
Consumer Power to Build Better Health Systems
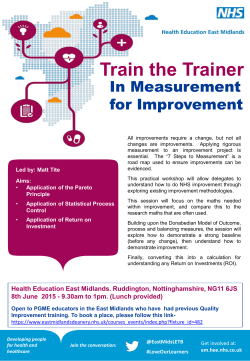
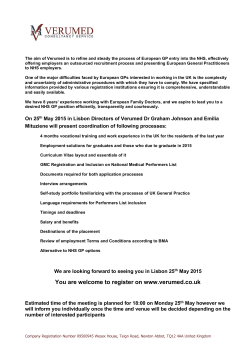
APRIL 2015 Consumer Power to Build Better Health Systems GLOBAL PERSPECTIVES ON INTEGRATING THE CONSUMER VOICE ACROSS HEALTH SYSTEMS WITH SUPPORT FROM: CONTENTS EXECUTIVE SUMMARY 3 KEY THEMES 6 Break down silos among consumer groups page 6 Foster open institutional and policy decision-making page 7 Elevate the patient experience in measuring health outcomes page 9 Harness digital networks page 10 Design and deliver care collaboratively page 8 Empower consumers and patients with data page 11 OPPORTUNITIES13 1 2 3 Establish an Engaging Consumers across Health Systems Working Group Enhance the utility of feedback from consumer review online portals for hospital and clinical settings Develop learning resources to help health institutions work with consumer groups 4 5 6 Invest in cultivating patient-centered attitudes among future health leaders Host a series of multi-national workshops to share lessons about patient reported outcomes measures Make health reporting data platforms more actionable REFERENCES15 CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 2 “Nothing about us, without us” This philosophy and rallying cry, used by consumer* advocates globally, has never been more relevant to the US health system. The Affordable Care Act is moving US health care to address population health in the environments in which consumers live, learn, work and play. The rising tide of chronic illnesses demands intensive self-care and heath awareness in individuals’ daily lives. Finally, consumer choice has become a powerful force in the US health ecosystem as the wealth of information available online about health topics such as insurance plans, hospital quality, patient satisfaction and medical knowledge has grown. To address these changes, health care professionals need to know about consumers’ lives, needs and experiences more than ever. Now is the time when the US health system must be redesigned to treat the whole person rather than just the maladies he or she may have; it is the time to build a culture of health. Integrating the consumer voice across the health system is, therefore, crucial. This report outlines ways in which the consumer perspective can be better incorporated into institutional decision-making, care design and delivery, health outcomes measurement, digital networks and data use. A unified consumer voice can provide valuable insights into the design and delivery of health care to maximize both clinical and quality of life outcomes. For example, in the 1980s and early 1990s, HIV activists, pharmaceutical companies and governments worked together to secure better health rights and timely access to new treatments, ultimately altering the course of the AIDS epidemic.1 More recently, consumer engagement has played a critical role in improving quality at the Beth Israel Deaconess Medical Center in Boston, where consumers sit on patient and family advisory councils and participate directly in hospital decision-making.2 have more than a token amount of power and influence” in these spheres.3 Entrenched power dynamics can limit how open institutional leaders are to consumers’ perspectives and how comfortable consumers feel sharing their views in those settings. Additionally, consumers may not always have the information or support they need to assess the quality of care being delivered and form recommendations commensurate with the complexity of the institutional problem at hand. As patient and consumer advocates, policymakers, hospital administrators, insurers and others seek to open doors wider to consumer involvement in health decision-making in the US, they can learn a great deal from global efforts that have succeeded in the same pursuits. For example, in Germany, patient representatives set government agendas and drive solutions to consumer issues by collaborating directly with payers and providers as equal members on Germany’s highest health decision-making body, the Federal Joint Committee. In the UK, the private sector and England’s National Health System (NHS) joined forces to build the iWantGreatCare website, a trusted country-wide resource that presents real-time data on quality and patient satisfaction in an easily digestible format to patients, consumers, providers and hospital administrators. These experiences can help answer some of the pressing questions about how to apply the consumer voice to turn the tide from disease-focused to people-focused care in the US. How can the consumer perspective add the most value to different components of the health system, such as policy, health intervention design and technology? What are the best ways to institutionalize the consumer voice in these channels? Where and how have such efforts already succeeded in improving health outcomes? What can the US learn from those examples? While consumer groups have become a fixture on many pharmaceutical, hospital and payer advisory boards, they often do not have the opportunity to exert meaningful influence. As Kristin Carman and her colleagues noted in their 2013 Health Affairs article, “It is still rare for patients to * A note about the use of “consumer” and “patient” in this report: While all patients are consumers of health care, not all consumers are patients. We define “patient” and “consumer” as such: patients require interaction with the health care system due to illness or injury, whereas consumers can be healthy and make elective decisions about health services and prevention. To address current health challenges, including the rise of chronic diseases, these roles should overlap closely across health systems so people are empowered to address health holistically. This perspective guides our use of “patient” and “consumer” throughout the report. CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 3 To begin to answer these questions, Rabin Martin hosted a roundtable of 13 consumer engagement experts in Berlin, Germany, in October 2014 during the World Health Summit with support from the Robert Wood Johnson Foundation. The following participants represented eight countries and a range of perspectives, including those of patient and consumer advocates, the private sector, health technology and policy experts, NGOs and providers: •Dr. Alexander Geissler | Senior Research Fellow, Department of Health Care Management at the Berlin University of Technology | Germany • Tenley Ghan | Senior Associate, Rabin Martin | USA – FACILITATOR • Johan Hjertqvist | Founder and President, Health Consumer Powerhouse | Sweden • Rebecca Hoppy | Managing Director, Rabin Martin | USA – FACILITATOR • Robert Johnstone | Board Member, European Patients Forum | UK • Dr. Ozge Karadag Caman | Hacettepe University, Institute of Public Health | Turkey • Jacqueline Mallender | Partner, Optimity Matrix | UK • Dr. Mahiben Maruthappu | Imperial College London | UK • Alison Moore | Associate, Rabin Martin | USA – FACILITATOR • Dr. Lloyd Nash | Chair & Co-Founder, Global Ideas Forum | Australia • Dr. Phillip Phan | Professor and Executive Vice Dean at The Johns Hopkins University Carey Business School and Core Faculty at the Johns Hopkins Medicine Armstrong Institute for Patient Safety and Quality | USA • Dr. Imran Qureshi | Executive Director, Doctors Advancing Patient Safety (DAPS) Global | UK • Sophia Schlette | Consultant, health systems knowledge management | Germany • Jan Schmitz-Hübsch | Director of Business Development & Projects, Munich Health Daman Holding | UAE • Erica van der Schrieck-de Loos | Senior Advisor, CBO Dutch Institute for Healthcare Improvement | Netherlands • Dr. Jeffrey L. Sturchio | President & CEO, Rabin Martin | USA – MODERATOR • Dr. Bach Tran | Lecturer in Health Economics at Hanoi Medical University | Vietnam During the roundtable, participants shared their experiences and knowledge related to efforts around the world that have enhanced consumer involvement in health systems and, in turn, led to better health outcomes. Participants later reviewed and provided feedback on this report. The recommendations from the roundtable include the following: BREAK DOWN SILOS AMONG CONSUMER GROUPS FOSTER OPEN INSTITUTIONAL AND POLICY DECISION-MAKING DESIGN AND DELIVER CARE COLLABORATIVELY ELEVATE THE PATIENT EXPERIENCE IN MEASURING HEALTH OUTCOMES HARNESS DIGITAL NETWORKS EMPOWER CONSUMERS AND PATIENTS WITH DATA CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 4 This report highlights examples that participants cited during the roundtable discussion and that Rabin Martin corroborated through follow-up research. The report also identifies opportunities for continued investigation about how institutions in the US can apply elements of these examples to augment consumer engagement efforts and to help broaden the US health system view of health beyond clinical outcomes. Ultimately, it proposes ideas for further research and initiatives in this area. Recommendations include: 1 Establish an “Engaging Consumers across Health Systems” working group to share best practices from around the world 2 Enhance the utility of feedback from consumer review online portals for hospital and clinical settings 3 Develop learning resources (e.g., training modules, toolkits, learning exchanges) to help health institutions work with consumer groups when delivering care 4 Invest in cultivating patient-centered attitudes among future health leaders 5 Host a series of multi-national workshops to share lessons about designing, implementing and standardizing patient reported outcomes measures (PROMS) across health systems 6 Make health reporting data platforms more actionable by linking them with community health services The magnitude and complexity of the health issues that the United States faces are vast – but so is the potential for the consumer perspective to improve health outcomes. Unleashing the power of the consumer voice at all levels can help health institutions in the US to adopt more holistic, collaborative and effective solutions to build a culture of health. CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 5 KEY THEMES How to integrate the consumer perspective across health systems BREAK DOWN SILOS AMONG CONSUMER GROUPS The patient and consumer voice can be stronger when unified on cross-cutting issues Unleashing the full power of the consumer voice requires unification. Fragmented and specialized advocacy groups can compete for resources and make it difficult to have significant influence or maintain bargaining power. One participant noted, “There seems to be a sense that, while diseasespecific advocacy groups may be very, very good, there is an opportunity to actually create a more coordinated approach, perhaps at a national level or a regional level.” In the UK, the mantra, “no decision about me, without me,” has been a unifying banner for consumer efforts to help steer the NHS’s 20-year road map to improve the country’s health, based on the 2002 Wanless Report (see Spotlight On: The Wanless Report). This phrase demands that patients be involved in decisions about their care and treatment and appears in patient and consumer advocacy group manifestos around the world. HIV/AIDS advocacy groups in the 1990’s used the phrase while working to integrate the GIPA Principle (greater involvement of people living with HIV/AIDS) into the Joint United Nations Programme on HIV/AIDS’s ongoing response to the epidemic.4 In the UK, groups including the National Kidney Federation, the Cure Parkinson’s Trust and the National AIDS Trust have each invoked the mantra throughout their interactions with the NHS. The force of this collective message has driven a cultural shift in how decision-makers view the role of consumers within the health system. “No decision about me, without me” – a variation on “nothing about us, without us” – is now embedded in the NHS Constitution and the government states that its first guiding principle is, “patients will be at the heart of everything we do.”5 In the Netherlands, the National Patient and Consumer Federation (NPCF), a national consumer advocacy group, serves as an umbrella organization to hundreds of smaller patient groups that represent three million people in total. The NPCF formed in 1992 because “it was important for patients groups to work together in order to have a stronger voice and become a significant national player.”8 The group uses a layered configuration that allows consumer groups to collaborate on cross-cutting issues, such as patient rights and access to care, at the national level while coordinating disease-specific approaches at the same time. It has often partnered with the Dutch government over the years on a range of patient group initiatives, including co-developing and implementing a coordinated education program to enhance consumer groups’ expertise and capacity to engage at the policy level.7 As Hester M. Van de Bovenkamp and Margo J. Trappenburg explain in their 2011 Health Care Analysis article on Dutch patient groups’ relationships with the government, “participants need to be able to look beyond their individual experiences, have strong negotiating skills and organizational, financial, medical and scientific knowledge to be able to talk to the other actors at the negotiating table.” With funding from the Dutch government, the NCPF continues to be a key source of this capacity-building.9 SPOTLIGHT ON: THE WANLESS REPORT (2002)6 In the UK, consumer groups came together in the early 2000s to make their perspectives heard in an NHS-commissioned effort to identify a 20-year roadmap to improve the country’s health. Around that time, the NHS commissioned a former banker, Derek Wanless, to conduct an assessment of the NHS’s long-term resource requirements. The 2002 Wanless Report drew on the expertise of 28 patient advocacy groups (among representatives from other sectors) and recommended that the NHS should move to ensure that all patients were “fully engaged” in managing their health to cope with rising demand and costs.7 As a result, the government called for integrating shared decision-making across NHS practices.7 CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 6 FOSTER OPEN INSTITUTIONAL AND POLICY DECISION-MAKING Consumers are able to contribute most meaningfully at the institutional level when they are welcomed by genuinely collaborative environments The attitudes and actions of an institution’s leadership – whether within a governmental body or a hospital steering committee – toward consumer representatives in decisionmaking processes play a substantial role in whether consumer representatives are able to be heard. As one participant recounted of time spent in England, “I’ve sat in clinical government committees where there is a patient member whose voice in that scenario was very welcome… but I found other committees where the patient is a member who doesn’t really have any input because the structure did not allow him to provide it – nobody actually had interest in true patient engagement.” While changing institutional leaders’ often deep-seated skepticism about the value that consumers and patients bring to decision-making is difficult, mobilizing consumers to elect open and inclusive leadership and improving medical professional competency frameworks for ongoing development (including curricula) are two effective strategies to move the needle. At the policy level, consumers can foster an open, collaborative environment with their votes. The German public did this successfully in the early 2000s when it elected a new government that would address the lack of patient representation at the decision-making level of Germany’s national health system. One participant familiar SPOTLIGHT ON: “WAS HAB’ICH?” (WASHABICH.DE)13 Medical student Anja Bittner created the website “Was Hab’Ich?” (in English, “What do I have?”) after a friend’s mother asked her for help in understanding her cancer diagnosis. Free of charge, patients can upload instructions they receive from a health professional that they find complicated or confusing through the “Was Hab‘Ich?” site and medical students translate them into language that is easier to understand. The site helps improve young doctors’ patient communication skills and patients’ understanding of their diagnoses simultaneously. The site has been very successful: over two-thirds of patients give feedback, 90% of which is positive. One-third of patients give a voluntary donation (the site’s primary revenue source). with the transition explained, “Our new health minister just said we need to do something about making decisions more transparent.” The new government restructured the country’s highest level of health decision-making, the Federal Joint Committee, to include patient representatives in equal number as those from provider and payer groups. “Now, patients are involved with everything,” the participant continued. Involving patient representatives in the Federal Joint Committee has contributed to enhancing the transparency of healthcare decision-making at the national level and has enhanced capacity of patient/consumer organizations to understand and participate in the decision-making process.10,11 The body’s decisions affect the 70 million members in Germany’s statutory health insurance system. It is also important to instill the value of the patient perspective in existing health accreditation frameworks, which can influence providers across the experience spectrum and future health care providers who might lead open and collaborative institutions one day. Participants stressed that the key to strengthening the consumer role in decision-making positions lies in improving patient-provider relationships. For example, UK doctors Trish Greenhalgh and colleagues have launched a campaign for “Real Evidence-based Medicine” – a call to reform “Evidence-based Medicine,” which has become standard practice for doctors in the last 20 years, to account for individual patient needs and circumstances, among other changes. While Greenhalgh’s movement is young, she and her colleagues note that a number of efforts are already in line with their campaign, such as the BMJ’s Too Much Medicine initiative.12 As their movement grows, “Real Evidence-based Medicine” may one day help providers value patient input more at a systems-level. Other experiences also can enrich the patient-provider relationship: the German website “Was Hab’Ich?”13 (see Spotlight On: “Was Hab’ich?”) uses young medical students as change agents to make the current health system friendlier to consumers’ health literacy needs. In the UK, the NHS recently launched the Better Training, Better Care Initiative to improve training for young medical staff and ensure better care and outcomes for patients. The program has piloted over 20 physician training initiatives in locations around England. For example, one pilot program sought to reduce patient waiting times in the ER. An evaluative survey of nursing, medical, and clinical training staff involved revealed an improvement of quality of care, patient experience, and patient safety. The final outcomes report on all pilots will be released in early 2015.14,15 CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 7 DESIGN AND DELIVER CARE COLLABORATIVELY Consumer groups can work with health care providers to build a bridge between health systems and the places where consumers live, work, learn and play A person’s environment and experiences have a substantial influence on his or her health. In the United States, health has traditionally been viewed as happening primarily in a doctor’s office. Shifting the health system to focus more on health at the community and population level will require a collaborative effort among health administrators, policymakers, communitybased organizations and consumers. Consumer involvement, in particular, is critical to helping health interventions and preventive health services translate effectively from theory to implementation on the ground. formal health care system or those that are afraid of authority structures, such as people living with HIV, intravenous drug users or sex workers. One participant explained, “among hidden groups it’s very difficult for the formal sector to approach them, so we use consumer groups to spread our message.” In Vietnam, the government collaborated with the WHO, community committees and community health workers to roll out a peer-to-peer educational effort to increase adherence to and effectiveness of antiretroviral therapy among people living with HIV. The project resulted in an 80% adherence rate among affected populations.19 Additionally, the Avahan AIDS Initiative in India has improved uptake of preventive health services and spurred positive health behaviors in Southern India by incorporating community members into its program planning and management. The organization recruited community members to join its planning One approach to bringing consumers and leaders of health frompicture-based its existingTTO peer networks of female sex is a 2. Figurecommittees 2 : The redesigned discharge pro forma. This example institutions together is co-creation (or co-production) – the idea workers (FSWs). The the diclofan FSWs 50mg helped design prescription for paracetamol 1g tdsservices for 14 daysthat in total, bd for 7 days, and that patients’ needs are better met when patients are involved included legal empowerment workshops for sex workers augmentin 625mg tds for 5 days. in an equal and reciprocal relationship with professionals. The three most important elements of a successful co-creation approach are 1) designing health institutions to encourage consumer involvement in their own care and self-management of their conditions; 2) helping consumers develop skills and confidence to participate in health intervention design and implementation; and 3) helping clinicians to support and motivate patients effectively.8 In the UK, the Health Foundation has invested nearly $8 million in the community-based CoCreating Health Programme (see Spotlight On: Co-Creating Health Programme) to test how co-creation might fit into NHS service delivery.16 Co-production for symbols-based adherence tool | Pakistan Peer-to-peer consumer networks can be invaluable for reaching and educating populations that lack access to the SPOTLIGHT ON: CO-CREATING HEALTH PROGRAMME16, 17, 18 The Co-Creating Health Programme started with eight pilot sites, working to test co-creation models that focused on various chronic disease states. The pilots delivered three training and information programs to support confidence and skill-building in people with chronic conditions; developing motivational and support skills; and changing health systems and ensure sustainability beyond the life of the program. So far, the pilots have reduced anxiety and depression, improved clinical outcomes in diabetes control, and decreased the number of specialist appointments among participants. Clayton M, Syed F, Rashid A, Fayyaz U. Improving illiterate patients understanding and adherence to discharge medications. BMJ Qual Improv Report 2012 and sensitization sessions for local leaders, youth organizations. These community-driven program additions were shown to be highly cost-effective when combined with basic HIV prevention services.20 In Pakistan, doctors worked with patients to coproduce culturally competent medication adherence tools after realizing that lack of health literacy among patients was a pervasive challenge to treatment. They consulted with patient groups to understand what would be more helpful and consequently changed written dosing instructions into drawings that depicted time of day at which the medications should be taken. The patient groups then validated the tools and confirmed that they were easy to understand. Patient understanding of instructions increased three-fold among illiterate patients who used the tools. This picture-based method is now also used in Canada and Mali.21 CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 8 ELEVATE THE PATIENT EXPERIENCE IN MEASURING HEALTH OUTCOMES Health systems must be designed to value both clinical outcomes and positive consumer experiences Quality care and consumer experience are linked inextricably. As one participant noted, “If somebody has great clinical care, but is so traumatized by their experience in the hospital, they will never go back on principle.” The US has begun to test patient-reported experience measures (PREMS) and patientreported outcomes measures (PROMS) to better assess health care outcomes. A PREMS measure – Hospital Assessment of Healthcare Providers and Systems (HCAHPS) survey – is now linked to a provider’s or an institution’s reimbursement from the Center for Medicaid Services.22 Additionally, the National Institutes of Health (NIH) has long invested in patient outcomes measurement tools through PROMIS (Patient Reported Outcomes Measurement Information System).23 However, there is a long way to go before these early efforts result in consistent national use of such tools. One challenge to incorporating patient outcomes and experience measures into care is ensuring that they coexist symbiotically with clinical guidelines and regulations. Addressing that balance is not yet a perfect science, as what patients want is not always what is best for them. For instance, providers may feel pressured to sacrifice medical best practice for a higher HCAHPs score (such as when a patient requests antibiotics when they are not medically necessary). At the EU level, Swedenbased Health Consumer Powerhouse has evaluated, monitored and compared healthcare systems among 35 countries since 2007 through indexed reports such as the Euro Health Consumer Index (EHCI). Based on metrics such as degree of patient involvement in patientprovider decision-making, the indices provide Euro Health Consumer Index Report guidance to consumers, 2014 Sweden governments and health Health Consumer Powerhouse system leaders about how to improve performance and strengthen consumer involvement in decision-making processes. The European Commission regards the EHCI to be the most informative and influential assessment on European health care, and many countries provide national comment on the results.25 For example, Serbia, rated last in the EHCI, invited HCP to offer recommendations on how to improve its nation’s health care.26 Across the Atlantic, the UK has made the tricky transition. In 2009, the UK’s NHS became “the first health care system in the world to measure what it produces in terms of health, rather than in terms of the production of health care”24 when it mandated PROMS (patient-reported outcomes measures) nationally for reporting outcomes after surgical treatment. Consumer groups such as the Commission for Patient and Public Involvement, healthtalkonline and the Picker Institute worked collaboratively with the NHS to develop these metrics. The NHS’s PROMs go a step further than the US’s HCAHPS in that the former focuses on how a patient perceives an outcome of care, rather than the latter’s concentration on a patient’s experience of receiving care. For example, where HCAHPS asks, “During this hospital stay, how often did the hospital staff do everything they could to help you with your pain?” PROMs request that a patient describe his or her pain on a scale from “I have no pain or discomfort, moderate pain or discomfort, or extreme pain or discomfort.” The UK is developing an Outcomes and Experience Questionnaire (OEQ), which combines both PREMs and PROMs into a short survey. CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 9 HARNESS DIGITAL NETWORKS Consumers and patients can use social media as a tool to communicate concerns to health systems leadership Social media has revolutionized how people around the world coalesce around issues. Private, consumer-driven review sites like healthgrades, RateMD and Vitals, that allow patients to review their experiences with specific providers, are gaining popularity rapidly in the US (see Figure 1).27 Regarding patient feedback portals, one roundtable participant noted, “Openness is critical not only for consumers and their families but also for providers, payers, and others….technology is an important enabler of this transfer.” FIGURE 1. Cumulative number of ratings and rated physicians27 (based on data from RateMDs.com) 400 # Ratings (thousands) 350 300 250 200 150 100 50 0 2005 2006 2007 Physicians 2008 2009 2010 Ratings Gao G, McCullough J, Agarwal R, Jha A. A changing landscape of physician quality reporting: Analysis of patients’ online ratings of their physicians over a 5-year period. Journal of Medical Internet Research. 2012 However, providers and health care administrators are understandably wary of the information that these sites collect. The number of voices coupled with the lack of accountability for content posted on these sites dilutes the utility and credibility of the sites among providers. Moreover, providers worry that negative reviews will hurt their reputation. Moderating and funneling consumer voices into more cohesive, verified feedback could make this type of input invaluable to patient and consumer advocacy groups, providers and hospital or clinic administrators alike. iWantGreatCare, the UK’s largest aggregator of patient reviews, has bridged the divide between consumer feedback and provider utility. The site analyzes patient reviews from all hospitals and clinics in the NHS and delivers quantitative and qualitative feedback in real-time to all institutions involved in a format they can use and trust. These include flags on unmet quality indicators and an analysis of what patients perceive to be the institution’s strengths and weaknesses. As one English hospital executive explained, “We had tried many methods to capture patient experience, but none had given the real-time detail and volume iWantGreatCare | United Kingdom | IWantGreatCare.com of feedback necessary to drive improved performance [that iWantGreatCare provided].”28 The site has been so successful that it recently partnered with the NHS to roll out patient feedback initiatives across the country, such as the Family and Friends Test, which produces a publicly-available cumulative score on patient satisfaction for every NHS health institution. The test creates incentive for NHS providers to listen to and act on the feedback they receive from iWantGreatCare, which can help them work toward a higher publicly-reported score. iWantGreatCare’s private sector approach to creating a consumer- and provider-friendly portal, coupled with the NHS’s access to networks of hospitals, allows it to merge consumer reviews with clinically relevant data across the health system. In India, women typically rely on word of mouth to determine where to seek maternal health care; however, the word of mouth recommendation can be incomplete and unrelated to care quality.29 To combat this issue, Merck for Mothers has partnered with the White Ribbon Alliance for Safe Motherhood India and Gram Vaani (an Indian social technology company) to create and conduct a pilot of a patient review service for maternal health, a free mobile phone platform that uses interactive voice response technology to reach low-income women with limited literacy. This platform helps to educate women on the quality of care they should expect, informs them about available health programs and services, and empowers them to make more informed health decisions. Quality ratings and feedback can also encourage providers and health officials to improve care. Early findings indicate that women were able to use the platform to learn more about maternal health, were able to rate care quality, and the majority of women felt the service would inform where they seek care in the future. Health providers and local government officials were receptive to receiving women’s feedback to improve care. Building on the field test’s success, Merck for Mothers hopes to develop a scalable model that encourages women to seek care in higher quality facilities and holds providers more accountable for offering quality care.30 CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 10 EMPOWER CONSUMERS AND PATIENTS WITH DATA Delivering data in a format that consumers can understand, embrace and use is crucial to navigating issues of consent, confidentiality, and privacy One of the most exciting and talked about trends in health technology is the potential power of “big data.” Data collection is now ubiquitous, captured by electronic health records, smart phones, apps, Fitbits, the Apple Watch and more. As one participant put it, “[Patients] are the ones who are going to own the small print data, you have to involve the patient, they have to be engaged.” However, from the consumer perspective, making data useable is still a challenge. towards achieving better health outcomes. For example, consumer representatives have helped the UK’s 100,000 Genomes Project – a plan to test the genomes of 100,000 patients and integrate the resulting data into medical care to improve screening and treatment for cancer, infection and rare diseases33 – understand how to best engage patients and consumers more broadly when the initiative launches. To understand and address the British public’s questions over patients’ rights, privacy and consent standards, Genomics England pursued a series of engagement activities with patients, such as meetings between cancer advocacy groups and Genomics England communications leadership.34 The project will make the UK the first country to introduce genome sequencing into its mainstream health system. The United Arab Emirates’ Health Authority – Abu Dhabi (HAAD) has helped consumers take action to improve their own health by providing health information through Weqaya, an easy-to-understand web portal. Weqaya aims to identify consumers with cardiovascular disease risk factors through widespread, free opt-out screening programs for all citizens (it has screened 94% of the Weqaya national screening program population) and empower | UAE NMC Healthcare flyer them to take steps to mitigate those risks. It does the latter by pooling of all a consumer’s data into one secure, cloud-based web portal that presents a simple snapshot of the consumer’s health with action items for improvement. The site also supports appointment booking, sends text message reminders and houses other eHealth and mHealth services.31 The Weqaya program has produced impressive health outcomes: among those using Weqaya, 79% were engaged with care (compared with 55% in control group), 42% had normal hemoglobin A1C ranges for diabetes (compared with 24% in control group), and 25% had healthy cholesterol levels (compared with 5% in control group).32 Understanding consumer attitudes toward unfamiliar but potentially life-saving types of health data, such as personal genetic sequencing, can help consumers and health professionals work together to apply valuable information CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 11 OPPORTUNITIES Consumer engagement across the US health system is essential to addressing the challenges that the country faces. This report highlights examples of how other countries have fortified the consumer movement, fostered inclusive leaders, co-designed health interventions, elevated patient experiences in measuring quality, harnessed the power of digital networks and empowered patients and consumers with data to achieve better health outcomes. The following opportunities based on the collective input of global roundtable participants have the potential to elevate the consumer perspective in achieving high-quality health in the US and should be investigated further. 1 Establish an Engaging Consumers across Health Systems Working Group to share best practices from around the world To capitalize on the recent conversation and momentum in the field, we recommend establishing a global working group to identify what works when integrating the consumer voice into health systems decision-making, starting with the participants from the Berlin roundtable. The purpose of the working group will be to refine the ideas raised further, develop action plans for the opportunities identified during this event, and explore additional questions that arose during discussion, such as: • In which of the findings categories are the gaps in understanding greatest? • How can we share lessons about incorporating the consumer perspective into health systems across borders more efficiently? • How do we scale up successful models for consumer involvement from one setting to another? • How can we recruit individuals from our respective sectors as champions for these ideas? As a next step, we propose identifying highest-priority findings and opportunities as a group and, based on that foundation, hosting a digital meeting (due to the group’s geographic diversity) to discuss next steps. From this point, the group can identify activities to help disseminate the findings from the roundtable across borders, such as compiling best practice case studies, analyzing country experiences in greater detail and conducting and publishing systematic reviews of the evidence base for key recommendations. 2 Enhance the utility of feedback from consumer review online portals for hospital and clinical settings US consumers and patients are increasingly turning to private, consumer-facing sites like healthgrades, RateMDs, and Vitals to decide where to get care and rate experiences with specific providers and health institutions. The UK’s iWantGreatCare demonstrates that crowd-sourced patient reviews can be powerful feedback mechanisms for health systems when they are filtered and processed appropriately. However, in the US, there is a large gap between consumers submitting these reviews and providers and health systems using that information to improve their practices. Adding features to patient review websites in the US such as easily digestible data presentation for hospitals and clinics, real-time reporting on potential quality flags, and comment verification for patient reviews can make review data more credible and useful for clinical practices. Furthermore, there may be opportunities to join the large patient base and accessible interfaces of popular consumer-friendly sites like RateMDs with the data that providers trust such as that in Medicare’s Hospital Compare website, which is based on results from the Hospital Consumer Assessment of Healthcare Providers and Systems.35 3 Develop learning resources (e.g., trainings, toolkits, learning exchanges) to help health institutions work with consumer groups when delivering care Creating resources based on other institutions’ experiences and proven results for hospitals and clinics can help institutions work better with consumers to co-produce health interventions that target not only clinical practice, but also local social determinants of health. Training and toolkits may include sample discussion guides and roles and responsibilities frameworks to guide collaboration between the institution and the consumer group(s). Learning exchanges build networks between institutions and groups working on similar consumer engagement challenges from different angles, helping all to view the issue at hand from a new, and potentially revelatory, perspective. The UK’s site-specific Co-Creating Health Programme provides a useful example: Co-Creating Health improved health outcomes for chronic obstructive pulmonary disease, depression, diabetes and musculoskeletal pain through a collaborative team of local consumers, clinicians and managers.36 Many of the resources that made this intervention successful are available on its “Person-centred Care Resource Centre” (http://personcentredcare.health.org.uk/) website. In the US, linking health delivery care teams with CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 12 local community organizations (e.g., YMCA, AARP) can also help to normalize use of community resources and other health pathways as tools in interventions. Involving patients and consumers directly in developing health interventions can mitigate disparities, create more culturally sensitive or alternative pathways for care and improve health outcomes. 4 Invest in cultivating patient-centered attitudes among future health leaders In response to the Affordable Care Act’s greater emphasis on and incentives for population health over clinical procedures, US medical schools are beginning to invest in programs that emphasize public health and bedside manner training.37 These schools can supplement some of their efforts with innovations in patient-provider communication and medical training tools from abroad. For instance, administrators at these schools – such as the University of Arizona College of Medicine38 – could form a network with Trish Greenhalg’s team and medical schools internationally implementing “Real Evidence-Based Medicine” to learn from each other’s successes and challenges. Additionally, launching a website in the US based on the German portal “Was Hab’Ich?” could help American medical students improve their patient communications skills and learn from real-life patient cases simultaneously. Efforts like these position young providers to be more open to listening to the consumer perspective in a variety of contexts, from the examination room to the board room, as they ascend the ranks of health institutions. 5 Host a series of multi-national workshops to share lessons about designing, implementing and standardizing patient reported outcomes measures (PROMs) across health systems Individuals working to scale up PROMs in the US, such as those at the National Quality Forum, could participate in a series of workshops with health leaders from other countries who have already achieved scale in their home countries, such as those from the NHS, to share experiences, challenges and subsequent strategies to achieve better quality health care by using patient-reported outcomes. The US has piloted a number of PROMS efforts, especially through the NIH’s PROMIS (Patient Reported Outcomes Measurement Information System) initiative, but has not yet made the leap to establishing systems-wide PROMS standards. Countries outside the US that have successfully integrated PROMS into their health systems quality metrics can teach US institutions how to do the same. 6 Make health reporting data platforms more actionable by linking them with community health services The US can use increasingly popular health tracker platforms, such as those developed for Fitbits, Jawbones and Apple Watches, to connect consumers with local health resources. While US programs like Project HealthDesign have investigated the potential for observations of daily living (ODLs) – sleeping schedule, eating patterns, mood, etc. – to inform clinical encounters, they can also be used to encourage users of ODL-compatible platforms to connect with community health resources, such as community fitness centers, support groups and social prescribing organizations like Health Leads.39 For instance, the devices that collect ODLs could push these suggested resources to their users when the they detect “triggers” related to health issues in the ODL data (e.g., for asthma, hypertension, or heart failure). This would help patients take control of their own care between appointments. A model that has already succeeded in this regard outside the US is the United Arab Emirates’ Weqaya platform, which helps consumers understand their screening data and connect not only with clinical resources, but also with non-traditional health interventions like wellness centers.40 Countries around the world face similar health challenges, such as an increasing chronic disease burden, aging populations and fragmented health systems. Common challenges create the opportunity to share solutions. This report outlines ways in which integrating the consumer perspective into health decision-making at all levels has strengthened health systems and improved health outcomes in a range of settings, and how it may have similar effects in the US. Continued exploration of the ideas generated during the Berlin Roundtable in October 2014 will promote valuable knowledge-sharing about consumer engagement best practices across borders and help the US make strides toward building a culture of health at home. CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 13 REFERENCES 1 Piot P. No time to lose: a life in pursuit of deadly viruses. New York, NY: W.W. Norton and Company, Inc. 2012 Laurance, J, et al. Patient engagement: four case studies that highlight the potential for improved health outcomes and reduced costs. Health Affairs. 2014; 33.9: 1627-34 2 Carman K, Dardess P, Maurer M, et al. Patient and family engagement: A framework for understanding the elements and developing interventions and policies. Health Affairs. 2013; 32(2): 223-231 3 Right to Health, Right to Life: Why we need to act now on HIV and human rights. High level meeting on HIV and human rights in the European Union and neighbouring countries. Joint United Nations Programme (UNAIDS). http://ec.europa.eu/health/sti_prevention/docs/ev_20130527_discussion_paper_en.pdf Published May 2013. Accessed November 25, 2014 4 Equity and Excellence: Liberating the NHS. National Health Service. https://www.gov.uk/government/uploads/system/uploads/attachment_data/ file/213823/dh_117794.pdf Published 2010. Accessed November 19, 2014 5 Wanless D. Securing our future health: Taking a long-term view, final report. April 2002. The Public Enquiry Unit, UK. http://si.easp.es/derechosciudadania/wp-content/uploads/2009/10/4.Informe-Wanless.pdf Published April 2002. Accessed November 19, 2014 6 Background briefing: No Decision about me without me. The Health Foundation and Patient Voices. http://www.health.org.uk/public/ cms/75/76/5620/4282/Background_briefing%20No%20decision%20about%20me%20without%20me.pdf?realName=wETEYR.pdf Published October 5, 2011. Accessed November 19, 2014 7 Patiëntenfederatie NPCF; Who we are and what we do. Nederlandse Patienten Consumenten Federatie website. http://www.npcf.nl/index. php?option=com_content&view=article&id=4164&Itemid=31. Updated April 2014. Accessed November 25, 2014 8 9 Bovenkamp H, Trappenburg M. Government influence on patient organizations. Health Care Anal. 2011; 19:329–351 doi: 10.1007/s10728-010-0155- 7 Weiterentwicklung der Patientenbeteiligung im deutschen Gesundheitswesen. Deutscher Behindertenrat. http://www.vzbv.de/mediapics/weiterentwicklung_patientenbeteiligung_06_2008.pdf Published 2008. Accessed November 19, 2014 10 Conklin A, Slote Morris Z, Nolte E. Involving the public in healthcare policy: An update of the research evidence and proposed evaluation framework. RAND Europe. 2010. 11 12 Greenhalgh T, Maskrey, N. “Evidence-based Medicine: A Movement in Crisis?” BMJ 2014;348:g3725 13 Ashoka innovators for the public. https://www.ashoka.org/fellow/anja-bittner Accessed November 19, 2014 Better Training Better Care infographic. 2012. NHS Health Education England. http://hee.nhs.uk/wp-content/blogs.dir/321/files/2012/09/Final-version-HHE-BTBC-Infographic-v9JPG.jpg Accessed November 19, 2014 14 Better training, better care. NHS Health Education England. 2014; 5:14. http://hee.nhs.uk/wp-content/blogs.dir/321/files/2012/09/BTBC-NewsMarch-April-V19-Final.pdf Accessed November 19, 2014 15 Co-creating health. The Health Foundation. http://www.health.org.uk/areas-of-work/programmes/co-creating-health/ Accessed November 25, 2014 16 Kosmala-Anderson J, Wallace M, Turner A, Bourne C. Self-reported effects of attending the Health Foundation’s Co-Creating Health Self-management programme for patients with type 2 diabetes mellitus in London, England. Arch Med Sci 2014; 10, 4: 773–781 doi: 10.5114/aoms.2014.44869 17 Turner A, Anderson J, Wallace L, Bourne C. An evaluation of a self-management program for patients with long-term conditions. Patient Educ Couns 2014; 10, doi:10.1016/j.pec.2014.08.022 18 Optimising HIV treatment access and retention in care: Linking community level interventions with healthcare delivery systems. Pangaea Global AIDS Foundation, WHO, UNAIDS. Published September 18-20, 2012 19 Vassall A, Chandrashekar S, Pickles M. Community mobilisation and empowerment interventions as part of HIV prevention for female sex workers in Southern India: a cost-effectiveness analysis. PLoS One. 2014; 9(10): e110562 20 Clayton M, Syed F, Rashid A, Fayyaz U. Improving illiterate patients understanding and adherence to discharge medications. BMJ Qual Improv Report 2012; 1: doi:10.1136/bmjquality.u496.w167 21 Hospital value-based purchasing program. Department of Health and Human Services Centers for Medicare and Medicaid Services. http://www. cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/Hospital_VBPurchasing_Fact_Sheet_ICN907664. pdf Published 2013. Accessed November 19, 2014 22 Quality matters. The Commonwealth Fund. December 2011/January 2012 Issue. http://www.commonwealthfund.org/publications/newsletters/ quality-matters/2011/december-january-2012/q-a Accessed November 19, 2104 23 Devlin N, Appleby J, The King’s Fund: Getting the most out of PROMS: Putting health outcomes at the heart of NHS decision-making. 2010. https://www.kingsfund.org.uk/sites/files/kf/Getting-the-most-out-of-PROMs-Nancy-Devlin-John-Appleby-Kings-Fund-March-2010.pdf Accessed November 19, 2014 24 25 European study ranks Bulgaria at healthcare’s bottom. Novinite. http://www.novinite.com/articles/139380/European+Study+Ranks+Bulgar- CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 14 ia+at+Healthcare’s+Bottom Published 2012. Accessed November 19, 2014 EHCI Newsletter. Health Consumer Powerhouse. http://www.healthpowerhouse.com/index.php?option=com_content&view=section&layout=blog&id=1&menu=yes&archive=news&Itemid=1&limitstart=9 Published December 2013. Accessed November 19, 2014 26 Gao G, McCullough J, Agarwal R, Jha A. A changing landscape of physician quality reporting: Analysis of patients’ online ratings of their physicians over a 5-year period. Journal of Medical Internet Research. 2012; Jan-Feb 14(1): e38.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3374528/ Accessed November 19, 2014 27 Case Study: Complete solution for all GP practices launched. I Want Great Care website. http://www.iwgc.org/case-studies/ Accessed November 19, 2014 28 Parmar V, Keyson D, deBont C. Persuasive technology to shape social beliefs: A case of persuasive health information systems for rural women in India,” Comms of the Assoc for Info Sys: 2009; 24 29 Amplifying women’s voices to improve the quality of maternal health care. Merck for Mothers Partners Newsletter. Merck for Mothers. http:// www.gramvaani.org/wp-content/uploads/2013/12/MfM-Partners-Newsletter-Dec-2013.pdf Accessed November 25, 2014 30 Innovation in addressing NCDs: A case study from Abu Dhabi. Actevis Consulting Group. Health G20 Report. http://issuu.com/actevisconsulting/ docs/ncds_abudhabi Accessed November 19, 2014. 31 Sheikh R. Abu Dhabi Weqaya programme tackling NCDs: Application to low and middle income health markets. ITU workshop on “E-health services in low-resource settings: requirements and ITU role.” Tokyo, Japan, Febrary 4-5, 2013. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&uact=8&ved=0CCMQFjAB&url=http%3A%2F%2Fwww.haad.ae%2FHAAD%2FLinkClick.aspx%3Ffileticket%3DVQX0QEUfbWc%253D%26tabid%3D1174&ei=tVN1VNu7JdCJsQSA24C4Aw&usg=AFQjCNHKRBxEhIvDtwAddEuR0LTdwzxj5Q&sig2=9Fzy0V8bu9ydesHv6quuIQ&bvm=bv.80642063,d.cWc Accessed November 25, 2014 32 Genomics England calls on the UK research community. Genomics England. http://www.genomicsengland.co.uk/gecip-domains-eoi-call/ Updated November 12, 2014. Accessed November 25, 2014 33 Notes of the meeting on 24th March, 2014 between patient advocates and Professor Michael Parker and Ms. Vivienne Parry of Genomics England, held at the Angel Building, Islington. Independent Cancer Patient’s Voice. http://independentcancerpatientsvoice.org.uk/app/download/5803451718/Notes+from+meeting+with+Genomics+England+on+24+03.pdf. Updated March 24, 2014. Accessed November 25, 2014 34 Hospital quality initiative overview. Centers for Medicaid and Medicare Services. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/downloads/HospitalOverview.pdf Updated July 2008. Accessed November 25, 2014 35 Realpe A, Wallace L. What is co-production? The Health Foundation. 2010. http://www.health.org.uk/areas-of-work/programmes/co-creating-health/impact/ Accessed November 19, 2014 36 Landro L. The talking cure for health care. The Wall Street Journal. April 8, 2013. http://online.wsj.com/articles/SB10001424127887323628804578 346223960774296 Accessed November 25, 2014 37 Mann S. After reform, more medical schools emphasize public health. Association of American Medical Colleges. https://www.aamc.org/newsroom/reporter/170156/public_health.html Published 2011. Accessed November 25, 2014 38 HealthDesign: Rethinking the power and potential of personal health records. The Robert Wood Johnson Foundation and Project HealthDesign. http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2014/rwjf412107 Updated April 2014. Accessed November 26, 2014 39 Harrison O and Hajat C. The Abu Dhabi cardiovascular program: The continuation of Framingham. Progress in Cardiovascular Diseases 2010; 53: 28-38. 40 Icons provided courtesy of www.flaticon.com under Creative Commons attribution license. CONSUMER POWER TO BUILD BETTER HEALTH SYSTEMS // 15 Participants mid-discussion at the Global Perspectives on Integrating the Consumer Voice across Health Systems Roundtable | Berlin, Germany | 19 October 2014 This report was prepared by Rabin Martin with funding from the Robert Wood Johnson Foundation. Many thanks to Tenley Ghan, Alison Moore, Rebecca Hoppy and Jeffrey L. Sturchio for their contributions to this report.








© Copyright 2026