
EYE EMERGENCIES
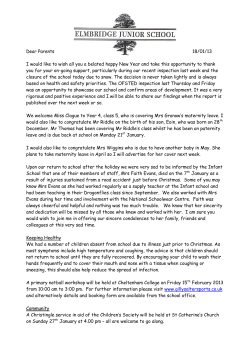
Martha Neighbor, MD EYE EMERGENCIES Objectives: 1. Discuss the visual acuity exam in patients with eye complaints explaining a. how it is performed b. how results should be documented on the chart c. why it is so important to measure d. which results should prompt an ophthalmology consultation 2. Describe 4 physical findings that suggest rupture of the globe 3. Explain how to perform the “swinging light” test for an afferent pupillary defect (APD) and list three etiologies for this finding 4. Compare and contrast the eye exam in patients with periorbital cellulitis vs. orbital cellulites Copyright UC Regents 1 Martha Neighbor, MD EYE EMERGENCIES I. Evaluation A. History 1. General: age, occupation, general medical condition, allergies 2. Specifics a. Duration b. Previous visual problems e.g. visual loss, trauma c. Circumstances surrounding injury/problem d. Changes in visual acuity (blurring, field of vision, halos) e. Photophobia or photosensitivity f. Pain, burning, itching g. Tearing, discharge B. Physical Examination 1. Visual Acuity a. Single best test for evaluation of eye and optic nerve b. DOCUMENT ON CHART BEFORE YOU INTERVENE c. Ideally includes distance and near vision d. Use Snellen chart, count fingers, hand movement, light perception e. Use topical anesthetics if needed to get patient cooperation f. Get BEST possible acuity, so use patient’s glasses or pinhole 2. Visual fields – test by direct confrontation using own visual fields as comparison of normal 3. Orbital rims – palpate for step off, crepitus, tenderness 4. Eyelids and tear apparatus a. Swelling, asymmetry, distortion b. Discharge, infection, parasites c. Lacerations 5. Extraocular Muscles a. Test for conjugate movement - in primary gaze and 6 cardinal positions b. Abnormalities may be due to trauma, myasthenia gravis, thyroid disease, diabetes, vascular disease 6. Conjunctiva - evert eyelids to examine palpebral conjunctiva a. Erythema – diffuse? Perilimbic? b. Discharge – serous, mucoid, purulent c. Edema? Chemosis? d. Foreign bodies e. Hemorrhage 7. Cornea a. May want to check for intact innervation with wisp of cotton for corneal reflex b. Opacities? Ulcerations? c. Fluorescein staining for loss of integrity of corneal epithelium Copyright UC Regents 2 Martha Neighbor, MD 8. Anterior Chamber a. Use penlight to check for chamber depth b. Flare and cell – normal aqueous fluid is cell and protein-free because of blood-aqueous barrier provided by ciliary epithelium. When this is disturbed, blood and protein and cells enter the anterior chamber. A narrow beam of light passed through the anterior chamber is normally reflected off the cornea and iris only. With flare will be able to see the beam of light passing through the anterior chamber, much like a movie projector beam in a smoky, dusty theater. With “cell” you can actually see “dust” particles. 9. Iris-asymmetry? Prolapse from previous surgery? 10. Pupil a. Should be equal, round, constrict equally to light and near vision testing b. Sphincter muscle innervated by parasympathetics and dilator innervated by sympathetics c. Which is the bad pupil? Probably the one that doesn’t constrict as well 20-25% of normals have some anisocoria (<1mm) • Horner’s syndrome – sympathetic defect resulting in ptosis, miosis, and facial anhydrosis o Anisocoria more pronounced in dark o Causes include central brainstem lesions from CVA or tumor, disturbances of sympathetic pathways in the apex of the lung and neck (get a CXR), or cluster headaches • Dilated pupil o Third nerve palsy-involves eye will be turned down and out, will be ptosis, problems turning involved eye in and up. If its compressive lesion pressing on the 3rd nerve the pupil will be large. A normal pupil with 3rd nerve ocular palsies suggest an ischemic injury to the 3rd nerve (e.g. Diabetes) in which the outer 3rd nerve papillary fibers are spared. The defect is in constriction and the anisocoria will be worse in bright light. o Pharmacalogic – accidental or intentinal use of mydriatrics. May be distinguished by lack of pupil constriction with cholinergic drops as pilocarpine. o Adies pupil – defect in ciliary ganglion or ciliary nerves. Pupil constricts with accommodation but light reaction is poor (“accommodates but doesn’t react”). Seen in young women, complain of blurred near vision, best to test in dimly lighted room, may follow varicella, often associated with decreased deep tendon reflexes Copyright UC Regents 3 Martha Neighbor, MD • Marcus Gunn pupil o Defect in afferent pathway of optic nerve o Reflects damage to retina or optic nerve o Detected by “swinging light test” – swing light from eye to eye every 3 seconds. Tests for asymmetric visual input to the brain Normally each time shine light in pupil, get brief constriction then dilation until stable pupil diameter Abnormal pupil constricts upon consensual testing, but dilates with direct testing Both pupils remain large when bad eye is stimulated and become smaller when the normal eye stimulated o Extensive retinal disease (retinal detachment) or optic nerve disease (optic neuritis) will cause a Marcus Gunn pupil. Cataracts, virteous blood will not 11. Lens-discoloration, cataract, foreign bodies 12. Vitreous-hemorrhage? Foreign bodies? 13. Fundi a. Optic disc should be pink, well demarcated edges (nasal may be blurred) b. Retinal vessels branch out at 2, 4, 8, and 10 o’clock c. Veins pulsate but 50% normals won’t have pulsating veins, therefore only helpful if you see them d. Macula - have patient look at fundoscope’s light e. Papilledema • Earliest sign is absence of venous pulsations • See venous congestion • Blurring of disc margins • Hemorrhage II. The red eye Differential diagnosis includes corneal abrasion, foreign body, conjunctivitis, iritis, glaucoma, episcleritis, scleritis A. Conjunctivitis – inflammation of conjunctiva which is a mucous membrane coating the inner surfaces of the eyelids and anterior sclera B. Viral 1. Usually self-limited, resolves without treatment in 10-14 days, highly contagious 2. Etiology - often adenovirus 3. Diagnosis a. Scant watery discharge b. Tearing c. Preauricular lymph node Copyright UC Regents 4 Martha Neighbor, MD 4. Treatment a. None vs. topical antibiotics b. Controversial – beware of unnecessary sulfa drugs and StevensJohnson syndrome c. Very contagious – warn not to share towels with family members, use tissue, not handkerchiefs 5. Herpes a. Simplex - can cause keratitis or uveitis appearing as dendritic or geographic ulcer or diffuse punctate keratitis with fluorescein exam • Should be seen by Ophthalmology for antiviral eye drops such as trifluorothymidine (Viroptic) • Topical steroids contraindicated as they may lead to perforation b. Zoster - think of if see vesicles in distribution of 5th cranial nerve (sometimes the eye symptoms precede the skin lesions) • Especially be concerned if the tip of the nose is involved (Hutchinson’s sign) since the nasociliary branch of the ophthalmic nerve innervates both the cornea and the tip of the nose • At SFGH patients with V1 Zoster immunosuppressed with HIV are admitted for IV acyclovir (may progress to Herpes encephalitis) call for Ophthalmology consult C. Bacterial - suggested by profuse purulent discharge with matting of eyelids 1. Etiologies - Hemophilus, Strep, E. coli, Proteus, Staph, Pseudomonas, Gonorrhea, etc. 2. Diagnosis - all purulent discharge should ideally be gram stained 3. Treatment - topical antibiotics as sulfacetamide, gentamycin, tobramycin a. Neomycin is highly sensitizing (26%) after 3 days use and shouldn’t generally be used 4. If not better in 48-72 hours should see Ophthalmologist 5. Complications - corneal ulceration – on slit lamp exam ulcer has an irregular margin and white stromal infiltrate 6. Special infections a. Gonococcal - adults have genital symptoms, exudate is very purulent, need topical and systemic treatment, get Ophthalmology consult b. Chlamydia in adults – may have genital symptoms, or may be a chronic conjunctivitis that is unresponsive to topical antibiotics, needs to be treated with oral doxycycline or tetracycline D. Allergic - seasonal symptoms, history of hay fever, asthma, eczema 1. Patient has allergic symptoms, clear watery discharge, that is first clear then white, thick, stringy 2. On conjunctival smear would see eosinophils 3. Patients have symptoms of itching and burning 4. Treatment – vasoconstrictors as Vasocon or Naphcon A eye drops plus cool compress or cromalyn 4% eye drops Copyright UC Regents 5 Martha Neighbor, MD III. Iritis The uveal tract consists of the iris, ciliary body, choroids layer or the retina. Inflammation of the anterior uveal tract is called iritis. It is usually unilateral A. Symptoms – painful red eye, photophobia, decreased vision (no discharge) B. Diagnosis 1. Perilimbal/ciliary flush 2. Miotic pupil with direct and consensual photophobia and pain with light testing 3. Fine keratic deposits on the posterior aspect of the cornea 4. Flare and cell in the anterior chamber C. Etiology - TB, syphilis, Reiter’s syndrome, ankylosing spondylitis, inflammatory bowel disease, Bechet’s disease, sarcoid, post-traumatic, idiopathic, trauma – order a PPD and VDRL D. Treatment - cycloplegics, topical steroids, Ophthalmology consult E. Complications - adhesions of the iris to cornea or lens, secondary glaucoma, retinal detachment IV. Glaucoma A. Pathophysiology – aqueous humor produced by the ciliary body passes through the pupil and absorbed by the trabeculae of the anterior chamber and drains into the Canal of Schlemm and then the aqueous veins B. Open angle glaucoma 1. Is defect in absorption of aqueous by the trabecular network resulting in gradual elevation of intraocular pressure (IOP) 2. Accounts for 90% of glaucoma 3. Is bilateral, insidious disease, often asymptomatic except for gradual loss of vision 4. Is the reason people over 35-40 years should have annual eye exams and pressure measurements C. Closed angle glaucoma 1. Also known as acute narrow angle glaucoma 2. Caused by narrow angle between cornea and iris that prevents aqueous fluid from reaching trabecular network where it can be absorbed 3. Symptoms are acute and may be precipitated by entering a dark room or administration of dilating eye drops 4. Symptoms a. Usually unilateral b. Headache, halo formation around lights, nausea, vomiting c. Decreased visual acuity d. Photophobia Copyright UC Regents 6 Martha Neighbor, MD 5. Diagnosis a. By hand light exam can see a shallow anterior chamber b. Edema of cornea c. Perilimbal injection d. Dilated, unreactive pupil e. Decreased visual acuity f. Fundoscopic exam – increased cup: disc ratio, notching or loss of neurovascular rim of the disc, hemorrhage in the disc g. IOP greater than 20 mmHg with tonometry 6. Treatment a. Miotics – tightens the trabecular meshwork to allow greater aqueous flow, pulls iris away from the angle to relieve obstruction. Examples – pilocapine, carbachol, echothiphate b. Epinephrine – increases aqueous outflow and decreases aqueous production c. Beta blockers – reduces the formation of aqueous fluid (Timolol) d. Carbonic anhydrase inhibitors – reduces formation of aqueous humor e. Hyperosmolar agents as mannitol or glycerin f. Acute treatment • Oral glycerin, 50% solution, 180cc • Acetazolamide, 250mg qid po (if not sulfa allergic) • Pilocarpine 2% 2gtt q 15 min. or timolol .25% or .5% 2 gtt bid • May use IV mannitol 20% solution 1.5 – 3gm/kg and IM or PO acetazolamide 500mg D. Episcleritis and Scleritis 1. Episcleritis a. Local inflammation of elastic membrane overlying the sclera b. Causes scratching, pricking feeling c. Vision normal, symptoms of sudden onset d. Usually in women aged 30-40 years e. See localized redness, salmon colored injection of section of sclera 2. Scleritis a. Destructive process of sclera seen in TB, H. zoster, gout, SLE, syphilis, collagen vascular disease b. Disease is chronic c. Get severe orbital aching, diffuse or nodular patches of deeply injected sclera, blue-red hue, lacrimation, photophobia d. Normal vision e. Need Ophthalmology consult, systemic steroids Copyright UC Regents 7 Martha Neighbor, MD V. Eye Trauma A. Corneal foreign bodies or abrasions 1. Topical anesthetic is both therapeutic and diagnostic 2. Diagnosis is made with fluorescein stain and slit lamp exam a. If corneal epithelium is disturbed, there will be increased uptake of the stain and the abrasion will appear dark green under cobalt blue light b. Metallic foreign bodies need to be removed with a 25 gauge needle held parallel to the cornea c. Foreign bodies from grinding metal should suggest the possibility of intraocular foreign body as well and orbital x-rays (dental panorex films or orbital CT) and Ophthalmology consult are advisable 3. Treatment a. Instill cycloplegic to treat associated spasm and photophobia b. Instill antibiotic ointment c. Arrange follow-up with Ophthalmologist within the next 24-48 hours B. Chemical burns to the eye - are a true eye emergency 1. Requires copious irrigation with water at once 2. Topical anesthetic drops make patient more comfortable 3. Alkali burns a. From lye, fresh lime found in plaster, mortar, concrete, also from ammonia, drain and oven cleaner b. Are most serious because alkali penetrates intraocularly and reacts with fats to form soaps, damaging cell membranes and allowing further penetration into the eye c. Need to irrigate until pH testing paper applied to the conjunctiva reads about 7.4 and recheck in 30 minutes to see that the pH has not changed d. Get Ophthalmology consult 4. Acid burns a. Acid usually does less damage, and is more localized because acid precipitates proteins and these make a physical barrier to further penetration and damage b. From splashes from car battery explosions c. Irrigate, slit lamp exam looking for corneal damage 5. Mace, tear gas a. Cause self-limited injury b. Conjunctival irritation, mild diffuse corneal damage Copyright UC Regents 8 Martha Neighbor, MD C. Blunt trauma - requires complete ocular exam 1. Rupture globe – an eye emergency a. Consider in all with severe trauma to periobital area b. Consider if the eyeball is soft, bloody c. Consider if the iris prolapses through the front of the eye d. Consider if there is a hyphema e. Consider if there is massive subconjunctival hemorrhage f. Consider if irregular, or pear shaped pupil g. Consider if lens opacity h. Treatment • Get visual acuity • Place metal eye shield or paper cup over eye • Keep patient quiet • Get Ophthalmology consult 2. Blow out fractures a. From blunt object (fist, ball, dashboard) striking the bony orbit and fracture of the weakest point which is the floor (.5mm thick) or medial wall of the orbit, resulting sometimes in entrapment of the eye contents in the fracture b. May see eyelid edema, nosebleed, lid ecchymosis, cheek and upper lip hypesthesia (from infraorbital nerve involvement as it crosses the floor of the orbit), orbital subcutaneous emphysema, diplopia, limitation of upward or downward gaze c. Requires no immediate intervention d. Needs eye consult in a few days e. Indications for repair (in 10-14 days) include enophthalmos greater than 2mm, persistent diplopia 3. Le forte II & III fractures may injure the lacrimal drainage system and result in a tearing eye or dacrocystitis 4. Blunt trauma with optic nerve damage may cause loss of vision and an afferent pupil defect (Marcus Gunn pupil) 5. Traumatic iritis – may have photophobia, blurred vision, headache, and pain. Treatment with prednisolone can prevent formation of synechiae between iris and cornea and lens 6. Massive orbital hematoma with proptosis, subconjunctival hemorrhage, increase in IOP (can threaten optic nerve, ophthalmic artery) and may require emergency lateral canthotomy to relieve the pressure. Symptoms include pain, nausea, vomiting, diplopia, proptosis, globe displacement, decreased vision 7. Hyphema – about 25% are associated with other eye injuries a. Blood in the anterior chamber, usually from tear in ciliary body b. Treatment includes cycloplegics c. Often admit for observation as rebleeding often occurs in 3-5 days after injury 8. Traumatic dislocation of lens – fluctuating vision, decreased vision, monocular diplopia 9. Cataract from lens capsule rupture and hydration of lens Copyright UC Regents 9 Martha Neighbor, MD D. Eyelid lacerations - can have severe underlying injury to eye with smallest of eyelid injuries, therefore examine eye carefully Consider eye consult for: 1. Full thickness lacerations (through the orbital septum) as they may require multiple layer repair to achieve the best cosmetic result. Also there is increased risk for orbital cellulites. Suspect this if you see prolapse of orbital fat into the laceration 2. Damage to the medical canthus, especially of the lower lid as this may involve the lacrimal drainage system and requires specialized repair. Suspect when the wound affects the lid margin between the puncta and medial one third of the eyelid 3. Wounds to the medial and lateral canthi may also interrupt canthal tendons and improper repair can result in shortening of the palpebral fissure 4. Deep transverse lacerations of the upper lid may involve the levator mechanism. Look for ptosis 5. Lid margin lacerations may involve the tarsal plate and require special care in repair. If more than 1mm of the tarsal plate is lacerated, threelayer closure is necessary (skin, orbicularis muscle, tarsus/palpebral conjunctiva) 6. Delay of 48-72 hours won’t compromise outcome of most eyelid lacerations E. Preseptal and Orbital Cellulitis 1. Preseptal (periorbital) Cellulitis – is an infection of only the lid and periorbital structures anterior to the periosteal extension called the orbital septum a. Diagnosis is made by physical examination b. See marked inflammation, erythema, edema of lids, with warmth and tenderness c. Vision is normal d. Eye appears white and “quiet” e. Pupil reflexes are normal f. Ocular motility is normal g. Etiologic agents – Staph, Strep, Hemophilus (in children); often from trauma, insect bites, impetigo h. Treatment • Cephalosporin • Warm compress for comfort 2. Orbital (postseptal) Cellulitis – much more serious, but less common a. Has similar findings to preseptal cellulites but also has orbital pain on eye movement b. Has decreased vision, may have pupillary reflex abnormalities i.e. Marcus Gunn pupil c. Ocular motility may be impaired d. Eye may be proptotic and red e. May be chemosis f. Etiology Copyright UC Regents 10 Martha Neighbor, MD • Trauma, ethmoid sinusitis in 60-80% of cases • Organisms are Staph, Hemophilus, Strep g. Usually need CT scan to assess sinus disease h. Treatment • Hospitalization • IV antibiotics, surgical drainage to decompress orbit VI. Painless Loss of Vision A. Central Retinal Artery Occlusion 1. True ophthalmologic emergency 2. Ophthalmic artery comes off the carotid and in turn branches into the central retinal artery. From sudden occlusion may get painless monocular loss of vision 3. Causes a permanent loss of vision if retina is ischemic more than 90 min. 4. Etiologies a. Embolic from heart or carotids, thrombotic b. Associated with drug abuse, artery spasm, hypertension, sickle cell disease, diabetes, vasculitis, ischemic heart disease c. Idiopathic 5. Diagnosis a. Acute loss of vision – may be finger counting, light perception, or blindness b. Pale fundus c. Arteries hard to see, veins are dark d. “Cherry red spot” where fovea (fed by choroidal vessels) appears hyperemic compared to ischemic retina e. Marcus Gunn pupil 6. Treatment a. Hyperventilation into paper bag or inhalation of 5-10% CO2 in 90-95% O2 for 5-10 min. q hr. b. Sublingual nitro c. Digital massage of eyeball for 5 seconds on, 5 seconds off d. Anterior chamber paracentesis of .2cc of aqueous at limbus with a 27 gauge needle done by an Ophthalmologist e. Treat IOP B. Temporal Arteritis - ischemic optic neuropathy 1. Will develop severe vision loss if untreated, may be abrupt or episodes of amaurosis fugax 2. Symptoms a. Malaise, headache, weight loss, jaw pain, scalp tenderness, PMR 3. Signs a. ESR greater than 50 b. Disc pallor, dilated, tortuous veins, cotton wool spots c. Afferent papillary defect (Marcus Gunn pupil) 4. Diagnosis - temporal artery biopsy 5. Treatment - oral steroids to prevent blindness – 80-100mg/day prednisone Copyright UC Regents 11 Martha Neighbor, MD C. Central Retinal Vein Occlusion 1. Usually presents with slow, painless loss of vision 2. Etiologies – D.M., hypertension 3. Diagnosis – hemorrhages and cotton wool exudates “blood and thunder” 4. Treatment – variable course of disease a. Get Ophthalmology consult b. Measure IOP D. Retinal Detachment 1. Causes gradual to sudden loss of vision 2. Males more than females 3. 50-60 year olds 4. Associated with aging, absence of lens, D.M., sickle cell, trauma, kidney disease, toxemia of pregnancy 5. Symptoms – cloudy vision, flashes of lights, floaters, shadow, curtain obscuring visual field 6. Diagnosis – by exam 7. Requires rapid repair – within 24-48 hours E. Eptic Neuritis 1. Refers to several conditions causing disease of optic nerve with loss of vision 2. Usually in 15-45 year olds 3. Symptoms a. Unilateral, sudden, severe loss of vision from focal demyelination of optic nerve b. Pain with eye movement 4. Signs a. Marcus Gunn pupil almost always present b. Central scotoma 5. Treatment a. Controversial b. Steroids may shorten course of symptoms and decrease pain but not clear they improve prognosis c. About 35% will develop multiple sclerosis within 4 years F. Other causes of Loss of Vision 1. Virteous hemorrhage 2. Migraine headaches 3. Hysterical a. Hold a large mirror in front of the patient and move it in an erratic pattern. The eye involuntarily tracks in order to maintain fixation b. Check for optokinetic nystagmus which can be performed by moving a lined paper in front of the patient c. “Magic” eye drops Copyright UC Regents 12 Martha Neighbor, MD Cross section of the eyelids. (Courtesy of C. Beard) Reproduced with permission from: Vaughn D, Asbury T, Riordan-Eva P: General Ophthalmology 13th Ed., Appleton and Lange, Norwalk CT, 1992. Copyright UC Regents 13 Martha Neighbor, MD Anterior chamber angle and surrounding structures. Reproduced with permission from: Vaughn D, Asbury T, Riordan-Eva P: General Ophthalmology 13th Ed., Appleton and Lange, Norwalk CT, 1992. Copyright UC Regents 14 Martha Neighbor, MD Cross section of the eyelids. (Courtesy of C. Beard) Reproduced with permission from: Vaughn D, Ashbury T, Riordan-Eva P: General Ophthalmology 13th Ed., Appleton and Lange, Norwalk CT, 1992. Copyright UC Regents 15 Martha Neighbor, MD EYE EMERGENCIES Case 1 A 57 year old woman presents to the ED complaining of 1 week of pain in her right eye increasing over the last several hours. She states she has a headache and feels nauseous, but has not vomited. She denies trauma or prior eye problems. The patient does not have her glasses, but using a Snellen chart, her visual acuity is 20/200 in the right eye and 20/70 in the left eye. The right eye appears red, and the pupil is 6 mm and unreactive to light, and the cornea appears somewhat hazy. The left pupil is normal. 1. 2. 3. 4. List four possible causes of this patient’s painful red eye. Why is it important to check the visual acuity in a patient with an eye complaint? How can you correct for refractive error in the patient who does not have their glasses/lenses? What is the significance of this patient’s abnormal visual acuity? Are there other tests that may assist in the diagnosis of this patient? How should this patient be treated? Case 2 A 6 year old boy is brought to the ED by his mother. She tells you she thinks he was struck in the eye by a stick while playing with his brother. The child is crying and holding his hand over his right eye. The patient is uncooperative, but seems able to count fingers correctly using his right eye. Examination shows an ecchymotic, swollen right upper eyelid. The pupil seems slightly oval in shape and there is a large subconjunctival hemorrhage laterally. 1. 2. 3. What is the worst possible diagnosis in this patient? What findings suggest this diagnosis? What is the significance of the patient’s ability to count fingers using the injured eye? How should you manage this patient now? Copyright UC Regents 16 Martha Neighbor, MD Answers Case 1 1. Causes of the “red eye” include conjunctivitis (bacterial, viral, allergic, chemical), iritis, acute glaucoma, corneal abrasions, trauma, infection. 2. The visual acuity is the single most important part of the eye exam, a very abnormal visual acuity as it suggests the patient may be a vision threatening problem. Always obtain the “best “ possible visual acuity meaning patients should wear their glasses/contact lenses, and there should be good light. Patients who do not have their glasses/lenses can have their refractive error largely corrected by using a pinhole. Patients over the age of 40-45 years, will have presbyopia, and will not be able to read a close card unless they have reading glasses or use a pinhole. The patient in Case 1 should have her visual acuity checked again reading the Snellen chart with a pinhole. The left (unaffected) eye now has a normal visual acuity, but the right (affected) eye is still only 20/200 which is very abnormal and of concern. 3. This patient’s history and exam is not suggestive of conjunctivitis or corneal trauma. Iritis is possible, but acute narrow angle glaucoma more likely. A slit lamp examination is appropriate looking for flare and cell in the anterior chamber, but intraocular pressure measurements are imperative. In this patient the right eye intraocular pressure is 50 mmHg, the left eye is 20 mmHg. (Normal is up to about 20 mmHg) 4. Acute narrow angle glaucoma is an emergency. Ophthalmology must be called immediately and treatment initiated with pilocarpine 2% drops (constricts iris/pupil and opens up drainage of aqueous fluid in angle). A beta-blocker such as timolol 0.5% will decrease aqueous humor production as will acetazolamide a carbonic anyhdrase inhibitor. Osmolar agents as oral glycerol or IV mannitol will decrease ocular volume and pressure. Case 2 1. The worst possible diagnosis associated with eye trauma is rupture (penetration) of the globe, a true ophthalmologic emergency. Findings suggestive of a ruptured globe in this patient include an oval shaped pupil as well as the large subconjunctival hemorrhage associated with eye trauma. Other findings worrisome for globe rupture include uveal material visible through the sclera, cataract, hyphema. 2. The child’s ability to only count fingers is very worrisome and suggestive of a significant vision threatening eye injury. However, this assumes that the visual acuity in this frightened child who is in pain and acute distress is indeed accurate. 3. Ophthalmology must be contacted immediately. The child should be calmed and placed in a quiet room. The eye should be protected from further damage by covering it with a metal shield or the top of a urinalysis specimen container. The patient’s tetanus immunization should be brought up to date. A CT scan of the orbit will probably be needed. Copyright UC Regents 17 Martha Neighbor, MD EYE EMERGENCIES Bibliography 1. Leibowitz H. The Red Eye. NEJM 2004 343;5:345-351 2. Shingleton BJ, O’Donoghue MW. Blurred Vision. NEJM 2000 343;8:556-562 3. Fingeret M, Onofrey BE, Talley DK. Management of ocular emergencies Optom Clin 1993;3(2):247-52 4. Emergency Medicine Clinics of North America August 1995 5. Santen SA, Scott JL. Ophthalmologic procedures 681-701 6. Barish RA, Naradzay JF. Ophthalmologic therapeutics 649-67 7. Rothenhaus TC, Polis MA. Ocular manifestations of systemic disease 607-30 8. Linden JA, Rener GS. Trauma to the globe 581-605 9. LaVene D, Halpern J. Jagoda A. Loss of vision 529-60 10. Handler JA, Ghezzi KT. General ophthalmologic examination 521-38 Copyright UC Regents 18











© Copyright 2026