
Medicaid Expansion Map Likely To Stay Same Due To GOP Wins
InsideHealthPolicy.com’s Inside CMS exclusive news on the most powerful agency in health care Vol. 17, No. 45 - November 6, 2014 Medicaid Expansion Map Likely To Stay Same Due To GOP Wins In Governors’ Races With the GOP’s strong showing in governors’ races Tuesday (Nov. 4), including fighting off challenges in what were billed to be six close races in non-Medicaid expansion states, a health care analyst says there won’t be any changes to the map of states that have expanded the Medicaid program and those states that have resisted expansion. Even though Republicans won governors’ mansions in three traditionally Democratic strongholds, the analyst doesn’t believe there will be a rollback of Medicaid expansion in those states. “Certainly the outcome of the elections does not provide an obvious opening for new states to expand,” said Elizabeth Carpenter, director of health care reform at consulting firm Avalere Health. An analysis put out by Avalere Health last Wednesday (Oct. 29) predicted that six states — Alaska, Kansas, Georgia, Florida, Maine and Wisconsin — could renew fights to expand Medicaid under the Affordable Care Act if their governors’ offices flipped from Republican to Democratic or Independent control. Avalere Health added a caveat to its analysis, saying control of the state legislatures in those states is the key to whether the fight to expand the program succeeds. “This is a key election for the future of the Medicaid program,” said Avalere CEO Dan Mendelson prior to continued on page 10 Piecemeal Approach To ACA Could Put Both Parties In Difficult Positions Weighing heavy on the minds of lobbyists is whether the incoming GOPled Senate will insist on repealing the Affordable Care Act in its entirety or hold votes on measures with bipartisan support, including repealing the device tax and employer mandate. The piecemeal approach stands a better chance of working, lobbyists say, and could benefit both parties, but it also could put lawmakers in both parties in awkward positions: Republicans could be attacked from the far right for improving the law, and Democrats might find themselves having to actually vote for piecemeal repeal bills that they signed onto but didn’t expect to actually pass. Senate Republicans are expected to hold a vote on full-repeal of the continued on page 12 Burwell Invites Reluctant Governors To Discuss Flexible Medicaid Options HHS Secretary Sylvia Burwell invited governors who are reluctant to expand Medicaid, and newcomers following Tuesday’s election, to discuss flexible options for expanding the program their own way. She pledged that federal funding would never dip below 90 percent and stressed that states expanding their programs could always back away in the future. Burwell told state Medicaid directors Tuesday (Nov. 4) that her top priority is expanding Medicaid, and she had an Election Day message: “If you’re interested in expanding, call me.” Burwell said she is willing to meet with incoming governors before their inaugurations. Citing Pennsylvania, Arkansas, Iowa and Michigan, Burwell continued on page 14 CMS Axes Sunshine CME Exclusion, But Most Payments Still Not Reported CMS moved forward with plans to drop the continuing medical education (CME) exemption from the Open Payments Program (sunshine law) and clarified in the 2015 final physicians pay rule that, if manufacturers and GPOs that fund CME events don’t have any say over who speaks or how the events use the money, then the payments don’t have to be reported because they fall outside the definition of indirect payment. The vast majority of stakeholders had worried when CMS first proposed axing the CME exclusion from the sunshine law that it would mean money manufacturers provide for CME events would have to be reported as indirect payments. Now the CME Coalition, which opposed CMS’ proposal to drop the continued on page 16 Retirements Make Way For Committee Shake-Ups Following 2014 Midterms The Children’s Health Insurance Program will be losing its champion, and House and Senate committees will see a leadership shake-up following Tuesday night’s mid-term election where all eyes watched as the GOP took control of the Senate for the first time in eight years and gained House seats. In addition to new GOP slots likely opening up on health care committees, key members of both the House and Senate are set to retire after the 2014 midterms, leading to expected changes across House Ways & Means and Energy & Commerce, as well as the Senate Finance Committee. Sen. Jay Rockefeller (D-WV) and Reps. Henry Waxman (D-CA) and John Dingell (D-MI) are set to retire, along with House Ways & Means Chair David Camp (R-MI). The Senate Finance Committee gavel is expected to go to Sen. Orrin Hatch (R-UT) following the Republican takeover of the Senate, lobbyists say. An analysis by Avalere Health says that with Republican control, Hatch will likely begin preparing for entitlement reform debates that would probably occur early in a new presidential administration in 2017. Prior to the election, Leslie Krigstein, director of congressional affairs at the College of Healthcare Information Management Executives, said that if the Republicans controlled both the House and Senate, there might be more room for “sensible criticisms and ideas around more niche areas of e-health policy, such as EHR regulation, medical device cybersecurity, telemedicine, quality measurement, and patient safety reporting.” Democrats on the Senate Finance Committee will lose Sen. Jay Rockefeller (D-WV) to retirement, which Julius Hobson, a senior policy advisor with Polsinelli, says means CHIP will lose it’s champion. Rockefeller has been the driving force behind the bipartisan CHIP program, and has used his position on the Senate Finance Committee to push for Congress to extend the program’s funding through 2019 during the lame duck session after the elections and before he leaves. Inside Health Policy previously reported that Rockefeller is concerned that if funding reauthorization for CHIP is not passed during the lame duck session, it may not happen. CHIP is slated to lose funding after Sept. 30, 2015, but Rockefeller has put forward a bill to fund the program through 2019. Reps. Frank Pallone (D-NJ) and Waxman, the ranking Democrat on the House Energy & Commerce Committee, introduced similar legislation in the House, but Waxman is also leaving Congress in January. Both Pallone and Rep. Anna Eshoo (D-CA) have expressed interest in Waxman’s position on the House Energy & Commerce Committee following his retirement and have gathered support. House Minority Leader Nancy Pelosi (DCA) has endorsed Eshoo for the position, saying in a September letter that “Anna has listened to Members, reflected their values and gained their strong support — more than 105 commitments, a majority of the Caucus.” Pallone, however, has more seniority and in September he also released a letter signed by 50 Democrats he says are gathering support for his campaign for the ranking member slot. Pallone also has the backing of the Congressional Black Caucus, Hobson notes, as well as the Congressional Hispanic Caucus. On the Republican side, the House Ways & Means Committee will see a new Chair next Congress, as Camp is retiring, and lobbyists expect that Rep. Paul Ryan (R-WI) will take the gavel. However, Rep. Kevin Brady (R-TX) has also expressed interest in the position. Brady is currently chair of the Ways and Means health subcommittee, where he has spearheaded bipartisan anti-fraud legislation, among other bills. — Michelle M. Stein Hot Documents Now Available on InsideHealthPolicy.com The following new documents are available on InsideHealthPolicy.com, our new online health news service. Subscribers to InsideHealthPolicy.com also have access to hundreds of other health-related documents, daily news updates, and a searchable archive of back issues. Avalere Analysis Of How Governors’ Races Could Lead To More Medicaid Expansion Disease Groups File Amicus Brief In Halbig, Say ACA Intended To Provide Subsidies Through Federal And State Exchanges CMS Releases Final Home Health Rates HHS OIG Posts 2015 Workplan Center For American Progress Offers Long Term Care Reform Proposal With Tax Credits For Purchase Of LTC Insurance NAMD Seeks More State-Federal Cooperation, Flexibility Around Quality Measures In CMS’ Medicaid Managed Care Updates CMS Issues Final Physician, Outpatient, ESRD Pay Rules 18 States Defend Administration’s Stance In Halbig Amicus Administration Says Employers Will Not Meet Minimum Value Standards If In-Patient Hospital/Physician Services Omitted From Coverage Not an online subscriber? Inside CMS subscribers can get a free, two-week trial to InsideHealthPolicy.com by calling 1-800-424-9068 or signing up at http://www.insidehealthpolicy.com/health_signup.asp. 2 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 SCOTUS Takes No Action on King; 18 States Back White House In Halbig The Supreme Court on Monday (Nov. 3) took no action on a high-profile case challenging the provision of ACA tax subsidies to people who purchase a qualified health plan through a federally-facilitated exchange, however the court did say that it will take another look at King v. Burwell at its conference on Friday (Nov. 7), according to the SCOTUS Blog. Meanwhile, the attorneys general of 18 states, including some led by GOP governors, on Monday (Nov. 3) filed an amicus brief supporting the administration’s stance in a similar case — Halbig v. Burwell — that will be heard by the full panel of judges in the U.S Court of Appeals for the District of Columbia Circuit on Dec. 17. Briefs in that case were due Nov. 3. Legal experts who support the ACA had expected that the high court would take no action on the case since there is no current split on the appellate level and no other urgent need to take up the case since there are similar arguments winding through the lower courts. Those supporting the case disagree and believe that the questions should be answered immediately to ease uncertainty. “The Supreme Court’s inaction is not surprising,” said Ron Pollack, executive director of Families USA. “The typical guidelines for Supreme Court review are absent at this moment in the King case: There is no constitutional issue presented and there are no conflicting rulings in the Circuit Courts of Appeals. “Additionally,” he said, “two other Circuits Courts of Appeals — the D.C. Circuit and the Tenth Circuit — are soon scheduled to hear appeals on similar claims. The Supreme Court did not, and should not have, intervened until this litigation runs its course in the lower appellate courts.” Families also filed an amicus brief supporting the administration’s stance in the Halbig case, arguing that there are numerous provision in the law that make it clear Congress intended to provide subsidies to residents of all states. At issue is whether the IRS overstepped in writing regulations that said the tax subsidies may flow to all Americans purchasing insurance through any exchange, even though the law specifically says the subsidies are available via an exchange “established by a State.” Opponents of the administration’s position say the law is clear and the subsidies should be narrowed, while supporters argue that Congress always intended the subsidies to be available regardless of whether the exchange is run by a state or the federal government. In July, a three-judge panel ruled against the administration in the Halbig case, but that ruling has since been vacated and the full panel will rehear the case in December. The same day as the Halbig ruling, an appeals court in Richmond ruled in favor of the administration in the King case. The King plaintiff’s then asked the Supreme Court for a review. In their amicus brief for the forthcoming Halbig hearing, the 18 states argue that “there is no plausible reason” why Congress would have intended to deny subsidies to citizens living in states with exchanges run by the federal government.” The state AGs also argue that, under the Pennhurst doctrine, Congress must notify states of conditions imposed under certain statutes. “But there was no such clear notice here,” they write. “To the contrary, state officials reasonably assumed that federal premium assistance would be available regardless of whether a state chose to establish its own exchange or rely on a federally-facilitated exchange.” The state officials add that the Tenth Amendment’s prohibition on federal coercion of states “provides yet another reason to reject appellants’ arguments.” The ACA under the King plaintiffs’ interpretation would raise constitutional issues by threatening harm to residents and to state insurance markets as a means to pressure states into setting up exchange, and constitutional-avoidance principles “weigh heavily against such an interpretation,” they add. The brief was led by Virginia Solicitor General Stuart Raphael and included attorneys general from Arkansas, California, Mississippi, New Hampshire, Delaware, Hawaii, New Mexico, New York, Illinois, North Carolina, Iowa, Oregon, Maine, Pennsylvania, Maryland, Vermont and Washington. — Amy Lotven OMHA Seeks Advice For Improving Pilots, Reducing Appeals Backlog The Office of Medicare Hearings and Appeals on Thursday (Oct. 30) asked providers how to unclog appeals of denied Medicare claims, and in addition to seeking for advice on the general program, OMHA asked how it should fix its programs aimed at relieving the backlog and whether new programs are needed. The agency has two pilots that have not been widely used, and OMHA acknowledged they must be changed to make them useful for providers. OMHA made the request a day after it held a forum on the appeals at the Administrative Law Judge level, which is the third level of appeals where many appeals are backed up. Earlier this year, OMHA created the Settlement Conference Facilitation Pilot to encourage settlements between Medicare and providers and medical-product suppliers. The agency also put forward a statistical sampling pilot to enable decisions on large numbers of appealed claims at once, based on a sampling of those claims. At the OMHA forum, OMHA Director of the Program Evaluation and Policy Division Jason Green said the pilots will be undergoing a six month evaluation. So far, there have been only 13 requests for the settlement conference facilitation pilot involving more than 2,300 appeals, and only one went to conference, he said. “Unfortunately, it did not result in an agreement, but we did learn a lot of lessons from that one, as did CMS,” Green said. Green also said there have been no offers from the statistical sampling pilot yet and no providers or suppliers have INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 3 requested to take part in the demonstration, though OMHA is considering making a few offers. Kim Brummett, vice president of regulatory affairs at the American Association for Homecare, said that while durable medical equipment suppliers are responsible for about a quarter of all the backlogged appeals, the settlement conference pilot and the statistical sampling pilot are not appealing to DME suppliers. The settlement conference requires all claims for a particular item in 2013 to be consolidated and filed together. This would take an inordinate amount of time for DME suppliers, Brummett says, because many appeals cover rental equipment, where claim denials — and the corresponding appeals — continue every month after initial claims are denied. Even if suppliers could put together monthly appeals for hundreds of rentals for a type of equipment, suppliers would still be hamstrung because the settlement conference only includes claims from 2013 not yet assigned to an ALJ. Because the pilot doesn’t mark claims that go through the settlement process as “approved,” the settlement process would not clear the way for claims from later months to be approved, and Medicare would continue to deny claims in subsequent years. The statistical sampling pilot raises similar issues around timing restrictions and the potential to cause ongoing denials, Brummett said. Brummett says the DME providers asked for a timely filing exemption for rental claims so suppliers can wait until the appeal on the initial rental equipment is decided before submitting other claims for the following months equipment rental. Such an exemption would keep the additional claims out of the appeals queue while suppliers wait for decisions on the original appeals. Although this approach would significantly cut down on the number of claims in the appeals backlog, Brummett said CMS has yet to allow for such an exemption. AAHomecare officials met with CMS about some of these issues months ago, Brummett said, and they plan to meet with OMHA again in the next few weeks to discuss how the pilot could be improved. The American Hospital Association said the settlement conference pilot doesn’t help hospitals because OMHA limited eligibility to Part B (outpatient) claims. Hospitals also are responsible for many of the claims in the appeals backlog, and AHA sued HHS over appeals-decision wait times. Lawrence Hughes, assistant general counsel for AHA, said the statistical sampling pilot raises a number of questions and concerns for hospitals. AHA said hospitals are concerned that it’s not clear how quickly OMHA intends to process requests for statistical sampling. Given the number of claims required by OMHA to participate — a minimum of 250 claims already assigned to an ALJ — and the limited 2013 timeframe when claims are assigned to an ALJ, it’s also not clear how many hospitals would have enough claims pending at the ALJ level to qualify, according to AHA. “We do recognize that we need to make some tweaks to these pilots to make them more valuable to you all in resolving these appeals,” Green said at the forum. — Michelle M. Stein CMS Bumps Dialysis Facilities’ Pay, Adds DME Policies In Non-Bid Areas CMS in its final dialysis pay rule for 2015 released Friday (Oct. 31) slightly increases pay rates for dialysis facilities by an average 0.3 percent, cuts durable medical equipment reimbursement to align with amounts paid in the durable medical equipment bidding program and adds measures to the quality incentive program. The agency projects that reimbursement changes will increase payments by 0.5 percent for hospital-based end-stage renal disease (ESRD) facilities and increase pay by 0.3 percent for freestanding facilities. CMS says urban facilities will see a 0.4 percent pay bump, while rural facilities will see a pay cut of 0.5 percent. Under the Affordable Care Act CMS is required to conduct more competitive bidding for durable medical equipment, and in the 2015 final ESRD pay rule the agency uses three methodologies based on information from the bid program to adjust fee schedule amounts for areas where the bid program hasn’t been implemented. CMS says the final rule is one of several for calendar year 2015 that reflects “a broader Administration-wide strategy to deliver better care at lower cost by finding better ways to deliver care, pay providers, and use information.” The first method adjusts the fee schedule for items and services based on regional prices with a national ceiling of 110 percent of the average regional prices and a floor of 90 percent of average regional prices. The second method adjusts the fee schedule amounts for non-contiguous areas based on the average of competitive bidding from those areas or the national ceiling, using whichever price is higher. For rural areas the national ceiling will be extended for areas outside a metropolitan statistical area, even if the state the area lies in is not considered a rural state. These methodologies were outlined in the proposed rule in July, and at the time the consultant group Applied Policy said the fee schedule adjustments would decrease durable medical equipment payments by more than $7 billion over five years, form 2016 through 2020. In the ESRD quality improvement program (QIP) CMS is reducing payments by up to 2 percent for facilities that do not meet or exceed performance goals. For 2017, CMS adds eight clinical measures and three reporting measures for the quality improvement program in the areas of anemia management, dialysis adequacy, vascular access type, patient experience of care, infections, hospital 4 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 readmissions and mineral metabolism management. For 2018, CMS adds 11 clinical measures and five reporting measures in the areas of anemia management, dialysis adequacy, vascular access type, patient experience of care, infections, mineral metabolism management, safety, pain management, depression management and hospital readmissions. The agency says these new measures are meant to incorporate more quality-of-life issues into the program. “The ESRD QIP is intended to promote high-quality care by dialysis facilities treating patients with ESRD. This program changes the way CMS pays for the treatment of ESRD patients by linking a portion of payment directly to facilities’ performance on quality measures,” CMS says. — Todd Allen Wilson Aetna Sees Profitability, Stability In Exchange; To Drop Non-ACA Plans Aetna CEO Mark Bertolini told investors this week that the company is making a modest profit from exchange business, but is losing money on its off-exchange individual plans, which the company suggested it will no longer be offering in hopes that individuals will transition to its exchange QHPs. Aetna officials also said that they expected about $320 million in receivables from the health law’s temporary reinsurance program, and, for the first time this year, recorded a net payable of $97 million related to the ACA risk adjustment and risk corridors. Officials said that the large insurer has about 600,000 people enrolled in qualified health plans (QHPs) purchased through the exchanges, and another 500,000 in off-exchange enrollment. The company’s total medical membership is at 23.6 million, but that is expected to fall by 200,000 primarily due to projected declines in the individual exchange and off-exchange market. Overall, the individual market is a loss year-to-date and for the year, Bertolini told investors, according to a transcript from Seeking Alpha. The exchanges are marginally profitable and there are losses in the off-exchange market, he adds. He said the company will no longer be selling non-ACA compliant plans, even though it would be allowed to do so under the administration’s transitional “keep your plan” policy. That business, he said of the off-exchange plans, will either decide to leave Aetna or will buy exchange plans which generally have higher premiums. Bertolini later told investors that he expects that the public exchanges will be more stable than the off-exchange market, which turns over about one-third of its membership every year. On pricing, Bertolini said that the market is rational and that Aetna’s products are “pretty much in the middle maintaining our competitive position.” He said that in areas where there have been concerns about how regulators would react to rate increases, officials have had conversations beforehand in order to “get the rates where we’re most comfortable.” Officials also said the company recorded $110 million in reinsurance receivables for the quarter, which makes a yearto-date total of $162 million. Aetna expects that the full reinsurance total could exceed $320 million. Additionally, for the first time, the company recorded a net payable of $97 million related to risk adjustment and risk corridors for the ACA compliant individual and small group plans, Aetna Chief Financial Officer Shawn Guertin said. Bertolini explained that the government has not provided official data to do the risk adjustment/risk corridor calculations, so Aetna is relying on a consultant who is gathering data from as many payers as possible in order to get a better assessment of where the company’s risk profile stands compared to the average. The data arrived in late September, and upon looking at the data — which he acknowledged is not perfect as some payers were missing - “it became fairly evident” Aetna would be in a payable position for risk adjustment. Aetna also reported that Medicaid enrollment grew by 44,000 members primarily related to the expansion. The company also added 14,000 members for Medicare Supplementary products, 22,000 new Medicare Advantage members and 5,000 dual eligibles. — Amy Lotven SUBSCRIPTIONS: 703-416-8500 or 800-424-9068 [email protected] NEWS OFFICE: 703-416-8577 Fax: 703-416-8543 [email protected] Health Group Publisher: Chief Editor: Managing Editor: Associate Editor: Contributing Editor: Donna Haseley ([email protected]) John Wilkerson ([email protected]) Michelle M. Stein ([email protected]) Todd Allen Wilson ([email protected]) Amy Lotven ([email protected]) Production Manager: Production Specialists: Lori Nicholson Daniel Arrieta, Michelle Moodhe Inside CMS is published every Thursday by Inside Washington Publishers, P.O. Box 7167, Ben Franklin Station, Washington, DC 20044. Subscription rates: $705 per year in U.S. and Canada; $755 per year elsewhere (air mail). © Inside Washington Publishers, 2014. All rights reserved. Contents of Inside CMS are protected by U.S. copyright laws. No part of this publication may be reproduced, transmitted, transcribed, stored in a retrieval system, or translated into any language in any form or by any means, electronic or mechanical, without written permission of Inside Washington Publishers. INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 5 CMS Slightly Raises Outpatient Payments, Moves To Package Some APCs CMS finished plans to shift hospital outpatient payments toward a more complete prospective payment system by bundling payments for certain primary procedures in the final hospital outpatient and ambulatory surgical center pay rule released Friday (Oct. 31). The rule also finalizes the pay schedule for Part B outpatient drugs, slightly raises hospitals’ expected outpatient payments over what the agency had proposed and finalizes a process to allow CMS to recover overpayments from Medicare Advantage and Part D (drug) plans. The final rule raises hospitals’ outpatient payment rates slightly from a 2.1 percent increase in the proposed rule to a 2.3 percent increase for 2015, including a market basket increase, outlier payments and a 0.2 percent cut required by law. Ambulatory Surgical Centers will see a 1.4 percent update in 2015, according to CMS. The agency says it will keep payments for Part B drugs in hospital outpatient departments at the average sales price plus 6 percent for certain drugs and biologicals that CMS pays for separately under the Outpatient Prospective Payment System (OPPS). The agency also finalizes a comprehensive-Ambulatory Payment Classifications policy for some Ambulatory Payment Classifications with a high-cost primary service that generally includes device implantation. The C-APCs move outpatient payments toward paying for larger packages of items and services rather than paying separately for each, the agency says, and IHP had previously reported that the shift makes the OPPS more consistent with a prospective payment system rather than a hybrid of a prospective payment and a fee schedule. CMS first laid out a C-APC policy in the 2014 payment rule, but didn’t implement it right away in order to “provide the agency and hospitals with more time to evaluate and comment further on the policy.” CMS finalizes 25 out of the 28 C-APCs laid out in the proposed rule. The agency says it dropped three of the proposed C-APCs because a number of higher cost non-comprehensive services are often performed alongside what is included in the APCs, and a single payment would cause hospitals to be significantly underpaid for these procedure combinations, the agency says. “By providing a single comprehensive payment for services assigned to C-APCs, Medicare is providing the hospital with improved incentives to provide efficient and high quality care at lower cost,” a CMS fact sheet says. The rule also finalizes a proposal for hospital outpatient outlier payments that it estimates will target about 1 percent of total outpatient spending. To be eligible, CMS says, the cost of a service must be more than 1.75 times the APC payment rate and more than the 2015 fixed dollar threshold of the APC payment plus $2,775. In the proposed rule, CMS said the cost of service would need to be more than the 2015 fixed dollar threshold of the APC payment plus $3,100. CMS also says it is finalizing a proposal to require physician certification for inpatient hospital stays only for outlier cases and long hospital stays that last 20 days or more. CMS currently requires a physician certification, which includes an admission order, for all inpatient admissions. The agency says that the admission order will continue to be necessary for all patients formally admitted to a hospital. The rule also lays out a process to allow CMS to recover overpayments that come from “erroneous payment data” submitted by Medicare Advantage Plans and Part D plans. MA and Part D plans are paid, in part, using information submitted to CMS by the plans, such as diagnosis data that CMS uses to risk adjust MA and Part D payments. If the plans submit inaccurate data, they can submit corrected data to CMS, and the agency notes that prior to setting up a system to recover such payments, CMS has typically just asked MA and Part D plans to make corrections voluntarily. CMS also lays out a three-level appeals process to MA and Part D plans to seek review of CMS’ decision that payment data are inaccurate. — Michelle M. Stein Final Doctor Pay Rule Delays Transparency Measure; Adds ACO Measures The final 2015 pay rule for physician services puts off pay-transparency measures until 2017; assigns the first pay rates for new care-management codes; implements Obamacare’s value-based pay modifier; finishes changes to several quality reporting initiatives, including for accountable care organizations; and combines pay for sedation and colonoscopy to avoid surprising seniors with copays for screening that is supposed to be free. The Physician Fee Schedule is among three pay rules that CMS published Friday evening (Oct. 31), the others covering dialysis and hospital outpatient services. One of the more closely watched policies in the physician payment rule is referred to as payment transparency. The current process does not let physicians comment on changes to payment before they take effect. That hadn’t been a problem when CMS approved some 90 percent of pay updates that physicians suggested as part of the American Medical Association’s Relative Value Scale Update Committee (RUC). However, now that CMS’ approval rate of RUC’s recommendations is around 65 percent, providers want the agency to publish pay rates in an annual proposed pay rule to give 6 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 them the opportunity to request changes. At issue is when CMS should implement that policy. The American Medical Association was at odds with a handful of specialists, including free-standing radiation therapists and gastroenterologists, over whether CMS should wait until 2017 to implement the transparency measure or implement it immediately. CMS found a way to please both. (See story p. 19.) The final rule also details what Medicare pays primary care doctors to manage a patient’s care. Medicare primarily pays for in-person care-management services, but last year CMS created new pay codes for managing care in phone calls and emails, if patients have two or more chronic conditions. This year’s rule provides more details on that policy, including payment rates. The final rule also includes policies that implement the value-based pay modifier, which bases reimbursement on the quality and cost of care that physicians provide. CMS must apply the value-based modifier in January. CMS excluded physician practices with fewer than 10 doctors from the increased pay cuts in 2017 — starting that year the providers in practices of 10 or more face up to a 4 percent pay cut from the value modifier. CMS also finished changes to several of the quality reporting initiatives, including the Physician Quality Reporting System, Medicare Electronic Health Records Incentive program and the Medicare Shared Savings Program, commonly called the ACO program. The rule also covers changes to the Physician Compare website on Medicare.gov. CMS also included a colonoscopy measure designed to avoid undermining the Obamacare policy of free screening services. Colonoscopies involve sedation, and sedation is paid separately, so even though patients get colonoscopies for free they have ended up with a copay for the anesthesia. The 2015 pay rule combines the two services so seniors aren’t surprised with copays for a screening service they thought was free. — John Wilkerson Georgetown Center Launches Online Navigator Resource Guide Georgetown University’s Center on Health Insurance Reforms has launched a new online resource for navigators and any others who may be answering consumer questions about the Affordable Care Act. The Navigator Resource Guide includes nearly 300 frequently asked questions and easy-to-read background information on key reform policies, CHIR says. The guidance is broken down into four sections, based on the different circumstances that are often presented by consumers. These include people without coverage; people with coverage; employers offering coverage; and postenrollment coverage issues. The guide will be updated in real time in order to keep pace with the regulatory landscape. It was developed with funding from the Robert Wood Johnson Foundation, and is part of a project that provides technical and policy support — including helping answer some of the most complex consumer questions — to in-person assisters in six states: Arizona, Arkansas, Florida, Georgia, Michigan and Ohio. It was also developed in collaboration with the Center for Budget and Policy Priorities, Georgetown’s Center for Children and Families and the Kaiser Family Foundation. — Amy Lotven CMS Finalizes 2015 Home Health Face-To-Face Changes, 0.3 Percent Cuts CMS released a home health pay rule Thursday (Oct. 30) that finalizes changes to the face-to-face and therapist reevaluation requirements and sets a 0.3 percent pay cut for home health agencies in 2015. The National Association for Homecare and Hospice says the final rule is a slight improvement over the proposed version, as the changes to face-toface assessments and therapy reassessment requirements are welcome. CMS’ final rule replaces the current therapy reevaluation requirements — which require reassessments on visits 13 and 19 — with a requirement that a qualified therapist reassess beneficiaries every 30 days. NAHC says the changes are good news, and the American Hospital Association says CMS’ changes are in line with its recommendations. The agency had originally proposed to make reassessments necessary every 14 days. The agency also had also solicited comments in the proposed rule on a potential home health value-based care purchasing model, which it is considering for 2016, and says in the final rule that, if it decides to move forward with such a model, it will ask for comments on a more detailed model proposal in future rulemaking. CMS says it is considering tying 5 percent to 8 percent of home health agencies’ payments to quality performance across various measures, and that the model would apply to all home health agencies in five to eight states the agency selects to participate in the model. CMS says some in the industry thought tying 5 percent to 8 percent of payments was too much considering home INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 7 health margins, especially when compared to the hospital value-based purchasing program. But others said a high payment incentive is a good thing because it will pay back providers for an investment in quality. Some in the home health industry have also complained that a 0.3 percent pay cut as finalized in Thursday’s rule, which includes the second of four years of rebasing cuts, is too large. The Partnership for Quality Home Healthcare has said that the rebasing cuts are so large that many home health providers will be operating at a net loss by 2017. The group has pushed for fraud-fighting legislation, post-acute care bundling and value-based purchasing instead of across-theboard cuts. The Medicare Payment Advisory Commission, however, told CMS in comments on the proposed rule that the rebasing cuts are too small. “As the Commission reported margins of 12 percent or higher for for-profit and non-profit home health agencies in 2012, we do not expect this rule to materially affect the operations of most agencies,” MedPAC said. NAHC says the rule’s changes to the Affordable Care Act’s face-to-face requirement — namely the elimination of the physician narrative requirement that led NAHC to sue CMS — are great news. The agency proposed to eliminate the physician narrative in the proposed payment rule after NAHC filed a lawsuit over provider frustrations with the required brief narrative describing patients’ clinical conditions and how they support home-bound services. Home health providers had complained there was confusion over what the narrative required, and claims were denied due to documentation issues over which they had little control. The final rule also says that if a home health claim is denied, the physician claim for certifying that patient’s eligibility for services will be denied as well. CMS’ final rule also says that home health agencies must submit 70 percent of their patient assessments beginning in 2015 as a condition of payment and for quality measurement purposes. — Michelle M. Stein HHS/IRS To Draft Rule Requiring Employers Cover Hospitalization The Obama administration will soon issue regulations requiring that employer plans adequately cover hospital and physician services — a move announced Tuesday (Nov. 4) aimed at closing an ACA loophole unveiled by news reports earlier this year that some employers were offering plans that met the administration’s minimal value standards, based on CMS’ MV calculator, even though they didn’t cover in-patient hospital services. The upcoming rule will allow employees already enrolled in plans lacking hospitalization coverage to get ACA subsidies to buy plans on an exchange. The administration says in a Nov. 4 notice that the upcoming regulations will ensure adequate hospital and physician services are included in all employer plans in order to meet the ACA’s minimal value threshold. The notice adds that employers who entered binding contracts prior to Nov. 4, as long as the plan year starts on or before March 1, 2015, will not be at risk of penalties under the employer mandate, and that employees of firms that are providing coverage without adequate provider services will not be barred from receiving subsidies if they choose to purchase a plan on an exchange. The move follows reports by Kaiser Health News earlier this year that some employers’ plans met the administration’s minimal value standards even though they didn’t provide in-patient hospital services While large employers do not need to cover all 10 of the essential health benefits, they still must offer a minimal value of at least 60 percent of the costs of the benefits provided by the plan. The notice affirms that an employer plan must offer in-patient and physician services, and cannot use the minimal value (MV) calculator as a safe harbor from penalties if such coverage is not available. The American Hospital Association, which says member had been alarmed by the situation and had expressed concerns to CMS, praised the latest move. “Comprehensive inpatient hospital coverage is critical. We are pleased that the Department of Health and Human Services and the Department of the Treasury will require that large employer health plans cover hospitalizations to meet the ACA’s minimum coverage standard,” AHA President Rich Umdenstock said in a statement.” He continued: “One of the goals of the ACA is to protect all Americans from receiving sub-standard health insurance coverage that leaves them vulnerable to poor health outcomes and potentially disastrous financial stress. While these types of insurance offerings may not be widespread, hospitals and health systems were deeply concerned about plans that potentially excluded important hospitalization and are pleased with the action to address the matter in the best interest of patients.” In the notice out Tuesday, HHS and IRS say they believe plans failing to provide substantial coverage for in-hospital services or for physicians services — or both — do not provide the minimum value intended by requirement. The departments say they will be proposing regulations shortly that will be finalized and applicable for 2015. But the departments add: Solely in the case of an employer that has contracted with and or has already begun enrolling employees in a so called “Non-Hospital/Non-Physician Services Plan” prior to Nov. 4, 2014 based on the employer’s reliance on the results of use of the MV calculator, that employer will not be subject to penalties under the mandate as long as that plan year begins no later than March 1, 2015. However, pending issuance of the rules, an employee will not be required to treat such plans as providing minimum 8 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 value, which means that they would have access to the subsidies. Additionally, HHS and IRS will require that employers offering the Non-Hospital/Non-Physician Services plans must not state to employees that the offer of coverage precludes an employer from getting the credits if otherwise eligible, and must correct any notices that say the opposite. If an employer offers another plan that does meet the threshold, however, the firm is permitted to advise an employee that they would not be eligible for credits upon choosing that plan. — Amy Lotven OIG Plans To Monitor Early Experiences With Drug Tracing System The HHS Office of Inspector General plans to evaluate supply chain stakeholders’ early experiences with trading drug transaction information as required at the beginning of next year. The HHS investigative arm will also probe FDA inspections of high-risk food facilities, drug sponsor compliance with clinical trial reporting requirements, FDA oversight of postmarketing studies of approved drugs and inspections of generic drug manufacturers, according to OIG’s work plan for fiscal 2015. The Drug Quality and Security Act mandates that an interoperable drug tracing system be created during the course of 10 years. Trading partners in the drug supply chain must exchange drug transaction information and histories in a single paper or electronic document starting Jan. 1, although dispensers have until July 1 to meet the requirement. “Together, this information forms the foundation of drug traceability and the security of the drug supply chain...We will interview trading partners about how they have successfully exchanged this information and what, if any, obstacles they have faced.” OIG expects to issue this assessment during fiscal 2015. Other reports expected during fiscal 2015: Drug sponsor compliance with clinical trial reporting requirements: OIG plans to evaluate the extent to which clinical trials are in compliance with requirements that certain studies be registered and the results reported in ClinicalTrials.gov. FDA oversight of postmarket studies: OIG plans to evaluate the extent to which FDA requires postmarket studies and clinical trials for new drug applications, and how the agency monitors and enforces these postmarketing requirements. Generic drug manufacturer inspections: OIG plans to study the scope of FDA inspections of generic drug firms, the results of inspections, and enforcement actions taken. The agency generally inspects these facilities before approvals and routinely thereafter. The Generic Drug User Fee Amendments includes new goals and funding for facility inspections. FDA inspections of high-risk food facilities: The Food Safety Modernization Act mandated that FDA more frequently inspect domestic food facilities based on risk and provided criteria for designating a facility as high risk. OIG plans to assess FDA’s designation and inspection of high-risk facilities. Drug compounding oversight: Medicare oversees the safety of drugs compounded at Medicare-participating hospitals through an accreditation and certification process. OIG plans to evaluate whether Medicare’s oversight of acutecare hospitals addresses recommended practices for drug compounding oversight. — Alaina Busch McBournie CMS: New Data To Show Steep Decline In Individuals With Inconsistencies CMS will soon release final data showing a “steep decline” from earlier estimates of the number of individuals with data matching problems on their exchange applications, an agency official said Wednesday (Oct. 29). The agency has already moved to terminate about 115,000 people with citizenship-related inconsistencies on their applications, and in September announced that 279,000 households, or about 360,000 individuals, could be at risk of losing all or part of their federal subsidies if they do not submit documents validating their income. In September CMS had said that it would take action on the income inconsistencies by Nov. 1, but has not updated the numbers since then. The agency did not reply to queries from Inside Health Policy when asked about the figures on Tuesday (Oct. 28). On Wednesday, agency spokesperson Aaron Albright said: “We anticipate releasing the final data matching numbers soon, which will show a steep decline in the original number of individuals and households with data matching issues. We are doing everything we can to make sure people who are eligible stay covered and that no one is receiving Marketplace coverage or premium assistance they shouldn’t.” Albright also confirmed that the new numbers will include figures on all data matching issues — not just income inconsistencies. The data matching issues are created when information consumers report on their exchange applications cannot be matched with existing electronic resources. HHS, and consumer advocates stress that an application inconsistency does not mean a consumer is ineligible for enrollment or subsides, but just that more documentation is needed. — Amy Lotven INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 9 CMS Looks To Expand PACE-Like Care To Younger Populations CMS is looking to launch a pilot to provide integrated care similar to the Program of All-Inclusive Care for the Elderly to a younger population, according to one CMS official. Those with the National PACE Association say expanding PACE to other populations that would benefit has been a goal for quite some time, and PACE programs would likely be well positioned to participate in any demonstration or pilot put forward by CMS. The population of younger people with disabilities is a big Medicaid population that could benefit from PACE-like care, according to Robert Greenwood, vice president of public affairs at the National PACE Association. But the ball is in CMS’ court, Greenwood says, and PACE organizations are looking for a Request For Proposals to see what CMS envisions as goals for the pilot. PACE programs currently serve those who are 55 or older and are certified by their state to need nursing home care but are still able to live safely in the community. There are currently 104 PACE programs operating in 31 states, according to the National PACE Association. The Medicare-Medicaid Coordination Office recommended in their most recent report to Congress that the PACE program be expanded to those ages 21-55 with disabilities. A CMS official recently explained that CMS doesn’t have the authority to change the eligibility requirements for the PACE program itself because the program — including what population it should serve — is laid out in the Balanced Budget Act of 1997, but the agency is interested in exploring the concept of whether more individuals would benefit from the interdisciplinary care and social interaction that a similar program could provide. Greenwood says that younger people with developmental disabilities, those with chronic care needs that require a steady environment rather than episodic care and some with behavioral health needs could likely benefit from PACE-like care. A pilot looking to provide such care would likely require those interested in participating to provide a variety of services similar to what’s required in the PACE program, so existing programs would be well suited to take part in a demonstration, whereas other potential sponsors might not be familiar with certain interdisciplinary care aspects, transportation or some other part of the PACE program, Greenwood says. PACE programs not only have integrated Medicare and Medicaid financing, but care delivery is patient-centered and interdisciplinary, Greenwood says. One thing existing programs will be looking for is to make sure that any pilot also allows programs to be integrated and interdisciplinary, and doesn’t become a provider-focused model that is closer to managed care, he added. PACE programs are already looking at changes that might be necessary to serve an expanded population, Greenwood says, and how an interdisciplinary team could be put together to best serve any other populations while they wait for an official Request for Proposals. — Michelle M. Stein Rollback In States With New GOP Govs. Unlikely . . . begins on page one Tuesday’s election. “Expansion will depend on both the outcomes of the governors’ races, as well as state legislative balance, as state legislatures often hold the keys.” But Republicans won in five of the six states Avalere looked at — Kansas, Georgia, Florida, Maine and Wisconsin — and Carpenter doesn’t see these governors moving to expand Medicaid. The race in Alaska between incumbent GOP Gov. Sean Parnell and Independent Bill Walker is still too close to call and may not be decided until all absentee ballots have been counted on Nov. 19. Early Tuesday (Nov. 4) HHS Secretary Sylvia Burwell made a pitch to Republican governors reluctant to expand Medicaid, saying CMS will work with them to expand the program in their own way, as it has done with Arkansas, Pennsylvania, Iowa and Michigan. “The law allows for flexibility so individuals with disabilities can continue to live in their communities, beneficiaries can access integrated care, and states can test new payment and delivery system reform models that can improve care while spending dollars more wisely,” Burwell said at the National Association of Medicaid Directors conference in Arlington, VA. But Carpenter said that Burwell’s entreaty will fall on deaf ears in the near future. She did note, however, that states that are already in negotiations with CMS to find alternative ways to expand Medicaid, such as Utah and Tennessee, will most likely continue with that process. In three states that have already expanded the program but saw Republicans win the governor’s races — Illinois, Massachusetts and Maryland — Carpenter doesn’t expect to see a rollback of the expansion because their state legislatures are still firmly in Democratic control. “It’s certainly difficult for any new governor to turn on a dime and take benefits away from people who already have them,” she said. “Any time there’s a change in power there is always a possibility for a new governor to make existing policy look more like their own approach to politics, but particularly in those traditionally heavy blue states I wouldn’t 10 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 anticipate significant changes to the Medicaid expansion.” Following is a break down of the races in the states where Avalere said Democratic or Independent wins could have renewed Medicaid expansion fights depending on the outcome of the elections: Alaska: Independent Bill Walker holds a slight lead over GOP incumbent Gov. Sean Parnell but the race is considered too close to call. Election observers expect the race to be decided by absentee ballots, which are due to come in by Nov. 14 and counted by Nov. 19. The Alaska governor’s race became competitive in September when Democratic candidate Byron Mallott dropped out of the race for governor and joined Walker’s campaign as the Independent’s running mate for lieutenant governor with the full blessing of the state Democratic Party. Following the election Alaska’s legislature remained in full control of the GOP. Florida: Republican incumbent Gov. Rick Scott beat back a challenge by former-GOP governor turned Democrat Charlie Crist. Crist had promised to expand Medicaid through an executive order should he win. Scott tried to expand Medicaid in 2013 but was stopped by a heavily-GOP controlled state legislature. Republicans continue to control the state’ legislature following the election. Georgia: GOP Gov. Nathan Deal beat Democrat Jason Carter, grandson of former President Jimmy Carter, and Libertarian Andrew Hunt. Republicans kept strong control of the State House in Tuesday’s elections. Kansas: Republican incumbent Gov. Sam Brownback fought off a fierce challenge from Democrat Paul Davis. Davis had gained the backing of a number of high-profile moderate Republicans angry with Brownback over a purge of moderate Republicans from the state legislature he helped orchestrate in 2012. Republicans retained firm control of the state legislature. Maine: Incumbent Republican Gov. Paul LePage won a three-way race against Democrat Mike Michaud and Independent Eliot Cutler. The race is reminiscent of the 2010 election, where Le Page eked out a win with a plurality of the vote against Cutler and Democrat Libby Mitchell. Democrats kept control of the state House of Representatives Tuesday, but some state Senate races are still in doubt leaving Republicans a chance to take control of the state’s upper chamber. Wisconsin: GOP Incumbent Gov. Scott Walker — who beat back a recall effort in 2012 and is listed as a possible Republican presidential candidate in 2016 — beat Democrat Mary Burke. The GOP kept control of the Wisconsin legislature Tuesday. — Todd Allen Wilson Howard: Matching Exposures To PPE Use Of Key Concern In Ebola Protection NIOSH chief John Howard this week outlined several major research priorities that he views as central to government - and industry-wide — efforts to protect workers from Ebola and other diseases, saying the need to match worker exposure levels to appropriate use of personal protective equipment — as well as to test methods for determining the amount of protection from a given type of PPE — are key research issues for infection control experts. Howard’s comments come as the health care industry struggles with the most effective procedures to prevent Ebola infections, especially after some cases appeared in the United States despite the proper usage, training and availability of PPE in environments of suspected Ebola. The Centers for Disease Control and Prevention has issued general guidance in the area and OSHA has begun dedicating more resources to fighting Ebola transmission in work settings. The NIOSH administrator, speaking at an Institute of Medicine conference in Washington on Monday, said the research priorities also have broader implications for pathogens even though Ebola is a major focus of present. Issues of crucial importance, according to Howard, include: 1. How to quantify worker exposure to match appropriate PPE with the required level of exposure protection. 2. The research needed to determine appropriate test methods to demonstrate that a given type of PPE will protect the worker. 3. What are the most effective donning and doffing procedures to prevent self-contamination. 4. Whether there are novel PPE designs that are more effective for health care workers to use in patient settings. 5. How best to understand PPE utilization in the health care system to better inform supply-chain issues. Howard noted that while experts have collected years of data in assigning the level of protection needed in industrial settings, similar assessments are very complex in health care settings “and I don’t think we’ve done a lot of research in that area. We need to do certainly more in that area.” Further research is needed to determine the “appropriate test methods” to demonstrate that PPE will work, he added. The detailed procedures workers use to put on and take off protective equipment requires deeper research as well, he said, because much of the emphasis has been on the donning and ensuring equipment is clean, but that it is “extremely important to prevent self-contamination” and focus on doffing procedures. He also suggested that research INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 11 must be directed toward “novel PPE designs that will be more effective for health care workers to use in patient care settings.” Also he noted that a key concern for health workers — the PPE supply-chain issue — is one not often considered as a research question but “we need to determine what metrics we’re going to use in the supply-chain management for this issue.” Research needs to focus on preventing any PPE shortages, he said. Howard also pointed to three biological behavior research priorities regarding Ebola: 1. How long the virus remains viable on surfaces including PPE, taking into consideration different bodily fluids. 2. What type of disinfectants and contact times are needed to inactivate the virus. 3. What are the best sampling methods to detect viable virus on services and PPE. Research needs to be done in controlled laboratory settings on sampling methods to develop the science to be able to go out and use in the field, according to Howard, who said the first step is to make sure that the type of sampling method is reliable and validated before using it in field studies. — Christopher Cole Study: It’s Difficult To Discern Exchange Plans’ Networks Most issuers offering plans in six major cities include high-ranked hospitals in their provider networks, but consumers may find it difficult to research which hospitals are covered because they must leave the exchange website in order to see the information, according to a new study. The report, put together by Urban Institute researchers with funding from the Robert Wood Johnson Foundation, examined the hospitals offered in exchange plans available in Denver, New York City (Manhattan), Portland, Providence, Baltimore and Richmond. The report found that every hospital in each city is included in at least one exchange plan. The study also looked at how the size of the plan impacted premiums, and found that while generally those with narrower networks had lower rates that was not always the case. “For example, Oscar in New York and CareFirst in Baltimore have very broad hospital networks but relatively low premiums. United in New York and Baltimore have broad networks and high premiums,” the study found. “Every hospital in these cities participates in at least one marketplace plan, and that’s an important takeaway,” said Kathy Hempstead, who directs coverage issues at the Robert Wood Johnson Foundation. “Some consumers may want to choose the cheapest plan, while others may want to choose a plan based on access to a particular provider. We need a marketplace where all of those choices are possible,” she added. The authors worried that it generally would be “cumbersome” for a consumer to discern the size of the hospital network. For all of the study cities, with the exception of Denver, a consumer must leave the exchange website and go to an insurer’s site to research provider networks. This can be difficult for less-computer savvy people and can also create distractions that may ultimately prevent people from purchasing a plan, the authors say. Such conditions mean that many consumers are likely unaware of exactly what they are purchasing via the exchanges and whether his or her desired facility, or provider, is included in the network, they add. “Future improvements to state-based and federally facilitated Marketplace websites should better enable consumers to view the size and quality of each plan’s network,” the study says. “In the meantime, this research indicates that in six major cities, most consumers can find a plan on the Marketplace that includes his or her desired hospital, and that even relatively narrow networks are likely to include at least one high-quality hospital.” — Amy Lotven McConnell Open To Piecemeal Repeal Of ACA . . . begins on page one Affordable Care Act, but that vote is viewed as for show because Democrats and the president most certainly will not go along with it. It’s what Senate Republicans do afterward that interests lobbyists. A spokesperson for Sen. Mitch McConnell (R-KY) said prior to Tuesday’s elections that the expected majority leader supports both full repeal and piecemeal measures, especially those with bipartisan support. Were McConnell to hold votes on smaller, bipartisan measures, such as the medical device tax repeal, employer mandate repeal or the insurance tax repeal, that would not equal giving up on full repeal. On numerous occasions, McConnell said the law must be repealed “root and branch.” When he said last week on Fox News that a stand-alone repeal bill would need 60 votes and would likely be vetoed, some thought he was softening his position against law. However, the McConnell spokesperson said those people are mistaken. “He didn’t give a history lesson to explain what reconciliation means,” McConnell spokesperson Don Stewart said, referring to the budget reconciliation process that requires only 51 votes. Budget reconciliation would likely have to wait until at least April, but much of the health law, including all the taxes and the employer and individual mandates, could be axed using that approach. Others say far-right conservatives will dictate Senate Republicans’ approach to Obamacare. If think tanks such as 12 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 Heritage Foundation and such Tea Party darlings as Sen. Ted Cruz (R-TX) attack piecemeal bills as surrendering by improving the law, moderate Republicans may not want to vote for them. Conversely, repealing parts of the law could put Democrats on the defense, too, lobbyists said. Many Democrats signed onto bills repealing sections of the law. Repealing the 2.3 percent excise tax on medical devices is a prime example — Democrats with concentrations of device companies in their states have said they favor repealing the tax. However, lobbyists say some of those Democrats likely didn’t expect those bills to actually pass. The Senate voted for a device-repeal budget amendment in March, but that measure merely expressed support for repealing the tax. Lobbyists say Democrats might find themselves in a difficult position if Republicans hold a vote on those individual repeal measures because they’ll be faced with the likelihood of Congress passing them. Lobbyists say it wouldn’t be that difficult for enough Democrats to squirm out of voting for those stand-alone measures to stay within the 60-vote filibuster threshold — the GOP Senate takeover is not filibuster-proof. Also, it would be easier for the president to veto tax measures unfamiliar to the public than it would be to veto measures that are unpopular with large segments of the public, such as the individual mandate, and most of the bipartisan support has been for those repeal proposals that don’t resonate with the general public. Avalere CEO Dan Mendelson said both parties would be wise to improve the law by agreeing to repeal a package of modest calibrations that improves the law and helps businesses. He listed repealing the device tax and the employer mandate as proposals with bipartisan support that could be combined with measures that Democrats like to forge a compromise. Except for Democrats from states with a lot of device makers, repealing the device tax hasn’t fit into the goals of most Democrats, but he believes Democrats would be open to repealing the tax if it were part of a package not intended to undermine the law. The president delayed the employer mandate twice, and former White House press secretary Robert Gibbs said the mandate is not needed. Mendelson said repealing it would be a double-edged sword. It would cost money because some companies would tell employees to seek insurance on the exchanges, where some would get government subsidies. However, it also would improve the risk pools for exchange insurance. Next year the employer mandate starts phasing in for businesses with more than 100 full-time equivalent employees. Many companies protest the mandate’s cost and administrative burden. Legislation to include lower-premium copper-tier plans on exchanges could be included to attract younger, healthier enrollees. Loren Adler, a research director at the Committee for a Responsible Federal Budget, said most of the repeal measures with bipartisan support add to the deficit. The nonpartisan budget think tank does not take a position on those Obamacare-repeal measures, other than that Congress should pay for them. Adler notes that rules in the Senate prohibit budget reconciliation from adding to the deficit but Congress could change that rule. Leavitt Partners also discusses the potential to use budget reconciliation as a means of pushing through certain reforms, yet the firm notes that the mechanism is subject to the so-called Byrd rule, which requires that legislation be germane, not add to the deficit and either decrease spending or increase revenues. Leavitt Partners’ primer spells out ways the GOP could push its priorities, including in the upcoming debt ceiling debate (current debt ceiling authority is set to expire on March 15), the appropriations process and the budget process. The GOP also could use committee hearing to shine light on problems with the ACA, the Leavitt primer says. The primer suggests the device tax and employer mandate would most likely be dealt with either during the debt SUBSCRIPTION ORDER FORM Sign me up to receive Inside CMS at $705 per year in the U.S. and Canada; $755 per year elsewhere (air mail). Name __________________________________________________ Affiliation _______________________________________________ Address _________________________________________________ City/State/Zip ____________________________________________ Phone __________________________________________________ E-mail __________________________________________________ To order by mail: Send this coupon to Inside CMS, P.O. Box 7167, Ben Franklin Station, Washington, DC 20044. To order by phone, fax or e-mail: Call 800-424-9068 (in the Washington, DC area, 703-416-8500). Fax to 703-416-8543. E-mail at [email protected] Please check one: Visa MasterCard Bill me Check enclosed (DC subscribers add 6% sales tax) Card number _________________________________________ Name on the card _____________________________________ Signature _______________________________________________ Exp. date ____________________________________________ INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 13 ceiling fight or potentially by eliminating IRS enforcement funding during appropriations. Similarly, Leavitt says that the individual mandate could be stripped or weakened during the debt ceiling fight or also by defunding the IRS. ACA measures that the group says could move through reconciliation include lowering premiums subsidies. Additionally, changes to the ACA’s Medicaid expansion, such as reducing the 90 percent match or allowing states to expand the program to residents with incomes up to 100 percent of the federal poverty level, could come into play in either reconciliation or the debt ceiling discussions. Leavitt says changing the definition of a full-time work week from 30 hours to 40 hours, which has already passed the House and has some Democratic support, replacing the Sustainable Growth Rate or altering Medicaid also could play into the debt ceiling fight. Although the issue has been quiet for some time, Levitt’s paper suggests it is possible that efforts to scale back the health law’s Essential Health Benefits could return during the debt ceiling debate — although the proposal would be politically unpopular for consumer advocates. —John Wilkerson, Amy Lotven Burwell Touts Economic Benefits Of Expansion . . . begins on page one noted that states do not have to offer a straight expansion of Medicaid, but by working with CMS states can expand the program in “their own way.” These states have adopted different models, such as Arkansas which used Medicaid expansion funding to funnel those eligible for Medicaid under the expansion into the state’s health exchange marketplace. “The law allows for flexibility so individuals with disabilities can continue to live in their communities, beneficiaries can access integrated care, and states can test new payment and delivery system reform models that can improve care while spending dollars more wisely,” Burwell said at the National Association of Medicaid Directors conference in Arlington, VA. She pointed out that the federal government will fund 100 percent of states’ Medicaid expansion through 2016, and assured Medicaid directors that federal funding would never dip below 90 percent thereafter. She also said that should states decide to expand the program and then don’t like the results the law allows them to back away. “The funding isn’t going away, and just as your state can choose to expand at any time, you can also reserve the right to change your mind,” Burwell said. “Not only that, Medicaid spending per enrollee continues to grow at slower than anticipated rates — we’re getting more bang for our buck.” Beyond improving the overall health of the residents of their states, Burwell said there are economic benefits for states that expand Medicaid. She cited a recent Kaiser report that found that state Medicaid costs are growing at a lower rate in states that have expanded the program when compared to states that haven’t. Burwell also noted a report issued in July by the President’s Council of Economic Advisers that said expansion states are expected to see 350,000 new jobs total by 2017, while non-expansion states are leaving 380,000 jobs on the table. Burwell said the ultimate goal is to expand affordable health care coverage to as many people as possible while improving quality and controlling costs. “We want every American to have access to quality health coverage they can afford,” Burwell said. “And we want to do everything we can to help support states to meet the needs of their constituents. Our belief is that your health care shouldn’t be caught up in red tape and it shouldn’t put your family in the red.” — Todd Allen Wilson Medicaid Chiefs Seek Flexible Quality Measures In New Managed Care Reg The National Association of Medicaid Directors is asking CMS to develop a joint federal-state framework for driving quality reforms in states’ manged care organizations that gives states flexibility to tailor programs to the diverse needs of their beneficiaries. NAMD’s recommendations came just days before CMS dropped hints about its plans for the first major updates to Medicaid managed care regulations in 12 years, with the agency saying the new regulations will come out next year. “We urge CMS to continue working with states to carefully plot a path forward around the quality framework in managed care that recognizes the variations between Medicaid programs and the risk-based approaches within each state,” NAMD writes to Cindy Mann, director of Medicaid and CHIP services. The letter marks the group’s fourth set of recommendations to CMS on planned updates to Medicaid managed care regulations. CMS, as it develops a joint federal-state quality strategy, should design a framework that drives greater alignment with other programs where Medicaid is the primary payer such as is the case for dual-eligibles, NAMD says. On Tuesday (Oct. 28) a CMS official speaking at the Medicaid Health Plans of America conference said the agency is looking to align Medicaid managed care with other public programs such as Medicare Advantage, dual eligible initiatives and qualified health plans sold in the exchanges, because many beneficiaries will move among those programs as their income fluctuates. NAMD would like to see a strategy that promotes a greater alignment of the quality requirements of the electronic 14 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 health records (EHR) incentive program. “This focus will drive the use of electronic quality measures, which will support a data-driven approach to delivery system transformation. Ultimately, this Medicaid-focused strategy is necessary to achieve alignment across a program with diverse populations and delivery approaches, and which needs to align with other payers such as Medicare,” NAMD says. The group warns that CMS should not put forward a national “one-size-fits-all” set of quality standards and measures. This is because states need to tailor their Medicaid managed care programs to the specific populations and needs of their varied beneficiaries, the Medicaid directors say. “(T)he plans designed to provide Medicaid services in each state are unique and difficult to compare at a national level. Because of these differences, we believe it is not appropriate for CMS to require a state’s health plan entities and providers to meet national benchmarks,” NAMD writes. Instead NAMD suggests that CMS develop a menu of core standards and quality benchmarks that states can pick and choose from to report on so that measures states assess are tailored to the specific populations treated in individual Medicaid managed care programs such as long-term care for people with “special needs.” In conjunction with this NAMD asks that CMS refrain from developing a national rating system — similar to other star rating systems the agency has in place — because such a system would fail to “account for the differences in state Medicaid programs and the subpopulations enrolled in risk-based entities.” “For example, an entity tailored to serve a state’s aged, blind, and disabled population would have substantially different features than an entity designed to serve a Medicaid expansion population,” NAMD says. NAMD says rather than a national system, states are best positioned to develop a quality-rating framework for consumers, noting that many states have already made progress in designing such tools for consumers and assistors. CMS should look to see what states have already done and promote and disseminate effective practices in this area, NAMD says. This, NAMD says, should be part of a broader effort on the agency’s part to identify best practices states are using to promote quality in their Medicaid managed care programs. The organization of state Medicaid directors says as part of this effort CMS should facilitate webinars and meetings where state Medicaid programs can have peer-to-peer discussions about what they find works best for their specific programs. Once core measure specifications are determined CMS should maintain those quality measures for three to five years, the organization says. NAMD notes that CMS often amends quality measures on an annual basis, “which can present a barrier to accurate longitudinal measurement and make it difficult drive quality improvement among health plan entities and providers.” “To the greatest extent possible, CMS should provide stability around the measure specifications over time to allow for meaningful improvement, while balancing this need with emerging scientific evidence,” NAMD says. NAMD’s recommendations came on the heels of a request for information from CMS’ innovation center on Medicaid managed care reforms involving pharmacy and medication management, value-based insurance design, telehealth, hospice care, long-term services and supports, network design, behavioral health and provider incentives. The agency’s innovation center said in a broader request for information issued Oct. 2 that health plans have increasingly come up with innovations in care delivery, plan design, beneficiary and provider incentives and network design. But use of these innovations in CMS stand-alone programs — such as Medicaid managed care, Medicare Advantage, Medicare Prescription Drug Plans — that use health plans as delivery systems has been limited, CMS said. — Todd Allen Wilson WellPoint Hopes To Retain 2014 Exchange Market Share In Year Two WellPoint officials reported Thursday (Oct. 30) that the insurer now has 751,000 members enrolled in exchange plans, down from 769,000 at the end of the second quarter but still more than the 600,000 the company had expected for 2014, and officials expressed hope the company would retain its market shares for 2015. WellPoint CEO Joseph Swedish said that the company plans to offer exchange plans in the same 14 states as in 2014, although in more service areas, and will build out on what he called a “tremendous success” over the years in terms of pricing and marketing efforts that drove enrollment. Swedish attributed the decline in exchange members to normal seasonal attrition, often seen in the third and fourth quarters. “Our sales assumptions are lining with what we expected, which was that many individuals would have life event changes [and] many individuals are getting jobs, in some cases moving from exchange into an employer-based coverage,” he said, according to a Seeking Alpha transcript. The trend is expected to continue going into the fourth quarter, with a ramp-up in growth starting in January, he added. WellPoint will participate in 139 rating regions this year. He said that while there will be some adjustments to the INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 15 marketplace strategy, “generally speaking in terms of our pricing, our marketing efforts, et cetera, I think it will look remarkably similar to the efforts that we employed in ’14.” Swedish added: “Long story short, we really continue to feel strongly about the value proposition we are bringing to the market. And as you may know, CBO estimates indicate something like 5 million lives may come into the exchange environment.” Swedish also said he believes that the company will be able to capture relatively the same share of the market in 2015 as it did last year. According to a recent Avalere analysis of 12 regions, WellPoint carries a large market share in California, Colorado, Connecticut, Indiana and Virginia. An investor pointed out that while the rate increases for 2015 have been modest, some of the benchmark plans had lower increases, which results in higher premiums for the subsidized consumers, and questioned if WellPoint expected to see some churn due to this. Swedish said it is fair to say there will be some degree of churn, which is common in every book of business and especially the individual market, but he added that WellPoint still expects to see net growth. “I don’t know that we’ll maintain exactly the same market share because it is very much dependent upon the competitive environment. But we think what’s probably most important for the consumer is predictability and affordability,” he said, noting that WellPoint’s pricing is “less volatile” than others have reported in recent filings. On margins, Swedish told investors that WellPoint remains comfortable with the goal of a 3 percent to 5 percent range, but noted that margins vary by market. “We have opportunities to improve margins in certain markets and, in fact, I would argue we have opportunities in all markets to improve margins,” he said. He said that the company expected the cost trends on exchange business to be much higher than non-exchange business trends. While that has proven to be true, the costs were not as high as expected, he added. Additionally, he said, once the exchange members are put into more managed care programs the underlying trends should migrate toward the non-exchange business trends, which would result in higher margins. “So we still think 3 to 5 (percent) is reasonable and our goal would be to eventually target closer to the 5 than the 3,” he said. The general characteristics of the exchange enrollees, including the average age, continue to “track well” with expectations, and product selection and benefit levels have also been consistent with predictions, Swedish said in prepared remarks. “We’ve been executing upon our exchange roll-out, and paid claims trends thus far are encouraging. But we recognize many of these new members only joined our enrollment rolls in May. Therefore, we continue to take a prudent view of reserves in light of the potential uncertainties associated with this membership and expect to gain more information as this block matures in the fourth quarter,” he said. Officials also said the company continues to book for reinsurance “as appropriate” and has a recorded a modest net payable for the risk corridors. WellPoint believes it will be in a “modest net receivable” position for the risk adjusters, but notes that official numbers are unlikely to be available until the second quarter of 2015. WellPoint also said it continues to lose small group members faster than had been expected. In its previous earnings call, WellPoint reported it had shed 218,000 members, and officials said the members have now declined by almost 300,000 year-to-date. Officials said that the strategy has been to try to catch members coming through any entry point — small group or public exchanges — by offering the most affordable products. The drop off in small business membership is expected to be a $400 million or so “headwind” for WellPoint, but officials said that enrollment in public exchanges should offset that as margins start to expand. For Medicaid the company said it has added 699,000 members year to data and believes that growth will continue in the fourth quarter. WellPoint now expects to add 450,000 to 475,000 Medicaid expansion members in 2014, officials said. —Amy Lotven CME Stakeholders: CMS Gave Us What We Want . . . begins on page one CME exclusion, is applauding the agency’s clarification. Stakeholder worries stemmed from CMS saying in the proposed rule that it was getting rid of the CME exclusion because it was redundant with another provision of the Sunshine Law which excludes indirect payments or transfers to medical professionals providing CME lectures as long as manufacturers are “unaware” of the lecturers’ identities for up to a year and a half after the indirect payment has been made. CME providers argued — as CMS notes in the final rule — that given the nature of CME it’s impossible for drug and device companies to remain ignorant of speakers’ identities that are publicly available on conference agendas and elsewhere, such as trade press accounts of speaker presentations. CMS clarified in the final rule that as long as a manufacturer or GPO gives “full discretion” to the CME provider as to how to spend the money and has no input on who speakers and presenters are then it doesn’t matter if a 16 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 manufacturer or GPO finds out who spoke at an event, because those payments do not qualify as an indirect payment. “(I)f an applicable manufacturer or applicable GPO provides funding to support a continuing education event but does not require, instruct, direct, or otherwise cause the continuing education event provider to provide the payment or other transfer or value in whole or in part to a covered recipient, the applicable manufacturer or applicable GPO is not required to report the payment or other transfer of value. The payment is not reportable regardless if the applicable manufacturer or applicable GPO learns the identity of the covered recipient during the reporting year or by the end of the second quarter of the following reporting year because the payment or other transfer of value did not meet the definition of an indirect payment,” CMS says in the final rule. CMS says this type of sponsorship by manufacturers of CME events is similar to a manufacturer giving an “unrestricted donation” — meaning the money has no strings attached — to a physician professional organization, that then decides to use the money for grants to physicians. In this case the manufacturer would not be required to report the donation as an indirect payment, because the manufacturer did not direct the organization to use the money for physician grants. “Therefore, because such payments are not indirect payments, we do not need to create an additional exclusion specific to continuing education indirect payments by modifying the indirect payment exclusion at §403.904(i)(1),” CMS says. Andrew Rosenberg, senior advisor for the CME Coalition, said since accredited CME providers don’t allow manufacturers or GPOs who sponsor or donate to a CME event to dictate how the money can be spent most CME payments won’t have to be reported. “As a practical matter, because the standards for commercial support inherent in most accredited CME already prohibit commercial supporters from paying speakers directly, suggesting speakers (e.g., providing a list), or otherwise controlling the nature or content of the educational program, there will not be any necessity to report CME payments under the Sunshine Act for most accredited CME programs. Therefore the CME Coalition applauds CMS for clarifying these important rules in such a manner,” Rosenberg said. Stakeholders had also worried that if money donated by a manufacturer was used to subsidize fees for attendees at a CME event or to help pay for educational materials then they would have to be reported as indirect payments if the CMS eliminated the specific CME exclusion. CMS says that these subsidies for attendees will not have to be reported as indirect payments as long as the manufacturer does not not direct the CME provider to subsidize fees for specific attendees. The agency says it will provide subregulatory guidance on the issue. — Todd Allen Wilson Amgen Sues Sandoz In Case Involving First Biosimilar Application Amgen has sued Sandoz, the first domestic biosimilar applicant that seeks to copy an Amgen product, charging the biosimilar applicant violated the law’s patent exchange process by not sharing its manufacturing information — a move closely watched by stakeholders because the outcome may drive key patent policies as FDA begins implementing the health law’s new biosimilar pathway. Sandoz was required to share with Amgen its filgrastim application and manufacturing processes, but did not, Amgen asserts in asking a federal court to prevent Sandoz from seeking FDA approval, among other legal requests. Amgen filed a lawsuit in the U.S. District Court for the Northern District of California last Friday (Oct. 24) alleging Sandoz with patent infringement, unfair competition and conversion — using Amgen’s product for its benefit and profit. The patent exchange process is untested and was expected to be a point of contention within the new biosimilar pathway. Amgen’s court filing shows that the two companies did not get past the first step of the statutorily mandated process. Sandoz said the legal action did not come as a surprise. “As Sandoz is the first company using the pathway to bring cost-effective biosimilars to market in the U.S., it is understandable that Amgen and Sandoz might take a different view of the (Biologics Price Competition and Innovation Act) provisions,” the company said in a statement. “We look forward to the court’s resolution of this matter and Sandoz will not comment further on the litigation at this stage.” New biosimilar applications are subject to 10-month review timelines under the Biosimilar User Fee Act and Amgen calculates that, absent the court intervening, FDA’s approval of Sandoz’s product could come in May or earlier. In July, FDA accepted Sandoz’s biosimilar filgrastim application — a copy of Amgen’s Neupogen. At that point, the two companies were supposed to engage in a series of exchanges to determine which patents, if any, the two companies would litigate. The process did not pan out as required, according to Amgen’s court filing. Amgen alleges that Sandoz’s actions are “part of a carefully orchestrated scheme to deprive Amgen of the substantive and procedural benefits of the BPCIA.” Within 20 days of receiving notice that FDA has accepted a biosimilar application for review, the applicant must INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 17 share a copy of the application, including manufacturing processes, with reference product sponsor. Sandoz was supposed to share its information by July 28 and Amgen still has not received the required materials, the company said in its court filing. Amgen asserts that Sandoz communicated its intent to “sidestep” the process laid out in statute and proposed an alternative that involved sharing the application, but not the manufacturing information. “On July 28, 2014, Amgen received a letter from Defendants stating that they ‘opted not to provide Amgen with Sandoz’s biosimilar application within 20 days of the FDA’s notification of acceptance,’” according to the court filing, which cites Sandoz’s letter. “Upon information and belief, Defendants’ failure to provide their BLA and manufacturing information was an attempt to prevent Amgen from learning the details of their process(es) for manufacture, to avoid patent infringement litigation on any manufacturing patents, and to avoid the patent exchanges required by the statute; and instead to go directly to litigation.” Amgen did not agree to follow an alternative procedure, according to the company’s court filing. Sandoz later communicated that an earlier July 8 letter served as the company’s notice of commercial marketing, which is required 180 days in advance of market entry. Amgen wants the court to prevent Sandoz from marketing its biosimilar until it meets its obligations under BPCIA, stop FDA review of the application, award compensatory damages and decree that Sandoz has committed patent infringement, among other requests. — Alaina Busch McBournie Amgen Seeks FDA Requirement On Biosimilar Applicants Patent Exchange Amgen, on the heels of a lawsuit targeting key patent processes associated with the first biosimilar application, filed a citizen petition asking FDA to create a certification process to ensure that companies filing a biosimilar application commit to following statutorily outlined procedures to share application and manufacturing information. Amgen said a new administrative mechanism would prevent companies from circumventing disclosure requirements that the company asserts are mandatory. Amgen, which also develops biosimilars, Thursday (Oct. 29) filed a citizen petition asking the agency to require biosimilar applications include a certification that the sponsor will provide the reference product sponsor with a copy of the application and information describing manufacturing processes. This information exchange is the crux of a lawsuit Amgen filed the week prior against Sandoz, which seeks to copy Amgen’s Neupogen with its application for biosimilar filgrastim. “As recent events demonstrate, this Congressionally-mandated scheme is at risk of being fundamentally undermined unless FDA acts to ensure that biosimilar applicants make the requisite disclosures,” according to the citizen petition, which was filed by the law firm Sidley Austin. “Specifically, at least one biosimilar applicant has chosen to disregard its obligations under subsection (l)(2)A), and has done so by relying on the belief that the disclosure mandated by subsection (l)(2)(A) is optional.” Within 20 days of receiving notice that FDA has accepted a biosimilar application for review, the applicant must share a copy of the application, including manufacturing processes, with reference product sponsor. This sets off a series of information exchanges to determine which patents, if any, the two companies would litigate or license, with the exchange happening concurrent to FDA’s review. Amgen filed a lawsuit in the U.S. District Court for the Northern District of California on Oct. 24 alleging that Sandoz sidestepped this required process, by proposing an alternative exchange where the originator would have access to the biosimilar application, but not the manufacturing information. Amgen contends that all the information is required, and points out in the citizen petition that reference product sponsors have no other way of knowing whether any patented manufacturing processes are being infringed upon. However, Sandoz, as the first company to engage in the pathway, asserts that the two companies have different interpretations of Biologics Price Competition and Innovation Act provisions. The Amgen citizen petition asserts that Congress considered and rejected optional exchange procedures, therefore showing this information exchange is required and necessary to ensure the biosimilar pathway operates as intended. “A certification requirement for biosimilar applications can be implemented without an appreciable burden on FDA,” according to the citizen petition. “Enforcement of the certification requirement can be achieved through existing practices and procedures.” Amgen also asserts that FDA has the authority to require this certification. The company says FDA has authority to establish regulations governing the approval of biologics. Further, applications must be submitted on prescribed forms and cannot be considered filed until FDA receives the pertinent information and data, Amgen adds. “The reference to ‘pertinent information’ is broad and means that FDA may refuse to file an application based on ‘administrative incompleteness,’” Amgen says in the petition. FDA could adopt a procedural policy requiring biosimilar applications include a statement that the company will share information with the reference product sponsor within 20 18 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 days, the company says. The requirement could be implemented several ways such as a modification to Form FDA 356h, Amgen says. Industry sources said FDA would likely reject the request. One source noted there was nothing in the BPCIA that provides a basis for requiring the certification and, with debate around the law, FDA has shied away from getting involved in patent decisions. “They’re not patent attorneys,” the source noted. FDA recently unveiled the “Purple Book,” which lists biologics, determinations of biosimilarity and interchangeability, and exclusivity determinations, but not patent information. — Alaina Busch McBournie Second Round Of State Innovation Model Grants Expected This Year Karen Murphy, the director of the CMS’ State Innovation Models Initiative, says she expects the next round of SIM grants will be awarded before the end of this year. At the National Association of Medicaid Directors’ conference on Wednesday (Nov. 5), Murphy said the applications across the country have been extremely strong, and giving states a year to design their innovation proposals was extremely important in putting together sound health care innovation plans. Under the first round of SIM grants, 16 states received funding to produce a State Health Care Innovation plan, and these states are required to apply for the second round. When the second round of the SIM grants was announced by the agency’s innovation center, CMS said it planned to award as much as $700 million in funding for up to 12 state-sponsored Model Testing cooperative agreements, and up to 15 states would be chosen for as much as $30 million in Model Design work. — Michelle M. Stein Freestanding Radiation Oncologists Pleased With Physician Pay Rule Freestanding radiation oncologists are pleased with CMS’ final physician pay rule because it puts on hold a technical change, which would have cut pay by 4 percent, delays separate pay cuts for a year and lets radiation oncologists comment on pay cuts before they potentially take effect in 2016. Until now, CMS published pay rates in an annual interim final rule — a process that didn’t allow providers to comment on those rates before they take effect. At the request of physician lobbyists, many lawmakers urged CMS to instead publish pay rates in an annual proposed pay rule to give physicians an opportunity to ask for changes. CMS agreed, but it initially proposed to implement that change in the 2016 pay cycle and to stick doctors with the changes to pay rates for 2015 using the system that doesn’t allow them to argue against pay cuts. Inside Health Policy reported on Friday that CMS didn’t give radiation oncologists their way on the so-called payment-transparency policy because the final version of the rule delays implementation of that policy until 2017. Freestanding radiation therapy facilities and a few others, such as urologists, urged CMS to implement the transparency policy immediately. However, Radiation Therapy Alliance Executive Director Andrew Woods says the final rule is a win for free-standing radiation oncology practices because it also puts off 2015 pay cuts. The American Medical Association wanted to put off the transparency measure until 2017 and use temporary Gcodes in the interim. Free-standing radiation oncology practice said that approach would have led to significant pay cuts for their services. They knew that the American Medical Association’s Relative Value Scale Update Committee (RUC) proposed cuts to their services for 2015, and G-codes are based on RUC proposals. CMS compromised in the final rule by delaying the transparency process until 2017 for all services, except radiation therapy and gastroenterology. For radiation therapy and gastroenterology, CMS will begin the transparency process in the 2016 pay cycle, and CMS will not cut pay for radiation therapy or gastroenterology in 2015. Woods says free-standing radiation centers are fine with that approach. Another huge win for free-standing clinics is that CMS put on hold its proposal to remove radiation treatment vaults as a direct cost for radiation treatment codes. That technical change would have cut average Medicare reimbursement for radiation oncology services by 4 percent. The Radiation Therapy Alliance fought that proposal, and CMS says in the final rule that it needs more time to study the idea. Woods says CMS didn’t reverse itself on either the vault policy or on the pay cuts that radiation oncologists were expecting. CMS merely delayed those decisions, but in doing so it gave industry time to make its case that the pay cuts are unfair. —John Wilkerson INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014 19 As part of $6.2 billion emergency funding request... White House Proposes Millions For Ebola Treatment Clinical Trials The White House Tuesday (Nov. 5) unveiled a multi-billion dollar fiscal 2015 emergency appropriations request to support Ebola efforts, such as the development and procurement of vaccines and treatments, to combat the ongoing outbreak — with the request including $157 million for the Biomedical Advanced Research and Development Authority, $238 million for the National Institutes of Health, $1.83 billion for the Centers for Disease Control and Prevention, and $25 million for FDA. Sen. Barbara Mikulski (D-MD) said the committee would evaluate the request and convene a hearing on Nov. 12 with participation from agencies involved in stemming the outbreak. In total, the administration requested $6.18 billion across several departments “to fortify domestic public health systems, contain and mitigate the epidemic in Africa; speed the research, development, and procurement of vaccines and therapeutics; and strengthen global health security.” Of that, $4.64 billion would go toward the immediate response to the outbreak and $1.54 billion would go toward a contingency fund to “meet unforeseen changes in the epidemic.” HHS would receive $2.43 billion, according to the proposal. The administration’s request would provide $333 million for the Public Health and Social Services Emergency Fund, with $157 million of those funds going toward BARDA for manufacturing vaccines and synthetic therapeutics for clinical trials, and $10 million for Ebola virus modeling and genetic sequencing. CDC’s $1.83 billion would fund a slew of activities, including procuring personal protective equipment for the Strategic National Stockpile, supporting more than 50 Ebola treatment centers in the United States and conducting clinical trials in affected countries to evaluate candidate vaccines. NIH’s $238 million would go toward clinical trials on investigational vaccines and therapies. Within the Department of Defense, the Defense Advanced Research Projects Agency (DARPA) would receive $112 million to support technology development, such as using antibodies from survivors to provide temporary immunity until a vaccine is available. DARPA would also develop new technologies to “shorten the vaccine development timeline from years to months.” The proposed $25 million in FDA funding would be for the “development, review, regulation, and post-market surveillance of vaccine and therapies,” according to the administration’s request. The money would fund additional staff for these activities. Mikulski said she will use three principles to evaluate the funding request. She wants to target resources toward West Africa to “fight this disease at the epicenter,” protect U.S. points of entry and support scientific advances. “That means not only tasking our critical public health and safety agencies to work together to prevent the spread of Ebola, but to also develop vaccines and treatments,” she said in a statement. “Our state and local health departments, our disease detectives at the CDC, scientists at the National Institutes of Health and nurses, doctors and other health care workers are leaning into this fight. We must support them and invest in their work.” Last week Reps. Anna Eshoo (D-CA) and Mike Rogers (R-MI), who have backed legislation bolstering medical countermeasure development, asked for more BARDA funding, arguing that the agency must be well resourced because it has the infrastructure to get a drug or vaccine prepared for use in the ongoing outbreak. The 2013 Pandemic and AllHazard’s Preparedness Reauthorization Act authorized $2.8 billion for BARDA’s Project BioShield from fiscal 2014 to 2018, but the program has received $255 million – 9 percent of the five-year authorized level, the lawmakers said in asking appropriators to ensure that the program is fully funded. Research!America President and CEO Mary Woolley called on lawmakers to respond to the funding request in a bipartisan manner. “Americans expect our nation’s leaders to present a unified front against national threats, allocating the funding needed to protect our nation,” she said in a statement. “We also expect common sense, which means treating an emergency as an emergency and refraining from haphazardly cutting funding for other priorities in order to ‘pay for’ protecting the American public. Sustained investments in research are necessary to enhance our capability to fend off and prevent other major health challenges that could disrupt medical progress and create economic instability.” – Alaina Busch McBournie 20 INSIDE CMS — www.InsideHealthPolicy.com — November 6, 2014







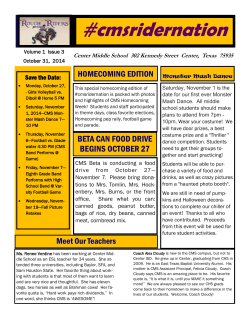
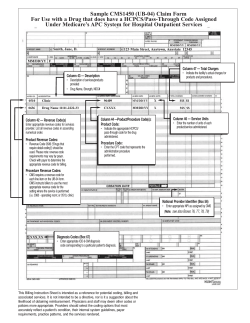

© Copyright 2026