
Document 258075
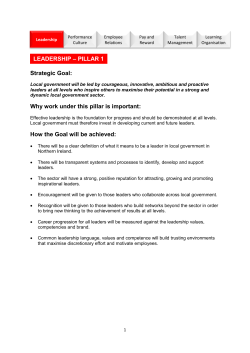
BOARD OF DIRECTORS PAPER – COVER SHEET Meeting Date: 30 July 2008 Agenda Item: 9 Paper No: E/7/08 Title: TRUST PERFORMANCE REPORT Purpose: To report on Trust performance against key indicators for the Trust in June 2008. Summary: All targets related to the Monitor compliance framework for June and quarter 1, where information is currently available, have been achieved. The Trust has already achieved the 15 week referral to treatment target for non admitted patients, nine months ahead of the required date, and the high percentage of patients treated within 18 weeks has continued to be maintained. Sustained delivery of the 4 hour maximum waiting in Accident and Emergency is a cause for concern and an action plan is in place to address the issues identified. The improvement work to ensure stroke patients are treated on a dedicated stroke ward is underway. Work is continuing with Social Services and Primary Care to improve delayed transfers of care Recommendation: For discussion and noting Prepared by: HEATHER HAUSCHILD Director of Operations Presented by: HEATHER HAUSCHILD Director of Operations This report covers: (Please tick relevant box) Assurance Framework Business Planning Healthcare Standards: Please specify which standard Local Delivery Plan 9 9 Complaints 9 Performance Management Finance 9 Strategic Development Foundation Trust Compliance Financial implications Other (Please specify) Legal implications YES / NO Indirectly YES / NO POOLE HOSPITAL NHS FOUNDATION TRUST Report to the Board of Directors – 30 July 2008 TRUST PERFORMANCE REPORT 1. INTRODUCTION 1.1 The Trust performance report for June 2008 is outlined in this report and is specifically focussed on Compliance with Monitor terms of authorisation and the contract agreed with the Bournemouth and Poole Primary Care Trust for 2008/09 as lead commissioners. 1.2 The report includes a balanced scorecard and a separate scorecard for each domain. 2. MONITOR PERFORMANCE (Appendix 1) 2.1 All Monitor access targets were achieved where information is currently available, during June and quarter 1 2008. 2.2 For Cancer Services, performance shown against the current targets relates to May 2008, the latest information available. 2.3 The Emergency Department have continued to deliver the 4 hour maximum waiting time, and the target was achieved at the end of June and for quarter 1. The position remains fragile, and a particularly difficult weekend (12 and 13 July) where 82 breaches were incurred have jeopardised achievement of the month end and looking forward to quarter 2 presents a significant risk. A comprehensive exception report and action plan has been submitted to the Director of Operations and is attached in Appendix 8. 2.4 An exception will be submitted to Monitor at the end of July in order to highlight the risk and notify the actions being undertaken to restore the position. 3. FINANCE (Appendix 2) 3.1 A separate report has been produced by the Director of Finance. 4. ACCESS AND TARGETS (Appendix 3) Transfers of Care 4.1 Delayed transfers of care reduced from 4.9% in May to 4.8% in June against a target of 3.5% and early indications for July are that delays are continuing to fall. Bed days lost for patients transferring to community hospitals were 559 for the period 2nd June to the 29th June of which 246 were for Christchurch. 4.2 Social Service delays reduced to 193 in June compared to 225 in May, of which 120 were attributable to Poole Social Services, and of these 29 were waiting a funding decision, and 25 waiting for a package of care in their own home. 1 4.3 An extensive work programme is underway with Primary Care and Social Service partners to address delayed transfers of care, in particular reviewing the process for Continuing Healthcare Assessment and ensuring every patient has a discharge plan. A more detailed report is provided by the Director of Operations on the current position by sector at Appendix 9. 4.4 The Trust has continued to maintain a high percentage of patients treated within 18 weeks and has already achieved the 15 week referral to treatment target for non admitted patients, nine months ahead of the required date, and is ahead of schedule to deliver the target for admitted patients, a significant achievement. 4.5 Negotiations are currently taking place with the Primary Care Trust on the level of funding required to achieve a 13 week wait by 31st March 2009 and an 8 week wait by March 2010. Details of costs and activity levels have been provided and the Trust is currently waiting for their response. 4.6 In April (the latest information available), the Trust did not achieve the target that 65% of patients admitted with a stroke spend 90% of their admission on a specialist stroke unit. An exception report has been submitted to the Director of Operations and a number of actions are taking place. In particular improving the information issued daily to the stroke co-ordinator to help facilitate more admissions to the stroke unit, and undertaking a review with the clinical management team of all patients with a stroke who are not admitted directly to the stroke ward to identify remedial action required. 5. CLINICAL QUALITY (Appendix 4) 5.1 The scorecard remains incomplete due either to time lags in data availability or where targets have yet to be agreed with the Primary Care Trust. Other than targets where publication of national guidance is awaited, all targets will be agreed with the Primary Care Trust before the end of Quarter 2. 6. EFFICIENCY (Appendix 5) 6.1 The four week rolling average percentage for Fractured Neck of Femurs treated within 48 hours was 48% and for all traumas was 74% as at week commencing 30th June. Case mix continues to compromise performance and six total hip replacement revisions were undertaken in June, each requiring a minimum of one theatre session to complete reducing available capacity for immediate trauma. Steps continue to be taken to implement the trauma expansion plan which will provide an additional two lists per week. These will commence in September, eventually the plan will lead to a total of six extra sessions per week. 6.2 The Trust is actively engaged in recruiting additional clinicians to improve preoperative waiting times and recruitment of additional theatre staff and an Anaesthetist is currently in progress. 6.3 A detailed and comprehensive review of trauma pathways involving both managers and clinicians is planned for October. The review will include identifying optimum pathways, comparing Trust processes with best practice elsewhere in the NHS, and will explore the idea of establishing a Trauma rehabilitation unit as an alternative to transferring patients to Christchurch Community Hospital. Theatres and Day Surgery 2 6.4 Day Theatre’s utilisation rate increased slightly to 71% although continues to remain below the target of 85%. The Service Redesign and Improvement Programme focussing on Day Theatres and utilisation rates have been rescheduled. A staff conversations event involving both clinician and managers will “kickstart” the work and will take place in September. The event will be chaired by the Director of Operations 6.5 Additional capacity is being commissioned from Community hospitals, although start dates have been deferred from those originally intended. As well as additional theatre sessions at Swanage, previously indicated, it is intended to provide an additional theatre list each week at Blandford Community Hospital for oral surgery day cases with effect from the 1st September. Start dates at Swanage have yet to be confirmed. Discussions are also taking place with Wimborne Community Hospital although there is limited additional capacity available to the Trust. 7 PATIENT EXPERIENCE (Appendix 6) 7.1 Clostridium Difficile performance is within contract levels and is notable as one of the best performances in NHS South West. 7.2 Targets remain to be agreed with the Primary Care Trust for complaints, the patient advice and liaison service, and patient surveys. 8. STAFF EXPERIENCE (Appendix 7) 8.1 A separate quarterly workforce report has been produced by the Director of Human Resources 9. CONCLUSION 9.1 While Monitor targets have been achieved for the end of Quarter 1 performance remains unsatisfactory in trauma and looking ahead to quarter 2 delivery of the 4 hour maximum waiting time target for Accident and Emergency remains fragile .A comprehensive action plan has been developed to ensure sustained achievement of the target. 9.2 Further improvement work is also required on stroke admissions to achieve the required target and this is underway 9.3 Work is progressing to reduce delayed transfers of care. The early implementation of the No Delays Scheme by August 2008 and the positive engagement from Royal Bournemouth and Christchurch hospitals Foundation Trust on orthopaedic rehabilitation is encouraging. HEATHER HAUSCHILD Director of Operations July 2008 ANDREW SPARKS Head of Performance and Redesign 3 Ratings External Assessments Current Predicted Annual Health Check Use of Resources Quality of Service Good Good Monitor Governance Risk Rating Red (Q4 2007-8) Green Reporting for Month of June 2008 Access and Targets Clinical Quality Finance Referral to Treatment (Admitted) 18 weeks Adverse Incidents - SUI Income and Expenditure Referral to Treatment (Non-Admitted) 18 weeks Adverse Incidents Income and Expenditure (Surplus / Deficit) Referral to Treatment (Non-Admitted) 15 weeks Cancer IOG compliance Cash Referral to Treatment (Admitted) 15 weeks Cancer Data Compliance Capital Cancer Access (62 days) - All Mental Health Capacity Act - May 2008 Financial Risk Rating Cancer Access (31 days) - All Mortality Elective Activity / Contract Cancer Access (31 days) - May 2008 NICE / Clinical Audit - May 2008 Non-Elective Activity / Contract Cancer Access (14 day first outpatient) - May 2008 NHSLA Standard A&E Attendances / Contract A&E Access (4 hours) Stop Smoking Services Day Cases activity / Contract A&E Access (2 hours) Maternity Standards Outpatient Activity / Contract Cardiac Access (call to needle) Breast Feeding Cardiac Access (RACPC) Smoking at Birth Patient Experience Elective Revascularisation MRSA Infections Outpatient Access (11 weeks) MRSA Root Cause Analysis Efficiency Elective Access (20 weeks) Elective Cancellations Clostridium Difficile Infections Diagnostic Access (6 weeks) - May 2008 % Trauma operated within 48 hrs Hygiene Code Diagnostic Access and Reports (4 weeks) % NOFS operated within 48 hrs Complaints Bowel Screening Patient Reported Outcome Measures Patient Advice and Liaison Service Breast Screening (Screening to normal) - May 2008 Theatre Utilisation - Main Patient Survey Breast Screening (Screening to Assessment) - May 2008 Theatre Utilisation - Day Breast Screening (Round Length) - May 2008 Day Case Rates (basket of 25) Cervical Screening Length of Stay Staff Turnover Stroke Service (Time on Unit) - April 2008 Pre-operative Bed Days Unplanned Vacancies Stroke Service (TIA treatment within 24 hrs) Excess Bed Days Absence Delayed Transfers of Care Bed Occupancy Staff Survey Staff Experience Agency Key Target not achieved action required Area Of Concern On Target New target under development or data not available for current reporting month 4 MONITOR COMPLIANCE - APPENDIX 1 Reporting for Month of June 2008 Standard Description Clostridium Difficile Contractual Target is 4.0 cases per 1,000 ordinary admissions. This equates to 176 cases per annum based on 44,000 ordinary admissions undertaken in the last financial year. Clostridium Difficile Contractual Target is 4.0 cases per 1,000 ordinary admissions. This equates to 176 cases per annum based on 44,000 ordinary admissions undertaken in the last financial year. MRSA MRSA PHFT acquired– (20 cases will be considered a breach) Target Qtr 1 - 44 Qtr 2 - 44 Qtr 3 - 44 Qtr 4 - 44 cases cases cases cases Source Weighting Quarter Monitor 1 Qtr Qtr Qtr Qtr 1234- 6 cases 6 cases 4 cases 4 cases Year to date cumulative TBC Referral to Treatment Non-admitted patients: maximum time of 18 weeks from point of referral to treatment Quarter Monitor Monitor 1 Monitor 1 Monitor 1 95% To be achieved from end December 2008 and monitored monthly thereafter Monitor 1 Maximum waiting time of four hours in A&E from arrival to admission, transfer or discharge Maximum waiting time of 31 days from diagnosis to treat to start of treatment 98% Quarter Monitor 0.5 98% Quarter (Target applies up to December 2008) Monitor 0.5 Cancer Access Maximum waiting time of two weeks from urgent GP referral to first outpatient appointment for all urgent suspect cancer referrals 98% Quarter (Target applies up to December 2008) Monitor 0.5 Cardiac Access People suffering heart attack to receive thrombolysis within 60 minutes of call (where this is the preferred local treatment for heart attack) 68% Month Monitor 0.5 Hygiene Code Compliance with Hygiene Code Compliance Annual Monitor Ad Hoc Monitor Quarter Monitor Cancer Access Each National Core Standard Monitor Governance Monitor Service performance score Rating Trust performance report for Trust Board 30th July 2008 May-08 Jun-08 Qtr 1 End of Year Forecast Comment 15 3 3 21 15 18 21 21 1 0 0 1 1 1 1 1 91.8% 94.9% 94.5% 93.7% 95.3% 96.6% 96.9% 96.3% 98.2% 98.5% 98.0% 98.2% 100% 100% 100% 1 month data lag 100% 100% 100% 1 month data lag 100% 100% 0 0 1 To be achieved from end December 2008 and monitored quarterly thereafter To be achieved from end December 2008 and monitored quarterly thereafter To be achieved from end December 2008 and monitored monthly thereafter A&E Access Apr-08 Year to date cumulative MRSA PHFT acquired– (20 cases will be considered a breach) Maximum waiting time of 31 days from Cancer Access decision to treat to start of treatment extended to cover all cancer Maximum waiting time of 62 days from all Cancer Access referrals to treatment Referral to Treatment Admitted patients: maximum time of 18 weeks from point of referral to treatment MRSA Monitoring period TBC 90% Less than 1.0 5 100% 100% 0.4 0 FINANCE - APPENDIX 2 Reporting for Month of June 2008 Standard Description Target Monitoring period Source Income and Expenditure (EBITDA) Earnings before interest, taxes, depreciation and amortization (EBITDA) (£'s , 000's) 13600 Month PHFT Income and Expenditure Surplus / (Deficit) (£'s, 000's) 3371 Month PHFT Cash £'s , 000's 13470 Month PHFT Capital £'s , 000's 4450 Month PHFT 4 Month PHFT Financial Risk Rating Elective Activity / Contract Elective activity verses contracted levels 100% Month PHFT Non-Elective Activity / Contract Non-Elective activity verses contracted levels 100% Month PHFT A&E Attendances / Contract A&E Attendances verses contracted levels 100% Month PHFT Day Cases activity / Contract Day Case activity verses contracted levels 100% Month PHFT Outpatient Activity / Contract Outpatient activity verses contracted levels 100% Month PHFT Trust performance report for Trust Board 30th July 2008 6 Weighting Apr-08 May-08 Jun-08 Qtr 1 End of Year Forecast 1,215 1,448 1281 3,945 13,600 360 591 431 1381 3371 10,200 11,484 11936 11,936 14,471 262 258 432 952 5,650 4 4 4 4 4 102.1% 95.0% 91.0% 96.2% 96.0% 109.2% 115.0% 107.3% 108.7% 109.0% 98.3% 104.4% 104.6% 102.4% 102.0% 120.1% 110.0% 118.6% 118.0% 118.0% 105.1% 104.3% 105.3% 104.9% 105.0% Comment ACCESS AND TARGETS - APPENDIX 3 Reporting for Month of June 2008 Standard Description Target Monitoring period Source Weighting Referral to Treatment Admitted patients: maximum time of 18 weeks from point of referral to treatment Referral to Treatment Non-admitted patients: maximum time of 18 weeks from point of referral to treatment 90% Month Monitor / PCT 1 Monitor / PCT 1 Referral to Treatment Admitted patients: maximum time of 15 weeks from point of referral to treatment Referral to Treatment Non-admitted patients: maximum time of 15 weeks from point of referral to treatment Maximum waiting time of 31 days Cancer Access from decision to treat to start of treatment extended to cover all cancer 90% To be achieved by March 2009 PCT 1 To be achieved by March 2009 PCT TBD To be achieved from end December 2008 and monitored quarterly thereafter Monitor / PCT 1 95% 95% Month 1 Cancer Access Maximum waiting time of 62 days from all referrals to treatment TBD To be achieved from end December 2008 and monitored quarterly thereafter Monitor / PCT 1 Cancer Access Maximum waiting time of 31 days from diagnosis to treat to start of treatment Maximum waiting time of two weeks from urgent GP referral to first outpatient appointment for all urgent suspect cancer referrals 98% Quarter (Target applies up to December 2008) Monitor / PCT 0.5 Quarter (Target applies up to December 2008) Monitor / PCT 0.5 Cancer Access A&E Access A&E Access Cardiac Access Cardiac Access Elective Revascularisation 100% Maximum waiting time of four hours in A&E from arrival to admission, transfer or discharge 98% Stretch target 50% of minor and intermediate attenders are seen within 2 hours People suffering heart attack to receive thrombolysis within 60 minutes of call (where this is the preferred local treatment for heart attack) 50% Maximum wait of 2 weeks for an appointment for the Rapid Access Chest Pain Clinic Maximum wait of 11 weeks 68% 0 greater than 14 days 0 Month Monitor / PCT Month Apr-08 May-08 Jun-08 Qtr 1 End of Year forecast or Forecast actual Comment 91.8% 94.9% 94.5% 93.7% 95.3% 96.6% 96.9% 96.3% 83% (79%) 87.4% (80%) 86.22% (81%) 85.5% 92.1% (90%) 93.4% (90%) 95.45% (90%) 93.7% 100 100 Not available yet 100 1 month Data Lag 100 100 Not available yet 100 1 month Data Lag 98.2 98.5 98.0 98.2 60 61 58 60 100 100 100 100 0 1 0 1 0 0 0 0 Performance against trajectory in brackets Performance against trajectory in brackets 0.5 PCT Month Monitor Month 0.5 PCT Month PCT Trust performance report for Trust Board 30th July 2008 7 Risk ACCESS AND TARGETS - APPENDIX 3 Reporting for Month of June 2008 Standard Description Outpatient Access No outpatient waits more than 11 weeks for a new appointment No elective waits more than 20 weeks inpatient appointment A maximum wait of 6 weeks for diagnostic investigations By 31 March 2009 all non-radiology diagnostics including reports are provided within 4 weeks and radiology diagnostics within 3 weeks, with 90% reported within 3 working days Elective Access Diagnostic Access Diagnostic Access and Reports Bowel Screening Proportion of men and women aged 60-74 taking part in bowel screening programme Target Monitoring period Source 0 Month PCT 0 Month PCT 6 weeks Month (Diagnostic Return) PCT 4 weeks Month PCT Data system to be developed for end Q2 100% of 60-74 year old eligible adults are offered screening for bowel cancer in the previous two years Month PCT Target deferred by PCT until screening programme commences 90% Month PCT Screening to normal results within 14 Breast Screening (screening to normal) days Breast Screening (screening to assessment) Breast Screening (round length) Cervical Screening Stroke Service Screening to assessment within 21 days 90% National Minimum Standard is 90% of eligible woman screened within 36 months Meet the cancer plan target of a 2 week turnaround for reporting cervical screening 90% Patients are treated on dedicated stroke unit Stroke Service Time to treatment for high risk TIA Delayed Transfers of Care Delayed transfers of care will be maintained at a minimal level subject to the development and implementation of a jointly agreed action plan executed by the PCT Month Weighting Apr-08 May-08 Jun-08 Qtr 1 End of Year forecast or Forecast actual 0 0 0 0 0 0 0 0 0 0 0 0 1 month data lag 91% 92% 90% 90% 90% 90% 98.4% 99.4% 90% PCT Month Comment 1 month data lag PCT 1 month data lag 100% Month PCT Target deferred by PCT until screening programme commences 65% of people admitted with a stroke patients spend 90% of their admission on a specialist acute stroke unit Month PCT 2 month data lag 25% treated within 24 hours Month PCT Q1 - 3.5% Q2 - 3.5% Q3 - 3.5% Q4 - 2% Month PCT 43% 34.2% 28.5% 28.6% 30.4% 6.2% 4.9% 4.8% 5.3% 1 month data lag Risk Trust performance report for Trust Board 30th July 2008 8 CLINICAL QUALITY - APPENDIX 4 Reporting for Month of June 2008 Standard Description Target Monitoring period Source Adverse Incidents Adverse Incidents The Provider will have a robust process for reporting adverse incidents Number of Adverse Incident Reports 100% SUI reports to PCT within 60 days TBD Quarter PCT Month PHFT Cancer IOG compliance Providers will be compliant with IOGs within national timescales 100% Quarter PCT Cancer Data Compliance Providers will ensure that they meet new national recording standards as per national Cancer Strategy 100% Quarter PCT Action plan to be reviewed after new guidance released in 2008 and shared with PCT on a quarterly basis Quarter PCT Mental Health Capacity Act Providers will meet the requirements of the Mental Health Capacity Act 2005 and develop a joint action plan across the local health community in line with new national guidance Weighting Apr-08 May-08 Jun-08 929 840 962 Qtr 1 End of Year Forecast Comment 2 month lag Data System to be developed by end of Q2 Data System to be developed by end of Q2 Mortality The benchmark is the average mortality rate for England and is standardised for diagnosis/procedure group, subgroup, admission type, age, sex, deprivation, month of admission (for some respiratory diagnoses) and financial year % Deaths against % Expected Deaths (Dr Foster) Month PHFT NICE / Clinical Audit The Provider will have robust processes for: Clinical audit NICE Technology Appraisals NICE Guidance and Interventional Procedures (as appropriate) Implementation of agreed actions following clinical audits Quarter PCT NHSLA Standard Achievement of NHSLA risk management standards Level 2 achievement Q4 Quarter PCT Stop Smoking Services Providers will ensure smoking status is recorded for all outpatients and inpatients and there is a record of signposting to ‘Quitter’ programmes The Provider will comply with all Health Care Commission maternity standards and vital signs Breast Feeding Initiation rates within 48 hours of birth (This figure is from questionnaires returned based on 90% completion) Percentage of women still smoking at birth TBD Annual PCT Audit to be planned As HCC standards and Vital Signs targets 68% Quarter PCT 3 month data lag Quarter PHFT Maternity Standards Breast Feeding Smoking at Birth Quarter Maximum 15% (stretch 12% for Bournemouth LAA) Trust performance report for Trust Board 30th July 2008 9 3 month data lag 74.7% 71.7% 71.4% 72.6% 7.8% 9.4% 9..3% 8.6% PCT EFFICIENCY - APPENDIX 5 Reporting for Month of June 2008 Standard Description Target Monitoring period Source Elective Cancellations 100% of patients who have operations cancelled for non-clinical reasons to be offered another binding date within 28 days, or the patient's treatment to be funded at the time and hospital of the patient's choice 100% Month PCT % Trauma operated within 48 hrs Trauma inpatients who are medically fit for surgery receive treatment within 48 hours 95% Month PHFT % NOFS operated within 48 hrs 95% Month PCT Patient Reported Outcome Measures Hip fractures who are medically fit for surgery receive treatment within 48 hours Providers will implement patient reported outcome measures, As a minimum this will cover nationally agreed areas hip and knee replacements, varicose vein ligations and inguinal hernia repair. TBD TBD PCT Theatre Utilisation - Main Needle to skin to end of operating 85% Month PHFT Theatre Utilisation - Day Needle to skin to end of operating 85% Month PHFT Day Case Rates (basket of 25) Day case (Healthcare Commission Basket of 25) percentage of elective discharges 75% Month (Dr. Foster) PHFT Length of Stay (Trust) The number of days between the date of admission and the date of discharge in a spell 3.5 days Month PHFT Pre-operative Bed Days The number of days between the date of admission and the date of operation The number of days above the long trimpoint TBD PHFT 3 month data lag PHFT 3 month data lag Bed Occupancy as per Thursday midnight snapshot 95% Month (Dr. Foster) Month (Dr. Foster) Month Excess Bed Days Bed Occupancy TBD Weighting Apr-08 May-08 Jun-08 Qtr 1 100% 100% 100% 100% 86% 84% 74% 81% Risk 75% 79% 48% 67% Risk Data System to be developed in line with national programme 89% 88% 91% 89% 75% 70% 71% 72% 2.9 2.7 2.8 2.8 PHFT 94.3 Trust performance report for Trust Board 30th July 2008 10 94.2 93.4 94.0 End of Year Forecast Comment Risk 3 month data lag PATIENT EXPERIENCE - APPENDIX 6 Reporting for Month of June 2008 Standard Description MRSA Infections MRSA PHFT acquired– (20 cases will be considered a breach of Contract). The stretch target is 15. MRSA Infections MRSA Root Cause Analysis MRSA PHFT acquired– (20 cases will be considered a breach of Contract). The stretch target is 15. 100% of diagnosed MRSA bactaraemias will have a root cause analysis within 28 days and this will be shared with the PCT Clostridium Difficile The Contractual Target is 4.0 cases per 1,000 ordinary admissions. This equates to 176 cases per annum Infections based on 44,000 ordinary admissions undertaken in the last financial year. The stretch target is yet to be confirmed with the PCT. Clostridium Difficile The Contractual Target is 4.0 cases per 1,000 ordinary admissions. This equates to 176 cases per annum Infections based on 44,000 ordinary admissions undertaken in the last financial year. The stretch target is yet to be confirmed with the PCT. Target Monitoring period Source Weighting Qtr 1 - 4 cases Qtr 2 - 4 cases Qtr 3 - 4 cases Qtr 4 - 3 cases Quarter Monitor / PCT 1 Year to date cumulative 100% Qtr 1 - 44 Qtr 2 - 44 Qtr 3 - 44 Qtr 4 - 44 cases cases cases cases Month Quarter Monitor / PCT Jun-08 Qtr 1 1 0 0 1 1 1 1 1 100 100 100 1 15 3 3 21 15 18 21 21 23 29 30 93 88 119 Year to date cumulative Compliance with Hygiene Code Compliance Annual Monitor Complaints Number of complaints received TBD Month PHFT Patient Survey May-08 The Provider will have in place a Patient Advice and Liaison Service (PALS) function that is easily accessible. The measure shows the number of PALs enquiries per month. The Provider will supply to the PCT a quarterly PALS report by trend by directorate. TBD Patient Satisfaction / feedback measures TBD End of Year Forecast Comment One April Bacteraemia was removed from the contract figures as it was community acquired. PCT Hygiene Code Patient Advice and Liaison Service Apr-08 Quarter Quarter Trust performance report for Trust Board 30th July 2008 11 PCT PHFT The target will change with over or under contract numbers. The current position has been clarified with the PCT by the Director of Finance. STAFF EXPERIENCE - APPENDIX 7 Reporting for Month of June 2008 Standard Description Staff Turnover Overall avoidable staff turnover under 11% and Auxiliaries/ HCAs under 13.5%. (To be reviewed in light of 2007/08 outturn) Unplanned Vacancies Target Monitoring period Source 11% Month Unplanned vacancies under 5%. 5% Absence Sickness absence rate below 4%. (By 31st March 2009). Monthly trajectories to achieve a 4% absence rate by 31st March 2009 based on 2007/8 cumulative absences are shown in brackets. First figure is rate for the month, second is cumulative rate for year to date, bracketed figure is trajectory based on 2007-08 results. 4% Staff Survey Staff Satisfaction / feedback measures Agency % Temporary staff used against % of total employed staff Weighting Apr-08 May-08 PCT 0.69 % (see comment) 0.74% (see comment) Month PCT 3.76% 3.96% 4.79% Month PHFT 4.08% 4.08% (4.38%) 3.88% 3.98% (4.11%) TBD Quarter PHFT TBD Month 5.62% 5.87% PCT Trust performance report for Trust Board 30th July 2008 12 Jun-08 Qtr 1 End of Year Comment Forecast 9.41% The cumulative Q1 turnover figure of 2.4% is consistent with achieving the target of <11%. 4.17% average < 5% Vacancies being actively recruited to at the end of June 2008. The quarter 1 figure is an average for the three months. 3.85% 3.93% (3.91%) 4.00% (3.91%) <4% The rate recorded for June 2007 (3.48%) was particularly good and set the cumulative trajectory for Q1 at a low level. This has been exceeded by this June's rate of 3.85%. However, with the summer months and the continued absence management programme, lower sickness levels can be anticipated making this rate of trajectory compatible with a year end outturn of below 4% 5.72% 5.74% 0.97% (see 2.40% (see comment) comment) The Q1 figure is an average over the three months. Appendix 8 Directorate of Medicine FOUR HOUR WAITING TIME TARGET – EMERGENCY DEPARTMENT 1 INTRODUCTION 1.1 Since April 2008 the Emergency Department’s performance against the 4-hour wait has been variable with more recent performance showing a steady decline, indicating that immediate attention is required. 1.2 This report provides a briefing for the Board of Directors on the current position and actions being taken to restore performance to the level expected of the Emergency Department. 1.3 Chart 1 below shows the Emergency Department performance against the 4-hour waiting time target. Chart 1 Emergency Department Performance 100.0 99.5 99.0 98.5 98.0 97.5 97.0 96.5 96.0 95.5 95.0 April May June % For Month 08/09 98.2 98.5 98.0 July Aug Sept Oct Nov Dec Jan Feb March % For Month 07/08 97.0 99.1 99.3 % Cumulative for Quarter 08/09 98.2 98.4 98.2 98.6 98.3 97.8 98.0 98.9 98.6 98.3 98.4 98.4 % Cumulative for Quarter 07/08 97.3 98.2 Target 98.0 98.0 98.5 98.6 98.5 98.2 98.0 98.5 98.5 98.1 98.3 98.3 98.0 98.0 98.0 98.0 98.0 98.0 98.0 98.0 98.0 98.0 2 CURRENT POSITION 2.1 The target of 98% of patients being discharged, transferred or admitted within 4 hours has been achieved each month since September 2007. However 82 patients breached the 4-hour target during the week ending 13th July 2008 which will prevent the trust meeting the target for July and, potentially, Quarter 2 2008/09. 2.2 A number of factors have been identified as adversely impacting the department’s performance against the four-hour waiting time target including: • Junior doctors are more reliant on senior supervision than ever before; • Inability to recruit to middle grade posts has meant the department has been short of 3 registrars since May 2008; 13 • We know that the department will experience two peaks of activity, or patients attending, each day. The first occurs at approximately 0900 Monday – Friday, and 1220 Saturday and Sunday. The second peak in patient presentation occurs around 1830 Monday – Friday; and 1700 Saturday and Sunday. Over the last 8 weeks the second peak that has occurred has gone on later, with up to 33% of daily attendances presenting between 1800 and 2200. This is at a time when the department is most vulnerable due to a decline in the number of senior medical decision makers supervising the Department. Unless this backlog can be cleared within 2 hours, then breaches will start to occur. • Considering the pattern of presentation to the department, consultant cover to the department needs to extend beyond 1800. This is currently difficult to achieve given that there are only three consultants; • More generally, medical / nursing capacity is not currently effectively aligned to demand; • Some of the processes supporting patient throughout within ED need to be reviewed as working practises and staffing levels have changed; • Nurse practitioners have left the department creating gaps in the rota; • The physical environment is inadequate during busy periods; specifically resuscitation rooms and paediatric areas; • Co-ordination of patients attending department is not robust enough during busy periods. 2.3 Much work has already been undertaken to strengthen the department’s position against the target; including, capacity and demand modelling, including reviewing rotas; developing nursing staff to assist medical staff; process mapping event to define and outline a more efficient process for managing patients attending as ‘minors,’ the acquisition of a new Emergency Department system, Symphony. 2.4 However it has been recognised that the recent performance demands that immediate and additional action be taken to ensure that, with the exception of clinical cases, no patient waits in excess of four – hours for discharge, admittance, or transfer. 2.5 A detailed action plan is provided as Appendix 8a that highlights the work already being undertaken, as well as the action taken immediately to strengthen the current position. 2.6 The Board of Directors are asked to consider the details of this exception report to assure itself that robust processes are in place to address the current difficulties. HEATHER HAUSCHILD Director of Operations July 2008 MARK MAJOR Business Manager, MCCG 14 Annexe A Exception Report - Four Hour Waiting Time Target – Emergency Department Medical Staffing Update • Middle grade starting 9th August 2008 providing support for 3 weeks. • SHO starting 18th August 2008 for 3 weeks and will provide additional cover to current establishment in the department. • The department has recruited 11 SHO’s to start 6th August with the 12th taking up post on the 25th August. The department is trying to identify a doctor who could work the rota until the 25th August. • Several additional doctors with ED experience have confirmed that they are able to provide additional sessions in August. • Agency middle grade starting 28th July – 10th August & 17th August – 25th August. • A clinical fellow has been identified that could work in the department. The doctor is scheduled to visit the department within the next few days. • A locum consultant has been arranged from 1st September 2008. An initial 3 month contract has been offered. • A second locum consultant is able to work for a three month period starting in August. This is to be discussed with Mr Reichl to ensure maximum return on the investment. Actions Short Term – 0 – 28 days Medium Term 1 – 6 months Long Term >6 months Status Action Complete Partially Complete Not Yet Complete G A R 15 Immediate / Short Term 1. Issue Identified Remedial Action Lead Due to the number of breaches that occurred 11th – 14th July, the position for the quarter is fragile. Doctor cover to be arranged for vulnerable times or shifts where there are gaps. DC By When Immediate Progress / Impact • • The principle area of concern is medical staffing MM Immediate Arrange for additional consultant sessions. GC Notify RBCH consultants that available sessions are available at Poole. GP’s working the front of house. Immediate Additional doctor arranged for Sat / Sun (19th & 20th) 1100 – 2300 Additional doctor arranged for Wed 16th Jul Gary Cumberbatch / Simon Bell to provide 3 hours consultant cover on Sat 19th Jul and Sun 20th Jul. SF Consultant at RBCH expressed an interest in additional sessions. GP’s agreed to work in minors out of hours. Fee agreed. Steve Frost is targeting several GP’s, including One GP already working as clinical assistant in ED will confirm availability once back from annual leave, w/c 28th July. 16 Progress Amber 2. The co-ordination of the department by the Nurse Co-ordinator is compromised when department is busy. Introduce a ‘Progress Chaser,’ role providing monitoring support to the nurse coordinator. SF Immediate Progress Chaser to escalate where patients reach 2 hours and no treatment plan is in place. Progress Chaser to commence Wed 16th July. Initially focussing on 1400 – 2200, the most vulnerable shift. Progress chaser will escalate those patients without treatment plan after 2 hours. Additional receptionists to support the back and the progress chaser. MM Additional receptionists being arranged for Sun & Mon to assist coordinator. 3. Breach / tracking board is slow to re-fresh and frequently crashes making patient tracking difficult. IT to investigate. MM 24th July 4. Insufficient numbers of nurse practitioners to provide an extended service to the front needed to support medical staff. Nurse practitioners from Out of Hours to undertake extra shifts in ED. MM 1st August IT to lock down the PC driving this hardware to prevent people from using it and altering the set up. Amber All NP’s offered double time to provide additional cover to ED. To date noone has come forward. Red Efforts to encourage additional NP’s will continue 17 Green 5. Department short of middle grade support as unable to recruit suitable candidates into vacancies. Medical staffing to continue to provide department with CV’s of suitable candidates. Med Staffing 1st August The remainder of July is now up to establishment. Green Several SHO’s / Middle grades with ED experience have confirmed availability for August. Medical staffing / department continue to cover gaps in rotas. Two middle grades arranged to support the department from 28th July 2008 through to the end of August. Registrar recruited with start date 29th July. 6. Non – clinically urgent children breaching 4 hour waiting target due to lack of medical staffing, a busy department and clinically urgent attendances. Agree and implement a process with the Paediatric department for getting children straight to the children’s ward throughout July whilst medical staffing an issue. MM 15th July 15th Aug 18 Process implemented Tuesday 15th July 2008 until end of July, where a certain cohort of medical children can be fast tracked to a ward and treated / discharged. Several patients have avoided delay as a result of this process. Full analysis will be undertaken at the beginning of Aug. Green 7. Insufficient details regarding breaches for analysis and learining. Co-ordinator to complete breach pro-forma for every breach. MM 1st June Pro-formas being completed for each patient breach allowing for more effective breach analysis. Green 8. Medical staff not recording time correctly Robust breach validation MM 1st June Time stamp provided to record time of discharge. Green Policy in place states that where there is evidence that demonstrate a time recorded is incorrect a change can be signed off by the ADO. 9. Disparity in clinical practice between nurse practitioners. Clarify expectations of role and communicate to all nurse practitioners. Minor head injuries are not being dealt with by all NP’s. Some are happy to see and treat otherwise require supervision. Consultants to provide additional training. Validation of all breaches takes place each week, each month and quarterly. SF 1st August Clear expectations of nurse practitioner role conveyed to those in post. Identify any training issues and resolve. Future NP’s will be recruited on a band 6 and will be promoted to band 7 having demonstrated clinical competence & confidence to a required level. 2 additional NP’s being recruited Oct 2008. 19 Green Medium Term Issue Identified Remedial Action Lead By When 10. Nurses are leaving the department to replace and repair plasters for patients residing elsewhere within the trust; for example, ortho & trauma wards. Quantify issue and feedback to Trauma Department. Data could underpin business case for extending plaster service. HR 1st Sept AIRs forms to be completed where nurses have to leave department. Numbers, times, details etc to be feedback to orthopaedics. Amber 11. Lodgers are spending > 4 hours in ED, slowing patient through put and preventing other patients from being admitted often resulting in 4 hour breaches. Quantify issue MM 15th Aug Report detailing all lodgers, time of attendance, waiting time has been generated for a one year period. Amber Performanc e Team 28th Sep Orthopaedic process redesign work to be undertaken in Sept 2008. Lodgers will be flagged as an issue impacting on four hour performance. 1st Jul Where an assessment has determined that a patient will be admitted to hospital, the patient is to go straight to the ward and not wait for an ortho SHO to assess. Data to underpin re-design. Heather Ramsden / Mandy Khan 20 Impact / Progress 12. 13. Nurses unable to suture causing delays to patients. Process for managing minors needs revising Provide suturing courses. Process mapping event to identify most effective way of managing minors Heather Ramsden / Mandy Khan 28th Sep Mike Reichl 1st Sept Two suturing courses already run. Red Skill assessment currently being undertaken for all nursing staff. Individuals unable to suture will attend an additional course. Two processes outlined and presented to group. Amber Group agreed, subject to numbers, to trial ‘see & treat.’ Meeting with Mike Reichl and Steve Frost to take place 22nd July 2008. 14. When department busy the co-ordinator is drawn into clinical practise thus not being able to effectively monitor department. Ring fence an individual from clinical practise to focus solely on co-ordinating patients through the department. Role could be clinical or non – clinical. 21 Steve Frost 1st Aug Progress chaser role commenced 16th July 2008 with senior HCA. 4 HCA’s have now been recruited to this role allowing a rota to be put into place for August 2008 Amber 15. Nursing Staff within Emergency Services are finding it increasingly difficult to cover shifts and staff shortages. Review method of payment to individuals working under a bank arrangement. HR 1st Jul Increase recruitment of bank nurses with experience of ED. Staff providing cover under a bank arrangement that have a permanent contract with the trust, will now be paid weekly. Green Dept to continue to arrange for rotation / Ansty nurses in addition to Thornberry / agency, nurses to provide cover to ED. 16. The department is vulnerable between 1800 and 2100 to activity peaks. Surges in attendances between these times leads to back-log and risks breaches. The number of senior decision (NP’s and Medical staff) makers within the department reduces during this period. Increase medical staffing and nurse practitioners during vulnerable times to reflect work loads. Mike Reichl / Gill Christian Steve Frost 22 tbc 1st Oct 4th and 5th consultant jobs agreed. Initial round of interviews abandoned due to a lack of applicant. Post due to be advertised in Nov with interviews scheduled for Jan / Feb 2009. Increasing Nurse Practitioner establishment in Oct by 2 and then an additional 2 NP’s every 6 months. Additional NP’s will enable the current service to be extended, more appropriately aligning staffing to demand. Amber 1st Aug Existing NP rota being reviewed and revised, where possible, to provide more ‘shop floor,’ cover between 1800 – 2200. 1st Sept Locum consultant takes up post from 1st Sept 2008. 1st Dec Workforce planning underway. Additional medical staffing arranged on an ad-hoc basis where cover required. Consultants to provide additional sessions at weekend when available and at agreed times. 17. Strengthen current process of escalation Implement reviewed escalation policy. Mark Major 1st Oct Inaugural meeting took place. Follow up meeting arranged and foundations of a policy drafted. 1st draft sent for consultation. 23 Amber 18. Patients waiting in CDU overnight for transport as ambulance service unable to provide transport service after 2000. Establish use of private ambulances. Steve Frost / Nick Caplin Dec 2008 Process designed and disseminated to nursing staff and reception staff for arranging for transport depending on their needs. Separate budget set up for the use of private taxis for patients who were clinically well. Spec document drafted to underpin a tender for a private ambulance firm. This will take place within 8 weeks. As an interim measure HUXSTEP will be used on an ad-hoc basis until a more formal arrangement is made. 19. Ward transfers delayed as ED staff cannot contact co-ordinators on wards. Nursing staff leave department to take patients to wards thus reducing nursing presence in ED. Patient transfer policy to be reiterated to all wards. Heather Hauschild Steve Frost tbc August Ansty ward and ED will liaise directly to arrange for patient admissions. Ward co-ordinators / board holders will wear earpieces so as to remain contactable at all times. 24 Amber 20. Issue Identified Remedial Action Lead By When Skill mix does not always reflect the demands of the department. Full review of nursing staff to take place to determine the number of nurses required to meet demand for all shifts. Steve Frost 15th July Review of nursing staff and skill mix required to run the current service through to 2010, has been carried out. This will be the blue print for moving towards ‘see & treat,’ model of managing minors. Green Mark Major 1st Nov ED environment reviewed. Amber Skill mix also to be defined for each shift. 21. The current method of monitoring / tracking patients through the department is not robust enough or accurate. It crashes and reports patients who have left the department. Until the new ED system is in place, this will continue to be an issue and a risk to the department performing against access targets such as the 4 hour wait. New ED system will track patient’s real time, flagging those nearing a deadline. It will allow for individual patient escalation to take place; for example, no management plan in place after 2 hours will be escalated to senior doctor. The dept, including CDU and the waiting area, can be monitored real time & remotely from any PC. Ansty and CMT will be able to pro-actively monitor patients with MAU identifying and transferring appropriate patients from ED. 25 Impact / Progress Project initiated. Project group assembled. Software delivered. Config process underway Training schedule being drafted. Long Term Issue Identified 22. Remedial Action Lead Nursing staff difficult to recruit. HR By When 31st Dec Impact / Progress Recruitment fair Red Review of recruitment process taking place 23. Current footprint does not support patient throughput. Capital development – Phase 1 Mike Reichl Dec 2008 Phase 1 of the capital redevelopment includes expanding CDI within current footprint 2011 Phase 2 will create 2 more resus rooms Red CDU inadequate Resus area inadequate Capital development – Phase 2 24. CDU cannot accommodate certain patients when no trained nurse in the facility. Review of CDU - function - environment - capacity Mike Reichl 31st Nov 25. Psychiatric Assessment team do not attend the department with the urgency needed to avoid breaching the four – hour waiting time target. If CDU is full patients requiring assessment will breach Time from referral to attendance by psychiatric assessment unit being audited. Mark Major 1st Aug On-site parking provided for Psychiatric team tbc PCT written proposal document outlining an Acute Psychiatric Assessment service for PCT 26 Red Amber acute wards. This will replace existing service. Document out for consultation and comment. 26. NICE guidelines regarding head injuries has resulted in more patients requiring CT scan. As patients are accompanied by ED nurses, additional demands are placed on nurses remaining in dept. CT scanner adjacent to Emergency Department. Capital development plans submitted to address this. Mike Reichl 2013 Red 27. Treatment nurse has to leave department to fetch medication for patients. • • • Additional dedicated porter Pharmacy in department Vending Machine Heathe r Ramsd en / Mandy Khan Q1 09/10 Red 28. Patients are being referred back to ED doctors for confirmation of no fractures present on x-rays. This is delaying • Business case for the installation of an x-ray workstation in ED to be submitted as part of business planning process. Mark Major • Implement radiographer led discharge. 2009 Trial demonstrated value of radiographer led discharge. Key HH MM Heather Hauschild Mark Major GC SF Gary Cumberbatch Steve Frost HR MK Heather Ramsden Mandy Khan 27 MR GC Mike Reichl Gill Christian NC DC Nick Caplan Debbie Cook Red Appendix 9 POOLE HOSPITAL NHS FOUNDATION TRUST DELAYED TRANSFERS OF CARE 1. INTRODUCTION 1.1 Delayed transfers of care have been problematic for the Trust for some time despite a number of measures having been undertaken by Health and Social Care partners from 2004/5 onwards. 1.2 The Trust position for 2007/08 was 4.76%, with the target of a maximum of 3.5% only having been achieved in Quarter 3. 1.3 The two main causes of delay remain waits for transfer to community hospitals (70% of all delays) and waits for social care intervention and placement. 1.4 Specific problem areas are high numbers of delays waiting for orthopaedic rehabilitation for Christchurch Hospital which is part of the Royal Bournemouth Hospitals NHS Foundation Trust and waits for assessment and placement by Poole Social Services. 1.5 The Board of Directors have been briefed regularly on the position and actions being taken to address delays generally and these two areas specifically. 1.6 For 2008/9 the position is as follows; 2008/9 April May June % 6.2% 4.9% 4.8% 2. PROPOSED ACTION 2.1 No Delays 2.1.1 The Bournemouth and Poole Primary Care Trust have worked actively with Poole Hospital NHS Foundation Trust and with Social Care partners to develop a robust action plan to address the issues identified. 2.1.2 In 2007/8 £680,000 was allocated for the development of the Poole Intermediate Care Scheme (PICS) which integrates health and social care services to avoid admissions wherever possible and to work with in the Trust on early supported discharge. Two geriatricians employed by Poole Hospital work with this team rotating into the community. The service commenced in December 2007 and has developed the scope and range of interventions in subsequent months. 2.1.3 PICS will be supplemented by a more comprehensive ‘No Delays’ scheme which includes the purchase by the Primary Care Trust of a number of nursing and rest home beds. This will be in place by 3 August 2008. initially £1 million was allocated to the ‘No Delays’ scheme, however, following our representation a further £500,000 was allocated to support placement for the elderly mentally ill, for whom longer term care is very problematic. Five orthopaedic rehabilitation beds have also been purchased as part of the scheme. 28 2.2 Orthopaedic Rehabilitation 2.2.1 Meetings have taken place with senior managers of the Royal Bournemouth Foundations Trust Hospitals and an action plan has been agreed as follows; • Patients to be identified strictly according to the protocol to ensure appropriateness of referral for rehabilitation consistently. • Intermediate Care Teams to review patients jointly with our therapists on a daily basis for three months to establish a common assessment and scope for diversion from inpatient care. • Royal Bournemouth Foundation Trust Hospitals are currently reviewing capacity and the feasibility of increasing inpatient facilities. • Poole Hospital has notified the Primary Care Trust and Royal Bournemouth that if delays for orthopaedic rehabilitation continue at present levels (typically 10-15 patients delayed at any one time) despite actions agreed, we will provide a local facility for rehabilitation. The feasibility and costings are currently being undertaken. However, it is recognised that patients who need inpatient rehabilitation are best served closer to their homes. 2.3 Poole Social Services 2.3.1 Delays for Poole Social Services have been running at around 180 bed days per month, double the target set with them last November. 75% of these delays were attributable to waits for elderly mentally ill patients (EMI), both for assessment and placement. Patients with mental illness have traditionally been referred to the community mental health team and working practices have not mirrored that of the hospital social work team. 2.3.2 As part of the pooled budget arrangements agreed 2008/9 an allocation has been set aside for social work assistants specifically to support EMI patients. It was also agreed that the community social work teams would be managed in conjunction with the Poole Intermediate Care Service and this has been implemented as of 1 July 2008. 2.3.3 Early indications are that a more robust response is being provided, and in early July there have been several days where no delays have been reported. 2.3.4 The Pooled Budget arrangements will be withdrawn if sustained improvement is not achieved. 2.4 Internal Arrangements 2.4.1 An extensive internal review has been undertaken to identify and address processes within the Trust some deficiencies have arisen in part due to changes in external processes that the Trust has struggled to assimilate. A range of actions have been taken and others are in progress. These are summarised below; • Ward Sisters/Charge Nurses have agreed to adopt focussed targets on discharge for their own ward areas. • An extensive training programme has been put in place for ward staff to include support on Continuing Health Care and managing complex discharge. 29 • The Hospital Discharge Liaison Team, which is funded by the PCT but works entirely within the Trust have been refocused and is being supported by the newly appointed Clinical Manager with the responsibility for discharge. He reports directly to the Director of Operations. • Therapists have agreed a single referral protocol with community partners. • Poole Hospital NHS Foundation Trust has agreed the relocation of a ward from Alderney Hospital (Bournemouth and Poole Primary Care Trust rehabilitation facility) for a three month period while the Unit is upgraded, in order to strengthen relationships with community staff and to avoid loss of capacity. • Monthly Liaison Meetings with Social Services and Matrons have been reinstated, chaired by the Director of Operations. • Documentation has been reviewed and a new adult inpatient record incorporating a more robust discharge planning tool will be sent to print in the next month. • Work is underway to strengthen our response to the Single Assessment Process. 3. NEXT STEPS 3.1 The principle objectives are to reduce bed occupancy and length of stay by taking delays to below 3.5%, and to improve the patient experience. 3.2 The ‘No Delays’ programme and the continued development of PICS is expected to have a significant positive impact in securing sustained improvement. 3.3 There is commitment from Poole Social Services to reshape their services to secure improvement. 3.4 While delays for Dorset community hospitals and intermediate care are less problematic they remain a factor and further work is required to ensure the action plan agreed with them in June 2008 is implemented. The Director of Operations has asked for confirmation of the current position. 3.5 Given the complexity associated with delayed discharge and the involvement of several agencies the activity and performance will continue to be routinely reviewed by the Board of Directors. 3.6 Risks remain around loss of capacity in the private care sector. Significant increases in emergency admissions particularly in trauma, and elderly care may also adversely affect the delayed discharge rate if the community is unable to generate sufficient capacity to accommodate increased demand. HEATHER HAUSCHILD Director of Operations July 2008 30











© Copyright 2026