
Read article here - USC Annenberg School for Communication and
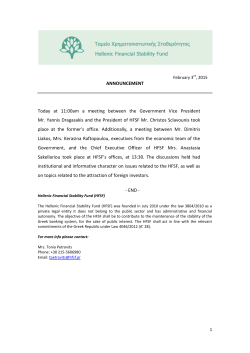
A Discourse of Relationships in Bioethics: Patient Autonomy and End-of-Life Decision Making among Elderly Korean Americans Author(s): Gelya Frank, Leslie J. Blackhall, Vicki Michel, Sheila T. Murphy, Stanley P. Azen, Kyeyoung Park Reviewed work(s): Source: Medical Anthropology Quarterly, New Series, Vol. 12, No. 4 (Dec., 1998), pp. 403-423 Published by: Blackwell Publishing on behalf of the American Anthropological Association Stable URL: http://www.jstor.org/stable/649596 . Accessed: 08/03/2012 14:22 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Blackwell Publishing and American Anthropological Association are collaborating with JSTOR to digitize, preserve and extend access to Medical Anthropology Quarterly. http://www.jstor.org GELYAFRANK Department of Occupational Science and Occupational Therapy and Department of Anthropology University of Souther California LESLIEJ. BLACKHALL Pacific Center for Health Policy and Bioethics and Assisted Home Hospice Thousand Oaks, CA VICKI MICHEL Loyola Law School Los Angeles, CA SHEILAT. MURPHY Annenberg School for Communication and Department of Psychology University of Southern California STANLEYP. AZEN Department of Preventive Medicine, School of Medicine University of Southern California KYEYOUNGPARK Department of Anthropology University of California at Los Angeles A Discourse of Relationships in Bioethics: Patient Autonomy and End-of-Life Decision Making among Elderly Korean Americans A two-year, multidisciplinary study (N = 800) was conducted on attitudes about end-of-life decision making among elderly individuals in four ethnic groups (African American, European American, Korean American, and Mexican American). On a quantitative survey, Korean Americans reported negative attitudes about the use of life-sustaining technology for themselves butpositive attitudes about its use in general. This article reports on an interview with a 79-year-old typical Korean American respondent to explain the contradiction in the survey data. Expectations among elderly Korean Americans include protecting family members with a life-threatening illness from being informed of their diagnosis and prognosis, and doing everything to keep them alive. Two conclusions, one substantive and the other methodological, are drawn: First, the bioethics discourse on individual rights (patient MedicalAnthropology Association. Quarterly12(4):403-423.Copyright? 1998AmericanAnthropological 403 404 MEDICAL ANTHROPOLOGY QUARTERLY autonomy) is insufficientto explain the preferences of many Korean Americansand must be supplementedwith a discourseon relationships. Second,the rigoroususe of qualitative,narrativemethodsclarifies quantitativedata and should not be dismissedas "anecdotal."[bioethics,endof-life decision making,ethnicity,Asian Americans,qualitativemethods, narrative] I amtheonewhois goingto die;so I don'tcontrolthesituation. -Mrs. Kim,79 yearsold,KoreanAmerican immigrant lthoughpatientautonomyhas been the dominantprinciplein bioethics in the United States for the past 25 years,consensusaboutits overridingimportanceis beginning to crumble.' Researchershave begun to recognize thatthe reigningconceptualizationof autonomyis limitedandillusory,andthatsocial relationshipsmay presentan equally and sometimesmore compelling frameworkfor bioethicsthanindividualrights(Callahan1996; Gaylin 1996; Gaylin and Jennings 1996).2Empiricalresearchby medical anthropologistshas contributed supportfor such critiques.For example, not all patientsexpect or want full disclosureabouttheircondition,andmanyprefertheirfamiliesto receiveandmanagesuch information (Goodet al. 1993;Gordon1994;GordonandPaci1997;Oronaet al. 1994). Expectationsaboutpatientautonomymay cause confusion for some patients when theirphysician,an expert,solicits theiropinion (Barneset al. 1994; Koenig andMarshall1994; Marshallet al. 1998). The mere suggestionof an aggressiveor invasivetreatmentoption such as mechanicalventilationmay be interpretedby patientsandtheirfamilies as a sign of hope: Why else, theyreason,would a doctorinflict pain?Moreover,patientsmay not explaintheirillness primarilyor exclusively in termsof Westernbiomedicine.In traditionalsocieties aroundthe world, illness and disability are commonly attributedto factors such as a breach in social relationshipssurroundingthe patientor supernaturalcauses. Such beliefs have implications for treatmentthat may conflict with biomedical procedures.3Consequently, clinicians often need a better fit between North American bioethics principlesand the preferencesand decision-makingstyles of the diverse patients they serve (Barker 1992; Davis and Koenig 1996; Koenig and Gates-Williams 1995;Marshall1992; Marshallet al. 1994; Muller 1994). In the short history of bioethics as a discipline in the United States, patient autonomyearnedits centralrole as a reactionto physicianpaternalism(Rothman 1991). It seems clearthatpatientsarebettersituatedthanphysiciansto evaluatethe appropriatenessof available medical treatmentsin relation to their life circumstances. But the dilemmas faced in health-caredecision making often are not framedas physicians versus patients.Rather,they are framed in terms of whom physicians should converse with: patients, their family, or both. The discourse aroundautonomyas the rightof individualpatientsdepictspatientsas being alone andunaffectedby relationshipsand, thus, undercutsan appreciationof the importance of patient-familyinteractionsin medicaldecision making.4In this articlewe argue that approaches to individual decision making that do not take relationships into accountare inadequate.As WillardGaylin writes, "Humanbeings are PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 405 productsof theirenvironmentas well as its creators;thereforeany considerationof the individualindependentof his relationshipsand communitiesis self-defeating" (1996:44). Serious considerationof a discourse of relationshipsmay help bioethicists and clinicians avoid certainproblemsthatarise when autonomy-basedpolicies are appliedat the end of life, such as in the use of advancecaredirectives(ACDs). The PatientSelf-DeterminationAct (PSDA) of 1991 requiresthathospitalsthatreceive federalfunds informpatientsabouttheirrightunderexisting statelaws to createa living will or durablepower of attorneyfor healthcare. Only a small percentageof Americanshad an ACD in place when the law was passed, and proponentsof the PSDA arguedthatincreasedpublic exposurewould resultin greateracceptanceof ACDs (Fletcher1989; Levin 1990; see also E. J. EmanuelandL. L. Emanuel1990; L. L. Emanueland E. J. Emanuel1989; L. L. Emanuelet al. 1991).5Currently,the numberof AmericanswithACDs remainslow, andinterventionsdesignedto increase use of ACDs typicallyhavefailedto generateutilizationratesof morethan20 percent in targetpopulations(HareandNelson 1991;Jacobsonet al. 1994;Sachset al. 1992). An even more compelling concern is thatEuropeanAmericans(whites) are much more likely to desire or possess advance care directives than otherraces or ethnicities (Blackhallet al. 1995; Caraliset al. 1993; Murphyet al. 1996; Sugarman et al. 1992; Teno et al. 1990). Such findings suggest thatgreaterpublicawareness alone will not significantlyincreasethe use of ACDs and thata betterunderstandingof the culturalfactorsthataffect their acceptanceis needed.6If bioethics policies are to meet the needs of patientswhose values are differentthanthose of the dominantwhite middle class,7more must be known about the diverse clinical situationsin which life-and-deathdecisions aremade. Methods This article stems from the two-year study "Ethnicityand Attitudestoward Advance Care Directives,"which surveyed 800 individuals,age 65 and over, residing in and aroundLos Angeles. The sample included 200 self-identifiedmembers in each of fourethnicgroups:AfricanAmerican,EuropeanAmerican,Korean American,and Mexican American.In year one, attitudesabout end-of-life decision making were elicited in face-to-faceinterviews by ethnically matchedinterviewers who used an extensive surveyprotocol.In year two, in-depthethnographic interviews,two hours in length, were then conductedwith ten percent(n = 80) of the original sample, in the individual'spreferredlanguage,by ethnicallymatched anthropologistconsultants.8These interviews were treatedas conversations,that is, as coconstructedspeech events (Gubriumand Holstein 1994; Mishler 1986).9 The excerpts quoted in this article are presentedin their actual sequence and in question-and-answerformat,ratherthan as a monologue, to emphasize their coconstructionby the interviewer. A subsamplein each ethnic group (n = 20) was selected for in-depthinterviews by first creatinga pool including only those individualswhose survey responses were typicalfor thatethnicgroup.In determiningtypicality,we paidattention particularlyto dimensions of the survey on which the four ethnic groups showed statisticallysignificantdifferences.Attitudesaboutpatientautonomywere the core items of analysis,with a few additionalitems basedon the uniqueresponse patterns for each ethnic group. Core items concerned physician truth telling 406 MEDICALANTHROPOLOGY QUARTERLY (Should the physician inform the patientabout a diagnosis of metastaticcancer? About a terminalprognosis?)and medical decision making (Who should make a decision aboutthe use of life-sustainingtechnology:the physician,family, or patient?). Of the 20 KoreanAmericansinterviewedin depth, 18 were chosen from the typicalcase pool. Next, two atypicalcases not in the pool were also selectedto provideinsightinto the diversitywithinthe KoreanAmericansample. One participant,Mrs.Hye-ranKim, was a typicalcase. Herviews represented those of the KoreanAmericansamplegenerallyand were distinctfrom the views of the threeotherethnic groups.Mrs.Kim's life story demonstrateshow a familycenteredapproachto medical decisionmakingis partof a broaderKoreancultural pattern.10 Ideally, the roles and responsibilitiesof family memberstowardone another,ratherthanself-interest,constitutethe paramountguidefor moralaction.Such values are modeled by parentsto children,articulatedas explicit principlesof behavior,andreinforcedthroughsocial sanctionsto become an intrinsicpartof one's character. Mrs.Kim's case was also typicaldemographically:In 1990 the Koreanpopulation in the United States was 798,849 (U.S. Departmentof Commerce 1992). More thanhalf of the Koreanimmigrantshave settled on the West Coast;the largest population,an estimated200,000, lives in Los Angeles (Bandon 1994). Among the fourgroupsin our study,KoreanAmericansarethe most recentto immigrateto the United Statesand tend to speakonly Korean.Most areparentsof highly skilled workersand professionalswho enteredfrom South Korea as adultsunderliberalized immigrationpolicies establishedby Congress in 1965. Not surprisingly,the elderly KoreanAmericanswere the least acculturatedgroupin the study," having been in this country an average of 12 years. Indeed, Mrs. Kim emigratedfrom Seoul 12 yearspriorto the studyand spoke Koreanonly. Like most of the Korean Americanswhom we interviewed,she was a permanentresidentin Californiaand was enrolledin Medi-Cal(the federal-stateMedicaidprogramin California).12 The qualitativemethodsused by manymedical anthropologists,includingthe sophisticatedanalysisof life storiesandothernarratives,arefrequentlyoverlooked or dismissed as "merelyanecdotal"by quantitativelyorientedclinical researchers. Ouruse of a rigorousmultimethoddesign,'3however, made it possible to use narratives to explain an otherwiseincomprehensiblecontradictionin the surveydata: Although KoreanAmericansreportedextremely negative attitudesabout the use of life-sustainingtechnology (LST) for themselves, they were extremelypositive about its use generally.'4Mrs. Kim explains this paradox:Although she did not want to be kept alive by LST, she believed thatit is her children'sduty to makethe decision forher.In her view, familymembersareobligatedto protectpatientsfrom learning that their illnesses are life threateningand must strive to keep patients alive "evenone moreday." Korean American Attitudes about Patient Autonomy A summaryfollows of KoreanAmericanattitudesabout patient autonomy, based on a quantitativesurveyconductedduringthe first year of the study (Blackhall et al. 1995). A stepwise multiplelogistic regressionanalysis showed thatethnicity is the most significantfactorto accountfor differencesin attitudesaboutpatient autonomyreportedby the four ethnic groups.Ethnicity accountedfor more 407 PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING TABLE 1 answers to the Respondents' question "Should the doctor tell the patient a diagnosis of metastaticcancer?" (p <.001). AfricanAmericans EuropeanAmericans Mexican Americans KoreanAmericans Yes No 89% 87% 65% 47% 11% 13% 35% 53% variability among the 800 respondents than did other demographic factors such as age, sex, religion, level of functional independence, level of education, and income.'5 Among the groups surveyed, Korean Americans were the least likely to believe that patients should be told the truth about the diagnosis and prognosis of a serious illness. Less than half (47%) agreed that doctors should tell patients about a diagnosis of metastatic cancer (see Table 1). Only 35 percent agreed that doctors should tell patients that they are dying (see Table 2). TABLE 2 Respondents' answers to the question "Should the doctor tell the patient that they are dying?" (p < .001). EuropeanAmericans African Americans Mexican Americans KoreanAmericans Yes No 69% 63% 48% 35% 31% 37% 52% 65% Korean Americans were most likely to believe that family members rather than patients should make decisions about the use of life-sustaining technology. Only 28 percent believed that patients should decide whether or not to use LST. A majority of Korean Americans (57%) believed that decisions about LST should be made exclusively by the family (see Table 3). (All differences cited above are statistically significant at the p < .001 level.) TABLE 3 Respondents' answers to the question "Who should make the decision whetherto put the patient on life support?"(p < .001). EuropeanAmericans AfricanAmericans Mexican Americans KoreanAmericans The patient The family 65% 60% 41% 28% 21% 26% 46% 57% The doctoror other designatedperson 15% 15% 14% 16% 408 MEDICALANTHROPOLOGY QUARTERLY TABLE 4 Respondents' likelihood of possessing an advance care directive(ACD) (p < .0001). Americans European MexicanAmericans AfricanAmericans KoreanAmericans 28% 10% 2% 0% Contraryto stereotypesaboutKoreans,talkingin advanceaboutdeath,even theirown deaths,is not completely prohibited.ElderlyKoreanAmericanstend to acceptdeathas a partof life: Virtuallyeveryonewe interviewedin year two of the studywas a memberof a mutualaid society (rotatingcreditunionthatfunctionsas a burialsociety) and had alreadymade funeralarrangementsfor themselves. But KoreanAmericanswere the most likely of our studyparticipantsto agreethat discussing deathwith a doctorcould be dangerousto patientsand thatadvanceplanning is not necessarybecausefamilies will know what to do when the time comes (Murphyet al. 1996). TABLE 5 Likelihood of possessing an advance care directive(ACD) among respondents who had knowledge of ACDs (p < .001). Americans European MexicanAmericans AfricanAmericans KoreanAmericans 40% 22% 17% 0% As reportedin Murphyet al. 1996, KoreanAmericanswere also least likely (0%)to possess an advancecare directive(ACD) (see Table 4). Even among individualswho hadknowledgeof ACDs, KoreanAmericanswereless likely thanothers to have an ACD in place. Of the 200 KoreanAmericanssampledin year one, only 20 had knowledge of ACDs, and of these, not one possessed a living will or a durablepower of attorney(see Table 5). The Case of Mrs. Kim: A Narrative Approach A narrativeapproachmade it possible to clarifyMrs.Kim's decision-making preferencesandpractices.16We paid explicit attentionto her use of Koreanethical principlesor values such as tori (duty, literally, "the properway of life")17 and hyodo (filial piety) throughthe stories she told abouther experiencesand expectations in healthcaresettings.In Excerpt1, for example,Mrs.Kim talks aboutherexperienceas a patientin which her family hid the fact of a cancerdiagnosis. Seven yearspriorto the interview,Mrs.Kim discoveredthatshe was having a vaginaldischarge.She informedher youngest daughter-in-lawaboutit and was takento see a Western-styledoctor who scheduled an operation.'8Before the operation took place, a periodduringwhich Mrs. Kim was takingtraditionalChinese medicines, her dischargestopped.Mrs. Kim's story makes the point that families should not PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 409 inform a patient about a diagnosis of cancer, even though the patient is naturally curious. Her children, not she, were responsible for making the decision about her treatment. Excerpt1 Hye-ranKim: So I told my childrenthatI didn'tneed the operationbecause the dischargehad stopped.My childrentold me thatI should follow the doctor's instructionsanyway;I should have the operation.After the operation,I was fine. For a year laterthey didn't tell me the truth.Then aftertwo years, they disclosed that I hadhad cancer-the early stage. So the doctortook out half of my womb, not all. Interviewer: Didn't you want to know [whatyourdisease was]? HRK: I would feel like a fool who didn'tknow enoughto be curious abouther own disease. [But]my childrendid a good thingfor me, not a badthing. If I hadresearchedwhatit was, then it would be bad for everyone. In Excerpt 2, Mrs. Kim explains in greater detail why it is unwise for patients to know their diagnoses. Disclosing a diagnosis of cancer to patients causes them to suffer and leads them to think obsessively about dying. When Mrs. Kim reflects upon her own case, she believes it was better to avoid such suffering.19 Excerpt2 Int: HRK: If anyone in yourfamily hadcancer,do you thinkit would be good to tell the personabouttheirdisease? Reflecting on my experience,if the patientwere to know their disease, it would cause anguish.So I thinkit would be betternot to informthe patient,andin thatway the patientcould pass away less fearfully.In the case of cancer,the patientcannotstop thinkingabouttheirown death:it is not good. In Excerpt 3, Mrs. Kim comments on the use of life-sustaining technologies such as CPR or mechanical ventilation on patients with a terminal prognosis. Although Mrs. Kim has not witnessed the use of LST among her friends, she is emphatic that it is not good to prolong the life of a fatally ill person. Excerpt3 Int: HRK: Int: HRK: Int: Then, among your friends,was thereanyonehospitalizedfor a seriousdisease? So far, none. In the [Buddhist]temple,20I see 85-, 86-year-old people. They come to the templeeven thoughthey don't have much energy. But they still come to the temple. ... Then you haven't known anyone living in bed with an oxy- gen mask for a long time? None I know. Accordingto Americanlaws, as long as the patient'sbreathing is not stopped,the patientwill remainalive regardlessof the chance of resuscitation,whetherthe patientis conscious or not. Then, if the functionof eitherthe heartor the lung stops, by using CPR they keep the patientalive. How do you feel aboutthis? 410 MEDICAL ANTHROPOLOGY QUARTERLY HRK: In my opinion,if the patientdoesn't have a chanceto live, then not using CPRwould be better.If theirlife is prolonged,it causes burdensto the childrenat home. In hospital,it is less burdensometo the children.Attendingthe patientis a bother.I don't thinkthatit is good for the fatallyill patient'slife to be prolonged.The one who would pass away shouldpass away. In Excerpt 4, Mrs. Kim discusses the difference between dying in the hospital and dying at home. Her concerns are expressed in terms of burdens placed on the children. In Korea, dying at home is preferred. But even though Mrs. Kim prefers to die at home, she sees no alternative to the American way of dying in the hospital. Mrs. Kim surprises the interviewer by suggesting, however, that dying in the hospital might be better than the Korean way because it relieves the family's responsibility to observe certain onerous rituals. Excerpt4 Int: HRK: Int: HRK: Int: HRK: Int: HRK: Int: HRK: Int: HRK: In America,people die in the hospital.And in Koreapeople usually die at home. How do you thinkaboutthis? In Korea,peopledie at home. It is the custom.Allowing the patientto die at home is the children'sresponsibility.If the childrenlet the patientdie in the hospital,people would regardit as not being filial. The Americanway is good, isn't it? Do you like the Americanway better? Yes, it doesn'tbotherthe childrenso much.If the patientpasses away in the hospital,they take the corpseto the morgue[laughing]. Thenit looks too lonely for the deadperson.In thatcase, no one goes to see the corpse in the hospitalexcept occasionally. The family stayshome. When I went to console a family who lost theirmother,the family stayedcomfortablyat home. Shouldthey stay up all night like in Korea? Sure.Sometimesthe Koreantraditionworksbetterin thatcase, butforbeingsimpleandpractical,theAmericanway is goodtoo. Hypothetically-it is only "if'-what would you like at the time of yourdeath? If I died here,the Americanway would be applied,andif I died in Korea,thenKoreanways shouldbe followed. Don't you agree?How can people ignorethe custom? Which would you like better? I don'taskthemto followtheKoreanway if I die in America,do I? It meansyou preferthe Koreanway. Yes, but it is not possible. And in Korea,it is not possible to use the Americanway.2' In Excerpt 5, Mrs. Kim is presented with a scenario about the use of LST with a terminally ill cancer patient. She describes what are proper decisions for various family members. The excerpt exemplifies Mrs. Kim's view of patient autonomy. The dominant principle is the fulfillment of responsibilities embedded in family relationships: One must do one's best for a family member, whether parent, child, or spouse. One must do everything to avoid letting a family member die. Family members, not dying patients, are expected to make medical decisions. PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING Excerpt5 Int: HRK: Int: HRK: Int: HRK: Int: HRK: Int: HRK: Int: HRK: 411 If the patientwere yourrelative,then whatkindof decision are you supposedto make? If the patientweremy child, then I would ask themto use the treatmentin orderto see my child alive even one more day. If the patientwere yourparent? If my parentwere aged andin such condition,well... as I would behavetowardmy child, I also would ask the same thing. I shouldn'tlet themdie. I would trymy best. If the patientwere you, then whatdo you expect yourchildren would decide for you? If my childrenwantedto see me even one moreday, then they mightask for the treatment.I am the one who is going to die; so I don't controlthe situation. Whenyou thinkaboutthe decision rightnow, would you want the treatmentin orderfor your life to be extendedif you were not conscious andhad almostno hope to live? I would ratherpass away sooner, if by having my life extended it causedpain. But for others,you would ask for the treatmentto extend the life? In othercases, if the patientwere eithermy child or my husband,thenI wouldrequestthe treatmentin orderto see them even a little longer. Then isn't thatcontradictory? Althoughit's a contradiction,it's the rightthing to do [tori]. Don't you thinkso? Would any childrenlet theirmotherdie withouttryingto save her by any means? Seen against the background of the North American bioethics discourse on individual rights, Mrs. Kim's statement in the preceding excerpt is startling: "I am the one who is going to die; so I don't control the situation." Mrs. Kim appreciates the contradiction in wishing to avoid medically futile treatment while giving control to family members who are obligated to ask for it. But, she says, giving control to her family members is more important, that is, tori, "the right thing to do." In Excerpt 6, Mrs. Kim elaborates on her views about the use of LST and ACDs. In common with other Korean Americans interviewed, Mrs. Kim expresses her willingness to accept death as a part of old age: "If I had such a terminal disease," she says, "then I would not have them use such treatment, since I have lived long enough." She further states that it is not good to sign an ACD in advance because the future cannot be known. She prefers her family to make any necessary decisions when the time comes. Excerpt6 HRK: Int: HRK: If I were in a certainterminalcondition,I would not want them to use it [LST]unless the treatmentcould makeme live again. In my opinion,if I had such a terminaldisease, then I would not have themuse such treatment,since I have lived long enough. If therewere a documentedarrangementin which the potential patient'sown decision were representedwith theirsignature, would you wantthis arrangement? I don't like to putmy signatureon anythingin advance. 412 MEDICAL ANTHROPOLOGY QUARTERLY Int: HRK: Int: HRK: Why? You neverknow your futureor yourfate;so why decide in advance? Then you would wantyour family to decide later? Yes. My family. In Excerpt 7, the interviewer skillfully engages Mrs. Kim in a fuller consideration of ACDs, appealing to her sense of tori. Excerpt7 Int: HRK: Int: HRK: Int: HRK: Int: HRK: Int: HRK: Don't you thinkthatsuch decision makingmightbe burdensome for your family? WhenI thinkaboutotherpeople whose lives areextendedby medication[whose lives otherwisewould end], thenI thinkthat it is betterfor those patientsto pass away gracefullyinsteadof being treatedwith the medication.This is my opinion. But the hospitalandthe childrenof those patientshave no choice, do they? In the United States,by takingmedication,terminalpatients' lives areextended;so therearesome patientswhose lives are prolongedin thatway for even a year. So the patient'sown decision is important.Whenthe patientis conscious, if they put theirown signatureon the papersaying thatthey don't wantsuch treatment,then such treatmentwould be avoidedlateron. But what if patientsdesire to live longer?WhenI observepatientshere, I believe they all wantto have such treatment. Then would you put your signatureon suchpapers? Sure.Why shouldmy life be prolongedif therewere no chance of living? But beforeyou said you wantedyour family to decide. Well, if I got a terminaldisease, I would ratherpass away sooner,but I don't know how my childrenwould deal with the situationeven if I put my signatureon the papersyou described. Several important points are raised here: First, Mrs. Kim actually reconsiders her position and says she would sign an ACD. Second, she appears to be influenced less by the argument based on tori ("Don't you think that such decision making might be burdensome for your family?") than one based on patient autonomy ("Well, if I got a terminal disease, I would rather pass away sooner."). Third, and most important for an accurate analysis of her narrative, however, Mrs. Kim affirms that her views in this part of the interview are only hypothetical ("But I don't know how my children would deal with the situation even if I put my signature on the papers you described"). She expects her children to interpret their tori as a mandate for using LST regardless of any statement that she might sign in advance. In Excerpt 8, the interviewer and Mrs. Kim discuss the general impermissibility of talking to a person about his or her death. Such conversations are necessary, of course, for implementing the Patient Self-Determination Act and for completing ACDs. Mrs. Kim, like other Korean Americans we interviewed, states that it is inappropriate to talk to a person about his or her death. But she is willing to discuss PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 413 her own death in the interview because she draws a sophisticated distinction between "research" and "real life." Excerpt8 Int: HRK: Int: HRK: Int: HRK: In orderto use thepaperthatI mentioned,it is necessaryto talk aboutdeathwhen the potentialpatientis still conscious and healthy.Whatdo you thinkaboutthis? It is not good to talkaboutdeathin advance. Even for the old people? I am also old. Althoughthe personmay be old, to talkon this issue in advanceis not good. If askedto sign such papers,without knowing one's future,how could I sign them? Then you don't feel good talkingaboutit with me? Yes, thatis fine. If it is aboutresearchandnot real life, fine. In Excerpt 9, Mrs. Kim is asked her opinion about how an ACD should be presented to a patient. She continues to speak hypothetically for purposes of the research interview, straddling a discourse of relationships (tori) or duty and a discourse of individual rights (patient autonomy). Mrs. Kim feels that the physician alone should offer the ACD. The document should be presented for her signature in a conversational style, in which her questions can be answered. Excerpt9 Int: HRK: Int: HRK: Int: HRK: Wouldn'tsome people feel reluctantto sign? Whatdo you think aboutthat? Concerningthe signing, if I becamesick and were asked to do this, then I would do it, butnow, since I don't know aboutmy future,my signaturewould not apply. In thatcase, who shouldask you to preparethe paperwork,to makedecisions with a signature? Can therebe anyoneelse besides the doctor? How should the doctorapproachyou aboutit? He shouldtell me thatmy disease is such andsuch, and ask me whetherI like this way or thatway. Then I might have my own preference. The process should be done in this question-andanswerstyle. In Excerpt 10, Mrs. Kim once again makes clear the conditional and hypothetical nature of her comments. Excerpt 10 Int: HRK: Int: HRK: If the patientbecomes criticalandthen unconscious,then how can the doctorknow whatthe patientwants? For me, I would say to the doctorthathe shouldlet me be: not use medicine. If you were not conscious, so you were not able to talk to your doctorlike that,then what? Then my sons shoulddecide. If they wantto see me even one more day, they would ask the doctorto use medicine,or if they wantme to pass away peacefully,thenthey would decide the otherway. It's up to themat thatpoint. 414 MEDICALANTHROPOLOGY QUARTERLY Int: HRK: I haveinterviewed severalKoreanpeopleonthisissue,andthe mostdifficultthingformeto understand is whytheintervieweesthemselveswouldn'twanttreatment, buttheywouldpermit thetreatment if thepatientsweretheirparents,in ordertoprolongtheirlivesbyevena day. Sure.Thatis therightbehaviorforchildren.If peopleheardthat a childhaddecidedto endtheirparents'lives,theywouldregardthechild'sbehavioras unfilial.Itis okayformeto talk aboutmyself,butthat'sbecausetherearenochildrenwhosay, "Letmymotherpassaway."If theyshouldaskmeto decideon myown,thenI wouldprefertopassawaysoonerwithoutpain. End-of-lifedecisionsaremorethana matterof personalconsciencein the Korean American community.Childrenwho "decided to end their parents' lives" would be judgedharshly.In the interview,Mrs.Kim points out thatshe may freely hypothesize signing an advancecare directive limiting end-of-life treatmentbecause she is confidentthather childrenwill not say, "Letmy motherpass away." She expects themto overrideany limitationon treatmentto whichtheirmothermay have agreedin the ACD. Implications of the Korean American Data: A Discourse of Relationships in Bioethics KoreanAmericanattitudesabout end-of-life decision making center on the importanceof relationshipsand the responsibilitiesof family membersratherthan on patientautonomy.Suchbeliefs andpracticesderive from the traditionalculture of Korea,22which has much in common with the cultures of neighboringEast Thereis diversityamong KoreanAmericans,much of it condiAsian countries.23 tioned by adaptationsmadeto life in the United States.24Mrs.Kim soundscontent and secure in her relationshipwith her children. Although the attitudesshe expresses are typicalof our sample,not all of the KoreanAmericanswe interviewed were as confidentof theirchildren'sactualsupportas Mrs. Kim. Respondentsfrequentlymentionedthateconomicpressures,arisingespecially when adultchildren andtheirspousesareemployedfull-timeor live in anotherpartof the country,contributedto intergenerational tensions and disappointmentsin fulfilling traditional Koreanfamily ideals. If childrenlack adequatefinancialresources,for example,theymaybe unable to requestfurthertreatmentfor theirparents.Living arrangementsare also critical. Whenchildrenresideaway fromtheirparents,in Koreaor elsewhere,it is very difficult for themto fulfill theirtraditionalfamilialduties. Mrs. Kim assumesthatthe Korean Americanfamily will function much the same as in Korea. But notions such as filial piety are undergoingmodification in the United States. Changing gender roles and economic stresses that result in women's fuller participationin the laborforce make it difficult for wives, daughters-in-law,and otherfemale kin to provide the same level of supportfor parentsthat was expected of them traditionally. Other institutionalpressures, including the implementationof federal laws such as the PatientSelf-DeterminationAct and state laws thatlimit how long a family may keep a corpseat home, also tend to force change. The resultis not so much a wholesale switchfrom traditionalKoreanto white Americanmiddle-class PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 415 values as it is the creation of a new syncretic ethnic culture (Kim and Hurh 1993; Park 1989). Koenig and Marshall (1994) argue that social scientists cannot "biopsy" attitudes or develop an "ethnic algorithm" that can be plugged into multicultural clinical situations and result in neat bioethical solutions. Every case is individual and circumstantial. Physicians need to negotiate with patients the treatments that will be acceptable for them, given a range of attitudes and practices within the patient's family and ethnic group. These negotiations require more than translation of autonomy-based bioethics policies across "language barriers" (Woloshin et al. 1995).25 A physician's discussion of end-of-life treatment decisions directly with elderly Korean American patients rather than their family may itself be experienced by the patient as impolite or even a violation. A number of bioethicists and social scientists have begun to address how to negotiate cultural factors in clinical ethics consultation (Heitman 1994; Jecker et al. 1995; Marshall and Koenig 1996; Orr et al. 1995). Before employing the otherwise promising strategy of dialogue with patients about specific treatment choices (Benjamin 1990), physicians must first reckon with family relationships as a locus of ethical responsibility and decision making.26 In other words, a discourse on relationships should supplement the discourse on individual rights. Although these discourses may seem to be mutually exclusive, as Mrs. Kim's case has shown, they are not. In its report Deciding to Forego Life-Sustaining Treatment, the President's Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research stresses that physician respect for the patient's values is one of the elements of good decision making: "The only time that the Commission finds it justified for a patient who could be informed and involved to be excluded is when that patient freely and knowingly transfers some decision-making authority to another" (1983:51 ).27We are not talking here about family members overriding the patient's autonomy. Most elderly Korean Americans in our study such as Mrs. Kim are saying, in effect, "Giving control to my family is the right thing. It is what I personally prefer and is my expression of autonomy." NOTES Acknowledgments.This is a reportfrom the study Ethnicityand AttitudestowardAdvance CareDirectives,which was fundedby the Agency for HealthCarePolicy Research, Grant No. R01HS0700101A1, Leslie J. Blackhall, principal investigator.The grant was sponsoredby the Pacific Centerfor HealthPolicy and Ethics, Universityof SouthernCalifornia.The authorswish to thankSung-joo Ko for his work as interviewer,transcriber,and translatorfor the KoreanAmericaninterviews.For theirsupportandcomments,we wish to thankDavid Blake, AlexanderM. Capron,Soo-Young Chin, David A. Goldstein,Deborah R. Gordon,SharonR. Kaufman,BarbaraA. Koenig, HenryLambert,PatriciaA. Marshall, and BarbaraMalcolm.A draftof this articlewas presentedat the AmericanAnthropological Association AnnualMeeting,Washington,DC, November 16, 1995, at the session "Narrative as Constructand as Construction:Stories in a World of Illness,"organizedby Cheryl MattinglyandLindaGarro. Correspondencemay be addressedto the first authorat the Departmentof Occupational Science and OccupationalTherapy,University of SouthernCalifornia,Center for HealthProfessions 133, 1540 E. AlcazarSt., Los Angeles, CA 90033. 416 MEDICALANTHROPOLOGY QUARTERLY 1. The principleof patient autonomyholds that individualshave the right to control what happensto them and, in particular,to make informeddecisions about their medical care (President'sCommission 1983). Accordingto this principle,patientsshouldbe told the truthabout their diagnosis and prognosis, about the risks and benefits of proposed treatments, and they should have the right to make decisions based on this information (BeauchampandChildress1994). 2. Callahan's(1996) positionin the bioethicsdebateaboutautonomyis thatamongthe four principlesin the "Georgetownmantra"(autonomy,beneficence,nonmalfeasance,and justice),justice should sometimes take priority.This defies the conventionalposition held by Veatch(1996), for example,thatno principlecan trumpautonomy(i.e., justify overcoming the individual'sright to decide). In our study, we arguenot that autonomy should be overcomebut thatit is morecomplicatedthanrepresentedby eitherposition.The CallahanVeatchdebaterelatesto a more generalone aboutthe properfoundationsfor ethics. Rawls (1971) arguesthat a just system is one in which laws aboutspecific kinds of situationsare basedon the judgmentof rationalindividualsin the "originalposition"(i.e., not presentlyin the situationthemselves).In otherwords,Rawls finds it possible to imagine a lone individual whose decisions would be valid withoutregardto his or her immediatesocial relationships. Sandel (1982) argues against Rawls that relationshipsprecede and constitute the person.Relationshipsmake us who we are as individualsand define our interests.Obligations, therefore,are as centralto our identityas rights.For a metacritiqueof Rawls andSandel that analyzes their work in terms of the underlyinguniversalistassumptionsthat they share,see Bauman1993. There are manydifferentsourcesin the West of a discourseon relationships,not just the communitarianone representedby Callahan,just as thereare many differentsourcesin Korea.Terms such as relationships,the West, Koreanculture,andethnicitygloss over distinctionsamongvariousepistemologicalandontologicalsources in both cultureswith regardto definingthe person,morality,andthe body. 3. See Landy 1977 for a generaloverview of the extensive cross-culturalliterature.A summaryof explanatoryor causal models of illness appearsin Csordas1989. For a particularlyclear example of conflict between biomedicaland traditionalcausal models in an oncology case in Mexico, see Hunt 1993. 4. H. LindemannNelson and J. LindemannNelson (1995) addressthe problemof includingfamilies in medicaldecision makingin mainstreamNorthAmericancontexts. They discuss a case in which a physicianis stymiedby a conflictbetweenan elderlypatient'sright to privacy and her adult daughter's right to informationas her mother's caretaker.The authorssuggest thatthe conflict could be handledbetterif the physicianwere to engage the motheranddaughterin a conversationaboutmutualobligations: What's missing from this way of approachingthe issue [i.e., the talk of individual rights]is any acknowledgmentof the specialclaimspeoplehave on each otherwithina settingof intimacy... . The relationsamong the people involved can't easily be capturedby talkof rights.Intimatesbelong to each otheras well as to themselves,andthis NelsonandLindemannNelson 1995:111] belonginghasmoralconsequences.[Lindemann 5. Accordingto a study published in 1987, only 9 percentof Americanshad written advancecare directives(Steiber 1987:72, cited in Emanuelet al. 1991:889). As a legislator introducingthe PSDA in the House of Representativesstated,"Recent surveys show that only 9 to 15 percentof the populationhave executedadvancedirectives.We believe this low numberis due, in part,to lack of knowledge"(Levin 1990:E944). 6. Culturalfactors may include not only traditionalbeliefs and values but distrustof the dominantmedical system due to socioeconomic disparitiesand the experience of discrimination.We hope to addresssuch issues in futurereportsfrom the study. 7. Lynn and Teno (1993) suggest thatthe meaningand usefulness of advancedirectives might be linked to a "middle-class"approachto healthcare. In Kelner's (1995) study of elderlyCanadianpatients(N = 38), almost all of whom were white Anglo-Saxons, more PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 417 thantwice as manypatients(n = 27) preferredto have a voice in decision makingat the end of life than to delegate making such decisions (n = 11). Middle-class patientswere more likely to preferexercisingcontrolat the end of life thanlower-classpatients. 8. Participantswere paid $20 for the survey interviewand $25 for the in-depthethnographicinterview.The ethnographicinterviewswere audiotaped,transcribedverbatiminto Korean,andtranslatedinto English.A semistructuredinterviewformataddresseda uniform set of domains across all four ethnic groups (N = 80). All questions were open-endedand conversational.The resultingqualitativedata include illness narratives,life stories,and responses to hypotheticalscenariosaboutmedicaldecision making. 9. This methodological stance holds that the interviewer's understandingis built throughthe course of the interviewand that negotiationsof meaningoccur between interviewer andinterviewee.Thatwhich comes first in an interviewprovidesa contextfor the interviewersto elicit for readersto interpretwhatever follows. Excerptsfrom the interview transcriptarenumberedto facilitatethe reader'ssense of the sequentialdevelopmentof Mrs. Kim's narrativewithinthe conversation. 10. Hauerwasand Burrell(1989) argue that considerationsof moralcharacteras revealed in life stories are importantto ethical decision making. Mrs. Kim was raised in a wealthy family butduringher marriagelived in hardtimes. Herhusbandwas a civil servant when the KoreanWarbrokeout in 1950. He could not get a job for the next 20 years. Mrs. Kim began to peddle small goods so that she could feed and educateher children.Her life storyemphasizeswhatshe counts as ethically important: Since he didn'twork,I thoughtI neededto makea living for my children.I didn'tknow much and, inexperienced,I startedto sell [changsa]. My work as a peddlerpaid well enough so thatI could feed andeducatemy children.I did the work for 20 years. .... I carried goods on my head and sold them. I fed and educated my children in that way.... My husbanddidn't earn any money at all for 20 years. He didn'thave a job. At thattime, while peddling,being old fashioned,I didn'treveal my peddlingeitherto my husbandor to my children.WhereverI encounteredacquaintanceswhile peddling, I felt more ashamedthanif I were caughtstealing.I madean effortto avoid people. In peddlingto providenecessities for herchildren,Mrs.Kim's moralactionformorethan20 years is sustainedby her parentalduty (tori). Self-sacrifice is valuedover protectingherself from shame. Mrs. Kim's moral actions are especially creditablebecause she protectedher family frombeing directlyconfrontedwith the fact of herpeddling,althoughit is hardto believe thather familyneverfoundout aboutit. The parallelwith nondisclosureof an unfavorable diagnosis is striking:The KoreanAmericanswe interviewedsaid thatpatientswho are dying often know their diagnosis and prognosis throughinference (nunchi),even though theirfamilies continueto protectthemfrom learningthe truthdirectly. 11. The MarinAcculturationScale (Marinet al. 1987), which was translatedinto Korean for use with the KoreanAmericansample, measuresthe degree to which individuals use theirnative languageversusEnglish in daily speaking,thinking,exposureto media,and socializing with others. 12. Mrs. Kim was interviewedin August 1994. State and federal policies currently threatento end the entitlementof legal residentslike Mrs. Kim to benefitsincludingSocial SecurityIncome (SSI) andMedicaid. 13. Some recentdiscussionsof the integrationof qualitativeandquantitativemethods for clinical researchincludeBrannen1992, Carey 1993, Morse 1991, Stangeet al. 1994, and Steckleret al. 1992. 14. An overwhelmingmajorityof KoreanAmericans(78%) and MexicanAmericans (79%)agreedwith the statement"Life sustainingmachinesshould neverbe stoppedeven if the patientappearsto be dying because there is always the chance of a miracle."In sharp contrast,only 33 percentof AfricanAmericansand29 percentof EuropeanAmericansconcurredwith this statement.Given a scenarioin which they were a patientin a coma with no 418 MEDICAL ANTHROPOLOGY QUARTERLY hope of recovery, very few KoreanAmericans(14%) wanted to be kept alive by CPR, a findingthatwas indistinguishablefromthatof EuropeanAmericans( 13%). 15. In the MexicanAmericansample,however, assimilationinto the mainstreamEnglish-speakingculturewas associatedwith more positive attitudesabout autonomy,which was correlatedwith level of educationandincome. 16. There is growing emphasison the importanceof narrativesor stories in clinical ethics consultation(see GordonandPaci 1997; Hauerwasand Burrell 1989; Hunter1991). See Kleinman's(1988) argumentthatlisteningto the illness narrativesof patientsshouldbe a centralfeatureof medicalpractice. 17. The word tori comes fromthe philosophicalandethical conceptof the Tao, or The Way. It expressesa generalizedprincipleof actingproperlyin humanrelationships. 18. The "Westerndoctors"seen by patientslike Mrs.Kim areoften Koreanphysicians practicingbiomedicine. 19. Mrs. Kim told a relatedstory,not presentedhere,concerningherconsultationwith an ophthalmologistabouta growthon her eyelid. In thatsituation,a Korean-speakingnurse informedMrs.Kim andherdaughter-in-lawthatthe growthon hereye was a cancer.Believing she had a fataldisease,Mrs.Kimbeganto putheraffairsin order.Laterthe symptomdisappearedand the diagnosis of cancer was acknowledgedto be a mistake. Mrs. Kim was referringalso to this story when she says thatavoiding sufferingis more importantthansatisfying the patient'scuriosity. 20. Mrs. Kim is a practicingBuddhist,and many of her peers are Christian.Religious differenceswere not significantpredictorsof KoreanAmericanattitudesconcerningpatient autonomy,however. Mrs. Kim's attitudesreflect syncretismamong Confucian, Buddhist, and folk or popularbeliefs (e.g., aboutthe role of Fate), as well as lessons drawnfrom her experiences in America. As Park points out, syncretism is common also among Korean Americanswho areborn-againChristians:"Theirnew Christianbelief system verifies various aspects of traditionalKoreanculture.Being born again is an ongoing process in which individualsmakechoices betweenKoreaninfluencesof Confucianism,Buddhism,andshamanism and newly discovered Americanideas representedby born again Christianity" (1989:287). 21. Koreansin the UnitedStatesarewell awareof statelaws thatlimithow long a body may be kept and thatmake it impossiblefor themto have traditionalfuneralslastingseveral days at home. 22. AnotherKoreanAmericaninterviewee(age 79, female) explainedthe reciprocal, intergenerationalnatureof hyodo (filial piety) by recountinga well-known folktale.It concerns the custom of Koryo-jang(Koryo-stylefuneral),which belongs to the medieval (Koryo) periodof Koreanhistory: The fundamentalbasis of humanlife is filial piety [hyodo]. Those who adhereto this value of filial piety always try not to make theirparentsworry, and they follow their parents'advice well.... Filial piety is the fundamentalbasis of our humanlife. Filial piety travelsalong the family line. Certainfamilies have devoted childrengeneration aftergeneration,as the old sayinggoes.. .. You know, thereused to be a customcalled "Koryofuneral"in Korea a long time ago. "Koryofuneral"is where a young father carrieshis elderlyfatheron a chikeh[anA-shapedbackframe]to abandonhim deep in the mountainto his death.Therewas a young fatherwho did that.While he was trudging to the mountainwith his agedfatherin his A-frameon his back,his young son toddled and followed him. Whenhis fatherunloadedhis grandfatherand also abandoned the A-frame there, the young boy said, "Father,let's also take the A-frame.""What for?""BecauseI will needit to carryyou hereto abandonyou whenyou areold."Hearing this, his fatherimmediatelychangedhis mind andtook his fatherbackhome. As you see in this story,everythinggoes down along the family line. You know, like father, like son. If you behave well for your parents in front of your children, your PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 419 childrenlearna good example, and, in theirturn,they will do well for you. A tradition is to be carriedon, you know. 23. Hoshino (1995) reportsa virtuallyidenticalpatternof medical decision making in Japan.Bowman (1996) found many similaritiesin the end-of-life treatmentpreferencesof elderlyChinese immigrantsin Canada.See also Kleesing 1992, Mullerand Desmond 1992, Nilchaikovitet al. 1993, andYeo 1995. 24. The adaptationof Koreanimmigrantshas been reportedin studiesin the following cities: Los Angeles (Hurhand Kim 1984, Park 1996), Chicago (Kim and Hurh 1993), New York (Park1989, 1997), San Francisco(Kieferet al. 1985), andToronto(Berryet al. 1987). 25. The U.S. Departmentof HealthandHumanServices Office for Civil Rights designates more than 10 percentof the populationin five states (California,New York, Texas, New Mexico, and Hawaii)as "LimitedEnglishProficient"(LEP).AsianPacific groupsconcentratedin WashingtonStateandCaliforniacomprise,respectively,43 percentand24 percent of the populationdesignatedas LEPin those states(Woloshinet al. 1995). 26. A parallel to the Korean Americanconcepts of tori and hyodo is presented by Freedman(1996), who discusses Jewish alternativesto bioethicaldecision makingbased in individualrights.In particular,the talmudiccategoryof morah,an aspectof filial duty usually translatedin Englishas "fear"butmeaningthe "subjugationof the family member'swill to theparent,"maybe invokedby peoplewho wanttheirfamiliesto makedecisionsforthem. 27. Similarly,the commission's earlierreportMakingHealth Care Decisions (President's Commission 1982) drawsattentionto family relationships.The introduction,for example, states explicitly that "family memberscan be of great assistance in understanding informationandmakingdecisions"(1982:5). REFERENCESCITED Bandon,Alexandra 1994 KoreanAmericans.New York:MacmillanPublishing. Barker,Judith 1992 CulturalDiversity-Changing the Contextof Medical Practice.WesternJournal of Medicine 157(3):248-254. Barnes,Donelle M., Anne J. Davis, andBarbaraA. Koenig 1994 InformedConsentin a Multi-CulturalPopulation:An Ethnographyof CancerPatients. Abstractof paper presented at eighth annual WIN Assembly, Phoenix, AZ, April. Bauman,Zygmunt 1993 PostmodernEthics. Oxford,England:Blackwell. Benjamin,Martin 1990 Splitting the Difference: Compromise and Integrity in Ethics and Politics. Lawrence:UniversityPressof Kansas. Beauchamp,Tom L., andJamesF. Childress 1994 Principlesof BiomedicalEthics.4th edition.New York:Oxford. Berry,J. W., Uichol Kim, ThomasMinde,andDoris Mok 1987 ComparativeStudies of AcculturativeStress. InternationalMigration Review 21(3):491-511. Blackhall,Leslie J., Sheila T. Murphy,Gelya Frank,Vicki Michel, and Stanley Azen 1995 EthnicityandAttitudestowardPatientAutonomy.Journalof the AmericanMedical Association 274(10):820-825. Bowman,Kerry 1996 Chinese CanadianAttitudestowardAdvance Directives. Ph.D. dissertation,Departmentof Anthropology,Universityof Toronto. 420 MEDICAL ANTHROPOLOGY QUARTERLY Brannen,J. 1992 Combining Qualitative and QuantitativeMethods: An Overview. In Mixing Methods:QualitativeandQuantitativeResearch.J. Brannen,ed. Pp. 3-38. Brookfield, VT: Avebury. Callahan,Daniel 1996 CantheMoralCommonsSurviveAutonomy?HastingsCenterReport26(6):41-42. Caralis,P. V., BobbieDavis, KarenWright,andEileen Marcial 1993 The Influence of Ethnicityand Race on Attitudes toward Advance Directives, andEuthanasia. Journalof ClinicalEthics4(2):155-165. Treatments, Life-Prolonging Carey,J. 1993 LinkingQualitativeand QuantitativeMethods:IntegratingCulturalFactorsinto Public Health.QualitativeHealthResearch3:298-318. Csordas,ThomasJ. 1989 The Sore That Does Not Heal: Cause and Concept in the Navajo Experienceof Cancer.Journalof AnthropologicalResearch42(4):457-485. Davis, Anne J., andBarbaraA. Koenig 1996 A Questionof Policy: Bioethics in a MulticulturalSociety. NursingPolicy Forum 2(1):6-11. Emanuel,EzekielJ., andLindaL. Emanuel 1990 Living Wills:Past,Present,andFuture.Journalof ClinicalEthics 1:9-19. Emanuel,LindaL., andEzekielJ. Emanuel 1989 The MedicalDirective:A New ComprehensiveAdvanceCareDocument.Journal of the AmericanMedicalAssociation261(22):3288-3293. Emanuel,LindaL., MichaelH. Barry,JohnD. Stoeckle, Lucy M. Ettelson,andEzekielJ. Emanuel 1991 Advance Directives for Medical Care-A Case for GreaterUse. New England Journalof Medicine324(13):889-895. Fletcher,JohnC. 1989 Remarkson the Patient Self-DeterminationAct. CongressionalRecord, Senate (October17):S13567-S 13570. Washington,DC: GovernmentPrintingOffice. Freedman,Benjamin 1996 Respectful Service and Reverent Obedience: A Jewish View on Making Decisions for IncompetentParents.HastingsCenterReport26(4):3 1-37. Gaylin,Willard 1996 WorshippingAutonomy.HastingsCenterReport26(6):43-45. Gaylin,Willard,andBruceJennings 1996 The Perversionof Autonomy.New York:Free Press. Good, Mary-JoDelvecchio, LindaHunt,TsunetsuguMunakata,andYasukiKobayashi 1993 A ComparativeAnalysis of the Cultureof Biomedicine: Disclosure and Consequences for Treatmentin the Practiceof Oncology. In Healthand HealthCarein Developing Countries.P. Conrad and E. Gallagher, eds. Pp. 180-210. Philadelphia: Temple UniversityPress. Gordon,DeborahR. 1994 The Ethics of Ambiguity and ConcealmentaroundCancer:Interpretationsof a Local ItalianWorld.In Interpretative Phenomenology:Embodiment,Caring,andEthics in HealthandIllness.P. Benner,ed. Pp. 279-322. ThousandOaks,CA: Sage. Gordon,DeborahR., andEugenioPaci 1997 DisclosurePracticesandCulturalNarratives:UnderstandingConcealmentandSilencearoundCancerinTuscany,Italy.SocialScienceandMedicine44(10):1433-1452. Gubrium,JaberF., andJamesA. Holstein 1994 AnalysingTalk and Interaction.In QualitativeMethods in Aging Research.J. F. GubriumandA. Sankar,eds. Pp. 173-188. ThousandOaks, CA: Sage. PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 421 Hare,J., andC. Nelson 1991 Will OutpatientsComplete Living Wills? A Comparisonof Two Interventions. Journalof GeneralInternalMedicine6(1):41-46. Hauerwas,Stanley,and David Burrell 1989 From System to Story: An AlternativePatternfor Rationalityin Ethics. In Why Narrative?Readings in NarrativeTheology. S. Hauerwasand L. G. Jones, eds. Pp. 158-190. GrandRapids,MI:William B. ErdmansPublishing. Heitman,Elizabeth 1994 CulturalDiversity and the Clinical Encounter:Inter-CulturalDialogue in MultiEthnicPatientCare.In Theological Analysis of the ClinicalEncounter.G. P. McKenney andJ. R. Sande,eds. Pp. 203-233. The Hague:KluwerAcademicPublishers. Hoshino,Kazumasa 1995 AutonomousDecision Making and JapaneseTradition.CambridgeQuarterlyof HealthcareEthics4(1):71-74. Huhr,Won M., andKwang ChungKim 1984 Adhesive SocioculturalAdaptationof KoreanImmigrantsin the U.S.: An AlternativeStrategyof MinorityAdaptation.International MigrationReview28(2):188-216. Hunt,LindaM. 1993 The Metastasis of Witchcraft:The Interrelationshipbetween Traditionaland Biomedical Concepts of Cancer in Southern Mexico. Collegium Antropologicum 17(2):249-256. Hunter,Katherine 1991 Doctors' Stories:The NarrativeStructureof Medical Knowledge.Princeton,NJ: PrincetonUniversityPress. Jacobson,Jay A., BarbaraE. White, MargaretP. Battin,Leslie P. Francis,David J. Green, andEvelyn S. Kasworm 1994 Patients'UnderstandingandUse of AdvanceDirectives.WesternJournalof Medicine 160(3):232-236. Jecker,Nancy, JosephCarrese,andRobertPearlman 1995 CaringforPatientsin Cross-Cultural Settings.HastingsCenterReport25(1):6-14. Kellner,Merrijoy 1995 Activists and Delegators:ElderlyPatients'PreferencesaboutControlat the End of Life. Social Science and Medicine41(4):537-545. Kim, KwangChung,andWon Moo Hurh 1993 Beyond Assimilation and Pluralism:Syncretic SocioculturalAdaptationof KoreanImmigrantsin the U.S. EthnicandRacialStudies 16(4):696-713. Kleinman,Arthur 1988 The Illness Narratives:Suffering,Healing,andthe HumanCondition.New York: Basic Books. Klessing,Jill 1992 The Effects of Values andCultureon Life-SupportDecisions. WesternJournalof Medicine 157(3):316-322. Koenig, BarbaraA., andJanGates-Williams 1995 UnderstandingCulturalDifference in Caringfor Dying Patients.WesternJournal of Medicine 163(3):244-249. Koenig, BarbaraA., andPatriciaMarshall 1994 Bioethics and the Politics of Race and Ethnicity:Respecting (or Constructing) Difference? Paper presented at the American AnthropologicalAssociation annual meeting,Atlanta,GA, December2. Landy,David 1977 Culture, Disease and Healing: Studies in Medical Anthropology. New York: MacmillanPublishing. 422 MEDICALANTHROPOLOGY QUARTERLY Levin, SanderM. 1990 PatientSelf-DeterminationAct of 1990. CongressionalRecord,Extensionsof Remarks,136(39) (April3):E943-E944. LindemannNelson, Hilde, andJamesLindemannNelson 1995 The Patientin the Family:An Ethicsof MedicineandFamilies.New York:Routledge. Lynn,J., andJ. M. Teno 1993 After the Patient Self-DeterminationAct: The Need for EmpiricalResearchon FormalAdvanceDirectives.HastingsCenterReport23(1):20-24. Marin,G., F. Sabogal,B. V. Marin,R. Otero-Sabogal,andE. Perez-Stable 1987 Developmentof a Short AcculturationScale for Hispanics.HispanicJournalof BehavioralScience 9:183-205. Marshall,PatriciaA. 1992 AnthropologyandBioethics.MedicalAnthropologyQuarterly6(1):49-73. Marshall,Patricia,andBarbaraA. Koenig 1996 Bioethics in Anthropology:Perspectiveson Culture,Medicine, and Morality.In Medical Anthropology:ContemporaryMethod and Theory. Revised edition. C. Sargent andT. Johnson,eds. Pp. 349-373. Westport,CT:PraegerPress. Marshall,Patricia,BarbaraA. Koenig,Donelle M. Barnes,andAnne J. Davis 1998 Multiculturalism,Bioethics,End of Life Care:Case Narrativesof LatinaCancer Patients.In HealthCareEthics:Issues for the 21st Century.J. ThomasmaandJ. Monagle, eds. Pp. 421-431. Gaithersburg,MD: Aspen Publishers. Marshall,Patricia,David C. Thomasma,andJurritBergsma 1994 InterculturalReasoning:The Challenge for InternationalBioethics. Cambridge Quarterlyof HealthcareEthics3(3):321-328. Mishler,Elliot G. 1986 ResearchInterviewing: ContextandNarrative.Cambridge,MA: HarvardUniversity Press. Morse,J. M. 1991 Approachesto Qualitative-Quantitative Triangulation.Nursing Research 40(2): 120-123. Muller,JessicaH. 1994 Anthropology,Bioethics,andMedicine:A ProvocativeTrilogy.MedicalAnthropology Quarterly8(4):448-467. Muller,JessicaH., andBrianDesmond 1992 EthicalDilemmasin Cross-CulturalContext:A ChineseExample.WesternJournal of Medicine 157(3):323-327. Murphy,SheilaT., JoycelynPalmer,StanleyAzen, Gelya Frank,Vicki Michel, andLeslie J. Blackhall 1996 Ethnicityand AttitudestowardAdvance Care Directives. Journalof Law, Medicine andEthics24(2):108-117. Nilchaikovit,Tana,JamesM. Hill, andJimmieC. Holland 1993 The Effectsof Cultureon Illness BehaviorandMedicalCare:Asian andAmerican Differences.GeneralHospitalPsychiatry15(1):41-50. Orona,Celia J., BarbaraA. Koenig,andAnne J. Davis 1994 CulturalAspects of Nondisclosure.CambridgeQuarterlyof Healthcareand Ethics 3(3):338-346. Orr,RobertD., PatriciaA. Marshall,andJamieOsborne 1995 Cross-CulturalConsiderationsin ClinicalEthicsConsultations.Archivesof Family Medicine4(2): 159-164. PATIENT AUTONOMY AND END-OF-LIFE DECISION MAKING 423 Park,Kyeyoung 1989 "BornAgain":WhatDoes It Meanto Korean-Americansin New YorkCity?Journal of RitualStudies3:287-301. 1996 Use and Abuse of Race and Culture:Black-KoreanTension in America. American Anthropologist98(3):492-499. 1997 KoreanAmericanDream:ImmigrantsandSmallBusinessin New YorkCity.Ithaca, NY: Corell UniversityPress. President'sCommissionfor the Studyof EthicalProblemsin Medicineand Biomedical and BehavioralResearch 1982 MakingHealthCare Decisions: The Ethical and Legal Implicationsof Informed Consentin the Patient-Practitioner Relationship.Washington,DC: GovernmentPrinting Office. 1983 Deciding to Forego Life-SustainingTreatment:A Reporton the Ethical,Medical andLegalIssuesinTreatmentDecisions.Washington,DC:GovernmentPrintingOffice. Rawls, John 1971 A Theoryof Justice.Oxford:OxfordUniversityPress. Rothman,DavidJ. 1991 Strangersat the Bedside: A History of How Law and Bioethics Transformed MedicalDecision Making.New York:Basic Books. Sachs, G. A., C. B. Stocking,and S. H. Miles 1992 Empowermentof the OlderPatient?A RandomizedControlledTrial to Increase Discussion and Use of Advance Directives.Journalof the AmericanGeriatricSociety 40(3):269-273. Sandel,MichaelJ. 1982 Liberalismandthe Limitsof Justice.Cambridge:CambridgeUniversityPress. Stange, K. C., W. L. Miller,B. F. Crabtree,P. J. O'Connor,and S. J. Zyzanski 1994 MultimethodResearch:Approachesfor IntegratingQualitativeand Quantitative Methods.Journalof GeneralInternalMedicine9(5):278-282. Steckler,A., K. R. McLeroy,R. M. Goodman,S. T. Bird,and L. McCormick 1992 Toward IntegratingQualitative and Quantitative Methods: An Introduction. HealthEducationQuarterly19(1):1-8. Steiber,S. R. 1987 Rightto Die: Public Balks at Deciding for Others.Hospitals61(5):72. Sugarman,J., M. Weinberger,andG. Samsa 1992 FactorsAssociatedwith Veterans'Decisions aboutLiving Wills. Archives of InternalMedicine 152(2):343-347. Teno, J., J. Fleischman,D. W. Brock,and V. Mor 1990 The Use of FormalPriorDirectives among Patientswith HIV-RelatedDiseases. Journalof GeneralInternalMedicine5(6):490-494. U.S. Departmentof Commerce 1992 1990 Census of Population;General Population Characteristics,United States. Washington,DC: GovernmentPrintingOffice. Veatch,RobertM. 1996 Which Groundsfor OverridingAutonomy Are Legitimate?HastingsCenterReport26(6):42-43. Woloshin,Steven,NinaA. Bickell,LisaM. Schwartz,FrancescaGany,andH. GilbertWelch 1995 Language Barriersin Medicine in the United States. Journalof the American MedicalAssociation273(9):724-728. Yeo, Gwen 1995 Ethical Considerationsin Asian and Pacific Island Elders. Clinics in Geriatric Medicine 11(1):139-152.





© Copyright 2026