
Chapter I I
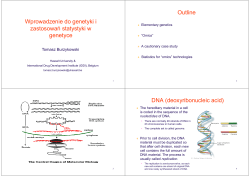
Chapter I INTRODUCTION Cancer is a class of diseases or disorders characterized by uncontrolled/ abnormal division of cells and the ability of these to spread, either by direct growth into adjacent tissue, or by implantation into distant sites by metastasis, in which cancer cells are transported through the bloodstream or lymphatic system. The abnormal cellular division of this is not subject to normal growth controls.1 It is one of the most dreadful diseases due to incurable affliction that insidiously attacks people of all cultures and ages. While, cancer is an ancient disease, the inability to cure cancer has persisted despite impressive advances in scientific knowledge and medical techniques. Though treatment remained the same, in the 16th and 17th centuries it became more acceptable for doctors to dissect bodies to discover the cause of death. The German prof. Wilhelm Fabry believed that breast cancer was caused by a milk clot in a mammary duct and the Dutch prof. Francocis de la, believed that this disease was the outcome of chemical processes, and that acidic lymph fluid was the cause of cancer. His contemporary Nicolaes Tulp believed that cancer was a poison that slowly spreads, and concluded that it was contagious.2 In the 18th century, it was discovered that the 'cancer poison' spread from the primary tumour through the lymph nodes to other sites (metastasis). The use of surgery to treat cancer had poor results due to problems with hygiene. The renowned Scottish surgeon Alexander Monro saw only two breast tumour patients out of 60 surviving surgery for two years. In the 19th century, asepsis (practice to reduce contaminants) improved surgical hygiene and as the survival statistics went up, surgical removal of the tumour became the primary treatment for cancer. When Marie Curie and Pierre Curie discovered radiation at the end of the 19th century, they stumbled upon the first effective non-surgical cancer treatment. The radiotherapy also the first signs of multi-disciplinary approaches to cancer treatment. The improvement in surgical reflects in diagnosing at an earlier and improvements in treatment. Cancer 1 Chapter I is presently responsible for about 25% of all deaths3 and on a yearly basis, 0.5% of the population is diagnosed with cancer. NOMENCLATURE The following terms may be used to designate abnormal growths: Neoplasia and neoplasm are the scientific designations for cancerous diseases. This group contains a large number of different diseases. Neoplasms can be benign or malignant. Cancer is a widely used word that is usually understood as synonymous with malignant neoplasm. It is occasionally used instead of carcinoma, a sub-group of malignant neoplasms. Because of its overwhelming popularity relative to 'neoplasia', it is used frequently instead of 'neoplasia', even by scientists and physicians, especially when discussing neoplastic diseases as a group. Tumour in medical language simply means swelling or lump, either neoplastic, inflammatory or other. In common language, however, it is synonymous with 'neoplasm', either benign or malignant. This is inaccurate since some neoplasms do not usually form tumours, for example leukemia or carcinoma. Paraneoplasia is a disturbance associated with a neoplasm but not related to the invasion of the primary or a secondary tumour. Disturbances can be hormonal, neurological, hematological, biochemical or otherwise clinical. TYPES OF TUMOURS There are over 200 different cancers. The various types of cancer are classified4 by the type of cell that resembles the tumour and, therefore, the tissue presumed to be the origin of the tumour. The following general categories are usually accepted: Carcinoma: malignant tumours derived from epithelial cells. This group represents the most common cancers, including the common forms of breast, prostate, lung and colon cancer. 2 Chapter I Lymphoma and leukemia: malignant tumours derived from blood and bone marrow cells. Sarcoma: malignant tumours derived from connective tissue, or mesenchymal cells. Mesothelioma: tumours derived from the mesothelisal cells lining the peritoneum and the pleura. Glioma: tumours derived from glia, the most common type of brain cell. Germinoma: tumours derived from germ cells, normally found in the testicle and ovary. Choriocarcinoma: malignant tumours derived from the placenta. Malignant tumours are usually named using the Latin or Greek root of the organ as a prefix and the above category name as the suffix. For instance, a malignant tumor of liver cells is called hepatocarcinoma; a malignant tumour of the fat cells is called liposarcoma. For common cancers, the English organ name is used. For instance, the most common type of breast cancer is called ductal carcinoma of the breast or mammary ductal carcinoma. Here, the adjective ductal refers to the appearance of the cancer under the microscope, resembling normal breast ducts. Benign tumours are named using -oma as a suffix with the organ name as the root. For instance, a benign tumour of the smooth muscle of the uterus is called leiomyoma and the common name is fibroid. FACTORS RESPONSIBLE FOR CANCER Cancer causing factors5 have been classified into three major groups include physical, viral and chemical carcinogens. Physical carcinogens include hard and soft X-rays, UV light, asbestos fibres and many other external agents. Viral carcinogens, which for decades were considered not to cause cancer but simply take advantage of a weakened cell, have been positively linked to the onset of specific cancers. Birkett's lymphoma, among Africans and South East China have 3 Chapter I been found to be caused by the Epstein-Barr virus. Cervical cancer is also believed to be associated with the Herpes Simplex Virus Type II, and certain leukemias and lymphomas are caused by the Human T-cell Leukemia virus. Chemical carcinogens are believed to be by far the greatest cause of cancer. They are substances that interact directly or indirectly with DNA, causing changes in the genetic code. TREATMENT OF CANCER Cancer can be treated by surgery, chemotherapy, radiation therapy, immunotherapy, monoclonal antibody therapy or other methods. The choice of therapy depends upon the location and grade of the tumour and the stage of the disease, as well as the general state of the patient. A number of experimental cancer treatments are also under development. Complete removal of the cancer without damage to the rest of the body is the goal of treatment. 1. SURGERY In theory, cancers can be cured if entirely removed by surgery, but this is not always possible. When the cancer has metastasized to other parts in the body prior to surgery, complete surgical excision is usually impossible. Examples of surgical procedures for cancer include mastectomy for breast cancer and prostatectomy for prostate cancer. 2. MONOCLONAL ANTIBODT THERAPY Immunotherapy is the use of immune mechanisms against tumours. These are used in various forms of cancer, such as breast cancer (trastuzumab/Herceptin) and leukemia (gemtuzumab ozogamicin/ Mylotarg). The agents are monoclonal antibodies directed against proteins that are characteristic to the cells of the cancer in question, or cytokines that modulate the immune system's response. 3. IMMUNOTHERAPHY Other, more contemporary methods for generating non-specific immune response against tumours include intravesical Bacille Calmette-Guerin (BCG) 4 Chapter I immunotherapy for superficial bladder cancer, and use of interferon and interleukin. Vaccines to generate non-specific immune responses are the subject of intensive research for a number of tumours, notably malignant melanoma and renal cell carcinoma. 4. RADIATION THERAPHY Radiation therapy also called as radiotherapy, X-ray therapy, or irradiation is the use of ionizing radiation to kill cancer cells and shrink tumours. Radiation therapy can be administered externally via external beam radiotherapy (EBRT) or internally via brachytherapy. Radiation therapy injures or destroys cells in the area being treated by damaging their genetic material, and enables to grow and divide. 5. HORMONAL SUPPRESSION The growth of some cancers can be inhibited by providing or blocking certain hormones. Common examples of hormone-sensitive tumours include certain types of breast and prostate cancers. Removing or blocking estrogen or testosterone is often an important additional treatment. 6. CHEMOTHERAPHY Chemotherapy is the treatment of cancer with drugs that can destroy cancer cells by impeding their growth and reproduction. The first drug used for cancer chemotherapy was not originally intended for that purpose. Mustard gas was used as a chemical warfare agent during World War I and was studied further during World War II. During a military operation in World War II, a group of people were accidentally exposed to mustard gas and were later found to have very low white blood cell (WBC) counts. It was reasoned that an agent that damaged the rapidly growing WBC might have a similar effect on cancer. Therefore, in the 1940s, several patients with advanced lymphomas were given the drug by vein, rather than by breathing the irritating gas. Their improvement, although temporary, was remarkable. That experience led researchers to look for other substances that might 5 Chapter I have similar effects against cancer. As a result, many other drugs have been developed to treat cancer, and drug development since then has exploded into a multi-billion dollar industry. The targeted-therapy revolution has arrived, but the principles and limitations of chemotherapy discovered by the early researchers still apply. Cancer treatment will be entirely based on person’s unique situation. Certain types of cancer respond very differently to a various types of treatment, so determining the type of cancer is a vital step toward knowing which treatments will be the most effective. The cancer's stage will also determine the best course of treatment, since early-stage cancers respond to different therapies than later-stage ones. Person’s overall health, lifestyle, and personal preferences will also play a part in deciding which treatment options will be best. Although chemotherapeutic drugs attack reproducing cells, they cannot differentiate between reproducing cells of normal tissues and cancer cells. The damage to normal cells can result in side effects. These cells usually repair themselves after chemotherapy. Several exciting uses of chemotherapy hold more promise for curing or controlling cancer. New drugs, new combinations of chemotherapy drugs and new delivery techniques are the expected advances in the coming years for curing or controlling cancer and improving the quality of life for people with cancer. Chemotherapeutic drugs are divided into several categories based on how they affect specific chemical substances within the cancer cells, which cellular activities or processes the drug interferes with, and which specific phases of the cell cycle the drug affects. These include DNA interactive agents, DNA topoisomerase I and II inhibitors, carbonic anhydrase (CA) inhibitors, CDK inhibitors, tubulin polymerization inhibitors, antimitotic agents, antimetabolites, and miscellaneous agents. 6 Chapter I TYPES OF CHEMOTHERAPHY DRUGS Chemotherapy drugs are divided into several groups based on how they affect specific chemical substances within cancer cells, which cellular activities or processes the drug interferes with, and which specific phases of the cell cycle the drug affects. ALKYLATING AGENTS These agents directly damage DNA to prevent the cancer cell from reproducing. As a class of drugs, these agents are not phase-specific and in other words, they work in all phases of the cell cycle. NITROSOUREAS Nitrosoureas act in a similar way to alkylating agents. They interfere with enzymes that help copy and repair DNA. They, too, are not phase specific. Unlike many other drugs, these agents are able to travel from the blood to the brain, so they are often used to treat brain tumours. ANTIMETABOLITES These are a class of drugs that interfere with DNA and RNA growth. These agents damage cells during the S phase and are commonly used to treat leukemias, tumours of the breast, ovary, and the gastrointestinal tract, as well as other cancers. ANTHRACYCLINES AND RELATED DRUGS Anthracyclines are antitumour antibiotics that interfere with enzymes involved in DNA replication. These agents work in all phases of the cell cycle. Thus, they are widely used for a variety of cancers. 7 Chapter I TOPOISOMERASE INHIBITORS TOPOISOMERASE INHIBTORS These drugs interfere with enzymes called topoisomerases, which are important in accurate DNA replication. They are used to treat certain leukemias, as well as lung, ovarian, gastrointestinal, and other cancers. MITOTIC INHIBITORS Mitotic inhibitors are plant alkaloids and other compounds derived from natural products. They can stop mitosis or inhibit enzymes from making proteins needed for reproduction of the cell. These work primarily during the M phase of the cell cycle but can cause cellular damage in all phases. CORTICOSTERI HORMONES Steroids are natural hormones and hormone-like drugs that are useful in treating some types of cancer such as lymphoma, leukemias, and multiple myeloma as well as other illnesses. When these drugs are used to kill cancer cells or slow their growth, they are considered chemotherapy drugs. DNA AS A CELLULAR TARGET FOR CHEMOTHERAPEUTIC AGENTS DNA has been considered a favored target for cancer chemotherapeutic agents. Indeed, many of the most effective clinical agents, such as alkylating and intercalating agents, are DNA interactive. Achieving the desired sequence specificity with DNA-interactive agents is considered to be one of the most formidable hurdles in the development of new agents to achieve therapeutic invention. The double helical structure of deoxyribonucleic acid (DNA) represents the richest source of information within a living organism. Importantly, its sequence codes not only for protein/enzyme synthesis via the process of translation, but it also codes for RNA synthesis, which, in light of the discovery of ribozymes, is likely to play a much larger cellular role than previously believed.6 8 Chapter I The structure of DNA (Fig. 1) was established by James Watson and Francis Crick in 1953.7 It consists of two ant parallel strands composed of the nucleotides adenine (A), thymine (T), guanine (G) and cytosine (C), supported on a sugar phosphate backbone. The nucleotides form unique hydrogen bonded pairs (purine with pyrimidine), AT and GC (Fig. 2). Besides the hydrogen bonds between the nucleotides, the double helix is stabilized by electrostatic interactions, vander Waals interactions, complex hydration/dehydration contributions composed of hydrophobic component, solvation electrostatics. The particular order of the bases that are arranged along the sugar-phosphate backbone is called the DNA sequence; the sequence specifies the exact genetic instructions required to create a particular organism with its own unique traits. There are three helical forms of DNA (A, B and Z) that differ with respect to various parameters that describe their three-dimensional structure. However, Bform DNA is the most common one and is more stable under high humidity conditions because water molecules stabilize the structure by forming a spine of hydration in the minor groove.8 Figure 1. Structure of DNA. 9 Chapter I Thymine Cytosine N O Sugar N N H H H N H N Adenine O O N N O Sugar H H N Sugar H N N N H N N N Sugar Guanine N Figure 2. Hydrogen bonding between A-T and G-C base pairs of DNA. In B-DNA, the GC and AT base pairs are stacked in a right-handed double helix, and are hydrogen bonded to one another. Because each base pair contains one two-ringed purine (A or G) and one single-ringed pyrimidine (T or C), the width of each base pair is similar contributing to the smooth cylindrical shape of the double helix. The base pairs are rotated by 36° with respect to each adjacent pair, so that there are 10 pairs per helical turn, each separated by 3.4 Å. This gives rise to two well-defined channels known as the minor and major grooves. The major groove is approximately 24 Å in width and much deeper than minor groove, which is only 10 Å in width.9 Due to it’s predominate form, B-DNA is used in the design of new DNA-binding antitumour drugs. EVALUATION OF DRUG-DNA INTERACTIONS Understanding the forces involved in the binding of proteins or small molecules to DNA is of prime importance due to two major reasons. Firstly, the design of sequence specific drugs having requisite affinity for DNA requires a knowledge how the structure of the drug is related to the specificity/affinity of binding and what structural modifications could result in a drug with desired qualities. Secondly, identifying the forces/energetics involved in such processes is fundamental to unraveling the mystery of molecular recognition in general and DNA binding in particular. 10 Chapter I In recent years, several advances have been made in the elucidation of drugDNA interactions. Spectral methods are available to evaluate the extent of DNAbinding and to know in which sequence the ligand binds. Physical methods like UV-spectroscopy, fluorescence, circular dichorism (CD), optical rotatory dispersion (ORD), IR, Raman spectroscopy and viscometry measurements have been used for the measurement of binding. Thermal denaturation studies on DNA are common and involve measuring the melting point of DNA alone and in the presence of a ligand (drugs). Binding will often stabilize the helix and elevate the melting temperature. However, none of these physical techniques allows determining the specific location of binding on a DNA strand. To do this two types of assays are used namely, strand cleavage assay and affinity cleavage assay.10 Other powerful techniques for studying DNA binding with short lengths of DNA includes NMR and X-ray crystallography,11 which can provide precise structural information about functional groups involved. Three dimensional 1H, 31P NMR experiments such as NOSEY or COSY can be used to locate precisely the ligand on the strand and which can be used in conjugation with computational methods to generate useful 3-dimensional models of ligand-DNA complexes. DNA ‘foot printing’ is an alternative approach that can be used for covalent and noncovalent binders, intercalaters and other type of adducts such as co-ordination complexes and triple helices.12 TYPES OF DRUGS THAT INTERACT WITH DNA The major groups of clinically important DNA reactive agents are covalent and non-covalent binders. 1. NON-COVALENT BINDERS INTERCALATORS Intercalators are molecules that insert perpendicularly into DNA without forming covalent bonds. The only recognized forces that maintain the stability of 11 Chapter I the DNA–intercalators complex, even more than DNA alone, are van der Waals, hydrogen bonding, hydrophobic, and/or charge transfer forces.13 In the early 1960s, Lerman14 conducted a number of physical studies on the interactions of DNA with planar aromatic cations, and concluded that planar aromatic molecules could bind to DNA by a process, which is termed as intercalation. This mode of binding has now been established for a large number of polycyclic aromatic systems which include amonafide and amsacrine (Fig. 3). There are also bis-intercalators like bis-phenazines, which consist of two intercalating moieties joined by a linker, capable of intercalation at two sites separated by a distance defined by the linker length. Other class of intercalators include ethidium bromide and mitoxantrone which is a simplified analogue of the anthracyclines that is easily synthesized and has less toxic side effects, which display antitumour activity by this mechanism. H 3C O N N CH 3 H 3 CO NHSO2 CH 3 H2 N NH2 HN O NH2 Amonafide N Br CH3 N Ethidium dibromide Amsacrine OH NH N N N N O N H N Me N H HN O OH HN O OH O Bis-phenazine Mitoxantrone NH OH Figure 3. DNA intercalators. 12 Chapter I 2. COVALENT BINDERS ALKYLATORS Alkylating agents were among the first anti-cancer drugs and are the most commonly used agents in chemotherapy today. Alkylating agents act directly on DNA, causing cross-linking of DNA strands, abnormal base pairing, or DNA strand breaks, thus preventing the cell from dividing. These agents are generally considered to be cell cycle phase nonspecific, meaning that they kill the cell in various and multiple phases of the cell cycle. Although alkylating agents may be used for most types of cancer, they are generally of greatest value in treating slowgrowing cancers. These are not as effective on rapidly growing cells. Examples of alkylating agents include cisplatin,15 nitrogen-mustards (mechlorethamine, chlorambucil)16 and ethylene amides, methane sulphonic acid esters, nitrosoureas, triazenes (Fig. 4). Figure 4. DNA alkylating agents. 3. DNA STRAND BREAKERS Some DNA-interactive drugs initially intercalate into DNA but then in certain conditions, react in such a way as to generate radicals. The reaction of these radicals with the sugar moieties leads to DNA strand scission. e.g. bleomycin and the enediyne antitumor antibiotics.17 In this category, recently discovered prodrug Phortress 18 (under clinical trials) included which acts by a novel mechanism of AhR (aryl hycrocarbon receptor19) binding and subsequent release of electrophilic intermediates which reacts with DNA in a lethal way leading to selective cell death (Fig. 5). 13 Chapter I Figure 5. DNA strand breakers GROOVE BINDERS Groove binding can be via either major or minor groove by covalently (irreversible) or non-covalently (reversible). 20 It is believed that groove binders with increased selectivity will produce a greater biological response for a given dose (and hence cause fewer toxic side effects) than non-selective groove binders. Molecules that target particular DNA sites also have the potential to be used for the selective suppression of transcription from particular gene sequences.21 For many years the major groove was the focus of most studies aimed at understanding sequence-specific DNA recognition. This emphasis grew largely out of the belief that complementary networks of hydrogen bonds provide the primary basis for specific DNA recognition. There are more hydrogen bond donors and acceptors on the major groove edge of each base pair than on the minor groove edge. There are, therefore, more opportunities for discriminating different base pairs using hydrogen bonds from the major groove. In the minor groove, the principal difference between base pairs is that G-C base pairs contain an exo-cyclic amino group that protrudes into the groove. This amino group makes the steric and electronic environment of the minor groove at G-C base pairs profoundly different from that at A-T base pairs. Thus, while designing ligands to discriminate A-T-rich and G-C-rich DNA sites in the minor groove seemed feasible, the potential for achieving greater sequence discrimination was regarded by many as limited. This picture of the potential for sequence-selective binding in the minor groove has 14 Chapter I changed considerably in the past few years because of several developments. In 1989, Wemmer and colleagues showed that distamycin, the prototypical A-T selective minor groove binder, can bind to DNA as an antiparallel dimer. This unexpected finding forced a re-evaluation of the nature of A-T selectivity and the role of a narrow minor groove in binding site selection. More importantly, the finding raised new possibilities for the design of minor groove binders that are selective for sequences containing mixed A-T and G-C base pairs, or for sequences containing only G-C base pairs. Most of the DNA interactive proteins bind in the major groove, while small molecules of less than 1000 Da, including many antibiotics bind in the minor groove e.g. distamycin,22 netropsin,23 CC-1065,24 pyrrolo[2,1-c][1,4]benzodiazepines,25 Hoechst 33258,26 Mitomycin C 27 (Fig. 6). Figure 6. Minor groove binders. 15 Chapter I ENZYME INHIBITORS Enzyme inhibitors are molecules that bind to enzymes and decrease their activity. Since blocking an enzyme's activity can kill a pathogen or correct a metabolic imbalance, many drugs are enzyme inhibitors. They are also used as herbicides and pesticides. The binding of an inhibitor can stop a substrate from entering the enzyme's active site and/or hinder the enzyme from catalysing its reaction. Inhibitor binding is either reversible or irreversible. Irreversible inhibitors usually react with the enzyme and change it chemically. Many drug molecules are enzyme inhibitors, so their discovery and improvement is an active area of research in biochemistry and pharmacology. A medicinal enzyme inhibitor is often judged by its specificity or lack of binding to other proteins and its potency (its dissociation constant, which indicates the concentration needed to inhibit the enzyme). A high specificity and potency ensure that a drug will have few side effects and thus low toxicity. Some of the example of enzymes wich play key role in cell division are cyclin-dependent kinase, carbonic anhydrase, tubulin polymerisation, topoisomerase I and II etc. CYCLIN-DEPENDENT KINASE (CDK) The cyclin-dependent kinases (CDKs) are a family of serine/threonine protein kinases that play a significant role in cell cycle division.28 In many forms of cancer a deregulation of CDK function and consequent loss of cell cycle control are observed. This suggests that the development of pharmacological inhibitors of CDKs may be an anticancer strategy.29 Uncontrolled cell growth and proliferation are hallmarks of all cancers and are directly linked to cell cycle dysregulation. Cyclin-dependent kinase 2 (CDK2) in complex with cyclins E and/or A is a key cell cycle regulator and continues to be an attractive target for the discovery of new antitumor agents.30 Classically, the cell cycle is defined as the sequence of events leading to the undisturbed division of a cell into two daughter cells. The exit of a differentiated cell from the resting G0 phase is marked by the first gap (G1) phase 16 Chapter I during which the cell prepares for DNA replication in the S phase. This is followed by the second gap phase (G2) that precedes the mitosis. Cell cycle regulatory proteins have been implicated previously in neuronal cell death.31 Cyclin A is produced in the G1 phase, then expressed during the S and G2 phases, while the expression of cyclin B is typically maximal during the G2–M phase transition and controls the passage through the M phase by primarily associating with and activating CDK2.32 3-Amino 9-thio (10H)-acridone and benzothiadiazines (Fig. 7) have inhibited CDK4 kinase activity in vitro. The growth inhibitory effect of benzothiadiazines against CDK4 is due to the partial competetion with ATP by binding to the ATPbinding pocket or by interfering with ATP binding.33 S O N H NH2 S O O NH N O N N Cl C2H 5 F HN S Figure 7. Aminothioacridone and benzothiadiazine exhibiting CDK4 inhibition. Lin and co-workers34 reported triazole-diamine analogues as cyclindependent kinase inhibitors. These compounds showed potent and selective CDK1 and CDK2 inhibitory activities and exhibited IC50 values up to 2.1 nM. S H 2NO2S O F N N N H N F F H 2NO2S NH2 O N H N NH 2 Figure 8. Diamino triazole and pyridine inhibiting CDK . 17 Chapter I CARBONIC ANHYDRASE (CA) The carbonic anhydrase (CA) family of Zn (II) metalloenzymes catalyzes the reversible hydration of CO2 to HCO3. These are involved in various physiological processes associated with pH control, respiration, transport of CO2/HCO3 between metabolizing tissues and the lungs, fluid secretion, biosynthetic reactions, such as the lipogenesis, gluconeogenesis and ureagenesis. 35 Reactions catalyzed by carbonic anhydrase: CO2 + H 2O HCO3 - + H + CA HCO3 - + H 2CO3 CO 2 + H+ H2O (in tissues) ( in lungs) There are fouteen different carbonic anhydrase isoforms have been identified in mammals. It has been known for some time that several of these isozymes are cytosolic (CA I, CAII, CA III, CA VII), CA IV is membrane-bound. CA V is present only in mitochondria, and CA VI is secreted in saliva. The inhibition of CAs has been exploited clinically for several decades for the treatment of a variety of conditions including glaucoma, epilepsy, and gastric ulcers. More recently, CA inhibition has been implicated as playing an important role in cancer progression.36 Generally, an aromatic or heteroaromatic sulfonamide moiety (ArSO2NH2) is the primary recognition element necessary for small molecules to bind the active site of CA. Coordination of the nitrogen atom of the ionized sulfonamide anion (ArSO2NH-) to the active site Zn (II) of CA facilitates this protein-small molecule interaction. Several classical clinical agents from this class of CA inhibitors include acetazolamide (AAZ), methazolamide (MZA), ethoxazolamide (EZA), dichlorophenamide (DCP), brinzolamide (BRZ), dorzolamide (DZA) and indisulam (IND) (Fig. 9) are in phase II clinical trials as an anticancer agent to treat solid tumours.37 18 Chapter I Figure 9. Sulfonamides inhibiting carbonic anhydrase. TUBULIN POLYMERISATION Microtubules (MTs), rigid and hollow cylindrical structures of about 25 nm diameter, are composed of - and -tubulin dimers (Fig. 10). They determine cell shape and play important roles in diverse processes such as cell division, cell motility and migration, cellular transport, and signal transduction. Both and tubulins exist in several isotypic forms and can undergo several post-translational modifications. In higher eukaryotes at least 14 tubulin isotypes have been reported that are expressed in a tissue specific manner. MTs are essential in a diverse array of eukaryotic cell functions, such as mitosis, cell motility, and intracellular organelle transport. Disruption of microtubule leads to cell cycle arrest at G2/M phase followed by apoptotic cell death.38 19 Chapter I Figure 10. Structure of microtubule. Three major classes of antimitotic agents, each with its binding site on tubulin, act to disrupt tubulin dynamics. Compounds that bind to the taxane binding site39 (e.g., paclitaxel and epothilone) act by preventing the depolymerization of tubulin, thus stabilizing microtubules. Compounds that bind to the vinca alkaloid domain (e.g., vincristine, dolastatins, and cryptophycins) and colchicine site binders (e.g., colchicine and combretastatins) inhibit the polymerization of tubulin.39 A number of natural, semi synthetic or fully synthetic new tubulin inhibitors are currently in clinical development like azaepothilone in advanced phase III clinical studies.40 Epothilones are more potent microtubule stabilizers than the taxanes, they are effective against cancer cell lines with high levels of drug resistance, and they induce the regression of taxane-resistant human tumors. Epothilone B (patupilone) has been presently being evaluated in phase III clinical trial. Ixabepilone (Fig. 11), a semi-synthetic analogue of epothilone B, has recently been granted US FDA approval for the treatment of chemotherapy-resistant advanced breast cancer.41,42 20 Chapter I Figure 11. Tubulin target chemotherapeutic agents. Other classes of compounds which exhibit anticancer activity through the inhibition of tubulin polymerization are podophyllotoxin,43 and nocodazole.44 Combretastatin A-4 (CA4) (Fig. 12), which is naturally occurring compound was found to be extremely active inhibitor of tubulin polymerization.45 The major problem associated with CA4 is poor bioavailability and low aqueous solubility.46 However its disodium phosphate prodrug was developed and is currently in phase II clinical trails against solid tumours.47,48 Figure 12. Tubulin interacting agents. 21 Chapter I Since, sulfonamides have been clinically used for many years and found to posses a large number of biological activities, including antibacterial, anticancer, diuretic, and antithyroid activities.49 Recently, sulfonamides have been used in retroviral therapy as HIV protease inhibitors.50 A structure-activity relationship (SAR) study identified two classes of antitumour sulfonamides, represented by N(3-chloro-7-indolyl)-1,4-benzenedisulfonamide (E7070) N-[2-[(4-hydroxy- and phenyl)amino]-3-pyridinyl]-4-methoxybenzene sulfonamide (E7010). E7070 and its analogues belong to a novel class of cell cycle inhibitors that inhibit cell cycle progression at multiple checkpoints. These compounds exert antitumour properties by targeting the G1/S and/or G2/M phases of the cell cycle.51 Recently, E7010 (Fig. 13) has been shown to block cells at mitosis by inhibiting tubulin polymerization. E7010 reversibly binds to the colchicine-binding site of -tubulin, and it displays antitumour activity against both rodent tumors and several types of human tumor xenografts.52 N O O S N H NH OCH 3 H2 NO 2S O O S N H HN Cl OH E7070 E7010 Figure 13. Tubulin polymerization inhibitors. BENZOTHIADIAZINES Benzothiadiazine derivatives (Fig. 14) have shown strong activity against several cancer cell line with ED50 up to 1.1 g/mL.53 Furthermore, Chern and coworkers have reported fused 1,2,4-benzothiadiazine 1,1-dioxides as potential 1adrenoreceptor antagonists as well as anticancer agents54 and styrylbenzo thiadiazine have exhibited antitumour polymerization.55 22 activity by inhibiting tubulin Chapter I H 3 CO O S O O N N N OH S O O N N N H N N N O S N N H Figure 14. Anticancer tricyclic benzothiadiazine derivatives. In addition to this, 1,2,4-benzothiadiazine ring system has shown various biological activities, for example, chlorothiazide and hydrochlorothiazide (Fig. 15) exhibits high degree of diuretic activity with lower toxicity.56 However, 7-chloro-3methyl-4H-1,2,4-benzothiadiazine 1,1-dioxide (diazoxide), is one of the most potent antihypertensive compound which is devoid of the diuretic action.57 O H 2NO2S Cl S O N O H2NO2S Cl N H Chlorothiazide S O NH O Cl N H S O N N H CH3 Diazoxide Hydrochlorothiazide Figure 15. Diuretic benzothiadiazines. Cyclothiazide (Fig. 16) has been found to be one of the most potent compounds in vitro that by removal of AMPA receptors desensitization enhances synaptic transmission, but it does not cross the blood-brain barrier. Later, IDRA 21 fulfills this requirement, by inducing cognitive impairments in patas monkey in improving cognition in rats, and in promoting the induction of long-term potentiation.58 Furthermore, this class of compounds have recently been shown to inhibit hepatitis C virus RNA-dependent RNA polymerase.59 H 2NO2S Cl O S O NH Cl O OH NH N H N H Cyclothiazide S O O IDRA-21 O N H CH3 N O R Anti-viral Figure 16. Bioactive benzothiadiazines. 23 N S R = alkyl Chapter I CURRENT AREA OF WORK As discussed above, the design and synthesis of agents capable of specifically inhibiting the expression of particular proteins critical for tumour cell proliferation, metastasis or drug resistance is an important. In recent years, combination chemotherapy with different mechanisms of action is one of the methods that is being adopted to treat cancer. Therefore, a single molecule containing more than one pharmacophore, each with different mode of action, could be beneficial for the treatment of cancer. PYRROLO[2,1-C][1,4]BENZODIAZEPINES AS DNA BINDING ANTITUMOUR ANTIBIOTICS 10 9 8 N 11 A 7 6 B 5 O H 11a N C 3 R8 1 2 CH3O HO H N R H3C H3CHN Tomaymycin (R7 = OCH3, R8 = OH, R = CH3) Prothracarcin (R7 = R8 = H, R = CH3) Sibanomycine (R8 = H, R7 = sibirosamine pyronoside as in , R = Et) H N OCH3 H CH3 O OH OH Sibiromycin 8 Chicamycin A OH N N H N H3CO OH O H N O CH3 O HO H N H3CO R1 CON R2 Anthramycin (R8 = CH3, R9 = R1 = R2 = H) Mazethramycin (R8 = R1 = CH3, R9 = R2 = H) Porothramycin B (R8 = H, R9 = R1 = R2 = CH3) O HO H O N R7 OCH3 N PBD ring system R8 OR9 H N O R1 R2 Neothramycin A ( R1 = H; R2 = OH) Neothramycin B ( R1 = OH, R2 = H) DC-81 (R1 = R2 = H) Figure 17. Naturally occurring PBDs. 24 Chapter I The pyrrolo[2,1-c][1,4]benzodiazepines (PBDs) are a family of DNAinteractive antitumour antibiotics derived from various Streptomyces species. To date thirteen structures which include anthramycin,60 mezethramycin,61 porothramycin,62 prothracarcin,63 sibanomycine,64 tomaymycin,65 sibiromycin,66 chicamycin A,67 neothramycin A, B68 DC-81,69 and abbeymycin70 have been isolated from various Streptomyces species (Fig. 17). PBD-DNA INTERACTIONS The known PBD natural products have a (S)-configuration at the C11aposition, which provides them with a right-handed twist when viewed from the Cring towards the A-ring. This has given the appropriate three-dimensional shape for isohelicity with the minor groove of DNA, leading to a snug fit at the binding site. Recemization at C11a can significantly reduce both DNA binding affinity and in vitro cytotoxicity. A synthetic PBD with the (R)-configuration at C11a was shown to be devoid of both DNA binding affinity and in vitro cytotoxicity. The N10-C11 imine moiety may exist in the hydrated form depending upon precise structure of the compound and the method of isolation or synthetic work up. Imines and methyl ether forms are interconvertable by dissolution of imine in methanol or by several cycles of refluxing the methyl ether in chloroform followed by evaporation of the solvent in vacuum. 71 N H H2 O N O H N N -H 2O O CH 3OH -CH 3OH OH H H N OCH 3 H N O 25 H 2O CH 3OH Chapter I The pyrrolo[2,1-c][1,4]benzodiazepine (PBD) interactions with DNA are unique since they bind within the minor groove of DNA forming a covalent aminal bond between the C11-position of the central B-ring and the N2 amino group of a guanine base.72 The cytotoxic and antitumour activity of PBDs are attributed to their ability to form covalent DNA adducts. Molecular modeling, solution NMR, fluorimetry and DNA foot printing experiments have shown that these molecules have a preferred selectivity for Pu-G-Pu sequences73 are oriented with their A-rings pointed either towards the 3' or 5' end of the covalently bonded DNA strand (as in case of anthramycin and tomaymycin). The PBDs have been shown to interfere with the action of endonuclease enzymes on DNA and to block transcription by inhibiting DNA polymerase in a sequence specific manner74 processes which may be relevant for the biological activity. NH2-Guanine-DNA H N OR H R =H R = CH3 N O NH2 N Guanine-DNA H N N O NH-Guanine-DNA H NH2-Guanine-DNA N N H N O O 26 Chapter I STRUCTURE-ACTIVITY RELATIONSHIPS Structure activity relationships (SAR) for this ring system have been derived by Thurston and co-workers as shown below. (g) Electron-donating substituents required at position 7,8 or 9 of A-ring (h) Bulky substituents at N10 (eg. acetyl) inhibit DNAbinding and cytotoxicity (b) (S)-Stereochemistry required at C11a R9 R8 R7 (f ) Sugar moiety at C7 enhances DNA-binding af f inity and cytotoxicity in some cell lines (a) An imine, carbinolamine methyl ether required at N10-C11 N 10 11 N H 11a O 3 1 2 (c) Replacement of C1 with an oxygen maintains cytotoxicity R (d) Endocyclic or exocyclic unsaturation at C2 enhances cytotoxicity and in vivo antitumour activity. Fully unsaturated C-ring leads to (e) Small substituents (eg. -OH) complete loss of DNA-binding tolerated at C3 in f ully saturated and cytotoxicity C-ring compounds SYNTHETIC APPROACHES FOR PYRROLO[2,1-C][1,4]BENZODIAZEPINES The first total synthesis of a carbinolamine containing PBD of anthramycin has been reported by Leimgruber in 1968.6475 Extensive reviews of the synthetic literature of the PBDs have appeared in 1994, 1998 and 2002.76 Various approaches to the synthesis of PBD antibiotics have been investigated, including hydride reduction of seven member cyclic dilactams,77 reductive cyclization of acyclic nitroaldehydes,78 iminothioether approach79 cyclization of aminothioacetals,80 deprotective cyclization of the diethylthioacetals via N10 protected precursors,81 oxidation of cyclic secondary amines,82 reductive cyclizations83 and solid phase approaches. 84 27 Chapter I KANEKO APPROACH (IMINOTHIOETHER REDUCTION) Kaneko and co-workers77a have developed an efficient method for the reduction of PBD dilactams to the carbinolamine using aluminium amalgam. This methodology has been extended to the preparation of bicyclic and tricyclic analogues of anthramycin, the total synthesis of some naturally occurring PBDs like chicamycin.79b By using this approach Baraldi and co-workers have synthesized some heterocyclic PBD analogues in which the A ring of PBD skeleton is replaced with a 1,3 or 1,5-disubstituted pyrazole nucleus. H N R1 R1 R2 H N R2 O H N O (i) R2 N R1 R2 N O R3 O R2 (v) S R1 R2 SR 4 H N N R3 O H N R3 S (iii) N H N R3 O (iv) + R3 (ii) R1 R2 H N R1 OCH 3 H H + R3 R1 H N S R1 R2 H N H N O H N SR 4 H N O R3 R3 R 1 = H, OH, OBn, OCH3 , OAc R 2 = H, OCH3 R 3 = H, = CH-CH 3 (E), OH (a), OAc (b), = CH-COOEt (E) R 4 = CH 3 Reagents and condit ions: (i) P 2S 5, C6 H 6, 80 o C or P2 S 5, NaHCO3 , CH3 CN, 15 min, or (pCH3 OC 6H 4PS 2 )2 , C 6H 6, 80 o C; (ii) Et 3 OBF4 , CH 2 Cl2 , KHCO3 or CH3 I, K 2CO3 , THF or DMF; (iii) AlHg, aq.THF or KH 2PO4 , 0-5 oC, 14 h; (iv) 0.1 N methanolic HgCl2 , 0 oC or SiO2 chromatography, 5 o C; (v) CH 3 OH. 28 Chapter I THURSTON’S APPROACH Thurston and co-workers70a have developed an efficient method for the synthesis of various PBDs containing carbinolamine moiety by employing mercuric chloride (HgCl2) and calcium carbonate (CaCO3) in aqueous acetonitrile at room temperature. RO H 3CO PhH2 CO (ii) NO2 H3 CO COOH (iii) COOH PhH 2 CO NO2 CH(SEt) 2 N H 3 CO O (i) aR=H b R = PhCH 2 (iv) RO N H (v) N H 3CO O (vi) PhH 2CO NH 2 H 3CO N CH(SEt)2 O a R = PhCH 2 b R=H Reagents and conditions : (i) PhCH 2Cl, THF, NaOH, H2 O, reflux, 48 h; (ii) SnCl4, HNO 3, CH 2 Cl2 , 25 o C,5 min; (iii) (COCl) 2, THF, DMF, 3 h then, pyrrolidine-2-carboxaldehyde diethyl thioacetal, Et3 N, H2 O, 0 oC, 1.5 h; (iv) SnCl2.2H2 O, MeOH, reflux, 45 min; (v) HgCl2 , CaCO3 , CH3 CN-H 2 O, 12 h; (vi) 10% Pd-C, EtOH, cyclohexadiene, 3 h. Baraldi and co-workers85 synthesized hybrid molecules containing PBD and minor groove binding oligo-pyrrole carriers, while Hurley and co-workers86 have synthesized AT-groove binding hybrids by using this approach. In the same manner Suzuki coupling of C7 aryl substituted PBDs have been synthesized by Thurston and co-workers.87 This B-ring strategy of Fukuyama and coworkers has also been employed for the synthesis of C2/C2'-exo-unsaturated PBD dimer, C2-C3/C2'-C3'endo unsaturated PBD dimer with remarkable covalent DNA binding affinity. 29 Chapter I C8-LINKED PYRROLO[2,1-C][1,4]BENZODIAZEPINE HYBRIDS In the search for compounds with better antitumour selectivity and DNA sequence specificity many C8-linked hybrids of pyrrolo[2,1-c][1,4]benzodiazepines have been prepared. In recent years, bifunctional DNA interactive agents comprising of two types of antitumour agents joined by a linker have attracted considerable attention as a new class of antitumour agents. These compounds are capable of recognizing heterogeneous DNA sequences. Baraldi and co-workers88 have been designed and synthesized distamycinPBD and netropsin-PBD conjugates as novel sequence selective C8-linked PBD hybrids. These hybrids containing 1 to 4 pyrrole units have been investigated for the sequence selectivity and stability of DNA drug complexes. H 2N H N H N HCl HN O N N O O n H N H3 CO O n = 1-4 Hurley and co-workers89 have synthesized novel DNA-DNA interstrand adenine-guanine cross-linking UTA-6026 compound. Preliminary in vitro tests showed that UTA-6026 has remarkably potent cytotoxicity to several tumour cell lines (IC50 = 0.28 nM in human breast tumour cell line MCF-7, IC50 = 0.047 nM in colon tumour cell line SW-480 and IC50 = 5.1 nM in human lung tumour cell line A549). H 3C N H H N N O O N O N H N H3CO O H O Lown and co-workers90 have also reported the synthesis of a series of PBDlexitropsin conjugates linked through the C8 position with a suitable linker. The conjugation has been achieved by amidic linkage to amine of the lexitropsin unit 30 Chapter I with the acid moiety of the linker attached to the PBD system. These compounds have been synthesized in view of the effect with sequence selective binding in DNA duplex. H N CH3 H 3C H N N H O N O O N H3 CO n H O n = 1-3 Denny and co-workers91 have designed and synthesized unsymmetrical DNA cross-linkers by linking the seco-1,2,9,9a-tetrahydrocyclopropa[c]benz[e]indo4-one (seco-CBI) to PBD moiety. These compounds have anticipated cross-linking between N3 of adenine and N2 of guanine in the minor groove of DNA. Cl O N O N H N H3CO O OH Thurston and co-workers92 have been reported the synthesis and anticancer activity of C8-epoxide linked pyrrolo[2,1-c][1,4]benzodiazepine. O N O H N H3CO O Recently, Wang and co-workers93 have designed and synthesized novel PBDindole conjugates. Further, these conjugates have been tested against a panel of 60 human cancer cell lines by NCI and demonstrated that PBD-indole conjugates exhibited a higher level of cytotoxic activity than the existing natural and synthetic PBDs and can activate the apoptotic pathway mediated by mitochondria. 31 Chapter I N O N H O H3 CO H N O Lown and co-workers94 have designed and synthesized novel PBDgylcosylated pyrrol and imidazole polyamide conjugates and described as water insoluble and water-soluble PBD conjugates. H OH HO N H N H HO H OH O O OCH 3 O H OH N N H N H n = 1, 2 H OH HO N H N OCH3 O H H OH CH3 O N O O O X NH n N CH 3 CH 3 HO OH N N H H O N H n N CH 3 CH 3 X = CH, n = 2 X = N, n = 2 Kamal and co-workers95 have synthesized a series of PBD conjugates by linking different DNA interacting ligands such as benzimidazole, polyaromatic hydrocarbons (pyrene amine and chrysene amine), anthraquinones, by using varying linker length to enhance the DNA binding affinity and antitumour activity. All these prepared molecules have shown good DNA binding affinity with better anticancer activity. 32 Chapter I H N N H 3C O N N (CH 2) n O N N H3 CO O n = 3-5 O H N (CH2 )n O N O H 3CO O H HN n O H 3CO N O n = 3-4 H O N H N O n = 3-4 Kamal and co-workers96 have designed and synthesized PBD-morpholine, N-methyl piperizine and N,N-dimethyl amine hybrids in attempts to improve the water solubility and cytotoxicity of the PBD compounds. O N O N H N H 3CO O APOPTOSIS AS CELLULAR TARGET FOR CANCER Apoptosis, is a physiological process that plays a essential role in controlling cell number in many developmental and physiological settings and in chemotherapyinduced tumour-cell killing.97-100 It is a genetically regulated biological process, guided by the ratio of proapoptotic and antiapoptotic proteins.101 Inhibition of apoptosis enhances the survival of cancer cells and facilitates their escape from immune surveillance and cytotoxic therapies. Among the principal molecules contributing to this phenomenon are the inhibitor of apoptosis (IAP) proteins, a family of anti apoptotic regulators that block cell death in response to diverse stimuli through interactions with inducers and effectors of apoptosis.102 There are two major apoptosis signaling pathways, that is, the death receptor (extrinsic) pathway and the mitichondria (intrinsic) pathway (Fig. 18)103 Apoptosis is executed by a subfamily of cysteine proteases known as caspases under most circumstances, activation of either pathway eventually leads to proteolytic cleavage 33 Chapter I and thus activation of caspases, that act as common death effector molecules. Caspases are responsible for many of the biochemical and morphological hallmarks of apoptotic ell death by cleaving a range of substrates in cytoplasm or nucleus.104 In mammalian cells, a major caspase activation pathway is the cytochrome c-initiated pathway. In this pathway, a variety of apoptotic stimuli cause cytochrome c release from mitochondria, which in turn induces a series of biochemical reactions that result in caspase activation and subsequent cell death.104 Disruption of mitochondrial fuction appears to be an early feature of apoptotic cell death. Several different biochemical changes have been shown, including the generation of reactive oxygen species (ROS), calcium flux, loss of the mitochondrial membrane potential, and cytochrome release.105 The mitochondrial pathway of apoptosis proceeds when molecules sequestered between the outer and inner mitochondrial membranes are released to the cytosol by mitochondrial outer membrane permeabilization (MOMP). This process is controlled by the BCL-2 family, which is composed of both pro- and anti-apoptotic proteins.106 Apoptosis is also highly characterized by a series of typical morphological events, such as DNA fragmentation, chromatin condensation, membrane blebbing and cell shrinkage. Cells undergoing apoptosis ultimately dissameble into membrane enclosed vesicles (apoptotic bodies) that are engulfied by neighbouring cells and phagocytes, thus preventing an inflammatory response.107 34 Chapter I Figure 18. Schematic representation of apoptosis pathway. Further, killing of cancer cells by current therapies is largely due to induction of apoptosis in tumour cells. Since a hallmark of human cancers is their resistance to apoptosis, there is a demand to develop novel strategies that restore the apoptotic machinery in order to overcome cancer resistance.108 Numerous novel approaches are currently being followed employing gene therapy and antisense strategies, recombinant biologics or classical organic and combinatorial chemistry in order to target specific apoptotic regulators.109-112 New drugs that could modulate the expression of molecules involved in the apoptotic pathway with the ability to induce apoptosis in multidrug-resistant or apoptosis resistant tumour cell lines are of great importance in cancer chemotherapy. Therefore the identification of apoptosis inducers represents an attractive approach for the discovery and develpomemt of potential anticancer agents.Moreover, by induceing apoptosis, these new agents may overcome tumour resitance to conventional anticancer agents.113 35 Chapter I REFERENCES 1. Benowitz, S. I.; Cancer. Ed.; Heights, B. N. J. Enslow Publishers, 1999, pp 1128. 2. Marilyn Yalom "A history of the breast" 1997 Publisher: New York: Alfred A. Knopf ISBN 0-679-43459-3. 3. Jemal, A.; Murray, T.; Ward, E.; Samuels, A.; Tiwari, R. C.; Ghafoor, A.; Feuer, E. J.; Thun, M. J. CA Cancer J. Clin. 2005, 55, 10. 4. The Merck manual of medical information, 2nd edition. Ed.; by Mark, H. Beers. Published by Merck research laboratories, Whitehouse Station, NJ, 2003. 5. Warshawsky, D.; Landolph, J. R. Molecular carcinogenesis and the molecular biology of human cancer. Published by CRC press, Taylor and Francis; 2006, pp 1-400. 6. (a) Cech, T. R. Annu. Rev. Biochem. 1990, 59, 543. (b) Michel, F.; Ferat, J. L. Annu. Rev. Biochem. 1995, 64, 435. 7. Watson, J. D.; Crick, F. H. C. Nature 1953, (London), 171, 737. 8. (a) Hsiang, Y. H.; Jiang, T. B.; Lieu, L. F. Mol. Pharmacol. 1989, 36, 371. (b) Yamashita, Y.; Kawada, S. Z.; Nakano, H. Biochemistry 1991, 30, 5838. (c) Franklin, R. E.; Gosting, R. G. Trans. Faraday Soc. 1954, 50, 298. 9. Dickerson, R. E. Scientific American 1983, 249, 87. 10. Patel, D. J.; Shapiro, L. Annu. Rev. Biophys. Chem. 1987, 16, 423. 11. Thurston, D.E.; Thomson, A. S. Chemistry in Britain 1990, 767, 1983. 12. Harris, T. M.; Stone, M. P.; Harris, C. M. Chem. Res. Toxicol. 1988, 1, 79. 13. (a) Waring, M. J.; Bailly, C. Gene 1994, 149, 69; (b) Rehn, C.; Pindur, U. Monatsh. Chem. 1996, 127, 631; (c) Baginski, M.; Fogolari, F; Briggs, J. M. J. Mol. Biol. 1997, 274, 253; (d) Shui, X.; Peek, M. E.; Lipscomb, L. A.; Gao, Q.; Ogata, C.; Roques, B. P.; Garbay-Jaureguiberry, C.; Wilkinson, A. P.; Williams, L. D. Curr. Med. Chem. 2000, 7, 59. 14. Lerman, L. S. J. Mol. Biol. 1961, 3, 18. 15. Sherman, S. E.; Lippard, S. J. Chem. Rev. 1987, 87, 1153. 36 Chapter I 16. Gilman, A.; Phillips, F. S. Science 1946, 103, 409. 17. Nicolaou, K. C.; Dai, W. M. Angew. Chem. int. Ed. Engl. 1991, 30, 1387. 18. Bradshaw, T. D.; Westwell, A. D.; Curr. Med. Chemistry, 2004, 11, 1241. 19. Bradshaw, T. D.; Trapani, V.; Vasselin, D. A.; Westwell, A. D. Curr. Pharm. Des.; 2002, 8, 2475. 20. Reddy, B. S. P.; Sondhi, S. M.; Lown, J. W. Pharmacol. Ther. 1999, 84, 1. 21. (a) Snyder, R.C.; Ray, R.; Blume, S.; Miller, D.M. Biochemistry 1991, 30, 4290. (b) Ho, S.N.; Boyer, S.H.; Schreiber, S.L.; Danishefsky, S.J.; Crabtree, C. R. Proc. Nat. Acad. Sci. USA. 1994, 91, 9203. 22. Zimmur, C. Prog. Nucleic Acid Res. Mol. Biol. 1975, 15, 285. 23. Wartell, R. N.; Larson, J. E.; Wells, R. E. J. Biol. Chem. 1974, 249, 6719. 24. Hurley, L. H.; Renolds, V. L.; Swernson, D. H.; Petzold, G. L. and Scahill, T. A.Science 1984, 226, 843. 25. Dwyer, P. J.; Shoemaker, D.; Zaharko, D. S.; Grieshaber, C.; Plowman, Cancer Chemother. Pharmacol. 1987, 19, 6. 26. Karlovsky, P.; deCock, A. W. Anal Biochem. 1991, 194, 192. 27. Maria, T. Chemistry and Biology, 1995, 2, 575. 28. Malumbres, M.; Barbacid, M. Trends in Biochem. Sci. 2005, 30, 630. 29. Fischer, P. M.; Gianella-Borradori, A. Expert Opin. Investig. Drugs 2003, 12, 955. 30. (a) Huwe, A.; Mazitschek, R.; Giannis, A. Angew. Chem., Int. Ed. 2003, 42, 2122. (b) Kong, N.; Fotouhi, N.; Wovkulich, P. M.; Roberts, J. Drugs Future 2003, 28, 881. 31. (a) Park, D.S., Morris, E.J., Greene, L.A., Geller, H.M.,. J. Neuroscience 1997, 17, 1256. (b) Nagy, Z. Neurobiology of Aging 2000, 6, 761. 32. Guadagno, T. M.; Newport, J. W. Cell 1996, 84, 73. 33. Kubo, A.; Nakagawa, K.; Varma, R. K.; Conrad, N. K.; Cheng, J. Q.; Lee, W.C.; Testa, J. R.; Johnson, B. E.; Kaye, F. J.; Kelly, M. J. Clinical Cancer Res. 1999, 5, 4279. 37 Chapter I 34. Lin, R.; Connolly, P. J.; Huang, S.; Wetter, S. K.; Lu, Y.; Murray, W. V.; Emanuel, S. L.; Gruninger, R. H.; Fuentes-Pesquera, A. R.; Rugg, C. A.; Middleton, S. A.; Jolliffe, L. K. J. Med. Chem. 2005, 48, 4208. 35. (a) Cabiscol, E.; Levine, R. L. J. Biol. Chem. 1995, 270, 14742. (b) Maren, T. H. In Carbonic Anhydrase-From Biochemistry and Genetics to Physiology and Clinical Medicine, Botre, F.; Gros, G.; Storey, B. T.; Eds.; VCH: Weinhein, 1991, pp 186207. (c) Supuran, C. T.; Scozzofava, A. Exp. Opin. Ther. Patents 2000, 10, 575. 36. (a) Scozzafava, A.; Owa, T.; Mastrolorenzo, A.; Supuran, C. T. Curr. Med. Chem. 2003, 10, 925. (b) Pastorekova, S.; Casini, A.; Scozzafava, A.; Vullo, D.; Pastorek, J.; Supuran, C. T. Bioorg. Med. Chem. Lett. 2004, 14, 869. 37. Beasley, Y. M.; Overell, B. G.; Petrow, V.; Stephenson, O. J. Pharm. Pharmacol. 1958, 10, 696. 38. Pasquier, E.; Kavallaris, M. IUBMB Life. 2008, 60, 165. 39. (a) Nicolau, K. C.; Dai, W.-M.; Guy, R. K. Angew. Chem. Int. Ed. 1994, 33, 15. (b) von Angerer, E. Expert Opin. Ther. Pat. 1999, 9, 1069. 40. Beckers, T.; Mahboobi, S. Drugs Future 2003, 28, 767-785. 41. Goodin, S. Am. J. Health. Syst. Pharm. 2008, 65, S10. 42. Pronzato, P. Drugs 2008; 68, 139. 43. Canel, C.; Moraes, R. M.; Dayan, F. E.; Ferreira, D. Phytochemistry 2000, 54, 115. 44. Kavallaris, M.; Verrills, N. M.; Hill, B. T. Drug. Resist. Update 2001, 4, 392. 45. Lin, C. M.; Ho, H. H.; Pettit, G. R.; Hamel, E. Biochem. 1989, 28, 6984. 46. Wang, L.; Woods, K. W.; Li, Q.; Barr, K. J.; McCroskey, R. W.; Hannick, S. M.; Gherke, L.; Credo, R. B.; Hui,Y-H.; Marsh, K.; Warner, R.; Lee, J. Y.; ZielinskiMozng, N.; Frost, D.; Rosenberg, S. H.; Sham, H. L. J. Med. Chem. 2002, 45, 1697. 47. Dowlati, A.; Robertson, K.; Cooney, M.; Petros, W. P.; Stratford, M.; Jesberger, J.; Rafie, N.; Overmoyer, B.; Makkar, V.; Stambler, B.; Taylor, A.; Waas, J.; Lewin, J. S.; McCrae, K. R.; Remick, S. C. Cancer Res. 2002, 62, 3408. 38 Chapter I 48. Buolamwini, J. K. Curr. Opin. Chem. Biol. 1999, 3, 500. 49. (a) Koyanagi, N., Nagasu, T., Fujita, F., Watanabe, T., Tsukahara, K., Funahashi, Y., Fujita, M., Taguchi, T., Yoshino, H., and Kitoh, K. Cancer Res. 1994, 54, 1702. (b) Scozzafava, A., Owa, T., Mastrolorenzo, A., and Supuran, C. T. Curr. Med. Chem. 2003, 10, 925. 50. Ghosh, K. A., Swanson, M. L., Cho, H., Leschenko, S., Hussain, A. K., Kays, S., Walker, E. D., Koh, Y., and Mitsuya, H. J. Med. Chem. 2005, 48, 3576. 51. Owa, T., Yoshino, H., Yoshimatsu, K., and Nagasu, T. Curr. Med. Chem. 2001, 8, 1487. 52. Nihei, Y., Suzuki, M., Okano, A., Tsuji, T., Akiyama, Y., Tsuruo, T., Saito, S., Hori, K., and Sato, Y. Jpn. J. Cancer Res. 1999, 90, 1387. 53. (a) Chern, J.-H.; Rong, J.-G. Tetrahedron Lett. 1991, 32, 2935. (b) Chern, J.-H.; Liaw, Y.-C.; Chen, C.-S.; Rong, J.-G.; Huang, C.-L.; Chan, C.-H.; Wang, A. H.J. Heterocycles 1993, 36, 1993. 54. (a) Chern, J.-W.; Tao, P.-L.; Wang, K.-C.; Gutcait, A.; Liu, S.-W.; Yen, M.-H.; Chien, S.-L.; Rong, J.-K. J. Med. Chem. 1998, 41, 3128. (b) Chern, J.-W.; Leu, Y.L.; Wang, S.-S.; Jou, R.; Lee, C.-F.; Tsou, P.-C.; Hsu, S.-C.; Liaw, Y.-C.; Lin, H.M. J. Med. Chem. 1997, 40, 2276. 55. Jiang, B.; Hesson, D. P.; Dusak, B. A.; Dexter, D. L.; Kang, G. J.; Hamel, E. J. Med. Chem. 1990, 33, 1721. 56. Werner, L. H.; Halamandaris, A.; Jr. Rica, S.; Dorfman, L.; de-Stevens, G. J. Am. Chem. Soc. 1960, 82, 1161. 57. Topliss, J. G.; Konzelmann, L. M.; Shapiro, E. P.; Sperber, N.; Roth, F. E. J. Med. Chem. 1964, 7, 269. 58. Braghiroli, D.; Puia, G.; Cannazza, G.; Tait, A.; Parenti, C.; Losi, G.; Baraldi, M. J. Med. Chem. 2002, 45, 2355. 59. Tedesco, R.; Shaw, A. N.; Bambal, R.; Chai, D.; Concha, N. O.; Darcy, M. G.; Dhanak, D.; Fitch, D. M.; Gates, A.; Gerhardt, W. G.; Halegoua, D. L.; Han, C.; Hofmann, G. A.; Johnston, V. K.; Kaura, A. C.; Liu, N.; Keenan, R. M.; Lin39 Chapter I Goerke, J.; Sarisky, R. T.; Wiggall, K. J.; Zimmerman, M.N.; Duffy, K. J. J. Med. Chem. 2006, 49, 971. 60. (a) Leimgruber, W.; Stefanovic, V.; Schenker, F.; Karr, A.; Berger, J. J. Am. Chem. Soc. 1965, 87, 5791; (b) Arora, S. K. Acta Crystallogr. 1979, B35, 2945. 61. Kunimoto, S.; Masuda, T.; Kanbayashi, N.; Hamada, M., Naganawa, H.; Miamota, M.; Takeuchi, T.; Umezawa, H. J. Antibiot. 1980, 33, 665. 62. Tsunkawa, M.; Kamei, H.; Konishi, M.; Miyaki, T.; Oki, T.; Kawakuchi, H. J. Antibiot. 1988, 41, 1366. 63. Shimizu, K. –I.; Kawamoto, I.; Tomita, F.; Morimoto, M.; Fujimoto, K. J. Antibiot. 1982, 35, 972. 64. Hara, M.; Tamaoki, T.; Yoshida, M.; Morimoto, M.; Nakano, H. J. Antibiot. 1988, 41, 702. 65. (a) Nishioka, Y.; Beppu, T.; Kohsaka, M.; Arima, K. J. Antibiot. 1972, 25, 660. (b) Tazuka, Z.; Takaya, T. J. Antibiot. 1983, 36, 142. 66. Leber, J. D.; Hoover, J. R. E.; Holden, K. G., Johnson, R. K.; Hecht, S. M. J. Am. Chem. Soc. 1988, 110, 2992. 67. Konishi, M.; Ohkuma, H.; Naruse, N.; Kawaguchi, H. J. Antibiot. 1984, 37, 200. 68. Takeuchi, T.; Miamota, M.; Ishizuka, M.; Naganawa, H.; Kondo, S.; Hamada, M.; Umezawa, H. J. Antibiot. 1976, 29, 93. 69. Kyowa Hakko Kogyo Co. Ltd., Jpn Kokai Tokyo Koho JP 58180487, 21 Oct 1983; Chem. Abstr. 1984, 100, 173150. 70. Hochlowski, J. E.; Andres, W. W.; Theriault, R. J.; Jackson, M.; McAlpine J. B. J. Antibiot. 1987, 40, 145. 71. Kopka, M. L.; Goodsell, D. S.; Baikalov, I.; Grzeskowiak, K.; Cascio, D.; Dickerson, R. E. Biochemistry 1994, 33, 13593. 72. (a) Thurston, D. E. Advances in the Study of Pyrrolo[2,1-c][1,4]benzodiazepine (PBD) Antitumour Antibiotics. Molecular Aspects of Anticancer Drug-DNA Interactions; The Macmillan Press Ltd.; London, U.K., 1993, pp 54-88; (b) 40 Chapter I Petrusek, R. L.; Uhlenhopp, E. L.; Duteau, N.; Hurley, L. H. J. Biol. Chem. 1982, 257, 6207. 73. (a) Hurley, L. H.; Reck, T.; Thurston, D. E.; Langley, D. R.; Holder, K. G.; Hertzberg, R. P.; Hwover, J. R. E.; Gallegher, G.; Faucette, L. F. Jr.; Mong, S. M.; Johnson, R. K. Chem. Res. Toxicol. 1988, 1, 258; (b) Boyd, F. L.; Stewart, D.; Remers, W. A.; Barkley, M. D.; Hurley, L. H. Biochemistry 1990, 29, 2387. 74. Puvvada, M. S.; Forrow, S. A.; Hartley, J. A.; Stephenson, P.; Gibson, I.; Jenkins, T. C.; Thurston, D. E. Biochemistry 1997, 36, 2478. 75. Leimgruber, W.; Batcho, A. D.; Czajkowski, R. C. J. Am. Chem. Soc. 1968, 90, 5641. 76. (a) Thurston, D. E.; Bose, D. S. Chem. Rev. 1994, 94, 433; (b) Kamal, A.; Rao, M. V.; Reddy, B. S. N. Khim. Getero. Soed. (Chemistry of Heterocyclic Compounds), 1998, 1588; (c) Kamal, A.; Rao, M. V.; Laxman, N.; Ramesh, G.; Reddy, G. S. K. Current Medicinal Chemistry – Anti-Cancer Agents 2002, 2, 215. 77. (a) Kaneko, T.; Wong, H.; Doyle, T. W. Tetrahedron Lett. 1983, 24, 5165; (b) Suggs, J. W.; Wang, Y. S.; Lee, K. S. Tetrahedron Lett. 1985, 26, 4871. 78. Lown, J. W.; Joshua, A. V. Biochem. Pharmacol. 1979, 28, 2017. 79. (a) Langlois, N.; Favre, F.; Rojas, A. Tetrahedron Lett. 1993, 34, 4635; (b) Kaneko, T.; Wong, H.; Doyle, T. W.; Rose, W. C.; Bradner, W. T. J. Med. Chem. 1985, 28, 388. 80. (a) Langley, D. R.; Thurston, D. E. J. Org. Chem. 1987, 52, 91; (b) Courtney, S. M.; Thurston, D. E. Tetrahedron Lett. 1993, 34, 5327; (c) Bose, D. S.; Jones, G. B.; Thurston, D. E. Tetrahedron 1992, 48, 751. 81. Wilson, S. C.; Howard, P. W.; Forrow, S. M.; Hartley, J. A.; Adams, L. J.; Jekins, T. C.; Kelland, L. R.; Thurston, D. E. J. Med. Chem. 1999, 42, 4028. 82. (a) Kamal, A.; Rao, N. V. Chem. Commun. 1996, 385; (b) Kamal, A.; Howard, P. W.; Reddy, B. S. N.; Reddy, B. S. P.; Thurston, D. E. Tetrahedron 1997, 53, 3223; (c) Kraus, G. A.; Melekhov, A. Tetrahedron 1998, 54, 11749. 41 Chapter I 83. Kamal, A.; Laxman, E.; Laxman, N.; Rao, N. V. Bioorg. Med. Chem. Lett. 2000, 10, 2311. 84. (a) Berry, J. M.; Howard, P. W.; Thurston, D. E. Tetrahedron Lett. 2000, 41, 6171; (b) Kamal, A.; Reddy, G. S. K.; Raghavan, S. Bioorg. Med. Chem. Lett. 2001, 11, 387. 85. Baraldi, P. G.; Balboni, G.; Cacciari, B.; Guiotto, A.; Manfredini, S.; Romagnoli, R.; Spalluto, G.; Thurston, D. E.; Howard, P. W.; Bianchi, N.; Rutigiiano, C.; Mischiati, C. and Gambari, R. J. Med. Chem. 1999, 42, 5131. 86. Zou, Q.; Duan, W.; Simmons, D.; Shyo, Y.; Raymond, M. A.; Dorr, R. T. and Hurley, L. H. J. Am. Chem. Soc. 2001, 123, 4865. 87. Cooper, N.; Hagan, D. R.; Tiberghien, A.; Ademefun, T.; Matthews, C. S.; Howard, P. W. and Thurston, D. E. Chem. Commun. 2002, 1764. 88. Baraldi, P. G.; Balboni, G.; Cacciari, B.; Guiotto, A.; Manfredini, S.; Romagnoli, R.; Spalluto, G.; Thurston, D. E.; Howard, P. W.; Bianchi, N.; Rutigiiano, C.; Mischiati, C. and Gambari, R. J. Med. Chem. 1999, 42, 5131. 89. Zou, Q.; Duan, W.; Simmons, D.; Shyo, Y.; Raymond, M. A.; Dorr, R. T. and Hurley, L. H. J. Am. Chem. Soc. 2001, 123, 4865. 90. Reddy, B. S. P.; Damayanthi, Y.; Reddy, B. S. N.; Lown, J. W. Anti-Cancer Drug Design 2000, 15, 225. 91. Tercel, M.; Stribbling, S. M.; Shephard, H.; Siim, B. G.; Wu, K.; Pullen, S. M.; Bottin, K. J.; Wilson, W. R.; Denny, W. A. J. Med. Chem. 2003, 46, 2132. 92. Wilson, S. C.; Howard, P. W.; Thurston, D. E. Tetrahedron. Lett. 1995, 36, 6333. 93. Wang, J. J.; Shen, Y. K.; Hu, W.-P.; Hsieh, M.-C.; Lin, F.-L.; Hsu, M.-K.; Hsu, M. H. J. Med. Chem. 2006, 49, 1442. 94. Kumar, R.; Lown, J. W. Org. Biomol. Chem. 2003, 1, 3327. 95. (a) Kamal, A.; Ramulu, P.; Srinivas, O.; Ramesh, G.; Kumar, P. P. Bioorg. Med. Chem. Lett. 2004, 14, 4791. (b) Kamal, A.; Ramesh, G.; Srinivas, O.; Ramulu, P. Bioorg. Med. Chem Lett. 2004, 14, 471. (c) Kamal, A.; Ramesh, G.; Ramulu, P.; Srinivas, O.; Rehana, T.; Sheelu, G. Bioorg. Med. Chem. Lett. 2003, 13, 3451. (d) 42 Chapter I Kamal, A.; Ramu, R.; Khanna, G. B. R.; Saxena, A. K.; Shanmugavel, M.; Pandita, R. M. Bioorg. Med. Chem. Lett. 2004, 14, 4907. (e) Kamal, A.; Srinivas, O.; Ramulu, P.; Ramesh, G.; Kumar, P. P. Bioorg. Med. Chem. Lett. 2003, 13, 3577. 96. Kamal, A.; Laxman, N.; Ramesh, G.; Srinivas, O.; Ramulu, P. Bioorg. Med. Chem. Lett. 2002, 12, 1917. 97. Wei, Y.; Fan, T.; Yu, M. Acta Biochim. Biophys. Sin. 2008, 40, 278. 98. Fulda, S. Int. J. Cell Biol.;2010, doi: 10.1155/2010/370835. 99. Thompson, C. B. Science 1995, 267, 1456. 100. Jiang, X.; Wang, X. Annu. Rev. Biochem. 2004, 73, 87. 101. Hu, W.; Kavanagh, J. J. Lancet. Oncol. 2003, 4, 721. 102. Vucic, D.; Fairbrother, W. J. Clin. Cancer Res. 2007, 3, 5995. 103. Hengartner, M. O. Nature 2000, 407, 770. 104. Degterev, A.; Boyce, M.; Yuan, J. Oncogene 2003, 22, 8543. 105. Snyderman, C. H.; Head Neck 2001, 409. 106. Chipuk, J. E.; Green, D. R. Trends Cell Biol. 2008, 18, 157. 107. Thornberry, N. A. Chem. Biol. 1998, 5, R97. 108. Fulda, S.; Expert Rev. Anticancer Ther. 2007, 7, 1255. 109. Fischer, U.; Schulze-Osthoff, K. Cell Death Differ. 2005 Aug;12 Suppl 1:942-61. 110. Mollinedo, F. Gajate, C. Apoptosis 2003, 8, 413. 111. Simoni, D.; Tolomeo, M. Curr. Pharm. Des. 2001, 7, 1823. 112. Fesik, S. W. Nat. Rev. Cancer 2005, 5, 876. 113. Zhang, H. Z.; Kasibhatla, S.; Kuemmerle, J.; Kemnitzer, W.; Ollis-Mason, K.; Qiu, L.; Crogan-Grundy, C.; Tseng, B.; Drewe, J.; Cai, S. X. J. Med. Chem. 2005, 48, 5215. 43











© Copyright 2026