
Corticosteroids in Peritonsillar Abscess Treatment: A Blinded Placebo-Controlled Clinical Trial
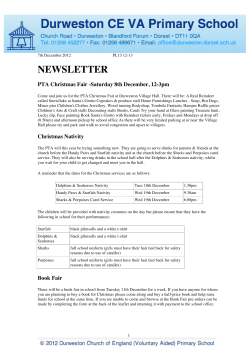
The Laryngoscope C 2013 The American Laryngological, V Rhinological and Otological Society, Inc. Corticosteroids in Peritonsillar Abscess Treatment: A Blinded Placebo-Controlled Clinical Trial Jason K. M. Chau, MD, MPH; Hadi R. Seikaly, MD, FRCSC; Jeffery R. Harris, MD, FRCSC; Cristina Villa-Roel, MD, MSc; Craig Brick, BSc; Brian H. Rowe, MD, MSc Objectives/Hypothesis: Sore throat is a common, benign emergency department (ED) presentation; however, peritonsillar abscess (PTA) is a complication that requires aggressive management. Use of systemic corticosteroids (SCSs) in PTA is occurring without clear evidence of benefit. This study examined the efficacy and safety of SCS treatment for patients with PTA. Study Design: Randomized, double-blind, placebo-controlled trial. Methods: A controlled trial with concealed allocation and double-blinding was conducted at two Canadian EDs. Following written informed consent, eligible patients received 48 hours of intravenous clindamycin and a single dose of the study drug (dexamethasone [DEX] or placebo [PLAC], intravenously [IV]). Follow-up occurred at 24 hours, 48 hours, and 7 days. The primary outcome was pain; other outcomes were side effects and return to normal activities/diet. Results: A total of 182 patients were screened for eligibility; 41 patients were enrolled (21 DEX; 20 PLAC). At 24 hours, those receiving DEX reported lower pain scores (1.4 vs. 5.1; P 5.009); however, these differences disappeared by 48 hours (P 5.22) and 7 days (P 5.4). At 24 hours, more patients receiving DEX returned to normal activities (33% vs. 11%) and dietary intake (38% vs 25%); however, these differences were not significant and disappeared by 48 hours and 7 days. Side effects were rare and did not differ between groups (P >.05). Conclusions: Combined with PTA drainage and IV antibiotics, 10 mg IV DEX resulted in less pain at 24 hours when compared to PLAC, without any serious side effects. This effect is short-lived, and further research is required on factors associated with PTA treatment success. Key Words: Peritonsillar abscess, sore throat, corticosteroids, relapse, randomized controlled trial. Level of Evidence: 1b Laryngoscope, 124:97–103, 2014 INTRODUCTION Classically called “quinsy” (derived from the Greek term kynanche, meaning “dog-strangle”) peritonsillar abscess (PTA) is regarded as the suppurative endpoint in the infectious continuum of pharyngitis, acute tonsilli- From the Department of Otolaryngology, University of Manitoba, Winnipeg, Manitoba, Canada (J.K.M.C.), Department of Surgery, Division of Otolaryngology–Head and Neck Surgery (H.R.S., J.R.H.), University of Alberta, Edmonton, Alberta, Canada, Department of Emergency Medicine (C.V.-R., C.B., B.H.R.), University of Alberta, Edmonton, Alberta, Canada, School of Public Health (C.V.-R., B.H.R.), University of Alberta, Edmonton, Alberta, Canada, University College Cork, Cork, Ireland (C.B.). Editor’s Note: This Manuscript was accepted for publication June 6, 2013. Presented at the 66th Annual Meeting of the Canadian Society of Otolaryngology–Head & Neck Surgery, Toronto, Ontario, Canada, May 20–22, 2012. The authors have no other funding, financial relationships, or conflicts of interest to disclose. Funding support for this project was generously provided by the University Hospital Foundation and the Department of Emergency Medicine Research Group at the University of Alberta (C.V.-R., C.B.). C.V.-R. is supported by the Canadian Institutes of Health Research (CIHR) in partnership with the Knowledge Translation branch. B.H.R. is supported by the CIHR as Tier I Canada Research Chair in Evidence-Based Emergency Medicine (Government of Canada). Send correspondence to Dr. Jason K. M. Chau, Department of Otolaryngology, University of Manitoba, GB421 Health Sciences Center, 820 Sherbrook Street, Winnipeg, Manitoba, Canada R3A 1R9. E-mail: [email protected] DOI: 10.1002/lary.24283 Laryngoscope 124: January 2014 tis, and peritonsillar cellulitis.1 Despite widespread antibiotic use to treat these infectious states, PTA remains the most common deep space infection of the head and neck in young adults.2,3 The incidence of PTA in the USA is approximately 30 cases per 100,000 people per year, with associated annual health care expenditures of $150 million.4 Its yearly peak incidence occurs in November to December and April to May, which parallels the incidence of streptococcal pharyngitis and acute tonsillitis.5,6 PTA occurs most commonly in those aged 20 to 40 years and affects males and females with equal frequency.2 Although PTA remains a common clinical entity encountered in various disciplines, significant debate exists with respect to the best methods of diagnosis, acute drainage, medical therapy, treatment setting, and indications for tonsillectomy, either urgent or elective. Management strategies vary,7 specifically with respect to the most effective method of abscess drainage and whether adjunctive systemic corticosteroids (SCSs) are beneficial. There is currently only one published report that has assessed the efficacy of adjunctive steroids in PTA treatment. Ozbek et al.8 found that patients who received corticosteroid therapy had improved recovery, as measured by several outcomes, over patients who received placebo. Despite this evidence, further studies are needed before recommendations for the routine use Chau et al.: Dexamethasone in PTA 97 of corticosteroids in PTA treatment can be made.9 We present a double-blind, placebo-controlled clinical trial comparing single-dose intravenous (IV) dexamethasone to placebo that further addresses this question. MATERIALS AND METHODS appearing vials for both dexamethasone and placebo. Vials were only administered to trial patients once enrollment had occurred and the abscess had been drained by needle aspiration. The use of identically looking vials for both the treatment drug and placebo also allowed for blinding of treatment group assignment and blinding of the outcome assessment and datahandling processes. Research Questions The primary research question addressed by this study was whether single-dose IV dexamethasone (10 mg), administered after needle drainage of a unilateral PTA, results in decreased pain levels when compared to placebo as measured with a validated subjective pain scale. Secondary questions included the effect of single-dose IV dexamethasone (10 mg) on mouth opening, body temperature, time to painless oral (per os [PO]) intake, and time to return to “normal” activity as compared to placebo. Setting This was a two-site trial including a single tertiary-level care academic referral center and a single community-based emergency clinic. Patient Recruitment and Enrollment Patient recruitment was achieved via telephone or pager referral to research staff by attending Emergency Physicians and Otolaryngology–Head & Neck Surgery residents. Consent was obtained by affiliated clinical research nursing staff from patients who met the following eligibility criteria: 1) age > 17 years, 2) PTA confirmed by needle aspiration of frank pus, 3) ability to comprehend and complete a written questionnaire, 4) English-speaking, and 5) competent to provide informed consent. Patients were excluded if they had received SCS treatment within 72 hours of presentation, had documented PTA within the previous 30 days (considered recurrent PTA), had a “dry tap” needle aspiration (no pus expressed), had bilateral PTA, or had complicated PTA requiring admission (e.g., severe dehydration, airway compromise, or involvement of another deep neck space). Treatment Groups, Randomization, Concealment, and Blinding Patients were assigned into either intervention or control groups after inclusion criteria were satisfied and the patient provided signed informed consent to participate in the trial. The a priori randomization strategy occurred at the level of the pharmacy and was to be by random computer number generation in blocks of 10, stratified by center. One hundred brown opaque vials, labeled with numerals ascending from 1 through 100, were prepared with either dexamethasone (10 mg of IV preparation) or placebo. These vials were delivered to the trial sites and kept in a designated locked area of the respective emergency department (ED) with access only available to study-affiliated nurses and assistants. Vials were used sequentially in order of ascending number starting at vial #1. The control intervention contained 10 ml of sterile saline, and the intervention consisted of 10 mg of dexamethasone phosphate (Sabex, Cassola, Italy; bin #00664227) with methylparaben (0.15%) and propylparaben (0.02%) preservative. The shelf life of both agents was 1 year. Concealment of allocation was achieved by keeping all randomization information solely at the involved dispensary pharmacy and by using identically Laryngoscope 124: January 2014 98 Study Protocol The PTA management included surgical and medical treatments as follows. Surgical. The surgical site was anesthetized with local injection of 0.5 to 1.0 mL of 1% Xylocaine with epinephrine, if no allergy history was present. Needle aspiration was performed with an 18-gauge needle mounted on an empty 10-mL syringe, without ultrasound guidance. The needle aspirate was sent for Gram stain as well as culture and sensitivity microbial analysis. Medical. All patients received an IV fluid bolus of 1 L of normal saline over 1 hour, IV analgesia (usually ketorolac 30 mg), and IV antibiotics. Ketorolac was preferentially administered as part of a narcotic sparring strategy of the regional EDs. If allergic sensitivity to ketorolac had been documented or reported by the patient, morphine was administered (2.5–5.0 mg IV). Most patients received IV clindamycin (600 mg every 8 hours) for 48 hours, with the first dose being delivered in the ED and subsequent doses administered in a dedicated outpatient IV clinic. If a history of an allergy to clindamycin was present, then IV cefazolin (Ancef 1 g every 8 hours) and metronidazole (Flagyl 500 mg IV every 8 hours) were administered. Following at least 48 hours of IV clindamycin, patients were converted to equivalent-dose oral preparations (e.g., clindamycin 300 mg three times daily) for 12 days to ensure a total duration of antibiotic therapy of 14 days. In patients who had a history of allergy to clindamycin, Clavulin (amoxicillin–clavulanic acid/Augmentin 875 mg PO twice daily) was prescribed. Data Collection At presentation and following informed consent, the patient’s history was documented, with demographic (e.g., sex, age), chief complaint, and associated upper aerodigestive tract symptom data being recorded. Associated symptoms of PTA were recorded, including progressive dysphagia, odynophagia, voice alteration, malaise, and lethargy. Social history and allergic history were also recorded in addition to any recent prescription antibiotic or steroid use. One of the study investigators performed and documented a physical examination, which included general appearance, vital signs including temperature, voice quality, trismus (poor mouth opening recorded using interincisor distance), and important oropharyngeal findings. Outcomes, Outcome Measures, and Follow-up The primary outcome in this trial was that of subjective, patient-reported levels of pain. This was measured on a 10-point visual analog scale (VAS) that has been well validated for measuring subjective pain levels in the ED patient population.10,11 Based on Gallagher et al. and Bijur et al.’s reports, a change score of 1.3 on a 10-point VAS in ER patients was chosen as the minimal clinically important difference (MCID) that would drive a subsequent change in PTA management protocols.10 Secondary outcomes included mouth opening (in centimeters), body temperature (in degrees Celsius), and time to painless PO intake (in hours). Mouth opening, as recorded as interincisor distance, was measured with a standard 12-cm Chau et al.: Dexamethasone in PTA Fig. 1. CONSORT diagram showing the flow of participants through each stage of a randomized trial. F-U 5 follow-up; PTA 5 peritonsillar abscess. ruler, with the smallest increments of measure being millimeters. The incisal surfaces of the mesial upper and lower incisors were used as reference measuring points in all patients. Body temperature was measured with a standard oral thermometer in units of degrees Celsius, with precision to the nearest 10th of a degree. Time to painless PO intake was measured in hours and subjectively reported by patients in a take-home diary. Follow-Up Data collection for the first 48 hours was achieved with self-reported patient diaries. The diaries required a grade 7 reading level (Canada) and were completed at enrollment and at each subsequent outpatient IV clinic visit for a total of 6 data collection points. A patient’s clinical progress was reviewed and examined by blinded research staff at the 24- and 48-hour time points in the outpatient IV clinic. Subjective patientreported diaries were checked for completeness and collected at the last IV outpatient clinic visit. Follow-up at the 7-day time point was performed by phone. Patients were given the on-call staff otolaryngologist’s office contact details to arrange follow-up for reassessment and possible tonsillectomy. Statistics Descriptive data included proportions and means with standard deviations or medians with interquartile range, as appropriate. Bivariate analyses for dichotomous and for continuous variables were performed by v2 tests, t tests, or Laryngoscope 124: January 2014 Mann–Whitney tests. Analyses for continuous variables over time were performed using analysis of variance. All analyses (including sample size and post hoc power calculations) were performed using STATA statistical software (release 10.0; (Stata Corporation, College Station, TX). Ethics The Health Research Ethics Board of the University of Alberta approved this trial. Informed written consent was obtained from each patient prior to enrollment. RESULTS Participants One hundred eighty-two patients were screened for eligibility, with 122 being deemed ineligible. Of these, 41 patients were enrolled (21 dexamethasone; 20 placebo). Figure 1 summarizes the screening process and shows the flow of participants through each stage of the trial according to the CONSORT guidelines for reporting randomized control trials. Figure 1 also outlines the various reasons for ineligibility and exclusion. The most common reason for patient exclusion was their receiving corticosteroids within 72 hours prior to presentation (23%). This trend became more prominent as the time course of the trial went on and resulted in the study being terminated early. Chau et al.: Dexamethasone in PTA 99 TABLE I. Comparison of Patient Demographics, Symptoms, and Clinical Characteristics. PLAC, n 5 20 DEX, n 5 21 Age, yr, median (IQR) 29 (21–37) 22 (19–29) .138 Male sex, No. [%] Marital status, No. [%] 14 [70] 14 [66.7] .819 10 [50] 13 [61.9] .524 7 [35] 3 [14.3] 15 [75] 11 [52.4] .21 3 [15] 5 [25] 7 [33.3] 8 [38.1] .035 9 [45] 7 [33.3] .662 5 (3–6) 5 (3–6) .957 18 [90] 20 [95.2] .606 .218 Characteristic P Demographics Single Married Work status, No. [%] Working School University education, No. [%] Smoker, No. [%] Symptoms at presentation Length of symptoms, d, median (IQR) Dysphagia, No. [%] Current diet, No. [%] Fluids only NPO Soft diet and DAT Currently on antibiotics, No. [%] Prior history of PTA, No. [%] 6 [30] 12 [57.1] 7 [35] 6 [28.6] 6 [30] 15 [75] 3 [14.3] 12 [57.5] .228 6 [30] 5 [23.8] .655 37.1 6 0.7 37.3 6 0.7 .729 2.8 (2–3.5) 3.1 (2.5–4.0) .175 1.2 (0.2–4.5) 3.0 (1.1–5.5) .094 663 662 .573 Clinical characteristics Body temperature, C, mean 6 SD Interincisor distance, cm, median (IQR) Amount of pus drained, mL, median (IQR) Pain score, /10 on VAS 6 SD DAT 5 diet as tolerated; DEX 5 dexamethasone; IQR 5 interquartile range; NPO 5 nothing by mouth; PLAC 5 placebo; PTA 5 peritonsillar abscess; SD 5 standard deviation; VAS 5 visual analogue scale. Primary Outcome Subjective pain scores. Analysis of patientreported pain scores at the 24-hour, 48-hour, and 7-day time points revealed significant differences between treatment groups exclusively at the 24-hour endpoint (Fig. 2). The dexamethasone treatment group had median pain scores of 1.4 after 24 hours versus the control group’s median score of 5.1. This significant difference of 3.7 disappeared at the 48-hour and 7-day time points. Intragroup analysis of change over time was performed and revealed a statistically significant change over time in the dexamethasone group but not the control group. Analysis of analgesic and anti-inflammatory use after 48 hours and 7 days revealed no significant differences between the treatment groups (Table II). Secondary Outcomes Body temperature was found to significantly differ at the 24-hour time point but not at the 48-hour measurement (Table II). Trismus, measured as interincisor distance, was not significantly different between groups; however, there was a trend to statistical significance at the 48-hour time point favoring dexamethasone (Table II). In terms of subjectively reported return to normal activity, significant differences between groups were noted at the 24-hour time point; however, these differences were nonsignificant at the 48-hour and 7-day measurements (Fig. 3). There were no significant differences found between groups in subjectively reported return to normal diet (Fig. 4). Complications and Side Effects Side effect profiles of both treatment arms were also recorded. Important side effects collected included nausea, vomiting, drowsiness, restlessness, muscle spasms, and diarrhea. As given in Table II, there were no significant differences noted in side effects at the 48hour and 7-day time points. Dropouts/Withdrawals Overall, only 1 patient from each group failed to provide 7-day follow-up; however, not all patients were captured at each follow-up. For example, at 48 hours 4 patient outcomes could not be ascertained (1 placebo, 3 dexamethasone). Patient Characteristics Demographic details of both treatment groups are compared in Table I. There were no significant differences noted except in level of educational achievement. Clinical data comparisons with respect to patient symptoms at the time of presentation to the ER are presented in Table I. There were no significant differences between groups noted. Baseline clinical measurements are also presented in Table I. There were no significant differences found between treatment groups. Laryngoscope 124: January 2014 100 Fig. 2. Comparison of subjectively reported pain scores at 24 hours, 48 hours, and 7 days in peritonsillar abscess patients receiving dexamethasone (dark boxes) or placebo (white boxes). Chau et al.: Dexamethasone in PTA TABLE II. Measurement of ED and Post-ED Cointerventions and Outcomes. PLAC, n 5 20 Intervention/Outcome DEX, n 5 21 P 9 (42.9) 5 (23.8) .606 .734 .867 1 Medication administered in the ED, No. (%) Analgesic Anti-inflammatory 7 (35) 6 (30) Medication taken within 48 hours, No. (%) Analgesic Anti-inflammatory 11 (55) 1 (5) 11 (52.4) 1 (4.8) Body temperature, C, mean 6 SD .004* .001* Baseline 37.1 6 0.7 37.3 6 0.7 .729 24 hours 48 hours 36.7 6 0.8 36.3 6 0.6 36.0 6 0.5 36.3 6 0.7 .008† 1 Fig. 4. Comparison of subjectively reported return to normal diet in peritonsillar abscess patients receiving dexamethasone (black bars) or placebo (gray bars). 3.1 [2.5–4.0] 3.9 6 1.3 .175 .059 DISCUSSION .509 .35 Trismus, interincisor distance, cm Baseline, median [IQR] 48 hours, mean 6 SD 2.8 [2.0–3.5] 3.3 6 1.2 Side effects at 48 hours, No. (%) Nausea Vomiting 4 (20) 2 (10) 2 (9.5) 3 (14.3) Drowsiness 8 (40) 6 (28.6) .66 Restlessness Muscle spasms 2 (10) 2 (10) 3 (14.3) 2 (9.5) .651 .844 0 0 Diarrhea Side effects at 7 days, No. (%) Nausea Vomiting Drowsiness Restlessness Muscle spasms Diarrhea 0 2 (9.5) .107 0 1 (4.8) .356 1 (5) 0 2 (9.5) 1 (4.8) .505 .356 0 2 (9.5) .107 2 (10) 4 (19) .287 *Analysis of variance. † Statistically significant. DEX 5 dexamethasone; ED 5 emergency department; IQR 5 interquartile range; PLAC 5 placebo; SD 5 standard deviation. Fig. 3. Comparison of subjectively reported return to normal activity in peritonsillar abscess patients receiving dexamethasone (black bars) or placebo (gray bars). Laryngoscope 124: January 2014 Despite widespread use of antibiotics for treating tonsillitis and pharyngitis, PTA remains a common clinical entity encountered in the ED. Although any age group can be affected, PTA is most common in adolescents and young adults between the ages of 20 and 40 years.2 The bacteriology has remained relatively constant during the past half century, with Streptococcus species being the most common organisms cultured.12,13 Despite its frequency, significant debate exists regarding PTA management7; specifically, the method of abscess drainage and the role of adjunctive corticosteroids. The use of systemic corticosteroids as adjunctive therapy has been reported as safe and effective, and has become more commonplace in recent years.14–16 This methodologically rigorous trial evaluated the effectiveness of dexamethasone compared to placebo. A statistically significant difference in subjective pain scores was found at the 24-hour post-treatment time point. An overall effect size of 3.7 was noted between treatment groups in favor of dexamethasone. This is 2.7 times the a priori chosen MCID of 1.3 that has been well validated in our target setting. This large effect size, emerging despite lower than expected enrollment, is undoubtedly clinically important and is certainly compelling evidence to advocate for a change in practice. Using a comprehensive search strategy, only one other published study was identified that assessed the efficacy of adjunctive steroids in PTA treatment. Ozbek et al.8 compared intramuscular methylprednisolone to placebo in a randomized prospective fashion. Patients were admitted to hospital and received either intramuscular (IM) methylprednisolone or placebo, along with abscess drainage by needle aspiration and intravenous antibiotics (which were continued for at least 2 days and until the patient improved). Specific outcomes assessed included hours hospitalized, throat pain, time to oral intake, fever, and trismus. The authors found a statistically significant difference in trismus severity, dysphagia levels, body temperature, and hours hospitalized favoring the use of steroids without noting any increase in frequency of complications. Chau et al.: Dexamethasone in PTA 101 Our present study differs from Ozbek’s in several aspects. First, we present a clinical trial on PTA management in an outpatient setting. Second, we compared treatment groups based on a primary outcome of subjective pain. Third, we employed a pain scale and MCID that have been well validated.10,11 Fourth, our trial assessed subjective return to normal activity, which although not a direct quality of life (QOL) measure, can reasonably be interpreted as a surrogate for overall QOL. Last, we compared IV dexamethasone, rather than IM methylprednisolone, to placebo. Dexamethasone administered intravenously was chosen because IM drug administration may have affected pain score reports and carries with it the potential complications of infection, hematoma, and myonecrosis. Moreover, there is greater support for use of dexamethasone in the published literature in our target population.14–16 Overall, we feel our study represents high-quality evidence in a North American context. No significant differences were noted in trismus severity or dysphagia levels in this trial. These findings contradict findings of the prior study.8 Whereas Ozbek8 noted significant improvement of trismus in the methylprednisolone group after 12 and 24 hours, we found no such difference. The units of measure employed may explain this difference. Interincisor distance measured to the nearest 10th of a centimeter was used in our trial, whereas percentage improvement scores are presented in Ozbek’s trial. Comparing change scores may predispose to finding differences not found when comparing objective measurements. Similarly with dysphagia levels, we found no significant differences between our treatment groups. This disparity from the prior published trial may be due to the outcome measures used. Objective assessment of ability to swallow water (as performed in Ozbek’s trial) is certainly different from subjective reports of time to return to a normal diet. Limitations This study has several potential limitations. First, the study was concluded prematurely due to increasing difficulty enrolling patients. Over the time course of the trial, patients received IV steroids prior to their presentation at the tertiary care ED more frequently, thus limiting our eligible patient pool. Despite the decision being made to stop prior to data analysis, a large and statistically significant effect size was identified. Post hoc power calculation confirmed that our sample of 41 patients was more than adequate to detect the observed difference between treatment groups >80% of the time. Second, with a small sample size, the groups were not exactly balanced and adjustment was not possible; however, the majority of imbalances favored the placebo group. Third, although it is likely that single-dose dexamethasone is relatively safe, it is important to point out that this study did not follow patients beyond 7 days and may have missed uncommon or delayed adverse events. Given the frequency of sore throats and PTA, additional studies may be required to assess the likeliLaryngoscope 124: January 2014 102 hood of rare or long-term adverse events such as PTA recurrence or deep neck space infection. Fourth, the protocol required needle aspiration and IV antibiotics as the minimal standard of care, and in a small proportion of (excluded) cases the aspiration failed. Although these patients were excluded (and therefore did not enter into our analysis), some may argue that surgical blade drainage should have been employed rather than needle aspiration, as the degree of anatomic decompression that is achievable is greater. It is possible that scalpel drainage may have expressed pus where the needle aspiration did not. Khayr’s work3 coupled with our own center’s experience led to the choice of needle aspiration, and we do not believe this choice invalidates the results of the trial. Finally, the allocation process, although concealed and blinded, was controlled by a noninstitutional pharmacy. This may have introduced uncontrolled bias; however, we believe these possible biases do not invalidate the observed results. CONCLUSION In the clinical setting of unilateral PTA treated with needle aspiration and IV antibiotics, a single 10-mg dose of IV dexamethasone administered following needle aspiration results in reduced subjective pain levels and improved patient QOL at 24 hours without any adverse side effects or morbidity when compared to IV antibiotics alone. This option should be considered in patients with unilateral PTA who have severe pain in the ED; however, due to the short-term transient nature of the benefit, the treatment decision should be weighed against possible later adverse events such as PTA recurrence or deep neck space infection. Acknowledgments The authors thank the research coordinators for the study at each site: Virginia Willis (University of Alberta Hospital, Edmonton, Alberta, Canada) and Debbie Boyko (Northeast Community Health Centre, Edmonton, Alberta, Canada). BIBLIOGRAPHY 1. Passy V. Pathogenesis of peritonsillar abscess. Laryngoscope 1994;104: 185–190. 2. Steyer TE. Peritonsillar abscess: diagnosis and treatment. Am Fam Physician 2002;65:93–96. 3. Khayr W, Taepke J. Management of peritonsillar abscess: needle aspiration versus incision and drainage versus tonsillectomy. Am J Ther 2005; 12:344–350. 4. Lyon M, Glisson P, Blaivas M. Bilateral peritonsillar abscess diagnosed on the basis of intraoral sonography. J Ultrasound Med 2003;22:993–996. 5. Belleza WG, Kalman S. Otolaryngologic emergencies in the outpatient setting. Med Clin North Am 2006;90:329–353. 6. Bisno AL, Gerber MA, Gwaltney JM, Kaplan EL, Schwartz RH, for the Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin Infect Dis 2002;35:113–125. 7. Johnson RF, Stewart MG. The contemporary approach to diagnosis and management of Peritonsillar abscess. Curr Opin Otolaryngol Head Neck Surg 2005;13:157–160. 8. Ozbek C, Aygenc E, Tuna EU, et al. Use of steroids in the treatment of peri-tonsillar abscess. J Laryngol Otol 2004;118:439–442. 9. Galioto NJ. Peritonsillar abscess. Am Fam Physician 2008;77:199–202. 10. Gallagher EJ, Liebman M, Bijur PE. Prospective validation of clinically important changes in pain severity measured on a visual analog scale. Ann Emerg Med 2001;38:633–638. Chau et al.: Dexamethasone in PTA 11. Bijur PE, Latimer CT, Gallagher EJ. Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Acad Emerg Med 2003;10:390–392. 12. Herzon FS, Harris P. Mosher Award Thesis. Peritonsillar abscess: incidence current management practices, and a proposal for treatment guidelines. Laryngoscope 1995;105:1–17. 13. Herzon FS, Martin AD. Medical and surgical treatment of peritonsillar, retropharyngeal, and parapharyngeal abscesses. Curr Infect Dis Rep 2006;8:196–202. Laryngoscope 124: January 2014 14. O’Brien JF, Meade JL, Falk JL. Dexamethasone as adjuvant therapy for sever acute pharyngitis. Ann Emerg Med 1993;22:212–215. 15. Wei JL, Kasperbauer JL, Weaver AL, Boggust AJ. Efficacy of single-dose dexamethasone as adjuvant therapy for acute pharyngitis. Laryngoscope 2002;112:87–93. 16. Marve-Valls EG, Stuckey A, Ernst AA. A randomized clinical trial of oral versus intramuscular delivery of steroids in acute exudative pharyngitis. Acad Emerg Med 2002;9:9–14. Chau et al.: Dexamethasone in PTA 103










© Copyright 2026