
HRSA Tells 50-Plus Drug Makers To Refund 340B Hospitals AMA Wants Reassessment,
InsideHealthPolicy.com’s Inside CMS exclusive news on the most powerful agency in health care Vol. 17, No. 43 - October 23, 2014 AMA Wants Reassessment, Alignment Of CMS Value-Based Programs The American Medical Association blasted CMS’ value-based programs — electronic health records’ meaningful use requirements, the Physician Quality Reporting System and the Value-Based Modifier — in a letter Tuesday (Oct. 21) asking that the programs be revamped and aligned so that physicians won’t face up to 13 percent in Medicare payment penalties by 2019. AMA says the value-based programs have unrealistic deadlines and requirements that, while having similar goals, are implemented in isolation creating confusion and hardships for physicians who can find themselves penalized under the programs for things they don’t control. “These programs, with often incomprehensible, conflicting requirements and flawed implementation processes, are all entering their penalty phases and pose a risk to the stability of the Medicare program that many policymakers do not seem to appreciate,” AMA writes in its letter to CMS administrator Marilyn Tavenner. The doctor’s organization says that the rules for these programs have become so complex and are in so much flux “that no one, often including the staff in charge of implementing them, can fully understand and interpret them.” Physicians have frequently told the AMA that most times they are unable to get through to continued on page 10 HRSA Tells 50-Plus Drug Makers To Refund 340B Hospitals The Health Resources and Services Administration has told more than 50 drug manufacturers to refund 340B hospitals for certain orphan drugs charged at non-discounted prices, complaining the companies did not follow the agency’s controversial orphan drug policy that has been the subject of two drug industry court challenges. HRSA told Inside Health Policy a letter was sent on Oct. 7 giving the manufacturers 30 days to “notify HRSA of plans to repay affected covered entities and to institute the offer of the discounted price in the future.” Pharmaceutical Research and Manufacturers of America had no comment on the letters. But the Safety Net Hospitals for Pharmaceutical Access and the continued on page 12 44 Percent Of Beneficiaries Opt Out Of California Duals Demonstration Nearly 44 percent of dual eligibles opted out of the California demonstration to coordinate care for beneficiaries eligible for both Medicare and Medicaid — a move that comes as CMS officials are studying why beneficiaries across duals demonstrations choose to opt out after passive enrollment. The opt-out rate in California’s demo, the largest duals demo in the country, is higher than some expected, but Molina Healthcare, whose plans participate in the demos, anticipated it. A CMS official said the duals demonstrations are still new and it’s more important to study why beneficiaries opt-out than it is to worry about how many don’t participate. continued on page 13 Binding Arbitration Proposed As Fix To Expensive Rx Prices In Part D Congress could allow for binding arbitration to help plans negotiate lower prices for unique specialty drugs, Harvard professors wrote in a January 2008 Health Affairs article that is getting new attention in light of the $94,500 price of a 12-week course of the newly approved hepatitis C drug Harvoni. The Center for a Responsible Federal Budget drew attention to the old proposal to help advance the debate over how, or whether, steps should be taken to control the price of specialty drugs. In the debate over specialty drug prices, health plans blame drug makers for price gouging and drug makers blame plans for shortsightedness and high cost-sharing, but there hasn’t been much discussion over what could be done continued on page 14 CMS, OIG Extend Fraud & Abuse Waivers Due To Delayed Rule On ACOs CMS and the HHS Office of Inspector General on Thursday (Oct. 16) extended waivers they had earlier granted for Accountable Care Organizations to get around some fraud and abuse laws, saying a proposed rule for the second round of the health law’s Shared Savings Program is still in the works and the agencies would benefit from ACOs’ input on whether the waivers are useful in their current form or should be changed. The agencies extended waivers involving the federal anti-kickback statute, physician self-referral law, and some civil monetary penalties law provisions through Nov. 2, 2015. CMS and the OIG issued an interim final rule establishing the waivers in 2011 for the Medicare ACOs. “In light of the planned issuance of a proposed rule and the importance of final waiver regulations that align with the Shared Savings Program, we believe the prudent course of action at this time is to extend the effectiveness of the Waiver IFC,” CMS’ extension says. “[W]e believe that an extension of the Waiver IFC will avoid impediments to the development of innovative care models envisioned by the Shared Savings Program and new approaches to the delivery of health care for beneficiaries.” The agencies also would like to know how ACOs are using the waivers, and whether the waivers are useful. CMS and OIG also say they would like stakeholder feedback on whether the waivers are providing enough protection for Medicare and beneficiaries around the harms associated with referral payments or payments to limit or reduce services. They ask whether the ACO situation in this area has changes since 2011 and should lead to additional rulemaking. The White House Office of Management and Budget in August rejected CMS’ proposed rule on the second round of ACO contracts, provider lobbyists told Inside Health Policy at the time. Providers had urged CMS for more than a year to revamp the Medicare Shared Savings Program, which is the Obamacare flagship policy for reforming Medicare, and congressional Medicare advisers sided with providers on many of their complaints shortly before OMB began reviewing CMS’ proposed rule. It’s neither clear which portions of the proposed regulation OMB asked CMS to redo nor when the agency will finish rewriting it. Contracts for the first ACOs run through 2015, and the ACOs must decide whether to sign the second threeyear contracts in the latter half of next year. Many ACOs have threatened to drop out of the program if CMS doesn’t make major changes to it. ACOs want to keep the option of a one-sided risk model, they want to know which patients they’re judged on, and they want bigger bonuses and lower savings thresholds, among other changes. Two thirds of ACOs in a survey by the National Association of ACOs said they are unlikely to adopt a two-sided risk model in the next round of contracts. — Michelle M. Stein Hot Documents Now Available on InsideHealthPolicy.com The following new documents are available on InsideHealthPolicy.com, our new online health news service. Subscribers to InsideHealthPolicy.com also have access to hundreds of other health-related documents, daily news updates, and a searchable archive of back issues. HGPII Report: GPOs Successfully Self-Regulate Through Ethics, Transparency Business Practices Public Citizen: Medical Malpractice Payments At Historic Low Not an online subscriber? Inside CMS subscribers can get a free, two-week trial to InsideHealthPolicy.com by calling 1-800-424-9068 or signing up at http://www.insidehealthpolicy.com/health_signup.asp. 2 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 CMS Assures Issuers They May Terminate Plans If FFM Subsidies End The agreements to participate in the federally-facilitated marketplace (FFM) that CMS sent to issuers last week include a new clause assuring issuers that they may pull out of the contracts, subject to state laws, should federal subsidies cease to flow. CMS did not say if the clause is meant as a safeguard against the potential impact of various highprofile lawsuits — including Halbig v. Burwell — that could end up in the Supreme Court next year, but stakeholders assume that is the point. The agency tells Inside Health Policy that the new clause was inserted at the request of issuers, and that both parties believe the clause is critical. Agreements must be signed and returned to CMS by Wednesday (Oct. 22). Plaintiffs in the suits argue that the ACA subsidies are limited to people enrolled through state-based exchanges and that the IRS overstepped its authority in allowing people enrolled through the FFM access to subsidies. Because the courts have split in their decisions, plaintiffs in one of the cases — King V. Burwell — petitioned the Supreme Court to take up the issue. It is therefore possible that the court could agree to examine the case during the plan year. The language in the clause says that CMS acknowledges that the issuer has developed its products for the FFM “based on the assumption that (advanced payment tax credits) and (cost-sharing reduction payments) will be available to qualifying (e)nrollees.” “In the event that this assumption ceases to be valid during the term of this Agreement, CMS acknowledges that Issuer could have cause to terminate this Agreement subject to applicable state and federal law,” the contract says. The agreements also affirm that CMS may terminate an issuer from the exchange, following a 60-day written notice, if the insurer “materially breaches” any part of the contract, unless the issuer responds to and rectifies the breach to CMS’ satisfaction within 30 days. However, notwithstanding CMS’ agreement to work with issuers who are willing to fix breaches, the agency says that any insurer served with a notice more than three times in a calender year may be terminated at CMS’ discretion. The language also says that an issuer’s inability to perform due to a CMS error will not be considered a breach. — Amy Lotven PCORI Participants Struggle To Avoid Discussing Cost In Hep C Rx Debate Participants at PCORI’s recent meeting on hepatitis C treatments struggled to avoid talking about cost because they said they wouldn’t be holding a meeting on the treatments were they not so expensive. The ACA-created Patient-Centered Outcomes Research Institute by law is not allowed to fund research on economic outcomes, but the institute put out an updated guidance last month saying it would consider research on how patients’ out-of-pocket costs affect access to care. PCORI met Friday (Oct. 17) to gather input from the public on comparative-effectiveness research on hepatitis C drugs. Participants discussed research that compares new hepatitis C drugs in real-world settings and research that evaluates when to treat patients and how to diagnose and manage them. Those categories go straight to the heart of restrictions that many state Medicaid programs are imposing on Gilead’s expensive new hepatitis C drugs. (The recently approved Harvoni costs $94,500 for a 12-week course.) States often require that patients be in the later stages of the infection before receiving the drugs; often don’t cover the drugs for residents addicted to alcohol and street drugs; and sometimes only allow specialists to prescribe the drugs, even though there are too few specialists to treat all the hepatitis C patients. Much of the debate at the meeting was over whether research is needed at all. Some participants, especially patient advocates, questioned the wisdom of spending limited PCORI funding for comparative-effectiveness studies on drugs that cure nearly everyone with few side effects. Also, some noted that drug companies, including Merck and AbbVie, are developing promising hepatitis C drugs and their research might answer many of the questions that participants raised, such as reinfection rates among drug addicts and alcoholics. But PCORI methodology committee member Naomi Aronson said the scientific rationale that state Medicaid programs are giving for prescribing restrictions “is not sound.” Like it or not, the reality is that states are restricting coverage of hepatitis C drugs because they can’t afford to cover them without taking money from other programs, she said. Given that reality, comparative-effectiveness research could be used to determine the harm in not treating people who are in earlier stages of the disease. Also, patients must cover up to 20 percent of drug costs so patients also likely want to know the consequences of delaying treatment, Aronson said. “One of the things that could be valuable to know is, under circumstances where there are limited resources and there needs to be some kind of prioritization of treatment, ‘What is the most beneficial, what is the least risky?” she said. “The reality of the financial situation at the state level is true and I hope that we can get the best evidence possible to help make the best decision,” she added. Lorren Sandt, executive director of Caring Ambassadors Program, said state Medicaid officials don’t believe data from drug companies on hepatitis C drugs. PCORI must decide to either send a strong message that the current INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 3 research data suffices or fund research solely to make it more difficult for Medicaid programs to restrict access. “I agree with you that your clinical trial data is solid,” she said, referring to drug companies. “I agree with you 100 percent. I think it’s wrong that they are ignoring it. But the arguments that we’re having in front of Medicaid programs is that they say there’s no data to prove these drugs work. So we need to address that. We need to come together as a group and say, ‘You’re wrong. They do work.” ... Or we have to fund it and get these patients care. ”—John Wilkerson JP Morgan: CA Enrollment News Shows Attrition Offset By New Sign-Ups Wall Street firm JP Morgan says in a recent “managed care” memo that California’s updated enrollment figures provide insight into the number of people who will churn off of exchange coverage and indicate that the impact may not be as negative as expected. California figures show that the number of people who drop out of exchange coverage is offset by new enrollees signing up through the special enrollment periods, leaving the total enrollment numbers essentially stable, JP Morgan writes. The firm says that the trend, if nationwide, offers a “modest positive” for hospitals, but its impact on managed care plans will depend on their margins. California accounts for about one-fifth of the total 7.3 million exchange enrollment, and the largest enrollment for major managed care plans WellPoint, Health Net and Molina Health, JP Morgan says. The memo also points out that the 7.3 million national figure, which CMS Administrator Marilyn Tavenner said is accurate as of Aug. 15, translated to 91 percent of the about 8 million people who had initially selected plans. The firm says that it had been presuming a paid rate of 85 percent, but it is possible the actual rate was lower than this but there was positive growth during the special enrollment periods. Covered California reported last week that of the 1.4 million individuals who selected plans during the initial open enrollment period, about 1.14 million (or 81 percent) effectuated coverage by paying their premiums. Another 150,000 have dropped out since then, leaving about 1.12 million people with effectuated coverage as of last week. This equates to a 1.6 percent monthly drop off rate, less than the 2.5 percent rate of decrease that had been expected, according to Covered California. The exchange also assumes that about 15 percent of the current enrollees will not renew their plans, which, when added to the monthly drop off rate, creates an annual enrollment decrease of 30 percent. Covered California had previously projected the annual rate of attrition would be 37 percent. The exchange did not provide updated growth presumptions, but JP Morgan notes that the officials had previously project a 43 percent increase — or 510,000 additional consumers — from the end of 2014 open enrollment to the end of the 2015 open enrollment. The forecast assumed a higher paid rate, but also higher annual churn, the firm says. Covered California also reports that from June to September, 200,000 people had selected a plan through a special enrollment period. JP Morgan points out that the 1.12 million figure does not include the 50,000 or so people who had selected plans in September. Assuming 80 percent of that 50,000 do pay their premiums, total enrollment would bump up to 1.16 million — a net increase of 20,000, or 2 percent, since the end of open enrollment, JP Morgan says. The state-based exchange says in a release that it expects 1.13 million Californians will be part of the forthcoming renewal process. Covered California says it sent its “first wave” of renewal notices to consumers last Wednesday (Oct. 15), and that consumers who complete the renewal process will hear from their plans in December. —Amy Lotven CMS Kicks Off Renewal Process One Month Prior To Open Enrollment CMS Wednesday began educating consumers on the forthcoming exchange insurance renewal process, announcing that different categories of individuals who enrolled or applied for coverage in year one will receive notices from healthcare.gov starting this week. The agency also announced that when consumers return to their marketplace applications about 90 percent of the information will be “pre-populated” with data. The pre-populated data will not include the applicant’s existing plan information, but a CMS official said that there are several ways consumers will be able to find that information in order to compare their coverage with other options. Marketplace notices were sent out Tuesday (Oct. 14), Kevin Counihan, director of CMS’ Center for Consumer Information and Insurance Oversight (CCIIO) and the first Marketplace CEO, said at an America’s Health Insurance Plans conference Wednesday. Counihan, who was making his first public appearance since taking the new position on Sept. 8, stressed that the second open enrollment period is more like the second half of the first year due to the newness of the renewal process. He also reiterated that while the site will be much improved from last year, it will not be perfect. CMS previously said that it would be sending out several different notices based on an enrollee or applicant’s income or other status. For example, CMS will send out a specific notice to individuals who applied and were determined eligible for coverage but did not enroll. The agency will also send targeted notices to people who enrolled, received a subsidy and who are at risk of potential tax repayments because their 2013 tax data indicate that they are earning between 350 percent and 500 percent of the federal poverty level. There is also a special notice for people who did not allow the IRS to automatically check their tax data, however CMS officials have said this involves a relatively small group of individuals. All of the notices include basic information on open enrollment and urge individuals to update their information by 4 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 Dec. 15, while also stressing that enrollees may make choices throughout the 90-day enrollment period. The letter also informs consumers that they will soon be receiving a notice from their issuer on whether their plan will be available in 2015, and on any changes to those benefits. Jessica Kendall, director of Families USA’s Enrollment Assistance Network, says that the notices appear to provide all the needed information. Families has been focusing on ensuring consumers are aware that there are navigators and other assisters available to help with enrollment. Kendall notes that research has shown that people who received in-person assistance were twice as likely to actually get enrolled. Health literacy is difficult for many consumers, so the more help they receive, the better, she says. Consumer advocates — and CMS officials — also are encouraging people to update their income information to ensure that they get accurate subsidies, and to shop for coverage as a new product may be more cost-effective than their current plan. Ben Walker, director of the CCIIO’s Eligibility Policy and Operations Branch, who spoke on an AHIP panel after Counihan’s speech, said that CMS will begin the auto-enrollment process around Dec. 16, although exact timing is still being worked out. Consumers who are automatically re-enrolled will receive two notices. One notice will inform them of their eligibility and the other will let them know that the process has been completed, he said. Walker also explained that the pre-populated application information will be available through “all channels,” including the web site, the call center and direct enrollment with an issuer. Additionally, he said, consumers who want to compare their existing coverage to other available plan options can plug their plan ID into a search function. Issuers in comments on the renewal process had pushed for CMS to include an easy way for consumers who wanted to remain in their existing plan to do so without having to visit plan compare, but CMS did not address that request in its final rule on the renewal process. There are a number of ways that consumers can get their Plan ID, Walker said. The first is through the issuer notice. If people lose those notices, the information can also be obtained through the healthcare.gov call center. Walker also said that the agency is working on a public-facing website that could help consumers pull up that information, but did not say when that would be ready to go live. He stressed that it is critical for CMS to maintain a strong partnership with issuers, and other stakeholders since the re-enrollment process will be so new. He also noted that CMS is committed to taking a careful look at what works and does not in order to make improvements in later years. With Nov. 15 several weeks away, the agency is now finalizing the plans and working on the “crosswalks” that tie products to one another so that the “core” of the auto-enrollment process is place, he said. CMS previously said that issuers seeking to participate in the federally-facilitated marketplace would be receiving notices about certification Wednesday (Oct. 15), but agency did not respond to queries on whether that happened as expected or on how many plans got the notices. Plans and CMS also continue to do full end-to-end testing, and Counihan said that early reports have been positive. — Amy Lotven NCPA Urges Passage Of Open Pharmacy Network, Generic Rx Pricing Bills The National Community Pharmacists Association said Tuesday (Oct. 21) it is pushing for action during the lameduck session on two House bills — one to allow any willing pharmacy to participate in Medicare Part D preferred pharmacy networks in medically underserved areas and one designed to control skyrocketing generic drug prices — that the advocacy group for independent pharmacies and small, regional pharmacy chains has been aggressively backing. However, NCPA officials say that uncertainty over which party will control the Senate come January and major legislative priorities faced by Congress during the lame-duck session — including expiration of the continuing resolution to fund the government in December and looming Medicare physician payment cuts — could mean the organization’s priority issues may have to wait until a new congressional session starts in January. NCPA CEO B. Douglas Hoey — who held a conference call with reporters Monday from the organization’s annual conference and trade expo in Austin, Texas — said by far the number one issue for his members is expanding Medicare Part D rules to allow independent pharmacies and regional pharmacy chains to participate in health plans’ preferred pharmacy networks. NCPA senior vice president of Government Affairs Steve Pfister said the NCPA was buoyed when CMS included any willing pharmacy provisions in its proposed Part D rule, but when the agency decided to scrap the provision in its final rule, saying the issue needed further study, the main options left were state and federal legislation. He said the organization is pushing for action on the House legislation — H.R. 4577, The Ensuring Seniors Access to Local Pharmacies Act — during the lame-duck session and working to have a companion bill introduced in the Senate. Pfister said the NCPA is hoping to find a larger vehicle for the legislation — which has not seen any action in the two House committees to which it has been referred. Failing action in the lame-duck session, Pfister said the NCPA is laying the groundwork to get lawmakers to take up INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 5 the issue in the next Congress. Pfister expects to see as many as 45 new House members and said that because of run-off provisions in Louisiana and Georgia it may not be clear which party controls the Senate until early-January. He said the NCPA has been actively supporting pro-patient and pro-pharmacy candidates ahead of the November midterm elections. The Pharmaceutical Care Management Association, which represents pharmacy benefit managers, strongly opposes the legislation, saying over the summer that opening up some preferred pharmacy networks to any willing pharmacy would cost the federal government $21 billion over 10 years — an argument the NCPA and the bills’ sponsors dismiss. Hoey said generic drug prices increases are the second biggest concern for NCPA members. Pharmacies are being reimbursed for lower generic drug prices often for months after a particular generic drug’s price is increased, he said. He pointed to a generic steroid cream that jumped in price from $100 a tube to $250 a tube, but pharmacies continued to be reimbursed at the $100 per tube rate for more than a month. He said the NCPA has worked with states on legislation to require PBMs to update the prices more quickly and applauded a CMS rule that goes into effect in 2016 that requires a seven-day time limit for generic drug price updates. Hoey said the NCPA has also asked Congress to look into why generic drug prices are rising dramatically. Pfister said the organization is hoping that Congress will hold hearings on generic drug pricing during the lame duck session. He said the hearings are a real possibility, citing a letter sent to HHS Secretary Sylvia Mathews Burwell last week by Sen. Bernie Sanders (I-VT) and Rep. Elijah Cummings (D-MD) asking what steps HHS is taking to address the issue. The two lawmakers also sent letters to 14 generic drug manufacturers giving them until Oct. 23 to answer questions justifying the price increases. “Historically, generic drugs have helped make medications affordable for millions of Americans, and they have resulted in huge savings for consumers and taxpayers. However, recent cost increases are now preventing some patients from getting the drugs they need to understand what factors are driving these price spikes,” Sanders and Cummings wrote. Pfister said the issue of generic drug prices became dormant after a series of NCPA meetings with lawmakers at the beginning of the year, but the organization is now hopeful of getting a hearing because Sanders and Cummings have taken the issue on “with a vengeance.” Sanders chairs the Senate Health, Education, Labor and Pensions subcommittee on primary health and aging, and Cummings is the ranking minority party member on the House Oversight and Government Reform Committee. — Todd Allen Wilson Nurses: Cut Medicare Pay If Hospitals Don’t Protect Workers Against Ebola The National Nurses Union said the president’s decision to tap a White House Ebola czar falls short unless the administration gives the czar power to cut off Medicare and Medicaid funds at hospitals that don’t meet the highest uniform, national workplace safety standards. The union’s press comes as worker health and safety advocates urge the Occupational Safety and Health Administration to step up efforts to issue a delayed infectious diseases rule that would protect health care and other workers. “What we need is a real czar to assure public safety, not a communicator, and the power to cut the hospitals’ Medicare and Medicaid funding if they still refuse to adhere to those standards and leave their patients, nurses and other caregivers at extreme risk,” NNU Executive Director RoseAnn DeMoro said Friday (Sept. 17). The president indicated he would tap Ron Klain, a former chief of staff to Vice President Joe Biden and also to then-Vice President Al Gore, for the new position. NNU for the past two months has called for greater protective standards against potential Ebola exposure for patients, registered nurses and other frontline health workers in all U.S. hospitals. DeMoro said that “only a direct mandate from the President or Congress to order hospitals to implement the highest possible standards and protocols will suffice to attack and eradicate the threat of Ebola in the U.S.” DeMoro wrote to the president earlier in the week asking that he invoke his executive authority to mandate uniform, national standards and protocols that all hospitals must follow to protect patients, registered nurses, other front-line healthcare workers, and the public. Late Thursday (Oct. 16) the group also posted an online petition inviting everyone to join the demand for the president and Congress to act. In a matter of hours, DeMoro said, more than 15,000 people signed the petition. The nurses union wants the administration to direct every healthcare employer to follow the Precautionary Principle and institute optimal personal protective equipment for Ebola that meets the highest standards used by Nebraska Medical Center, or a higher standard, including: • “Full-body hazmat suits that meet the American Society for Testing and Materials (ASTM) F1670 standard for blood penetration, the ASTM F1671 standard for viral penetration which leaves no skin exposed or unprotected. • “National Institute for Occupational Safety and Health-approved powered air purifying respirators with an assigned protection factor of at least 50 — or a higher standard as appropriate. • “At least two direct-care registered nurses caring for each Ebola patient with additional RNs assigned as needed 6 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 (based on the direct care RN’s professional judgment), with no additional patient care assignments. • “Continuous interactive training with the RNs who are exposed to patients, continuous updated training and education for all RNs that is responsive to the changing nature of disease, and continuous interactive training and expertise from facilities where state-of-the-art disease containment is occurring. • “If the Employer has a program with standards that exceed those used by Nebraska Medical Center, the higher standard shall be used. The Ebola pandemic and the exposure of healthcare workers to the virus represent a clear and present danger to public health. We know that without these mandates to healthcare facilities, we are putting registered nurses, physicians and other healthcare workers at extreme risk. They are our first line of defense. We would not send soldiers to the battlefield without armor and weapons.” NNU’s press comes as industrial hygienists urge OSHA to quickly issue an infectious diseases rule. The American Industrial Hygienists Association wrote OSHA chief David Michaels Wednesday (Oct. 15) that such a standard is an absolute necessity to assist in controlling the virus. Meanwhile, OSHA this week issued a fact sheet for workers and employers in non-healthcare and non-laboratory settings that are tasked with cleaning surfaces that may be contaminated with Ebola. The guidance warns the use of chemical disinfectants may require an employer to train workers about how to protect themselves against chemical hazards. In some cases, “additional respiratory protection (e.g., respirators) may be necessary to protect workers from exposure to Ebola and/or chemical disinfectants,” OSHA says “In instances where workers may be exposed to bio-aerosols (e.g., as a result of spraying liquids or air during cleaning) suspected or known to contain Ebola virus, additional respiratory protection is needed. In these cases, medically qualified qualified workers must use, at a minimum, a NIOSH-approved, fit-tested N95 respirator,” OSHA adds. Meanwhile, California’s OSHA program on Friday (Oct. 17) issued its own Ebola guidelines aimed at protecting health care workers, emergency responders, laboratory staff, mortuary workers, airline flight crews and airport staff, and quarantine operations staff. — Donna Haseley Medicare Rights Center Urges CMS To Improve MA Appeals Processes The Medicare Rights Center is asking CMS to make improvements to Medicare Advantage plans’ appeals processes by giving beneficiaries more information and auditing plans more often, as the beneficiary advocates say managing coverage denials and appeals is a consistent concern for MA beneficiaries. In a recently released “Medicare Snapshot” on MA denials and appeals, the center says that over a third of beneficiaries calling the national helpline have difficulty handling coverage denials and appeals. While that number includes feefor-service appeals, Stacy Sanders, federal policy director for the Medicare Rights Center, says that the majority of calls the center receives about appeals are related to either MA plans or Part D (drug) plans. Beneficiaries can ask MA plans to take another look at denials as the first step of the MA appeals process. After reconsideration from a plan, beneficiaries can request a review by an independent review entity, followed by a hearing with the Administrative Law Judge. The next step is taking the appeal to the Medicare Appeals Council. Plans are required to send beneficiaries a notice explaining why coverage was denied as part of the appeals process, but the Medicare Rights Center notes that in 2013, 89 percent of audited MA and Part D sponsors sent beneficiaries denial letters that either didn’t include an adequate rationale for why the plan denied coverage or contained incorrect information. The MRC says that CMS made a note of the issue in a memo looking at 2012 audits, though the situation didn’t improve during the next year, the MRC says. Medicare Rights Center says it often hears from beneficiaries who have had their cases dismissed because of narrow technicalities or delays the beneficiary can’t control. In nearly 70 percent of cases where a beneficiary requests an independent review outside of the MA plan, MRC says, there is no specific data available on why the reviews are dismissed or withdrawn, the MRC says. The snapshot says that “[w]hile limited public data is available on how well MA plans address appeals and grievances, audit data made available by the Centers for Medicare & Medicaid Services (CMS) suggests significant room for improvement.” The beneficiary advocates ask CMS to make more data on plan-level appeals and grievances available. More information should be available on MA and Part D pharmacy transactions, coverage determinations and redeterminations, the MRC says. The center also suggests that CMS needs to enhance monitoring and enforcement of how the MA plans handle grievances and appeals to make sure the information given to beneficiaries is accurate and efficient. Sanders says enhanced monitoring should include additional audits. “In particular, CMS should enforce strict compliance with notice rules and requirements to effectuate timely decisions, holding beneficiaries harmless when a plan fails to meet the standards,” the snapshot says. The beneficiary advocacy group also asks CMS to restructure the appeals process so that more proactive outreach from the health plans is required to prove that coverage isn’t appropriate, rather than expecting beneficiaries INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 7 to be able to build a legal case to show coverage should apply. The center also asks that CMS and plans provide better consumer education on how plans work — particularly around coverage and access rules. Plans should also be required to send copies of materials that they use when denying a claim to the beneficiaries and the independent review entity evaluating an appeal, MRC says. Currently, CMS tells beneficiaries in a booklet on appeals: “If you appeal the plan’s decision, you may want to ask for a copy of your file containing medical and other information about your case. Your plan may charge you for this copy.” The Medicare Rights Center says that plans should be required to send materials with plain language reasons for denials and also cite excerpts from plan or CMS rules that the plan used to deny care. But the plan should also include all information about those rules — including the information that might weigh in the beneficiaries’ favor, MRC says. Beneficiary resources that help represent beneficiaries in appeals situations, like the State Health Insurance Assistance Programs, should also be expanded, MRC says. — Michelle M. Stein Companies Want FDA To Make Early Biologic Exclusivity Determinations Companies developing biologics want FDA to begin the process of determining biologic exclusivity earlier than it has planned in recent draft guidance and assert that the agency has gone beyond its statutory mandate in asking them to prove their product’s exclusivity instead of automatically granting it. Biosimilar sponsors seeking to copy innovator drugs want the ability to request and weigh in on exclusivity determinations, and to ensure the process does not lead to “evergreening” — constantly extending the product’s market protections. FDA laid out the process for determining biologic exclusivity in a draft guidance document issued in August that was quickly followed by the “Purple Book,” which lists product exclusivity information publicly. The agency said these critical determinations will not always be made when the agency licenses a product, but the Biotechnology Industry Organization and Pharmaceutical Research and Manufacturers of America urge FDA to weigh in as early as possible during the development process. They stress that this information will inform investment decisions. “Where eligibility for exclusivity instead depends on scientific issues regarding product structure or safety, purity, or potency, it may be necessary in some cases to wait until the (biologics license application) has been filed, but we would ask the agency to make a good faith effort to provide an initial answer earlier whenever possible,” PhRMA says, commenting on the guidance. The agency should make the exclusivity determination before or soon after the BLA is filed, the industry group asserts. BIO lays out some examples. If the exclusivity eligibility depends on the relationship of the applicant and another entity, the determination could likely be made before the BLA submission. If the exclusivity determination hinges on a an analysis of a previously licensed product and a new submission, FDA should make the decision no later than when the BLA is approved and provide guidance if possible. BIO asks that the final guidance address when FDA will make exclusivity determinations, including for existing products. The Generic Pharmaceutical Association says biosimilar sponsors could have relevant information about the reference product and “a strong interest in timely exclusivity determinations.” As a result, GPhA asks that FDA create a mechanism to allow biosimilar applicants, not just the BLA holder or the agency itself, to request an exclusivity determination. “Indeed, decisions about biosimilar development programs may hinge on whether or not the reference product has exclusivity and, if so, when that exclusivity expires,” said GPhA President and CEO Ralph Neas. “Accordingly, the Draft Guidance should be amended to recognize the contributions and interests of other stakeholders, particularly on complex scientific issues like those required for an exclusivity determination.” Biologics receive 12 years of exclusivity. Product changes such as those resulting in a new indication, route of administration or dosing schedule, are statutorily excluded from triggering a new exclusivity period. However, some structural changes resulting in a change in safety, purity or potency could warrant a new exclusivity period. To help FDA make these determinations, the agency guidance document suggests sponsors submit a list of all licensed biological products that are structurally related to the product, note for which of those related products the sponsor or one of its affiliates is the current or previous license holder, describe the structural difference between the proposed product the other structurally related products listed, and note evidence of the change in safety, purity or potency. Hospira, which is developing biosimilars, wants FDA to make more of the exclusivity determination process public. The company asks that FDA publish the submitted list of structurally similar products in the “Purple Book” when the product is approved. The agency also should collect and take into account feedback from stakeholders before finalizing a decision, Hospira says. The company also notes that there is no appeals process, and FDA does not specify whether the determination is a final agency action, meaning it could be appealed in court under the Administrative Procedures Act. In addition to the timing of the exclusivity determination, companies raise concerns about the decision itself. Innovator companies are cautious about having to request exclusivity and the information they must provide, while biosimilar developers raise concerns about innovator companies attempting to unnecessarily extend their exclusivity. BIO and PhRMA describe the process of requesting exclusivity and submitting information as “burdensome,” saying 8 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 it puts the onus on companies to prove that they have exclusivity. Twelve years of exclusivity should be granted by default if the application in question is not a supplement or a subsequent application to a previously approved product, BIO says. “Further, in the Draft Guidance FDA describes the first licensure determination as ‘challenging’ and fraught with ‘scientific and technical complexities’ and indicates that it views reference product exclusivity as something for which a sponsor must qualify, rather than something that arises by default or presumption,” BIO says, adding that this interpretation is inconsistent with the statute. Hospira says FDA’s interpretation of what constitutes a modification of a biologic’s structure compounds concerns by some stakeholders that statutory language could leave products vulnerable to an “evergreening loophole.” FDA says it will presume that products affecting a different molecular target resulted in a change in safety, purity and potency, and the company takes issue with this stance. Hospira says molecular targets were not mentioned in the statute and it would be an expansion of the legal language if FDA allows additional exclusivity when it otherwise would not have been granted. “Hospira believes that this ‘presumption’ goes far beyond what is required by the statutory language and potentially creates an arbitrary bias in favor of reference product sponsors, to the detriment of Hospira and other biosimilar sponsors — and the general public,” Hospira tells FDA. GPhA also raises concerns with how FDA will determine which product changes trigger more exclusivity. The guidance says that if the product affects the same molecular target as a previously licensed product, the sponsor should provide data to show that there is a structural change. BIO and PhRMA warn that FDA could deter companies from improving or developing new products if there is a high evidentiary standard for proving a change in safety, purity and potency. — Alaina Busch McBournie Large Drug Firms’ Buys Of Smaller Ones Seen As Factor In Drug Price Hikes Some drug price-control advocates say recent moves by big pharmaceutical companies to buy smaller biotechnology companies that have developed specialty drugs are contributing to rising drug costs and a lack of transparency around how those drugs are priced — though others say such a business model has been common for years, and the recent highprofile acquisitions by Roche and Gilead Sciences simply serve to highlight this model. FDA’s approval of drug maker giant Roche’s $94,000 a year drug for a fatal lung-scarring disease, coming soon after Gilead Science’s release of both hepatitis C drugs Sovaldi and Harvoni, highlight a trend of larger drug makers buying smaller organizations and then pricing the drugs at the center of those acquisitions as whatever price the companies believe they can get away with, according to Larry McNeely, policy director for the National Coalition on Health Care. This business model adds fuel to the fire of overpricing specialty drugs, McNeely told Inside Health Policy — especially when drugs are available in other countries at cheaper rates. If this were one or two instances, the health system could handle it, but the trend of overpriced drugs is a broader one, McNeely said. Once more companies see what Gilead and Roche are able to do, there could be a bigger move in this direction, he added. Drug giant Roche bought InterMune Inc. last month as the company awaited FDA approval of the idiopathic pulmonary fibrosis drug Esbriet. The drug was priced at $94,000 a year — though one industry analyst thought the company could have priced it higher. Esbriet was previously available in Europe and Canada, though the price in some countries is around half of what it costs in the United States. Esbriet, along with Ofev, are the first treatments approved for idiopathic pulmonary fibrosis. Roche’s move follows Gilead’s purchase of Pharmasset, which had planned to price Sovaldi at $36,000. Gilead instead priced the cost for a 12-week treatment at $84,000, and priced the combination drug Harvoni at $94,500. One industry analyst, however, says that big pharmaceutical companies buying smaller biotechnology companies has been a trend for more than five years — though it’s rare to see a company as far along with drug development as InterMune when bought out by Roche. Bigger companies would like to control the application process at FDA, and some believe big pharmaceutical companies are best served by buying smaller biotechnology companies and marketing their products rather than conducting the actual research and development themselves, the analyst said. The recent examples of Roche and Gilead show acquisitions involving particularly high-priced drugs that are drawing attention and highlighting a trend that will likely continue, the analyst said. With these business models, there are questions around whether companies should look at the research and development costs when setting prices or whether they should look at acquisition costs, which might be higher, the analyst said. Mark Gibson, the director of the Center for Evidence-based Policy, noted Roche’s move to purchase InterMune so close to FDA approval of the IPF drug and pointed out that companies charging high amounts for some specialty drugs are not the ones who developed them. They simply looked and priced the drugs around what the market will bear, Gibson said at a recent America’s Health Insurance Plans conference on state issues. Big pharmaceutical companies purchasing smaller companies that are on the verge of gaining approval for a new INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 9 drug and then selling those drugs at high costs is a trend that the industry will likely see increase, Gibson later told IHP, as companies are looking to make a profit. There’s a double standard when looking at rationing by price Gibson said at the conference, as it’s not just about plans not covering something. There’s also rationing when a company won’t sell drugs at a price that’s affordable. But there is a conundrum around finding enough of a return on investment on new drugs to ensure innovation, he added. At some point we need to decide if a drug maker is a health care provider, Gibson said. If they are, then the health care sector should look at whether there are ethical standards other providers are held to that drug companies should also be expected to meet. There is interesting innovation occurring in the pharmaceutical space, but right now we are rewarding companies that have nothing to do with innovation, McNeely said. — Michelle M. Stein AMA Blasts CMS Over Programs’ Implementation . . . begins on page one the CMS Help Desks when they have questions about the programs, and that when they do finally get their calls answered CMS staff are frequently unable to answer their questions, the letter states. The AMA’s tough critique of CMS’ value-based programs mirrors comments sent to the agency last month by the Association of American Medical Colleges and the American Hospital Association that said CMS is moving “too far, too fast” in implementing penalties for the PQRS and VBM programs. Many doctors are confused about the MU Stage 2 and PQRS quality measurement requirements, incorrectly believing that if they report quality measures for one of the programs they have fulfilled the requirements for both, the AMA says. The organization notes that under MU Stage 2, physicians must meet 125 different criteria per patient. The AMA reiterates problems and recommendations for the MU program that it detailed in a “blueprint” for fixing the program that it sent to CMS last week. The organization asks the agency to do away with the “all or nothing” incentive and penalty provision of the program. Additionally the organization asks CMS to shorten the 2015 reporting period to 90 days. The group also calls CMS out for allowing physicians to attest to meaningful use using older certified software because newer versions were unavailable in many areas, and then failing to update its own systems ahead of the Oct. 1 deadline to allow use of the older systems, leaving many doctors facing non-compliance penalties even though they made good-faith efforts to attest using the older software. The AMA does thank CMS for listening to its concerns and after updating systems earlier this month — but after the doctors’ deadline — and allowing physicians until the end of November to attest to MU. “MU compliance requires investment in poor-performing, non-interoperable systems, despite the fact that achieving interoperability across the nation’s health care records system was the principal goal of the legislation that created the incentive program. Overly complex certification requirements have prevented many vendors from being able to deliver timely, updated products, jeopardizing full-year reporting in 2015,” the AMA writes. In the PQRS program, AMA says doctors do not get timely data about their results, in turn leaving them with little or no time to fix problems before having to submit the next year’s report. The AMA contends the registration and submission process for PQRS is complicated, time consuming and filled with website glitches that make the process overly difficult and burdensome for physicians to comply with. The organization also complains that there is no formal appeals process for the program, and are asking CMS to establish one. The organization asks CMS to align the different quality measurement requirements in MU, PQRS and VBM and allow physicians’ attestation in one of the programs to count for all three. It notes that 2012 data showed that 40 percent of provider groups of 25 physicians or more did not have enough data to calculate “reliable cost and quality measures” for the VBM and expected that smaller practices would have even less data. Additionally, the AMA contends that under VBM inappropriate cost and outcome measures have been implemented that penalize physician groups that see the most high-risk and sickest patients, noting that these practices are three times more likely to have poor quality scores and four time more likely to have poor cost scores. The AMA says that within the VBM program “(r)ules, by necessity, are being constructed on the fly, change every year, and are now so complicated that it takes several weeks to get an answer from CMS on details of the program. Physicians are largely unaware that the VBM even exists, and a key report intended to help make them aware is difficult to access and for many practices will not include all the information they need to avoid VBM penalties in future years.” The burdensome requirements and separate penalties for each program that increase each year — sometimes doubling from year to year as in the case of the VBM — when coupled with 2 percent annual cuts due to deficit reduction sequestration can by 2019 add up to more than 13 percent in payment cuts to physicians that could leave them struggling to keep their practices viable, the AMA says. The organization notes that this does not include the 24 percent Sustainable 10 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 Growth Rate (SGR) payment cuts schedule to go into effect in late-March if Congress does not repeal or replace the program or put off SGR cuts for another year as it did in February. The AMA says it is willing to help CMS conduct a “realistic assessment” of the value-based programs and the problems they face, as well as finding ways to move forward. “To be clear, the AMA has a great deal of sympathy for CMS and the position it finds itself in. It is hard to take the long view in an agency struggling to meet unrealistic deadlines with inadequate resources and a flawed IT platform. However, the current strategy of aggressively moving forward with policies that place an ever increasing burden on both CMS and physicians, combined with the flawed roll-out of the Medicare claims data release and Open Payments program and the problems with these programs, threatens to do serious damage to the agency’s image and to physician confidence in the government’s stated goal of achieving a health care system that delivers more value for the dollar,” the AMA concludes. — Todd Allen Wilson Worker Health Experts Urge OSHA To Release Rule Due To Ebola Crisis Industrial health experts are urgently calling on OSHA, and also taking their case directly to the White House, to move forward as rapidly as possible on a rulemaking to tackle infectious diseases in health care settings — pressure that follows close on the heels of at least two U.S. health workers testing positive for the Ebola virus. An official with the American Industrial Hygiene Association (AIHA), which is spearheading the profession’s call for a long-sought rule on the subject, tells Inside OSHA Online there is also rampant concern that Congress and others in government are neglecting to involve experts in the worker health field in formulating response plans. AIHA wrote an Oct. 15 letter to President Obama, OSHA, NIOSH and the Centers for Disease Control and Prevention to convey that many workers are worried about the disease’s potential spread in occupational settings. “Recent news reports have confirmed what many have feared — the Ebola virus has now become active in the United States,” Peter O’Neil, AIHA executive director, says in the letter to Obama. “With the first death of a patient in Texas and the ensuing confirmation of at least two healthcare workers testing positive for the virus, American workers are now expressing concern for their health and safety,” he says. “There is additional concern about the U.S. health care sector’s readiness to provide adequate health protections as cases of Ebola begin to emerge.” Whether there is an adequate supply of personal protective equipment (PPE) in hospitals is of paramount concern, according to AIHA, which says an adequate supply is “crucial to avoid spread of the disease to workers. The Ebola crisis underscores the need of the health care community to re-emphasize PPE and other safety precautions.” But AIHA, in addition to existing protective measures, wants more comprehensive OSHA regulations. OSHA chief David Michaels has indicated that, though timing is unclear, the agency is working stringently on such a rule. The agency reportedly wants to send the rule to a small business review by next month. Industrial hygienists say that with Ebola’s emergence in the United States it is key to move forward quickly with infectious disease regulations, which it characterized as “delayed.” “This rule would provide increased protections and recommendations for America’s healthcare workers,” O’Neil wrote. “The rule is an absolute necessity to assist in controlling this virus.” The hygienists group also wants agencies to engage with each other and outside stakeholders “in efforts to separate the misleading information from the science in how best to protect workers from this virus. In support of these initiatives, AIHA is urging you to back these efforts and request Congress to appropriate the necessary funds to carry out this important work. Diseases like Ebola create public concern for the health and safety of healthcare workers SUBSCRIPTIONS: 703-416-8500 or 800-424-9068 [email protected] NEWS OFFICE: 703-416-8577 Fax: 703-416-8543 [email protected] Health Group Publisher: Chief Editor: Managing Editor: Associate Editor: Contributing Editors: Donna Haseley ([email protected]) John Wilkerson ([email protected]) Michelle M. Stein ([email protected]) Todd Allen Wilson ([email protected]) Amy Lotven ([email protected]) Production Manager: Production Specialists: Lori Nicholson Daniel Arrieta, Michelle Moodhe Inside CMS is published every Thursday by Inside Washington Publishers, P.O. Box 7167, Ben Franklin Station, Washington, DC 20044. Subscription rates: $705 per year in U.S. and Canada; $755 per year elsewhere (air mail). © Inside Washington Publishers, 2014. All rights reserved. Contents of Inside CMS are protected by U.S. copyright laws. No part of this publication may be reproduced, transmitted, transcribed, stored in a retrieval system, or translated into any language in any form or by any means, electronic or mechanical, without written permission of Inside Washington Publishers. INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 11 and it is only a matter of time before this concern spreads to other workers.” The industrial hygiene field is well-positioned to help in the response, the group argues. “As an organization, AIHA’s members and goals focus on preventing occupational illness and injury as a fundamental principle of the industrial hygiene field. This makes our members uniquely qualified to protect worker health, as AIHA plays a unique role at the crossroads of manufacturers, practitioners, and the government. As the crisis evolves, AIHA believes that the role of industrial hygienists will become increasingly important as more and more workers become concerned.” Aaron Trippler, AIHA director of government affairs, says it was disconcerting that at a recent hearing of the House Energy and Commerce Committee to address Ebola concerns there was a “lack of mention” of recruiting either OSHA or NIOSH to help stop the crisis. Lawmakers in that hearing grilled CDC chief Tom Frieden about the administration’s response to Ebola. Trippler says that “CDC’s overburdened” with the issue and that it needs help from other agencies such as OSHA. “They need to include people who have the expertise.” — Christopher Cole Drug Makers Aren’t Offering Orphan Drug Discounts . . . begins on page one National Rural Health Association say that most drug manufacturers have disregarded HRSA’s interpretive rule laying out its orphan drug discount policy. “We fully support the Health Resources and Services Administration’s enforcement action against the many pharmaceutical manufacturers who are not following the government’s rule on orphan drug pricing,” SNPHA President Ted Slafsky said in a statement. “The government has clearly and correctly interpreted the law as requiring them to provide discounts to rural and cancer hospitals when an orphan drug is used to treat a common condition.” NRHA CEO Alan Morgan also said that drug manufacturers ignoring the policy should be obligated to provide refunds to the 340B hospitals. HRSA told IHP the agency moved to contact the manufacturers after 340B stakeholders alerted HRSA that the 340B price wasn’t available for orphan drugs. PhRMA previously sued HRSA over the agency’s orphan drug policy, which said that manufacturers needed to provide drug discounts through the 340B program for orphan drugs if the drugs were used off-label or to treat anything other than a specific orphan condition. Though the court threw out the original rule that laid out the policy, the agency in July released a second interpretive rule that laid out essentially the same policy. “[T]he Court did not invalidate HRSA’s interpretation of the statute. HHS/HRSA continues to stand by the interpretation described in its published final rule,” HRSA’s website states. PhRMA has since sued again over the interpretive rule. HRSA did not say what enforcement action the agency could potentially take against manufacturers if they don’t comply with the letters and provide refunds to the 340B hospitals. In a Frequently Asked Questions portion of the agency’s website, however, the agency says that while the orphan drug interpretive rule is not binding, the statute is binding and “[a] manufacturer’s or covered entity’s failure to comply with the statutory requirements could subject a manufacturer or covered entity to an enforcement action by HRSA, which could include refunds to covered entities in the case of overcharges, as well as a termination of a manufacturer’s Pharmaceutical Pricing Agreement.” “In deciding whether and in what circumstances to take enforcement action, HRSA will necessarily be required to interpret the statute,” the FAQ says. If a manufacturer or covered 340B stakeholder has a different interpretation of the statute and is subject to enforcement action, HRSA says the manufacturer would have a chance to “advocate for a different interpretation of the statute” while defending itself against the enforcement actions. — Michelle M. Stein Nurses Join Campaign Questioning Validity Of Some Health Care Practices The American Academy of Nursing will begin a pilot program in Texas to study whether nurses and patients should shy away from five health care practices, as suggested by the American Board of Internal Medicine Foundation’s “Choosing Wisely” campaign. The nursing organization says it plans to engage multiple stakeholders — including physicians, nurses, consumer groups, patients and their families, nursing schools and others — in its pilot program, with the goal of expanding its list of questionable practices and moving the program into five additional states in the next year. In its first five Choosing Wisely recommendations, the AAN says nurses shouldn’t automatically start continuous fetal heart rate monitoring for women in labor without risk factors; shouldn’t let older patients just lay in bed or only get up to move to a chair during hospital stays; shouldn’t use physical restraints with older, hospitalized patients; shouldn’t wake patients for routine care unless the patient’s condition or care specifically requires it; and shouldn’t place or maintain a urinary catheter in a patient unless there is a specific indication to do so. The AAN is one of the first non-physician groups to make recommendations to the Choosing Wisely campaign, for 12 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 which nearly 100 medical specialty societies have identified more than 250 tests and procedures that they describe as overused and inappropriate in the past two years. AAN president Diana Mason said the the criteria the organization used for recommending practices to question was that the practices have to be within the domain of the discipline of nursing; have a high impact; and be based on evidence. The practices AAN says nurses should avoid include: Continuous electronic fetal heart rate monitoring for low-risk pregnancies: AAN secretary Karen Cox said evidence does not support using continuous electronic fetal heart rate monitoring for women in labor with low-risk pregnancies, and the practice has been linked with an increase in cesarean and instrumental births without an associated improvement in perinatal outcomes. The AAN instead recommends intermittent auscultation — checking the fetal heartbeat for at least a minute with a hearing device following a series of contractions. The organization says this allows women more freedom of movement during labor, which enhances their ability to manage labor pain and uses gravity to speed labor. Keeping older adults bedridden during hospital stays: Cox said, although for years bed rest was thought to be essential for overcoming illness or injury, evidence shows a lack of walking increases the length of hospital stays, leads to more rehabilitative services and increases the risk of falling after being released from the hospital. AAN says older adults who walk during their hospital stays are discharged from the hospital sooner, recover more quickly from surgery and have improvement in their ability to perform basic daily activities. Using restraints with older hospitalized patients: Cox said older patients are restrained in hospitals at a much higher rate than other adults. She said restraints do not keep people safe from falls or injuries, but have a negative impact on physical, psychological and recovery outcomes. AAN says that restraints are often used with older adults when they have behavioral expressions of discomfort or have a change in medical status. Instead the organization says by working with multidisciplinary teams and geriatric nurses as well as the patient’s family and other care-givers, nurses can anticipate, identify and resolve problems without the use of restraints. Waking patients for routine care when their condition or care doesn’t require it: Despite the long standing perception that patients must be monitored at specific intervals around the clock, Cox said studies show sleep deprivation hurts cognitive and physical function, breathing, circulation, hormonal function, metabolism and the immune system. Placing or maintaining a urinary catheter without a specific indication to do so: Cox said catheter-associated urinary tract infections are among the most common health care-associated infections in the United States, and they can lead to serious complications. AAN says these infections can be prevented by reducing use of in-dwelling urinary catheters and removing catheters as soon as possible. “This represents an important milestone for the effort, as patients rely on the trusted voice of nurses to help them navigate a world filled with increasingly complex health information,” said Daniel Wolfson, executive vice president and COO of the ABIM Foundation, in announcing the initiative Thursday (Oct. 16). “The new Choosing Wisely list from the Academy will serve as a guide for conversations between patients, nurses and all members of the care team in identifying the best course of care for each individual patient.” AAN has not yet determined which five states it will expand its Choosing Wisely pilot program to, following the roll out in Texas. — Todd Allen Wilson CA Duals Demo Opt-Out Higher Than Some Expected . . . begins on page one California, Illinois, Massachusetts and other states participating in the demonstration automatically, or “passively,” enrolled beneficiaries, although the National Senior Citizens Law Center earlier this year asked CMS and California to suspend passive enrollment because of a number of problems. Amber Cutler, a staff attorney with the NSCLC, said CMS and the states have addressed many of the passive enrollment problems NSCLC brought up, but the problems have not necessarily been eliminated. She added that California’s opt-out rate is higher than the advocates had expected. California has been phasing in passive enrollment by county since April, and the California Department of Health Care Services’ website says the opt-out rate for the program, including voluntary disenrollment, was about 44 percent, and it reached almost 50 percent in Los Angeles County. Lisa Rubino, senior vice president for Medicare, duals and exchange at Molina Healthcare, said opt-out rates in Molina plans participating in duals demos range from 25 percent in Illinois to 50 percent in California. Those numbers are within the expected range for those states, Rubino said. When Molina created the expected rage, it looked to its experiences with dual eligible special need plans and Massachusetts’ opt-out rates, which were lower. It’s hard to know exactly why the opt-out rates differ between demonstrations, Rubino said, but the size of INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 13 California’s demonstration — which is the biggest in the country — could be part of the reason. Rubino said it’s also important to remember that this is a three year demonstration, and it’s only really been running for a few months. A CMS official recently echoed those sentiments. The agency is tracking the number of opt outs, but it’s too early to release those numbers, the official said. CMS is studying the reasons for opting out, including whether doctors are influencing beneficiaries. Rubino said some doctors tell beneficiaries they will no longer treat them if they participate in duals demos. That’s not helping, Rubino said, and Molina is educating beneficiaries about the benefits of the program. This is occurring in both California and Illinois, she said, despite the fact that there are protections for beneficiaries around continuity of care. Molina is looking to mine fee-for-service data for providers serving dual eligible beneficiaries and create contracts with them to help increase continuity of care, Rubino said. Cutler said the NSCLC has heard anecdotally of doctors talking patients out of joining the demonstration in California, particularly in LA county. However, it’s difficult to determine the prevalence of that practice, she added. The CMS official said a certain amount of opt-out is healthy for those who feel served by the current system and have put together their own network of providers in Medicaid and Medicare. Cutler said it’s also important to account for the disenrollment rates of those who participate in the demonstration before deciding to leave. The reasons for not participating could be different for those who try out the demo before disenrolling, compared to those who opt-out before enrollment. However, with the real focus on implementation issues that have come from passive enrollment, there isn’t yet a real sense of how the demonstration is working once people are involved. — Michelle M. Stein Arbitrator Would Set Rx Prices If Deals Not Reached . . . begins on page one to make drugs more affordable to patients. There has been some talk of spreading the cost of expensive drugs over decades, much like a house mortgage, but plans don’t like the idea much and say the drug industry is pushing the idea, yet the Pharmaceutical Research and Manufacturers of America hasn’t responded to repeated requests for its position on that approach. Loren Adler, research director at the Committee for a Responsible Federal Budget, said he highlighted the old Health Affairs article because he believes the binding arbitration proposal could offer a compromise. “It has the benefit of possibly hitting the sweet spot between free-rein pricing on the backs of a government-imposed monopoly (through patent protection) and calls for government price setting, by focusing on unique, noncompetitive drugs and giving both sides a chance to present their case,” he wrote in an email. Neither PhRMA nor the Campaign for Sustainable Rx Pricing, which is the lead organization blasting hepatitis C drug prices, responded for this article. Richard Frank, a health economics professor at Harvard Medical School, and Joseph Newhouse, a health policy professor at Harvard University, wrote the article about six years before FDA approved Gilead Science’s first breakthrough drug for hepatitis C, Sovaldi, yet they anticipated much of what plans are warning about now. “PDPs’ ability to negotiate lower prices for unique drugs is limited,” they wrote, referring to prescription drug plans. “In the Medicare context, there will surely be strong political pressure not to allow PDPs to leave unique (and presumably superior) products off the formulary. Thus, the threat of exclusion from coverage because of a high price is unlikely to be credible and, because of the formulary regulations, may even be precluded.” While Frank and Newhouse raised concerns with Medicare Part D’s ability to handle high-priced drugs, in recent months commercial plans and Medicaid directors have done most of the complaining of high drug prices because Medicare protects private Part D plans against unexpected high drug spending. In fact, the authors say those extra protections for plans expose tax payers that much more because neither plans nor beneficiaries nor drug makers have much to loose when drug companies hike prices. “The combination of patent protection, lack of competitor drugs, and insurance coverage for a high percentage of the patient’s cost effectively puts the patent system on steroids,” the authors say. They propose a process that encourages the government and drug manufacturers to negotiate but does not let CMS or drug makers determine take-it-or-leave prices. In the case of drugs with no close substitutes (like Harvoni), the government and manufacturers would be given a deadline to negotiate a price. If they fail to agree on a price, they would enter into binding arbitration similar to the process used to negotiate salaries for baseball players. Drug makers and the government likely would choose an arbitrator, each side would present their cases and suggest a price, and the arbitrator would set a price.—John Wilkerson 14 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 Vit als: A Vitals continued on next page Health P olicy Blog Po Excerpts of Inside Health Policy Blogs Medicare Spending Decline Could Reverse With Swell Of Specialty Drugs The slowdown in Medicare spending is largely due to a slowdown in drug spending that might very well reverse itself if the swell of specialty drugs drives up spending as much as some predict, an article in Health Affairs states. The authors, both analysts at the nonpartisan think tank Committee for a Responsible Federal Budget, write that the disproportionate role played by prescription drug spending has somehow mostly escaped attention. “Despite constituting barely more than 10 percent of Medicare spending, our analysis shows that Part D has accounted for over 60 percent of the slowdown in Medicare benefits since 2011 (beyond the sequestration contained in the 2011 Budget Control Act),” analysts at the write. The outsized role of drugs in the recent Medicare spending slowdown might be bad news, they write. The socalled patent cliff is primarily responsible for lower Part D spending — many blockbuster brand-name drugs lost patent protection in recent years. “It is unclear whether these trends in the prescription drug market will continue or are temporary phenomenon — with the recent rise of specialty drugs, highlighted by the $1,000/pill Hepatitis C treatment Sovaldi, the tide may already be shifting. Moreover, it is unclear that a permanent Rx drug technological slowdown would be a positive development, even if it meant lower costs. — John Wilkerson Study Finds Wide Gaps In Health Literacy Among Americans Three-quarters of those surveyed by the American Institutes for Research (AIR) said they have a strong understanding of how to use health insurance, but only one in five were actually able to correctly calculate how much they would owe for a routine doctor’s visit when faced with copayments, deductibles and co-insurance. The new survey highlights a literacy gap that the authors say could result in many Americans dealing with unexpected out-of-pocket expenses. “Because many people believe they know more than they actually do about health insurance, they may not fully understand their options before committing to a particular health plan, or they may face the shock of high out-of-pocket expenses they didn’t expect,” study co-author Kathyrn Paez, a principal researcher at AIR, said in a release. The survey also found that younger people, those with lower incomes and minorities, have less knowledge because they are all less likely to be insured. However, as Paez notes, they are the groups most likely to use the health insurance marketplace. The survey of 828 adults aged 22-64 looked at four key pieces of health insurance literacy, including knowledge of terms and concepts, information-seeking skills, document literacy and reasoning skills. On average, the respondents answered 60 percent of the knowledge and skill items, although they were much more familiar with more common terms, such as “premiums,” than with more complex issues like “step therapy,” the survey found. Many had little understanding of plan types, with about half able to identify a health maintenance organization (HMO), and 23 percent able to identify the characteristics of a preferred provider organization (PPO). — Amy Lotven NCQA Report Shows Mixed Bag On Provider Performance Health care providers improved on some quality measures in recent years, but performance was a mixed bag, a report by the National Committee for Quality Assurance states. Provider performance improved steadily on nearly half of the measures, but progress stalled in many areas and progress on a handful of measures showed consistent, significant decline. The number of people enrolled in plans that report quality results doubled in the past 11 years to more than 171 million, which accounts for 54 percent of the U.S. population. “That means more Americans than ever can benefit from the accountability that public reporting of quality results brings. Providers, payers, consumers and others also have more insight into health plan performance than ever before,” an NCQA release states. There were a few bright spots on the use of antibiotics. For the first time in seven years, providers improved performance on an antibiotic use measures. However, performance remained low on other measures of judicious antibiotic use. There also were poor results on behavior-health measures, with a bright spot: More kids with attention deficit hyperactivity disorder received recommended treatment. Performance on mental-health and addiction treatment was weakest. “Fortunately, a proliferation of new measures is bringing needed attention to behavioral health and has the potential to improve care in this vital area,” the NCQA release states. — John Wilkerson Public Citizen Alleges FDA Is Hiding Opposition To Journal Reprint Guide Public Citizen thinks FDA is subverting the public feedback process by not posting comments on recent guidance that proposes to let companies communicate new information about risks and benefits not included on drug labeling. The group, which opposes the guidance, points out that since the comment period for the document closed in August, FDA has posted one of the 1,781 comments it received. In a letter sent to HHS Wednesday (Oct. 22) Public Citizen also calls for the withdrawal of the guidance. The draft guidance lays out recommended practices for the distribution of reprints or digital copies of articles that include new risk information for drugs not included in FDAapproved labeling. The comment period closed Aug. 25, and Public Citizen filed a Freedom of Information Act request INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 15 Oct. 15 for the full text of all the comments. “The draft guidance ultimately lets the pharmaceutical industry tell doctors that medications are safer than they really are. If finalized as written, it will be very dangerous to public health and safety,” said Sidney Wolfe, senior adviser of Public Citizen’s Health Research Group. “It is likely that a large proportion of the 1,780 undisclosed comments are in objection to this reckless proposed FDA guidance. By not making these comments public, it looks as if the FDA is trying to cover up opposition to the inherent dangers of the proposal.” Public Citizen has been critical of FDA’s proposal, saying the agency is cowing to industry by permitting companies to under-emphasize the significance of certain risks that appear on FDA-approved labeling. The group sent a letter to HHS Secretary Sylvia Burwell this week requesting HHS step in and require FDA to withdraw the guidance. However, key industry groups like the Medical Information Working Group and Pharmaceutical Research and Manufacturers of America said they believe the FDA guidance sets too high of a bar for disseminating efficacy information and goes against recent court rulings protecting commercial speech. — Stephanie Beasley Michigan Becomes Fourth State To Enact ‘Right To Try’ Law Michigan Friday (Oct. 17) became the fourth state to enact a “Right To Try” law allowing patients access to experimental treatments without FDA approval, according to the Goldwater Institute, a group backing state-level action on the issue. The new law comes on the heels of similar laws in Colorado, Louisiana and Missouri. The new Michigan law allows patients suffering from advanced illnesses to receive experimental treatments if other therapies have failed, and such treatment would only be allowed under a doctor’s supervision. Medical professionals and health care facilities are protected from liability if there are negative drug outcomes. “Allowing Michiganders dealing with extremely difficult medical situations to try alternative treatment options could extend or save their lives,” said Michigan Gov. Rick Snyder (R), who signed the state’s “Right To Try” bill into law last week. The law follows a recent push from the Goldwater Institute for FDA to treat all experimental drugs the way the agency has been treating experimental Ebola drugs. [79376] “Terminally ill people don’t have time to wait for new drugs to make their way through the decade-long approval process,” said Darcy Olsen, president of the Goldwater Institute. “Right To Try lets patients work directly with their doctors to access promising investigational medicines now.” — Erin Durkin Senate Approps, House Oversight Panels Plan Ebola Response Hearings Senate Appropriations Chair Barbara Mikulski (D-MD) announced a full committee hearing Nov. 6 in Washington on on the U.S. government response to the Ebola outbreak. The Senate hearing follows a similar probe last week by the House Energy and Commerce Committee. On the House side, the Oversight Committee will hold a hearing Friday (Oct. 24), despite the congressional recess, 16 examining whether the government is adequately training and equipping American health care workers and military personnel who treat patients infected with the deadly virus. Mikulski’s move to get the appropriations panel more directly involved in understanding the government-wide response comes shortly after Congress approved a spending package that includes devoting funds at the behest of the Obama administration to fighting the spread of Ebola, particularly in West Africa. — Christopher Cole Two Republicans Want Congress To Reconvene, Address Ebola Sen. David Vitter (R-LA) and Scott Garrett (R-NJ) asked congressional leaders to reconvene to coordinate a response to the ongoing Ebola outbreak, with the lawmakers advocating a travel ban as other lawmakers on both sides of the aisle have done recently. Separately, the House Oversight and Government Reform Committee will hold a hearing Friday (Oct. 24) to examine the government’s response to the outbreak. Criticizing the administration’s reaction to the outbreak, the two Republicans called for legislation. “Congress must vote on legislation to implement commercial flight restrictions on African countries affected by the Ebola virus,” according to the letter, sent to Senate Majority Leader Harry Reid and House Speaker John Boehner. “This would be a common-sense step to prevent the spread of Ebola.” The House Energy and Commerce Committee’s oversight panel held a hearing this week and the administration, including FDA, touted efforts to combat the outbreak. — Alaina Busch McBournie Judicial Watch Sues DC Exchange Over Congress’ SHOP Enrollment The conservative consumer group Judicial Watch on Wednesday (Oct. 15) filed suit against the District of Columbia’s health insurance exchange on behalf of a DC resident, arguing that exchange officials encouraged lawmakers, staffers and their dependents to enroll in coverage through the small business exchange (SHOP) even though access is supposed to be limited to employers with fewer than 50 workers. The suit says that officials looked the other way as congressional offices filed papers claiming that they employed 45 workers, even though Congress employs upwards of 20,000 people. The plaintiff, DC resident Kirby Vining, received the exchange applications through a Freedom of Information Act request filed last month. “The documents we obtained from the D.C. Health Exchange show that every member of Congress who has enrolled in Obamacare has obtained their insurance coverage (and any taxpayer subsidies) through fraud,” Judicial Watch President Tom Fitton alleges. “The District of Columbia government should not be a party to this fraud and should stop allowing Congress to participate in an exchange created for small D.C. Businesses,” he adds. According to the suit, the DC SHOP has enrolled 12,359 members of Congress or their staff and dependents, which equals 86 percent of the 14,289 people who enrolled in the exchange. The suit charges that exchange officials, who were also named in the suit, encouraged and helped congressional INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 staffers enroll in coverage in the DC exchange, which the suit says was built using funding from DC taxpayers. Under the ACA, congressional members and staff must enroll in coverage offered through a health insurance exchange, which created fears that staffers would lose their access to employer-sponsored health benefits because such contributions cannot be used in the individual exchange. A final rule by the Office of Personnel Management released in September 2013 said that eligible staff may enroll through SHOP and that the congressional office may be considered “qualified employers” regardless of the size requirements in the definition of a qualified employer as long as the office offers coverage of full-time employees who are purchasing coverage from the exchange for the purpose of receiving the government contribution, CMS explains in a Sept. 30, 2013 frequently asked question document. — Amy Lotven CMS Awards $29.1 Million In Exchange Grants To Three States CMS awarded approximately $29.9 million in “level one” exchange establishment grants to Massachusetts, Rhode Island and Virginia, coming as the establishment grants authorized under the Affordable Care Act will be phased out as of Jan. 1, 2015, after which state-based exchanges must be sustainable on their own. States may continue to use money allocated in 2014 for certain projects throughout next year, CMS has said. Rhode Island received $5,874, 736 to continue working its exchange by “improving and enhancing” its processes and IT systems, according to CMS. Specifically, the funding will be used to create contact center “pop ups” that will help reduce wait times during peak enrollment times, deploy mobile assisters to help renew coverage for about 25,000 people, improve health literacy, support consumer service representatives by providing access to a Deloitte-staffed contact center technology team, build an automated consumer premium refund functionality, and build new functionality for financial data. Rhode Island has received eight exchange grants — including a planning grant, an early innovator grant, five “level one” grants and a “level two” grant.] Massachusetts Commonwealth Health Insurance Connector Authority received $13.9 million to support the educational efforts to help transition residents to Affordable Care Act plans. “Funding from this grant will support a multifaceted outreach and enrollment campaign that includes direct mail and phone calls, public awareness events and application events, a statewide advertising and marketing campaign, and development of a training computer based environment for internal and external stakeholders,” according to CMS. Massachusetts has received six grant awards, including a planning grant, an early innovator grant, three “level one” grants and one “level two” grant. Virginia’s Department of Medical Assistance Services received $9.3 million in funds that will be used to establish an agreement with Virginia’s Community Healthcare Association, which represents 28 federally qualified community health centers (FQHC) and one rural health clinic, to support in-person assisters who will work from those clinics on outreach and education efforts. Virginia has received a planning grant and three “level one” grants. The awards stem from an application round that ended on Aug. 15. Another deadline for grants passed on Tuesday, Oct. 15, leaving states one more opportunity, Nov. 14, to apply for funding. — Amy Lotven Citizens Against Gov’t Waste Seeks To Show Urgency For Biosimilars A poll sponsored by Citizens Against Government Waste shows that 77 percent of respondents think FDA should finish setting up the biosimilar pathway “right away without more red tape, so patients in this country can have access to these prescription drugs.” The poll, conducted by Lincoln Park Strategies, shows there is public interest in biosimilars and bringing down the cost of medications, said Elizabeth Wright, director of CAGW’s health and science division. Further, 78 percent of respondents said they agree, with 57 percent strongly agreeing, that health care costs are “out of control” and biosimilars could encourage competition and lower prices. Wright highlighted that industry stakeholders lack direction on labeling, naming and interchangeability. “I think people are getting anxious and we’re getting anxious,” she said. One thousand likely voters were interviewed as part of the poll, which was conducted from Sept. 30 to Oct. 2 through an Internet survey, according to the data, which was unveiled this week. “We wanted to sort of gauge where the public is on this,” Wright said. She interpreted the polling data as showing people are interested in the biosimilar pathway and want to see these products on the market. She highlighted the poll’s findings that 37 percent strongly support and 51 percent somewhat support the introduction of biosimilars in the United States, based on the fact that they have been offered as an alternative to brand drugs in European and Asian countries and have lowered costs by as much as 40 percent. The poll consisted of 26 questions and 14 percent of respondents associated as a strong Republican, 20 percent as an Independent and 22 percent as a strong Democrat, with various other levels of political association. The poll had a margin of plus or minus 3.1 percentage points and a 95 percent confidence level. “I think it’s a very consistent picture of where Americans are,” said Stefan Hankin president of Lincoln Park Strategies. Hankin noted that prescription drug costs are a concern for the majority of people and he pointed to data points showing that respondents think generic drugs are helpful in lowering healthcare costs and should be accessible. The poll comes as other stakeholders, including biosimilar developers, are clamoring for details about the new INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014 17 pathway, including information on reimbursement policies and health care provider outreach to prep the market. Consumer groups focusing on economic policies have been jumping into the debate around biosimilars in recent months as industry groups and interested companies have long lobbied states on substitution policies and the World Health Organization on a naming scheme. The global body is meeting this week to discuss its plan for distinguishable names via a biological qualifier attached to an International Nonproprietary Name. In July CAGW and other taxpayer-focused groups wrote FDA asking the agency to move the biosimilar pathway forward. The groups also raised concerns that the innovator biologic industry’s push for distinguishable names could slow FDA’s efforts to put the pathway in place. — Alaina Busch McBournie Industry Report: GPOs Are Ethical, Transparent & Can Self-Regulate A report released Monday (Oct. 20) by the Healthcare Group Purchasing Industry Initiative (HGPII) asserts that group purchasing organizations use ethical business standards that show the industry can self-regulate. The report comes in advance of a Government Accountability Office report, expected in November, that will examine whether GPO contracting practices led to generic drug shortages that forced hospitals to turn to compounding pharmacies. The report, written by law firm Arent Fox for HGPII, is the ninth in a series of annual reports that show HGPII participants adhere to a set of six principles that ensure ethical and transparent business practices for GPOs that are designed to provide quality healthcare products for hospitals while reducing costs. Report authors, former Rep. Philip English (R-PA) and former Sens. Byron Dorgan (D-ND) and Robert Bennett (R-UT), say the firm only produces the yearly ethics report for HGPII and does not lobby for the trade group. “This demonstrates that self-regulation can be and is effective,” Dorgan said during a web briefing on the report. “Our evaluation of that effectiveness each year is a demonstration that this works.” English said the report confirms that the 11 GPOs that participate in HGPII adhere to the initiative’s six core principles; scrupulously avoid conflicts of interests among their employees; keep administrative fees to 3 percent; use transparent bidding and awards processes; keep contract terms to between two and three years; limit “sole source” contracts; only bundle contracts for related items; promote innovative products; have internal grievance policies that protect whistle blowers; have active and accessible grievance processes for vendors; regularly conduct ethics and best practices training for employees; participate in yearly HGPII best practices training; and promote diversity among vendors they contract with. The 11 GPOs that participate in HGPII include Amerinet Inc., Children’s Hospital Association, GNYHA Ventures Inc., HealthTrust Purchasing Group, HPS, Innovatix LLC, MedAssests Inc., Novation LLC, Premier Inc., Texas Purchasing Coalition and Yankee Alliance. As part of their participation, the HGPII-aligned GPOs take part in the yearly report by submitting answers to a 100-question public accountability questionnaire; participate in follow-up interviews based on their answers to the questionnaire; undergo randomly selected site visits; and participate in the annual HGPII Best Practices Forum. “I believe the healthcare supply chain is currently more transparent, more accountable and more wedded to a culture of best practices and business ethics than at any time in history,” English said based on the report. “GPOs are continuing to apply new supply chain innovations to healthcare, while expanding their product and service offerings to members.” The report stated that 96 to 98 percent of hospital supply purchases are made through GPOs, and English pointed out that two of the industries largest firms are part of HGPII. Lee Perlman of GNYHA Ventures and chair of the HIGPII board said member GPOs take the process to implement ethical and transparent business practices very seriously. “We’re very, very proud to be the most transparent part of the healthcare supply chain ecosystem” Perlman said. “I think what we created now almost a decade ago is a standard as Congressman English indicated for what is self-regulation and transparency. We believe we do a terrific job everyday.” English said the report will be presented to Congress in December. Before that, however, it is expected that the GAO will release its report on the contracting practices of GPOs with compound pharmacies. The GAO report is a response to November 2012 letters from Democratic lawmakers Reps. Ed Markey (MA), Henry Waxman (CA), John Dingell (MI), Frank Pallone (NJ), Diana DeGette (CO), and Anna Eshoo (CA), seeking to determine whether GPO contracting practices led to generic drug shortages that forced hospitals to use compounding pharmacies to fill drug shortages. The letters came out of a House investigation of a 2012 fungal meningitis outbreak linked to a compounding pharmacy that left 12 people dead. — Todd Allen Wilson 18 INSIDE CMS — www.InsideHealthPolicy.com — October 23, 2014






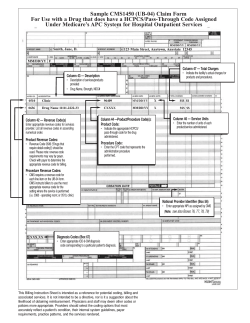



© Copyright 2026