative mating (Johnson, 1980). Assortative mating means that individuals with poor health, smokers, those with behavioral disturbances, etc. will be less likely to marry but if they do, their spouses are also more likely to marry those with similar characteristics and therefore die within a short period of one another thereby increasing the impact of the “widowhood effect.” The higher mortality of unmarried individuals and the higher mortality associated with widowhood could thus be due to their inherent similarities among couples (Kiernan, 1988; Martikainen et al., 2005; Mastekaasa 1992). While the associative mating artifact may account for some widowhood effects, an assortative mating artifact cannot account for the stronger widowhood effect among Jews because their healthier lifestyles and greater longevities overall should have an opposite effect on widowhood (i.e., they should live longer). 334 / ABEL AND KRUGER A major advantage of our data base was that deaths could be compared over a broad age range, which is sometimes not possible using other data bases such as Medicare records which only include individuals 65 years of age and older (e.g., Elwert & Christakis, 2006; Schaefer et al., 1995). There are, however, several major shortcomings related to our data base such as the absence of personal information about health, cause of death, weight, etc. that are possible using Medicare and similar data bases (e.g., Elwert & Christakis, 2006). We also do not know if there are socioeconomic status differences between these two groups, whether these were first or higher order marriages, or whether those buried in these cemeteries were born in the United States or were recent immigrants. We also were unable to compare Jews and Catholics buried in other types of cemeteries for the practical reason that religious affiliation is not part of tombstone inscriptions in these cemeteries. While religious symbols for Jews (e.g., a star) indicate religious identity, no such marking symbol denotes Catholicism. Also problematic is the inability to take into account individuals who were cremated. While some individuals may still have markers erected in their memory, we are unable to determine anything about such individuals. Despite these shortcomings, the present data indicate that religious identity affects survival of widowers after the death of their spouses. REFERENCES Abel, E. L. (2008). Changes in gender discrimination after death. Omega, 58, 147-152. Abel, E. L. (2009). Death gods. Westport, CT: Greenwood Press. Abel, E. L, Kruger, M. L., & Abel, J. R. (2008). Beth El: Michigan’s oldest Jewish cemetery. Markers, 25, 67-93. Berado, F. M. (1970). Survivorship and social isolation: The case of the aged widower. Family Coordinator, 19, 11-15. Bowlby, J. (1980). Attachment and Loss. New York: Basic Books. Brown, S. L., Nesse, R. M., House, J. S., & Utz, R. L. 2004. Religion and emotional compensation: Results from a prospective study of widowhood. Personality and Social Psychology Bulletin, 30, 1165-1174. Chen, J. H., Bierhals, A. J., Prigerson, H. G., Kasl, S. V., Mazure, C. M., & Jacobs, S. (1999). Psychological adjustment to sudden and anticipated spousal loss among older widowed persons. Journal of Gerontology, 56B, S237-S248. Derosas, R. (2003). Watch out for the children! Differential infant mortality of Jews and Catholics in nineteenth-century Venice. Historical Methods, 36, 109-131. Elwert, F., & Christakis, N. A. (2006). Widowhood and race. American Sociological Review, 71, 16-41. THE WIDOWHOOD EFFECT / 335 Engstrom, G., Khan, F., Ziab, E., Ijerntorpa, I., Pessah-Ramussen, H., Norrving, B., & Janzona, L., et al. (2004). Marital dissolution is followed by an increased incidence of stroke. Cerebrovascular Diseases, 18, 318-324. Foster, G. S., & Hummel, R. L. (1995). The Adkins-Woodson Cemetery: A sociological examination of cemeteries as communities. Markers, 11, 92-117. Foster, G. S., Hummel, R. L., & Adamchak, D. J. (1998). Patterns of conception, natality and mortality from Midwestern cemeteries: A sociological analysis of historical data. The Sociological Quarterly, 39, 473-489. Goldbourt, U., Yaari, S., & Medalie, J. H. (1993). Factors predictive of long-term coronary heart disease mortality among 10,059 male Israeli civil servants and municipal employees. Cardiology, 82, 100-121. Gove, W. (1973). Sex, marital status and mortality. American Journal of Sociology, 79, 45-57. Granquist, P., & Hagekull, B. (1999). Religiousness and perceived childhood attachment: Profiling socialized correspondence and emotional compensation. Journal for the Scientific Study of Religion, 38, 254-273. Harley, B. & Firebaugh, G. (1993). Americans’ belief in an afterlife: Trends over the past two decades. Journal for the Scientific Study of Religion, 32, 269-278. Haveman, M. (1999). A sociological analysis of children’s gravestones. Illness, Crisis and Loss, 7, 266-286. Hood, R. W., Spilka, B., Hunsberger, B., & Gorsuch, R. (1996). The psychology of religion. An empirical approach. New York: Guilford Press. Hu, Y., & Goldman, N. (1990). Mortality differentials by marital status: An international comparison. Demography, 27, 231-250. Hummer, R. A., Rogers, R. G., Nam, C. B., & Ellison, C. G. (1999). Religious involvement and U.S. adult mortality. Demography, 36, 273-286. Idler, E. L., & Kasl, S. V. (1997). Religion among disabled and nondisabled persons: II. Attendance at religious services as predictor of the course of disability. Journal of Gerontology, 52B, 306-316. Johnson, R. A. (1980). Religious Assortive Marriage in the United States. New York: Academic Press. Kephart, W. M. (1950). Status after death. American Sociological Review, 15, 635-643. Kiernan, K. E. (1988). Who remains celibate? Journal of Biosocial Science, 20, 253-263. Koenig, H. G., Hays, J. C., Larson, D. B., George, L. K., Cohen, H. J., McCullough, et al. (1999). Does religious attendance prolong survival?: A six-year follow-up study of 3,968 older adults. Journal of Gerontology, 54A, M370-M377. Kraus, A. S., & Lilienfield, A. M. (1959). Some epidemiologic aspects of the high mortality rate in the young widowed group. Journal of Chronic Diseases, 10, 207-217. Lee, G. R., De Maris, A., Bavin, S., & Sullivan, R. (2001). Gender differences in the depressive effect of widowhood in later life. Journal of Gerontology, Series B, 56, S56-S61. Lillard, L.A., & Panis, C. (1996). Marital status and mortality: The role of health. Demography, 33, 313-327. Martikainen, P., Martelin, T., Nihtila, E., Majamaa, K., & Koskinen, S. (2005). Differences in mortality by marital status in Finland from 1976 to 2000: Analyses of changes in marital-status distributions, socio-demographic and household composition, and cause of death. Population Studies, 59, 99-115. 336 / ABEL AND KRUGER Mastekaasa, A. (1992). Marriage and psychological well being: Some evidence on selection into marriage. Journal of Marriage and the Family, 54, 901-911. Matthews, D. E. and Farewell, V. T. (2007). Using and understanding medical statistics. New York: Karger, 2007. Oxman, T. E., Freeman, D. H., & Manheimer, E. D. (1995). Lack of social participation or religious strength and comfort as risk factors for death after cardiac surgery in the elderly. Psychosomatic Medicine, 57, 5-15. Parkes, C. M., Benjamin, B., & Fitzgerald, R. G. (1969). Broken heart: A statistical study of increased mortality among widowers. British Medical Journal, 1, 740-743. Petersen, W. (1975). Population. New York: Macmillan. Pihlblad, C. T., Adams, D., & Rosencranz, D. (1972). Socio-economic adjustment to widowhood. Omega, 3, 295-305. Rosenwaike, I. (1990). Mortality patterns among elderly American Jews. Journal of Aging and Judaism, 4, 289-303. Schaefer, C., Quesenberry, C. P., & Wi, W. (1995). Mortality following conjugal bereavement and the effects of a shared environment. American Journal of Epidemiology, 141, 1142-1152. Shaver, P. R., & Mukulincer M. (2005). Attachment theory and research: Resurrection of the psychodynamic approach to personality. Journal of Research in Personality, 39, 22-45. Silverman, R. P., & Nickman, S. L. (1996). Introduction: What’s the problem? In D. Klass, R. P. Silverman, and S. L. Nickman (Eds.), Continuing bonds: New understandings of grief (pp. 3-27). Washington, D.C.: Taylor & Francis. SPSS. (2008). Statistical Package for the Social Sciences. Chicago, IL: SPSS, Inc. Stroebe, M. S., & Stroebe, W. (1993). The mortality of bereavement. In M. S. Stroebe, W. Stroebe, & R. O. Hansson (Eds.), Handbook of Bereavement (pp. 175-195). New York: Cambridge University Press. Umberson, D., Wortman, C. B., & Kessler, R. C. (1992). Widowhood and depression: Explaining long-term gender differences in vulnerabilities. Journal of Health and Social Behavior, 33, 10-24. Van-Grootheest, D. S., Beekman, A. T., Van-Groenou, B., & Deeg, D. J. 1999. Sex Differences in depression after widowhood. Do men suffer more? Social Psychiatry and Psychiatric Epidemiology, 34, 391-398. Van Straten, J., & Snel, H. (2006). The Jewish “Demographic Miracle” in Nineteenthcentury Europe. Historical Methods, 39, 123-131. Waite, L. (1995). Does marriage matter? Demography, 32, 483-504. Waskowic, T. D., & Chartier, B. M. (2003). Attachment and the experience of grief following the loss of a spouse. Omega, 47, 77-91. Wortman, C. B., & Silver, R. C. (1989). The myths of coping with loss. Journal of Consulting and Clinical Psychology, 57, 349-357. Wyke, S., & Ford, G. (1992). Competing explanations for associations between marital status and health. Social Science & Medicine, 34, 523-532. Yanrreng, H., & Goldman, N. (1990). Mortality differentials by marital status: An international comparison. Demography, 27, 233-250. Young, F. W. (1960). Graveyards and social structure. Rural Sociology, 25, 446-450. THE WIDOWHOOD EFFECT / 337 Xu, X., Hudspeth, C. D., & Bartowski, J. P. (2005). The timing of first marriage: Are there religious variations? Journal of Family Issues, 26, 584-618. Direct reprint requests to: Ernest L. Abel, Ph.D. C.S. Mott Center for Human Growth and Development Wayne State University 275 East Hancock Detroit, MI 48201 e-mail: [email protected]






© Copyright 2025