
Intralesional Sodium Thiosulfate for the Treatment of Calciphylaxis
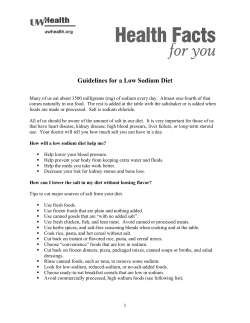
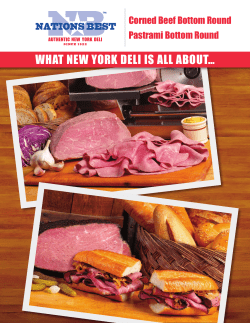
Research Case Report/Case Series Intralesional Sodium Thiosulfate for the Treatment of Calciphylaxis Lauren Strazzula, BA; Sagar U. Nigwekar, MD; David Steele, MD; William Tsiaras, MD, PhD; Meghan Sise, MD; Sabina Bis, MD; Gideon P. Smith, MD, PhD; Daniela Kroshinsky, MD, MPH IMPORTANCE Calciphylaxis is a potentially fatal disorder of abnormal calcium deposition. Patients commonly present with painful retiform to stellate purpuric lesions that often undergo ulceration and necrosis, increasing the risk of infection and life-threatening sepsis. Treatment is multifaceted, and improved outcomes have been demonstrated with intravenous sodium thiosulfate; however, the use of this medication can be limited by its adverse effects. The use of topical sodium thiosulfate has been successfully reported for superficial calcium deposits in the skin from other processes. Therefore, we hypothesized that intralesional (IL) sodium thiosulfate may be an effective treatment for the deeper lesions of cutaneous calciphylaxis. We provide a retrospective case review of 4 patients with calciphylaxis who were treated with IL sodium thiosulfate. OBSERVATIONS Four patients with biopsy-proven cutaneous calciphylaxis were treated with IL sodium thiosulfate (250 mg/mL) in areas of clinically active disease. The patients tolerated the medication well, with only transient localized discomfort during injection. All 4 patients had complete healing of their ulcers and remission of disease. CONCLUSIONS AND RELEVANCE Intralesional sodium thiosulfate may be an effective and well-tolerated treatment for localized calciphylaxis. This novel approach requires further research and investigation. Corresponding Author: Daniela Kroshinsky, MD, MPH, Department of Dermatology, Massachusetts General Hospital, 50 Staniford St, Boston, MA 02114 ([email protected]). JAMA Dermatol. 2013;149(8):946-949. doi:10.1001/jamadermatol.2013.4565 Published online June 12, 2013. C alciphylaxis is an often fatal vasculopathy characterized by calcium deposition in the media of small vessels leading to mural proliferation, thrombosis, and fibrosis resulting in downstream ischemia and necrosis of surrounding local tissue.1 This disorder is most prevalent in patients with end-stage renal disease, but additional risk factors include a longitudinally elevated calcium-phosphorus product (Ca2+ × PO4), female sex, diabetes mellitus, warfarin therapy, protein C or S deficiency, cholecalciferol supplementation, autoimmune disease, and obesity.1,2 Patients with calciphylaxis are at risk for many complications, including ulceration, poor wound healing, local infection, and sepsis. Mortality approaches 80%.3 Standard treatment for calciphylaxis has aimed at removing potential triggers and providing local wound care. In 2004, Cicone et al4 reported the successful use of intravenous (IV) sodium thiosulfate in the treatment of calciphylaxis. Since then, several studies have supported the use of this medication; however, its application may be limited by adverse effects, such as gastrointestinal upset, metabolic acidosis, and sodium overload.5,6 Thus, alternative approaches for the treatment of calciphylaxis are needed. Sodium thiosulfate has been used topically for the treatment of other disorders of cutaneous calcium deposition, namely, calcinosis cutis.7,8 However, to our knowledge, there 946 JAMA Dermatology August 2013 Volume 149, Number 8 Downloaded From: http://jamanetwork.com/ on 09/09/2014 Author Affiliations: Department of Dermatology, Massachusetts General Hospital, Boston (Strazzula, Tsiaras, Bis, Smith, Kroshinsky); Department of Nephrology, Massachusetts General Hospital, Boston (Nigwekar, Steele); Department of Internal Medicine, Massachusetts General Hospital, Boston (Sise). are no reports in the literature describing this type of localized delivery of sodium thiosulfate for the treatment of calciphylaxis. Because the deeper histopathologic features of calciphylaxis are unlikely to be reached by topical therapeutic agents, we hypothesized that intralesional (IL) sodium thiosulfate may effectively treat patients with localized cutaneous disease. Report of Cases Case 1 A 66-year-old woman with a history of stage III chronic kidney disease (estimated glomerular filtration rate, 50 mL/min/1.73m2), diabetes, hypertension, hyperlipidemia, and hypothyroidism presented to the dermatology clinic with calciphylaxis. Six months earlier, after minor trauma to her left leg, an exquisitely painful ulceration had developed, which was treated at an outside hospital with wound care, debridement, and multiple courses of oral antibiotics, without improvement. Three months later, wound biopsy findings were consistent with a diagnosis of calciphylaxis or pyoderma gangrenosum. One month later, findings of another biopsy confirmed the diagnosis of calciphylaxis. The patient was treated with prednisone, cyclosporine, and pain management. jamadermatology.com Sodium Thiosulfate Treatment of Calciphylaxis Case Report/Case Series Research Figure 1. Clinical Photographs of Patient 1’s Left Leg A B C D A, Large ulceration on the posterior aspect of the leg extends circumferentially, with surrounding purpura indicating active disease. B, As the ulcer gradually decreased in size, remaining areas of purpura were injected with sodium thiosulfate. C, At 12 weeks, the ulcer was nearly healed, with no signs of active disease. D, Six months after presentation, the ulcerations had healed. She then presented to our institution for a second opinion because of increased pain and enlargement of her ulcer. Further questioning revealed that hypocalcemia had been diagnosed 4 years earlier, and the patient had started taking oral calcitriol (0.25 μg/d). She also began taking over-the-counter calcium, cholecalciferol, aspirin with calcium, and a multivitamin with calcium daily. Given concerns that this regimen triggered her calciphylaxis, these medications were discontinued. Her parathyroid hormone (PTH), calcium, and cholecalciferol levels were normal. Her serum creatinine level of 1.1 mg/dL (reference range, 0.60-1.5 mg/dL) (to convert to micromoles per liter, multiply by 88.4) and phosphorus level were slightly elevated, at 4.8 mg/dL ( reference range, 2.6-4.5 mg/ dL) (to convert to millimoles per liter, multiply by 0.323). Physical examination showed a circumferential 12 × 18.5cm2 irregularly bordered ulcer on the left leg with areas of hypergranulation, fibrotic debris, and foci of stellate purpura indicative of active disease. Sodium thiosulfate (1 mL) was injected into the active violaceous border (unless otherwise noted, the concentration of IL sodium thiosulfate was 250 mg/mL in all patients). The patient was instructed to apply col- lagenase twice daily to the fibrotic areas, and silver nitrate was applied to areas of fibrosis and hypergranulation. One week later, the patient returned to the clinic with decreased pain. Examination revealed a small remaining focus of purpura (Figure 1A). During the next month, 3 additional injections of sodium thiosulfate (each 3-4 mL) were administered into areas of persistent purpura, and the patient’s symptoms improved rapidly (Figure 1B and C). She tolerated each injection well, complaining only of transient local pain during injection. Laboratory values at baseline and after the second treatment revealed no notable metabolic adverse events. Pain management and local wound care were continued, with steady improvement. Six months after presentation, the patient’s ulcer was completely healed (Figure 1D). jamadermatology.com Downloaded From: http://jamanetwork.com/ on 09/09/2014 Case 2 A 68-year-old obese woman with a history of stage III chronic kidney disease (estimated glomerular filtration rate, 49 mL/ min/1.73m2), paroxysmal atrial fibrillation treated with warfarin, diabetes, and hypertension was referred to the dermatology clinic for a nonhealing ulcer on her left leg. JAMA Dermatology August 2013 Volume 149, Number 8 947 Research Case Report/Case Series Sodium Thiosulfate Treatment of Calciphylaxis Figure 2. Clinical Photographs of the Medial Aspect of Patient 4’s Right Thigh A B A, Cutaneous necrosis with overlying dry eschar and surrounding purpura. B, Twenty weeks after presentation, the ulcer was completely healed. The ulcer had first appeared 8 months earlier and was thought to be secondary to trauma. She was treated by her primary care physician with wound care, antibiotics, and outpatient wound debridement. Six months later, she was evaluated by a general surgeon and underwent wound debridement and vacuumassisted closure placement in the operating room, followed by split-thickness skin grafting. Tissue sent for evaluation at this time was consistent with calciphylaxis. The PTH and phosphorus were elevated at 80 pg/mL (reference range, 10-60 pg/mL) (to convert to nanograms per liter, multiply by 1.0) and 4.9 mg/dL, respectively. Creatinine, calcium, and cholecalciferol levels were normal. On presentation to the dermatology clinic, the patient reported that her ulcer was nearly healed but noted the development of a new, mildly painful ulcer on the medial aspect of her left ankle. Examination disclosed a poorly defined erythematous plaque with central ulceration and fibrinous debris. There was no evidence of active disease, and the patient was treated with local wound care. She was seen by the nephrology service, and treatment was started with alendronate, sevelamer, and pentoxifylline. Warfarin treatment was discontinued. Four weeks later, the patient returned to the clinic with exquisite pain and worsening of the left ankle ulcer, which had enlarged and developed a stellate violaceous rim. Sodium thiosulfate (1 mL) was injected around the rim and in the center of the wound. Wound care consisted of collagenase and a fenestrated silicone dressing. At week 6, the patient reported marked improvement, and the ulcer was again injected with 1 mL of sodium thiosulfate. At week 8, the areas of purpura were nearly resolved, and there was good evidence of regranulation. She was treated with another 1 mL of sodium thiosulfate. Other than mild transient pain, the patient tolerated all of the injections well, with no adverse events. Laboratory values at baseline and after the second treatment revealed no metabolic abnormalities. By week 11 the purpura had completely resolved, and at week 20 the patient no longer had pain, and her ulcer was healed. 948 JAMA Dermatology August 2013 Volume 149, Number 8 Downloaded From: http://jamanetwork.com/ on 09/09/2014 Case 3 A 65-year-old obese woman with stage IV chronic kidney disease (estimated glomerular filtration rate, 20 mL/min/ 1.73m2), diabetes, and hypertension was referred to the dermatology clinic by the nephrology service for suspected calciphylaxis. Laboratory values included elevated PTH and phosphorus levels, at 130 pg/mL and 5.8 mg/dL, respectively. The patient reported a 3-week history of painful nodules on both thighs. Examination revealed erythematous tender plaques with significant induration on the lateral parts of her thighs and focal areas of violaceous subcutaneous nodules. Initial skin biopsy results were nondiagnostic, but a second biopsy confirmed the diagnosis of calciphylaxis. Treatment was started with sevelamer and cinacalcet. Two weeks later, the patient returned to the dermatology clinic with excruciating pain around her biopsy site. At examination, she had superficial ulceration around the biopsy sites with foci of early stellate purpura and surrounding induration on the lateral aspect of her right thigh. She was treated with 2 mL of IL sodium thiosulfate around the rim of the lesion and given hydrocolloid dressings for local wound care. At week 4, she noticed decreased pain and resolution of her purpura but thought that her ulcer was still expanding. More sodium thiosulfate was injected, 1 mL each in the ulcer on the right thigh and the purpuric lesions on the right medial leg and left lateral thigh. The patient was seen weekly, receiving 14 rounds of IL sodium thiosulfate over the following 15 weeks. Depending on ulcer size, between 1 and 3 mL of IL sodium thiosulfate was injected into each lesion, with steady improvement. She tolerated each injection well, without any adverse events other than local discomfort from the procedure. Laboratory values at baseline and twice throughout treatment revealed no metabolic acidosis. At 25 weeks after initial biopsy, the ulcerations had healed. Case 4 A 67-year-old obese man with stage II chronic kidney disease (estimated glomerular filtration rate, 64 mL/min/1.73m2), a history of atrial fibrillation taking warfarin therapy, chronic lowerextremity edema, hypertension, and gout was admitted to the hospital with right thigh swelling and pain. Two weeks earlier, he had been admitted with an elevated international normalized ratio of 12.8 that had no known precipitant. A dermatology consultation was requested. Physical examination revealed an indurated violaceous plaque with overlying stellate necrosis and ulceration on the medial aspect of the right thigh with associated tenderness, scored as 12 on a scale of 1 to 10 (Figure 2A). Large indurated plaques with retiform purpura were seen on the right lateral and left medial thighs. Findings from a skin biopsy confirmed a diagnosis of calciphylaxis. Creatinine, calcium, and phosphorus levels were within normal limits. Treatment was started with sevelamer, sildenafil, and pentoxifylline, along with pain management and local wound care. The lesion on the medial aspect of the patient’s right thigh was injected for 3 consecutive days with 2 mL of sodium thiosulfate (250 mg/mL diluted 1:1 with 1% lidocaine), and treatment with IV sodium thiosulfate (12.5 g/d) was started several days later. The patient tolerated the injections well, and daily laboratory measurements revealed no metabolic acidosis. The injected area imjamadermatology.com Sodium Thiosulfate Treatment of Calciphylaxis Case Report/Case Series Research proved rapidly, with decreased pain. The adjacent uninjected areas continued to ulcerate, and the dosage of IV sodium thiosulfate was increased to 25 g/d. On hospital day 33, the patient was discharged to a rehabilitation facility, where he continued to receive IV sodium thiosulfate for approximately 3 months until it was discontinued because of severe nausea and decreased oral intake requiring nasogastic tube placement. He was followed up in the dermatology clinic, and his ulcerations continued to improve markedly. Five months later, his ulcerations had healed, and there was no recurrence of disease (Figure 2B). Discussion Sodium thiosulfate is a versatile inorganic salt that has been used intravenously for decades. Historically, this medication was used in the treatment of cyanide poisoning. It was later shown effective in treating calcium-mediated disorders.9 The mechanism of sodium thiosulfate in the treatment of calcium-related disorders is thought to be multifactorial. Evidence has shown that it acts as an anticalcification agent, with vasodilatory and antioxidant properties.10 Some research11 suggests that sodium thiosulfate inhibits the precipitation of calcium in tissues by increasing calcium solubility, and others12 hypothesize that sodium thiosulfate combines with calcium, forming a salt that can later be dialyzed. Although randomized clinical trials have not been performed in patients with calciphylaxis, IV sodium thiosulfate has emerged as an effective treatment for this potentially fatal disorder. Topical sodium thiosulfate has been used for a variety of cutaneous disorders, with more recent reports of use in calcium deposition disorders.4,7,8 Subcutaneous sodium thiosulfate treatment has only been reported in the treatment of mechloretha- ARTICLE INFORMATION Accepted for Publication: April 2, 2013. Published Online: June 12, 2013. doi:10.1001/jamadermatol.2013.4565. Author Contributions: Dr Kroshinsky had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Smith, Kroshinsky. Acquisition of data: Nigwekar, Steele, Tsiaras, Sise, Bis, Kroshinsky. Analysis and interpretation of data: Strazzula, Nigwekar, Kroshinsky. Drafting of the manuscript: Strazzula, Nigwekar, Steele, Kroshinsky. Critical revision of the manuscript for important intellectual content: Strazzula, Tsiaras, Sise, Bis, Smith, Kroshinsky. Administrative, technical, and material support: Nigwekar, Steele, Tsiaras, Sise, Bis, Kroshinsky. Study supervision: Tsiaras, Bis, Kroshinsky. Conflict of Interest Disclosures: None reported. REFERENCES 1. Wilmer WA, Magro CM. Calciphylaxis. Semin Dial. 2002;15(3):172-186. jamadermatology.com Downloaded From: http://jamanetwork.com/ on 09/09/2014 mine hydrochloride extravasation to neutralize this alkylating chemotherapy and prevent local tissue damage.13,14 Although, to our knowledge, no clinical trials have examined the safety and efficacy of subcutaneous sodium thiosulfate in humans, its administration in extravasation injuries is currently the standard of care in oncologic nursing practice.13,14 An advantage in treating dermatologic diseases is the accessibility of the target organ. Intralesional administration of medication is generally a low-risk, highly targeted method of delivery that can more deeply penetrate the skin than topical preparations, while avoiding systemic distribution. Given that IL sodium thiosulfate is already safely used in extravasation injury, we hypothesized that it may be an effective treatment in patients with localized calciphylaxis, which warrants further study. In particular, IL sodium thiosulfate may be valuable in nonuremic patients who lack the vascular access required for regular repeated doses of IV sodium thiosulfate. In addition, local delivery of sodium thiosulfate could bypass the potential adverse effects of IV administration, such as hypotension caused by rapid infusion, metabolic acidosis, or gastrointestinal upset. The main limitation of IL sodium thiosulfate is injection site discomfort, but pretreatment with topical anesthetic and/or dilution with lidocaine may be helpful. In our series, the medication was well tolerated, and complete wound healing was achieved in all patients. These results are limited somewhat by the fact that in some patients IL sodium thiosulfate was not given in isolation. In particular, our patient 4 received IV sodium thiosulfate after one of his lesions had been injected with IL sodium thiosulfate. However, we believe that the rapid reduction in pain and resolution of purpura observed in the treated lesion, compared with the untreated lesions, support our hypothesis. More research is needed to explore this novel approach to the treatment of calciphylaxis. 2. Nigwekar SU, Wolf M, Sterns RH, Hix JK. Calciphylaxis from nonuremic causes: a systematic review. Clin J Am Soc Nephrol. 2008;3(4):1139-1143. 9. Yatzidis H. Successful sodium thiosulphate treatment for recurrent calcium urolithiasis. Clin Nephrol. 1985;23(2):63-67. 3. Hafner J, Keusch G, Wahl C, et al. Uremic small-artery disease with medial calcification and intimal hyperplasia (so-called calciphylaxis). J Am Acad Dermatol. 1995;33(6):954-962. 10. Hayden MR, Goldsmith DJ. Sodium thiosulfate: new hope for the treatment of calciphylaxis. Semin Dial. 2010;23(3):258-262. 4. Cicone JS, Petronis JB, Embert CD, Spector DA. Successful treatment of calciphylaxis with intravenous sodium thiosulfate. Am J Kidney Dis. 2004;43(6):1104-1108. 5. Selk N, Rodby RA. Unexpectedly severe metabolic acidosis associated with sodium thiosulfate therapy in a patient with calcific uremic arteriolopathy. Semin Dial. 2011;24(1):85-88. 6. Schlieper G, Brandenburg V, Ketteler M, Floege J. Sodium thiosulfate in the treatment of calcific uremic arteriolopathy. Nat Rev Nephrol. 2009;5(9):539-543. 11. Papadakis JT, Patrikarea A, Digenis GE, et al. Sodium thiosulfate in the treatment of tumoral calcifications in a hemodialysis patient without hyperparathyroidism. Nephron. 1996;72(2):308-312. 12. Musso CG, Enz P, Vidal F, et al. Use of sodium thiosulfate in the treatment of calciphylaxis. Saudi J Kidney Dis Transpl. 2009;20(6):1065-1068. 13. Polovich M, Whitford JN, Olsen M. Chemotherapy and Biotherapy Guidelines and Recommendations for Practice. 3rd ed. Pittsburgh, PA: Oncology Nursing Society; 2009. 14. Schulmeister L. Extravasation management: clinical update. Semin Oncol Nurs. 2011;27(1):82-90. 7. Wolf EK, Smidt AC, Laumann AE. Topical sodium thiosulfate therapy for leg ulcers with dystrophic calcification. Arch Dermatol. 2008;144(12):1560-1562. 8. Bair B, Fivenson D. A novel treatment for ulcerative calcinosis cutis. J Drugs Dermatol. 2011;10(9):1042-1044. JAMA Dermatology August 2013 Volume 149, Number 8 949







© Copyright 2026