
▼ 23 N D
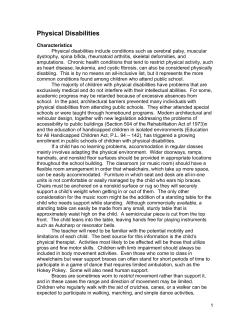
23 ▼ NEUROMUSCULAR DISEASES KATHARINE N. CIARROCCA, DMD, MSED MARTIN S. GREENBERG, DDS ADI GARFUNKEL, DDS ▼ CEREBROVASCULAR DISEASE ▼ CEREBRAL PALSY Cerebrovascular Accident or Stroke Transient Ischemic Attack Oral Health Considerations Clinical Manifestations Treatment Oral Health Considerations ▼ CAVERNOUS SINUS THROMBOSIS ▼ BELL’S PALSY Clinical Manifestations Treatment ▼ MULTIPLE SCLEROSIS Etiology and Epidemiology Clinical Manifestations Diagnosis Treatment Oral Health Considerations ▼ GUILLAIN-BARRÉ SYNDROME Clinical Manifestations Treatment and Prognosis ▼ MYASTHENIA GRAVIS ▼ AMYOTROPHIC LATERAL SCLEROSIS Clinical Manifestations Treatment Oral Health Considerations Clinical Manifestations Treatment Oral Health Considerations ▼ MUSCULAR DYSTROPHY ▼ PARKINSONISM: PARKINSON’S DISEASE (PARALYSIS AGITANS) Clinical Manifestations Treatment Oral Health Considerations Etiology and Pathogenesis Clinical Manifestations Treatment Oral Health Considerations ▼ EPILEPSY Classification of Seizures Clinical Manifestations Treatment of Seizures Oral Health Considerations ▼ HUNTINGTON’S DISEASE (HUNTINGTON’S CHOREA) Clinical Manifestations Treatment Oral Health Considerations 592 593 Neuromuscular Disease Diseases that affect both nerve and muscle tissue encompass a broad range of symptoms that often have profound implications for the successful management of the dental patient. The diseases discussed in this chapter include only those that affect the orofacial region or that have a significant effect on dental practice. ▼ CEREBROVASCULAR DISEASE Cerebrovascular disease includes all disorders that cause damage to the blood vessels supplying the brain, thereby producing neurologic damage. “Stroke” and “cerebrovascular accident” (CVA) are terms used to describe an acute neurologic injury resulting from a severe interruption in the flow of blood to the brain. Complete cessation of the flow may render an irreversible cerebral infarct within a period of 3 or 4 minutes. General symptoms following stroke include variable motor paralysis, sensory loss, visual difficulties, and speech impairment. Epidemiologic studies have shown that cerebrovascular disease is the third leading cause of death in developed countries, with a prevalence of 0.8% of the total population affected. It is estimated that more than 400,000 individuals are affected by stroke annually in the United States. The majority of patients are over 60 years of age. The overall mortality rate following stroke is 25% in the first month and 50% within 5 years. Cerebrovascular Accident or Stroke Approximately 80% of strokes are associated with the development of atherosclerosis leading to cerebral ischemia and infarction. The remaining 20% of cases are caused by cerebral hemorrhage.1 Deposition of atheromas in artery walls predisposes a patient to the development of thrombosis and embolus formation, which results in infarction of the area of the brain supplied by the occluded vessel. A thrombus is a clot in the vasculature that forms from the constituents of blood and may be occlusive or attached to a vessel without obstructing the lumen. An embolus is a clot, composed of a detached thrombus, mass of bacteria, or other foreign body, that originates from a distant site in the body and occludes a vessel. Atheromas commonly develop in the branching portions of the arterial system, particularly at the origin of the internal carotid artery. Additional sites of thrombus formation associated with stroke include the vertebral, basilar, and middle cerebral arteries. LACUNAR INFARCTION Lacunar infarcts are small lesions (usually < 5 mm in diameter) that occur in the distribution of the short penetrating arterioles in the basal ganglia, circle of Willis, pons, cerebellum, anterior limb of the internal capsule, and (less commonly) deep cerebral white matter. Lacunar infarcts are associated with poorly controlled hypertension or diabetes. Symptoms usually include unilateral motor or sensory deficit without visual field deficit or disturbance of consciousness or language. The neurologic deficit produced by the lacunar infarct may progress over 24 to 36 hours before stabilizing; however, the prognosis for recovery from the deficit produced by a lacunar infarct is usually good, with partial or complete resolution occurring over the following 4 to 6 weeks in many instances. CEREBRAL INFARCTION A cerebral infarction occurs when there is ischemia and necrosis of an area of the brain after a reduction of blood supply to a level below the level necessary for cell survival. The two major causes of cerebral infarction are thrombosis and embolism, often the result of atherosclerosis. Emboli frequently originate in atherosclerotic plaques in any vessel of the neck, such as the carotid artery. The emboli break off, pass through the vasculature, and ultimately occlude an intracranial vessel, thus causing a stroke. Thrombosis of an intracranial vessel may also lead to stroke. The resulting deficit depends on the particular vessel involved and the extent of any collateral circulation. Carotid artery atherosclerosis, for example, will most frequently cause infarction in the region of the brain supplied by the middle cerebral artery. Occlusion of this artery results in contralateral signs such as facial weakness, head and eye deviation, flaccid hemiparesis or hemiplegia, and hemisensory loss. Thromboembolic cerebral infarction also occurs as a complication of other diseases. Many of the emboli that occlude intracranial vessels arise from thrombi that have formed in the left side of the heart. Emboli originating from the heart are often the result of thrombus formation after acute myocardial infarction, chronic atrial fibrillation, or rheumatic heart disease. Hypertension is an important risk factor in the development of thrombosis, particularly at the carotid bifurcation. Treatment of severe hypertension is essential for the prevention of stroke since it is estimated that the risk of stroke increases sevenfold in individuals with uncontrolled hypertension. Septic emboli may result from bacterial endocarditis, particularly when the mitral valve is involved. Other causes of ischemia and infarction of the brain include decreased blood flow secondary to sudden severe hypotension, acute hypertension causing spasm of the cerebral vessels, and hematologic abnormalities such as thrombocytosis, anemia, and cavernous sinus thrombosis. CEREBRAL HEMORRHAGE Hemorrhage of intracranial vessels may also cause stroke. The two most common reasons for hemorrhage are (1) rupture of an aneurysm and (2) an arteriovenous malformation (AVM) that hemorrhages spontaneously, often secondary to hypertension or following the administration of anticoagulant medication. The majority of cases are aneurysmal. Aneurysms are localized dilations of arteries, caused by structural weakness of vessel walls. True aneurysms are found in arteries with normal wall structures that have been damaged by conditions such as atherosclerosis, mycotic infections, and syphilis. False aneurysms occur after the traumatic rupture of arteries and their subsequent repair by fibrous tissue. The size of the aneurysm is important in determining its tendency to rupture, a tendency that is aggravated by smoking, alcohol con- 594 sumption, or strenuous exercise. The sequelae of hemorrhage from ruptured aneurysms are usually sudden and severe, ranging from seizures and coma to death. In the acute situation, it is vital to distinguish ischemic stroke from hemorrhagic stroke by the use of computed tomography (CT) without contrast. CLINICAL MANIFESTATIONS AND TREATMENT OF STROKE Strokes due to ischemia may be classified clinically either as a stroke in evolution or as a completed stroke. “Stroke in evolution” is a descriptive term used to indicate a condition in which symptoms associated with cerebral ischemia become progressively worse while the patient is under observation. The etiology is often related to the propagation of a thrombus in the carotid artery. Treatment should be immediate and consists of controlling severe hypertension (> 185/110). However, decreasing milder hypertension may actually increase infarction in a patient with acute thrombosis. The use of thrombolytic agents such as recombinant tissue plasminogen activator may decrease the severity of a stroke in carefully selected patients, but intracranial hemorrhage complicates this therapy. This regimen attempts to minimize the extent of permanent neurologic damage due to ischemia. Anticoagulants (such as heparin) or antiplatelet therapy with aspirin may also be used. Daily low doses of aspirin are recommended to decrease the incidence of thromboembolic strokes.2 A completed stroke caused by a thrombus often evolves slowly, and the full neurologic picture may take hours or even days to emerge. This clinical picture commonly includes hemiplegia, aphasia, and cranial nerve defects involving nerves V, VII, IX, and X. Symptoms of stroke caused by an embolus develop suddenly. It is not preceded by transient ischemic attacks (see below); rather, the stroke itself evolves rapidly because the clot originates elsewhere and suddenly blocks a cerebral vessel. Whatever the cause of the neurologic damage, the resultant infarct may enlarge for a period of 4 to 5 days because of cerebral edema. Repair is dependent on good collateral circulation and is accomplished by the formation of fibrogliotic scar tissue. Significant clinical improvement may occur after 3 weeks, when the cerebral edema has subsided.3 After a completed stroke, treatment focuses on the prevention of further neurologic damage, through the reduction of underlying risk factors and by rehabilitation procedures, including speech and physical therapy. An intracranial hemorrhage should also be treated as a medical emergency of airway maintenance and requires the transfer of the patient to an intensive care unit with close monitoring. Blood pressure should be maintained in the 140/90 range. Fluid intake should be limited. Treatment with fibrinolytic drugs such as tranexamic acid might reduce new episodes of bleeding. Cerebral edema may be treated with dexamethasone and diuretics. The surgical treatment of a hemorrhaging aneurysm or an AVM consists of closing off the blood vessels that supply the area and removing the abnormality. This procedure has generally yielded high success rates. Principles of Medicine Transient Ischemic Attack A transient ischemic attack (TIA) is a sudden but reversible neurologic deficit that lasts from a few minutes to 24 hours. Approximately 30% of individuals with a history of TIA experience a completed stroke within a 5-year period.4 The frequency of TIAs varies considerably, ranging from multiple daily attacks over an extended period to only a few attacks before a true stroke occurs. ETIOLOGY An important cause of transient cerebral ischemia is embolization. In many patients who experience these attacks, a source is readily apparent in the heart or a major extracranial artery to the head, and emboli sometimes are visible in the retinal arteries. Cardiac causes of embolic ischemic attacks include rheumatic heart disease, mitral valve disease, cardiac arrhythmia, infective endocarditis, and mural thrombi complicating myocardial infarction. An ulcerated plaque on a major artery to the brain may also serve as a source of emboli. Hematologic causes of ischemic attacks include polycythemia, sickle cell disease, and hyperviscosity syndromes. CLINICAL MANIFESTATIONS The symptoms of TIAs vary markedly among patients; however, the symptoms in a given individual tend to be constant in type. Onset is abrupt and without warning, and recovery usually occurs rapidly, often within a few minutes. During the attack, a wide variety of neurologic signs and symptoms can develop, depending on which site of the brain is affected by ischemia. Repeated short periods of arm and hand weakness are associated with focal ischemia in the contralateral frontal lobe. If the vertebrobasilar arterial system is involved, short episodes of dizziness, diplopia, dysarthria, facial paresthesia, and headache are common symptoms. TREATMENT Treatment of TIAs should be initiated as soon as the diagnosis is established and should be directed toward the correction of the immediate pathologic problem (eg, embolism). In addition, measures to control the primary underlying problem (eg, hypertension or coagulopathy) should be undertaken. Anticoagulant therapy with either heparin or coumadin is often used, but there is little convincing evidence that anticoagulant drugs are of value. Treatment with aspirin, however, significantly reduces the frequency of TIAs and the incidence of stroke in high-risk patients. Dipyridamole is also used but is not as effective; when added to aspirin, it offers no advantage over the use of aspirin alone for stroke prevention.5 Vascular surgical endarterectomy is now often used as an alternative treatment of TIAs caused by carotid stenosis. After surgery, a reduction in the frequency of TIAs and their progression to stroke has been observed.4 Oral Health Considerations As the first line of medical management of stroke patients is often anticoagulant therapy, the patient may have a predis- 595 Neuromuscular Diseases position to excessive bleeding. A thorough medical history with an accurate medication list that includes dosages is essential. In addition, it may be necessary to confer with the patient’s physician to obtain current coagulation values (ie, PT, INR) so as to ensure that the patient is stable for more invasive dental treatment. Xerostomia is a common side effect of the medications used in the management of cerebrovascular disease and related disease processes. Patients who are thus affected can then be susceptible to a higher caries rate. Meticulous oral hygiene, more frequent recalls, saliva substitutes, and fluoride application can aid in the maintenance of the dentition.6 Stroke patients can also have physical disabilities, which can affect the orofacial area and can alter the provision of dental care. Patients with hemiplegia or hemiparesis may need additional help in home care. Patients with weakness in the muscles of the orofacial area may have poor control of oral secretions, a reduced gag reflex, and changes in their ability to masticate, leading to poor nutrition. Patients with apraxia affecting the orofacial region may have impaired voluntary movements, such as protruding the tongue, expectorating, and lip puckering. In general, dental treatment should not present major problems for most poststroke patients. Careful history taking, checking of blood pressure prior to treatment, avoidance of lengthy appointments, and general reassurance are all important factors in the provision of dental treatment for patients with a history of stroke. ▼ CAVERNOUS SINUS THROMBOSIS Cavernous sinus thrombosis, usually secondary to dental, nasal, or ocular infections, is a rare but severe complication because of its possible fatal outcome. Infections of the maxillary dentition may spread to the cavernous sinus through openings in the cranial bones or through emissary veins connecting the extra- and intracranial systems. Venous propagation begins with the facial vein and proceeds through the ophthalmic vein, which is an affluent of the cavernous sinus. In most cases, patients experience rapid swelling of the face and eyelids. The classic neurologic signs of acute cavernous sinus thrombosis are exophthalmos, periorbital edema, retinal vein thrombosis, and involvement of the ophthalmic division of the trigeminal nerve and trochlear and abducent nerves, leading to ptosis, dilated pupils, and lack of corneal reflexes. Treatment consists of immediate antibiotic therapy and the removal of the source of infection whenever possible. ▼ MULTIPLE SCLEROSIS Multiple sclerosis (MS) is a chronic neurologic disease associated with the demyelination of axons within the central nervous system. The disease occurs more frequently among women. The average age of onset is during the fourth decade of life, but MS may occur at any age. The disease presents in the form of recurrent attacks; in some cases, the attacks are years apart. The most common symptoms following an acute exacerbation include impairment of vision, muscular incoordination, and bladder dysfunction. The general histologic features are multiple disseminated plaques or areas of demyelination within the central nervous system. Etiology and Epidemiology The specific etiology of MS has not been clearly determined. An immunologic basis is strongly suggested by the presence of activated T lymphocytes and autoantibodies to glycoproteins detected in MS lesions. In addition, it is considered probable that both genetic and environmental factors are involved, with infection as the major environmental agent. Both viral and bacterial infections can initiate or precipitate attacks of MS. Evidence that implicates certain viruses in the initiation of the disease has been documented; increased antibody titers against measles virus, rubella virus, mumps virus, Epstein-Barr virus, herpes simplex viruses 1 and 2, and human herpesvirus 6 (HHV-6) have been found in the cerebrospinal fluid and serum. To date, none of these viruses has been isolated from the lesions of MS, and no specific relationship between MS and a specific microorganism has been proven. Further data supportive of an infectious etiology for MS include the observation that MS has occurred in clusters in specific populations, the prime example being the increased incidence of MS in the population of the Faroe Islands following foreign troop occupation during World War II.7 Genetic influences also appear to play a significant role in the development of MS. Studies of identical twins have shown that if one twin suffers from MS, there is a 26% chance that the other twin will also be affected by the disease. A preponderance of specific human leukocyte antigen (HLA) types has also been noted in MS patients.8,9 The most accepted general finding related to the etiology of MS is the fact that disease prevalence increases with distance from the equator; for example, MS is most common in northern Europe, Canada, and New Zealand. There are no obvious reasons for this geographic difference in disease prevalence. Clinical Manifestations The clinical signs and symptoms of MS depend on the site of the demyelinating lesion. The lesions may occur almost anywhere in the central nervous system, but they have a predilection for certain areas. More than 60% of individuals with MS have visual disturbances caused by demyelinating lesions of the second cranial nerve. The loss of vision usually occurs over a period of several days, with partial recovery within 1 month. Other ophthalmic symptoms include “color blindness” and diplopia caused by involvement of the third, fourth, and sixth cranial nerves. Uhthoff ’s sign, found in MS, is characterized by rapid vision loss following a body temperature increase that is associated with strenuous exercise. Another important sign of ocular disturbance associated with MS is Marcus Gunn’s pupillary sign, which can be elicited in patients with unilateral optic neuritis in the following manner: a bright light is shone into each eye separately; when this 596 light is moved from the normal to the affected eye, the pupil of the latter dilates rather than constricts. Weakness or paresthesia of the extremities, with an increase in the deep tendon reflexes, is another common early finding in cases of MS. An important feature of motor nerve function in MS patients is the relative fluctuation of symptoms on a daily basis. These symptoms may remit for long periods and then suddenly reverse, leading to paraplegia. Other common signs of the disease include bladder dysfunction, euphoria, ataxia, vertigo, and generalized incoordination. The majority of cases of MS are chronic and are characterized by exacerbations and remissions over a period of many years. During acute episodes, severe neurologic involvement is evident. This slowly resolves, but some permanent neurologic involvement remains after each episode. The extent and severity of the permanent involvement varies considerably from patient to patient. In mild cases, little permanent effect is noted, and patients may have a normal life span. In severe acute cases, total paralysis may occur within months. Overall, it has been found that approximately 70% of patients with MS live for more than 25 years after the onset of the disease. Diagnosis The diagnosis of MS is clinical and is based on the age of the patient, the presence of neurologic signs that cannot be explained by a single lesion, the progressive nature of the disease, and a history of exacerbations and remissions. There are no definitive laboratory tests for MS, but demyelinating changes can be seen on magnetic resonance imaging (MRI) in more than 90% of cases.4 The presence of increased immunoglobulins (specifically immunoglobulin G [IgG]) in the cerebrospinal fluid without infection is another diagnostic indicator of the disease. Treatment Evidence suggests that high doses of intravenous corticosteroids may arrest the progress of MS; about 85% of patients with relapsing-remitting MS show objective signs of neurologic improvement during treatment with intravenous corticosteroids. Long-term treatment with immunosuppressants may reduce the frequency of relapse in patients with MS. Azathioprine is probably the safest drug in this category and has reduced relapse to 70% of study patients in 3 years, compared to 80% of patients in the placebo group. Administration of methotrexate appears to be the best therapy for slowing deterioration in patients with chronic progressive MS. The use of interferon-γ-1b and -1a has shown promise; both have been shown to reduce clinical attacks and lesions detectable by contrast-enhanced MRI by approximately 30% when compared to placebo. Other nonpharmacologic measures, such as total lymphoid irradiation, plasmapheresis, and immunoglobulin therapy, have had marginal benefit.10 Oral Health Considerations Certain clinical manifestations of MS affect the orofacial region; three are of particular interest to the dentist: trigem- Principles of Medicine inal neuralgia, sensory neuropathy of the trigeminal nerve, and facial palsy.11 Trigeminal neuralgia (TGN) is present in about 2% of cases of MS and is an initial manifestation in 0.3% of cases.12 In those cases in which MS is associated with TGN, there appears to be an earlier age of onset, and symptoms are commonly bilateral. Pain is normally severe and lancinating, but trigger zones may be absent. In time, the pain often becomes less severe but more continuous. Effective drug therapy includes the use of carbamazepine, baclofen, gabapentin, or phenytoin. When medication proves inadequate, thermocoagulation, surgical sectioning of the nerve, or alcohol injection may be considered. Sensory neuropathy secondary to MS can be progressive and difficult to diagnosis. It most often affects the second and third divisions of the trigeminal nerve, has a sudden onset, and is painful. Neuropathy to the mental nerve can cause numbness of the lower lip and chin. Facial paralysis appears later in the course of the disease. It may be difficult to distinguish between the paralysis caused by MS and that due to Bell’s palsy, but up to 24% of MS sufferers may experience facial paralysis.11 ▼ AMYOTROPHIC LATERAL SCLEROSIS Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig disease and motor neuron disease, belongs to a group of degenerative diseases affecting both the upper and the lower motor neurons of the central nervous system. The principal symptoms are weakness and wasting, which normally begin in the upper extremities and are invariably unilateral at onset. The estimated prevalence of ALS in the United States is reported as 2 to 7 per 100,000 persons, with slightly more males than females affected. The average age of onset is between the fourth and sixth decades of life. The etiology is unknown, although the disease is familial in 10% of cases when it is inherited as an autosomal dominant or autosomal recessive trait.1 The degenerative changes of ALS can be seen in the corticospinal tracts (upper motor neurons), the motor cells of the brainstem, and the anterior horn cells of the spinal cord (lower motor neurons). Clinical Manifestations In the most typical form of ALS, stiffness of the fingers, awkwardness in tasks requiring fine finger movements, and slight weakness or wasting of the hand muscles are the first indications of the disease. Cramping and fasciculation of the muscles of the forearm, upper arm, and shoulder girdle also appear. Before long, the triad of atrophic weakness of the hands and forearms, light spasticity of the arms and legs, and generalized hyperreflexia (in the absence of sensory changes) leaves little doubt as to the diagnosis. After some time, the disease affects all regions, including the muscles of mastication, facial expression, and tongue, leading to difficulties in mastication and speech. Dysfunction of the temporomandibular joint and the 597 Neuromuscular Diseases development of malocclusion may also occur as the disease progresses. Aspiration pneumonia is the cause of death in most patients with ALS. Treatment There is no effective treatment for this disease, and the course is one of progressive deterioration, with a mean survival of 3 years. Ceftriaxone, gabapentin, guanidine hydrochloride, gangliosides, interferons, and cyclophosphamide are a few of the long list of agents that have all proven to be ineffective. Only supportive measures can be used.13 Oral Health Considerations Muscles of the orofacial area can be affected by the disease process of ALS. The most striking physical effect of ALS relates to the declining function of the muscles used for breathing. As the patient may not be able to cough or clear the throat, a reclining position for dental treatment is contraindicated due to the increased risk of aspiration.14 In addition, a hyperactive gag reflex can pose a problem. Although it provides assurance that no dental debris will be aspirated, every effort must be made not to induce gagging or vomiting. Topical anesthetics should be avoided, patients should be nil per os (NPO) for 12 hours prior to treatment, and the dentist should avoid contact with soft-tissue areas that may induce gagging. Topical fluoride may also induce nausea. Finally, patients with ALS may have difficulty with oral hygiene. Not only will these patients be challenged with physical disabilities that limit their effectiveness in maintaining oral hygiene, they are also faced with a loss of the natural clearing ability of the oral cavity because of decreased muscular activity of the tongue and the perioral musculature.14 Mechanical toothbrushes, fluoride rinses, and more frequent periodontal recall may benefit these patients greatly. ▼ PARKINSONISM: PARKINSON’S DISEASE (PARALYSIS AGITANS) Parkinsonism is a neurodegenerative disorder characterized by rigidity, tremors, bradykinesis, and impaired postural reflexes. The most common form of parkinsonism is Parksinson’s disease (paralysis agitans), but parkinsonism is seen in a variety of disorders such as postencephalitic parkinsonism, arteriosclerotic parkinsonism, and post-traumatic parkinsonism following closed head injury. Parkinson’s disease was first described by James Parkinson in 1817. It is an idiopathic disease that mainly affects adults in middle or late life. The reported prevalence rate in the general population is 130 in 100,000 persons; however, among those who are older than 60 years of age, the rate is considerably higher.15,16 striatum. Experiments to reduce dopamine levels in animals have clearly shown that the classic symptoms of Parkinson’s disease can be observed following this procedure. Thus, a low dopamine level will result in hypokinesia whereas a high level will lead to hyperkinesia. Symptoms similar to parkinsonism may also be induced by drugs that cause a reduction of dopamine in the brain, the most common of the drugs being phenothiazine derivatives. When drugs such as these are terminated, symptoms also quickly subside. Although a definite etiology has not been established, the most likely explanation is that the disease results from a combination of accelerated aging, genetic predisposition, exposure to toxins, and an abnormality in oxidative mechanisms.15,16 Clinical Manifestations Tremor, rigidity, bradykinesia, and postural instability are the cardinal features of parkinsonism and may be present in any combination. The tremor is most conspicuous at rest, is enhanced by emotional stress, and tends to be less severe during voluntary activity. Rigidity (an increase in resistance to passive movement) is responsible for the characteristically flexed posture seen in many patients. The most disabling symptoms are due to bradykinesia, manifested as a slowness of voluntary movement and a reduction in automatic movements such as the swinging of the arms while walking. The onset of the disease is generally insidious. Mild stiffness of the muscles of the extremities and tremor of the hands are frequently early signs. The typical hand tremor is often called a “pill-rolling” movement, characterized by the rubbing of the thumb against the fingers, and is particularly pronounced when the patient is otherwise at rest. The general stiffness progresses slowly until significant disability is noted by the patient. Walking becomes more difficult, and the patient develops a slow shuffling gait with a stooped position. As the ability to perform voluntary movements decreases, patients usually experience an inability to coordinate separate or independent movements. Many of the signs of Parkinson’s disease are found in the head and neck. The typical “masklike” facial appearance with infrequent blinking and lack of expression is caused by bradykinesis. The muscle rigidity also causes difficulty in swallowing, resulting in drooling. Speech becomes labored because of the lack of muscle control, and mandibular tremor results in masticatory difficulties, especially in those with removable dental appliances. Abnormalities in oral behavior, such as purposeless chewing, grinding, and sucking movements, are also well recognized in patients with Parkinson’s disease and make dental treatment especially difficult. Treatment Etiology and Pathogenesis MEDICAL MEASURES In idiopathic parkinsonism, dopamine depletion due to degeneration of the dopaminergic nigrostriatal system in the brainstem leads to an imbalance of dopamine and acetylcholine, neurotransmitters that are normally present in the corpus Drug treatment is often not required early in the course of parkinsonism. Patients with mild symptoms but no disability may be helped by amantadine. This drug improves all of the clinical features of parkinsonism, but its mode of action 598 Principles of Medicine is unclear. Anticholinergics are more helpful in alleviating tremor and rigidity than in alleviating bradykinesia, but these drugs have many side effects. Levodopa, a dopamine precursor that can cross the blood-brain barrier, improves all the major features of parkinsonism. This drug is used solely as replacement therapy for the underlying dopamine deficiency; it will neither halt nor reverse the degenerative process affecting brainstem neurons. Side effects associated with this drug therapy may be minimized by using a combination of levodopa and carbidopa. Carbidopa prevents the destruction of levodopa in the bloodstream, enabling lower (and therefore less toxic) dosages to be prescribed. Dopamine agonists act directly on dopamine receptors, and their use in the treatment of parkinsonism is associated with a lower incidence of the response fluctuations and dyskinesias that occur with long-term levodopa therapy. The two most widely used agonists are bromocriptine and pergolide, which are equally effective ergot derivatives. Pramipexole and ropinirol are two newer dopamine agonists that are not ergot derivatives; they are more selective, have fewer side effects, and may produce a longer-lasting response than the older ergot derivatives.17 ▼ HUNTINGTON’S DISEASE (HUNTINGTON’S CHOREA) GENERAL MEASURES, SURGICAL MEASURES, AND BRAIN STIMULATION Treatment Physical therapy or speech therapy can help many patients. Surgical procedures, such as thalamotomy or pallidotomy, may be helpful for patients who become unresponsive to medical treatment or who experience intolerable side effects from medications. Finally, high-frequency thalamic stimulation is effective in suppressing the rest tremor of Parkinson’s disease. Because electrical stimulation of the brain has the advantages of being reversible and of causing minimal or no damage to the brain, its use is being explored.17 Oral Health Considerations Patients with Parkinson’s disease can pose a multitude of challenges to the dental practitioner. Patients must often be treated in the upright position, making access to certain areas of the oral cavity difficult for the dentist. In addition, anxiety in a Parkinson’s disease patient can increase both the tremor and the degree of muscle rigidity. Due to dysphagia and an altered gag reflex, special precautions must be taken to avoid the aspiration of water or materials used during dental procedures. In patients who suffer with hypersialorrhea, maintaining a dry field in procedures that require such can be especially difficult.18 Xerostomia, on the other hand, is a common side effect of antiparkinsonism medications; the consequent root caries and recurrent decay must be diligently treated. Patients also often have difficulty maintaining their dentition because of their physical disability. For all of these reasons, more frequent recall may be necessary. When dental treatment is finished, the patient should be warned to take care when moving from a supine position to a standing position since levodopa has a significant orthostatic hypotensive effect. Huntington’s disease is a hereditary degenerative disease of the central nervous system, characterized by chorea (involuntary movements) and dementia. It is inherited in an autosomal dominant manner and occurs throughout the world and in all ethnic groups, with a prevalence rate of about 5 per 100,000. Clinical onset is usually between 30 and 50 years of age. The disease is progressive and usually leads to a fatal outcome within 15 to 20 years The gene responsible for the disease has been located on the short arm of chromosome 4.19 Clinical Manifestations The earliest manifestation of the disease consists of depression or irritability, coupled with a slowing of cognition. There are subtle changes in coordination and minor choreiform movements appear. The main clinical manifestation is progressively worsening choreic movements that can be observed in the face, tongue, and head. With time, the hyperkinesia becomes aggravated, and movements can become violent, with difficulty in speech and in swallowing. There is no cure for Huntington’s disease; progression cannot be halted, and treatment is purely symptomatic. Treatment is usually dependent on dopamine receptor blocking agents such as haloperidol and phenothiazines, which temporarily reduce the hyperkinesis and the behavior disturbances.19 Oral Health Considerations Dysphagia and choreic movement of the face and tongue will make dental treatment especially challenging. Sedation with diazepam may be considered. Whenever possible, dentures should be avoided because of the danger of fracture or the accidental swallowing of the dentures.18 ▼ CEREBRAL PALSY The term “cerebral palsy” refers to a group of disorders with motor manifestations due to nonprogressive brain damage occurring before or after birth. The incidence of cerebral palsy (CP) is 2 to 6 in every 1,000 live births. There are a multiplicity of causes of CP. Anoxia and ischemia during labor have been implicated, but congenital infections such as toxoplasmosis, rubella, Cytomegalovirus disease, herpes simplex, syphilis, and influenza have also been associated with CP or mental retardation.1,20 Clinical Manifestations The clinical manifestations of CP can be spastic, dyskinetic, ataxic, or a combination affecting one or all four limbs. The spastic forms of CP are the most common, and the legs are most commonly affected. Speaking problems are prevalent, with dysarthria, chewing, and swallowing difficulties. Drooling is both a functional and esthetic inconvenience. In hemiplegic 599 Neuromuscular Diseases cases of CP, the right side is more often involved. Sometimes, there are seizures associated with mental retardation. The dyskinetic type is characterized by athetotic purposeless movement, involving both agonist and antagonist muscles, that is increased by voluntary activity. During either natural or induced sleep, the movements cease. Head movements and facial grimacing are characteristic. One should not be misled by the appearance of the patient since most CP patients are intellectually normal. Treatment With improved perinatal care, both anoxia and perinatal infections have been markedly reduced, thus leading to a reduction in the incidence of CP. The key to success in the management of CP is teamwork and a planned approach to the individual child’s problem. Many children with CP have normal intelligence and should not be penalized because of dysarthria or involuntary movements. Physiotherapy should be instituted as early as possible in order to prevent contractures, and orthopedic surgery has been used occasionally with some degree of success.21 If the patient suffers from seizures, appropriate drug therapy is instituted (see “Epilepsy,” later in this chapter). Oral Health Considerations Children with CP show an increased incidence of enamel defects, the cause of which is not clear. A much more bothersome finding is the sialorrhea and drooling experienced by CP patients. This develops in the absence of orofacial and neck muscle coordination. One treatment, sialodocholoplasty (the relocation of salivary gland ducts into the tonsillar fossa and the removal of the sublingual salivary glands), has been shown to be effective.22 Less invasive management of sialorrhea includes a systemic medication such as glycopyrolate and anticholinergic agents.23 ▼ BELL’S PALSY Bell’s palsy is recognized as a unilateral paresis of the facial nerve. The dysfunction has been attributed to an inflammatory reaction involving the facial nerve. A relationship has been demonstrated between Bell’s palsy and the isolation of herpes simplex virus 1 from nerve tissues.24–26 Bell’s palsy must be differentiated from other causes of facial nerve palsy, including Lyme disease, herpes zoster of the geniculate ganglion (Ramsay Hunt syndrome), and tumors such as acoustic neuromas.27 Clinical Manifestations Bell’s palsy begins with slight pain around one ear, followed by an abrupt paralysis of the muscles on that side of the face. The eye on the affected side stays open, the corner of the mouth drops, and there is drooling. As a result of masseter weakness, food is retained in both the upper and lower buccal and labial folds. The facial expression changes remarkably, and the creases of the forehead are flattened. Due to impaired blinking, corneal ulcerations from foreign bodies can occur. Involvement of the chorda tympani nerve leads to loss of taste perception on the anterior two-thirds of the tongue and reduced salivary secretion. Treatment The only medical treatment that may influence the outcome is the administration of systemic corticosteroids within the first few days after the onset of paralysis, but this therapy should be avoided if Lyme disease is suspected. Combining steroids with antiherpetic drugs such as acyclovir may decrease the severity and length of paralysis.28 It is also helpful to protect the eye with lubricating drops or ointment and a patch if eye closure is not possible. When paralysis-induced eye opening is permanent, intrapalpebral gold weights are inserted, thus closing the upper eyelid. Facial plastic surgery and the creation of an anastomosis between the facial and hypoglossal nerves can occasionally restore partial function and improve appearance for patients with permanent damage. ▼ GUILLAIN-BARRÉ SYNDROME Guillain-Barré syndrome (acute idiopathic polyneuropathy)is an acute symmetrical ascending polyneuropathy, often occurring 1 to 3 weeks (and occasionally up to 8 weeks) after an acute infection. The Guillain-Barré syndrome often follows a nonspecific respiratory or gastrointestinal illness but has also been described after a few specific infections (such as with Cytomegalovirus, Epstein-Barr virus, Enterovirus, Campylobacter jejuni, or Mycoplasma) and after immunization. There is a worldwide incidence of 1.6 to 1.9 cases per 100,000 population per year.29 The disorder probably has an immunologic basis, but the precise mechanism is unclear. Clinical Manifestations The syndrome often begins with myalgia or paresthesias of the lower limbs, followed by weakness, which often ascends to involve abdominal, thoracic, and upper-limb muscles. In severe cases, respiration is compromised. Involvement of the autonomic nervous system by the disease process may induce changes in blood pressure and pulse rate. From an oral medicine perspective, the interesting feature of this disease is the fact that impaired swallowing or paresthesias of the mouth and face may be early signs of the disease. The seventh cranial nerve is frequently involved, and bilateral facial weakness is common. Involvement of other cranial nerves may result in ptosis or facial myokymia. Dysarthria, dysphagia and diplopia may develop in severe cases. Treatment and Prognosis The paralysis in Guillain-Barré syndrome may progress for about 10 days and may then remain relatively unchanged for about 2 weeks. The recovery phase is much slower and may take from 6 months to 2 years for completion. Permanent signs of neurologic damage can persist in some patients. Treatment with prednisone is ineffective and may actually affect the outcome adversely by prolonging recovery time. 600 Plasmapheresis is of value; however it is best performed within the first few days of illness and is best reserved for clinically severe or rapidly progressive cases.1 ▼ MYASTHENIA GRAVIS Myasthenia gravis (MG) is a disease characterized by progressive muscular weakness on exertion, secondary to a disorder at the neuromuscular junction. Acetylcholine normally transmits the impulse from nerve to muscle at the neuromuscular junction, and cholinesterase hydrolyzes acetylcholine. In patients with MG, autoantibodies that combine with and may destroy the acetylcholine receptor sites at the neuromuscular junction are present, preventing the transmission of nerve impulses to the muscle. The origin of the autoantibodies is unknown, but other findings linking MG to autoimmunity include the incidence of thymoma in MG patients, the improvement of symptoms after thymectomy, and the association of MG with other diseases involving abnormal immune phenomena, such as pemphigus, pemphigoid, systemic lupus erythematosus, and rheumatoid arthritis. The disease occurs more frequently in women than in men, particularly during the third and fourth decades of life.30 Clinical Manifestations The initial signs of this disease commonly occur in areas innervated by the cranial nerves (frequently, the eye muscles). Patients present with ptosis, diplopia, difficulty in chewing or swallowing, respiratory difficulties, limb weakness, or some combination of these problems. In some patients, the disease remains confined to the eye muscles, but in most cases, it progresses to other cranial nerves as well as to the shoulders and limbs. MG follows an unpredictable course, and exacerbations and remissions occur frequently. In severe advanced cases, respiratory difficulty arises. Diagnosis is made initially on the basis of clinical presentation. The inability of a patient to continually blink the eyes voluntarily is highly suggestive of MG. The clinical diagnosis can be confirmed by the dramatic improvement of symptoms with the administration of a short-acting anticholinesterase; it will antagonize the effect of cholinesterase on acetylcholine, allowing increased levels of this chemical at the neuromuscular junction. Specific tests for detecting the antiacetylcholine receptor antibody are now available for confirmation of diagnosis. Treatment Anticholinesterase drugs such as neostigmine and pyridostigmine bromide provide symptomatic benefit without influencing the course of the disease.30 In patients with more severe disease, remission may be achieved by thymectomy. In other cases, long-term cortico-steroids and immunosuppressive drugs are necessary. Plasmapheresis has been of temporary value in patients with severe exacerbations of MG. Principles of Medicine Oral Health Considerations Oral and facial signs are an important component of the clinical picture of MG. The facial muscles are commonly involved, giving the patient an immobile and expressionless appearance. This has led to the incorrect diagnosis of psychiatric disease in MG patients. Tongue edema may also be present in MG, making eating difficult for patients.31 Patients whose muscles of mastication are weakened can also experience consequent difficulty in chewing; these patients will be unable to finish chewing a bolus of food because of the easy fatigability of the muscles. It is essential to be aware that this may be an early sign of disease. The patient’s masticatory muscles may become so tired that the mouth remains open after eating. An important indication of MG is a patient who must hold his jaws closed with his hand. When treating known MG patients, the dentist must be aware that a respiratory crisis may develop from the disease itself or from overmedication. If a patient is at risk for developing a respiratory crisis, dental treatment should be performed in a hospital where endotracheal intubation can be performed. The airway must be kept clear because aspiration may occur in patients whose swallowing muscles are involved. Adequate suction and the use of a rubber dam are aids in these cases. The dentist should avoid prescribing drugs that may affect the neuromuscular junction, such as narcotics, tranquilizers, and barbiturates. Certain antibiotics, including tetracycline, streptomycin, sulfonamides, and clindamycin, may reduce neuromuscular activity and should be avoided. ▼ MUSCULAR DYSTROPHY Muscular dystrophy (MD) is a genetic disease characterized by muscle atrophy that causes severe progressive weakness. The primary biochemical defect has not been identified, but evidence is accumulating to implicate an enzymatic dysfunction at the muscle surface membrane. Clinical Manifestations The various forms of MD are genetically determined myopathies characterized by progressive muscular weakness and the degeneration of muscle fibers. The muscular dystrophies are classified according to mode of inheritance, age at onset, and clinical features. DUCHENNE’S MUSCULAR DYSTROPHY Duchenne’s muscular dystrophy is the most common form of MD and is seen almost exclusively in young males. This type of MD is a result of a mutation of the dystrophin gene located on the short arm of the X chromosome.32 Clinical manifestations begin during the first 3 years of life. Affected children appear normal at birth and may be extremely placid. Early signs are difficulty in walking, frequent falling, and the inability to run. Symptoms progress as muscles continue to atrophy. Initially, the atrophy is marked although muscles may appear even larger than normal, primarily because of the fat deposi- 601 Neuromuscular Diseases tion in the muscles. Pseudohypertrophy of muscles frequently occurs at some stage. Intellectual retardation is common, and there may be skeletal deformities, muscle contractures, and cardiac involvement. Serum levels of the enzyme creatine phosphokinase are elevated in affected males as well as in female carriers. At the end of the first decade of life, the child will be unable to walk and will be bedridden. Respiratory muscles will begin to be affected, and most patients die in the late teenage years or early twenties. A better understanding of pulmonary problems and improved treatment of respiratory infections have increased the life span of these patients. The muscles of the pelvis and femoral region are most severely affected by the Duchenne form of MD, but the muscles of the face, head, and neck are not involved. BECKER’S MUSCULAR DYSTROPHY Becker’s MD is a milder expression of the disease, caused by mutation of the dystrophin gene. There is a wide range of presenting symptoms that vary in severity from a slightly milder form of the disease resembling Duchenne’s MD to an asymptomatic elevation of creatine kinase. The age of onset is between 5 and 25 years, with a mean age of 11 years.32 The progression of Becker’s MD is slow, and patients may have a normal life span. FACIOSCAPULOHUMERAL DYSTROPHY Facioscapulohumeral dystrophy is inherited as an autosomal dominant trait and affects both males and females. Symptoms do not usually begin until the second decade of life. It is not as universally devastating as the Duchenne form of MD, and some patients may live a normal life span with minimal physical disability. The muscles of the face and pectoral girdle are most severely involved, and these patients characteristically exhibit weakness of the arms, winging of the scapulae, and weakness of the muscles of the eyes and mouth. LIMB-GIRDLE DYSTROPHY Limb-girdle MD is inherited, usually as an autosomal recessive trait; however, it may also be sporadically or dominantly inherited. It affects both sexes and has its onset in the second and third decades of life. The weakness starts in either the shoulders or the pelvis but will eventually spread to both. This is characteristically a slowly progressing form of MD. Facial muscles are not involved. MYOTONIC DYSTROPHY Myotonic dystrophy is a multisystem disorder inherited as an autosomal dominant trait through a locus on chromosome 19.1 The signs and symptoms may appear at any time from birth to the age of 40 years, and the disease is characterized by progressive muscular weakness, myotonia, cataracts, cardiac abnormalities, hypogonadism, and frontal balding. The most severe involvement occurs in the muscles of the head and neck and in the distal extremities. Myotonia is the persistence of the contraction of muscles; in this form of MD, the patient is unable to relax the muscles after contraction. This symptom can be best observed in the forearm, thumb, and tongue. Wasting of muscles and subsequent weakness are as prominent as in other forms of MD. Involvement of the facial muscles and hands is especially striking. Cardiac abnormalities may include a prolapsed mitral valve and atrial flutter; patients with more advanced cases have severe cardiac fibrosis.33 Treatment All forms of MD are incurable, and no satisfactory method of retarding the muscle atrophy exists. Corticosteroids have been shown to decrease the rate of muscle loss, but only in the short term. A physical therapy program will help to delay the development of joint contractures, and orthopedic procedures may help to counteract deformities. The ultimate outcome in severe forms of the disease is grave.34 Oral Health Considerations Oral and facial signs are prominent in the facioscapulohumeral and myotonic forms of MD. Patients with the myotonic-type disease develop severe atrophy of the sternomastoid muscles, with a resultant difficulty in the ability to turn the head. The muscles of facial expression and mastication are also commonly affected, such that the patient has difficulty in chewing or in pursing the lips. Weakness of the facial muscles and enlargement of the tongue due to fatty deposits has been occasionally observed. Patients with the oculopharyngeal form of the disease have significant difficulty in swallowing. Occlusal abnormalities have also been reported in patients with MD. This is thought to result from the lack of the proper muscle tension necessary to keep the teeth properly aligned in the dental arch. If the tongue is enlarged and the facial muscles are weak, the teeth will be pushed out. Other abnormalities include macroglossia, anterior open bite, and (occasionally) temporomandibular joint dysfunction. OCULOPHARYNGEAL MUSCULAR DYSTROPHY ▼ EPILEPSY A rare form of MD, oculopharyngeal MD is inherited as an autosomal dominant trait and is characterized by the late onset of chronically progressive ptosis and dsyphagia. Symptoms may begin at any age and consist of progressive weakness of levator palpebrae and chronic contraction of the frontalis muscle. The patient will maintain a chin-up head position and will have difficulty in swallowing solid food initially and liquids later. A late weakness of limb-girdle muscles may occur. Epilepsy is a condition characterized by abnormal, recurrent, and excessive neuronal discharges precipitated by many different disturbances within the central nervous system. These aberrant discharges may cause episodes of sensory and motor abnormalities as well as loss of consciousness. Each episode of aberrant neurologic activity is referred to as a seizure. Epilepsy is common, affecting approximately 0.5% of the population in the United States.35 Although the disease may occur at any 602 stage of life, the age of the patient at the onset of seizures is closely associated with the various causes of epilepsy. Infants are much more likely to suffer from epilepsy after complications at birth, such as anoxia, intracranial injury, metabolic disorders, and congenital malformations. Predominant causes in children and adolescents include trauma and acute or febrile infections whereas young adults who have engaged in alcohol or drug abuse commonly suffer from generalized seizures after periods of severe abuse. Epilepsy in older adults may occur as a complication of any of the previously mentioned causes but is more often associated with cerebrovascular diseases such as stroke and tumor. Classification of Seizures Seizures can be categorized in various ways, but the descriptive classification proposed by the International League Against Epilepsy is clinically the most useful. Seizures are divided into those that are generalized and those that affect only part of the brain (partial seizures)36 (Table 23-1). Simple partial seizures originate from one localized area of the brain and do not feature loss of consciousness. In contrast, complex partial seizures, often referred to as temporal lobe or psychomotor seizures, are associated with an impairment of consciousness. The majority of generalized seizures are called either absence (petit mal) seizures or tonic-clonic seizures (grand mal). The remaining generalized seizure types described in the classification (ie, myoclonic or infantile seizures and clonic, tonic, and atonic seizures) are usually found in childhood and carry a poorer prognosis for normal childhood development. “Status epilepticus” refers to a period of recurrent seizure attacks without recovery between each attack. All forms of seizure may progress to a period of status epilepticus. Clinical Manifestations Nonspecific changes such as headache, mood alterations, lethargy, and myoclonic jerking alert some patients to an impending seizure hours before it occurs. These prodromal symptoms are distinct from the aura that may precede a gener- TABLE 23-1 International Classification of Epileptic Seizures Partial (focal) seizures Simple partial seizures Complex partial seizures Partial seizures leading to secondarily generalized seizures Generalized Seizures Absence seizures Typical Atypical Myoclonic seizures Clonic seizures Tonic seizures Tonic-clonic seizures Atonic seizures (astatic seizures) Adapted from Kelley WN, DeVita VT Jr, Dupont HL, Harris Ed Jr. Internal medicine for dentistry. 2nd ed. Philadelphia: J.B. Lippincott; 1992. Principles of Medicine alized seizure by a few seconds or minutes and that is itself a part of the attack, arising locally from a restricted region of the brain. The most common type of seizure is the tonic-clonic or grand mal seizure; 90% of epileptics experience it alone or in combination with another type of seizure. A grand mal seizure characteristically begins with an aura. The aura may be experienced as epigastric discomfort, as an emotion, or as an hallucination of hearing, vision, or smell. The aura is followed seconds to minutes later by unconsciousness, a cry, and tonic muscle spasms; this rigid phase lasts about 30 seconds. Because of the spasm of the respiratory muscles, the patient does not breathe and becomes cyanotic during this period. The tonic phase is followed by a clonic phase composed of convulsive jerky movements, incontinence, and tongue biting (Figure 23-1). The patient may injure him- or herself seriously if he or she is near hard or sharp objects.A postictal state characterized by headache, confusion, lethargy, occasional temporary neurologic deficit, and deep sleep usually follows a grand mal seizure. The number, severity, and duration of grand mal seizures vary considerably from one patient to another. Status epilepticus, a severe form of the disorder, occurs when a series of seizures follow each other before the patient is able to regain consciousness. Absence or petit mal seizure is the second most common type of seizure, and it occurs without an aura and with few or no clonic or tonic movements. Absence seizures present almost exclusively in children and frequently disappear during the second decade of life. A single seizure lasts just seconds. The patient loses consciousness and appears to stare into space. He or she continues normal activity immediately after the seizure is over. Petit mal seizures may occur several times each day, and severe cases may interfere with school and social activities. Around puberty, approximately 50% of persons who experience petit mal seizures will develop tonic-clonic seizures. Treatment of Seizures For patients with recurring seizures, drug treatment is prescribed with the goal of preventing further attacks and is usually continued until there have been no seizures for at least 3 years.35 The drug with which treatment is best initiated depends on the type of seizures to be treated. The dose of the selected drug is gradually increased until seizures are controlled or until side effects prevent further increase. If seizures continue despite treatment at the maximal tolerated dose, a second drug is added. The second drug’s dose is increased, depending on the patient’s tolerance, and the first drug is then gradually withdrawn. In the treatment of partial and secondarily generalized tonic-clonic seizures, the success rate is higher with carbamazepine, phenytoin, or valproic acid than with phenobarbital or primidone. Gabapentin, topiramate, and lamotrigine are newer antiepileptic drugs that are effective adjunctive therapy for partial or secondarily generalized seizures. In most patients with seizures of a single type, satisfactory control can be achieved with a single anticonvulsant drug.37,38 The choice of medication is usually related to individual tolerance and efficacy, but it should be remembered that all of 603 Neuromuscular Diseases A B FIGURE 23-1 A, Bilateral human bites of the upper lip, received during an epileptic seizure. B, Traumatic injury (bite) to tongue occurred during an epileptic seizure. these drugs produce significant but different side effects, including blood dyscrasias, anemia, and alteration of hepatic function. Oral Health Considerations Patients with epilepsy may be treated in the private dental setting. A thorough medical history should indicate what type of seizures the patient has, how well the seizures are controlled, the frequency and duration of seizures, the potential triggers for seizures, and what to expect if the patient has a seizure. Treatment planning may be altered, however, depending on the status of the seizure disorder. As a general rule, it is better to place a fixed prosthesis rather than a removable appliance because of the potential for removable appliances to become dislodged during a seizure.39 Patients who are taking anticonvulsant drugs are subject to gingival overgrowth. This overgrowth is most often associated with patients who are taking phenytoin (Figure 23-2). About half of the patients placed on phenytoin will show evidence of gingival enlargement, usually within 2 to 18 months after starting the medication. The etiology is still unknown, but there appears to be an increase in the number of fibroblasts in the A connective tissues.40 Gingival overgrowth may occur at any age but seems to affect younger patients to a greater degree than adults. Men and women are equally affected. There does not appear to be a correlation between dosage and the incidence of gingival overgrowth. There is strong clinical evidence of a correlation between poor oral hygiene and the amount of tissue enlargement. Clinically, phenytoin gingival overgrowth starts in the interdental papillae and occurs only where teeth are present. The papillae enlarge buccally and lingually. The enlarged areas are firm, pink, and covered with normal mucosa. The severity of the hyperplasia varies. In some patients, the enlarged gingivae may involve just one or two papillae; in other cases, the crowns of the teeth are completely covered with gingival tissue. The best treatment of phenytoin gingival overgrowth begins with prevention. Little doubt remains that careful oral hygiene can prevent or at least minimize the gingival enlargement. Soon after being placed on anticonvulsant therapy, each patient should be referred to a dentist for oral hygiene instruction and gingival curettage. Patients who have not been properly managed and who develop gross gingival enlargement will require gingivectomy. Curettage B FIGURE 23-2 A, Phenytoin gingival overgrowth in a 17-year-old girl. The enlarged tissues are light pink and fibrous, and they show no evidence of edema, inflammation, or ulceration. B, Patient with phenytoin gingival overgrowth following electrocautery of enlarged gingival tissues. The excess maxillary gingival tissue had been removed 10 days previously. The excess mandibular gingival tissue had just been removed. Fractures of the mesioincisal angles of the maxillary first incisors occurred during a seizure. 604 and careful attention to oral hygiene must follow the surgery, or the hyperplastic tissue will return. It is known that side effects other than gingival overgrowth also occur in patients taking phenytoin. This includes megaloblastic anemia, hirsutism, and lymphadenopathy. Changes in connective tissue and bone (including osteomalacia, thickening of the heel pad and of the calvarium, and coarse facies) have also been reported.40 Routine dental treatment for patients with well-controlled epilepsy may be performed with no change from normal treatment. There is no reason to increase the dose of anticonvulsant therapy prior to dental treatment, and routine use of sedation is not indicated. ▼ REFERENCES 1. Gilroy J. Basic neurology. 3rd ed. New York: McGraw-Hill; 2000. 2. Adams HP Jr, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute ischemic stroke. Stroke 1996; 27:1711–8. 3. Wolf PA, Clagett GP, Easton JD, et al. Preventing ischemic stroke in patients with prior stroke and TIA: a statement for healthcare professionals from the stroke council of the American Heart Association. Stroke 1999;30:1991–4. 4. Victor M, Ropper AH. Adams and Victor’s principles of neurology. 7th ed. New York: McGraw-Hill; 2001. 5. Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of TIAs. From the Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks of the Stroke Council of the American Heart Association. Circulation 1994;89:2950–65. 6. Ostuni E. Stroke and the dental patient. J Am Dent Assoc 1994;125:721–7. 7. Kurtzke JF, Hellested K. Multiple sclerosis in the Faroe Islands: clinical and epidemiological features. Ann Neurol 1979;5:6. 8. Sadovnick AD, Ebers GC. Genetics in multiple sclerosis. Neurol Clin 1995;13:99–118. 9. Mumford CJ, Wood NW, Kellar-Wood H, et al. The British Isles survey of multiple sclerosis in twins. Neurology 1994;44:11–5. 10. Rudick RA, Cohen JA, Weinstock-Gutman B, et al. Management of multiple sclerosis. N Engl J Med 1997; 337:1604–11. 11. Chemaly D, Lefrancois A, Perusse R. Oral and maxillofacial manifestations of multiple sclerosis. J Can Dent Assoc 2000; 66:600–5. 12. Gale D, Prime S, Campbell MJ. Trigeminal neuralgia and multiple sclerosis, a complex diagnosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:398–401. 13. Houde SC, Mangolds V. Amyotrophic lateral sclerosis: a team approach to primary care. Clin Excell Nurse Prac 1999; 3(6):337–45. 14. Asher RS, Alfred T. Dental management of long-term amyotrophic lateral sclerosis: case report. Spec Care Dentist 1993;13(6):241–4. 15. Lang AE, Lozano AM. Parkinson’s disease. Part 1. N Engl J Med 1998;339:1044–53. Principles of Medicine 16. Lang AE, Lozano AM. Parkinson’s disease Part 2. N Engl J Med 1998;339:1130–43. 17. Olanow CW, Koller WC. An algorithm for the management of Parkinson’s disease: treatment guidelines. Neurology 1998;50(3 Suppl 3):S1–57. 18. Kieser J, Jones G, Borlase G. Dental treatment of patients with neurodegenerative disease. N Z Dent J 1999;95(422):130-4. 19. Quinn N, Schrag A. Huntington’s disease and other choreas. J Neurol 1998;245(11):709-16. 20. Bass N. Cerebral palsy and neurodegenerative disease. Curr Opin Pediatr 1999;11(6):504–7. 21. Dabney KW, Lipton GE, Miller F. Cerebral palsy. Curr Opin Pediatr 1997;9(1):81–8. 22. Becmeur F, Horta-Geraud P, Brunot B, et al. Diversion of salivary flow to treat drooling in patients with cerebral palsy. J Pediatr Surg 1996;31(12):1629–33. 23. Bachrach SJ, Walter RS, Trzcinski K. Use of glycopyrrolate and other anticholinergic medications for sialorrhea in children with cerebral palsy. Clin Pediatr 1998;37(8):485–90. 24. Murakami S, Mizobuchi M, Nakashiro Y, et al. Bell’s palsy and herpes virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med 1996;124:27–30. 25. Sanchez Rodriguez A. Bell’s palsy in association with herpes simplex virus infection. Arch Intern Med 1998;158(14):1577–8. 26. Nasatzky E, Katz J. Bell’s palsy associated with herpes simplex gingivostomatitis: a case report. Oral Surg Oral Med Oral Pathol 1998;86(3):292–6. 27. Billue JS. Bell’s palsy: an update on idiopathic facial paralysis. Nurse Pract 1997;22(8):88,97–100,102–5. 28. Adour KK. Bell’s palsy treatment with acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol 1996; 105:371–8. 29. Van der Meche FG, Aan Doorn PA, Meulstee J, et al. Diagnostic and classification criteria for the Guillain-Barre syndrome. Eur Neurol 2001;45(3):133–9. 30. Keesey J. Myasthenia gravis. Arch Neurol 1998;55(5):745–6. 31. Davison SP. Swollen tongue: a presentation of myasthenia gravis. Otolaryngol Head Neck Surg 1997;116(2):244–6. 32. Ptacek L. The familial periodic paralyses and nondystrophic myotonias. Am J Med 1998;104:58–70. 33. Arahata K. Muscular dystrophy. Neuropathology 2000 Sep; 20 Suppl:S34-41. 34. Urtizberea JA. Therapies in muscular dystrophy: current concepts and future prospects. Eur Neurol 2000;43(3):127–32. 35. Browne TR, Holmes GL. Epilepsy. N Engl J Med 2001; 344(15):1145–51. 36. Proposal for revised clinical classification of epileptic seizures. From the Commission on Class and Terminology of the International League Against Epilepsy. Epilepsia 1981; 22:489–501. 37. Bradie MJ, Dichter MA. Antiepileptic drugs. N Engl J Med 1996;334:168–75. 38. Mattson RH. Medical management of epilepsy in adults. Neurology 1998;51 Suppl 4:515–20. 39. Sanders BJ, Weddell JA, Dodge NN. Managing patients who have seizure disorders: dental and medical issues. J Am Dent Assoc 1995;126:1641–7. 40. Perlik F, Kolinova M, Zvarova J, et al. Phenytoin as a risk factor in gingival hyperplasia. Ther Drug Monit 1995;17(5):445–8.











© Copyright 2026