
Document 108388
PRIMARY CARE
Revisiting the Use of Honey for
Treating Chronic Wounds
Ann Reese, M SN, RN, C W O C N , G N P ; Deborah Willoughby, PhD, RN, A C N S ;
Stephanie C. Davis, PhD, R N , FNP- BC; Toni Silver, RN, APN-BC, C W C N ; and
Tad Venn, MD
Honey was used as a wound dressing in ancient times but was
replaced by antiseptics and antibiotics in the 19th and 20th
centuries, respectively. Hone}' has recently regained favor—
with scientific evidence to back it up—as a treatment for
chronic wounds. Honey is being used lo manage venous,
al, diabetic, and pressure ulcers and burns, panicukjjffpThose
infected b}> methicillin-resistant StaphylococfigJ^iureus
vancomycin-resistant enLero&gd.'&to^^mJstiave
an evidence-based revi0tajOjUngS^^^^ical-grade
chronic wounds, andMiffojMH^BHRions
findings for nurse pi
•'"•""i'.'.'B'
r
0
performed
hone}'for
of these research
O
ne percent to 2 % o f the inhabitants o f developed countries
have a chronic w o u n d In the
United States, more than 6 m i l l i o n
c h r o n i c w o u n d s are treated each
year, at a cost o f >520 b i l l i o n . "
Wounds are considered chronic if
Lhey do not heal w i t h i n 3 months/
D e p e n d i n g o n the cause, chronic
wounds may be classified into one
o f four categories: venous ulcers,
arterial ulcers, diabetic ulcers, and
pressure ulcers (Table i ) . Venous
ulcers, w h i c h occur as a result o f
chronic
venous
insufficiency,
account for about o n e - h a l f o f
chronic lower-extremity wounds,
and affect 0.14%-2% o f the popul a t i o n . " Arterial ulcers result f r o m
poor arterial perfusion and comprise ~ 2 5 % o f leg ulcers.' Diabetic
ulcers occur in patients w i t h diabetes mellitus ( D M ) and art due to
impaired circulation and sensation
in the lower extremities. The prevalence o f foot ulcers in patients with
DM is 12.7%." This patient group
also has a l i f e t i m e risk o f 15%2 5 % o f developing a lower-extremity ulcer, m a k i n g D M the wading
cause o f n o n - t r a u m a t i c amputations in the United States. Pressure
ulcers are caused by unrelieved pressure or shear, which causes damage
to the tissue: the prevalence of pressure ulcers rises w i t h age.'
•
27
PRIMARY CARE
Treatment o f chronic w o u n d s
poses a challenge. A favorable outcome, represented by a healing
wound, depends o n maintaining a
moist w o u n d bed, removing necrotic tissue w i t h o u t h a r m i n g healthy
tissue, and preventing and treating
infection. Some readers may be surprised to learn that the application
o f honey to chronic w o u n d s has
been shown to facilitate a healing
w o u n d environment.'•'
The use o f honey as a treatment
for wounds dates back to the time
o f the ancient Egyptians and
Creeks." Therapeutic use o f honey
was abandoned i n the latter half o f
the 19th century and early 20th
century following the i n t r o d u c t i o n
o f antiseptics and then antibiotics.
However, the d e v e l o p m e n t
of
m u l t i - d r u g - r e s i s t a n t bacteria and
the rising incidence o f chronic
wounds have led to a reconsiderat i o n o f the use of honey i n treating
wounds.
:
1
The US f o o d and O r u g A d m i n i s t r a t i o n has approved t w o
therapeutic honeys for use i n this
country. Medihoney Antibacterial
Medical Honey and Active Manuka
Honey. Both honeys are derived
f r o m the m a n u k a bush in NewZealand (also k n o w n as Leptospermum scoparium). These honeys
have been sterilized, but not inactivated, through gamma irradiation,
w h i c h destroys Clostridium spores.
I TABLE 1
The honeys contain a unique manuka factor, w h i c h gives t h e m a d d i t i o n a l antibacterial activity and
distinguishes t h e m as therapeutic
honeys. These honeys are safe, easy
to use, and cost effective, and have
emerged as w o u n d treatments that
can achieve a variety o f therapeutic
outcomes.••' O f note, culinary
honey purchased i n a supermarket
is not medical grade and not suitable for this use.
Some NTs may be unaware o f
recent research supporting the use
of
honey
in w o u n d
care."
A l t h o u g h evidence suggests that
honey is beneficial in treating
acute w o u n d s , this integrative
review examines the use o f honey
as a treatment for chronic wounds,
identifies indications for the use of
honey in this regard, describes the
a p p l i c a t i o n procedure, and discusses parameters that must be
m o n i t o r e d as indicators o f treatment effectiveness.
Honey-making Pnxess
Bees collect nectar f r o m flowering
plants and then transport the nectar to worker bees in a hive,
Hnzymes in the worker bees' stomachs, t w o o f w h i c h are i m p o r t a n t
to w o u n d healing, break d o w n the
nectar so that it is b o t h more
digestible for the bees and less like!v to be attacked bv bacteria w h i l e
stored i n the hive. The first
enzyme, glucose oxidase, converts
glucose to gluconolactone, w h i c h
yields gluconic acid and hydrogen
peroxide. The second enzyme, catalase, w h i c h is active i n l. scoparium,
helps manage biobimlen (ie, the
a m o u n t o f bacteria or. a w o u n d
surface before it is sterilized) i n
w o u n d f l u i d , tissue, b l o o d , and
other b o d y f l u i d s .
Bees then
spread the nectar t h r o u g h o u t the
honeycombs, where some o f the
water evaporates f r o m it, resulting
in honey.
Therapeutic Effects of Honey
H o n e y affects w o u n d healing
through five modes o f action: (1)
a n t i m i c r o b i a l properties, (2) antii n f l a m m a t o r y properties, (3) prom o t i o n o f w o u n d debridement
w i t h eschar or slough, (4) provision o f a moist w o u n d e n v i r o n ment, and (5) reduction o f w o u n d
m a l o d o r . ' ' A l t h o u g h the mechanisms by w h i c h honey exerts its
therapeutic effects are n o t well
understood,
researchers
have
s h o w n that it exerts antimicrobial
effects against even antibiotic-resistant bacteria.'
Honey, even w h e n diluted to a
5 % concentration, has been shown
to be effective against clinical isolates o f m e t h i c i l l i n - r e s i s t a n t
Staphylococcus aureus (MRSA), S
TYPES OF CHRONIC WOUNDS
Type
Cause
Comment
Venous ulcers
Chronic venous insufficiency
Account for about one-naif of chronic lower-extremity wounds; affect 0.14%-2% of
the population
Arterial ulcers
Poor arterial perfusion
Comprise -25% of leg ulcers; may not heal as well with honey therapy
Diabetic ulcers
Impaired circulation and
sensation in lower extremities
12.7% of patients with DM have foot ulcers; lifetime risk of developing a lowerextremity ulcer omong patients with DM Is 15%-25%; leading cause of non-traumatic
amputations in the United States
Pressure ulcers
Unrelieved pressure or shear
Prevalence rises with age
aureus, vancomycin-sensitive enterococci (VSE), vancomycin-resistani enterococci (VRE), Pseudomcmas
aeruginosa, beta-hemolytic streptococci, Alcaligenes faecalis, Cilrobacter
freundii, Escherichia colt, kmerobacter
aerogenes, Klebsiella
pneumoniae,
Mycobacterium
phlei,
Salmonella
California,
Salmonella
enteriiidis,
Salmonella typhimurium,
Shigella
sonnei, Staphylococcus
epidermidis,
Staphylococcus capitis, Staphylococcus
haemolyticus, Staphylococcus
simulans, and Staphylococcus
warneri.'"
-"• To date, honey has n o t been
s h o w n to i n h i b i t the g r o w t h o f
Serratia marcescens or Candida albicans, or to i n h i b i t the g r o w t h o f
Pseudomonas aeruginosa i n patients
w i t h cystic fibrosis.
1
14
Several properties o f honey are
thought to play a role in its a n t i m i crobial activity. The acidic p H (3.24.2) of honey may help stimulate
Fibroblast activity w i t h i n
the
w o u n d . " Honey's osmolarity pulls
intracellular fluid into the w o u n d ,
w h i c h dilutes the honey. Glucose
oxidase is then activated, w h i c h
produces hydrogen peroxide at l o w
levels, thereby decreasing bacterial
g r o w t h . The hydrogen peroxide
produced is 1000 times lower than
the 3 % s o l u t i o n typically used to
clean w o u n d s , ' " but even at this
l o w concentration, the hydrogen
peroxide maintains its a n t i m i c r o bial activity." '
1
The antibacterial effect
of
honey is d e t e r m i n e d by its p l a n t
source a n d how it was processed."
ViuJlai and Menon ~ compared the
antibacterial activity o f four different types o f h o n e y — k h a d i k r a f t
honey, m a n u k a honey, heather
honey, and local honey f r o m beekeepers i n a south I n d i a n v i l l a g e —
against a total o f 152 strains o f
Pseudomonas cultured f r o m diabetic ulcers, infected burns, a n d
b l o o d . The four honeys were d i l u t -
ed w i d i sterile Mueller-Hinton agar
to o b t a i n concentrations ranging
f r o m 1 % to 25%. N u t r i e n t agar
w i t h o u t honey served as the
growth control and chloroxylenol
was the antiseptic c o n t r o l The
lowest concentration o f honey that
prevented g r o w t h on the isolates
was recorded as the m i n i m u m
inhibitory concentration ( M I C ) .
Khadikraft honey was the most
effective against P aeruginosa, w i t h
an M I C o f 11%; an M I C o f 2 0 %
was needed for the other three
honeys. Pseudomonas species are
frequently resistant to a n t i m i c r o bial therapy, but honey that has an
M I C o f 10%-20% is effective i n
preventing its growth in wounds. "
A l t h o u g h chronic i n f l a m m a t i o n appears to decrease w h e n
honey therapy is used, c l i n i c a l
studies have not been able to clearly identify h o w this anti-inflammatory effect occurs." Monocytes are
activated by honey to release interl e u k i n (II.)-6, I L - 1 , and t u m o r
necrosis factor-1.' Pain is reduced
in the w o u n d because o f the
decreased edema, w h i c h improves
circulation. S u b r a h m a n y a m et a f
compared honey w i t h silver sulfadiazine in a r a n d o m i z e d c o n t r o l l e d trial ( R C I ) i n 60 patients
w i t h burns, and f o u n d that honey
decreased free radicals stimulated
by excessive i n f l a m m a t i o n , thereby
reducing scarring.
W o u n d debridement by honey
has been n o t e d t h r o u g h several
mechanisms. Autolytic debridement occurs because o f the extra
moisture pulled f r o m l y m p h f l u i d .
The o s m o t i c action cleanses the
w o u n d base and softens slough
and necrotic tissue
Hydrogen
peroxide p r o d u c e d by honey
chemically also debrides the
w o u n d ; the honey reacts w i t h ferrous ions, p r o d u c i n g the radical
hydroxy!, w h i c h causes antibacteri4
11
al activity.••' In an RTC comparing
the effectiveness o f manuka honey
and h y d r o g e l dressing in 73
patients w i t h necrotic lowerextremity ulcers infected w i t h S
aureus ( n = 41), MRS A (n = 16), or
P aeruginosa ( n = 16), MRSA was
eliminated i n 70% o f the manuka
honey-treated w o u n d s versus 16%
o f the hydrogel-treated w o u n d s
after 4 weeks.' P aeruginosa was
eliminated i n 3 3 % o f honey-treated w o u n d s versus 5 0 % o f the
hydrogel-treated w o u n d s . The
authors concluded that w h e n the
slough is d e b r i d e d and MRSA is
e l i m i n a t e d , the i n f e c t i o n rate is
decreased.
The moist environment cieated
by the honey protects the w o u n d ,
reduces i n f e c t i o n rates, reduces
pain, debrides necrotic tissue, and
promotes g r a n u l a t i o n tissue form a t i o n . ' ' E p i t h e l i a l i z a t i o n can
occur o n the surface o f the w o u n d
rather t h a n below the eschar, as
occurs in dry wounds. The w o u n d
bed is protected by honey's h i g h
viscosity, w h i c h provides a barrier
to i n f e c t i o n , and by the osmotic
activity o f honey, w h i c h promotes
autolytic and mechanical debridem e n t . " ' H o n e y also
reduces
w o u n d odor. W h e n honey is used
to treat w o u n d s , glucose, rather
than a m i n o acids, is produced as
the bacteria metabolize serum and
dead cells. Lactic acid is then produced, w h i c h is less m a l o d o r o u s
d i a n a m m o n i a , amines, or sulfur
compounds.'
2
4
Synthesis of the Literature
A systematic literature search was
done using the electronic databases C I N A H I . a n d M e d l i n e and the
Web engine Google Scholar and
the key words honey, wounds, and
chronic wounds. Thirty-four articles
were reviewed and assessed for
v a l i d i t y The authors evaluated
RCTs and case series to ascertain
the effect o f honey o n c h r o n i c
w o u n d s such as l o w e r - e x t r e m i t y
ulcers, pressure ulcers, bums, diabetic ulcers, and s l o w - h e a l i n g
wounds i n oncology.
Lower-extremity U l c e r s — I n a
comparative study, C e t h i n a n d
C o w m a n - ' used manuka honey to
treat 8 patients w i t h c h r o n i c leg
ulcers that h a d n o t s h o w n
i m p r o v e m e n t w i t h other w o u n d
care for 4 weeks. W o u n d o d o r was
e l i m i n a t e d after the first h o n e y
a p p l i c a t i o n , p a i n d u r a t i o n was
decreased f r o m 2 hours to 30 m i n utes (per patient report), and the
size o f the w o u n d was reduced by
5 4 . 8 % after 4 weeks o f therapy.
Smith et al-'" applied Medihoney to
11 chronic lower-extremity venous
ulcers that had failed to respond to
various treatments, i n c l u d i n g compression, topical silver, n o n adherent dressings,
and a n t i b i o t i c
therapy. A l l o f the w o u n d s healed
after 3-6 weeks o f continuous treatment. Robson et a l ' f o u n d that the
average t i m e to h e a l i n g was 100
days i n the Medihoney g r o u p versus 140 days i n the standard-therapy ( c o n t r o l ) g r o u p f o r lowerextremity ulcers.
5
In 3 case studies o f patients
w i t h leg ulcerations, use
of
M e d i h o n e y p r o m o t e d significant
healing over 2-8 weeks a n d
reduced pain (per patient report)
and infection (per repeat swab cultures) in ail cases." In a study o f 6
patients w i t h non-healing wounds,
use o f honey produced the favorable outcomes o f granulation and
reduction o f bacterial b u r d e n over
a mean of 4 weeks. ' One patient i n
this study w h o had been experiencing severe p a i n was able to stop
using an o p i o i d analgesic after 17
days o f honey gel treatment and n o
longer needed any analgesic after 6
weeks o f treatment. Use o f honey
achieved the goals o f reducing bacterial load, i n f l a m m a t i o n , and
pain. By contrast, i n a study conducted o n patients over a 12-week
time period, k i l l et a!-"' f o u n d that
honey w i t h compression, c o m pared w i t h compression alone, d i d
not significantly increase h e a l i n g
o f venous leg ulcers.
D i a b e t i c U l c e r s — H o n e y was
used i n an elderly man w i t h chronic diabetic heel and forefoot ulcers
o f 14 m o n t h s ' d u r a t i o n . " ' The
patient had lost t w o toes, had
undergone four surgeries, and had
been hospitalized 5 times i n
attempts to heal the ulcers.
Cultures o f the w o u n d were positive for MRSA, V'RK, and Pseudomonas, H o n e y was a p p l i e d daily;
after 2 weeks, g r a n u l a t i o n tissue
was noted. The ulcers resolved over
12 months.
Pressure
Ulcers—Van
der
W e y d e n used honey dressings to
treat 2 patients w i t h pressure
ulcers. One patient had a stage 3
ulcer a n d the other patient had a
stage 4 ulcer; b o t h patients' ulcers
healed after 8-11 weeks o f treatment. The patient w i t h the stage 4
sacral w o u n d had been treated for
4 weeks w i t h a hydrocolloid dressing, w i t h l i t t l e effect. However,
after 1 week o f honey treatment,
the necrotic tissue began to break
d o w n and after 3 weeks, the
necrotic tissue was gone. G r a n u l a t i o n tissue was noted after 4
weeks. The other patient had been
treated w i t h a hydrocolloid dressing for 3 weeks, w i t h no improvement. One week after starting the
honey dressing, improvement was
n o t e d , and after 23 days, the
w o u n d was shallow and granulating. A c t o n " used honey to debride
pressure ulcers, w i t h favorable
results. In one case in w h i c h a
necrotic pressure ulcer h a d been
present for ) m o n t h , the necrotic
w
tissue was absent after 5 days o f
treatment. I n another case, a
necrotic h i p w o u n d was clean after
8 weeks o f h o n e y use. A 5-week
RCT assessed the use o f honey i n
15 patients w i t h 25 stage 2-3 pressure ulcers versus e t h o x y - d i a m i n oacridine/nitrofurazone
i n 11
patients w i t h 25 stage 2-3 pressure
ulcers. The honey-treated group,
relative to the control group, experienced approximately 4 times the
rate o f pressure ulcer healing.
0
Burns—Subrahmanyam et al
treated 100 patients w i t h burns
w i t h a honey dressing or a silver
sulfadiazine dressing. At 7 and 14
days, greater healing was noted earlier i n the honey group than i n the
silver sulfadiazine group. The silver
sulfadiazine group showed persistent infection on bacterial cultures,
whereas cultures i n the honey
g r o u p were 9 0 % sterile. These
authors reported that 50 patients
w i t h b u m s treated w i t h early exci
sion and skin grafting instead o f
honey h a d better f u n c t i o n a l and
cosmetic results after 3 months.
W o u n d s in Patients
with
Cancer—Honey has been used to
treat s l o w - h e a l i n g w o u n d s i n
patients w i t h cancer, particularly i n
neonate a n d pediatric populations.
In a study by Simon et a l , honey
was f o u n d effective against nosoc o m i a l w o u n d infections. These
investigators studied w o u n d cultures g r o w i n g MRSA, VR1-, and P
aeruginosa f r o m 14 patients whose
slow w o u n d healing was related to
chemotherapy and radiation toxicity, m a l n u t r i t i o n f r o m nausea/
v o m i t i n g , mucositis, or infection.
Healing was noted after an average
use o f 22 days i n a l l w o u n d s .
Patients a n d their parents were
pleased w i t h the results.
, :
Implications for NP Practice
Assessment—The T I M E frame-
TABLE 2
FREQUENCY OF HONEY DRESSING CHANGES
Type of Honey Dressing
Amount of Exudate
Frequency of Dressing Changes
Honeycolloid
Light drainage
Change every 4-7 days
Honey gel/ointment
Light to moderate drainage
Cover wi*h an occlusive dressing and change daily
initially and every 2-3 days as drainage decreases
Honey alginate
Moderate to heavy drainage
Change daily initially and then extend to 2-3 days
as drainage decreases; change outer dressing pm
w o r k for w o u n d healing, developed by Schultz et a l , " focuses o n
preparing the w o u n d bed by m o d i fying factors that delay or prevent
healing. W o u n d - b e d p r e p a r a t i o n
includes management o f 4 factors:
T = nonviable or deficient tissue;
I = infection or i n f l a m m a t i o n ;
M = moisture imbalance; and
E = a non-advancing or undermined w o u n d edge.
NPs can use this framework i n the
office to aid i n assessment o f
w o u n d healing.
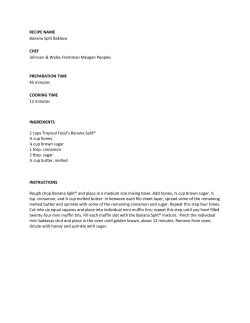
Choosing
an
\npropriate
Dressing — H o n e y dressings are
available i n different forms, the
type used depends on the a m o u n t
o f w o u n d exudate." W o u n d s are
first cleaned u s i n g a facilityapproved w o u n d cleanser. The
outei margins are protected w i t h
s k i n prep. Hie dressing is applied to
fit w i t h i n the w o u n d margins. For a
lightly d r a i n i n g w o u n d , use o f a
honeycolloid (non-adhesive) w i t h out a cover dressing is suggested.
For a lightly to moderately draining
wound, use of a honey gel/ointment
and an occlusive dressing designed
to maintain a moist environment is
indicated. One challenge w i t h use
o f a liquid/gel honey is ensuring
that i t stays in place; this preparat i o n may n o t be o p t i m a l for a leg or
a b d o m i n a l w o u n d . Frequency o f
dressing changes depends o n the
a m o u n t o f drainage (Table 2). A n
outer dressing that becomes saturated is changed p r o m p t l y to avoid
maceration o f the peri-wound skin
and to prevent c o n t a m i n a t i o n . As
drainage decreases, dressings are left
on for longer periods o f time, typically 4-7 days/ For moderately to
heavily d r a i n i n g wounds, another
available dressing is Medihoney, a
5 % calcium alginate and 9 5 %
Lepiospermum honey that is frequently used o n lower-extremity
ulcers under a compression w r a p . - "
1
5
A l t h o u g h honey is generally
safe w h e n used to treat wounds, a
few contraindications exist. Patients
w i t h a k n o w n history o f allergy to
honey or bee v e n o m s h o u l d n o t
use honey dressings. Patients w i d i
D M need to m o n i t o r dieir b l o o d
glucose levels m o r e frequently
because o f the risk for hyperglycemia.'" Furthermore, h o n e y
should not be used on stable, dry
eschar o n heels, as diis is the body's
natural protection, or on w o u n d s
that need surgical debridement/-'
Evaluation of Therapy--As
w i t h any topical dressing, these
questions must be answered w h e n
assessing the effectiveness o f honey
in treating a w o u n d : (1) Have redness and s w e l l i n g (ie, i n f l a m m a t i o n ) decreased? (2) Has p a i n
decreased? (3) What is the c o n d i t i o n o f the surrounding skin? Is it
improving? ( 4 ) Is the n u m b e r o f
dressing changes decreasing over
time? ( I f not, the honey may n o t
be effective because o f the amount
o f drainage.) (5) Has the necrotic
tissue d i m i n i s h e d ? (6) Is the
w o u n d odor decreasing? (7) Is the
treatment cost-effective? "' F.ven
t h o u g h honey has atuibacterial
properties, systemic antibiotics
may still be needed. M o n i t o r i n g
the w o u n d is required.
1
Implications for Education
Nurse practitioners and w o u n d
care nurses must be educated
about the use o f honey and its
i n d i c a t i o n for the treatment o f
chronic wounds. Honey dressings
are easy to apply, non-adherent to
the w o u n d base, and less p a i n f u l
than other dressings o n removal."
H o n e y can be used i n cavity
w o u n d s or a sinus tract because the
residual can be cleaned out at
dressing changes. 1 loney is appropriate for w o u n d s w i t h moderate
to heavy amounts o f drainage, w i t h
slough or eschar needing chemical
debridement, and w i t h an odor/'
Honey for w o u n d treatment must
be o f a medical grade that is regulated safe, effective, and cast-effective.
11
Implications for Research
Further studies specifically RCTs,
are needed to assess the use of
newly developed honey-impregnated dressings. According to Simon et
a f - many case studies, but o n l y a
few RCis, have been reported
PRIMARY CARE
regarding the therapeutic use o f
honey. More data are needed t o
assess the effect o f medical grade
honey at the molecular level (ie, its
antimicrobial and antioxidant
activity and elimination o f free radicals
within
the w o u n d ) . '
A d d i t i o n a l clinical studies are
needed t o d e t e r m i n e o p t i m a l
dosage regimens for antimicrobial
efficacy.'
11
Conclusion
Use o f honey as a treatment for a
variety o f wounds is supported by
research. 1 loney has antibacterial
activity against MRSA, Pseudomonas, a n d VRP,; i t also reduces
odor and helps debride w o u n d s .
Honey's anti-inflammatory activity
has been s h o w n to reduce edema
and exudate a n d m i n i m i z e scarr i n g . ' H o n e y can be r e m o v e d
painlessly w i t h use o f a non-adherent dressing. Use o f honey is gradually becoming more widespread
and may be w e l l received by
patients, w h o perceive i t to be a
natural product ' " •
1
of h o n e y o n 'planktonic' a n d b i o l i t m - e m b e d d e d
chronic
svound
bacteria.
S<:,ititl ]
Inject
-Mfcni C.ompiVmnit .\l,-,l. 2 0 0 7 ; ] s(-l j : 4 3 9 441
Ply
19. M o l a n P C lie introducing hones- in the m a n -
2009;41(3):341-347.
2
agement o f w o u n d s a n d iili:crs-lheory and p i a r ice
P a i d Np. l.raiiiik MS. kan.ik.uis NK, el al.
Comparison
of w o u n d
edutation
20
schools in the U n i t e d Stales. United Kingdom.. a n d
iiused C.'ifiiJ'leiifi-M.' Alli'rn,it
T h o m a s I )\ H a r d i n g k l , . W o u n d healing. ii< I
Werdin
H
leunenhaus
21. C o o p e r
M . Schallei Ml..
Rennekampff H O hvidetue-hast'd
1
Ueickoll I' l o n a s - "
- i * \ . u : M L . u ai
34
•
KA. Molan
I'C
Harding
\
Slaphylococeus .uiretis from irtecieci svounds I N
Surg. 2 0 0 9 : 9 169-177
S,i
3.
22. C u i t i n j ! K t Hones a n d u , nentporars- w o u t u l
t.ettmi C C o w m a n s. Hacteiiolotiical changes
\h',l.
1999:921 (i):2S.l-2S5.
;
in sloughy venous leg ulcers treated with m a n u k a
care
honey
J 0 0 7 . 5 if l i ) 4 9 ^4.
o r hsdioj>el
a n 111'I
H«»i<j
I
( i-mc
2 0 l W ; ! 7 t « . ; - 2 4 l 247
6
an
(isvri'ieiv
bum
2 0 0 1 : 1 4 ( 1 ) 141 1 4 i
7
24
C i i l j a m M l , Harper l)K, D a l e II. Kucktey C V .
A n e r i a ! disease in chronic leg ulceration: a n underulcer
Br
Med
I
(Chi
Re,
m a n u k a hones
C e n t e r s for Disease C o n t r o l a n d Prevention.
rtrein
2000-2002. t I M l V B
2d. S m i t h
Uo<b
in leg ulceration,
T.
l.t-fit'1
s e n o u s leg w o u n d s
tniY>t.
2007:1 ] V ( 5 ) 12,9-122.2.
K.
medical
l.t;9)'S22-S2^
t p-relimina^' case series . W r
Ostomy
2007:34(2) 1 84-190
25
hones:
fb / Cann.'ii,
i.t. l i c a o r . e n i tor w o u n d s
care
Her 2(io,s.s;4) C . r x k i s l k S i
a n o p t i o n ior care i n the U n i t e d duties. /
I V e i i i u i ' Ojlsmn U > t i : l w n < e \ N f < 2 0 0 9 V , ( } ) 00-bS
. " ) . f.ddy 1. C,ideonser
t . e i h m C I.llitaev of hor.ey .is a d e s i o u g h i n g
c:\ervitsv
:d a n i e n t
HVMA
honey
in c l i n i c a l
Hr
;
,
M lop.cai honey to: c i a 2tIL»7>::>4f d): ».>4 /i.Vs,
r
40. Van der Weyden KA. lite u v o f honey lot he
treatment of two patients w i t h pressure ulcers, i f ' /
lite u s e of m e d i c a l
practice
2O1IS:
I , M ' : M . " C i')iif,ll. ,i.;,' :.v>-|
betic loot ulcers / /-u.'i: /Vuci
200S:S(2):H-35.
I.1. A c t o n (.'. [ l u n s v o o d y C
grade
evidence.
\'i;,..
I..II A l i , ( W y c i s A. W a U c r N . I loney as a t - p ;
11. Pieper [I, H o n e y - b a s e d dressings a n d w o u n d
lauriMl.
|K. l o p i c . i i
27. Sare 11 U ' g ulcer m a n a p e m e i u svith topical
ing l o r h e a l i n g pressure ulcers. / llc-u.'tif
age:::
Ilaaft
Slrt'H tVeuilii l 2 I A ' 9 . 2 2 I 2 J : ( M I - 7 !
10. l . u u e s U . l i s e r i . P.lTeaiveness o f a h o n e y dress-
12
hi: S\'oi,i:,: ;
i x p l O S [ X t m u m h o n e y ( M e d i h o t K s ) ill r e i a k l t r u i l
11. T o m i c - C a n i c M . C e l l u l a r a n d m o l e c u -
Sun
l999;S(8):4l'i-
2005;.-(li:IO-i.S.
per:,;;:;:, w i t h dia-
lar basis of w o u n d healing i n diabetes. / C/i/i
(.ottUiMW
Cure.
L,i).
Mortal IV'Wi Rep. 2 0 n 3 ; s 2 ( 4 s ) : I 0 9 S n 0 2 .
•).
M o l a n K i . I h e role o f hones in the manrge-
2.S. ( , e t h m C ( . o w n u m s. (.iase series o f use o l
History o f fool u.cer a m o n g
b e t e s — t i n n e d Stales
A n n Jfcrns f - i v Ofdisiers.
41S
1987.294(C>>77):929-931.
H.
wound healing
rnenl o f s v o u n d s . I Wnunil
h a z a r d ' L o t h i a n a n d f o r t h Valley k g
study.
Md'nigc
el a l . fffects v>: topical a p p h : u i o n o f h o n e y o n
2003; 1(2): 14-20
estimated
lii'iiml
Dsivmy
23. S u b i a h m a n y a i u M . ^i.'.hapi re \ Naiiane \ s ,
Itugjcs M- C l o s s SI t h e p r e w i i e n c e o t leg u k e r -
a t i o n : a review ot the literature. f.U'\1.-\'
Sun. 200.1;8( 1 2 ) S ! 4 S 2 0 .
Cvmmunit)-
Nurs
.11
200ti:l 7 ( > 0 ) : S W - S 4 4
A t r o n C M e d i h u n e s : a complete ssoutid b e d
preparation
14. l.usbyPt.. C o o m b e s A , W i l l k i i i s u n 1M. Honey:
product
IJr / \rj.r..:.200iS:l 7( II j : S 4 4 -
S41S.
a potent agcnl for w o u n d h e a l i n g ' j Uemii/ Oidmiy
C o n n i i i T i c c A'urs. 2 0 0 2 : 2 9 ( 0 ) 2.9.s i J O .
32. S i m o n
IS
W o u n d care svith antibacterial honey ( M e d i h o n e y )
R o b s o n V. D o d d S, I h o m a s s. S t a n d a r d i z e d
antibacterial h o n e v (Medihotlt->)
w i t h standard
Mr
A, Sotka
in pediatric
therapy m w o u n d care: r a n d o m i z e d clinical trial. I
K, \\tsz:iiewsky C
liemaloloys omniums
.N'HI.V 2l)09;ls3( *):S6S-57.-i
K
suciitific
i n o s a f r o m i n i e c t e d h u m s . / Hum (..m- Reiiuk
2005:13(4 supplj.S I - M i
2 0 O 2 . 2 3 ( f t ) : ? S 6 -370.
trench
siaphvlocotxi
c
W o u n d healinjt a n d I I M f
a[ip!icaiicis.
(less concepts a n d
iVtuniii
fie;j,ur
lif^'ii
34. L a y - f l u m e k H o n e y m svou:ui i a i e : effects
V M . Cooper
HA. M o l a n
PC The
c l i n i i a l application a n d patient benefit
anlih.iclcrir.1 activity o f honey against (n.igulasc
negative
.Su/'pn/t I .
33. schult/. C M o z i i i g u l>. Kiiiiwiii'lli M, Cla.stori
hone*, in i u h i b h i n g strains o l Pseuduniuil.is aerug-
17
et a l .
Ciliicer 2 0 0 f v l 4 ( l ) : 9 1 . 9 7 .
1 d. (:<ioper RA. Halas L M o l a n P C I he efficacy o f
;.s
Racteria, b i o t i l m .ir.it u u n e v a study of the effects
r
strait-gics for i r e a t m c m o f chronic w o u n d s . 11 ten
I
Aniimiiinu
Oienhniser
2005.3<a : ).\\s-2 i l
References
lv i-
A n t i b a c t e i i a l actisits ot hoiu-y against strains o f
managemeni
J
Ann Reese is a wound care specialist
and geriatric nurse practitioner at
Greenville Hospital System University
Medical Croup in Greenville, South
Carolina. Deborah Willoughby, is an
undergraduate coordinator and professor and Stephanie C. Davis is an assistant professor, both at the School of
Nursing at Clemson University in
Clemson, South Carolina. Toni Silver is
a wound care specialist and Tad Venn
is a staff physician, both at Network
Geriatric Services in Spartanburg,
South Carolina. The authors state that
they do not have a financial interest in
or other relationship with any commercial product named in this article.
M2(}tl,S:{6)2'I
:7i.
Surj'. 2002;S9( 111): 1 JIM-1-'(IS.
4.
2 0 0 2 : 4 S ( 11).28-40.
SUtuige.
S i m o n A. I r a y n o i k. S.imos k. et a). Medital
hones lor w o u n d ; arc—still ::,.- latest lesort ' , r : J
C c i m a n v F.p'uMy 2008; 11
.V
(fsumij Wminl
in niedicd
\tullai V, M e n u n I Bactercidat acti\it\ o l d l f
33
A n d e r s o n I l i o n e y dressi;:i;s in svound e r e .
Times. 2006. l 0 2 . ( 2 2 ) : 4 0 - 4 : .
ferenl :>pcs ot n o n e s j^ainst citmc.ii a n d en\n
i,'v I v ^ n s i
mental
proiessionais. f i r ; Sim. 2 0 0 s : ! 1
isolates ot' I V i n i o m o n a s a e r u g i n o s a . ;'
THE AMERICAN ;OUR.VA, FOR N\KSt P R A C " H I O N £ R 5 ${rV!S£W/K>::~Q-ii*
Br 1 \:<>:
200t-,-!7( 11 ).s<0-s ((,.
70" ; ' . O l
flavin S I ioncy: a quisle :'; r hc.-.ithc ::e
) : ^ J 4 b Js.'-
COMMENTARY
P e
o
l
/
l
M
M
:
£
Jowe^AL
f r . a a y . J u l y 2 ? . 20D.
B7
I can heal wounds with honey and so can you
T
A L L E N DENNISON
he Crowne Plaza Hotel in Warwick
resembles a decent beehive even on
a slack day. It is swarming with conferees and employees moving in and
out of chambers consuming sweet food.
Some people arrive by air from nearby T.F.
Green AiTport on low-cost fares. There is a
high soda! organization.
Next week, on July 25-29, management
will show extreme cooperation in welcoming
20 beehives and 500 beekeepers for the annual meeting of the Eastern Apiculture Society.
They will have talks on Colony Collapse Disorder, practical beekeeping including a bee
yard, the business of keeping an apiary and
treating illness with bee products and stings.
On Wednesday they will be regaled by
Rhode Island's own Charlie Hall and the
Ocean State Follies, who will sting them all in
a show they will not soon forget. If you have
even a passing interest in bees, I recommend
that you go to the Web site eastemapiculture
.org and sign up for a day or two.
fluid hits the honey, small amounts of hydn>
I am presenting my literature review and gen peroxide are produced, very toxic to bacwork among the elderly in healing wounds teria but not to fibroblasts and healing elewith honey, based on 30 years of office prac- ments. Honey derived from medicinally actice and work as a medical director of Kver- tive nectars such as tea tree and eucalyptus
green House Health Center, a nursing home may have additional value, and the Food and
in East Providence. 1 remember a comic T V Drug Administration has allowed their imroutine with Met Brooks interviewing Sid portation and marketing.
Caesar posing as a great Egyptologist. "So
Topical antibiotic creams and ointments —
professor, what is the secret of Tutankha- both over the counter and prescription — are
men's Tomb?" Quipped Caesar, "Twenty commonly used for skin infections and
years of research and 1 should tell you?"
wound healing. These include neosporin,
1 am going to tell you. Speaking of F.gyp- bacitracin, "liipte-antibiotic" ointments and
tian tombs, did you know that urns of honey mupirocin. They sterilize the wound but also
were found undegraded in several tombs in kill healing elements, leading to delayed
ancient Egypt? This tells volumes about the wound closure. And they often lead to confusamazing chemical nature of honey for ing red bypersensibviiy reactions.
wound-healing, to say nothing of the long asAdditionally, more and more bacteria are
sociation ol the bees and humans.
growing resistant to antibiotics, which is a
How does honey help to heal wounds and terrific threat to all of us. Some are costly. We
why is it superior to neosporin, bacit racin and should avoid these tike the plague. My wife,
prescription mupirocin (bactroban)? Honey Jane Denruson, M.D., is a pediatrician and
is bee spit but it is also their energy currency beekeeper. As our house experienced colony
and their bank account. Just as "people get collapse with drone migration of our four
funny about their money" so, too, do bees get boys to New York City and Washington, my
funny about their honey. They hate bears, wife had the time to take the Bee Course ofbacteria and yeasts that may steal or spoil the fered by Rhode Island Beekeepers Associahoney, For the bears they have stingers, for tion (RIBA) and start some hives. At the
the inicro-onjanisms they put amazing stuff monthly RIBA meetings I spoke with the oldin the honey. They also seal the hive with an er beekeepers and was fascinated to learn of
antimicrobial substance called propilis.
honey's medicinal benefits. Some of the older
Honey is a mixture of concentrated sugars beekeepers suggested that 1 try using honey
that immediately dehydrate a bacterial cell, mixed with Aquaphor ointment on my parendering it immobile, though without neces- tients with minor wounds and ulcers. Honey
sarily killing it. Young Dr. Keith Monchik, of at body temperature gets runny and dribbles
on clothes, leading to poor treatment adherthe Orthopedic Service at Rhode Island Hospital (RIH), went to Haiti with our team from ence. Aquaphor was already my favorite
healing ointment. It is well suited to mixing in
the Ocean State to treat earthquake victims.
They ran out of usual wound-carc creams equal parts with honey because the lanolin
quickly but a senior military nurse reminded and mineral oil holds both aqueous and oily
the team that sugar packs from their rations parts together to treat a wound
always work in a pinch to keep a wound from
getting infected through the same mechanism. He reported gratifying results to the
RIH medical staff.
The high osmotic value of honey draws fluids out of wounds. This decreases tissue pressure, thus admitting more new blood, with, of
course, oxygen, as well as healing elements
>
t^^il.m l «
m
, .
n
n
vi,C*Om Will,
AC fhP
Mixing large batches withmc help of my
mother in law, Jane Mackenzie, R.N., is
sticky business indeed. She helps me pot it
into little cosmetic jars for use in the nursing
home. We heal the aquaphor to 110 degrees in
the microwave but never put raw honey in the
microwave because it would rum its special
qualities. And 1 urge you all: "Do this al
hornet." You can't buv it already made up.
If I were to try to sell this as a medicament,
the Food and Drug Administration could
have me jailed and impound all my ointment,
because adequate studies on the effectiveness and safety of this compound have not
been done. I lowever. iwo imported products,
Medihoney and Manuka Honey, have passed
FDA approval for wound-healing, 'lhey are
derived from the eucalyptus and tea tree
plant, respectively, whose nectars have supposedly superior qualities. These honeys are
irriadiated lu inactivate trace amounts of botuiinum toxin and bacteria.
i believe that raw honey needs no such
help and that such help might even he counter-productive This treatment and the importation increases the cost of treatment, witb
small nibes going for S5() to $100.1 insist on
the real thing when treating serious or stubbom wounds hut for everyday use the product from your home lab will work very well
on your cuts, burns and skin tears.
If you have diabetes and or congestive
heart failure peripheral arterial-supply problems, no ointment is going to help. The problem is under the skin. You need a doctor for it.
I invite colleagues and hospitals to begin randomized controlled trials on using local raw
honey head to head against imported honey
and the usual wound-care products. My hypothesis is that we can control at low cost,
such superbugs as methacillin-resistam staphyllococus aureus and vancomyrin-resistant enterococcousand the emergence of further resistant superbugs by avoiding the usual antibiotics.
;
Meanwhile, we'd be encouraging the development of new local hives, which are so
important to pollination — and thus plant life
and the broader ecosystem — nationally.
You may be interested in using hee stings to
treat disease and honey to desensitize yourself to allergies. On July 2<i Ihe Apilhcrapy
Association will make a presentation. You
can find out information on the schedule and
admission at eastemapiculture org.
AMen Dcnnison. M.O., is an assistant beenccper
and internist practicing in Barnngton ana East
Providence.







© Copyright 2026