
Correspondence Malpractice claims: Outcome evidence Lawyers, litigation, and liability: Can they make
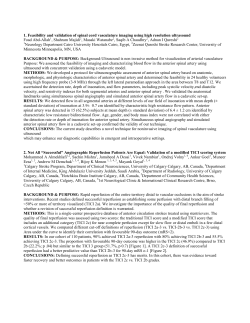
Correspondence Malpractice claims: Outcome evidence Lawyers, litigation, and liability: Can they make patients safer? To the Editor: The recent article by Glick1 and the accompanying cautionary editorial2 are quite interesting and provocative and are a timely reminder that the neurologist is not immune from lawsuits. Currently, there are a total of 18 million lawsuits per year in the United States and tort reform is just an illusion. Malpractice claims and settlements are indeed complex and thus, the information provided may be erroneous if used as a surveillance tool. For example, some of the largest awards in medical litigation have been made for neurologic impairment in children. Sympathetic awards seem to be based on the degree of plaintiff disability rather than evidence of negligence of culpable acts. Recent years have seen changes in our understanding of birth asphyxia and the epidemiology of cerebral palsy (CP) and most cases of CP are not due to birth asphyxia. In addition, no intervention including caesarean section has ever been shown to prevent CP.3 Thus, the presence of CP does not establish substandard medical care or that birth hypoxia occurred. Yet, undaunted by these facts, a handful of the same neurologic and obstetric experts are not deterred from testifying alleging negligence. Glick cites the Massachusetts malpractice experience (1989 – 1999), yet the prior review from Safran et al.4 from 1980 –1989 was more informative. They found that expert witness testimony for plaintiffs was by out-of-state neurologists, whereas defense experts were all from Massachusetts. Additionally, a panel review of plaintiff experts’ opinions was found to be inaccurate in 56%. Similar experiences in other large states have identified traveling expert witnesses, with good credentials, making marginal or pseudoscientific association that ultimately leads to junk justice.5 What can be done to lessen the effect of this thriving cottage industry who have several individuals advertising their credentials in various law journals? Thus, flawed expert testimony is a major problem that often leads to erroneous verdicts and needs to be addressed more vigorously by the American Academy of Neurology (AAN) and other specialty organizations. In January of 1998, the American Medical Association passed resolutions 121 and 216 indicating that expert witness testimony should be considered the practice of medicine and therefore subject to peer review and disciplinary sanctions. Thus, malpractice databases are not sensitive or specific in detection of medical errors as long as flawed expert testimony exists. Although there is a perception of fairness to this adversarial system, the reality is that many plaintiff attorneys know who to call for a specific opinion. A review of more than 150,000 closed claims (January 1985– December 1996)6 reveals that neurologists have the highest indemnity paid per file of all specialties ($216,724 vs $149,658). This alarming statistic, when critically analyzed, reveals that failure to diagnose, lack of informed consent, poor documentation, and poor doctor–patient relationships are major issues. There is often a fine line between negligent medicine and poor quality of care or inherent risks of disease. Malpractice database information is complex and often flawed. Neurologists should pause to consider that a physician’s behavior in developing strong doctor–patient relationships, as well as giving proper informed consent (especially with use of antiepileptic drugs, corticosteroids) and documentation, will reduce the chances of claims for negligence. Medical–legal information should be part of the education of residents and practitioners. Perhaps the time is right for the AAN to develop an instructional video, in conjunction with medical malpractice carriers, to be used in every residency program. This would be a useful first step in educating physicians about medical–legal problems. Michael I. Weintraub, MD, FACP, FAAN, Valhalla, NY Reply from the Author: My article1 attempted to stimulate further interest in neurologic adverse events, and Dr. Weintraub has responded, citing other work that is “more informative” to his 1738 NEUROLOGY 57 November (1 of 2) 2001 concerns. Indeed, other work is more relevant to issues of negligence, the tort system, expert witnesses, indemnification, and overall risk management, which I did not address, although these do challenge the neurologic profession. I intended, rather, to contribute to a process of establishing an epidemiology of neurologic errors and adverse outcomes that should help to inform educational objectives and priorities. The nub of the issue is the current limitations, which I emphasized, of malpractice claims databases and whether we can extract some useful information on neurologic, as opposed to legal, outcomes. I advocated further prospective research and analysis that might better separate the “wheat” of true adverse events from the “chaff” of litigation and judicial determination, and I do not believe that this process need wait for reform of the tort system or of standards for expert witnesses. There is a large amount of useful but unused data that could be accessed. I appreciate Dr. Weintraub’s suggestion that medical– legal education should be enhanced at the residency level. An even more fundamental goal, however, would be to heighten awareness of the sources of patient harm caused by error and strengthen commitments to participating in systematic prevention. Thomas H. Glick, MD, Cambridge, MA Reply from the Editorialists: We appreciate Dr. Weintraub’s comments. They certainly add to the reasons for why information contained within medical malpractice databases may not be highly predictive of medical error. As stated in our editorial,2 we fully agree with alternate educational approaches targeted toward neurology residents. These include teaching systems design and quality improvement, teaching multidisciplinary teamwork skills, facilitating open communication about adverse events and performance failures with colleagues, teaching communication skills, and promoting a culture of nonpunitive reporting. These suggestions only become more compelling given the Accreditation Council for Graduate Medical Education’s Outcome Project, which outlines six new core competencies for evaluating graduate medical trainees: patient care, practice-based learning and improvement, interpersonal of communication skills, professionalism, and system-based practice (http://www.acgme.org). The AAN and its Graduate Medical Education Subcommittee have an opportunity to take a national leadership role in implementing and evaluating these new competencies for graduating residents, two of which (interpersonal and communication skills and system-based practice) that have direct relevance to a safer and less litigious health care system. Robert G. Holloway, MD, MPH, Rochester, NY Copyright © 2001 by AAN Enterprises, Inc. References 1. Glick TH. Malpractice claims: outcome evidence. Neurology 2001;56: 1099 –1100. 2. Holloway RG, Panzer RJ. Lawyers, litigation and liability: can they make patients safer? Neurology 2001;56:991–993. 3. Nelson KB. The neurologically impaired child and alleged malpractice at birth. Neurol Clin 1999;17:283–293. 4. Safran A, Skydell B, Ropper S. Expert witness testimony in neurology: Massachusetts experience 1980 –1990. Neurol Chronicle 1992;2:1– 6. 5. Huber T. Galileo’s revenge: junk science in the court room. New York: Basic Books, 1991. 6. Medical Liability Mutual Insurance Company (MLMIC). Specialty bulletin, December 1997. Welding-related parkinsonism: Clinical features, treatment, and pathophysiology To the Editor: In the case-controlled study comparing 15 career welders with parkinsonism to a control group with idiopathic PD, Racette et al.1 concluded that parkinsonism among welders does not differ from idiopathic PD, except for an earlier age at onset. Welding, then, only unmasks PD in predisposed subjects. We would suggest, however, that some welders have parkinsonism that differs from idiopathic PD, and is due to a specific precipitant found in welding materials. Some welding applications employ steel–manganese alloys, and excessive exposure to manganese (Mn) can produce parkinsonism. Furthermore, at an early stage this parkinsonism may differ from idiopathic PD in several important ways. Later, however, it may be quite similar to idiopathic PD and hence may be categorized as early-onset idiopathic PD. Mn toxicity is typically associated with hyperintense signal abnormalities in the globus pallidus bilaterally on MRI.2 18 [ F]FDOPA PET scans are also typically normal, in contrast to PD; presumably because the disorder has a postsynaptic origin.3 Serum and urine Mn levels may be elevated. Finally, the clinical presentation of manganism includes general constitutional symptoms, cognitive disturbances, emotional liability, visual and auditory hallucinations, flight of ideas, and an akinetic–rigid syndrome with intermittent dystonic posturing of the limbs and sometimes severe dystonia of the trunk.4 Several findings in the patients of Racette et al.1 suggest that they did not happen to include cases of manganism. The seven reported MRI scans were normal or showed nonspecific changes in one. The two reported [18F]FDOPA scans revealed findings consistent with idiopathic PD, i.e., presynaptic changes. There was no reference to Mn levels. Finally, the clinical features did not include the other findings associated with manganism.5 Further complicating the study of PD in welders is the finding that manganism may progress, even after discontinued exposure to the toxin, so that the symptoms more closely resemble those of idiopathic PD. The characteristic MRI findings of manganism may also reverse. Thus, in an elderly population of welders, it may be difficult to distinguish persons with idiopathic PD from those with late-phase manganism. Welding, then, may unmask idiopathic PD as suggested by Racette et al.1; however, we would also suggest that at least one specific welding-associated etiology, manganism, can produce a form of secondary parkinsonism that at least early in the course has distinct clinical and laboratory features, though later it may be very indistinguishable from idiopathic PD. Ahmed H. Sadak, MD, Paul E. Schulz, MD, Houston, TX Reply from the Authors: We appreciate Sadek and Schultz’s interest in our article1 and their speculation that Mn exposure from welding may produce typical delayed-onset PD. However, we do not believe that our data provide evidence for their hypothesis, although we do agree that Mn toxicity may lead to progressive parkinsonism.6 It is important to appreciate the limitations of our findings. We identified subjects that appeared to have typical PD and yet retrospectively had exposure to welding. By this selection criteria, we would have excluded patients that began with atypical features such as those than occur with acute manganism. Thus, our group of welders with PD did not have historical evidence of magnanism or any condition beginning with atypical features followed by gradual progression to typically appearing PD. We did not obtain Mn levels in any of our patients, including six that were still welding at the time of diagnosis in our center. These patients also had no evidence of atypical parkinsonism, other features typical of manganism, or MRI evidence of manganism. Serial evidence of resolving MRI findings in these six patients would thus be not pertinent because they had no MRI abnormalities to resolve. Therefore, our study provides no support for the speculation of Drs. Sadek and Schultz that Mn toxicity from welding exposure may lead to delayed and progressive typical PD. Our study does represent the first detailed clinical investigation of welders with PD, suggesting that welding may act as an accelerant for the development of PD. We noted that our study was not an epidemiologic study and does not prove that welding causes PD, nor do we have data identifying the potentially toxic agent from welding exposure. We still believe that our data support our original conclusion that welding “acts as an accelerant to cause PD” and does not warrant further speculation. Brad A. Racette, MD, Joel S. Perlmutter, MD, St. Louis, MO Copyright © 2001 by AAN Enterprises, Inc. References 1. Racette BA, McGee–Minnich L, Moerlein SM, Mink JW, Videen TO, Perlmutter JS. Welding-related parkinsonism: clinical features, treatment, and pathophysiology. Neurology 2001;56:8 –13. 2. Nelson K, Golnick J, Korn T, et al. Manganese encephalopathy: utility of early magnetic resonance imaging. Br J Ind Med 1993;50:510 –513. 3. Wolters EC, Huang CC, Clark C, et al. Positron emission tomography in manganese intoxication. Ann Neurol 1989;26:647– 651. 4. Lee JW. Manganese intoxication. Arch Neurol 2000;57:597–599. 5. Huang CC, Chu NS, Lu CS, Chen RS, Calne DB. Long-term progression in chronic manganism: ten years of follow-up. Neurology 1998;50:698 – 700. 6. Lu CS, Huang CC, Chu NS, Calne DB. Levodopa failure in chronic manganism. Neurology 1994;44:1600 –1602. Why are stroke patients excluded from tPA therapy? An analysis of patient eligibility To the Editor: The report of Barber et al.1 of the exclusion of stroke patients from treatment with tissue plasminogen activator (tPA) raises some important issues for stroke physicians. The authors’ finding that a third of the patients excluded from tPA treatment based on clinical assessment of “mild” stroke severity or “improvement” ultimately had a poor outcome is of particular concern. We recently experienced an illustrative case. An 82-year-old woman presented to an affiliated hospital 20 minutes after the sudden onset of left hemiplegia and neglect. The emergency physician contacted the stroke fellow at our hospital after his examination for advice. A CT scan was performed and was reported negative. The treating physician was reluctant to proceed with tPA treatment after the CT scan because the patient had improved from complete paralysis to mild weakness on the left side. The patient was immediately transferred to our hospital for expert assessment. On arrival, she was conversant. Motor deficits were mild. However, she had gaze deviation, neglect, and hemisensory loss, with an NIH Stroke Scale (NIHSS) score of 12. MRI was contraindicated owing to pacemaker. Perfusion CT revealed an abnormality in the right temporal region and CT angiography (CTA) revealed occlusion of the inferior division of the right middle cerebral artery (MCA). IV tPA was administered. The next day, repeat CTA showed recanalization of the right MCA; her NIHSS score was 1. It has been our impression that emergency clinical assessment of stroke severity may be particularly problematic for patients with right-hemisphere syndromes without major motor deficits, such as the patient presented. Although the severity of the clinical deficits in right-hemisphere stroke may not be as immediately obvious as the dysphasia caused by left-hemisphere lesions, the resulting disability is at least as great.2 The NIHSS has a greater weighting for aphasia than neglect.3,4 For a given NIHSS score, the volume of right-hemisphere strokes on chronic CT is larger than the volume of left-hemisphere strokes.4 We have found that for 59 patients presenting with an NIHSS score 5 or less who had an MRI within 24 hours of stroke onset, the mean acute diffusionweighted MRI lesion volume for right-hemisphere strokes was 8.8 cm3, compared with 3.2 cm3 on the left (p ⫽ 0.04). We would be interested to know what proportion of the patients in the authors’ series who were excluded from treatment because of mild or improving deficits presented with right-hemisphere stroke, and whether right-hemisphere cases were overrepresented in the group with subsequent poor outcome. The inappropriate use of clinical exclusion criteria for tPA identified by the authors is of great concern. We believe that equal rigor must be used to ensure the inclusion of deserving patients for tPA treatment as that used to exclude those at greater risk of treatment complications. The current definition of “improving” stroke is too ambiguous. We agree with the authors that noninvasive neuroimaging techniques such as diffusion and perfusion MRI, MR angiography, CTA, or transcranial Doppler ultrasonography can be useful in making the decision to treat with tPA when there is uncertainty on clinical grounds alone. John N. Fink, FRACP, Magdy H. Selim, MD, PhD, Sandeep Kumar, MD, Gottfried Schlaug, MD, Boston, MA Reply from the Authors: We completely agree mild stroke and so called “neurologic improvement” are no guarantee of good recovery.1 Although a neurologic score may be suggestive of a mild stroke, the behavioral consequences can often be functionally disastrous. In the case described by Fink et al., a patient with a righthemisphere stroke improved (because the NIHSS score had declined) and this led to an initial decision not to treat the patient. The National Institute of Neurological Disorders and Stroke November (1 of 2) 2001 NEUROLOGY 57 1739 (NINDS) study is based on NIHSS scores, which can be unevenly low for right-hemisphere strokes (because the score is so dependent on language), i.e., a low score with right-brain involvement belies the severity of the stroke. Following transfer of this patient and sophisticated neuroimaging, the patient improved, but then a large perfusion deficit was discovered. The decision was reversed and treatment was given, because of the large perfusion deficit, resulting in an extremely good neurologic outcome. Therefore, the patient was treated, despite the improvement, based on persistent ischemia, rather than using the NINDS rules. There is an excess risk of symptomatic intracranial hemorrhage unless there is strict adherence to the NINDS criteria.5 By sticking to these rules, we have maintained low risks of intracerebral hemorrhage and have extended our single-center study of effectiveness to a national study (the Canadian Activase for Stroke Effectiveness Study [CASES]), which has now collected over 1,000 under-3-hour stroke patients who have been treated with TPA.6 As described in our article,1 we have become increasingly concerned about those patients who are excluded from TPA therapy based on the NINDS rules. We found that no fewer than one-third of patients who were denied treatment because the stroke was either too “mild” or the “neurologic score was improving” ended up either dead or dependent at 3 months. We would presume that they were at a relatively low risk of treatmentinduced intracerebral hemorrhage, but there is no randomized data that suggest that these patients would benefit from the intervention. Assuming that the risk is low or lower, we believe that these patients should be studied in a randomized, prospective trial. We, too, have been very impressed with the eloquence of the CT scan. The unenhanced scan provides a surrogate for diffusion MRI.7 Our scoring system, the Alberta Stroke Program Early CT Score (ASPECTS), has been used both in Calgary and throughout Canada to help predict those patients who are most likely to benefit.8 Randomizing patients based on an ASPECT score goes beyond the NINDS trial. It is our current thinking that by using the ASPECT score8 to minimize risk, we could break out of the so-called “NINDS box.” For those with a good ASPECT score, we could treat (or at least randomize to a new trial) patients beyond 3 hours, those who wake up with a deficit, or those who have an unknown time at onset. We would also propose that those patients who are judged to be either too mild or who are recovering (assuming the ASPECT score is good) might also benefit from intervention with low risks of hemorrhage. What is exciting about the report of Fink et al. is that it presages the use of a CT perfusion index (perhaps a P-ASPECT score) that will allow us to pick those patients who are too mild or who are improving but have a persistent ischemic attack with a transient neurologic deficit.9 We predict that perfusion CT and careful quantitation of unenhanced CT (ASPECTS) will allow us to design trials that are more inclusive, affording safe TPA therapy to more patients with stroke. At the end of the day, it is our contention that we are excluding far too many stroke victims from TPA therapy and feel that our study of patient eligibility might predict what a new more inclusive trial might look like.1 8. Barber PA, Demchuk AM, Buchan AM, for the ASPECTS Study Group. Validity and reliability of a quantitative computed tomography score predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet 2000;355:1670 –1674. 9. Buchan AM. Aspects of stroke imaging. Can J Neurol Sci 2001;28:99 – 100. Bilateral movement enhances ipsilesional cortical activity in acute stroke: A pilot functional MRI study To the Editor: We read with great interest the article by Staines et al.,1 which reported functional MRI findings in two patients with stroke during unilateral and bilateral hand movement. In the early stages, bilateral movement enhanced activation in the primary motor cortex of the affected hemisphere compared with unilateral paretic hand movement. However, at later stages, activation of the affected hemisphere did not differ between unilateral and bilateral movement. This was not due to decreased activation with bilateral movement, but to increased activation with movement of the paretic hand as recovery progressed. We obtained analogous results in a group of 30 patients with hemiplegic stroke (19 men and 11 women; mean age 64.9 ⫾ 11.9 years) making use of transcranial Doppler ultrasonography (TCD). Our patients were examined within the first week (T1), 1 month (T2), and 6 months after stroke (T3). Blood flow velocities in both middle cerebral arteries were measured with TCD while they performed a 2-minute sequential thumb-to-finger opposition task. Changes in mean flow velocity (MFV) were taken as indices of cerebral activation. As we have previously reported,2 the response of the damaged side to contralateral movement (paretic hand) was low at T1 and T2, but increased with time and reached a normal pattern (similar to that of healthy controls) at T3. Additionally, we compared the response of the affected hemisphere to bilateral movement with the response to contralateral movement in the same patients (unpublished data). At T1, the MFV increment with bilateral movement (mean ⫾ SD, 8.14 ⫾ 8.97%) was higher than the increment with affected hemisphere during early stages of stroke. This phenomenon could be related to interhemispheric influence that takes place when both hands move simultaneously.4 It would be very interesting to analyze whether bilateral motor tasks can improve recovery of the paretic limb during stroke rehabilitation.5 M.L. Cuadrado, PhD, J.A. Arias, PhD, Madrid, Spain Reply from the Authors: We appreciate the interest of Drs. Cuadrado and Arias in our study. These authors have previously used TCD to measure blood flow velocities in the middle cerebral artery of the stroke-affected hemisphere in hemiplegic stroke patients performing finger-to-thumb opposition tasks with the affected hand.2 Compared with the healthy hemisphere, flow velocity in the middle cerebral artery of the stroke-affected hemi- Alastair M. Buchan, MD, Calgary, Alberta, Canada Copyright © 2001 by AAN Enterprises, Inc. References 1. Barber PA, Zhang J, Demchuk AM, Hill MD, Buchan AM. Why are stroke patients excluded from TPA therapy? An analysis of patient eligibility. Neurology 2001;56:1015–1020. 2. Ween JE, Alexander MP, D’Esposito M, Roberts M. Factors predictive of stroke outcome in a rehabilitation setting. Neurology 1996;47:388 –392. 3. Brott T, Adams HP, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989;20:864 – 870. 4. Woo D, Broderick JP, Kothari RU, et al. Does the National Institutes of Health Stroke Scale favor left hemisphere strokes? Stroke 1999;30:2355– 2359. 5. Buchan AM, Barber PA, Newcommon N, et al. Effectiveness of t-PA in acute ischemic stroke: outcome relates to appropriateness. Neurology 2000;54:679 – 684. 6. Hill MD, Lawrence K, Buchan AM. Canadian Activase for Stroke Effectiveness Study (CASES): a multi-stakeholder collaboration. Can J Neurol Sci 2001;28:232–238. 7. Barber PA, Demchuk AM, Hill MD, et al. A comparison of CT versus MR imaging in acute stroke using ASPECTS: will the “new” replace the “old” as the preferred imaging modality? Stroke 2001;32:325. Abstract. 1740 NEUROLOGY 57 November (1 of 2) 2001 Figure. Bar graph showing percentage of changes during unilateral (paretic hand; white bars) and bilateral (both hands; gray bars) movement on the damaged side in stroke patients at T1 (acute stage). T2 (subacute stage), and T3 (chronic stage). Data are presented as mean ⫾ SEM. n.s. ⫽ Nonsignificant. sphere was decreased at 1 week and 1 month poststroke, but near normal by 6 months. Here, they report data from 30 patients showing that bilateral movement enhances mean flow velocity in the middle cerebral artery of the stroke-affected hemisphere early after stroke. As the authors point out, this is a clear demonstration that observations using different but complementary techniques (TCD and fMRI) are converging to the same conclusion. fMRI is sensitive to changes in deoxyhemoglobin concentration, providing a blood oxygen level– dependent (BOLD) response from which neural activity is inferred. Along with oxygen extraction fraction and blood volume, blood flow velocity is a crucial component to observed changes in fMRI signal intensity. Although the two techniques are maximally sensitive at different vascular diameters, it may be possible in the future to combine TCD and fMRI to determine what component of the observed BOLD changes are attributable to flow velocity changes at the level of capillaries, arterioles, and venules. Data from our study and that of Cuadrado and Arias provide evidence of possible interhemispheric influences on cortical motor reorganization early after stroke. Based on a previous report6 showing disinhibition of regions surrounding a primary motor cortical infarct, one may have expected increased neuronal activity associated with unilateral movement early after stroke. However, the two patients reported in our study both had lesions that involved nonprimary motor regions and largely spared the primary motor cortex. This may have resulted in a loss of inputs that modulate the background activity levels of GABAergic interneurons within the primary motor cortex, rendering them overactive. Activity of contralesional motor regions may then have modulated activity within the ipsilesional cortex. A recent publication7 demonstrated the importance of GABA in the primary motor cortex for short-term, practice-dependent plasticity. Future work combining multiple functional neuroimaging techniques with transcranial magnetic stimulation and analyses of specific lesion locations in patients who show facilitation with bilateral movement may provide better insight into the specific mechanisms underlying these interhemispheric relationships in recovery from stroke. W. Richard Staines, PhD, William E. McIlroy, PhD, Simon J. Graham, PhD, Sandra E. Black, MD, Toronto, Ontario, Canada Copyright © 2001 by AAN Enterprises, Inc. References 1. Staines WR, McIlroy WE, Graham SJ, Black SE. Bilateral movement enhances ipsilesional cortical activity in acute stroke: a pilot functional MRI study. Neurology 2001;56:401– 404. 2. Cuadrado ML, Egido JA, González–Gutiérrez JL, Varela-de-Seijas E. Bihemispheric contribution to motor recovery after stroke: a longitudinal study with transcranial Doppler ultrasonography. Cerebrovasc Dis 1999; 9:337–344. 3. Stroemer RP, Kent TA, Hulsebosch CE. Neocortical neural sprouting, synaptogenesis, and behavioral recovery after neocortical infarction in rats. Stroke 1995;26:2135–2144. 4. Eliassen JC, Baynes K, Gazzaniga MS. Anterior and posterior callosal contributions to simultaneous bimanual movements of the hands and fingers. Brain 2000;123:2501–2511. 5. Mudie MH, Matyas TA. Can simultaneous bilateral movement involve the undamaged hemisphere in reconstruction of neural networks damaged by stroke? Disabil Rehabil 2000;22:23–37. 6. Liepert J, Stroch P, Fritsch A, Weiller C. Motor cortex disinhibition in acute stroke. Clin Neurophysiol 2000;111:671– 676. 7. Ziemann U, Muellbacher W, Hallett M, Cohen LG. Modulation of practice-dependent plasticity in human motor cortex. Brain 2001;124: 1171–1181. Relative pupil-sparing third nerve palsy: Etiology and clinical variables predictive of a mass To the Editor: We read with great interest the article by Jacobson1 concerning relative pupil-sparing third nerve palsy. He reports that compressive mass lesions were a common cause of relative pupil-sparing third nerve palsy. We performed brain MRI and MR angiography in 3366 patients between April 2000 and March 2001. Among those patients, we also encountered one unique patient who had pupil-sparing third nerve palsy caused by an intracavernous carotid artery aneurysm. We would like to dis- cuss this patient and the mechanism of pupillary sparing by mass lesions compressing the oculomotor nerve. A 95-year-old woman with hypertension and diabetes mellitus was diagnosed with diabetic external ophthalmoplegia in the right eye 5 years before. Her oculomotor symptoms progressed gradually. Recently, she developed headache and complete ptosis in the right eyelid. Neuro-ophthalmological examination revealed severe degree of third nerve palsy without pupil involvement in the right eye. Her pupils were 2.0 mm in equal size. Light reactions were normal in both eyes. Other neurologic examination remains normal. Brain MRI and MR angiography disclosed a giant aneurysm (2.8 cm in diameter) in the right anterior cavernous sinus. Jacobson1 suggests that compressive mass lesions cause relative pupil-sparing third nerve palsy, in addition to third nerve infarction. Our patient had a giant aneurysm in the anterior cavernous sinus. Duration of external ophthalmoplegia in our patient was 5 years. We speculate that slow, expanding mass lesions compressing the oculomotor nerve contribute to pupil-sparing third nerve palsy. Several of Jacobson’s patients also had slow, enlarging mass lesions such as intracavernous carotid artery aneurysms and parasellar meningioma. Nineteen of his patients were evaluated within 3 weeks from the initial symptom. We would like to know the duration of third nerve palsy in his 10 patients with mass lesions. Another report indicates that a 69year-old woman had isolated oculomotor superior division palsy caused by a large aneurysm in the anterior portion of the cavernous sinus.2 In compressive third nerve palsy, the topographic relationship and the degree of compression between the parasympathetic pupilloconstricutor fibers of oculomotor nerve and mass lesions might play a crucial rule in the mechanism of pupillary sparing. Otherwise, ischemic damage could induce pupil-sparing third nerve palsy in patients with third nerve infarction or diabetes mellitus. We would also like to know the age of Jacobson’s patients with mass lesions. Our patient was 95-years-old. It is suspected that pupil-sparing third nerve palsy by compression may occur in older patients, in comparison with younger patients. Our patient had a history of hypertension and diabetes. In senile patients with persistent pupil-sparing third nerve palsy, we should cautiously evaluate mass lesions compressing the oculomotor nerve using MRI and MR angiography, although those patients have vascular risk factors. K. Ikeda, MD, PhD, M. Tamura, MD, Ohashi; Y. Iwasaki, MD, M. Kinoshita, MD, Tokyo, Japan Reply from the Author: I thank Ikeda et al. for their interest in my paper. For clarification, I indicated in the Results section that “all but five patients were evaluated within 3 weeks from first symptoms.” This result referred to the entire study population, Table Clinical features of 10 patients with mass lesions compressing the oculomotor nerve and causing relative pupilsparing third nerve palsy Patient No. Age, y/sex Duration of symptoms 1 75/M 3 wk Prostate metastasis 2 76/F 2 wk Meningioma 3 58/F 3 wk Intracavernous carotid artery aneurysm 4 87/F 1.5 y Dolichoectatic intracavernous carotid artery 5 83/F 8y Meningioma 6 59/M 5 mo Metastasis of unknown origin 7 88/F 3 wk Lymphoma 8 64/M 2d Plasmacytoma Etiology 9 69/M 8d Prostate metastasis 10 64/F 2 wk Lung metastasis November (1 of 2) 2001 NEUROLOGY 57 1741 not just those with mass lesions. The information requested is summarized in the table. Daniel M. Jacobson, MD, Marshfield, Wisconsin Copyright © 2001 by AAN Enterprises, Inc. References 1. Jacobson DM. Relative pupil-sparing third nerve palsy: etiology and clinical variables predictive of a mass. Neurology 2001;56:797–798. 2. Silva MN, Saeki N, Hirai S, Yamaura A. Unusual cranial nerve palsy caused by cavernous sinus aneurysms: clinical and anatomical considerations reviewed. Surg Neurol 1999;52:143–149. Serial MR angiography and contrast-enhanced MRI in chickenpox-associated stroke To the Editor: I appreciated the interesting report by Singhal et al.1 of a case of uncomplicated chickenpox followed 4 months later by right putamenal infarction. MR angiography convincingly demonstrated stenoses of the right middle cerebral artery and distal right internal carotid artery. The authors acknowledge the probable relationship of such chickenpox-associated stroke to the syndrome of herpes zoster ophthalmicus with delayed contralateral hemiplegia, and, except for the patient’s age, their case can be closely compared, even angiographically, with my own report of almost 30 years ago.2 In their case as in mine, virtually the same segment of the distal internal carotid artery appears to have been involved. With the recent impetus to childhood varicella immunization, it is to be hoped and expected that such cases will become increasingly rare, so that future generations will be spared not only chickenpox but herpes zoster, including herpes zoster ophthalmicus with delayed contralateral hemiparesis. In addition, I believe that the speculations in my 1974 article relating herpes zoster to the syndrome of granulomatous angiitis of the central nervous system remain viable, suggesting that varicella immunization may also achieve a progressive suppression of the latter disease. Gordon J. Gilbert, MD, St. Petersburg, FL Copyright © 2001 by AAN Enterprises, Inc. References 1. Singhal AB, Singhal BS, Ursekar MA, et al. Serial MR angiography and contrast-enhanced MRI in chickenpox-associated stroke. Neurology 2001;56:815– 817. 2. Gilbert GJ. Herpes zoster ophthalmicus and delayed contralateral hemiparesis. Relationship of the syndrome to central nervous system granulomatous angiitis. JAMA 1974;229:302–304. Vitamin B12 and folate in relation to the development of Alzheimer’s disease To the Editor: We read with interest the article by Wang et al.1 on the association of low serum levels of vitamin B12 and folate with AD occurrence. We think that it is difficult to establish a clinical diagnosis of AD in patients with deficiency of vitamin B12 or folate. AD in this situation could be hardly differentiated from other kinds of dementia, particularly from dementia associated with B12 deficiency and vascular dementia. Cobalamin (vitamin B12) is a cofactor in several metabolic pathways, and its deficiency may be associated with dementia. The authors have controlled the hemoglobin levels. Nevertheless, the dementia caused by vitamin B12 deficiency may not be accompanied by anemia. Dementia may be the sole manifestation of cobalamin deficiency.2 The most important pathway in the nervous system that is adversely affected by cobalamin deficiency involves the conversion of homocysteine to methionine. Demyelination clearly plays a major role in the neuropathogenesis of cobalamin deficiency, and cognitive changes can occur as a result of central demyelination.3 Furthermore, it was recently shown that high levels of homocysteine are associated with poor word recall in the elderly.4 High homocysteinemia can be caused by deficiencies of folate or vitamin B12. Another issue to be considered refers to the differentiation of vascular dementia. Elevated plasma levels of homocysteine have been implicated recently as a risk factor for atherosclerosis and stroke. Homocysteine may be directly toxic to endothelium or may be thrombogenic. Patients with vascular dementia were found to have significantly higher homocysteinemia, a potentially contrib1742 NEUROLOGY 57 November (1 of 2) 2001 uting factor. Elevated plasma homocysteine levels increase the risk of silent brain infarction in the elderly.5 The results of the neurologic examination in a patient with vascular dementia may be unremarkable. The Hachinski Ischemic Scale has been used in this study. However, no imaging study was performed. The cognitive disorder of vascular dementia itself is heterogeneous and may take several different forms. The pleomorphic nature of vascular dementia contributes to diagnostic problems. Although determination of the serum level of vitamin B12 is the principal diagnostic test for cobalamin deficiency, this test is neither completely sensitive nor specific. We think that additional testing for evidence of deficiency should be performed in patients with low levels of vitamin B12 in that situation, such as measures of homocysteine and methylmalonic acid levels. We think that the relation between vitamin B12 and folate and the development of AD is not yet established. Carlos R.M. Rieder, MD, PhD, Daniele Fricke, MD, Porto Alegre, RS, Brazil Reply from the Authors: We thank Rieder and Fricke for their interest in our study. Their letter made three main points: 1) diagnostic difficulty in differentiating AD from dementia due to B12 deficiency; 2) possible inclusion of vascular cases in the AD group, which may explain the association between vitamin deficiency and neurodegenerative dementia; and 3) inaccuracy of serum B12 level as clinical marker of tissue B12 deficiency. Although we agree with Rieder and Fricke on the relevance of the first two points, we are still convinced that the low sensitivity and specificity of serum B12 level does not invalidate our results, as was extensively discussed in our article.1 Regarding the first point, we agree that it is difficult to establish a clinical diagnosis of AD in patients with low vitamin B12 or folate levels. Indeed, in the absence of other neurologic or nonneurologic manifestations of vitamin deficiency, only biopsy may help to differentiate AD cases from dementia caused by B12 deficiency. With this problem in mind, all the clinical diagnoses in our study were made by physicians who carefully evaluated all causes of dementia and excluded any systemic conditions. In addition, to improve the quality of our diagnosis, we adopted a double diagnostic procedure, in which two senior clinicians were involved.1,6 In response to the second comment, we acknowledge that it is more than likely that our clinical-based AD diagnoses are contaminated by mixed cases. However, our findings remained unchanged after taking into account all vascular diseases. Further, neuroimaging would only have partially solved the problem of misclassification of mixed cases in the AD group. Given the observational nature of our study, we cannot identify whether B12 deficiency is involved in the neurodegenerative mechanisms, or if it is acting through vascular mechanisms, which may accelerate the clinical expression of AD.7 Our population-based study can only suggest that vitamin B12 and folate may be related to the development of clinicallydiagnosed AD and dementia. Even when a cut-off of 250 pmol/L was used to define low levels of B12, an increased risk of clinicallydiagnosed AD was found. This definitely indicates the importance of monitoring vitamin B12 and folate levels in the elderly. Additional observational studies confirming our findings with clinical and experimental investigations exploring these possible mechanisms underlying the reported associations, are warranted. H.X. Wang, A. Wahlin, H. Basun, J. Fastbom, B. Winblad, and L. Fratiglioni, Stockholm, Sweden Copyright © 2001 by AAN Enterprises, Inc. References 1. Wang HX, Wahlin A, Basun H, Fastbom J, Winblad B, Fratiglioni L. Vitamin B12 and folate in relation to the development of Alzheimer’s disease. Neurology 2001;56:1188 –1194. 2. Goebels N, Soyka M. Dementia associated with vitamin B(12) deficiency: presentation of two cases and review of the literature. J Neuropsychiatry Clin Neurosci 2000;12(3):389 –394. 3. Chatterjee A, Yapundich R, Palmer CA, et al. Leukoencephalopathy associated with cobalamin deficiency. Neurology 1996;46:832– 834. 4. Morris MS, Jacques PF, Rosenberg IH, Selhub J. Hyperhomocysteinemia associated with poor recall in the third National Health and Nutrition Examination Survey. Am J Clin Nutr 2001;73:927–933. 5. Matsui T, Arai H, Yuzuriha T, et al. Elevated plasma homocysteine levels and risk of silent brain infarction in elderly people. Stroke 2001; 32:1116 –1119. 6. Fratiglioni L, Grut M, Forsell Y, et al. Clinical diagnosis of Alzheimer’s disease and other dementia in a population survey. Agreement and causes of disagreement in applying DSM-III-R criteria. Arch Neurol 1992;49:927–932. 7. Snowdon DA, Greiner LH, Mortimer JA, Riley KP, Greiner PA, Markesbery WR. Brain infarction and the clinical expression of Alzheimer disease. The Nun Study. JAMA 1997;277:813– 817. Cerebrotendinous xanthomatosis To the Editor: We read with interest the NeuroImage report,1 Letter to the Editor,2 and Reply from the Authors3 on chenodeoxycholic acid (CDCA) treatment in cerebrotendinous xanthomatosis (CTX). We followed 20 CTX cases,4 most of whom are receiving CDCA treatment and are neurophysiologically evaluated.5 An 11-year neurophysiologic follow-up in five patients indicated improvement in nerve condition velocities, as well as visual- and motor-evoked potentials (personal data). In our experience, CDCA clinically stabilizes CTX, arresting the progression that is evident in untreated cases. However, as reported by Somenuk and Koffman,2 in Italy we had difficulty prescribing CDCA because it has not been commercially available since 1997. In collaboration with the pharmaceutical unit of our hospital, we ordered CDCA from Industria Chimica Emiliana (ICE), Reggio Emilia, and produced 250 mg caps that we supplied directly to patients, enabling them to continue therapy. This also allowed us direct control of drug intake and its efficacy from the clinical and biochemical point of view. We agree with Dr. Salen on the inefficacy of ursodeoxycholic acid treatment.3 Antonio Federico, MD, and Maria Teresa Dotti, MD, Siena, Italy Reply from the Authors: Until further data are published, chenodeoxycholic acid will remain the treatment of choice for cerebrotendinous xanthomatosis. We are pleased to hear that our colleagues in Italy have found a manufacturer willing to supply them with it. James D. Fleck, MD, Indianapolis, IN Copyright © 2001 by AAN Enterprises, Inc. References 1. Fleck JD, Biller J, Mathews VP. Cerebrotendinous xanthomatosis. Neurology 2000;55:601. 2. Samenuk P, Koffman BM. Re: Chenodeozycholic treatment of cerebrotendinous xanthomatosis. Neurology 2001;56:695– 696. Letter. 3. Salen G. Re: Chenodeoxycholic acid treatment of cerebrotendinous xanthomatosis. Neurology 2001;56:695– 696. Letter. 4. Federico A, Dotti MT. Cerebrotendinous xanthomatosis. In: Vinken PJ, Bruyn GW, eds. Handbook of clinical neurology. Amsterdam: Elsevier, 1996, 599 – 613. 5. Mondelli M, Rossi A, Scarpini C, Dotti MT, Federico A. Evoked potentials in cerebrotendinous xanthomatosis and effect induced by chenodeoxycholic acid. Arch Neurol 1992;49:469 – 475. November (1 of 2) 2001 NEUROLOGY 57 1743











© Copyright 2026