
Propofol Pretreatment Attenuates Aquaporin-4 Over-Expression and Alleviates Cerebral Edema After
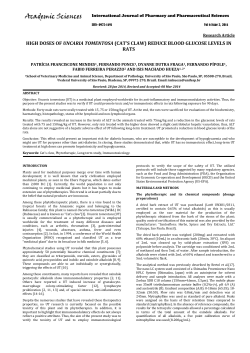
Propofol Pretreatment Attenuates Aquaporin-4 Over-Expression and Alleviates Cerebral Edema After Transient Focal Brain Ischemia Reperfusion in Rats Yue-Ying Zheng, MS* Yun-Ping Lan, MS* Hui-Fang Tang, PhD† Sheng-Mei Zhu, MD, PhD* BACKGROUND: Cerebral edema is a major threat for stroke victims. Most studies have focused on the neuroprotective activities of propofol, addressing infarct volume rather than cerebral edema. Aquaporin-4 (AQP4) plays an important role in maintaining brain water homeostasis under various neurological insults. We explored the effect of propofol pretreatment on cerebral edema in a rat model of brain ischemia reperfusion and assessed the involvement of AQP4. METHODS: To induce brain ischemia reperfusion, we introduced a silicone-coated monofilament nylon suture into the origin of the middle cerebral artery, withdrawing it after 90 min. Treatment groups (n ⫽ 32), received propofol (0.1 mL 䡠 kg⫺1 䡠 min⫺1) infusion for 30 min before occlusion; the vehicle group (n ⫽ 32) and the sham-operated group (n ⫽ 28), which received the intralipid vehicle at the same time and rate. To assess cerebral infarct volume, we used 2, 3, 5-triphenyltetrazolium chloride staining; wet– dry weight ratio was the basis for cerebral edema estimation, and we used immunohistochemistry and Western blot to detect AQP4 expression. RESULTS: The wet– dry weight ratio decreased from 86.89% ⫾ 0.71% in the vehicle group (n ⫽ 6) to 72.42% ⫾ 0.74% in the propofol group (n ⫽ 6), corresponding to an average decrease of 16%. In parallel and based on immunohistochemical semi-quantification, the propofol group exhibited remarkable attenuation of AQP4 over-expression in the ischemic border zone compared with the vehicle group: 1.28 ⫾ 0.03 vs 1.40 ⫾ 0.05, n ⫽ 7, respectively; P ⬍ 0.05. Values derived from Western blot quantification were similarly decreased in the propofol group compared to the vehicle group: 20.85% ⫾ 4.18% vs 31.67% ⫾ 3.23%, n ⫽ 4, respectively; P ⬍ 0.05. However, infarct volume and neurologic deficit in postischemic rats in the propofol group were not statistically different from values in the vehicle group. CONCLUSIONS: We conclude that prestroke treatment with propofol reduces postischemic cerebral edema in rats, possibly through inhibiting AQP4 over-expression in the boundary zone of ischemia. (Anesth Analg 2008;107:2009 –16) P ropofol (2, 6-dilsopropylphenol) is an IV anesthetic extensively used in clinical practice and characterized by its rapid induction and quick patient recovery from its effects. In addition, propofol is in widespread use as a sedative for intensive care patients. Results of in vitro From the *Department of Anesthesiology, the First Affiliated Hospital, School of Medicine, Zhejiang University, People’s Republic of China; and †Department of Pharmacology, School of Medicine, Zhejiang University, Hang Zhou, People’s Republic of China. Accepted for publication July 18, 2008. Supported by the Zhejiang Provincial Science Technology Foundation of China (No.2006C33066) and the Medical Science Research Foundation of Health Bureau of Zhejiang Province of China (No. 2007A057). Address correspondence and reprint requests to Sheng-Mei Zhu, MD, PhD, Department of Anesthesiology, The First Affiliated Hospital, School of Medicine, Zhejiang University, 79 Qingchun Road, 310003, HangZhou, People’s Republic of China. Address e-mail to [email protected]. Copyright © 2008 International Anesthesia Research Society DOI: 10.1213/ane.0b013e318187c313 Vol. 107, No. 6, December 2008 and in vivo studies are inconsistent regarding the neuroprotective activities of propofol and possible mechanisms of action; suggestions have included reduction in cerebral metabolism,1 antioxidant activity,2 antiexcitotoxic properties,3 modulation of inhibitory neurotransmitter action and excitatory neurotransmitters,4,5 or influence on neuronal apoptosis.6,7 Therefore, the impact of propofol on cerebral ischemia and its mechanism of action remain to be clarified. Cerebral edema is a serious complication in association with stroke.8,9 The sequelae are severe, with increased intracranial pressure and herniation not only aggravating neurologic outcome but also threatening life.10 Results of studies on the antiedema effect of propofol are less frequently reported. Some surgical procedures, such as carotid endarterectomy and aneurysmal clipping, carry an enhanced risk of cerebral edema; in addition, some high-risk patients with preexisting cerebrovascular disease are prone to cerebrovascular occlusion events in the perioperative period. Thus, if one of the anesthetic outcomes of propofol 2009 Figure 1. The whole experimental procedure and the flow chart. Arterial blood pressure measurement and blood sampling were performed 30 min before the onset of ischemia, 15 min after propofol administration, 15 min after ischemia and 15 min after reperfusion (A). (B) shows that 92 animals were randomized to 3 groups and further subdivided for various outcomes. administration includes alleviation of edema induced by postoperative stroke, these findings would be significant. Aquaporin-4 (AQP4), a member of the transmembrane water channel protein family, is involved in cerebral edema and brain water homeostasis. AQP4 is strongly enriched at the brain– blood and brain– cerebral spinal fluid interfaces.11,12 Changes in AQP4 in animals coincide with cerebral edema development evoked by brain ischemic reperfusion injury.13,14 AQP4 deficiency reduces cytotoxic edema resulting from focal brain ischemia or water intoxication15,16 but aggravates vasogenic cerebral edema induced by brain tumor, freeze injury, or intraparenchymal fluid infusion.17 In this study, we explored whether propofol pretreatment reduces cerebral edema in a rat model of brain ischemia reperfusion and the involvement of AQP4. METHODS The Medical Faculty Ethics Committee of Zhejiang University approved the study protocol. All experimental procedures were performed in accordance with the Guide for the Care and Use of Experimental Animals. Male Sprague-Dawley rats (230 –280 g), obtained from the Experimental Animal Center in the Zhejiang Academy of Medical Sciences, were allowed free access to water and laboratory chow before experimentation. 2010 The experimental procedure and a flow chart are showed in Figure 1. Rats were anesthetized with chloral hydrate (400 mg/kg, ip) and then allowed to breathe spontaneously in oxygen-enriched air (fraction of inspired oxygen [Fio2]: 40%) through a facemask. The left femoral artery was cannulated with a polyethylene tube for arterial blood pressure monitoring (PC-Lab, Kelong, Nanjing, China) and blood sampling, and the left femoral vein was used for drug administration. Arterial blood pH, Pao2, and Paco2 were monitored by Blood Gas Analyzer (Blood Gas Analyzer ABL 330, Leidu, Denmark) and blood glucose with a OneTouch Basic Blood Glucose Monitoring System (LifeScan). The physiological variables were recorded before the operation (as baseline), 15 min after drug exposure, 15 min after ischemia, and 15 min after reperfusion. Rectal temperature was maintained at 37.0 ⫾ 0.5°C with a heating pad throughout the surgical procedures. Rats were then randomly assigned to one of three groups. The propofol group (n ⫽ 32) received propofol (2,6-diisopropylphenol) in an intralipid emulsion (Diprivan®, Astra-Zeneca, Caponago, Milano, Italy, 10 mg/mL) IV infused at a rate of 0.1 mL 䡠 kg⫺1 䡠 min⫺1 for 30 min until the onset of the middle cerebral artery occlusion (MCAo). The vehicle group (n ⫽ 32) and the sham-operated group (n ⫽ 28) received the lipid vehicle only (Intralipid, Fresenius Kabi, Verona, Italy) at the same dose and rate. Propofol Lessens AQP-4 Over-Expression and Cerebral Edema ANESTHESIA & ANALGESIA We then prepared the animals for MCAo as previously described.18 Briefly, after a midline cervical incision, the right external carotid artery as well as its branches were carefully exposed, ligated, and cut. A 0.2-mm silicone-coated monofilament nylon suture (diameter of the round tip: 0.26 – 0.28 mm) was introduced into the right internal carotid artery through the right external carotid artery stump. We used laser Doppler flowmetry (ML191, AD Instruments Pty) to measure regional cerebral blood flow, as reported.19 A sudden decrease of regional cerebral blood flow from 100% (before ischemia) to 50% or less confirmed correct placement of the suture. Regional cerebral blood flow returned to 98% ⫾ 8% with removal of the suture 90 min after occlusion to allow reperfusion. Finally, after ligation of the right external carotid artery and closure of the skin incision, the animal recovered. After awakening from anesthesia, the animals were maintained in an air-conditioned room at 24°C. Except for the lower depth of the inserted intraluminal suture, the sham-operated animals underwent the same surgical process. At 24 h of reperfusion, a single observer blinded to group assignment put the rats through a neurologic examination, grading each animal on a scale of 0 – 4, as previously reported.18 The criteria were as follows: 0 ⫽ no observable deficit; 1 ⫽ left forelimb flexion or failure to extend fully when lifting the animal by the tail; 2 ⫽ circling to the left side but normal posture at rest; 3 ⫽ leaning to the left side at rest; 4 ⫽ unable to walk spontaneously or stroke-related death. Animals included in the subsequent study had a neurologic score ⬎1 for the rats subjected to the MCAo or ⫽ 0 for the sham-operated rats. These rats were anesthetized with chloral hydrate and decapitated. After rapid removal, the brains (n ⫽ 8 for the propofol group and the vehicle group, respectively; n ⫽ 6 for the shamoperated group) were sectioned coronally into slices 2 mm thick by a special brain matrix, then stained with 0.05% 2,3,5-triphenyl-tetrazolium chloride at 37°C for 30 min in the dark.20 After fixation of the slices in 0.1 M phosphate-buffered 10% formaldehyde for 24 h at room temperature, we used a digital camera to obtain images of the brain slices, which we traced and quantified using Image Tool 3.0. To reduce the impact of brain edema on infarct area, we subtracted the noninfarct area in the right hemisphere from the total area of the left hemisphere to obtain the infarct area in the right ischemic hemisphere in each slice.21 To calculate the total infarct volume in each brain, we multiplied the thickness (2 mm) for the infarct area of each brain slice in the same brain and then summed these values. Values used for analysis were thus the absolute total infarct volume (mm3) and the percentage of infarct brain volume over total brain volume. To quantify cerebral edema, we used the wet– dry weight method. After rapid removal 24 h after ischemia–reperfusion injury, the brains (n ⫽ 6 rats for each group) were divided into the ipsilateral and Vol. 107, No. 6, December 2008 contralateral hemispheres. Each brain tissue was placed on a piece of aluminum foil. After the wet weight of the hemisphere was measured, the tissue was dried at 110°C for 24 h to obtain the dry weight. We calculated the brain water content in the ischemic hemisphere using the following equation: %water ⫽ (wet weight ⫺ dry weight)/wet weight ⫻ 100%.22 In addition, 8-m coronal sections (beginning at the bregma and extending 4 mm caudally) were cut from each brain from the included rats (n ⫽ 8 for the propofol group and the vehicle group, respectively; n ⫽ 6 for the sham-operated group) with a cryomicrotome (CM3050, Leica, Germany) for immunohistochemical examination. After incubation with 0.3% hydrogen peroxide for 10 min, sections were blocked with 2% normal goat serum for 10 min at room temperature. Then brain sections were placed overnight at 4°C with anti-AQP4 (Chemicon; rabbit, 1/200) followed by polyperoxidase-anti-mouse/rabbit IgG (PV-900 polymer detection system, Zhongshan Biotechnology CO, China) for 1 h at 37°C. After each incubation, sections were rinsed with phosphate buffered saline for 3 ⫻ 5 min. Finally, diaminobenzidine was added to the sections. Phosphate buffered saline took the place of the primary antibody as the negative control. We used an optical microscope to photograph the diaminobenzidine staining as an indicator of immunolabeling. To semi-quantify AQP4 expression, we used optical density (OD) measurements in three different fields in both the border region of ischemia and the corresponding part of the contralateral hemisphere (⫻200). A pathological image analysis system allowed detection of the OD (Hpias-1000, Wuhan, China), which we used to calculate a ratio of OD between the ischemia hemisphere and the contralateral hemisphere, as reported.13 An independent observer from the pathology department performed the measurements. To quantify AQP4 expression further, we performed Western blot analysis. At 24 h of reperfusion, cortical brain tissues from the boundary zone adjacent to the ischemic core in both the propofol and vehicle groups were dissected on ice as described23 and stored at ⫺70°C until use; the corresponding tissue in the sham-operated group was also dissected (n ⫽ 4 rats for each group). Tissues were homogenized using a Polytron homogenizer in RIPA buffer (Kangchen Biotechnology, Shanghai, China) containing protease inhibitor cocktail (P8340, Sigma). After homogenization and centrifugation at 12000g at 4°C for 30 min, the resultant supernatant was collected. Protein samples (50 g) were subjected to 12% Sodium dodecyl sulfatepolyacrylamide gel electrophoresis and transferred to nitrocellulose membranes. The membranes were blocked by 5% fat-free milk, then incubated with a rabbit polyclonal antibody against AQP4 (Chemicon; 1/500) or a rabbit monoclonal antibody against -actin (Sigma; 1/1000) in Tris-Buffered Saline Tween-20 © 2008 International Anesthesia Research Society 2011 Table 1. Summary of Physiological Parameters at Sampling Time Points Variables MAP (mm Hg) Baseline 15 min after 15 min after 15 min after Pao2 (mm Hg) Baseline 15 min after 15 min after 15 min after Paco2 (mm Hg) Baseline 15 min after 15 min after 15 min after Glucose (g/L) Baseline 15 min after 15 min after 15 min after pH Baseline 15 min after 15 min after 15 min after Sham group (n ⫽ 6) Vehicle group (n ⫽ 6) Propofol group (n ⫽ 5) drug exposure ischemia reperfusion 123 ⫾ 3 119 ⫾ 3 116 ⫾ 6 117 ⫾ 4 119 ⫾ 8 121 ⫾ 5 123 ⫾ 2 118 ⫾ 9 118 ⫾ 7 109 ⫾ 4 115 ⫾ 9 128 ⫾ 7 drug exposure ischemia reperfusion 146 ⫾ 6 137 ⫾ 3 135 ⫾ 2 142 ⫾ 5 139 ⫾ 2 141 ⫾ 3 133 ⫾ 2 136 ⫾ 3 140 ⫾ 4 135 ⫾ 3 136 ⫾ 5 144 ⫾ 7 drug exposure ischemia reperfusion 43.2 ⫾ 1.7 41.0 ⫾ 1.5 42.7 ⫾ 1.9 43.5 ⫾ 1.6 44.8 ⫾ 1.5 40.6 ⫾ 1.3 40.0 ⫾ 1.6 42.9 ⫾ 1.4 44.7 ⫾ 1.8 42.2 ⫾ 1.5 44.0 ⫾ 1.6 40.1 ⫾ 2.0 drug exposure ischemia reperfusion 6.05 ⫾ 0.98 6.24 ⫾ 0.98 6.12 ⫾ 0.62 6.19 ⫾ 0.74 5.65 ⫾ 0.30 5.89 ⫾ 0.44 6.15 ⫾ 0.39 5.99 ⫾ 0.40 5.95 ⫾ 0.40 6.23 ⫾ 0.27 6.32 ⫾ 0.19 5.92 ⫾ 0.40 drug exposure ischemia reperfusion 7.38 ⫾ 0.02 7.36 ⫾ 0.02 7.34 ⫾ 0.03 7.35 ⫾ 0.01 7.34 ⫾ 0.03 7.40 ⫾ 0.03 7.36 ⫾ 0.02 7.38 ⫾ 0.01 7.40 ⫾ 0.04 7.38 ⫾ 0.03 7.36 ⫾ 0.02 7.35 ⫾ 0.01 Values are expressed as mean ⫾ SEM. Repeated-measures ANOVA with the Least. Significant Difference Post Hoc test was used. MAP ⫽ mean arterial blood pressure; PaO2 and PaCO2 the pressure of O2 and CO2 in arterial blood. overnight at 4°C. After washing, the membranes were reacted with the horseradish peroxidase-conjugated antirabbit IgG (1:1000, Zhongshan, China) for 2 h at room temperature. Immunoreactive bands were visualized by ECL chemiluminescence (ECL Kit, Santa Cruz Biotechnology) and exposed on radiograph film to reveal the AQP4 band (30 kDa) and -actin (43 kDa). The integrated densities value was analyzed with a computerized image analysis system (Gel-pro Analyzer 4.0, Media Cybernetics). The results of AQP4 expression were expressed as the percentage change over -actin. The sample size calculation was based on previous studies. The primary end-point of the study was wet– dry weight ratio. Paczynski et al.,24 in a rat model of ischemic stroke, showed that the mean and standard deviation of wet-dry weight ratio was 83.3% and 0.85%, respectively. We assumed that propofol can reduce cerebral edema assessed by wet-dry weight ratio by 2%. Based on these data, a sample size of 5 rats was needed for each group to detect a difference of 2% among the 3 groups with a type I error of 0.05 and a power of 0.85, using Turkey HSD test. Allowing for possible dropouts, we chose to use six rats for each group. We arbitrarily chose a similar sample size for the other subgroups. Statistical analysis was performed among propofol, vehicle and sham-operated groups and their respective subgroups with the statistical software (SPSS 13.0 for Windows, SPSS). Data are presented as Mean ⫾ 2012 sem. We used one-way analysis of variance (ANOVA) followed with the Least Significant Difference Post Hoc test for most parameters, except that we compared the neurological deficit scores with the nonparametric Mann-Whitney U-test, the physiological parameters with repeated measures ANOVA with the Least Significant Difference Post Hoc test, and mortality using the 2 test. A P value ⬍0.05 was considered statistically significant. RESULTS Table 1 shows the physiologic variables. Propofol pretreatment decreased mean arterial blood pressure 15 min after propofol infusion, but the change was not statistically significant. Arterial blood gas variables and blood glucose concentrations among the three groups at all sampling points also did not differ significantly. Of the original 92 animals, 3 died before the following examination: 1 in the vehicle group (3% mortality) and 2 in the propofol group (6% mortality). In addition, we excluded one rat each from the propofol group and the vehicle group because of failure to meet the neurologic deficit score criteria. The neurologic evaluation of rats at 24 h after transient MCAo reperfusion revealed that, compared with the vehicle (n ⫽ 6), propofol pretreatment (n ⫽ 6) tended to improve the neurologic outcome, but the difference did not rise to the level of statistical significance (P ⫽ 0.165, Mann-Whitney U-test). Propofol Lessens AQP-4 Over-Expression and Cerebral Edema ANESTHESIA & ANALGESIA DISCUSSION Figure 2. Effects of propofol pretreatment on edema formation induced by ischemia reperfusion injury in rats. Brain edema was determined by the increase of ischemic hemisphere water content (n ⫽ 6 for each group). Results are expressed as mean ⫾ sem *P ⬍ 0.05 versus sham operation group; **P ⬍ 0.01 versus sham operation group; #P ⬍ 0.05 vs vehicle group; ##P ⬍ 0.01 versus vehicle group; one-way ANOVA. We found no statistical differences between the vehicle and propofol groups in absolute infarct volume (278.97 ⫾ 36.25 mm3, n ⫽ 7 vs 223.3 ⫾ 67.37 mm3, n ⫽ 7, one-way ANOVA, P ⫽ 0.351) or in the percentage of nonviable tissue volume over the total brain volume (17.05% ⫾ 1.20% vs 13.77% ⫾ 3.87%, P ⫽ 0.241), which we calculated by measuring consecutive coronal slices stained by 2,3,5-triphenyl-tetrazolium chloride. The ischemic hemisphere in the propofol group exhibited a significantly lower water content increase compared with vehicle: 72.42% ⫾ 0.74% vs 86.89% ⫾ 0.71%, (P ⫽ 0.000; one-way ANOVA, n ⫽ 6 rats/group; Fig. 2), corresponding to an average decrease of 16%. In Figure 3B(a– c), representative low-magnification pictures show expression of AQP4 mainly on astrocytic endfeet around brain vessels, with changes in expression in the border zone of the lesion after brain ischemia-reperfusion injury. The borders of the ischemia are represented in a schematic drawing (Fig. 3A). The OD ratio in the vehicle group (n ⫽ 7) was significantly higher than in the sham-operated group (n ⫽ 6). However, the ratio in the propofol group (n ⫽ 7) was significantly smaller compared to that of the vehicle group (1.28 ⫾ 0.03 vs 1.40 ⫾ 0.05, P ⫽ 0.02, one-way ANOVA, Fig. 3C). Western blot analysis confirmed the immunohistochemistry results, showing the AQP4 protein as a single 30-kDa band (Fig. 4A). Control blots without primary antibody to AQP4 showed no specific AQP4 bands (data not shown). Compared with shamoperated rats, AQP4 protein concentration in the boundary zone of the lesion increased significantly at 24 h after reperfusion in both the vehicle and propofol groups. Propofol pretreatment markedly reduced AQP4 over-expression compared with intralipid vehicle treatment (20.85% ⫾ 4.18% vs 31.67% ⫾ 3.23%, P ⫽ 0.041, one-way ANOVA; n ⫽ 4 for each group; Fig. 4B). Vol. 107, No. 6, December 2008 Our objective was to characterize the effects of propofol pretreatment prior to ischemia in inhibiting formation of brain edema. We used MCAo as an experimental model to induce brain edema and found that MCAo-90 min followed by reperfusion for 24 h elicited brain edema and upregulated AQP4 expression in the penumbra region. Propofol infusion before ischemia ameliorated brain edema and attenuated AQP4 over-expression. However, we did not observe that propofol significantly improved neurologic deficits or decreased brain infarct volumes. According to previous reports, 24-h postischemia is the time of peak edema,25 leading us to choose this time point for our study. AQP4 is a bidirectional water channel protein, concentrated in cerebral spinal fluid– brain and blood-brain interfaces. Our study showed that MCAo-90 min and reperfusion at 24 h caused AQP4 upregulation in rats, as detected by immunochemistry and Western blot analysis. However, others have also demonstrated changes in AQP4 levels after ischemia using other models. In a model of MCAo-30 min in mice, AQP4 over-expression in the periinfarct zone was not significant at 24 h after reperfusion but was at 48 h.13 AQP4 expression conversely decreased 23 h after brain transient ischemia 90 min.26 These varying results may have been from differences in species used (mouse versus rat), age of animals studied (young versus adult), or the severity of the ischemia and reperfusion (different duration in ischemia or reperfusion). Meanwhile, we identified AQP4 down-regulation in a rat MCAo model in the propofol group accompanied by an obvious reduction in cerebral edema. According to the classification of cerebral edema based on the pathophysiologic mechanism, cytotoxic edema develops by the time point of reperfusion at 24 h.27 Others have speculated that AQP4 over-expression enhances a rapid influx of water and is responsible for the development of cytotoxic edema after focal brain ischemia28; thus, AQP4 downregulation may alleviate cerebral edema. No studies of which we are aware have clearly connected the action of propofol and AQP4. The mechanism may involve reversible protein phosphorylation and amino acid neurotransmitters. Protein kinase C is one of the potential phosphorylation sites of AQP4, and water permeability activity alters with its phosphorylation.29 Protein kinase C activator inhibited ischemia-induced up-regulation of AQP4 and attenuated brain swelling in a MCAo model 30 Moreover, protein kinase C–mediated protein phosphorylation is a target for general anesthetic effects in the central nervous system, including propofol.31 Therefore, protein kinase C can reasonably be suggested as a possible key location for propofol regulation of AQP4 expression during brain ischemia-reperfusion injury. © 2008 International Anesthesia Research Society 2013 Figure 3. Effects of propofol pretreatment on aquaporin-4 (AQP4) expression at 24 h after middle cerebral artery occlusion (MCAo) reperfusion in rats. (A) The boxes in the schematic drawing represent the areas selected as the border of the lesion. (B) Representative low-magnification images illustrate AQP4 immunohistochemical staining in the ischemic boundary zone of an injured animal that received the intralipid vehicle (a, n ⫽ 7), an injured animal that received propofol (b, n ⫽ 7), and a sham-operated animal that received intralipid (c, n ⫽ 6). “Phosphate buffered saline” is a negative control (d). (C) AQP4 expression was evaluated by calculating the ratio of the optical density of AQP4 immunolabeling in the ischemic hemisphere (ISCH) and in the control hemisphere (CTL). The ratio for AQP4 in the propofol group significantly decreased compared with the vehicle group. Results are mean ⫾ sem **P ⬍ 0.01 versus sham-operated group; #P ⬍ 0.05 versus vehicle group, one-way ANOVA. Figure 4. Effects of propofol pretreatment on aquaporin-4 (AQP4) expression as revealed by Western blot (A, n ⫽ 4 for each group); data are summarized in (B). The AQP4 band migrated at 30 kDa, and AQP4 expression was downregulated with infusion of propofol at a rate of 0.1 mL 䡠 kg⫺1 䡠 min⫺1 prior to ischemia compared with intralipid administration (“vehicle”). Results are expressed as mean ⫾ sem *P ⬍ 0.05 versus sham-operated group, #P ⬍ 0.05 versus vehicle group, one-way ANOVA. 2014 Another related factor may be the amino acid neurotransmitter, glutamate. One study showed that astrocytic swelling that glutamate elicited seemed to correlate with AQP4.32 Knock-out AQP4 in mice results in altered glutamate levels in the brain.33 Nevertheless, propofol could decrease extracelluar glutamate levels by many possible mechanisms.34 –36 Glutamate might therefore be another factor in the mechanism by which propofol regulates AQP4 expression. These ideas need to be further verified in vitro and in vivo. We did not identify a significant neuroprotective role of propofol, a finding consistent with the results of Ridenour et al.37 They demonstrated that propofol had no greater neuroprotective effect than their halothane control, which was not recognized as a neuroprotectant. In contrast, other authors have reported that propofol pretreatment reduced infarct area and improved neurologic deficits after incomplete ischemia-reperfusion injury.1,38 Again, differences in species, study models, baseline anesthetics, and the timing and dose of infused propofol may explain these discrepancies. Further study is necessary to optimize Propofol Lessens AQP-4 Over-Expression and Cerebral Edema ANESTHESIA & ANALGESIA the propofol dose, the time and the sample size to achieve maximum benefit. In addition, another possible explanation for the differences could be neurologic scoring. Although the neurologic scoring used here has been extensively applied, it has never been validated for it seems able to differentiate among various infarct volumes.39 A six-point neuro-scoring displayed a more significant correlation with infarct volume40 and might be more suitable for such studies. Meanwhile, a slightly later observation time might improve evaluation of the neuroprotective potential of propofol.40 We used rectal temperature monitoring in this experiment because transcranial temperature measuring was not available. Pericranial temperature monitoring is more suitable than rectal temperature in terms of experimental neuroprotection41; however, because core temperature stayed within a narrow range among the three groups, we infer that there would be no difference in the brain-to-core-temperature relationship among the groups. Because there is no absolute relationship between the electroencephalographic suppressive effect and the neuroprotective effect of propofol,5 we did not monitor electrical status. In conclusion, regulation of AQP4 levels could be an important mechanism in maintaining brain water homeostasis. Propofol pretreatment exerts an antiedema effect in rats in a MCAo model, an effect that is partly correlated with AQP4 down-regulation in the border of the infarct zone. This study may open new avenues of investigation into the antiedema effect of propofol. ACKNOWLEDGMENTS We thank Dr. Wei-Zhong Gu for assisting in analyzing immunohistological results and Yu Zhou for establishing the MCAo model in the rat. REFERENCES 1. Kochs E, Hoffman WE, Werner C, Thomas C, Albrecht RF, Schulte am Esch J. The effects of propofol on brain electrical activity, neurologic outcome, and neuronal damage following incomplete ischemia in rats. Anesthesiology 1992;76:245–52 2. Ergun R, Akdemir G, Sen S, Tasci A, Ergungor F. Neuroprotective effects of propofol following global cerebral ischemia in rats. Neurosurg Rev 2002;25:95– 8 3. Hans P, Bonhomme V, Collette J, Albert A, Moonen G. Propofol protects cultured rat hippocampal neurons against N-methylD-aspartate receptor-mediated glutamate toxicity. J Neurosurg Anesthesiol 1994;6:249 –53 4. Ito H, Watanabe Y, Isshiki A, Uchino H. Neuroprotective properties of propofol and midazolam, but not pentobarbital, on neuronal damage induced by forebrain ischemia, based on the GABAA receptors. Acta Anaesthesiol Scand 1999;43:153– 62 5. Wang J, Yang X, Camporesi CV, Yang Z, Bosco G, Chen C, Camporesi EM. Propofol reduces infarct size and striatal dopamine accumulation following transient middle cerebral artery occlusion: a microdialysis study. Eur J Pharmacol 2002;452: 303– 8 6. Englelhard K, Werner C, Eberspacher E, Pape M, Stegemann U, Kellermann K, Hollweck R, Hutzler P, Kochs E. Influence of propofol on neuronal damage and apoptotic factors after incomplete cerebral ischemia and reperfusion in rats: a long-term observation. Anesthesiology 2004;101:912–7 Vol. 107, No. 6, December 2008 7. Iijima T, Mishima T, Akagawa K, Iwao Y. Neuroprotective effect of propofol on necrosis and apoptosis following oxygen-glucose deprivation–relationship between mitochondrial membrane potential and mode of death. Brain Res 2006;1099:25–32 8. Bounds JV, Wiebers DO, Whisnant JP, Okazaki H. Mechanisms and timing of deaths from cerebral infarction. Stroke 1981;12: 474 –77 9. Steiner T, Ringleb P, Hacke W. Treatment options for large hemispheric stroke. Neurology 2001;57(Suppl 1):S61—S68 10. Unterberg AW, Stover J, Kress B, Kiening KL. Edema and brain trauma. Neuroscience 2004;129:1021–9 11. Rash JE, Yasumura T, Hudson CS, Aqre P, Nielsen S. Direct immunogold labeling of aquaporin-4 in square arrays of astrocyte and ependymocyte plasma membranes in rat brain and spinal cord. Proc Natl Acad Sci USA 1998;95:11981– 6 12. Verkman AS. Aquaporin water channels and endothelial cell function. J Anat 2002;200:617–27 13. Ribeiro Mde C, Hirt L, Bogousslavsky J, Regli L, Badaut J. Time course of Aquaporin expression after transient focal cerebral ischemia in mice. J Neurosci Res 2006;83:1231– 40 14. Taniguchi M, Yamashita T, Kumura E, Tamatani M, Kobayashi A, Yokawa T, Maruno M, Kato A, Ohnishi T, Kohmura E, Tohyama M, Yoshimine T. Induction of aquaporin-4 water channel mRNA after focal cerebral ischemia in rat. Brain Res Mol Brain Res 2000;78:131–7 15. Manley GT, Fujimura M, Ma T, Noshita N, Filiz F, Bollen AW, Chan P, Verkman AS. Aquaporin-4 deletion in mice reduces brain edema after acute water intoxication and ischemic stroke. Nat Med 2000;6:159 – 63 16. Manley GT, Binder DK, Papadopoulos MC, Verkman AS. New insights into water transport and edema in the central nervous system from phenotype analysis of aquaporin-4 null mice. Neuroscience 2004;129:983–91 17. Papadopoulos MC, Manley GT, Krishna S, Verkman AS. Aquaporin- 4 facilitates reabsorption of excess fluid in vasogenic brain edema. FASEB J 2004;18:1291–3 18. Longa EZ, Weinstein PR, Carlson S, Cummins R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989;20:84 –91 19. Zhou Y, Wei EQ, Fang SH, Chu LS, Wang ML, Zhang WP, Yu GL, Ye YL, Lin SC, Chen Z. Spatio-temporal properties of 5-lipoxygenase expression and activation in the brain after focal cerebral ischemia in rats. Life Sci 2006;79:1645–56 20. Joshi CN, Jain SK, Murthy PS. An optimized triphenyltetrazolium chloride method for identification of cerebral infarcts. Brain Res Brain Res Protoc 2004;13:11–17 21. Lin TN, He YY, Wu G, Khan M, Hsu CY. Effect of brain edema on infarct volume in a focal cerebral ischemia model in rats. Stroke 1993;24:117–21 22. Zhan C, Yang J. Protective effects of isoliquiritigenin in transient middle cerebral artery occlusion-induced focal cerevral ischemia in rats. Pharmacol Res 2006;53:303–9 23. Yokota C, Kaji T, Kuge Y, Inoue H, Tamaki N, Minematsu K. Temporal and topographic profiles of cyclooxygenase-2 expression during 24 h of focal brain ishemia in rats. Neurosci Lett 2004;357:219 –22 24. Paczynski RP, Venkatesan R, Diringer MN, He YY, Hsu CY, Lin W. Effects of fluid management on edema volume and midline shift in a rat model of ischemic stroke. Stroke 2000;31:1702– 8 25. Gueniau C, Oberlander C. The kappa opioid agonist niravoline decreases brain edema in the mouse middle cerebral artery occlusion model of stroke. J Pharmacol Exp Ther 1997;282:1– 6 26. Amiry-Moghaddam M, Otsuka T, Hurn PD, Traystman RJ, Haug FM, Froehner SC, Adams ME, Neely JD, Agre P, Ottersen OP, Bharedwei A. An alpha-syntrophin-dependent pool of AQP4 in astroglial end-feet confers bidirectional water flow between blood and brain. Proc Natl Acad Sci USA 2003;100: 2106 –11 27. Rosenbeg GA, Estrada EY, Dencoff JE. Matrix metalloproteinases and TIMPs are associated with blood-brain barrier opening after reperfusion in rat brain. Stroke 1998;29:2189 –95 28. Yu GL, Wei EQ, Zhang SH, Xu HM, Chu LS, Zhang WP, Zhang Q, Chen Z, Mei RH, Zhao MH. Montelukast, a cysteinyl leukotriene receptor-1 antagonist, dose- and time-dependently protects against focal cerebral ischemia in mice. Pharmacology 2005;73:31– 40 29. Gunnarson E, Zelenina M, Aperia A. Regulation of brain aquaporins. Neuroscience 2004;129:947–55 © 2008 International Anesthesia Research Society 2015 30. Kleindienst A, Fazzina G, Amorini AM, Dunbar JG, Glisson R, Marmarou A. Modulation of AQP4 expression by the protein kinase C activator, phorbol myristate acetate, decreases ischemia-induced brain edema. Acta Neurochir Suppl 2006;96:373–7 31. Hemmings HC Jr, Adamo AI, Hoffman MM. Biochemical characterization of the stimulatory effects of halothane and propofol on purified brain protein kinase C. Anesth Analg 1995;81:1216 –22 32. Han BC, Koh SB, Lee EY, Seong YH. Regional difference of glutamate-induced swelling in cultured rat brain astrocytes. Life Sci 2004;76:573– 83 33. Fan Y, Zhang J, Sun XL, Gao L, Zeng XN, Ding JH, Cao C, Niu L, Hu G. Sex and region- specific alterations of basal aminoacid and monoamino in the brain of AQP4 knock– out mice. J Neurosci Res 2005;82:458 – 64 34. Yamakura T, Sakimura K, Shimoji K, Mishina M. Effects of propofol on various AMPA-, kainate- and NMDA-selective glutamate receptor channels expressed in Xenopus oocytes. Neurosci Lett 1995;188:187–90 35. Lingamaneni R, Birch ML, Hemmings HC Jr. Widespread inhibition of sodium channel– dependent glutamate release from isolated nerve terminals by isoflurane and propofol. Anesthesiology 2001;95:1460 – 6 2016 36. Sitar SM, Hanifi-Moghaddam P, Gelb A, Cechetto DF, Siushansian R, Wilson JX. Propofol prevents peroxide-induced inhibition of glutamate transport in cultured astrocytes. Anesthesiology 1999;90:1446 –53 37. Ridenour TR, Warner DS, Todd MM, Gionet TX. Comparative effects of propofol and halothane on outcome from temporary middle cerebral artery occlusion in the rat. Anesthesiology 1992;76:807–12 38. Lee Y, Chung C, Oh YS. Effectiveness of porpofol pretreatment on the extent of deranged cerebral mitochondrial oxidative enzyme system after incomplete forebrain ischemia/ reperfusion in rats. J Korean Med Sci 2000;15:627–30 39. Nedelmann M, Wilhelm-Schwenkmezger T, Alessandri B, Heimann A, Schneider F, Eicke BM, Dieterich M, Kempski O. Cerebral embolic ischemia in rats: correlation of stroke severity and functional deficit as important outcome parameter. Brain Res 2007;1130:188 –96 40. Zausinger S, Hungerhuber E, Baethmann A, Reulen H, SchmidElsaesser R. Neurological impairment in rats after transient middle cerebral artery occlusion: a comparative study under various treatment paradigms. Brain Res 2000;863:94 –105 41. Busto R, Dietrich WD, Globus MY, Valdés I, Scheinberg P, Ginsberg MD. Small differences in inraischemic brain temperature critically determine the extent of ischemic neuronal injury. J Cereb Blood Flow Metab 1987;7:729 –38 Propofol Lessens AQP-4 Over-Expression and Cerebral Edema ANESTHESIA & ANALGESIA











© Copyright 2026