
Document 147772
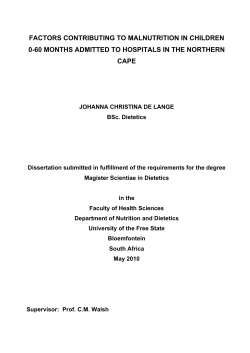
Oedematous malnutrition Michael H N Golden Department of Medicine and Therapeutics, University of Aberdeen, Aberdeen, UK Correspondence to: Prof Michael H N Golden, Department of Medicine and Therapeutics, University of Aberdeen, Foresterhill, Aberdeen AB2S2ZD, UK Oedema as a result of famine has been know since biblical times: the children of Israel, during their wanderings in the desert thought that the fungus that grows on acacia roots (mana) protected them against oedematous malnutrition [Deuteronomy: 8-4; Nehemiah: 9-21]. Even the typical skin changes of kwashiorkor were recognised: 'our skin was black like an oven because of the terrible famine' [Lamentations: 5-10]. The specific nutrients involved and the pathophysiological processes leading to the oedema and skin lesions still cause controversy. The problems raised by nutritional oedema and the inadequacy of current physiological explanations were raised in the classical reviews of McCance1 and Keys2, and remain unresolved. In the early decades of this century most work was done in Germany, where the condition in children was know as Mehlnahrschaden3, or 'flour dystrophy', because it was recognised in poor children weaned to a diet predominantly or exclusively of cereal flour, although detailed dietary data were not published. There was controversy over the cause, but protein deficiency was most commonly cited on the basis of low plasma protein concentrations and uncertainty over the requirements for dietary protein. The condition was also recognised in the tropics by Guillon in 1913, where it was termed Bouffissure-d'Annam, or 'swelling [disease] of Vietnam'; detailed studies and photographs of the patients were published in the French literature4. In the Spanish literature, the same condition was described in 1908 and became know as Sindrome Policarencial Infantil, or multi-deficiency syndrome, with reports in many local journals from most of Latin America5. From 1934, the Spanish ascribed the disease to multiple vitamin deficiencies. There were occasional reports in the English literature both from temperate British Medical Bulletin 1998;54 (No. 2): 433-444 C The British Coundl 1998 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 Oedematous malnutrition in the child or adult is not caused by protein deficiency; such a concept can lead to fatal therapeutic error in oedematous malnutrition treatment. On the other hand, deficiency of protein, or the other type II nutrients, is common and causes stunting and wasting. In kwashiorkor, the deficiency is more likely to be due to one or several type I nutrients, particularly those involved with anti-oxidant protection. Tropical medicine: achievements and prospects 434 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 regions6'7 and the tropics8. However, it was only following the Williams' report in the Lancet9, which gave the syndrome its usual name, kwashiorkor, that this disease of poverty became widely recognised. Following World War II, when general interest in malnutrition was intense because of concentration camp experience, assessment missions showed that kwashiorkor was common throughout the world. Active research groups formed in about 15 developing countries and international agencies formed standing committees. Most groups concentrated upon protein metabolism in the belief that protein deficiency was the underlying cause of kwashiorkor and energy deficiency the cause of marasmus. Many pertinent observations were made at this time; however, the legacy of the concepts of these early workers is found, largely unchallenged, in most textbooks of today. After the Great War, Denton reported the production of oedema in rabbits by feeding them a diet of carrots10. Attempts to repeat these experiments were unsuccessful. However, a number of American groups11"13 produced oedema in dogs by 'plasmapheresis'. The animals were repeatedly venesected of about one-third of their blood volume, the cells washed, resuspended in saline and re-infused. Aseptic technique was not used, the animals were subjected to repeated episodes of profound hypotension and all components of plasma were removed; nevertheless, as the plasma proteins fell the animals became salt sensitive and oedematous. At this time the pathophysiology of kwashiorkor and of nephrotic syndrome were thought to be the same. In the literature on nephrotic syndrome doubts were expressed because of the frequent, unexpected and spontaneous resolution of the oedema following a fever with no change in plasma proteins14 and the long-lived response to plasma infusion despite the plasma albumin returning to pretreatment level within days15. Williams16 ascribed kwashiorkor to weaning to a maize based diet and showed that they responded to a high protein diet of milk and marmite. During the Second War, Keys2 gave adult volunteers cabbage, potatoes and salty soups to simulate the diet of prisoners of war; they developed oedematous malnutrition, but their plasma oncotic pressure was not particularly low; he cited numerous studies from the literature to support the finding of non-concordance between plasma proteins and oedema. Of special interest are the studies of Youmans et at17'18 who investigated families of American subsistence farmers who had 'endemic' nutritional oedema, and yet their plasma proteins were normal. The importance of these studies is that the diet of the families was maize based: the same staple that William's patients in the Gold Coast (Ghana) were taking. In a remarkable wartime study, Petrides19 induced kwashiorkor in several children by feeding them the diets of the poor of Athens, he found that they did not respond to egg white but did British Medical Bulletin 1998;54 (No. 2) Oedematous malnutrition British Medical Bulletin 1998;54 (No. 2) 435 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 to egg yolk; this supports the view that the deficiency was corrected by some other component of egg yolk apart from the protein. After the World War II, McCance1 studied German prisoners returning from Russian camps. Like Keys, he concluded that the underlying cause could not be protein deficiency. When McCance visited the MRC unit in Uganda, he saw children with gross skin lesions that were not prevalent in the adults, very low plasma proteins and a rapid respond to milkbased diets. Unfortunately, he concluded that nutritional oedema in adults and in children must be completely different entities20. However, in the studies of kwashiorkor in Germany3, during the siege of Budapest21 and in Vietnam4, skin lesions were also uncommon in children. When the Uganda Unit moved to The Gambia, Whitehead22 found that the hormonal profiles of children with kwashiorkor in the two countries were different and, as an extension of the concept that adults and children were different, he then proposed that there were different pathophysiological types of kwashiorkor. Attempts by Widdowson and McCance and many others to reproduce kwashiorkor in animals with low protein diets have failed. The animals develop severe growth retardation, but not nutritional oedema. The only convincing animal model was produced in Uganda by feeding primates the diets of young children23; experiments that have never been repeated or exploited. McCance did not take into account the differences in endemic infection between temperate and tropical studies, particularly malaria. The geographical regions where kwashiorkor is common are generally malarious, although eradication of malaria has not eliminated kwashiorkor. To show the profound effect that such infection can have on plasma albumin, Keys14 had experimentally infected syphilitics, and later normal New York civil servants, with malaria and had shown a dramatic fall in plasma albumin with the onset of infection. The first serious attack on the protein deficiency hypothesis came from Gopalan15, who examined the diets of village children in India. He could find no antecedent dietary difference between those who developed marasmus and those who developed kwashiorkor. This work was unfairly criticised by those who believed in protein deficiency on the grounds that it was not formally reported in a peer review journal. Hansen26, in South Africa, was able to initiate cure of kwashiorkor with entirely synthetic diets. In an early series of experiments in Jamaica, children were kept in a stable condition and baseline measurements of protein turnover were made for a few hours after admission. They were given low protein diets during this time and, surprisingly, showed a marked clinical improvement. The period of low protein feeding was cautiously extended and the children improved remarkably, with a lowered mortality, on a diet Tropical medicine: achievements and prospects Protein deficiency Once protein deficiency had been exonerated from causing kwashiorkor, the way was opened to examine the real effects of protein deficiency in man. All animal species, given a low protein diet, reproducibly and predictably fail to grow normally; and, with time, become nutritional dwarfs. Indeed, early supplementation experiments with children showed that provision of extra milk leads to increased growth29"31. In retrospect, there are many examples of the average height of children and adults in populations subsisting upon low-protein staple diets being lower than those receiving a higher-protein staple food (for example, Nicol32). Experiments with adults and children show that there are no acute clinical effects of a protein-free diet, apart from weight loss, for at least several weeks. One of the major defects of the protein-deficiency hypothesis of kwashiorkor is that affected infants are not usually stunted in height, whereas those with marasmus are usually much more stunted. The concept of protein deficiency in man and animal causing stunting has now been extended to other nutrients whose deficiency causes similar effects33-34. A rational classification of the nutrients into those which cause specific clinical signs (type I) and those that cause growth failure (type II) then explains how anthropometrically normal or even obese people can be iron or thiamine deficient, while deficiency of other nutrients such as protein, sulphur, phosphorus, zinc or potassium leads 436 British Medical Bulletin 1998;54 (No. 2) Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 supplying less protein than they were calculated to have had before admission. During this time, they lost all their oedema without any change in their serum albumin level27; the rate of loss of oedema was entirely independent of the protein content of the diet28. The early argument that kwashiorkor was due to protein deficiency because of the response to diets rich in protein is fallacious: is a headache due to aspirin deficiency because it is cured by aspirin? However, posed in a negative form, the same argument has impeccable logic; if a headache gets better without aspirin then it was not due to aspirin deficiency! The demonstration that kwashiorkor could be cured with a diet lower in protein than the diets taken by poor children in Jamaica showed that some other cause had to be found for kwashiorkor apart from protein deficiency. These results, which are similar to those obtained by McCance with adults, also remove the rationale for considering adult and childhood oedematous malnutrition to be intrinsically different and to have a different physiological basis. The findings of Keys, McCance and Youmans thus added force to the contention that we do not know the aetiology of oedematous malnutrition in either adults or children. Oedematous malnutrition British Medial Bulletin 1998;54 (No. 2) 437 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 to stunting and wasting. Failure to appreciate both the difference in types of deficiency and the interdependence of the 'growth nutrients' may underlie the very poor results of most supplementation programmes in the developing world35 and the very high and unchanging prevalence of stunting (about 50% of the world's population). The inadequate convalescence and failure of children to catch-up after an episode of acute illness, such as diarrhoea or pneumonia, can be ascribed to failure to provide this specific portfolio of type II nutrients: the poor growth is usually ascribed to the infection alone, although children on a normal diet quickly regain what they have lost, whereas children on a poor diet will become stunted even if they do not have frequent infection36. Recently I have described 209 children with kwashiorkor who were being breast-fed, in some cases exclusively, in African refugee camps. The mothers were not themselves anthropometrically malnourished (Golden and Grellety, unpublished). In this group, the amount of oedema and mortality was the same in the breast-fed and weaned children. The breast-fed children grew slightly more slowly than the weaned children. The concentration of protein and the other type II nutrients are stoutly maintained in breast milk and maternal deficiency of these nutrients would express itself in maternal weight loss. This again suggests that kwashiorkor is not due to deficiency of protein or any other type II nutrient. These data, and the lack of stunting in many of these patients, suggest that kwashiorkor is attributable to deficiency in the type I category of nutrients. Despite mounting evidence, it was not generally accepted that protein deficiency dos not cause kwashiorkor, largely because there was no replacement paradigm, and the pioneers maintained their belief in this aetiology37. Gopalan25 had proposed that there was some intrinsic difference between the children who developed kwashiorkor and those who developed marasmus, and termed kwashiorkor a 'dysadaptation' to their hostile environment. Without a more concrete hypothesis, such a supposition could not be tested. Also rejecting protein deficiency, Hendrikse38 proposed that kwashiorkor was due to aflatoxin poisoning because he found higher circulating levels of aflatoxin in kwashiorkor than marasmus. However, these results are more likely to be explained by the liver dysfunction and failure to metabolise aflatoxin in kwashiorkor, because the excretion of aflatoxicol in the urine is the same in the two conditions39. Liver samples sent to Hendrikse from Jamaica for blind analysis did not support this aetiology (Table 1). Shrikantia40, using a bioassay, had reported that children with kwashiorkor had high levels of circulating ferritin. When immunoassays became available we confirmed this observation in Jamaica41 and confirmed that there was iron overload by measuring the excretion of iron following the administration of desferrioxamine42. Iron is a potent Tropical medicine: achievements and prospects Table 1 Aflatoxin concentrations in liver samples taken from children dying of kwashiorkor or marasmus in Jamaica Diagnosis Aflatoxin Type (pg/g) Kwashiorkor Kwashiorkor Kwashiorkor Kwashiorkor Kwashiorkor Kwashiorkor Kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmic-kwashiorkor Marasmus Marasmus Marasmus 0 0 0 0 0 4 90 0 0 0 0 0 1052 2500 0 698 25,608 _ B2 G2 _ B1 B1 M2 B1 free radical catalyst, that is extremely toxic if not strictly compartmentalised and firmly bound to specific proteins. The levels of transferrin in kwashiorkor are very low42 and we calculated that most of the children would have free iron available for free-radical cycling. Iron overload has since been confirmed in South Africa43 and free iron in the plasma directly demonstrated44. Oxidant stress Jackson was pursuing the hypothesis that glycine was a limiting amino acid in growth and measured red-cell soluble sulphydryls, mainly glutathione, to examine glycine metabolism in malnutrition. He found the level to be very low in kwashiorkor45 and suggested that this was due to dietary protein deficiency. However, glutathione is a potent cellular reductant controlling the oxo-reductive potential of the cell and is a free radical scavenger. It is also a critical cofactor of enzymes that dispose of the products of free-radical injury and, by maintaining cellular sulphydryls in a reduced state, enables cellular function. Indeed, tissue glutathione levels had been used as a measure of the degree of the imbalance between free-radical generation and their disposal (oxidative stress)46. Golden and Ramdath47 confirmed Jackson's observation using a specific assay and showed that the low glutathione was not a function of oedema per se, by finding normal values in children with nephrotic 438 British Medical Bulletin 1998;54 (No. 2) Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Oedematous malnutrition British Medical Bulletin 1998;54 (No. 2) 439 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 syndrome and congestive heart failure. We then investigated the enzymes responsible for maintaining glutathione in the reduced state, hexosemonophosphate shunt (glucose-6-phosphate dehydrogenase, G6PD; 6phospho-gluconate dehydrogenase, 6PGD) and glutathione reductase, and found them to be much more active in all forms of malnutrition than in control children48. In response to an oxidative stress, there is increased activity of G6PD and 6PGD to provide additional NADPH for glutathione reduction. When this supply is adequate, NADPH levels are maintained; when the rate of oxidation of glutathione exceeds the capacity to supply reducing equivalents, the NADPH level can fall despite the increased rate of its supply. We found that NADPH levels were normal in marasmus but reduced in kwashiorkor with a corresponding rise in NADP+. These results confirm that there is an oxidative stress in kwashiorkor: such results could not be produced by protein deficiency. The oxidised form of glutathione, GSSG, is toxic to cells because it reacts with protein sulphydryls. For this reason, if the maximum rate of GSSG reduction is less than its rate of production, GSSG is actively exported from the cell. It is for this reason that the glutathione level inside the cell falls and can be used as an index of oxidative stress. During treatment it takes about 2 weeks before the NADPH and GSH levels return to normal values. In kwashiorkor, a relative deficiency of anti-oxidants with lipid peroxidation also explains a previously puzzling observation by Waterlow49. He found that hepatic mitochondria from children with kwashiorkor had normal rates of oxidative phosphorylation immediately after isolation, but within minutes of exposure to air they lost function; more so with vigourous homogenisation. The lipid fraction from the children's liver biopsies rapidly poisoned rat liver mitochondria, which otherwise functioned normally for several hours. Whether such oxidative stress causes all the clinical features of kwashiorkor is uncertain. When normal red cells are incubated with enzyme inhibitors (bis-chloronitrosourea, BiCNU) so that the level of glutathione is reduced to the levels seen in kwashiorkor, there is an increase in the membrane leak to electrolytes so that the cellular sodium concentration rises, potassium concentration falls and the sodium pump is stimulated50. These are precisely the abnormalities seen in oedematous malnutrition51-52. There is also a very close relationship between the amount of liver damage, as measured by gamma-glutamyl-transferase levels, and the level of glutathione (Golden and Ramdath, unpublished), as well as the plasma ferritin concentration. There is also a relationship between the red-cell glutathione and the amount of liver fat measured by ultrasound (Doherty, Ramdath and Golden, unpublished). The appearance and evolution of the skin lesions of kwashiorkor exactly mirror those of sun-burn, an unequivocal radical generated injury, with Tropical medicine: achievements and prospects an initial increase in pigmentation and then direct dermal damage. The skin lesions do resemble those of pellagra; indeed, kwashiorkor and pellagra were confused in early descriptions. Our findings help to explain this on the grounds of similar mechanisms. However, in pellagra the niacin deficiency leads to a lack of reducing equivalents for oxidised glutathione due to a low concentration of NADPH, whereas in kwashiorkor the total NADP(H) levels are normal48 and the oxidative stress comes from elsewhere. The mortality rate in hospitals, from severe malnutrition, has not changed in about 40 years at between about 20—40%53, despite the fact that under refugee camp conditions mortality rates of 5-10% are achieved54. Why should this be? First, the concept that kwashiorkor is due to protein deficiency has led to diversion of effort and criticism of the research that is conducted55. Secondly, the protein deficiency concept has led to treatment with high protein diets. At the end of the war, the POWs were initially treated with protein hydrolysates and mortality was very high56. This experience was not applied to the disease in childhood. Several abnormal amino-acid metabolites are excreted in kwashiorkor57"60. These metabolites are similar to those found in inborn errors of metabolism and come from an acquired loss of the enzymes of the catabolic pathways61'62. To give such a patient a high-protein diet, before the enzymatic machinery has recovered, is against all experience in treating inborn errors of metabolism. Initially, Collins63 treated adults with kwashiorkor in the Somalian famine of 1992/93 with the standard high protein diets available. When he switched to a low protein diet, similar to that used in children64, the mortality rate fell to one-quarter, the rate of loss of oedema improved dramatically and the patients quickly regained their appetites. The very concept that kwashiorkor was due to protein deficiency, and that the mainstay of treatment should, therefore, be protein replacement as one would do with any other 'deficiency', seems to have maintained the high mortality rates for the past half century. It is unclear how oxidative stress causes oedema. That it can is shown by the oedema of newborn infants with vitamin E deficiency65, birds with selenium deficiency, and the oedema of pure radical injury such as exposure to ionising radiation. Subcutaneously injected dye dissipates rapidly66 as if the interstitial hyaluronate and glycose-amino-glycans were disrupted and interstitial water was in a free state. Such damage to the interstitium, with loss of the normal negative charge, if generalised, 440 British Medical Bulletin 1998;54 (No. 2) Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 Mortality Oedematous malnutrition 10 n r KM M Diagnosis would explain our findings of effacement of the podocytes onto the glomerular basement membrane67 and invasion of normally resistant cells, such as hepatocytes, with herpes simplex virus in kwashiorkor68. In a therapeutic feeding centre experiencing a cholera outbreak, we have recently observed that the attack rate in children and adults with kwashiorkor is about 1 % whereas for those with marasmus it was 25 % (Golden and Grellety, unpublished). Disruption of complex carbohydrates would also explain this observation. The oxidative stress comes mainly from infection, from ingested aflatoxin and bacterial endotoxins and from small bowel overgrowth. Diseases such as measles are harbingers of kwashiorkor in susceptible populations. In kwashiorkor, in comparison to marasmus, there seems to be a specific increase in the levels of leukotrienes69, a product that would not be expected if glutathione were limiting since glutathione is one of its precursors. Furthermore, we have estimated the endogenous production of nitric oxide, from arginine, by measuring the excretion of nitrate in malnourished children on a nitrate-free diet (Fig. 1). The high levels of nitrate production are similar to those seen in other syndromes which resemble aspects of kwashiorkor metabolically, such as toxic shock syndrome, multi-organ failure and adult respiratory distress syndrome. Like these conditions, kwashiorkor is an acute disease; the history is usually of only a few days and frequently presents with hypovolaemia. This is due to uncontrolled vasodilatation. The second reason for the high mortality rate from kwashiorkor in most hospitals is that these children are diagnosed as being 'dehydrated' on the basis of British Medical Bulletin 1998;54 (No. 2) 441 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 Fig. 1 Nitric oxide production, measured as urinary nitrate excretion whilst taking a nitrate free diet in children with kwashiorkor (K), marasmic-kwashiorkor (MK) or marasmus (M) over the first 24 h after admission or as soon as the children were sufficiently well to have a 24 h urine collection performed. r Tropical medicine: achievements and prospects References 1 McCance RA. The history, significance and aetiology of hunger oedema. In: Studies in Undernutntion: Wuppertal 1946-9. MRC Special Report Series No 274. London: HMSO, 1951; 21-86 2 Keys A. The edema problem. In: Keys A, Brozek J, Henschel A, Mickelsen O, Taylor HL. (eds) The Biology of Human Starvation. Minneapolis: University of Minnesota, 1950; 921 3 Czerny A, Keller A. Des kmdes ernahrung, emabrungsstorungen und ernabrungstherapie. Leipzig: Deuticke, 1928 4 Normet L. La bouffissure d'Annam. Bull Soc Pathol Exotiaue 1926; 3: 207-13 5 Autret M, Behar M. Sindrome policarendal infantil (kwashiorkor) and its prevention in Central America. Rome: Food and Agriculture Organization, 1954; 181 6 Bloch C E Diseases of infants due to prolonged feeding with excess carbohydrates. BMJ1921; 1:293 7 Abt IA. Injuries produced by starch. JAMA 1913; 14: 1275-7 8 Procter RAW. Medical work in a naove reserve. Kenya Med} 1926; 3: 284-9 9 Williams CD. Kwashiorkont a nutritional disease of children associated with a maixe diet. Lancet 1935; 2: 1151-2 10 Demon MC, Kohman E. Feeding experiments with raw and boiled carrots. / Biol Chem 1918; 36: 249-63 11 Weech AA, Snelling CE, Goettsch E. The relationship between plasma protein content, plasma specific gravity and edema in dogs maintained on a protein inadequate diet and in dogs rendered edematous by plasmapheresis. / Cltn Invest 1933; 12: 193-216 442 British Medical Bulletin 1998;S4 (No. 2) Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 their hypovolaemia and perhaps a history of frequent small mucoid stools which the mother reports as diarrhoea. It is a contradiction in terms to say that a person can be over hydrated (oedematous) and under hydrated simultaneously. These oedematous patients, who have both a high extracellular and high intracellular sodium content (c.f. Lot's wife who was also a pillar of salt) are often 'rehydrated' intravenously or with ORS (90 mM/1 Na). They die from heart failure70, which is easily misdiagnosed as pneumonia in these children. In kwashiorkor, because of the cell membrane leak, the intracellular potassium is reduced as well as the sodium increased. If this defect is corrected precipitously then there is the danger of the induced NaVK+ATPase exporting sodium from the intracellular compartment faster than the kidney can excrete the excess, particularly if the interstitial defect is also corrected and fluid shifts from the interstitial to the intravascular space. Acute volume overload, hypokalaemia and death can result from this disequilibrium syndrome71. Until we know much more about the details of the disordered physiology and how it should be safely corrected, it would be unwise to administer large doses of anti-oxidants to these patients. A toxin free, lowprotein, low sodium, high potassium diet with adequate amounts of phosphate and magnesium and which contains the known type 1 nutrients in 'replacement' amounts is prudent. There should be adequate easily absorbed carbohydrate, to prevent hypoglycaemia and limited fat at this stage. Nevertheless, using such diets and treating the inevitable infections blindly, the mortality is still usually between 5-10%. This is a tragedy, because the patients that recover are absolutely normal without any known long-term sequelae. Oedematous malnutrition British Medical Bulletin 1998;54 (No. 2) 443 Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 12 Darrow DC, Hopper EB, Cary MK. Plasmapheresis edema. 1. The relation of reduction of serum proteins to edema and the pathological anatomy accompanying plasmapheresis. / Clin Invest 1932; 11: 683-99 13 Maver MB. Nutritional edema and 'war dropsy'. JAMA 1920; 74: 934-41 14 Loeb RF, Atchley DW, Richards DW, Benedict EM, Driscoll ME. On the mechanism of nephrotic edema./ Gin Invest 1932; 11: 621-39 15 Squire JR. The nephrotic syndrome. BMJ 1953; ii: 1388-99 16 Williams CD. A nutritional disease of childhood associated with a maize diet. Arch Dis Child 1933; 8: 423-33 17 Youmans JB, Bell A, Donley D, Frank H. Endemic nutritional edema. 1. Clinical findings and dietary studies. Arch Intern Med 1932; 50: 843-54 18 Youmans JB, Bell A, Donley D, Frank H. Endemic nutritional edema. 2. Serum proteins and nitrogen balance. Arch Intern Med 1933; 51: 45-61 19 Petrides EP. Hunger edema in children. / Pediatr 1948; 32: 333-50 20 McCance RA. Malnutrition in Uganda. Indian J Med Res 1971; 59 (Suppl): 132-42 21 Kerpel-Fronius E. The pathophystology of infantile malnutrition. Budapest Akademiai Kiado, 1983; 1-312 22 Whitehead RG, Coward WA, Lunn PG, Rutishauser ME. A comparison of the pathogenesis of protein-energy malnutrition in Uganda and The Gambia. Trans R Soc Trap Med Hyg 1977; 71: 189-95 23 Coward DG, Whitehead RG. Experimental protein-energy maLnutrition in baby baboons. Attempts to reproduce the pathological features of kwashiorkor as seen in Uganda. Br J Nutr 1972; 28: 223-37 24 Taylor HL, Mickelsen O, Keys A. The effect of induced malaria, acute starvation and semistarvation on the electrophoretic diagram of the serum proteins of normal young men. / Clin Invest 1949; 28: 273-81 25 Gopalan C. Kwashiorkor and marasmus: evolution and distinguishing features. In: McCance RA, Widdowson EM. (eds) Calorie Deficiencies and Protein Deficiencies. London: Churchill, 1968; 48 26 Hansen JDL, Howe EE, Brock JF. Aminoacids and kwashiorkon Lancet 1956; ii: 911—3 27 Golden MH, Golden BE, Jackson AA. Albumin and nutritional oedema. Lancet 1980; i: 114-6 28 Golden MH. Protein deficiency, energy deficiency, and the oedema of malnutrition. Lancet 1982; i: 1261-5 29 Orr JB. Milk consumption and the growth of school children. Lancet 1928; i: 202-3 30 Spies H, Dreizen S, Snodgrasse RM, Arnett CM, Webb-Peploe H. Effect of dietary supplement of non fat milk on human growth failure. Am J Dis Child 1959; 98: 187-97 31 Malcolm LA. Growth retardation in a New Guinea boarding school and its response to supplementary feeding. Am J Clin Nutr 1970; 24: 297-305 32 Nicol BM. The protein requirements of Nigerian peasant farmers. BrJ Nutr 1959; 13: 307-20 33 Golden MH. The role of individual nutrient deficiencies in growth retardation of children as exemplified by zinc and protein. In: Waterlow JC. (ed) Linear Growth Retardation in Less Developed Countries. New York, NY: Raven, 1988; 143 34 Golden MH. The nature of nutritional deficiency in relation to growth failure and poverty. Ada Paedtatr Scand 1991; 374: 95-110 35 Beaton GH, Ghassemi H. Supplementary feeding programs for young children in developing countries. Am J dm Nutr 1982; 35: 864-916 36 Dagnelie PC, van Staveren WA, Hautvast JG. Stunting and nutrient deficiencies in children on alternative diets. Acta Paediatr Scand Suppl 1991; 374: 111-8 37 Waterlow JC. Protein-energy malnutrition: the nature and extent of the problem. Clin Nutr 1997; 16 (Suppl 1): 3-9 38 Hendrickse RG. Kwashiorkor: die hypothesis that incriminates aflatoxins. Pediatrics 1991 88: 376-9 39 Coulter JB, Hendrickse RG, Lamplugh SM et al. Aflatoxins and kwashiorkor: clinical studies in Sudanese children. Trans R Soc Trop Med Hyg 1986; 80: 945-51 40 Srikantia SG. Ferrinn in nutritional oedema. Lancet 1958; i: 667—8 41 Golden MH, Golden BE, Bennett FL High ferritin values in malnourished children. In: Mills CF, Bremner L, Chesters JK. (eds) Trace Element Metabolism in Man and Animals 5. Aberdeen: Commonwealth Agricultural Bureau, 1985; 7-75 42 Ramdadi DD, Golden MH. Nonhaematological aspects of iron nutrition. Nutr Res Rev 1989; 2: 29-49 Tropical medicine: achievements and prospects 444 British Medical Bulletin )998;54 (No. 2) Downloaded from http://bmb.oxfordjournals.org/ by guest on September 9, 2014 43 Dempster WS, Sive AA, Rosseau S, Malan H, Heese HV. Misplaced iron in kwashiorkor. Eur J Gin Nutr 1995; 49: 208-10 44 Sive AA, Dempster WS, Malan H, Rosseau S, Heese HD. Plasma free iron: a possible cause of oedema in kwashiorkor. Arch Dis Child 1997; 76: 54-6 45 Jackson AA. Blood glutathione in severe malnutrition in childhood. Trans R Soc Trop Med Hyg 1986; 80: 911-3 46 Sies H. Hydroperoxides and thiol oxidants in the study of oxidative stress in intact cells and organs. Iru Sies H (ed). Oxidative Stress. London: Academic Press, 1985: 73-90 47 Golden MH, Ramdath DD. Free radicals in the pathogenesis of kwashiorkor. Proc Nutr Soc 1987; 46:53-68 48 Golden MH, Ramdath DD, Golden BE. Free radicals and malnutrition. In: Dreosti IE. (ed) Trace Elements, Micronutnents and Free Radicals. Totowa, NJ: Humana Press, 1991; 199 49 Waterlow JC. Oxidative phosphorylation in the livers of normal and malnourished human infants. Proc R Soc Lond B Biol Sci 1961: 155: 96-114 50 Forrester TE, Golden MH, Brand S, Swales J. Reduction in vitro of red cell glutathione reproduces defects of cellular sodium transport seen in oedematous malnutrition. Eur J Clin Nutr 1990; 44: 363-9 51 Patrick J, Golden MH. Leukocyte electrolytes and sodium transport in protein energy malnutrition. Am] Gin Nutr 1977; 30: 1478-81 52 Kaplay SS. Erythrocyte membrane Na* and K* activated adenosine triphosphatase in proteincalorie malnutrition. Am ) Clin Nutr 1978; 31: 579-84 53 Schofield C, Ashworth A. Why have mortality rates for severe malnutrition remained so high?. Bull World Health Organ 1996; 74: 223-9 54 Prudhon C, Briend A, Laurier D, Mary JY, Golden MH. Comparison of weight and height-based indices for assessing the risk of death in severely malnourished children. Am J Epidemiol 1996; 144: 116-23 55 Golden MH. Issues in Kwashiorkor. Lancet 1994; 343: 292 56 Vaughan J, Pitt Rivers R. The value of hydrolysates in the treatment of severe starvation. Proc R Soc Med 1945; 38: 395 57 Whitehead RG. An unidentified compound in the serum of children with kwashiorkor (proteincalorie malnutrition). Nature 1964; 204: 389 58 Whitehead RG, Milburn TR. Metabolites of phenylalanine in the urine of children with kwashiorkor. Nature 1962; 196: 580-1 59 Whitehead RG, Arnstein HRV. Imidazole acrylic acid excretion in kwashiorkor. Nature 1961; 190: 1105-6 60 Whitehead RG, Matthew CE. The analysis of urine of children suffering from kwashiorkor. East AfrMedJ 1960; 37: 384-90 61 Burch HB, Arroyave G, Schwartz R et al. Biochemical changes in liver associated with kwashiorkor. / Clin Invest 1957; 36: 1579-87 62 Waterlow JC, Patrick SJ. Enzyme activity in fatty livers in human infants. Ann NY Acad Sci 1954; 57: 750-63 63 Collins S, Myatt M, Golden BE. The dietary treatment of severe malnutrition in adults. Am ] Clin Nutr 1998; In press 64 Golden MH. Severe malnutrition. In: Weatherall DJ, Ledington JGG, Warrell DA. (eds) Oxford Textbook of Medicine. Oxford: Oxford University Press, 1996; 12-78 65 Hassan H, Hashim SA, Van Itallie TB, Sebrell WH. Syndrome in premature infants associated with low plasma vitamin E levels and high polyunsaturated fatty acid diet. Am J Clin Nutr 1966; 19: 147-57 66 Winick M. Hunger Disease: Physicians of the Warsaw Ghetto. New York, NY: Wiley, 1979; 1-156 67 Golden MH, Brooks SE, Ramdath DD, Taylor E. Effacement of glomerular foot processes in kwashiorkor. Lancet 1990; 336: 1 4 7 2 ^ 68 Brooks SE, Taylor E, Golden MH, Golden BE. Electron microscopy of herpes simplex hepatitis with hepatocyte pulmonary embolization in kwashiorkor. Arch Pathol Lab Med 1991; 115, 1247—9 69 Mayatepek E, Becker K, Gana L, Hoffmann GF, Leichsenring M. Leukotrienes in the pathophysiology of kwashiorkor. Lancet 1993; 342: 958-60 70 Wharton BA, Howells GR, McCance RA. Cardiac failure in kwashiorkor. Lancet 1967; ii: 384-7 71 Patrick J. Death during recovery from severe malnutrition and its possible relationship to sodium pump activity in the leucocyte. BMJ 1977; i: 1051-4









© Copyright 2026