
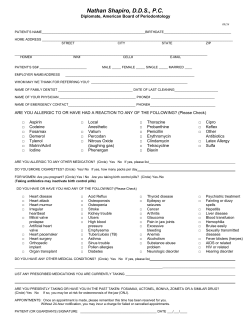
Acupuncture Medical History Form
MEDICAL HISTORY RECORD All information I Case No. Medicare is treated as confidential I No. Last Name First Address City Medicaid unless you grant permission No. Middle Daytime By Doctor Phone May I contact either of these Doctors for your past health records? Yes No IF LIVING Family History D D I Zip Phone all information. I Birth date D Male D Occupation Marital Status I Last Family or Referring I Doctor Physical Examination Date Phone No. What are your present medical symptoms? Any blood relatives who have or have had any of the listed conditions V Yes No Death Cause V Yes No Relationship Father Asthma Hay Fever Mother Arthritis Insanity Brothers (Circle Sisters Sex) Allergies Kidney Disease 1. M F Anemia Leukemia 2. M F Alcoholism Migraine 3. M F Bleeding Tend. Nervous Break'n 4. M F Cancer Obesity Colitis Rheumatism 5. M F D D Husband Wife Female Home Phone Relationship IF DECEASED r.-_l--:::-H_E-;-A-;::L,..,T,...H-;::---i Death Age Good Fair Poor Age I Date Daytime phone State Person to notify in emergency to release it. Please print and complete Today's Congenital Sons (circle Daughters sex) Rheumatic Heart Diabetes Stroke Relationship Fever 1. M F Epilepsy Suicide 2. M F Goiter Stomach 3. M F High BI. Press. Tuberculosis 4. M F Heart Disease Ulcers 5. M F 6. M F Do You Smoke HABITS No Daily Consumption: _______ Pkqs, .0 0 _______ Cups .0 0 _________ oz. .0 0 v Yes Drink Coffee Drink Alcohol Drink Beer. 0 ________ oz. v .0 .0 Aspirin, Bufferin, Anacin 0 Barbiturates.... ....0 Antacids.......... Antibiotics . v Blood Thinning Cort~one Pills Cough Medicine Digitalis Fall Asleep Easily ..0 0 Birth Control Pills 'O Dilantin Hormones Awaken Early 0 Blood Pressure Pills 0 Insulin, Diabetic Pills O 0 MEDICATIONS v If Taken Operations you have had: Drugs you are allergic to: Diseases requiring Year you have had hospitalization Describe any serious injuries accidents you have had v WOMEN only: Are you still having regular monthly menstrual periods?.... Have you ever had bleeding between your periods? Do you have very heavy bleeding with your periods? Do you feel bloated and irritable before your period? Are you now on or have you ever taken the birth control pill? Have you ever had a miscarriage? Have you ever had a discharge from the nipple of your breast? Do you regularly have the cancer test of the cervix? How many children born alive.... __ How many stillbirths ................................•••..•....••.... How many premature births ............................••••... Date of last menstrual period ......••••... __ How many miscarriages . How many cesarean operations... .. . Any complications of pregnancy? (explain) Item 4702 Year .. .. .. -------------------- Yes 0 0 0 .. .0 .0 0 0 .0 No 0 0 0 0 0 0 0 0 v 0 Iron or Poor Blood Med 0 O 0 O Laxatives Phenobarbital... Shots...... 0 Thyroid Med. Tranquilizers 0 Sleeping Pills. .0 .. .. .. .. 0 0 0 0 v Vitamins Water Pills. Weight Reducing Other (Iist) 0 .0 0 .. Pills _ 0 .0 Serious illness not requiring hospitalization Year or When? _ When? _ When? When? When? Date of last test _ _ _ _ MEN only: Have you ever had: Loss of sexual activity? For how lonq? Treatment for genitals (private parts)?... Discharge from penis? Hernia (rupture)? Prostate trouble? v Yes 0 No 0 ......0 ....0 0 .. .0 0 0 0 0 _ MEN and WOMEN: Do you frequently have severe headaches V Yes No ...0 o ..... Have you recently (If yes, answer the following): Do they cause visual trouble? Do they awaken you at night? .. Do they hurt most in the back of the head and neck? 0 Awakens you at night? .. 0 0 Is relieved by antacid medications? 0 0 Is relieved with milk or eating? ...0 0 Occurs while eating or immediately 0 0 Is relieved by a bowel movement? .. ..0 0 Causes loss of appetite? V Yes No .. Does aspirin relieve them? V Yes No Do you frequently Have you ever fainted? .0 0 Have you ever had a convulsion? .0 0 Bleeding gums? Spells of dizziness? 0 0 Double vision? 0 0 Trouble swallowing? Spells of weakness of arm or leg? .0 0 Pains in ear? . .0 0 Hoarseness? 0 0 Nosebleeds? .0 0 Ringing in ears? Have you ever had shortness breath? of .. v Yes No Have you had pain or tightness in the chest which begins: .. .0 0 When exerting yourself? .. 0 0 When walking against a wind? .. Which awakens you at night? ..... ....0 0 Do you have a chronic cough? . ...0 .. Climbing a flight of stairs?.... Which causes you to cough? by wheezing? Have you ever coughed blood? .. .. Do you cough up much sputum? v Yes Have you had? Burning when urinating? .0 No .. . v Yes have: .. No 0 A sore tongue? .0 0 Nausea and vomiting? 0 0 0 Radiates down the arm? . ....... 0 0 Disappears When walking up a hill? . ......0 0 Occurs only at rest? 0 After a heavy meal? ...................... ......0 0 When walking fast? 0 0 When upset or excited? . ...... 0 0 When walking in cold weather? ..0 0 Palpitations. ...... .0 0 If you have chest pain or tightness .0 0 Do you sleep on more than one pillow? ................... .0 0 ....0 0 When or since when? ,Have you recently had: Pains in calves of legs when v Yes No 0 0 walking? .0 0 0 0 Cramps in legs at night? .0 0 0 0 Pain in the big toe? .. 0 0 Trouble starting to urinate? .0 0 Varicose veins? 0 0 Trouble holding the urine? 0 0 Phlebitis or inflamed leg veins? .0 0 0 0 Swelling in the ankles .0 0 0 0 To get up frequently at night? Passed a kidney stone? .. .. If you have had a change in bowel habit recently answer the following: When or since when? v Yes No Crampy pain in abdomen? 0 0 diarrhea and constipation? ..0 0 Pain during or after bowel movement? .0 Alternating Mucous in the stool?... ......................0 0 0 Blood in the stool? .0 0 Ribbon like stools? 0 0 Black stools? 0 0 Require use of strong laxatives or enemas? .0 0 o 0 . No 0 0 o o v Yes No .. .. 0 0 ...0 0 . please explain When or since when? Describe briefly your present medical symptoms and anything else we should know about your health. o v Yes if you rest? Loss of control of bladder? . ...... .0 .............. 0 o .0 No 0 o ..................... .0 o . v Yes .................. o ................................ .0 o . after? ...............•........... .............•........ .. ....................... No 0 ............................. 0 o ............ .0 ............ .. .............................. 0 o . Blood in the urine? Dark colored urine? . V Yes ................. ........................... .0 ..0 .. Do they feel like a tight hat band? . Accompanied which: . Is brought on by eating fried foods, gassy foods? Do they occur on one side of the head? DOing your usual work? had pain in the stomach Occurs 1-2 hours after a meal? . 0 0 0 0 0 0







© Copyright 2026