
Medicare Prescription Drug Benefit Manual Table of Contents Transmittals for Chapter 6
Medicare Prescription Drug Benefit Manual Chapter 6 – Part D Drugs and Formulary Requirements Table of Contents (Rev. 10, 02-19-10) Transmittals for Chapter 6 10 - Definition of a Part D Drug 10.1 - General 10.2 - Covered Part D Drug 10.3 - Commercially Available Combination Products 10.4 - Extemporaneous Compounds 10.5 - Medical Supplies Associated with the Delivery of Insulin 10.6 - Medically-Accepted Indication 10.6.1 - Retrospective Determination of a Medically-Accepted Indication 10.7 - Drug Purchased in Another Country 10.8 - Drugs Used to Treat Opioid Dependence 10.9 - DESI Drugs 10.10 - Over-the-Counter Products (OTCs) 10.11 - Common Home Infusion Drugs 10.12 - Bundling of Home Infusion Drugs Under a Part C Supplemental Benefit 10.13 - Inhaler Supplies 10.14 - Vaccine Administration 10.14.1 - Elements of Vaccine Administration 10.14.2 - Establishment of Multiple Vaccine Administration Fees 10.14.3 - Other Vaccine Administration Considerations 20 - Part D Exclusions 20.1 - Excluded Categories 20.2 - Drugs Covered Under Medicare Part A or B 20.2.1 - Exhausted Part A Benefits 20.2.2 - Part D Sponsor Due Diligence in Prior Authorization of Part B Versus Part D Coverage Determination 20.3 - Coverage of Supplemental Drugs Under Enhanced Alternative Coverage 20.4 - Application of General Exclusion Provisions 30 - Formulary Requirements 30.1 - Pharmacy and Therapeutics (P&T) Committee 30.1.1 - Membership 30.1.2 - Conflict of Interest 30.1.3 - P&T Committee Member Disclosure to CMS 30.1.4 - Meeting Administration 30.1.5 - Formulary Management 30.1.6 - Formulary Exceptions 30.1.7 - P&T Committee Role in Transition 30.2 - Provision of an Adequate Formulary 30.2.1 - Formulary Categories and Classes 30.2.1.1 - Application of Existing or New Drugs into the Current Version of the USP Model Guidelines 30.2.2 - Formulary Benefit Management Tools 30.2.2.1 - Formulary Submission of “Safety-Related” Utilization Management Edits 30.2.3 - Long-term Care Accessibility 30.2.4 - Specialty Tiers 30.2.5 - Protected Classes 30.2.6 - Submission of Multiple Formularies 30.2.7 - Formulary Performance and Content Review 30.2.8 - Formulary Submission Timeline 30.3 - Formulary Changes 30.3.1 - Limitation on Changes in Therapeutic Classification 30.3.2 - Limitation of Formulary Changes Prior to Beginning of Contract Year 30.3.3 - Midyear Formulary Changes 30.3.3.1 - Policy Regarding Formulary Changes 30.3.3.2 - Formulary Maintenance Changes 30.3.3.3 - Non-maintenance (Other) Formulary Changes 30.3.4 - Provision of Notice Regarding Formulary Changes 30.3.4.1 - Beneficiary Notice Requirements 30.3.4.2 - Notice for Other Entities 30.3.4.3 - Provision of Notice Regarding Safety-Related Formulary Changes 30.3.4.4 - Notice Requirements for Pending Formulary Changes 30.3.5 - Formulary Change Notice in Advance of Upcoming Contract Year 30.4 - Transition 30.4.1 - Transition Requirements 30.4.2 - General Transition Process 30.4.3 - New Prescriptions Versus Ongoing Drug Therapy 30.4.4 - Transition Timeframes and Temporary Fills 30.4.4.1 - Timeframe and Transition Fills in the Outpatient Setting 30.4.4.2 - Timeframe and Transition Fills in the Long Term Care Setting 30.4.4.3 - Transition Extension 30.4.5 - Transition Across Contract Years 30.4.6 - Emergency Supply for Current Enrollees 30.4.7 - Level of Care Changes 30.4.8 - Edits for Transition Fills 30.4.9 - Cost-sharing Considerations 30.4.10 - Transition Notices 30.4.11 - Public Notice of Transition Process 30.5 - Provider and Patient Education Appendix A - Common Acute Care Home Infusion Drugs Appendix B - Part D Drugs/Supplemental Drugs Summary Table Appendix C - Medicare Part B versus Part D Coverage Issues Appendix D - The Most Commonly Prescribed Drug Classes for the Medicare Population 10 - Definition of a Part D Drug (Rev. 2; Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D drugs are defined in Title XVIII of the Social Security Act (the Act) and in the regulations (42 CFR 423.100). Part D sponsors are responsible for making appropriate coverage determinations and ensuring that covered Part D drugs meet the requirements in this section. 10.1 - General (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) Subject to the exclusions specified in section 20 of this chapter, a Part D drug means a drug that may be dispensed only upon a prescription, is being used for a medically-accepted indication as defined by section 1927(k)(6) of the Act, and is one of the following: A drug that is described in sections 1927(k)(2)(A)(i) through (iii) of the Act; A biological product described in sections 1927(k)(2)(B)(i) through (iii) of the Act; Insulin described in section 1927(k)(2)(C) of the Act; Medical supplies associated with the delivery of insulin; A vaccine licensed under section 351 of the Public Health Service Act and its administration. CMS considers it best practice for Part D sponsors to consider the proper listing of a drug product with the FDA as a prerequisite for making a Part D drug coverage determination. The FDA is unable to provide regulatory status determinations through their regular processes if a drug product is not properly listed. Therefore, Part D sponsors should begin the drug coverage determination process by confirming that a prescription drug product national drug code (NDC) is properly listed with the FDA. CMS interprets “dispensed only upon a prescription” as meaning a drug that is recognized by the Food and Drug Administration as a prescribed drug requiring “Rx only” on its label per section 503(b)(4) of the Federal Food Drug and Cosmetic (FD&C)Act. Additionally, Part D sponsors must recognize a physician‟s authority to delegate prescribing where authorized by State law. Generally, in retail pharmacy, standing orders and protocols are methods used by physicians to delegate and define their prescribing authority to non-physician providers such as pharmacists. Standing orders are typically pre-approved documents for a specific drug or vaccine, contain a set of required clinical criteria and permit administration of the drug without physician examination, as long as the required clinical criteria are met. A protocol is similar to a standing order but is generally broader in scope and may include multiple drugs and extensive clinical criteria. When these and other recognized delegation tools are used in accordance with Federal and State laws, the Part D requirement of “upon a prescription” will be satisfied. 10.2 - Covered Part D Drug (Rev. 2; Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A covered Part D drug is a Part D drug that is included in a Part D sponsor‟s formulary, or treated as being included in a Part D plan‟s formulary as a result of a coverage determination or appeal under 42 CFR 423.566, 423.580, and 423.600, 423.610, 423.620 and 423.630, and obtained at a network pharmacy or an out-of-network pharmacy in accordance with 42 CFR 423.124. 10.3 - Commercially Available Combination Products (Rev. 2; Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Commercially available combination prescription drug products that contain at least one Part D drug component are Part D drugs when used for a “medically-accepted” indication, unless CMS makes the determination that such product, as a whole, belongs in one of the categories of drugs excluded from coverage under Part D. If CMS has not provided guidance to exclude a specific combination product, such combination product, so long as it contains at least one Part D drug component, should be considered a Part D drug (unless it is excluded from coverage under Part D for another reason). 10.4 - Extemporaneous Compounds (Rev. 2; Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Compounded prescription drug products can contain: (1) all Part D drug product components; (2) some Part D drug product components; or (3) no Part D drug product components. Only costs associated with those components that satisfy the definition of a Part D drug are allowable costs under Part D because the compounded products as a whole do not satisfy the definition of a Part D drug. The labor costs associated with mixing a compounded product that contains at least one Part D drug component can be included in the dispensing fee (as defined in 42 CFR 423.100). For compounds containing all generic products, the generic cost-sharing should be applied. If a compound contains any brand name products, the Part D sponsor may apply the higher brand name cost-sharing to the entire compound. 10.5 - Medical Supplies Associated with the Delivery of Insulin (Rev. 2; Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Medical supplies directly associated with delivering insulin to the body, including syringes, needles, alcohol swabs, gauze, and insulin injection delivery devices not otherwise covered under Medicare Part B, such as insulin pens, pen supplies, and needle-free syringes, can satisfy the definition of a Part D drug. However, test strips, lancets and needle disposal systems are not considered medical supplies directly associated with the delivery of insulin for purposes of coverage under Part D. Insulin syringes equipped with a safe needle device, in their entirety (syringe and device), are also Part D drugs and should be managed like any other Part D drug the sponsor places on its formulary. Part D sponsors must make safety enabled insulin syringes available on their formularies for all of their institutionalized beneficiaries. 10.6 - Medically-Accepted Indication (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Section 1860D-2(e)(1)(B) of the Act limits “medically-accepted indication,” by reference to section 1927(k)(6) of the Act, to any use of a covered Part D drug which is approved under the Federal Food, Drug, and Cosmetic Act, or the use of which is supported by one or more citations included or approved for inclusion in any of the compendia described in section 1927(g)(1)(B)(i) of the Act. The compendia are: I. American Hospital Formulary Service Drug Information, II. DRUGDEX Information System, and III. United States Pharmacopeia-Drug Information (or its successor publications).1 Part D sponsors are responsible for ensuring that covered Part D drugs are prescribed for “medically-accepted indications.” Part D sponsors may rely on utilization management policies and procedures to make such determinations but pharmacists are not required to contact each prescriber to verify whether a prescription is being used for other than a medically-accepted indication. “Medically-accepted indication” refers to the diagnosis or condition for which a drug is being prescribed, not the dose being prescribed for such indication. Part D sponsors may have dose limitations based on FDA labeling, but an enrollee may request (and be granted) an exception to a dose restriction through the formulary exception process based on medical necessity criteria. Additionally a Part D drug must be used for a medically-accepted indication that facilitates the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member (except for Part D vaccines). Consequently, if a drug works on medical equipment or devices and is not used for a medically-accepted indication of therapeutic value on the body, it cannot satisfy the definition of a Part D drug. For example, a heparin flush is not used to treat a patient for a medically-accepted indication, but rather to dissolve possible blood clots around an infusion line. Therefore, heparin‟s use in this instance is not therapeutic but is, instead, necessary to make durable medical equipment work. It would therefore not be a Part D drug when used in a heparin flush. 10.6.1 - Retrospective Determination of a Medically-Accepted Indication (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) 1 CMS is considering whether to establish a process for identifying successor publications for purposes of Section 1927(g)(1(B)(i) and will provide further notification of any decision to establish such a process. Part D sponsors may retrospectively identify and confirm – either as part of their retrospective review programs required under 42 CFR 423.153, or incident to another utilization management review – that a dispensed drug was not prescribed for a medically-accepted indication for a particular individual (see the example below, in which this occurred because a dosage issue resulted in the case being flagged). Example: An individual receives a prescription and takes a drug within a common dosing regimen (i.e., one tablet daily). Several months later, that individual‟s physician writes a new prescription for an increased dosage of that drug. The second prescription triggers a quantity limit (for example, based on safety limits) and, as a result, the individual‟s physician submits evidence to support an exception to the quantity limit. Based on that evidence, the Part D sponsor makes a determination that the drug was not prescribed for a medically-accepted indication. When it was not reasonable to expect a Part D sponsor to require prior authorization to ensure a drug is being used for an accepted medical indication, CMS would not expect the sponsor to recover payments made to pharmacies or attempt to obtain reimbursement from enrollees. However, Part D sponsors must send notice of coverage determination decisions to affected enrollees (i.e., those for whom a coverage determination is made based on lack of evidence of a medically-accepted indication) in accordance with the rules provided in 42 CFR 423.566 through 423.576. Such notification must include the following information: The name of the affected covered Part D drug, The reason why the Part D sponsor is no longer covering the drug for the member, Alternative drugs on the Part D sponsor‟s formulary, and expected cost-sharing for those drugs, and The enrollee‟s right to a redetermination. CMS expects a Part D sponsor to consider the enrollee‟s health situation, and continue to cover the drug to the extent it determines that doing so is necessary to avoid risk to the enrollee‟s health while providing for a transition to another form of treatment. 10.7 - Drug Purchased in Another Country (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors must exclude Part D drugs from qualified prescription drug coverage if they are not used and sold in the United States. In addition, Part D sponsors may only pay for drugs that satisfy the definition of Part D drug. In general, such definition requires FDA approval for sale in the United States. Therefore, even if the manufacturer has FDA approval for a drug, the version produced for foreign markets usually does not meet all of the requirements of the U.S. approval, and thus it is considered to be unapproved. 10.8 - Drugs Used to Treat Opioid Dependence (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors must include coverage for Part D drugs, either by formulary inclusion or via an exception, when medically necessary for the treatment of opioid dependence. Coverage is not limited to single entity products such as Subutex®, but must include combination products when medically necessary (e.g., Suboxone®). For any new enrollees, CMS requires sponsors to have a transition policy to prevent any unintended interruptions in pharmacologic treatment with Part D drugs during their transition into the benefit. This transition policy, along with CMS‟ nonformulary exceptions/appeals requirements, should ensure that all Medicare enrollees have timely access to their medically necessary Part D drug therapies for opioid dependence. A Part D drug is defined, in part, as “a drug that may be dispensed only upon a prescription.” Consequently, methadone is not a Part D drug when used for treatment of opioid dependence because it cannot be dispensed for this purpose upon a prescription at a retail pharmacy. (NOTE: Methadone is a Part D drug when indicated for pain). State Medicaid Programs may continue to include the costs of methadone in their bundled payment to qualified drug treatment clinics or hospitals that dispense methadone for opioid dependence. 10.9 - DESI Drugs (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) For a drug to be available for reimbursement by a Part D sponsor it must meet the definition of a Part D drug. Section 1860D–2(e)(1) of the Social Security Act (the Act) generally defines a Part D drug to include those drugs that may be dispensed only upon a prescription and that meet the requirements of section 1927(k)(2) of the Act. Section 1927(k)(2) generally requires that the drug be approved by the FDA or otherwise described under sections 1927(k)(2)(A)(ii) or (A)(iii) of the Act. These provisions address those drugs affected by the Drug Amendments of 1962 (amending the Federal Food, Drug & Cosmetic Act), which require that a new drug be proven effective, as well as safe. FDA‟s Drug Efficacy Study Implementation (DESI) evaluates the effectiveness of those drugs that had been previously approved on safety grounds alone. FDA indicates that these drugs, and those identical, related, and similar to them, may continue to be marketed until the administrative proceedings evaluating their effectiveness have been concluded, at which point continued marketing is permitted only if a new drug application (NDA) or abbreviated new drug application (ANDA) is approved. The vast majority of the DESI proceedings have been concluded, but a few are still pending. The definition of a Part D drug does not include less than effective (LTE) DESI drugs or those identical, related or similar drugs to the LTE DESI drug. As FDA continues to undertake reviews under the DESI program and announces results of its hearings, CMS would expect Part D sponsors to adjust their formularies accordingly, as they should with any other applicable FDA drug product announcement. If a sponsor discovers the presence of any LTE DESIs on its formulary based on an FDA announcement or otherwise, it should remove these drugs from the formularies on accordance with section 30.3.2 10.10 - Over-the-Counter Products (OTCs) (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The definition of a Part D drug does not include OTCs. Therefore, Part D sponsors cannot cover OTCs under their basic prescription drug benefit or as a supplemental benefit under enhanced alternative coverage. However, CMS will allow Part D sponsors the option to provide OTCs as part of their administrative costs structure. Refer to chapter 7, section 60, of this manual for further discussion of this option. When an existing formulary product switches to an OTC status during the contract year, any existing inventory of the previous legend product (manufactured under the legend New Drug Application (NDA) and possessing the legend National Drug Code (NDC) number) will continue to satisfy the Part D drug definition. Given the potential for beneficiaries requiring conversion to other therapeutically equivalent legend products, CMS strongly recommends immediate notification of affected enrollees using the notification criteria outlined in section 30.3.4. CMS will direct sponsors to remove the converted legend product from their formulary at the next formulary submission window after the OTC product becomes available. Providing the OTC product at no cost to beneficiaries, as outlined in chapter 7, section 60, of this manual, will not satisfy CMS‟ formulary requirements and Part D sponsors may need to add additional drugs when the OTC is removed from its formulary. However, adjudication of the legend product may continue as long as the market holds residual inventory. 10.11 - Common Home Infusion Drugs (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS has identified a list of acute care drugs that are most commonly utilized in the home infusion setting. The use of these drugs or drug classes often results in an earlier hospital discharge and reduced healthcare costs. Rapid access to these agents is imperative for these health care transitions. It is CMS‟ expectation that Part D sponsors will not implement policies that could potentially delay or restrict beneficiary access to these important agents. In general, should prior authorization or other utilization management edits apply to any of these agents, CMS would expect that Part D sponsors handle these in an expedited manner in order to facilitate hospital discharge in appropriate time frames. In addition, it is CMS‟ expectation that Part D sponsors ensure appropriate beneficiary access to these drugs or drug classes via formulary inclusion. See Appendix A for a list of commonly utilized home infusion drugs. 10.12 - Bundling of Home Infusion Drugs Under a Part C Supplemental Benefit (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) 2 If, based on an FDA announcement, a Part D sponsor recognizes and removes a non-Part D drug from its formulary; CMS expects that Part D sponsors will provide 60 days of advance notice of the formulary removal. Part D sponsors that offer Medicare Advantage (MA) prescription drug plans may choose to provide Part D home infusion drugs as part of a bundled service as a mandatory supplemental benefit under Part C, provided the sponsor consistently applies the option (i.e., in a given contract year, the plan either always covers a particular home infusion drug as part of a bundled service under Part C, or always covers a particular home infusion drug under Part D). Given uniform benefits requirements, sponsors electing this option must also ensure that the bundled service is available to all enrollees of any MA-PD or cost plan in which it chooses to provide Part D home infusion drugs as a mandatory supplemental benefit under Part C. In addition, plans electing this option must ensure that the bundle of services (which includes both infusion drugs and the services and supplies associated with infusion drugs) is available to all plan enrollees -- including those residing in long-term care facilities -- as a mandatory supplemental benefit under Part C. Interested Part D sponsors must appropriately assign these costs to the Part C component of their bids to account for these bundled drugs. They must also provide, through the Formulary Submission module, a file that clearly identifies the Part D home infusion drugs that will be offered as part of a mandatory supplemental benefit under Part C for the following contract year. CMS will review sponsors’ home infusion drug files as part of our formulary review process to ensure that only home infusion drugs are included as part of the Part C supplemental benefit. Effective with contract year 2010, CMS waives the definition of a Part D drug at 42 CFR 423.100 with respect to Part D drugs covered as part of a bundled benefit under a Part C supplemental benefit. Waiver of the definition of a Part D drug will improve benefit coordination of home infusion therapy between Parts C and D, particularly since the services and supplies necessary for home infusion are never covered under Part D but would be provided as part of a bundle of service under a Part C mandatory supplemental benefit. However, this waiver is conditioned on the application of zero cost sharing for the bundle of home infusion services provided under a Part C supplemental benefit. Thus, sponsors will not qualify for the waiver and, in turn, will not qualify to cover Part D home infusion drugs as part of a bundle of services under a Part C supplemental benefit without indicating on their Plan Benefit Packages (PBPs) that the applicable cost sharing for this bundle of services is $0. In addition, the requirement that Part D sponsors‟ formularies include at least two Part D drugs that are not therapeutically equivalent and bioequivalent in each category and class of covered Part D drugs – except where a particular category or class includes only one Part D drug – at 42 CFR 423.120(b)(2)(i) is waived for Part D sponsors for applicable formulary categories or classes when Part D home infusion drugs are provided as part of a bundled service as a mandatory supplemental benefit under Part C. Waiver of the requirement at 42 CFR 423.120(b)(2)(i) will allow Part D sponsors choosing to provide Part D home infusion drugs as a part of bundled service under a Part C mandatory supplemental benefit to improve benefit coordination of home infusion therapy between Part C and Part D. This improved benefit coordination promotes continuity of care and cost avoidance of more expensive institutional care by facilitating continuous access to home infusion drugs, as well as the costs of administration and supplies associated with that therapy. Part D sponsors choosing to provide Part D home infusion drugs as part of a bundled service must indicate on their marketed formularies that certain drugs may be covered under the sponsor‟s medical, rather than its prescription, benefit. For more information, consult the model formulary available at: http://www.cms.hhs.gov/PrescriptionDrugCovContra/PartDMMM/list.asp#TopOfPage. 10.13 - Inhaler Supplies (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The definition of a Part D drug includes a drug that is described in section 1927(k)(2)(A)(i) of the Social Security Act. This section specifically defines a “covered outpatient drug” as one that is approved for safety and effectiveness as a prescription drug under section 505 of the Federal Food, Drug, and Cosmetic Act, which requires submission by the manufacturer of an NDA or ANDA. In general, only those accessories for meter dose inhalers (MDIs), Dry Powder Inhalers (DPIs), or Nasal Spray Inhalers (NS) that are included on the NDA or ANDA, listed on the package insert, and specifically packaged with the drug product itself are eligible to meet the definition of a Part D drug. If the accessories (i.e., actuator, chamber) are sold separately or are not included on the drug product‟s NDA or ANDA, they would not meet the definition of a Part D drug. 10.14 - Vaccine Administration (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Beginning on January 1, 2008, the Part D program will cover vaccine administration costs associated with Part D vaccines. CMS interprets this statutory requirement to mean that the Part D vaccine administration costs are a component of the negotiated price for a Part D-covered vaccine. In other words, the negotiated price for a Part D vaccine will be comprised of the vaccine ingredient cost, a dispensing fee (if applicable), and a vaccine administration fee. This interpretation recognizes the intrinsic linkage that exists between the vaccine and its corresponding administration, since a beneficiary would never purchase a vaccine without the expectation that it would be administered. In general, CMS believes that Part D vaccines, including the associated administration costs, should be billed on one claim for both in- and out-of-network situations. For example, if an innetwork pharmacy dispenses and administers the vaccine in accordance with State law, the pharmacy would process a single claim to the Part D sponsor and collect from the enrollee any applicable cost-sharing on the vaccine and its administration. Alternatively, if a vaccine is administered out-of-network in a physician‟s office, the physician would provide the vaccine and its administration and then bill the beneficiary for the entire charge, including all components. The beneficiary would, in turn, submit a paper claim to the Part D sponsor for reimbursement for both the vaccine ingredient cost and administration fee. 10.14.1 - Elements of Vaccine Administration (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Vaccine administration fees should be subject to negotiations between Part D sponsors and pharmacies. CMS expects that sponsors will take into consideration the elements reflected in existing Part B vaccine administration fees when establishing their own vaccine administration fees. For example, Part B considers the immunizing professional‟s time in physically delivering the vaccine to a beneficiary, the resources encompassing the supplies (syringe, gauze, band-aid, alcohol prep pad, etc.), the indirect costs of the office, and professional liability. 10.14.2 - Establishment of Multiple Vaccine Administration Fees (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors will have the discretion to implement either a single vaccine administration fee for all vaccines or multiple administration fees based on type of vaccine, variance in provider type, and product administration complexity. CMS plans to retrospectively review vaccine administration fees to look for outliers and potentially discriminatory practices that would impact beneficiary access to Part D vaccines. 10.14.3 - Other Vaccine Administration Considerations (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors may implement drug utilization management tools to determine if a vaccine is necessary; however, in the absence of any information showing previous immunization (i.e., claims data), the Part D sponsor should make payment available for a vaccine and its administration consistent with Advisory Committee on Immunization Practices (ACIP) recommendations. 20 - Part D Exclusions (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) 20.1 - Excluded Categories (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D drugs do not include drugs or classes of drugs, or their medical uses, which may be excluded from coverage or otherwise restricted under section 1927(d)(2) of the Act, except for smoking cessation agents. Excluded: Agents when used for anorexia, weight loss, or weight gain (even if used for a noncosmetic purpose (i.e., morbid obesity)). Agents when used to promote fertility. Agents when used for cosmetic purposes or hair growth. Agents when used for the symptomatic relief of cough and colds. Prescription vitamins and mineral products, except prenatal vitamins and fluoride preparations. Nonprescription drugs. Covered outpatient drugs which the manufacturer seeks to require as a condition of sale that associated tests or monitoring services be purchased exclusively from the manufacturer or its designee. Barbiturates. Benzodiazepines. Agents when used for the treatment of sexual or erectile dysfunction (ED). ED drugs will meet the definition of a Part D drug when prescribed for medically-accepted indications approved by the FDA other than sexual or erectile dysfunction (such as pulmonary hypertension). However, ED drugs will not meet the definition of a Part D drug when used off-label, even when the off label use is listed in one of the compendia found in section 1927(g)(1)(B)(i) of the Act: American Hospital Formulary Service Drug Information, United States Pharmacopeia-Drug Information (or its successor publications), and DRUGDEX Information System. Not Excluded: Prescription drug products that otherwise satisfy the definition of a Part D drug are Part D drugs when used for AIDS wasting and cachexia due to a chronic disease, if these conditions are medically-accepted indications as defined by section 1927(k)(6) of the Act for the particular Part D drug. Specifically, CMS does not consider such prescription drug products being used to treat AIDS wasting and cachexia due to a chronic disease as either agents used for weight gain or agents used for cosmetic purposes. Part D drugs indicated for the treatment of psoriasis, acne, rosacea, or vitiligo are not considered cosmetic. Vitamin D analogs such as calcitriol, doxercalciferol, paricalcitol and dihydrotachysterol, when used for a medically-accepted indication as defined by section 1927(k)(6) of the Act, are not excluded because CMS interprets the exclusion of prescription vitamin D products as being limited to products consisting of ergocalciferol (vitamin D2) and/or cholecalciferol (vitamin D3). Prescription-only smoking cessation products. Prescription Niacin Products (Niaspan, Niacor). Cough and cold medications are eligible to meet the definition of a Part D drug in clinically relevant situations other than those of symptomatic relief of cough and colds. For example, when cough medications are used for a medically-accepted indication that treats a cough produced by a medical condition unrelated to symptomatic cough and cold. In such circumstances, such as the treatment of cough to alleviate bronchospasm in asthma, CMS does not consider these cough medications as excluded drugs. See Appendix B for further clarification of Part D coverage or non-coverage of specific products/drugs/drug categories. 20.2 - Drugs Covered Under Medicare Part A or B (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D specifies that a drug prescribed to a Part D eligible individual cannot be considered a covered Part D drug if payment for such drug „„...is available (or would be available but for the application of a deductible) under part A or B for that individual.‟‟ CMS interprets this to mean that if payment could be available under Part A or Part B to the individual for such drug, then it will not be covered under Part D. Consequently, drugs covered under Parts A and B are considered available (and excluded from Part D) if a beneficiary chooses not to pay premiums or if a beneficiary has enrolled in Part B but that coverage has not yet taken effect. See Appendix C for further explanation and clarification of specific issues regarding coverage under Medicare Part B. 20.2.1 - Exhausted Part A Benefits (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The issue of applicability of Part D coverage has also arisen in the context of inpatients in acute care hospital settings (including long-term care (LTC) hospitals, which are certified as acute care hospitals) who have exhausted their Part A inpatient stay benefit, but who require and continue to receive a level of care that qualifies them for a Part A inpatient stay. Drugs provided in an inpatient setting to an individual who has exhausted his or her lifetime inpatient hospital benefit under Part A are not drugs that could be covered under Part A for that individual. Unlike a beneficiary who, for example, chooses not to buy into Part B, there is no way for an individual who has exhausted his or her Part A inpatient stay benefit to obtain coverage under Part A for his or her drugs; therefore, Part D coverage may be available to a Part D enrollee who has exhausted his or her Part A inpatient stay benefit and who remains in that inpatient setting (provided the drug would otherwise be covered under Part D). See chapter 5, section 50.5.4, regarding sponsor contracting requirements when a beneficiary has exhausted inpatient Part A benefit days. 20.2.2 - Part D Sponsor Due Diligence in Prior Authorization of Part B Versus Part D Coverage Determination (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors may rely upon physician information included with the prescription, such as diagnosis information (e.g., to determine whether the prescription is related to a Medicare covered transplant) or location of administration (e.g., to determine if the prescription is being dispensed for a beneficiary in a nursing home) to the same extent they rely on similar information acquired through documentation from physicians on prior authorization forms. Assuming the indication on the script is sufficient to make the coverage determination, there is no need in such cases to require additional information to be obtained from the physician. To the extent that the Part D sponsor requires its contracted pharmacies to report the information provided on the prescription to assist in the determination of Part B versus Part D coverage, the sponsor may rely on the pharmacist‟s report of appropriate information to make the coverage determination under Part D. For example, for cases in which prednisone is prescribed for a condition other than immunosuppression secondary to a Medicare-covered transplant, and this is indicated on the prescription, a sponsor may cover the drug under Part D without seeking further information from the prescribing physician. This clarification should not be construed to indicate that a Part D sponsor may not impose prior authorization or other procedures to ensure appropriate coverage under the Medicare drug benefit. The Part D sponsor is ultimately responsible for making the initial Part D coverage determination. However, CMS believes that the sponsor will have met appropriate due diligence standards without further contacting a physician if necessary and sufficient information is provided on the prescription, and the contracted pharmacy is able to communicate this information to the sponsor in order to make the coverage determination. CMS encourages industry trade collaboration with Part D sponsors to streamline Part B vs. Part D coverage determinations. For instance, CMS has received comments recommending that as Part D sponsors learn of a beneficiary‟s transplant status they record this in an electronic database which could be shared with subsequently enrolled Part D sponsors minimizing data collection and speeding appropriate coverage determinations. CMS also encourages further utilization of locator codes in claims for long term care beneficiaries who are ineligible for Part B drugs under the durable medical equipment benefit based on their place of residence. 20.3 - Coverage of Supplemental Drugs Under Enhanced Alternative Coverage (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor may include coverage of drugs that would meet the definition of a Part D drug but for the application of section 20.1 (these are known as “supplemental drugs,” as provided in section 10.2 of chapter 5 of this manual) as a supplemental benefit under enhanced alternative coverage. 20.4 - Application of General Exclusion Provisions (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) In accordance with section 1860D-2(e)(3) of the Act, a Part D sponsor may exclude from qualified prescription drug coverage any Part D drug: For which payment would not be made if items and services are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member (except for Part D vaccines); or Which is not prescribed in accordance with the Part D sponsor. Such exclusions are coverage determinations subject to reconsideration and appeal. Unlike other Part D drugs that may be excluded when not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member, Part D vaccines may only be excluded when their administration is not reasonable and necessary for the prevention of illness. 30 - Formulary Requirements (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor that uses a formulary under its qualified prescription drug coverage must meet requirements for the following: Pharmacy and Therapeutics committee; Provision of an adequate formulary; Transition process; Limitation on changes in therapeutic classification; Provision of notice regarding formulary changes; Limitation of formulary changes prior to beginning of contract year; Provider and patient education; and Formulary changes during the contract year. 30.1 - Pharmacy and Therapeutics (P&T) Committee (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor‟s formulary must be developed and reviewed by a P&T committee that meets specific requirements with respect to: Membership; Conflict of interest; P&T member disclosure to CMS; Meeting administration; Formulary management; Formulary exceptions; and P&T committee role. 30.1.1 - Membership (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors‟ P&T committee membership must satisfy the following requirements: P&T committee members must come from various clinical specialties that adequately represent the needs of sponsors‟ enrollees. A majority of the P&T committee members must be practicing physicians, practicing pharmacists or both. At least one P&T committee practicing pharmacist and one practicing physician must be an expert in the care of elderly or disabled persons. At least one P&T committee practicing pharmacist and one practicing physician must be independent and free of conflict with respect to the Part D sponsor and pharmaceutical manufacturers. Such P&T committee members may have certain non-employee relationships with pharmaceutical manufacturers (for example consulting, advisory, or research relationships) and still be considered independent and free of conflict provided those relationships do not constitute significant sources of income and they do not otherwise have a conflict of interest that would compromise their independence. In addition, panel providers in a staff model HMO may be considered independent and free of conflict to the extent that any remuneration received from a Part D sponsor is limited to his or her clinical responsibilities for the care of plan enrollees. 30.1.2 - Conflict of Interest (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) P&T committee members should sign a conflict of interest statement revealing economic or other relationships with entities affected by drug coverage decisions that could influence committee decisions. 30.1.3 - P&T Committee Member Disclosure to CMS (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) In the event the Part D sponsor has entered into a confidential agreement such that the Pharmacy Benefits Manager (PBM) will not disclose its P&T committee membership to the Part D sponsor, then it is the Part D sponsor‟s responsibility to notify CMS that this information will be submitted by the sponsor‟s PBM. Moreover, the Part D sponsor must ensure that the PBM notifies CMS of the P&T committee membership. The Part D sponsor maintains ultimate responsibility for adhering to and otherwise fully complying with all terms and conditions of its contract and the sponsor must ensure that the PBM notifies the sponsor that this information has been successfully submitted to CMS. 30.1.4 - Meeting Administration (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The Part D sponsor‟s P&T committee should meet on a regular basis, but no less than quarterly. P&T committee decisions regarding formulary development or revision must be documented in writing. 30.1.5 - Formulary Management (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsor‟s P&T committee will consider the following: The P&T committee must review for clinical appropriateness the practices and policies for formulary management activities, such as prior authorizations, step therapies, quantity limitations, generic substitutions and other drug utilization activities that affect access. P&T committee recommendations regarding these activities are advisory only and not binding on the Part D sponsor. Formulary management decisions must be based on scientific evidence, and may also be based on pharmacoeconomic considerations that achieve appropriate, safe and cost effective drug therapy. The P&T committees will be required to establish and document procedures to ensure appropriate drug review and inclusion. This includes documentation of decisions regarding formulary development and revision and utilization management activities (42 CFR 423.120(b)(1)(viii)). P&T committee recommendations regarding which Part D drugs are placed on a sponsor‟s formulary are binding on the Part D sponsor. Clinical decisions by the P&T committee should be based on scientific evidence and standards of practice, including peer reviewed medical literature, well-established clinical practice guidelines and pharmacoeconomic studies, as well as other sources of appropriate information. Drugs‟ therapeutic advantages in terms of safety and efficacy must be considered when selecting formulary drugs and placing them on formulary tiers. The P&T committee will make a reasonable effort to review a new FDA approved drug product (or new FDA approved indication) within 90 days and will make a decision on each new FDA approved drug product (or new FDA approved indication) within 180 days of its release onto the market, or a clinical justification will be provided if this timeframe is not met. The P&T committee will evaluate and analyze treatment protocols and procedures related to the sponsor‟s formulary at least annually. The P&T committee will approve inclusion or exclusion of the therapeutic classes in the formulary on an annual basis. Part D sponsors that change PBMs mid-year are required to continue the existing formulary. Decisions regarding formulary inclusion made by the previous PBM‟s P&T committee are binding on the assuming PBM. CMS will not approve negative formulary change requests for the purpose of aligning an existing formulary with that of a new PBM. 30.1.6 - Formulary Exceptions P&T committees must review for clinical appropriateness protocols and procedures for the timely use of and access to both formulary and non-formulary drug products. Part D coverage determinations and appeals information can be found in chapter 18 of this manual. 30.1.7 - P&T Committee Role in Transition (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) At a minimum, a sponsor‟s transition process, the minimum requirements of which are detailed in section 30.4, will address procedures for medical review of non formulary drug requests and, when appropriate, a process for switching new Part D sponsor enrollees to therapeutically appropriate formulary alternatives failing an affirmative medical necessity determination. CMS will look to transition process submissions for assurances that a sponsor‟s P&T committee will review and provide recommendations regarding the procedures for medical review of nonformulary drug requests. P&T committee involvement will help ensure that transition decisions appropriately address situations involving enrollees stabilized on drugs that are not on the sponsor‟s formulary (or that are on the formulary but require prior authorization or step therapy under a sponsor's utilization management requirements) and which are known to have risks associated with any changes in the prescribed regimen. 30.2 - Provision of an Adequate Formulary (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS encourages Part D sponsors to submit formularies similar to those in widespread use today. CMS will check the formulary to ensure inclusion of a range of drugs in a broad distribution of therapeutic categories and classes, in order to satisfy the Medicare Modernization Act (MMA) requirement that a sponsor‟s categorization system does not substantially discourage enrollment by any group of beneficiaries. CMS will consider the specific drugs, tiering and utilization management strategies employed in each formulary. CMS will identify outliers from common benefit management practices for further evaluation. Sponsors may be asked to provide written clinical justification for unusual benefit features that are identified as outliers. 30.2.1 - Formulary Categories and Classes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D formularies must include drug categories and classes that cover all disease states. CMS will evaluate the sufficiency of a Part D sponsor‟s formulary categories and classes in conjunction with the formulary drug list to ensure that the formulary provides access to an acceptable range of Part D drug choices. Part D sponsors that utilize a classification system that is consistent with the United States Pharmacopedia (USP) classification system, available at www.usp.org, will qualify for a safe harbor, meaning that CMS will approve their formulary classification system. For sponsors that choose to adopt an alternative to USP‟s classification structure, CMS will check the sponsor‟s proposed classification system to determine if it is similar to USP or other commonly used classification systems, such as the American Hospital Formulary Service (AHFS) Pharmacologic-Therapeutic Classification (information available at www.ashp.org/ahfs). Each category or class must include at least two drugs (unless only one drug is available for a particular category or class, or only two drugs are available but one drug is clinically superior to the other for a particular category or class), regardless of the classification system that is utilized. The two drug minimum requirement must be met through the provision of two chemically distinct drugs. In other words, Part D sponsors will not meet this requirement by including only two dosage forms or strengths of the same drug, or a brand name drug and its generic equivalent. Aside from the inclusion of two drugs in each category or class, multiple strengths and dosage forms should also be available for each covered drug. This should encompass dosage forms used commonly in LTC facilities and home infusion. CMS may require more than two drugs for particular categories or classes if additional drugs present unique and important therapeutic advantages in terms of safety and efficacy, and their absence from the sponsor‟s formulary would substantially discourage enrollment by beneficiaries with certain disease states. 30.2.1.1 - Application of Existing or New Drugs into the Current Version of the USP Model Guidelines (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) For those formularies that utilize the USP Model Guidelines classification structure, there are several methods to accommodate new Part D drugs that come on to the market during the contract year. These methods may also be utilized to accommodate existing Part D drugs that cannot be classified under the USP Model Guidelines. CMS expects one of the four options listed below to be used for the above mentioned situations. 1. Addition of a Part D drug into an existing USP category or class. In the event that a new Part D drug is approved and is to be added to the formulary, the newly approved Part D drug may fit into the current classification system. For instance, if a new protease inhibitor is approved, this drug would be added to the formulary in the USP Antivirals category, under the Anti-HIV Agents, Protease Inhibitors class. 2. Placement of a Part D drug into an “Other” class. In the current USP Model Guidelines, USP listed an “Other” class under various categories. Should a new Part D drug receive approval that can not be placed into an existing class, and the particular USP category contains an “Other” class, the new drug may be placed into the “Other” class. 3. Addition of a new class under an existing category. If a new Part D drug is approved that does not fit into an existing class, but is appropriate for a particular category, then a new class may be displayed under an existing category. This method would also apply to formularies that utilize AHFS or an other classification structure. 4. Miscellaneous Therapeutic Agents. If an existing or newly approved Part D drug does not fit into any existing category, a “Miscellaneous Therapeutic Agents” category may be displayed on the formulary. 30.2.2 - Formulary Benefit Management Tools (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS will look to existing best practices to check that Part D sponsors‟ use of prior authorization, step therapy, and quantity limits is consistent with such practices. CMS will look to current industry standards as well as appropriate guidelines that might be found from expert organizations and to the use of such standards in existing drug sponsors that are widely used by seniors and people with disabilities. CMS will ensure that sponsors‟ use of such tools is consistent with best practices. CMS will also compare formularies among the applicants to analyze the comparative use of practices such as prior authorization, step therapy, and quantity limits. Part D sponsors should be consistent with the FDA approved label when applying prior authorization to assess beneficiaries‟ eligibility for coverage. In cases where a sponsor may fall outside of best practices, the sponsor will be asked to provide a reasonable justification for its practices. CMS‟ expectation is that formulary benefit management tools will be used in Part D formularies consistent with the way they are applied in existing formulary systems. 30.2.2.1 - Formulary Submission of “Safety-Related” Utilization Management Edits (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS continues to require Part D sponsors to submit utilization management requirements, such as prior authorization, step therapy and quantity limits not based upon the FDA‟s maximum daily dose limits, as part of their Health Plan Management System (HPMS) formulary submission. See chapter 7 of this manual for more information on drug utilization management tools. CMS does not require Part D sponsors to submit all point-of-sale (POS) safety related edits as part of their HPMS formulary submission. Specifically, CMS does not require Part D sponsors to submit those POS safety edits implemented to satisfy the concurrent drug utilization review requirements set forth in 42 CFR 423.150(c)(2). These edits are typically applied at the point-ofsale or point-of-distribution and assist the pharmacist in identifying and/or preventing inappropriate drug therapy. These utilization review edits include the following: ● Screening for potential drug therapy problems due to therapeutic duplication; ● Age/gender-related contraindications; ● ● ● ● Over-utilization and underutilization (e.g., early refill); Drug-drug interactions; Incorrect drug dosage or duration of drug therapy; and Drug-allergy contraindications 30.2.3 - Long-term Care Accessibility (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors will be required to provide medically necessary prescription drug treatments for enrollees in the general Medicare population, as well as those enrollees who reside in LTC facilities. For example, it is CMS‟ expectation that sponsors provide coverage of dosage forms of drugs that are widely utilized in the LTC setting, such as unit dose products and liquid, chewable, and parenteral preparations. Further, while nebulized solutions may not be required on all formularies, CMS would expect sponsors to also cover these dosage forms under circumstances in which Part B coverage is not available. When determining days supplies for residents in LTC facilities, Part D sponsors should follow industry best practices and allow for at least 31 days per fill. 30.2.4 - Specialty Tiers (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) 42 CFR 423.578(a)(7) allows Part D sponsors to exempt a formulary tier, in which it places very high cost and unique items, from tiered cost-sharing exceptions. In order to ensure that a Part D sponsor does not substantially discourage enrollment by specific patient populations reliant upon these medications, CMS will only approve specialty tiers within formularies and benefit designs that comply with the following: Only one tier is designated a specialty tier exempt from cost-sharing exceptions. Cost-sharing associated with the specialty tier is limited to 25% after the deductible and before the initial coverage limit (or an actuarially equivalent for sponsors with decreased or no deductible under alternative prescription drug coverage designs). Only Part D drugs with sponsor negotiated prices that exceed the dollar-per-month amount established by CMS in the annual Call Letter may be placed in the specialty tier. CMS will apply an upfront evaluation across all plans for drugs that exceed the dollarper-month threshold and are intended for inclusion in the specialty tier. If not all drugs (including all strengths) within a category or class meet the criteria for inclusion in the specialty tier, the sponsor must ensure that placement of the remaining drugs among the other tiers of the formulary does not substantially discourage enrollment. Part D sponsors will need to evaluate the negotiated prices at the drug product strength, package size, and formulation level in order to determine appropriate inclusion of the drug in the Part D plan‟s specialty tier. If a Part D drug product is available in multiple strengths, package sizes and formulations, CMS will only allow inclusion on the specialty tier of those strengths, package sizes and formulations that would reasonably exceed the dollar-per-month threshold. As a result, Part D sponsors should be prepared to locate smaller package sizes, strengths, and formulations of the very same drug on a tier other than the specialty tier if the smaller size cannot satisfy the monthly dollar threshold. Part D sponsors must evaluate the long acting nature of some drug formulations and calculate the monthly cost across the drug's full duration of action. For example, if the specialty tier threshold was $600 dollars, a long acting formulation with a plan negotiated price of $900 dollars that lasts for 3 months would not be eligible for the plan's specialty tier since the monthly cost is only $300 dollars. 30.2.5 - Protected Classes (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) Part D sponsor formularies must include all or substantially all drugs in the immunosuppressant (for prophylaxis of organ transplant rejection), antidepressant, antipsychotic, anticonvulsant, antiretroviral, and antineoplastic classes. CMS instituted this policy because it was necessary to ensure that Medicare beneficiaries reliant upon these drugs would not be substantially discouraged from enrolling in certain Part D plans, as well as to mitigate the risks and complications associated with an interruption of therapy for these vulnerable populations. Formularies must include substantially all drugs in these six categories that are FDA approved by the last CMS specified HPMS formulary upload date for the upcoming contract year. New drugs or newly approved uses for drugs within the six classes that come onto the market after the CMS specified formulary upload date will be subject to an expedited P&T committee review. The expedited review process requires P&T committees to make a decision within 90 days, rather than the normal 180-day requirement. At the end of the 90 day period, these drugs must be added to Part D plan formularies. “Substantially all” in this context means that all drugs and unique dosage forms in these categories are expected to be included in sponsor formularies, with the following exceptions: multi-source brands of the identical molecular structure; extended release products when the immediate-release product is included; products that have the same active ingredient or moiety; and dosage forms that do not provide a unique route of administration (e.g., tablets and capsules versus tablets and transdermals); Part D sponsors may not implement prior authorization or step therapy requirements that are intended to steer beneficiaries to preferred alternatives within these classes for enrollees who are currently taking a drug. This prohibition applies to those beneficiaries already enrolled in the plan as well as new enrollees who were actively taking drugs in any of the six classes of clinical concern prior to enrollment into the plan. If a sponsor cannot determine at the point of sale that an enrollee is not currently taking a drug (e.g., new enrollee filling a prescription for the first time), sponsors shall treat such enrollees as currently taking the drug. For HIV/AIDS drugs, utilization management tools such as prior authorization and step therapy are generally not employed in widely used, best practice formulary models. Part D sponsors may conduct consultations with physicians regarding treatment options and outcomes in all cases. Part D sponsors may apply prior authorization to establish appropriate payment under Part B or Part D, even if the beneficiary is currently taking the drug. In Part B versus Part D situations, CMS expects Part D sponsors will work aggressively to eliminate any interruptions of current therapy. 30.2.6 - Submission of Multiple Formularies (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS recognizes that sponsors may wish to submit more than one formulary in order to offer enhanced access to Part D drugs. CMS has the responsibility to ensure that there are meaningful differences between multiple formulary submissions from one organization to reduce confusion amongst beneficiaries. CMS may request that sponsors withdraw a formulary in which no meaningful differences can be demonstrated. 30.2.7 - Formulary Performance and Content Review (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) Regardless of the classification system chosen, CMS will review and approve drug lists that are consistent with best practice formularies currently in widespread use today. The current formulary requirements are subject to change and/or revision. CMS requires formulary drug lists to pass the following checks: CMS will review formularies to ensure representation of USP formulary key drug types on all Part D formularies. Part D sponsors whose formularies are identified as outliers will be contacted and their formularies will require re-evaluation. CMS will review tier placement to ensure that the formulary does not substantially discourage enrollment of certain beneficiaries. When developing their formulary tier structure, sponsors should utilize standard industry practices. Tier 1 should be considered the lowest cost-sharing tier available to beneficiaries. Any and all subsequent tiers within the formulary structure will be higher cost-sharing tiers in ascending order. For example, drugs in Tier 3 will have a higher cost-share for beneficiaries than drugs in Tier 2. Best practices in existing formularies and preferred drug lists generally place drugs in a less preferable position only when drugs that are therapeutically similar (i.e., drugs that provide similar treatment outcomes) are in more preferable positions on the formulary. The CMS review will focus on identifying drug categories that may substantially discourage enrollment of certain beneficiaries by placing drugs in non-preferred tiers in the absence of commonly used therapeutically similar drugs in more preferred positions. CMS will analyze formularies to determine whether appropriate access is afforded to drugs or drug classes addressed in widely accepted treatment guidelines which are indicative of general best practice. Examples of these may include asthma, diabetes, chronic stable angina, atrial fibrillation, heart failure, thrombosis, lipid disorders, hypertension, chronic obstructive pulmonary disease, dementia, depression, bipolar disorder, schizophrenia, benign prostatic hyperplasia, osteoporosis, migraine, gastroesophageal reflux disease, epilepsy, Parkinson‟s disease, end stage renal disease, hepatitis, tuberculosis, community acquired pneumonia, rheumatoid arthritis, multiple sclerosis and HIV. Part D sponsors should be aware of treatment guidelines impacting those enrollees residing in LTC facilities, such as CDC‟s annual Morbidity and Mortality Weekly Report (MMWR) on prevention and control of influenza. This list of conditions does not represent an exhaustive list, but merely serves as another check in the review process. CMS will analyze the availability and tier position of the most commonly prescribed drug classes for the Medicare population (Appendix D). This list is derived from Part D claims data. The drugs identified will be expanded to the class level and used in the formulary review process. CMS understands that sponsors will not provide identical coverage of these drug classes, and CMS‟ review will focus on ensuring that sponsors present a balanced formulary. These drug classes will cover common diseases and conditions, and will allow CMS to ensure that sponsors are covering the most widely used medications, or therapeutically similar medications, for the most common conditions. CMS will review all Part D sponsors‟ formularies to ensure they contain all commercially available vaccines (unless excluded due to available reimbursement under Part B, e.g., influenza or pneumococcal vaccines). Sponsors will only be allowed to use drug utilization management tools to: o Assess the necessity of vaccines that are less commonly administered in the Medicare population, such as anthrax and yellow fever vaccines; o Facilitate use of vaccines in line with Advisory Committee on Immunization Practices (ACIP) recommendations; and o Evaluate potential reimbursement of those vaccines that could be covered under Part B when directly related to the treatment of an injury or direct exposure to a disease or condition (e.g., tetanus). All formularies will be evaluated using the criteria above in this section. Outliers for each area of review will be further evaluated by CMS to determine whether the outlier is deemed potentially discriminatory. Examples of this may include a lack of appropriate drug classes to treat certain diseases, a lack of sufficient drugs in a therapeutic class, inappropriate tier placement that would discriminate against a group of beneficiaries, or missing drugs that would cause discrimination. If any of the outliers appear to create problems of access, sponsors will have the opportunity to present reasonable clinical justifications. 30.2.8 - Formulary Submission Timeline (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors that fail to meet formulary submission and re-submission deadlines during the formulary approval process may face a CMS determination that CMS cannot approve their Part D bids. For most Part D sponsors, a failure to obtain bid approvals will result in the termination of their Part D sponsor or MA organization contracts effective at the end of the existing contract year. In the case of an initial Part D sponsor or MA organization contract applicant, CMS would decline to enter into a contract with the organization. All Part D sponsors that fail to meet CMS established formulary timelines will be precluded from entering into a contract with CMS. Such a determination would be made on the basis that the organization had failed to submit a bid which CMS could approve, a determination that would not be subject to a request for appeal under Subpart N of 42 CFR 423 (for Part D sponsors) and 42 CFR 422 (for MA organizations). 30.3 - Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The removal of any drug, whether a Part D drug or a supplemental drug offered as a supplemental benefit under an enhanced alternative benefit design, is subject to the formulary change guidance contained in the following sections. 30.3.1 - Limitation on Changes in Therapeutic Classification (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Except as CMS may permit to account for new therapeutic uses and newly approved Part D drugs, a Part D sponsor may not change formulary categories and classes after the last CMS specified HPMS formulary upload date for the upcoming contract year. 30.3.2 - Limitation of Formulary Changes Prior to Beginning of Contract Year (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Except when the Food and Drug Administration deems a Part D drug unsafe or a manufacturer removes a Part D drug from the market, a Part D sponsor may not remove a covered Part D drug from its formulary, or make any change in preferred or tiered cost-sharing status of a covered Part D drug, between the beginning of the annual coordinated election period described in section 42 CFR 423.38(b) and 60 days after the beginning of the contract year associated with the annual coordinated election period. 30.3.3 - Midyear Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Both industry best practices and the best interests of Medicare beneficiaries call for limited formulary changes during the contract year. CMS believes that formulary stability is extremely important so that enrollees maintain access to the benefit they chose during enrollment as represented to them by the sponsor. However, prescription drug therapies are constantly evolving, and new drug availability, medical knowledge, and opportunities for improving safety and quality in prescription drug use at a low cost will inevitably occur over the course of the year. As recognized in the statute and regulations, these new developments may require formulary changes during the year in order to provide high-quality, low-cost prescription drug coverage. 30.3.3.1 - Policy Regarding Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) The following is CMS‟ policy regarding formulary changes: Part D sponsors may expand formularies by adding drugs to their formularies, reducing copayments or coinsurance by placing a drug on a lower cost-sharing tier, or deleting utilization management requirements at any time during the year. Formulary Maintenance Changes: After March 1, Part D sponsors may make maintenance changes to their formulary, such as replacing brand name with new generic drugs or modifying formularies as a result of new information on drug safety or effectiveness. Non-maintenance (Other) Formulary Changes: Part D sponsors may only remove Part D drugs from their formulary, move covered Part D drugs to a less preferred tier status, or add utilization management requirements. For these additional types of formulary changes approved by CMS, Part D sponsors should make such formulary changes only if enrollees currently taking the affected drug are exempt from the formulary change for the remainder of the contract year. CMS must approve any changes to a Part D sponsor‟s formulary; however, Part D sponsors are not required to obtain CMS approval for drugs that have been withdrawn from the market by either the FDA or a product manufacturer. 30.3.3.2 - Formulary Maintenance Changes (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) In order to promote best practices and protect the interests of Medicare beneficiaries, CMS will generally give positive consideration to the following types of formulary changes: Removal or placement in a less preferred tier of a brand name drug upon the availability and addition of an A-rated generic or multi-source brand name equivalent, at a lower tier or cost to the beneficiary. Removal of a non-Part D drug inadvertently included on the formulary. Addition of utilization management tools based upon a new FDA “black box” warning. Removal of a drug based upon a new FDA market withdrawal notice. Removal of a drug based on long term shortage and market availability (described in chapter 5, section 50.13). Removal or placement in a less preferred tier based upon new clinical guidelines or information recognized by CMS (e.g., CDC‟s recommendation against using older antivirals for treatment and prophylaxis of the flu). The addition of utilization management when necessary to effectuate other approved formulary changes (e.g., prior authorization on a brand name drug when generic is now available on formulary at a lower cost), to help determine B vs. D coverage (subject to CMS guidance on least burdensome ways to make this determination), or to promote safe utilization of a Part D drug based upon new clinical guidelines or information. Part D sponsors will need to provide a justification when submitting formulary maintenance change requests, but they may assume that change requests based upon these justifications are approved if they do not hear from CMS within 30 days of submission. 30.3.3.3 - Non-maintenance (Other) Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Experience with formulary management indicates that the vast majority of formulary changes are “maintenance” changes that would generally be approved by CMS. CMS will review additional types of non-maintenance formulary change requests and their corresponding justification. Part D sponsors should make such formulary changes only if enrollees currently taking the affected drug are exempt from the formulary change for the remainder of the contract year. These additional types of change requests include, but are not limited to: Changing preferred or non-preferred formulary drugs, adding utilization management, or increasing cost sharing on preferred drugs (unrelated to the reasons stated above); Removing dosage forms; or Exchanging therapeutic alternatives (either by formulary addition/removal or tier exchanges). If CMS disapproves a formulary change request, the justification for disapproval will generally be based on one of the following: The reasonableness and/or necessity for the proposed change in the context of preventing any appearance of “bait and switch” in the formulary. Medicare beneficiaries select Part D sponsors, in part, based on the formulary that is marketed during annual open enrollment and, therefore, have a legitimate expectation that they will have continuing access to coverage of the Part D drugs they are using throughout the contract year. This beneficiary expectation will be balanced against the sponsor‟s desire to practice good formulary management in order to provide a low-cost, high-quality prescription drug benefit that continues to effectively meet the needs of beneficiaries. Part D sponsors may avoid any appearance of a “bait and switch” concern by exempting enrollees who are currently using the affected drugs from the formulary change for the remainder of the contract year. The proposed change on its face in the context of substantially discouraging enrollment by certain beneficiary groups. The impact of the proposed change on the formulary as a whole to ensure the formulary continues to satisfy the minimum formulary requirements established by CMS. Because these additional types of change requests will require more extensive review by CMS, Part D sponsors must not implement such changes until they receive explicit notification of approval from CMS and must not issue any beneficiary notices of such forthcoming changes prior to receiving explicit and affirmative CMS approval. 30.3.4 - Provision of Notice Regarding Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors must provide notice of formulary changes as outlined in the following sections. Additionally, for formulary maintenance changes (described in section 30.3.2), CMS will not require Part D sponsors to wait for approval before sending notice of a proposed formulary change to required parties. For these changes, a Part D sponsor may choose to provide notice to CMS and other required parties at the same time. Part D sponsors will provide notice to CMS via the HPMS system, which will also require plans to specify the intended effective date. Although sponsors may provide notice to all required parties prior to receiving CMS approval, sponsors might prefer to wait so that they do not risk sending notice of a change that is subsequently disapproved by CMS. For formulary non-maintenance or “other” changes (described in section 30.3.3.3), Part D sponsors must not issue any beneficiary notices until CMS has explicitly approved the non-maintenance change. 30.3.4.1 - Beneficiary Notice Requirements (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Prior to removing a covered Part D drug from its formulary, or making any change in the preferred or tiered cost-sharing status of a covered Part D drug, a Part D sponsor must either: Provide direct written notice to affected enrollees at least 60 days prior to the date the change becomes effective; or At the time an affected enrollee requests a refill of the Part D drug, provide such enrollee with a 60 day supply of the Part D drug under the same terms as previously allowed and written notice of the formulary change. If a beneficiary is not “affected” by a formulary change (in other words, exempted from a formulary change), notice is not required. The written notice must contain the following information: The name of the affected covered Part D drug; Whether the Part D sponsor is removing the covered Part D drug or changing its preferred or tiered cost-sharing status; The reason why the Part D sponsor is removing such covered Part D drug from the formulary, or changing its preferred or tiered cost-sharing status; Alternative drugs in the same therapeutic category or class or cost-sharing tier and expected cost-sharing for those drugs; and The means by which enrollees may obtain a coverage determination under 42 CFR 423.566 or exception under 42 CFR 423.578. As an alternative to providing written notice, Part D sponsors may provide such notice electronically if, and only if, an enrollee affirmatively elects to receive such notice electronically. 30.3.4.2 - Notice for Other Entities (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Prior to removing a covered Part D drug from its formulary, or making any change in the preferred or tiered cost-sharing status of a covered Part D drug, a Part D sponsor must provide at least 60 days notice to CMS, State Pharmaceutical Assistance Programs (as defined in 42 CFR 423.454), entities providing other prescription drug coverage (as described in 42 CFR 423.464(f)(1), authorized prescribers, network pharmacies, and pharmacists prior to the date such change becomes effective. To the extent possible, sponsors may elect to provide State Pharmaceutical Assistance Programs, entities providing other prescription drug coverage (as described in 42 CFR 423.464(f)(1), authorized prescribers, network pharmacies, and pharmacists an annual notice providing information on the sponsor‟s formulary change policy (i.e., length of notice, methods of communication with beneficiaries, and any electronic notices providers may receive at the pointof-sale regarding formulary status) and the sponsor‟s Web site where these entities can verify the formulary status of particular drugs. 30.3.4.3 - Provision of Notice Regarding Safety-Related Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors may immediately remove from their formularies covered Part D drugs deemed unsafe by the Food and Drug Administration or removed from the market by their manufacturer without meeting the advance notice requirements specified in this section. However, Part D sponsors must provide retrospective notice of any such formulary changes to affected enrollees, CMS, State Pharmaceutical Assistance Programs (as defined in 42 CFR 423.454), entities providing other prescription drug coverage (as described in 42 CFR 423.464(f)(1), authorized prescribers, network pharmacies, and pharmacists consistent with the requirements set forth in this section. CMS expects that this retrospective notice will occur as soon as possible to inform enrolled beneficiaries of potential safety concerns surrounding medications they are taking, especially those beneficiaries who may have a 90 day supply and will not interact with the pharmacy for an extended period. In instances where there has been an announcement of a market withdrawal, but the withdrawal has not yet taken place, Part D sponsors may opt to either remove the drug immediately with a retrospective notice to “affected enrollees” or provide an advance notice. CMS expects Part D sponsors to consider all pertinent information available from the FDA related to the withdrawal. 30.3.4.4 - Notice Requirements for Pending Formulary Changes (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) When a Part D sponsor notifies CMS of a formulary change in HPMS, the change is assigned a prospective effective date. During the period of time between when a Part D sponsor has notified CMS of a prospective change and the actual effective date of that change, Part D sponsors must ensure appropriate beneficiary protections are implemented should a beneficiary who has not been notified of the change present with a new prescription for the drug whose formulary status is changing. For maintenance changes outlined in section 30.3.3.2, the Part D sponsor must implement the beneficiary notice requirements contained in section 30.3.4.1 (i.e., 60 days of advance written notice before implementing the change for the individual). For example, assume on March 1st, a Part D sponsor notifies CMS via HPMS that it is removing a brand name drug from its formulary due to the availability of a new generic. The sponsor indicates the effective date for this formulary change will be May 1st. If a beneficiary were to present on April 1st with a new prescription for the brand name drug pending removal, the Part D sponsor would provide written notice of the change and not implement the change until June 1st, in order to provide the full 60 days of advance notice to that beneficiary. A Part D sponsor may elect to provide written notice to all of its enrollees of a pending formulary maintenance change in lieu of notifying only the “affected enrollees.” Such an approach would satisfy the beneficiary notice requirements in section 30.3.4.1 because all enrollees, including “affected enrollees” would receive advance notice of a formulary change. In addition, it would preclude the plan from needing to extend the formulary change effective date for those enrollees who present with a new prescription for the drug between the date when a Part D sponsor notifies CMS of a prospective change and the actual effective date of that change. However, Part D sponsors are still required to provide advance written notice of a formulary change and a 60 day-supply of the drug whose formulary status is changing to those beneficiaries who enroll in the plan after the initial advance formulary change notice, as described above. For non-maintenance changes outlined in section 30.3.3.3, the Part D sponsors must not implement the formulary change for a beneficiary who presents with a new prescription for a pending formulary drug. In accordance with our non-maintenance formulary change policy, enrollees currently taking the affected drug must be exempt from the formulary change for the remainder of the contract year. For example, assume on March 1st, a Part D sponsor notifies CMS via HPMS it is removing a drug from its formulary with no replacement. CMS approves the change. The sponsor indicates the effective date for this formulary change will be May 1st. If a beneficiary were to present on April 1st with a new prescription for the drug pending removal, the Part D sponsor would not implement this change for the beneficiary for the remainder of the contract year. 30.3.5 - Formulary Change Notice in Advance of Upcoming Contract Year (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Enrollees must receive an annual notice of change (ANOC) by October 31st prior to the upcoming contract year. The ANOC is intended to outline benefit changes for the upcoming year including changes in cost-sharing and drug tier structures. Because the upcoming year‟s formulary is viewed as a new formulary, Part D sponsors are not required to identify specific drug changes impacting enrollees in their explanation of benefits, or provide a 60-day notice of changes for the upcoming year‟s formulary. However, enrollees must receive a comprehensive or abridged formulary with the ANOC, which will provide enrollees with at least 60 days to review the new formulary to determine if their medications are covered and whether the costsharing for their covered medications will change in the upcoming contract year. 30.4 - Transition (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor must provide for an appropriate transition process for new enrollees prescribed Part D drugs that are not on its formulary. The transition policy must satisfy the requirements in the following sections. 30.4.1 - Transition Requirements (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor‟s transition process is necessary with respect to: (1) the transition of new enrollees into prescription drug plans following the annual coordinated election period; (2) the transition of newly eligible Medicare beneficiaries from other coverage; (3) the transition of individuals who switch from one plan to another after the start of the contract year; (4) enrollees residing in LTC facilities; and (5) in some cases, current enrollees affected by formulary changes from one contract year to the next. In addition, sponsors should consider how to expedite transitions to formulary drugs for enrollees who change treatment settings due to changes in level of care. Transition process requirements will be applicable to non-formulary drugs, meaning both: (1) Part D drugs that are not on a sponsor‟s formulary, and (2) Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a plan's utilization management rules, since a formulary drug whose access is restricted via utilization management requirements is essentially equivalent to a non-formulary Part D drug to the extent that the relevant utilization management requirements are not met for a particular enrollee. A Part D sponsor‟s transition process must address situations in which an individual first presents at a participating pharmacy with a prescription for a drug that is not on the formulary, unaware of what is covered by the plan or of the sponsor‟s exceptions process for providing access to Part D drugs that are not covered. This may be particularly true for full-benefit dual eligible beneficiaries who are auto-enrolled in a plan and do not make an affirmative choice based on review of a plan‟s benefit relative to their existing medication needs. Part D sponsors must have systems capabilities that allow them to provide a one time, temporary supply of nonformulary Part D drugs (including Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a sponsor‟s utilization management rules) in order to accommodate the immediate needs of an enrollee, as well as to allow the sponsor and/or the enrollee sufficient time to work out with the prescriber an appropriate switch to a therapeutically equivalent medication or the completion of an exception request to maintain coverage of an existing drug based on medical necessity reasons. 30.4.2 - General Transition Process (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Part D sponsors must ensure that they have provided their enrollees who have used a transition benefit with the appropriate assistance and information necessary to enable them to better understand the purpose of the transition. Steps that sponsors should consider to ensure a meaningful transition include: Analyzing claims data to determine which enrollees require information about their transition supply. Contacting those enrollees to ensure they have the necessary information to enable them to switch to a formulary product or as an alternative to pursue necessary prior authorizations or formulary exceptions. Increasing call center capacity, including pharmacy help lines, to respond to an anticipated increase in call volume from affected enrollees regarding the sponsor‟s transition process. Making arrangements to continue to provide necessary drugs to an enrollee by extending the transition period, on a case-by-case basis, if the enrollee‟s exception request or appeal has not been processed by the end of the minimum transition period. 30.4.3 - New Prescriptions Versus Ongoing Drug Therapy (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) CMS is aware that it may be difficult for Part D sponsors to distinguish between new prescriptions for non-formulary Part D drugs and refills for ongoing drug therapy involving nonformulary Part D drugs. For example, some new enrollees may need to switch pharmacies when they enroll in a new Part D plan (or when they enroll in Part D for the first time) and, depending on State law, their prescriptions may not transfer from pharmacy to pharmacy. In other words, some enrollees may need to present at their new network pharmacy with a new prescription for use at that pharmacy, even if that prescription is for ongoing drug therapy. CMS recognizes that it may be difficult for sponsors to distinguish between ongoing drug therapy and a brand-new prescription for a non-formulary Part D drug. Although Part D sponsors may attempt to follow up with prescribing physicians and pharmacies to ascertain the status of a prescription presented during the transition period, CMS clarifies that if a sponsor is unable to make this distinction at the point of sale, it will be required to apply all transition process standards to a new prescription for a non-formulary Part D drug. In other words, a brand-new prescription for a non-formulary drug will not be treated any differently than an ongoing prescription for a non-formulary drug when a distinction cannot be made at the point of sale. 30.4.4 - Transition Timeframes and Temporary Fills (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Within the first 90 days of coverage under a new plan, plans must provide a temporary fill when the beneficiary requests a refill of a non-formulary drug (including Part D drugs that are on a plan‟s formulary but require prior authorization or step therapy under a plan‟s utilization management rules). This 90 day timeframe applies to retail, home infusion, long-term care and mail-order pharmacies. CMS believes it makes sense to both limit and define the amount of time during which a transition process is applicable to new enrollees. Thus, plans will be required to provide a temporary supply fill anytime during the first 90 days of a beneficiary‟s enrollment in a plan. Since certain enrollees may join a plan at any time during the year, this requirement will apply beginning on an enrollee‟s first effective date of coverage, and not only to the first 90 days of the contract year. This 90 day timeframe assists those beneficiaries transitioning from other prescription drug coverage who obtained extended (e.g., 90-day) supplies of maintenance drugs prior to the last effective date of their previous coverage. 30.4.4.1 - Timeframe and Transition Fills in the Outpatient Setting (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) In the outpatient setting, the one-time, temporary supply of non-formulary Part D drugs – including Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a sponsor‟s utilization management rules – must be for at least 30 days of medication, unless the prescription is written by a prescriber for less than 30 days. Part D sponsors should note that, outside the long-term care setting, such a temporary fill may be a onetime fill only. 30.4.4.2 - Timeframe and Transition Fills in the Long Term Care Setting (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) The temporary supply of non-formulary Part D drugs – including Part D drugs that are on a Part D sponsor's formulary but require prior authorization or step therapy under a sponsor's utilization management rules – for a new enrollee in an LTC facility may be for up to 31 days (unless the prescription is written for less than 31 days). CMS is requiring up to a 31-day transition supply given that many LTC pharmacies and facilities dispense medications in 31-day increments. However, unlike in the outpatient setting, sponsors must honor multiple fills of non-formulary Part D drugs, including Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a sponsor‟s utilization management rules, as necessary during the entire length of the 90-day transition period. Beginning with contract year 2010, CMS is permitting Part D sponsors the option of sending required transition fill notices to network long term care pharmacies. In addition to sending enrollees residing in LTC facilities a model transition notice via U.S. mail within 3 business days of the transition fill, Part D sponsors may elect to send the beneficiary transition notice to the LTC pharmacy serving the beneficiary’s LTC facility. The LTC pharmacy must then ensure delivery of the notice to the beneficiary within 3 business days of the fill. Part D sponsors electing this option must update their existing transition policy to specifically address that: 1. The sponsor maintains documentation of the LTC pharmacies’ willingness to be delegated transition notice responsibilities; and 2. The sponsor maintains a fully functional electronic communication process with the LTC pharmacy once a transition fill has occurred (within 3 business days). 3. The LTC pharmacy will maintain a process that demonstrates notice has been provided to the beneficiary (or his/her representative) within the 3-day period. This option must be in place prior to the start of the 2010 contract year; otherwise, the Part D sponsor must continue to provide notice directly to the beneficiary (or his/her designated representative) via U.S. mail. 30.4.4.3 - Transition Extension (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor may need to make arrangements to continue to provide necessary drugs to an enrollee via an extension of the transition period, on a case-by-case basis, to the extent that his or her exception request or appeal has not been processed by the end of the minimum transition period. It is vital that sponsors give affected enrollees clear guidance regarding how to proceed after a temporary fill is provided, so that an appropriate and meaningful transition can be effectuated by the end of the transition period. Until that transition is actually made, however, either through a switch to an appropriate formulary drug, or a decision is made regarding an exception request, continuation of drug coverage is necessary, other than for drugs not covered under Part D. 30.4.5 - Transition Across Contract Years (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) After enrollees receive their ANOC on October 31st of a given year, CMS expects sponsors to select one of the following two options for effectuating an appropriate and meaningful transition for enrollees whose drugs are no longer on the formulary. These transition requirements apply both to drugs that are removed from a sponsor’s formulary from one contract year to the next, as well as to formulary drugs that remain on formulary but to which a new prior utilization or step therapy restriction is added from one contract year to the next: Provide a transition process for current enrollees consistent with the transition process required for new enrollees. In order to prevent coverage gaps, sponsors choosing this option are expected to provide a temporary supply of the requested prescription drug (where not medically contraindicated) and provide enrollees with notice that they must either switch to a drug on the sponsor‟s formulary or get an exception to continue taking the requested drug; or Effectuate a transition for current enrollees prior to the start of the new contract year. In effectuating this transition, sponsors must aggressively work to (1) prospectively transition current enrollees to a therapeutically equivalent formulary alternative; and (2) complete requests for formulary and tiering exceptions to the new formulary prior to the start of the contract year. If a sponsor approves such an exception request pursuant to chapter 18 of this manual, the sponsor shall authorize payment prior to January 1 of the new contract year. If, however, sponsors have not successfully transitioned affected enrollees to a therapeutically equivalent formulary alternative or processed an exception request by January 1 they will be expected to provide a transition supply beginning January 1 and until such time as they have effectuated a meaningful transition. Part D sponsors that can identify objective information demonstrating that a meaningful transition has occurred (such as the processing of an exception request and/or evidence of a new prescription claim for a formulary alternative processed in the month of December) do not have to provide access to a transition supply in the new contract year for that beneficiary. However, lacking such objective evidence, the sponsor is expected to provide a transition supply in the new contract year and provide the corresponding transition notice. Part D sponsors must extend their transition policies across contract years should a beneficiary enroll into a plan with an effective enrollment date of either November 1 or December 1 and need access to a transition supply. For example, if a beneficiary enrolls effective December 1, in a plan whose transition policy affords a 90-day transition period for LTC enrollees and that beneficiary requires a transition supply in mid-December, the sponsor must offer a full 90-day transition period beginning December 1 (including a one-time, 30-day transition supply) and extending into the following contract year. In addition, sponsors must send beneficiaries with a November 1 or December 1 effective enrollment date an ANOC as soon as practicable after the effective enrollment date. This ANOC will serve as advance notice of any formulary or benefit changes in the following contract year. 30.4.6 - Emergency Supply for Current Enrollees (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) Since, as a matter of general practice, LTC facility residents must receive their medications as ordered without delay, Part D sponsors must cover an emergency supply of non-formulary Part D drugs for LTC facility residents as part of their transition process. During the first 90 days after a beneficiary's enrollment, he or she will receive a transition supply. However, to the extent that an enrollee in an LTC setting is outside his or her 90-day transition period, the sponsor must still provide an emergency supply of non-formulary Part D drugs – including Part D drugs that are on a sponsor's formulary that would otherwise require prior authorization or step therapy under a sponsor's utilization management rules – while an exception or prior authorization is requested. These emergency supplies of non-formulary Part D drugs – including Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a sponsor‟s utilization management rules – must be for at least 31 days of medication, unless the prescription is written by a prescriber for less than 31 days. 30.4.7 - Level of Care Changes (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) In addition to circumstances impacting new enrollees who may enter a plan with a medication list that contains non-formulary Part D drugs, other circumstances exist in which unplanned transitions for current enrollees could arise and in which prescribed drug regimens may not be on sponsor formularies. These circumstances usually involve level of care changes in which a beneficiary is changing from one treatment setting to another. For example, beneficiaries who enter LTC facilities from hospitals are sometimes accompanied by a discharge list of medications from the hospital formulary with very short term planning taken into account (often under 8 hours). Similar situations may exist, for example, for beneficiaries who are discharged from a hospital to a home; for beneficiaries who end their skilled nursing facility Medicare Part A stay (where payments include all pharmacy charges) and who need to revert to their Part D plan formulary; for beneficiaries who give up hospice status to revert to standard Medicare Part A and B benefits; for beneficiaries who end an LTC facility stay and return to the community; and for beneficiaries who are discharged from psychiatric hospitals with drug regimens that are highly individualized. For these unplanned transitions, beneficiaries and providers must clearly avail themselves of sponsor exceptions and appeals processes. CMS has streamlined the grievance, coverage determination, and appeals process requirements in order to ensure that beneficiaries receive quick determinations regarding the medications they need. In all cases, CMS makes it clear that a Part D sponsor is required to make coverage determinations and redeterminations as expeditiously as the enrollee‟s health condition requires. Effective transition of care at time of discharge to home is a major concern in LTC. Ensuring appropriate medication reconciliation in the community is a safety issue, and requires predischarge planning. This optimally involves prescriptions being written and transmitted to the patients’ families in the week before discharge, to assure that the medications are obtained in advance of community discharge, to prevent a gap in care. The billing date may appear to overlap the skilled nursing home stay, but the medications, which may be dispensed by either the LTC or a retail pharmacy, are to be used in the home setting. While Part A does provide reimbursement for “a limited supply” to facilitate beneficiary discharge, beneficiaries must be permitted to have a full outpatient supply available to continue therapy once this limited supply is exhausted. This is particularly true for beneficiaries using mail-order pharmacy, home infusion therapy, or residing in rural areas where obtaining a continuing supply of drugs may involve certain delays. The current standard of care promotes caregivers receiving outpatient Part D prescriptions in advance of discharge from a Part A stay. When an enrollee is admitted to or discharged from an LTC facility, he or she will not have access to the remainder of the previously dispensed prescription (through no fault of his or her own) and, therefore, sponsors must allow the enrollee to access a refill upon admission or discharge. An early refill edit is a utilization management tool used to promote compliance and to prevent waste. An early refill edit cannot be used to limit appropriate and necessary access to an enrollee's Part D benefit. For example, if a patient gets a prescription for 30 tablets for a 30 day supply (i.e., 1 tablet daily), but the prescriber changes the dose to 2 tablets daily after only 10 days, it would be inappropriate for a sponsor to deny as "too soon" a claim for a new prescription with the new dosage because the enrollee will not have enough medication to last until the originally scheduled refill date. However, even with these protections, there may exist some period of time in which beneficiaries with level of care changes have a temporary gap in coverage while an exception is processed. For this reason, CMS strongly encourages Part D sponsors to incorporate processes in their transition plans that allow for transition supplies to be provided to current enrollees with level of care changes. 30.4.8 - Edits for Transition Fills (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor must ensure that a new enrollee is able to leave a pharmacy with a temporary supply of non-formulary Part D drugs without unnecessary delays. Part D sponsors may only apply certain drug utilization management edits during a beneficiary‟s transition period. Drug utilization management edits that are appropriate during a beneficiary‟s transition period include the following: Edits to help determine Part B vs. Part D coverage; Edits to prevent coverage of non-part D drugs (i.e., excluded drugs); and Edits to promote safe utilization of a Part D drug (e.g., quantity limits based on FDA maximum recommended daily dose; early refill edits). While Part D sponsors may implement step therapy or prior authorization edits during transition, they may do so only if such edits are resolved at the point of sale. For example, if a prescriber writes a prescription for 5mg tablets at 2 tablets daily, Part D sponsors might have dose optimization edits in place to require the prescription to be changed to 10mg tablets, 1 tablet daily. However, during transition, Part D sponsors would need to allow pharmacies to override this edit if the prescriber will not authorize the change at point of sale. In other words, the beneficiary should leave the pharmacy with sufficient quantity of medication (either 5mg or 10mg tablets) to last the plan allowable days supply, unless the prescriber originally wrote for a lesser days supply. If the dose optimization edit (or any other step therapy/prior authorization edit) is overridden at point of sale for transition purposes only, but not permanently, the beneficiary must be so notified so that he or she can begin the exception process if necessary. As part of their transition process submissions to CMS, sponsors should describe any edits on transition drugs and their process for resolving those edits at the point of sale. CMS notes that although Part D sponsors may implement quantity limits for safety purposes or drug utilization edits that are based on approved product labeling during a beneficiary‟s transition period, to the extent that the prescription is dispensed for less than the written amount due to a plan edit, sponsors must provide refills for that transition supply (at least a 30-day supply in an outpatient setting and a 31-day supply with multiple refills in an LTC setting). For example, if a beneficiary presents at a retail pharmacy with a prescription for 1 tablet per day for 30 days and a plan has a quantity limit edit in place that limits the days supply to 14 per prescription for safety purposes, the beneficiary would receive a 14-day supply (consistent with the safety edit). At the conclusion of the 14-day supply, the beneficiary should be entitled to another 14-day supply while he/she continues to pursue an exception with the Part D plan, or a switch to a therapeutic alternative that is on the plan‟s formulary. Irrespective of transition, all of these edits are subject to exceptions and appeals. For example, if a quantity limit edit (based on maximum recommended daily dose) results in the dispensing of a quantity that is less than indicated on the prescription and is less than the plan allowable days supply (as determined by the prescribed daily dose), Part D sponsors must ensure that beneficiaries are made aware of this quantity limit and that an exception is required to obtain a greater quantity. Part D sponsors must expeditiously process such exception requests so that beneficiaries will not experience unintended interruptions in medically necessary Part D drug therapies and/or will not inappropriately pay additional cost-sharing associated with multiple fills of lesser quantities when the originally prescribed doses of Part D drugs are medically necessary. A Part D sponsor does retain the authority to deny access to quantities or doses during transition (i.e., where clearly articulated safety limits established by the FDA or based upon the same peer reviewed medical literature or well-established clinical practice guidelines used by the P&T committee in formulary management have been exceeded). Prior to implementing such a denial, a Part D sponsor should ensure and track that both: (1) an initial transition supply has been provided up to the maximum limit, and (2) the sponsor has assisted the beneficiary or physician in filing an exception or that an exception has been processed. 30.4.9 - Cost-sharing Considerations (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor may charge cost-sharing for a temporary supply of drugs provided under its transition process. Cost-sharing for transition supplies for low-income subsidy (LIS) eligibles can never exceed the statutory maximum copayment amounts. For non-LIS enrollees, a sponsor must charge cost-sharing based on one of its approved drug cost-sharing tiers (if the sponsor has a tiered benefit design), and this cost-sharing must be consistent with cost-sharing that the sponsor would charge for non-formulary drugs approved under a coverage exception. 30.4.10 - Transition Notices (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A successful transition process is contingent upon informing enrollees and their caretakers about their options for ensuring that enrollees‟ medical needs are safely accommodated within a Part D sponsor‟s formulary. An enrollee who receives a temporary supply of a non-formulary Part D drug at a network pharmacy might simply assume that, by virtue of filling his or her prescription, that the plan will cover that drug for the remainder of a the contract year. For this reason, sponsors must provide enrollees with appropriate notice regarding their transition process within a reasonable amount of time after providing a temporary supply of non-formulary Part D drugs (including Part D drugs that are on a sponsor‟s formulary but require prior authorization or step therapy under a sponsor‟s utilization management rules). Part D sponsors will be required to send a written notice, via U.S. First Class mail, to each enrollee who receives a transition fill. This standard is consistent with CMS‟ requirement that other beneficiary communications, including formulary change notices and explanations of benefits, be sent via U.S. First Class mail. In addition, this notice must be sent to each affected enrollee within 3 business days of the temporary fill. CMS believes this turnaround is necessary in order to provide an affected enrollee with sufficient time -- especially in light of CMS‟ 30-day transition fill policy in the outpatient setting -- to work with his or her prescriber to switch to a therapeutically equivalent drug that is on the plan‟s formulary or to process an exceptions request. The notice must include the following elements: That the transition supply provided is temporary and may not be refilled unless a formulary exception is approved; That the enrollee should work with the sponsor as well as his or her health care provider to identify appropriate therapeutic alternatives that are on the sponsor‟s formulary and that will likely reduce his or her costs; That the member has the right to request a formulary exception, the timeframes for processing the exception, and the member's right to request an appeal if the sponsor issues an unfavorable decision; and The sponsor‟s procedures for requesting a formulary exception. CMS provides Part D sponsors with a model letter that they may submit to CMS under the file and use certification process. CMS expects that sponsors will make prior authorization or exception request forms available upon request to both enrollees and prescribing physicians and via a variety of mechanisms -- including by mail, fax, email, and on sponsor Web sites. To the extent that sponsors have the capacity, CMS encourages them to provide any prior authorization or exception request forms a beneficiary will need to effectuate a transition with the transition notice. In addition, CMS strongly encourages point-of-sale notification of enrollees about transition supplies by pharmacists. CMS has worked with the pharmacy and drug benefit industry, including the National Council for Prescription Drug Programs (NCPDP), to incorporate a workaround process for using structured payment coding in the message field of billing transaction responses indicating that a particular fill is a transition supply. This process is consistent with the current NCPDP 5.1 standard. For more information about Standardized Claims Messaging see chapter 14, section 50.5. 30.4.11 - Public Notice of Transition Process (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) As a general matter, CMS believes Part D sponsors must make general information about their transition processes available to beneficiaries in a manner similar to information provided on formularies and benefit design. It is likely that individuals will base their decision on which prescription drug best meets their needs on a variety of factors. Having information about a sponsor‟s transition process in plan enrollment materials and Web sites, as well as on the Medicare Prescription Drug Plan Finder, may reassure beneficiaries that there will be procedures in place to assist them in switching to therapeutic alternatives or in obtaining a formulary exception where appropriate. It will also serve to educate advocates and other interested third parties – for example, State Medicaid agencies – about sponsor transition processes. CMS will make plan transition process information available via a required link from the Medicare Prescription Drug Plan Finder to individual sponsor Web sites. 30.5 - Provider and Patient Education (Rev. 2, Issued: 07-18-08; Effective/Implementation Date: 07-18-08) A Part D sponsor must establish policies and procedures to educate and inform health care providers and enrollees concerning its formulary. See the marketing guidelines on CMS‟ Web site at http://www.cms.hhs.gov/PrescriptionDrugCovContra /07_RxContracting _Marketing.asp#TopOfPage for more information on acceptable formulary marketing methods. Chapter 6 - Appendix A Common Acute Care Home Infusion Drugs (This is a tool to assist plans in recognizing common Home Infusion drugs. It does not represent an exhaustive list of such drugs). 5-HYDROXYTRYPTAMINE 3 (5-HT3) ANTAGONISTS AMINO ACIDS AMINO DERIVATIVE PENICILLINS AMINOGLYCOSIDES AZOLE ANTIFUNGALS BETA-LACTAM, OTHER CEPHALOSPORIN ANTIBACTERIALS, 1ST GENERATION CEPHALOSPORIN ANTIBACTERIALS, 2ND GENERATION CEPHALOSPORIN ANTIBACTERIALS, 3RD GENERATION CEPHALOSPORIN ANTIBACTERIALS, 4TH GENERATION COLISTIMETHATE COLONY STIMULATING FACTORS DEXTROSE 10%/NACL 0.45% DEXTROSE 10% DEXTROSE 10% / NACL 0.2% DEXTROSE 2.5% DEXTROSE 2.5% / LACTATED RINGERS DEXTROSE 2.5% / NACL 0.45% DEXTROSE 5% DEXTROSE 5% / LACTATED RINGERS DEXTROSE 5%/NACL 0.2% DEXTROSE 5%/NACL 0.225% DEXTROSE 5%/NACL 0.33% DEXTROSE 5%/NACL 0.45% DEXTROSE 5%/NACL 0.9% TETRACYCLINES ECHINOCANDIN ANTIFUNGALS ELECTROLYTES ERYTHROPOIETINS EXTENDED SPECTRUM PENICILLINS GLUCOCORTICOIDS-SYSTEMIC GLYCOPEPTIDE ANTIBACTERIALS H1 BLOCKING AGENTS, SEDATING HEPARIN LACTATED RINGERS LINCOMYCIN ANTIBACTERIALS LIPIDS LOOP DIURETICS LOW MOLECULAR WEIGHT HEPARINS MACROLIDES MISCELLANEOUS ANTIBACTERIALS NATURAL PENICILLINS OPIOID ANALGESICS, LONG-ACTING OPIOID ANALGESICS, SHORT-ACTING OXAZOLIDINONE ANTIBACTERIALS PENICILLINASE-RESISTANT PENICILLINS POTASSIUM CHLORIDE PROTON PUMP INHIBITORS QUINOLONES SODIUM CHLORIDE SOLUTION SULFONAMIDES Chapter 6 – Appendix B Part D Drugs/Part D Supplementary Drugs This table provides Part D coverage clarifications for specific products/drugs/drug categories in accordance with statutory and regulatory requirements for Part D drugs. This is not an exhaustive list but only addresses those products/drugs/drug categories that have been the subject of frequently asked questions. Specific products not identified in this table should always be evaluated against the statutory and regulatory definition of a “Part D drug” before drawing conclusions from this table. This table does not address Part B versus Part D coverage questions. Product/Drug/Drug Category (Listing is NOT all-inclusive) May be covered under basic Part D benefit (when used for “medically accepted indication”3 and not covered under Medicare Parts A or B) Agents when used for anorexia, weight loss, or weight gain No Agents when used for cosmetic purposes or hair growth No Agents when used for symptomatic relief of cough and colds No 3 Comments Prescription drug products being used to treat AIDS wasting and cachexia are not considered agents used for weight gain or agents used for cosmetic purposes, and therefore such products are NOT excluded under such exclusion categories. Treatments indicated for psoriasis, acne, rosacea, or vitiligo are NOT considered cosmetic. Cough and cold medications are eligible to meet the definition of a Part D drug in clinically relevant situations other than those of symptomatic relief of cough and colds. For example, when cough medications are used for a medically accepted indication that treats a cough produced by a medical condition unrelated to symptomatic cough and cold, CMS does not consider these cough medications as excluded drugs [such as the treatment of cough to alleviate bronchospasm in asthma]. Medically Accepted Indication for purposes of Part D is an FDA labeled indication or an indication supported by citation in either the American Hospital Formulary System (AHFS), USP-DI (or its successor publications), or Drugdex. Product/Drug/Drug Category (Listing is NOT all-inclusive) Antihistamine/Decongestant Combinations (RX) Barbiturates Benzodiazepines Blood glucose testing strips May be covered under basic Part D benefit (when used for “medically accepted indication”3 and not covered under Medicare Parts A or B) Yes, except when being used for symptomatic relief of cough and cold No No No Electrolytes/Replenishers: *Potassium Sodium Calcium Magnesium Erectile (ED) Dysfunction Drugs Yes No Extemporaneous Compounds, including sterile compounding of IV‟s and total parenteral nutrition Fioricet® (Bultalbital, APAP, Yes, but only costs for Part D drug components may be billed under Part D No Comments NOT directly associated with injection of insulin *Potassium Iodide products are excluded from Part D as Iodine products (minerals) because they are not used for potassium supplementation. Agents when used for the treatment of sexual or erectile dysfunction, unless such agents are used to treat a condition, other than sexual or erectile dysfunction, for which the agents have been approved by the Food and Drug Administration. In addition, ED drugs will meet the definition of a Part D drug when prescribed for medically accepted indications approved by the FDA other than sexual or erectile dysfunction such as pulmonary hypertension. However, ED drugs will not meet the definition of a Part D drug when used off-label, even if the off label use is listed in one of the compendia found in section 1927(g)(1)(B)(i) of the Act. Dispensing fee may include labor costs associated with mixing a compounded drug product that contains at least one Part D drug component Part D drug components used solely as vehicles in a compound may be covered under Part D (e.g., D5W, Normal Saline) See Commercially Available Combination Product/Drug/Drug Category (Listing is NOT all-inclusive) May be covered under basic Part D benefit (when used for “medically accepted indication”3 and not covered under Medicare Parts A or B) Caffeine) Fioricet® with Codeine Yes Fiorinal® (Butalbital, ASA, Caffeine) No Fiorinal® with Codeine Yes Fosamax plus D Yes Heparin/Saline Flushes Injectable or IV Iron products such as Iron Dextran, Iron Sucrose and Sodium ferric gluconate Insulin No Yes Insulin syringes Yes IV Solutions for hydration therapy Klonopin® (Clonazepam) Lancets Less-than-effective DESI Drugs (and those drugs identical, related or similar) Leucovorin Calcium Librax® Comments Product Policy Section 10.3 See Commercially Available Combination Product Policy Section 10.3 See Commercially Available Combination Product Policy Section 10.3 See Commercially Available Combination Product Policy Section 10.3 See Commercially Available Combination Product Policy Section 10.3 See Section 10.6. Prescription vitamin/mineral product No Syringes are NOT covered for injection of other Part D drugs Yes No No Benzodiazepine NOT directly associated with injection of insulin See Section 10.9 No Yes No Limbitrol® (Amitriptyline/chlordiazepoxide) Yes Megestrol Acetate and Growth Hormone when used for AIDS Yes Less-than-effective DESI drug See Commercially Available Combination Product Policy Section 10.3 Prescription drug products that otherwise satisfy the definition of Part D drug are Product/Drug/Drug Category (Listing is NOT all-inclusive) May be covered under basic Part D benefit (when used for “medically accepted indication”3 and not covered under Medicare Parts A or B) wasting and cachexia Methadone Primidone (Mysoline®) Nonprescription/Over-thecounter (OTC) drugs 4 Omacor® Phenobarbital PhosLo® Polysaccharide Iron Complex 4 Yes, except when indicated for the treatment of opioid dependence Yes No, except insulin and supplies associated with the injection of insulin Yes No Yes No Comments Part D drugs when used for AIDS wasting and cachexia if these conditions are "medically accepted" indications, as defined by section 1927(k)(6) of the Social Security Act (SSA), for the particular Part D drug. Specifically, CMS does not consider such prescription drug products being used to treat AIDS wasting and cachexia as either agents used for weight gain or agents used for cosmetic purposes, and therefore such products cannot be excluded from the Medicare Prescription Drug Benefit by reference to section 1927(d)(2) of the SSA. A Part D drug is partially defined as “a drug that may be dispensed only upon a prescription”. . . . Consequently, Methadone is not a Part D drug when used for treatment of opioid dependence because it cannot be dispensed for this purpose upon a prescription at a retail pharmacy. NOT considered a barbiturate Supplies associated with the injection of insulin include syringes, alcohol wipes, insulin pens and pen needles, gauze, and alcohol Barbiturate Prescription vitamin/mineral product Part D plans may include OTC drugs in step therapy protocols as part of their cost effective drug utilization management program. However, OTC drugs included in these step therapy protocols are considered administrative costs, not Part D drugs. Product/Drug/Drug Category (Listing is NOT all-inclusive) Prescription niacin products May be covered under basic Part D benefit (when used for “medically accepted indication”3 and not covered under Medicare Parts A or B) Yes Comments Prescription niacin products are approved by the Food and Drug Administration as safe and effective drugs, are used therapeutically for the treatment of dyslipidemia, and do not serve as nutritional supplements or address a vitamin deficiency. These products are used at dosages much higher than appropriate for nutritional supplementation. For these reasons, CMS has concluded that these products should not be considered prescription vitamins for purposes of Part D coverage, and therefore, are not universally excluded from coverage under the Medicare prescription drug program. Prescription vitamins and mineral products, except prenatal vitamins and fluoride preparations Examples: B vitamins (Folic Acid, Cyanocobalamin) Vitamin K (phytonadione) Vitamin D (ergocalciferol and cholecalciferol) Zinc (sulfate, acetate) Iron Iodine Multivitamin additives for parenteral nutrition Smoking cessation drugs (OTC) Smoking cessation drugs (RX) Sterile Saline/water for Irrigation Suboxone®, Subutex® Vitamin D Analogs (Calcitriol, doxercalciferol, paricalcitol, and dihydrotachysterol) No No Yes Yes Yes NOT considered prescription vitamins Yes Chapter 6 – Appendix C - Summary of Coverage Policy MEDICARE PART B VERSUS PART D COVERAGE ISSUES This document is not a statement or promise of coverage, but rather a high level summary of when something may be covered under Parts A, B or D, if all other coverage requirements are met. Appropriate coverage policies and guidance must be consulted for final coverage determinations. Introduction This document provides an overview of outpatient prescription drug coverage policies under Medicare. Beneficiaries who are inpatients of hospitals or skilled nursing facilities (SNF) during covered stays may receive drugs as part of their treatment. Typically, the payment for drugs is bundled into the Medicare Part A payments made to these types of facilities.5 Under the hospice benefit, beneficiaries receive drugs that are medically necessary for symptom control or for pain relief. In general, references are seen to five major categories of Medicare Part B drug spending: 1. drugs billed by physicians and typically provided in physicians offices (such as chemotherapy drugs); 2. drugs billed by pharmacy suppliers and administered through durable medical equipment (DME), such as respiratory drugs given through a nebulizer; 3. drugs billed by pharmacy suppliers and self-administered by the patient (such as immunosuppressive drugs and some oral anti-cancer drugs); 4. separately billable drugs provided in hospital outpatient departments; and 5. separately billable End Stage Renal Disease (ESRD) drugs such as erythropoietin (EPO). Regional differences in Part B coverage policies for drugs can occur in the absence of a national coverage decision. A drug for which coverage is available under Part A or Part B, as it is being “prescribed and dispensed or administered” with respect to the individual, is excluded from the definition of a Part D drug and, therefore, cannot be included in Part D basic coverage. Medicare Part A and Part B Covered Drugs Part A/B Covered Drugs Set by Statute Traditional Medicare (Part A/B) does not cover most outpatient prescription drugs. Medicare bundled payments made to hospitals and skilled nursing facilities generally cover all drugs provided during a stay. Medicare also makes payments to physicians for drugs or biologicals that are not usually self-administered. This means that coverage is usually limited to drugs or biologicals administered by infusion or injection. However, if the injection is generally selfadministered (e.g., Imitrex), it is not covered. 5 If these drugs are provided as part of a Medicare Part A covered inpatient hospital or skilled nursing facility stay, they are generally bundled in the Medicare Part A payment to the facility. The exception with regard to inpatient hospital services is clotting factor which is paid separately. For covered SNF stays certain high cost chemotherapy drugs are billed separately along with preventive injections (e.g. flu shots). If a beneficiary does not have Part A coverage, if Part A coverage for the stay has run out or if a stay is non-covered, hospitals and SNFs can be paid for most categories of Part B covered drugs. Despite the general limitation on coverage for outpatient drugs under Part B, the law specifically authorizes coverage for the following: Durable Medical Equipment (DME) Supply Drugs. These are drugs that require administration by the use of a piece of covered DME (e.g., a nebulizer, external or implantable pump). The statute does not explicitly cover DME drugs; they are covered as a supply necessary for the DME to perform its function. The largest Medicare expenditures for drugs furnished as a DME supply are for inhalation drugs, which are administered in the home through the use of a nebulizer (e.g., albuterol sulfate, ipratropium bromide). The other category of drugs Medicare covers as a DME supply are drugs for which administration with an infusion pump in the home is medically necessary (e.g. some chemotherapeutic agents). Immunosuppressive Drugs. Drugs used in immunosuppressive therapy (such as cyclosporine) for a beneficiary who has received a Medicare covered organ transplant. Hemophilia clotting factors. Hemophilia clotting factors for hemophilia patients competent to use such factors to control bleeding without medical supervision, and items related to the administration of such factors. Oral Anti-Cancer Drugs. Drugs taken orally during cancer chemotherapy provided they have the same active ingredients and are used for the same indications as chemotherapy drugs that would be covered if they were not self-administered and were administered as incident to a physician‟s professional service. Oral Anti-emetic Drugs. Oral anti-nausea drugs used as part of an anti-cancer chemotherapeutic regimen as a full therapeutic replacement for an intravenous antiemetic drug within 48 hours of chemotherapy administration. Pneumococcal vaccine. The vaccine and its administration to a beneficiary if ordered by a physician. Hepatitis B vaccine. The vaccine and its administration to a beneficiary who is at high or intermediate risk of contracting hepatitis B.6 Influenza vaccine. The vaccine and its administration when furnished in compliance with any applicable state law. The beneficiary may receive the vaccine upon request without a physician‟s order and without physician supervision. 6 High risk groups currently identified include: individuals with ESRD; individuals with hemophilia who received Factor VIII or IX concentrates; clients of institutions for individuals for the mentally handicapped; persons who live in the same household as a hepatitis B Virus (HBV) carrier; homosexual men; illicit injectable drug abusers. Intermediate risk groups include: staff in institutions for the mentally handicapped and workers in health care professions who have frequent contact with blood or blood-derived body fluids during routine work. Antigens. These are prepared by a physician (usually an allergist) for a specific patient. The physician or physician‟s nurse generally administers them in the physician‟s office. In some cases the physician prepares antigens and furnishes them to a patient who has been taught to self-administer them at home. Erythropoietin (EPO). EPO for the treatment of anemia for persons with chronic renal failure who are on dialysis. Parenteral Nutrition. Parenteral nutrients are covered under the prosthetic benefit. They are available to beneficiaries who cannot absorb nutrition through their intestinal tract. Parenteral nutrition is administered intravenously and is regulated as a drug by the FDA. Intravenous Immune Globulin Provide in the Home. The Medicare Modernization Act created a benefit for the provision of intravenous immune globulin (IVIG) for beneficiaries with a diagnosis of primary immune deficiency disease. Coverage is provided if a physician determines that the administration of IVIG in the patient‟s home is medically appropriate. Payment is limited to that for the IVIG itself and does not cover items and services related to administration of the product. Part B Covered Drugs in the Context of a Professional Service Drugs furnished “Incident To” a Physician‟s Service. These are injectable or intravenous drugs that are administered predominantly by a physician or under a physician‟s direct supervision as “incident to” a physician‟s professional service. The statute limits coverage to drugs that are not usually self-administered.7 In order to meet all the general requirements for coverage under the “incident-to” provision, an FDA approved drug or biological must: Be of a form that is not usually self-administered (as determined by the A/B Contractor); Must be furnished by a physician; and Must be administered by the physician, or by auxiliary personnel employed by the physician and under the physician‟s personal supervision. The charge, if any, for the drug or biological must be included in the physician‟s bill and the cost of the drug or biological must represent an expense to the physician. Drugs and biologicals furnished by other health professionals may also meet these requirements. Drugs furnished by a Medicare Advantage Organization “Incident To” a Physician‟s Service. If a drug could be covered under Part B when furnished by a physician who incurred an expense in procuring the drug, it could also be covered under Part B in the case of a Medicare Advantage (MA) plan physician when the MA organization has incurred the expense of procuring the drug, and the drug is administered to an enrollee in the MA plan. Under Pub. 100-02, Medicare Benefit Policy Manual, chapter 15, section 60.1, drugs can be covered as “incident to” 7 If a drug is not self-administered by more than 50 percent of Medicare beneficiaries, it is considered “not usually self-administered”. physicians‟ services if they “represent an expense to the physician or legal entity billing for the services or supplies.” Applying this principle to the case of a not-usually self administered drug administered by an MA plan physician to an MA plan enrollee, if the MA organization supplies the drug to the plan physician, it is the “legal entity billing” for the drug, since it is the entity that receives payment from Medicare that includes the cost of such a drug. Consequently, if the MA organization supplies the drug to the network provider, the MA organization should account for the drug under its A/B benefits. If a network pharmacy supplies the drug directly to the beneficiary, the drug must be accounted for under its Part D benefits. Separately Billable ESRD Drugs. Most drugs furnished by dialysis facilities are separately billable. The largest Medicare expenditures for such drugs are for erythropoietin (EPO) which is covered for dialysis beneficiaries when it is furnished by independent and hospital-based ESRD facilities, as well as when it is furnished by physicians. Separately billable drugs provided in Hospital Outpatient Departments. Medicare continues to pay separately for drugs, biologicals and radiopharmaceuticals whose median cost per administration exceeds an amount (or threshold amount) determined by CMS, while packaging the cost of drugs, biologicals, and radiopharmaceuticals whose median cost per administration is less than an amount (or threshold amount) determined by CMS into the procedures with which they are billed. Drugs covered as Supplies or - “Integral to a Procedure.” Some drugs are covered as supplies that are an integral part of a procedure which is a diagnostic or therapeutic service, including radiopharmaceuticals (both diagnostic and therapeutic) and low osmolar contrast media. Other examples of drugs covered under the “integral to a procedure” provision include eye drops administered before cataract surgery. Blood. Medicare does make separate payment for blood and blood products and these products are regulated as biological agents by the FDA. Drugs furnished as a part of a service in these provider settings. 1. Drugs packaged under the Hospital Outpatient Prospective Payment System (OPPS); 2. Drugs furnished by ESRD facilities and included in Medicare‟s ESRD composite rate; 3. Osteoporosis drugs provided by home health agencies under certain conditions; 4. Drugs furnished by critical access hospitals‟ (CAH) outpatient departments; 5. Drugs furnished by a rural health clinic (RHC); 6. Drugs furnished by federally qualified health centers (FQHC); 7. Drugs furnished by community mental health centers (CMHC); 8. Drugs furnished by ambulances; 9. Separately billable drugs provided in comprehensive outpatient rehabilitation facilities (CORF). Part D Covered Drugs Definition of a Part D Covered Drug A Part D covered drug is available only by prescription, approved by the Food and Drug Administration (FDA) (or is a drug described under section 1927(k)(2)(A)(ii) or (iii) of the Act), used and sold in the United States, and used for a medically accepted indication (as defined in section 1927(k)(6) of the Act). A covered Part D drug includes prescription drugs, biological products, insulin as described in specified paragraphs of section 1927(k) of the Act, vaccines licensed under section 351 of the Public Health Service Act and for vaccine administration on or after January 1, 2008, its administration. The definition also includes medical supplies directly associated with delivering insulin to the body, including syringes, needles, alcohol swabs, gauze, and insulin injection delivery devices not otherwise covered under Medicare Part B, such as insulin pens, pen supplies, and needle-free syringes, can satisfy the definition of a Part D drug. CMS defines those medical supplies to include syringes, needles, alcohol swabs, gauze, and those supplies directly associated with delivering insulin into the body. Part D Supplementary (Excluded) Drugs The definition of a covered Part D drug excludes any drug for which as prescribed and dispensed or administered to an individual, payments would be available under Parts A or B of Medicare for that individual, even though a deductible may apply. In addition, the definition of a covered Part D drug specifically excludes drugs or classes of drugs, or their medical uses, which may be excluded from coverage or otherwise restricted under Medicaid under section 1927(d)(2) of the Act, with the exception of smoking cessation agents. The drugs or classes of drugs that may currently be otherwise restricted under Medicaid include: Agents when used for anorexia, weight loss, or weight gain (even if used for a noncosmetic purpose (i.e., morbid obesity)). Agents when used to promote fertility. Agents when used for cosmetic purposes or hair growth. Agents when used for the symptomatic relief of cough and colds. Prescription vitamins and mineral products, except prenatal vitamins and fluoride preparations. Nonprescription drugs. Covered outpatient drugs which the manufacturer seeks to require as a condition of sale that associated tests or monitoring services be purchased exclusively from the manufacturer or its designee. Barbiturates. Benzodiazepines. Agents when used for the treatment of sexual or erectile dysfunction (ED). ED drugs will meet the definition of a Part D drug when prescribed for medically-accepted indications approved by the FDA other than sexual or erectile dysfunction such as pulmonary hypertension. However, ED drugs will not meet the definition of a Part D drug when used off-label, even when the off label use is listed in one of the compendia found in section 1927(g)(1)(B)(i) of the Act: American Hospital Formulary Service Drug Information, United States Pharmacopeia-Drug Information (or its successor publications), and DRUGDEX Information System. ED drugs meet the definition of a Part D drug only when used for FDA-approved indications. While these drugs or uses are excluded from basic Part D coverage, Part D sponsors can generally include them as part of supplemental benefits, provided they otherwise meet the definition of a Part D drug. Because over-the-counter (OTC) drugs do not otherwise meet the definition of a Part D drug, they may not be included as part of supplemental benefits; however, under certain conditions as part of a plan utilization management program, OTC drugs can be provided at no cost to enrollees. The cost of these drugs to the Part D sponsor would be treated as administrative costs under such programs. Other Resources 1. Pub. 100-02, Medicare Benefit Policy Manual, Chapter 15. “Covered Medical and Other Health Services”. Section 110 2. Pub. 100-02, Medicare Benefit Policy Manual Chapter 15. “Covered Medical and Other Health Services” Section 50.2. 3. Reference Guide for Medicare Physician & Supplier Billers, Helping Front Office Personnel Navigate Medicare Rules for Part B Claims Processing. MedLearn Matters, Second Edition, October 2006. Chapter 6 – Appendix C - Summary of Coverage Policy ATTACHMENT I Part B Drugs and Part D Coverage Chart Drugs are covered under Part B in a variety of settings and under a variety of payment methodologies. Some drugs are paid on a cost basis or are part of a prospective payment, including: drugs packaged under the outpatient prospective payment system (OPPS); drugs furnished by End-Stage Renal Disease (ESRD) facilities and included in Medicare‟s ESRD composite rate; osteoporosis drugs provided by home health agencies under certain conditions; and drugs furnished by: critical access hospitals‟ outpatient departments (CAHs); rural health clinics (RHCs); federally qualified health centers (FQHCs); community mental health centers (CMHCs); and ambulances. In addition, there are 13 categories of drugs for which separate payment is made under Part B8, including: drugs furnished “incident to” a physician‟s service; separately billable ESRD drugs; separately billable drugs provided in hospital outpatient departments; durable medical equipment (DME) supply drugs; drugs covered as supplies; drugs used in immunosuppressive therapy; blood clotting factors; certain vaccines; antigens; parenteral nutrition; certain oral drugs used in cancer treatment; separately billable drugs provided in comprehensive outpatient rehabilitation facilities (CORFs); and intravenous immune globulin provide in the home.9 The following chart groups the various categories of Part B coverage according to the extent to which they present some ambiguity for billing entities and/or Part D sponsors with regard to whether coverage should be under Part B or Part D. This ambiguity has different implications for stand alone Part D sponsors and for Medicare Advantage-Prescription Drug (MA-PD) Plans (including PACE plans and Section 1876 Cost plans which are treated similarly to MA-PDs). For stand alone Part D sponsors, the sponsor needs to determine whether it should make any payment. For MA-PDs, the MA organization needs to determine whether a payment should be assigned to its Part D spending or to its spending for Part B services. 8 If these drugs are provided as part of a Medicare Part A covered inpatient hospital or skilled nursing facility stay, they are generally bundled into the Medicare Part A payment to the facility. The exception with regard to inpatient hospital services is clotting factor which is paid separately. For covered SNF stays certain high cost chemotherapy drugs are billed separately along with preventive injections (e.g., flu shots). If a beneficiary does not have Part A coverage, if Part A coverage for the stay has run out or if a stay is non-covered, hospitals and SNFs can be paid for most categories of Part B covered drugs. 9 Medicare does make separate payment for blood and blood products under Part A and Part B. Although these products are regulated as biologicals by FDA, they are not administered in a context that would not be covered under Part A or Part B. Therefore, generally these products are not Part D drugs. As a result, they are not included in this discussion. A. Situations in which a billing entity would have to decide whether for a given drug to bill Part B or Part D based on characteristics of beneficiary or medical use of the drug. Relationship between Part B and Part D Coverage 1. The same drug dispensed by a pharmacy may be covered under Part B or Part D depending on the characteristics of the beneficiary. 2. The same drug provided by an infusion/DME supplier may be covered under Part B or Part D depending on the characteristics of the beneficiary or method of administration. Categories of Separately Billable Part B Drugs Drugs used in immunosuppressive therapy for a transplant covered under Medicare. Comments Pharmacists would bill Part B or the individual‟s Part D plan based on information received from the individual or the Part D plan. Part B would be billed if the individual had a Medicarecovered transplant; otherwise, the Part D plan would be billed. (Part D plan eligibility systems could contain a marker for members who had a Medicare covered transplant. This information could come from a question included on the Part D sponsor‟s enrollment or coordination of benefit (COB) survey form.) In determining whether to pay for an immunosuppressive drug under Part D, it would not be appropriate for a Part D sponsor to institute a general policy of requiring a Part B claim rejection, as a substitute for maintaining information on transplant status and paying claims based on that information. Such a policy would be disruptive to beneficiaries and pharmacies and would unnecessarily increase Part B contractor costs. Instead a prior authorization requirement would be appropriate. The supplier would need to know whether the therapy was being provided because of a non-functioning digestive tract. If so, Part B would be billed. Otherwise this would be a Part D drug. a. Parenteral nutrition or intradialytic parenteral nutrition (IDPN) (for individuals with a nonfunctioning digestive tract). It would not be appropriate for Part D sponsors to routinely require a rejection of a claim under Part B before processing a Part D claim. Such a policy would be disruptive to beneficiaries and pharmacies and would unnecessarily increase Part B contractor costs. However, if a Part D sponsor had evidence b. Infusible DME supply drugs indicating that a particular claim for parenteral nutrition should be covered under Part B, it would be reasonable to require a rejection by Part B before processing in this case. In general, the supplier would bill Part B if the drug was administered using an infusion pump and bill the Part D plan for infusion using other methods (e.g., IV push). While professional services and supplies related to the administration of the infused drug are not payable under Part D, some coverage may be available under Part A or B home health benefits, under Medicaid, or from secondary commercial health benefits. As a rule, drugs infused using an implantable pump would be covered under Part B. Drugs infused in the home using an external pump are covered under Part B if they are included under the local coverage policy of the applicable Medicare DME MAC. In the case of a beneficiary in a hospital, or a SNF bed, (1) who does not have Part A coverage, (2) whose Part A coverage for the stay has run out or (3) whose stay is noncovered -- infusible DME supply drugs are not covered under Part B because the law limits coverage under Part B‟s DME benefit to those items that are furnished for use in a patient‟s home, and specifies that a hospital or SNF cannot be considered the beneficiary‟s “home” for this purpose. In this case, coverage for the drugs would be available under Part D. (see Attachment II, INFUSION DRUGS, Question 3 for other facilities which cannot be considered a beneficiary‟s “home” for DME purposes.) The fact that coverage is available for a particular drug under Part B with the use of an infusion pump does not mean that coverage under Part D using some other method of administration automatically can be denied. There is no Part B coverage in the home for infusion drugs administered without an c. Intravenous immune globulin (IVIG) provided in the home for individual with diagnosis of primary immune deficiency disease 3. The same drug dispensed by a pharmacy may be covered under Part B or Part D depending on how the drug is used in treatment and the medical condition for which the drug is being prescribed. a. Certain oral chemotherapy agents used in cancer treatment for which there is an infusible version of the drug. infusion pump (e.g., IV push). There is also no Part B coverage in the home for infusion drugs administered with an infusion pump unless the drug is specifically covered under the local coverage policy of the applicable Medicare DME MAC. Therefore, determinations about Part D sponsor payment for these other methods of administration and for drugs administered with an infusion pump but not covered by the local DME MAC policy should be based on the question of whether the drug is on the sponsor‟s formulary. The supplier would bill Part B if the diagnosis is primary immune deficiency disease. IVIG provided in the home for other diagnoses would be a Part D benefit. As discussed above, it would not be appropriate, as a general rule, for Part D sponsors to require a rejection of a claim under Part B before processing a Part D claim. Prior authorization programs could be used to ensure medical necessity in accordance with the Part D sponsor‟s policy. Pharmacists would need to determine the reason for treatment. If related to cancer treatment, Part B would be billed; otherwise, the Part D plan should be billed. To the extent that a Part B-covered oral anti-cancer drug has no other medically accepted indication besides cancer treatment, Part D sponsors should not include these drugs on their formularies because of Part B coverage. For the drugs that have other medically accepted indications, prior authorization programs or other mechanisms to obtain diagnostic information could be used to ensure appropriate payment. b. Oral anti-emetics used in 2. Pharmacists would need to determine the reason for treatment. cancer treatment as a full If both related to cancer treatment and a full replacement for replacement for intravenous administration within 48 hours of cancer treatment, intravenous treatment. Part B would be billed; otherwise, the Part D plan should be billed. NOTE: In order to receive Part B payment, CMS currently requires that the prescribing physician indicate on the prescription that the oral anti-emetic is being used “as a full therapeutic replacement for an intravenous anti-emetic drug as part of a cancer chemotherapeutic regimen.” 4) The same vaccine may be covered under Part B or Part D depending on the characteristics of the beneficiary. Hepatitis B vaccine for individuals at high or intermediate risk. If based on a prior authorization program or other mechanism to obtain diagnostic information, a Part D sponsor determined that a) a Part B-covered oral anti-emetic was being billed, and b) the drug was being furnished in the context of cancer treatment for use within 48 hours of cancer treatment, the Part D sponsor should deny payment. Such drugs dispensed for use after the 48-hour period, or any oral anti-emetic prescribed for conditions other than the effects of cancer treatment, would be Part D drugs. Physicians would need to determine the level of risk of the individual. If the individual is at high or intermediate risk, Part B would be billed. For all other individuals, prior authorization programs could be used to ensure appropriate level of risk. B. Situation where the form of the drug determines where it is covered. Relationship between Part B and Part D Coverage The same drug provided by a DME supplier or a pharmacy may be covered under Part B or Part D depending on its form (i.e., for use in nebulizer or in metered dose inhaler) Categories of Separately Billable Part B Drugs Inhalation DME supply drugs Comments Certain inhalation drugs are generally covered under Part B when used with a nebulizer in the home. These drugs would not be covered under Part D for use with a nebulizer. However, if these drugs were delivered with a metered dose inhaler or other non-nebulized administration, they would be Part D drugs. In the case of a beneficiary in a hospital, or a SNF bed, (1) who does not have Part A coverage, (2) whose Part A coverage for the stay has run out or (3) whose stay is non-covered -- inhalation DME supply drugs are not covered under Part B because the law limits coverage under Part B‟s DME benefit to those items that are furnished for use in a patient‟s home, and specifies that a hospital or SNF cannot be considered the beneficiary‟s “home” for this purpose. In this case, coverage for the drugs would be available under Part D. (See Attachment II, INFUSION DRUGS, Question 3 for other facilities which cannot be considered a beneficiary‟s “home” for DME purposes.) C. Situations where Part B coverage is in the context of another service. Relationship between Part B and Part D Coverage The same drug dispensed by a pharmacy is covered under Part B if provided as part of a service in a provider setting, physician‟s office or home. Categories of Separately Billable Part B Drugs 1. Drugs furnished “incident to” a physician service 2. Separately billable ESRD drugs 3. Separately billable drugs in HOPDs 4. Separately billable drugs in CORFs 5. Drugs packaged under the OPPS 6. Drugs furnished by ESRD facilities and included in Medicare‟s ESRD composite rate 7. Osteoporosis drugs provided by home health agencies under certain conditions Comments Generally, if a beneficiary presents at a pharmacy with a script it would be a Part D drug. The availability of Part B coverage in a provider setting or physician‟s office should not result in a refusal of coverage under Part D for drugs dispensed by a pharmacy. This is the case because coverage is not available under Part B as the drug is being “prescribed and dispensed or administered” with respect to the individual. Thus, for example, while Part B covers certain injectables provided “incident to” a physician services, injectables dispensed by a pharmacy are not being “furnished” by a physician and would be Part D drugs. Part D sponsors should deny claims submitted by members for Part B-covered injectables if they are administered in a physician office from a physician‟s supply. Part D sponsors can subject injectables and infusables that would be covered under Part B as “incident to” a physician service, to a prior authorization program. To the extent that the sponsor determines based on medical literature that there exist serious 8. Drugs furnished by CAHs outpatient departments 9. Drugs furnished by RHCs 10. Drugs furnished by FQHCs 11. Drugs furnished by CMHCs 12. Drugs furnished by ambulances. safety concerns such that it would go against accepted medical practice for a particular injectable or infusable to be dispensed directly to an enrollee, the claim can be denied as not "reasonable." Safety-based reasonableness determinations will need to be made on a case-by-case basis, since circumstances will vary. In general, however, there are very few instances when an injectable or infusable drug could not be reasonably dispensed directly to the patient. D. Completely unambiguous situations. Relationship between Part B and Part D Coverage 1) Unique drugs never dispensed by a pharmacy. Categories of Separately Billable Part B Drugs Non-DME drugs covered as supplies (including radiopharmaceuticals (both diagnostic and therapeutic) and low osmolar contrast media.) Comments 2) Drugs that would not be covered under Part D because of Part B coverage. 1. Blood clotting factors 2. Antigens Pneumococcal and influenza vaccines These categories would not be a Part D benefit and should not be included on a Part D sponsor‟s formulary. This category of drugs is those used for diagnostic or therapeutic purposes in a provider or physician office setting. CMS would assume that these drugs are not dispensed by pharmacies. Chapter 6 – Appendix C - Summary of Coverage Policy ATTACHMENT II Part B v. Part D Drug Q’s and A’s EXCLUSIONS RELATED TO MEDICARE COVERAGE UNDER PART A OR PART B Question 1 – Should Part D sponsors deny claims for drugs covered under Part A or Part B of Medicare? Answer 1 – Drugs, or uses of drugs, for which coverage is available under Part A or Part B are excluded from the definition of a Part D drug and, therefore, cannot be included in Part D basic coverage. Unlike the list of supplementary drugs, these drugs, or uses of drugs, cannot be included in supplemental coverage. There are two important considerations in determining whether a claim to Part D can be denied based on the availability of coverage under Part A or Part B of Medicare. First, the exclusion from the definition of a Part D drug for drugs covered under Parts A or B is based on whether coverage is available under Part A or Part B for the drug as it is being “prescribed and dispensed or administered” with respect to the individual. Thus, the same drug may be covered under different circumstances under both programs and coverage generally cannot be determined based solely on the drug itself. Since most Part B drug coverage is available in a provider setting or physician‟s office rather than as drugs dispensed by pharmacists, there are very limited situations when a drug claim submitted by a pharmacy should be denied based on the availability of coverage under Part A or Part B. Second, to the extent a drug could be covered under part B as prescribed and dispensed or administered, Part D sponsors should view coverage as “available” under Part B regardless of whether or not an individual is actually enrolled in Part B. Question 2 – Can a Part D sponsor require that coverage be denied under Part A or Part B before making payment under Part D? Answer 2 – Generally, no. In limited instances, prior authorization programs may be necessary to determine whether the diagnosis of the individual or the particular use of a drug is consistent with Part D coverage, but it would not be appropriate to routinely require a denial from Part A or Part B before making payment in lieu of prior authorization. Such a policy would be disruptive to beneficiaries and pharmacies and would unnecessarily increase Part B contractor costs. Question 3 - What happens if a Part D sponsor makes payment for a drug and later determines that the drug was covered under Part B as prescribed and dispensed or administered? Answer 3 - If the drug as prescribed and dispensed or administered was covered under Part B on that day, the payment by the Part D sponsor would have been in error and it should seek recovery from the billing entity, which should bill Part B instead. Question 4 - In the case of a newly approved drug that may be covered under one of the Part B benefit categories, can a Part D sponsor defer a coverage decision until Part B makes a decision? Answer 4 - No. Once a drug is approved by the FDA it is a Part D drug. While it is not automatically a covered Part D drug, that is, it may not be included on a Part D sponsor‟s formulary, a member could request coverage on an exception basis. For Medicare Part B coverage, a determination has to be made as to whether the approved drug fits in a benefit category (e.g., a drug covered as a supply of an external infusion pump used at home). In the vast majority of cases these determinations are delegated to the individual contractors. If a drug has a Medicare Part B benefit category and the drug is being “prescribed and dispensed or administered” as covered under Part B, the drug is no longer a Part D drug. Question 5 - How will Part D sponsors determine whether a drug is covered under Part B? Answer 5 - First, it is important to keep in mind that in most cases Part B drug coverage should not impact payment decisions by Part D sponsors since Part B coverage is generally in a provider setting or physician's office rather than for drugs dispensed at a pharmacy. Payment for a particular drug can be denied only if there is Part B coverage as the drug is prescribed and dispensed or administered. The fact that a claim is received for a drug that is sometimes covered by Part B is not a basis for denial since the Part D sponsor would have to determine whether the drug is being prescribed and dispensed or administered on the basis under which Part B coverage is available. This will generally involve interaction between the Part D sponsor and the Medicare Part B contractor with jurisdiction in that geographic area for that drug. With regard to new drugs, as decisions are made nationally or by individual A/B contractors, this information will be available on the CMS and contractor Web sites. INFUSION DRUGS Question 1 - Since Part B covers infusion drugs in the home, can a Part D sponsor reject any claim for home infusion? Answer 1 – No. Part B coverage is generally limited to a number of drugs that require the use of an infusion pump in the home. Any agents administered in the home via IV drip or push injection would be covered under Part D. This could include the same drugs that are covered under Part B when furnished through the use of an infusion pump. Question 2 – Does Part B cover drugs that require an external infusion pump in the case of a beneficiary in a hospital or SNF bed who does not have Part A coverage, whose Part A coverage for the stay has run out or whose stay is non-covered? Answer 2 – No, drugs that require an external infusion pump are not covered under Part B under those circumstances because the law limits coverage under Part B‟s DME benefit to those items that are furnished for use in a patient‟s home, and specifies that a hospital or SNF cannot be considered the beneficiary‟s “home” for this purpose. Question 3 - What other facilities cannot be considered the beneficiary’s “home” under the law for purposes of receiving the Medicare DME benefit? Answer 3 – In addition to a hospital, a SNF or a distinct part SNF, the following facilities cannot be considered a home for purposes of receiving the Medicare DME benefit: a nursing home that is dually-certified as both a Medicare SNF and a Medicaid nursing facility (NF); a Medicaid-only NF that primarily furnishes skilled care; a non-participating nursing home (i.e., neither Medicare or Medicaid) that provides primarily skilled care; and an institution which has a distinct part SNF and which also primarily furnishes skilled care. Question 4 - If the infusion services are furnished in an outpatient provider setting, can a Part D sponsor deny a claim? Answer 4 – Yes. If a physician office or hospital outpatient department bill for infusion administered in those settings, the claim should always be denied because of coverage in those settings under Part B. Question 5 – Since Part B covers intravenous immune globulin (IVIG) provided in the home, should a Part D sponsor deny claims for this drug? Answer 5 – It depends. Part B coverage for IVIG in the home is for individuals whose diagnosis is primary immune deficiency disease. Part D would provide coverage for IVIG in the home for all other medically accepted indications. Prior authorization requirements could be used to ensure appropriate payment in accordance with the Part D sponsor‟s medical necessity criteria. It would not be appropriate to routinely require a rejection of a claim under Part B before processing a Part D claim. Such a policy would be disruptive to beneficiaries and pharmacies and would unnecessarily increase Part B contractor costs. Question 6 – Since Part B covers parenteral nutrition under certain circumstances, should Part D sponsors deny these claims? Answer 6 – It depends. Part B coverage for parenteral nutrition is limited to individuals with a non-functioning digestive tract. So if parenteral nutrition is being provided based on this condition, the claim should be denied. For all other medically accepted indications, coverage would be under Part D. Prior authorization programs could be used to ensure appropriate payment. As a general policy, it would not be appropriate to require a rejection of a claim under Part B before processing a Part D claim. However, if a Part D sponsor had a reasonable basis for assuming that a particular claim would be covered under Part B, it could require a rejection by Part B before processing. ORAL ANTI-CANCER DRUGS Question 1 - With regard to oral anti-neoplastics, we understand that if they have an IV form, they are covered under Part B. It is our thinking then, that we could exclude those that are used solely for cancer under this premise since they would be covered under Part B. Answer 1 – Yes. Part D sponsors should not include on their formularies the oral anti-cancer agents covered by Part B whose only medically accepted indication is as an anti-cancer agent. They should always deny claims for these drugs. For the drugs that have other medically accepted indications, Part D sponsors should deny claims for these drugs when used for cancer treatment but when these drugs are used for other indications they would be Part D drugs. The use of the drug could be determined through a prior authorization program. ORAL ANTI-EMETICS Question 1 - Do pharmacies bill oral anti-emetics under Part B or Part D? Answer 1 - It depends. Before billing either Part B or Part D, pharmacists would need to determine the reason for treatment. If it is related to cancer treatment and is a full replacement for intravenous administration within 48 hours of cancer treatment, Part B would be billed; otherwise, Part D should be billed.10 In order to receive Part B payment, CMS currently requires that the prescribing physician indicate on the prescription that the oral anti-emetic is being used “as a full therapeutic replacement for an intravenous anti-emetic drug as part of a cancer chemotherapeutic regimen.” If (based on a prior authorization program) a Part D sponsor determines that a Part B-covered oral anti-emetic drug is being billed, and that the drug is being furnished in the context of cancer treatment for use within 48 hours of such treatment, the Part D sponsor should deny payment since coverage is available under Part B. Such drugs dispensed for use after the 48-hour period, or any oral anti-emetic prescribed for conditions other than treatment of the effects of cancer treatment, would be Part D drugs. IMMUNOSUPPRESSANTS Question 1 - Do pharmacies bill oral immunosuppressants under Part B or Part D? 10 There may be some local A/B contractor variance regarding the 48 hour interval for the oral anti-emetics granisetron and dolasetron. Part D sponsors should contact their local A/B contractor for more information regarding these drugs. Answer 1 - It depends. Pharmacists would bill Part B or the individual‟s Part D plan based on information received from the individual or sources substantiating the patient‟s transplant. Part B would be billed if the individual had a Medicare covered transplant; otherwise, the Part D plan would be billed. INJECTABLES Question 1 - Can claims submitted by pharmacies for injectable drugs be denied based on Part B coverage in a physician office “incident to” a physician service? Answer 1 – No. The exclusion from the definition of a Part D drug of drugs covered under Parts A or B is based on whether coverage is available under Part A or Part B for the drug as it is being “prescribed and dispensed or administered” with respect to the individual. Thus, the same drug may be covered under different circumstances under both programs. As a result, coverage cannot generally be determined based solely on the drug itself. The fact that an injectable is covered under Part B in a physician‟s office or hospital outpatient department or other provider setting does not mean that these drugs should be excluded from the Part D sponsor‟s formularies, or that a Part D sponsor can deny a claim from a pharmacy based on availability of Part B coverage in a physician‟s office. If, however, a member submits an outof-network claim for an injectable drug administered in-office from a physician‟s supply, and this drug is covered in that setting by the Part B contractor for that area, such a claim should be denied by the Part D sponsor based on Part B coverage. (Of course, an MA-PD plan would not deny such a claim, but rather pay it under the A/B benefit.) Question 2 - An injectable drug that a Medicare contractor considers to be usually not selfadministrable (e.g., injectable chemotherapy drugs) can only be covered under Part B as “incident to” a physician service if it is obtained by a physician and administered as part of a physician service. Can Part D sponsors require prior authorization for these medications when dispensed by a pharmacy? If the sponsor determines that the drug will be administered in a physician office, can the sponsor deny the claim because the practice of the patient taking the drug to the physician’s office for administration is unsafe and because coverage is available under Part B if the physician obtained and administered the drug? Answer 2 - Part D sponsors determine the scope of their own prior authorization programs subject to CMS review to ensure that such programs have a sound medical basis and do not discriminate against beneficiaries with certain medical conditions. To the extent that a sponsor‟s prior authorization program applies to injectables and infusables that would be covered under Part B as “incident to” a physician‟s service, and the sponsor determines based on medical literature that there exist serious safety concerns such that it would go against accepted medical practice for a particular injectable or infusable to be dispensed directly to a member, the claim can be denied as not "reasonable." Thus, the dispensing of that particular drug to that member may be excluded by the Part D sponsor under Section 1862(a)(1)(A) of the Social Security Act as applied to Part D under 1860D-2(e)(3)(A) of the Act. This same safety concern would not exist, however, if the claim for the drug was being submitted by an infusion supplier. Safety-based reasonableness determinations will need to be made on a case-by-case basis, since circumstances will vary. In general, there are very few instances when an injectable or infusable drug could not be reasonably dispensed directly to the patient. All drugs are in some sense hazardous. This is not a unique characteristic of injectables and infusables. Some situations that would present safety concerns in dispensing directly to a patient who is transporting the drug to a physician‟s office for administration include: The drug itself presents a bona fide public safety hazard (e.g., highly radioactive substance or an environmentally hazardous chemotherapeutic agent) that requires chain of custody handling to ensure use of appropriate equipment (i.e., safety hood) or persons of special qualifications. The drug requires special handling to preserve biologic activity and the patient is incapable or unwilling to do so. (For instance, a vaccine that must be kept frozen could be a problem if the patient had to transport it a long distance in summer heat.) The patient presents a high risk of diversion or inappropriate use. (For instance, giving a heroin addict a vial of morphine.) The patient has demonstrated unreliability, aversion, or unwillingness in transporting drugs to his doctor‟s office. (For instance, with respect to dispensing injectable psychiatric meds.) In the absence of a serious safety concern based on the individual situation, however, there is no basis for denying a prescription presented at a pharmacy based on the availability of Part B coverage in another setting (e.g., physician office). Finally, it is CMS‟ understanding that the practice of “brown-bagging” drugs is opposed by medical societies. CMS continues to urge them to reinforce this message with their members. Question 3 – Most Medicare Advantage plans treat most non-self-injectables as a medical benefit. Do they have to treat them as a Part D benefit? Answer 3 - If an injectable drug is covered under Part B in a provider or physician office setting, it will continue to be covered under Part B in those settings. If an injectable drug is not covered in a provider setting (e.g., determined by the contractor to be usually self-administered), then it will need to be covered under Part D. In addition, claims for non-Part-B-covered injectables whether usually self-administered or not, when dispensed and submitted by pharmacists could be covered under Part D. However, Part D plans could establish medical necessity criteria for limiting coverage of injectable drugs in physician offices. Question 4 - What are Part D sponsors to do if their region includes multiple A/B contractor areas and these contractors have differing policies with regard to injectable drugs? Answer 4 – A Part D sponsor will have to modify its coverage based on the variation in Part B coverage across contractor areas within its region. That is, assume that there are two contractor areas within a Part D sponsor‟s region, Contractor A and Contractor B. Further assume that Contractor A covers injectable X when furnished in a physician office but Contractor B does not. As a result of this difference in Part B coverage, injectable X is a Part D drug when furnished in a physician office for members residing in Contractor B‟s area, but not in Contractor A‟s area. In either area, injectable X would be covered under Part D if dispensed by a pharmacy. For MA-PD plans, rules for selecting local coverage determinations apply. That is, if a local MA plan‟s service area includes more than one contractor area, the plan may seek approval from CMS to apply uniformly to all of the plan‟s enrollees local coverage policies that are the most beneficial to enrollees. Regional MA plans can select a set of local coverage policies to apply uniformly to their enrollees without CMS pre-approval. In either case, if the selected contractor covers injectable X, the MA-PD would treat injectable X as a basic A/B benefit. If the selected contractor does not cover injectable X, the MA-PD would treat it as a Part D drug. Question 5 –What about new injectable drugs? Answer 5 - As new injectables are approved by FDA, Part B contractors or CMS would continue to make coverage decisions regarding drugs provided incident to a physician‟s service based on whether the drug is “not usually self-administered.” Injectables not covered under Part B as incident to a physician‟s service would become Part D drugs. However, there is no requirement for Part D sponsors to provide coverage of non-Part-B-covered drugs in the physician office setting if the drugs can be safely self-administered and there is no medical necessity for administration in that setting. INHALATION DRUGS Question 1 - Can claims submitted by a pharmacy for inhalation drugs delivered through metered-dose inhalers be denied based on Part B coverage of inhalation drugs used with a nebulizer? Answer 1– No. Since there currently is no coverage under Part B for inhalation drugs delivered through metered-dose inhalers and dispensed by a pharmacy, these drugs would be covered under Part D. Question 2 – Does Part B cover inhalation drugs used with a nebulizer in the case of a beneficiary in a hospital or SNF bed who does not have Part A coverage, whose Part A coverage for the stay has run out or whose stay is non-covered? Answer 2 – No, inhalation drugs used with a nebulizer are not covered under Part B under those circumstances because the law limits coverage under Part B‟s DME benefit to those items that are furnished for use in a patient‟s home, and specifies that a hospital or SNF cannot be considered the beneficiary‟s “home” for this purpose. (See list above (INFUSION DRUGS, Question 3) for other facilities which cannot be considered a beneficiary‟s “home” for DME purposes. VACCINES Question 1 – Are all vaccines be covered under Part D? Answer 1 – No. There are a number of vaccines that remain covered under Part B. For instance, pneumococcal and influenza vaccines are not covered under Part D because of Part B coverage. Hepatitis B vaccine is covered under Part B for individuals at high or intermediate risk; for all other individuals, it would be covered under a Part D benefit. Part B also covers certain vaccines reasonable and necessary for the treatment of an illness or injury. All other currently available vaccines and all future preventative vaccines could be covered under Part D. Question 2- If a Part D sponsor determines through a prior authorization program that a hepatitis B vaccine is going to be administered by a physician can the Part D sponsor deny the claim based on Part B coverage in the setting? Answer 2 – No. Since the Part B benefit for hepatitis B vaccine is separate from the “incident to” benefit, the determination about whether it is a Part D drug depends solely on characteristics of the beneficiary. However, if the Part D sponsor determines based on Medicare Part B guidelines that the individual is at high or medium risk for hepatitis B, the claim should be denied. For all other individuals, the vaccine would be a “Part D drug”. Question 3 - Medicare Part B covers hepatitis B vaccine for high and intermediate risk groups if ordered by a doctor of medicine or osteopathy, how are these groups defined? Answer 3 – The high risk groups for whom vaccination is covered include: • • • • • • Individuals with End stage renal disease (ESRD); Individuals with hemophilia who received Factor VIII or IX concentrates; Clients of institutions for individuals for the mentally handicapped; Persons who live in the same household as a hepatitis B Virus (HBV) carrier; Homosexual men; and Illicit injectable drug abusers Intermediate risk groups include: • • Staff in institutions for the mentally handicapped; and Workers in health care professions who have frequent contact with blood or bloodderived body fluids during routine work. ANTIGENS Question 1 – If a pharmacy submits a claim for antigens should a Part D sponsor make payment? Answer 1 – No. Antigens are covered only under Part B. BLOOD CLOTTING FACTORS Question 1 – If a pharmacy submits a claim for blood clotting factors should a Part D sponsor make payment? Answer 1 – No. Blood clotting factors are covered under Part A and Part B. Chapter 6 – Appendix C - Summary of Coverage Policy ATTACHMENT III Web sites for Part B Coverage Information Pub. 100-04, Medicare Claims Processing Manual http://www.cms.hhs.gov/Manuals/IOM/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=1&sortOrder=ascending&itemID=CMS018912&intNumPerPage=10 Pub. 100-02, Medicare Benefit Policy Manual http://www.cms.hhs.gov/Manuals/IOM/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=1&sortOrder=ascending&itemID=CMS012673&intNumPerPage=10 Medicare Coverage Database http://www.cms.hhs.gov/mcd/search.asp AB MAC and DME MAC contact information http://www.cms.hhs.gov/apps/contacts/ Chapter 6 - Appendix D (Rev. 10, Issued: 02-19-10, Effective/Implementation Date: 03-01-10) The Most Commonly Prescribed Drug Classes for the Medicare Population 3- HYDROXY- 3- METHYLGLUTARYL COENZYME A (HMG COA) REDUCTASE INHIBITORS 5 ALPHA- REDUCTASE INHIBITORS ADENOSINE DIPHOSPHATE P2Y12 INHIBITORS ALPHA 1- ADRENERGIC BLOCKING AGENTS ALPHA- ADRENERGIC AGONISTS ALPHA- ADRENERGIC AGONISTS, OPHTHALMIC ANGIOTENSIN II RECEPTOR ANTAGONISTS HORMONAL AGENTS, STIMULANT/ REPLACEMENT/ MODIFYING (THYROID) INSULIN, INTERMEDIATE- ACTING INSULIN, LONG- ACTING INSULIN, SHORT- ACTING LAXATIVES LEUKOTRIENE RECEPTOR ANTAGONISTS LINCOMYCIN ANTIBACTERIALS ANGIOTENSIN- CONVERTING ENZYME (ACE) INHIBITORS LOCAL ANESTHETICS ANTI- INFLAMMATORIES, INHALED CORTICOSTEROIDS LOOP DIURETICS ANTIARRHYTHMICS - CLASS IA/ II/ III/ IV LTC DRUGS- AMINO DERIVATIVE PENICILLINS (CHEWABLE) ANTICHOLINERGICS ANTICOAGULANTS LTC DRUGS- AMINO DERIVATIVE PENICILLINS (ORAL LIQUID) LTC DRUGS- ANTIEMETICS (SUPPOSITORY) ANTIDEPRESSANTS, OTHER LTC DRUGS- BRONCHODILATORS, SYMPATHOMIMETIC (SHORT- ACTING SOLUTION) ANTIEMETICS ANTIHERPETIC AGENTS ANTISPASMODICS, GASTROINTESTINAL LTC DRUGS- HISTAMINE2 (H2) BLOCKING AGENTS (ORAL LIQUID) LTC DRUGS- LOOP DIURETICS (ORAL LIQUID) LTC DRUGS- MACROLIDES (ORAL LIQUID) ANTISPASMODICS, URINARY ANTISPASTICITY AGENTS ANXIOLYTICS ATYPICALS AZOLE ANTIFUNGALS, ORAL LTC DRUGS- NONSTEROIDAL ANTIINFLAMMATORY DRUGS (ORAL LIQUID) MACROLIDES MISCELLANEOUS ANTIBACTERIALS NICOTINIC ACID NITROFURAN ANTIBACTERIALS BETA- ADRENERGIC BLOCKING AGENTS WITH VASODILATING PROPERTIES NONSELECTIVE BETA- ADRENERGIC BLOCKING AGENTS BETA- ADRENERGIC BLOCKING AGENTS, OPHTHALMIC BETA- LACTAM, PENICILLINS BIGUANIDES NONSTEROIDAL ANTI- INFLAMMATORY DRUGS OPHTHALMIC AMINOGLYCOSIDES OPHTHALMIC ANTI- ALLERGY AGENTS BIPOLAR AGENTS BISPHOSPHONATES, ORAL BOWEL PREPARATION PRODUCTS OPHTHALMIC PROSTAGLANDIN AND PROSTAMIDE ANALOGS OPIOID ANALGESICS, LONG- ACTING OPIOID ANALGESICS, SHORT- ACTING BRONCHODILATORS, ANTICHOLINERGIC OPIOID ANALGESICS, SHORT- ACTING WITH APAP BRONCHODILATORS, SYMPATHOMIMETIC (LONG- ACTING) PHOSPHODIESTERASE III/ ADENOSINE UPTAKE INHIBITORS BRONCHODILATORS, SYMPATHOMIMETIC (SHORT- ACTING) POLYENE ANTIFUNGALS CALCIUM CHANNEL BLOCKING AGENTS (NONDIHYDROPYRIDINES) CALCIUM CHANNEL MODIFYING AGENTS POTASSIUM SUPPLEMENTS POTASSIUM- SPARING DIURETICS CARDIOSELECTIVE BETA- ADRENERGIC BLOCKING AGENTS CARDIOVASCULAR AGENTS, OTHER PROGESTINS PROTECTANTS, GASTROINTESTINAL CEPHALOSPORIN ANTIBACTERIALS, 1ST GENERATION PROTON PUMP INHIBITORS CEPHALOSPORIN ANTIBACTERIALS, 2ND GENERATION CHOLESTEROL ABSORPTION INHIBITORS CHOLINESTERASE INHIBITORS QUINOLONES SEDATIVES/ HYPNOTICS SELECTIVE ESTROGEN RECEPTOR MODIFIERS DIHYDROPYRIDINES DOPAMINE AGONISTS, NONERGOT DOPAMINE PRECURSORS ESTROGENS FIBRATES SEROTONIN/ NOREPINEPHRINE REUPTAKE INHIBITORS SKELETAL MUSCLE RELAXANTS SMOKING CESSATION AGENTS SODIUM CHANNEL INHIBITORS SULFONAMIDES GAMMA- AMINOBUTYRIC ACID (GABA) AUGMENTING AGENTS GLUCOCORTICOIDS, OPHTHALMIC GLUCOCORTICOIDS- SYSTEMIC SULFONYLUREAS TETRACYCLINES THIAZIDE DIURETICS GLUCOCORTICOIDS- TOPICAL- MEDIUM POTENCY GLUCOCORTICOIDS-TOPICAL-HIGH POTENCY GLUTAMATE PATHWAY MODIFIERS THIAZOLIDINEDIONES TRICYCLICS VASODILATORS, DIRECT- ACTING ARTERIAL GLUTAMATE REDUCING AGENTS VASODILATORS, DIRECT- ACTING ARTERIAL/ VENOUS HISTAMINE1 (H1) BLOCKING AGENTS, MILDLY/ NON- SEDATING HISTAMINE2 (H2) BLOCKING AGENTS XANTHINE OXIDASE INHIBITORS Transmittals Issued for this Chapter Rev # Issue Date R10PDB 02/12/2010 R2PDB 07/18/2008 Subject Chapter 6 Part D Drugs and Formulary Requirements Initial release of chapter Impl Date 03/01/2010 CR# N/A 07/18/2008 N/A









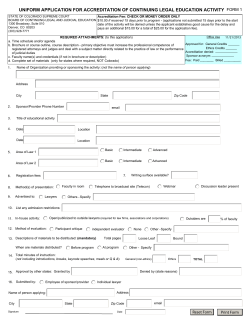
© Copyright 2026